 Morgane Jaloustre1
Morgane Jaloustre1 Robert Cohen1,2,3
Robert Cohen1,2,3 Valérie Biran4
Valérie Biran4 Fabrice Decobert1
Fabrice Decobert1 Richard Layese5,6Etienne Audureau5,6
Richard Layese5,6Etienne Audureau5,6 Nolwenn Le Saché7Marie Chevallier8Mohamed Riadh Boukhris9Pascal Bolot10
Nolwenn Le Saché7Marie Chevallier8Mohamed Riadh Boukhris9Pascal Bolot10 Laurence Caeymaex1,2,†Manon Tauzin1*†with the SEPREVEN study Group‡
Laurence Caeymaex1,2,†Manon Tauzin1*†with the SEPREVEN study Group‡
- 1Neonatal Intensive Care Unit, Centre Hospitalier Intercommunal de Creteil, Creteil, France
- 2Faculty of Medicine, University Paris Est Creteil, Creteil, France
- 3Groupe de Pathologie Infectieuse Pédiatrique, Paris, France
- 4Neonatal Intensive Care Unit, APHP, CHU Robert Debré, Paris, France
- 5Assistance Publique-Hôpitaux de Paris AP-HP, Hôpital Henri Mondor, Unité de Recherche Clinique (URC Mondor), Creteil, France
- 6University Paris Est Creteil, INSERM, IMRB, CEpiA Team, Creteil, France
- 7Pediatric Intensive Care and Neonatal Medicine, Bicêtre Hospital, AP-HP, Le Kremlin-Bicêtre, France
- 8Neonatal Intensive Care Unit, CHU Grenoble Alpes, Grenoble, France
- 9Department of Neonatology, CHU Lille, Lille, France
- 10Neonatal Intensive Care Unit, Centre Hospitalier de Saint-Denis, Saint-Denis, France
Background: Health care-associated primary bloodstream infections (BSIs), defined as not secondary to an infection at another body site, including central line-associated BSI, are a leading cause of morbidity and mortality in patients in neonatal intensive care units (NICUs). Our objective was to identify factors associated with severe morbidity and mortality after these infections in neonates in NICUs.
Methods: This ancillary study of the SEPREVEN trial included neonates hospitalized ≥2 days in one of 12 French NICUs and with ≥ 1 BSI during the 20-month study period. BSIs (all primary and health care-associated) were diagnosed in infants with symptoms suggestive of infection and classified prospectively as possible (one coagulase-negative staphylococci (CoNS)-growing blood culture) or proven (two same CoNS, or ≥1 recognized pathogen-growing blood culture). BSI consequences were collected prospectively as moderate morbidity (antibiotic treatment alone) or severe morbidity/mortality (life-saving procedure, permanent damage, prolonged hospitalization, and/or death).
Results: Of 557 BSIs identified in 494 patients, CoNS accounted for 378/557 (67.8%) and recognized bacterial or fungal pathogens for 179/557 (32.1%). Severe morbidity/mortality was reported in 148/557 (26.6%) BSIs. Independent factors associated with severe morbidity/mortality were corrected gestational age <28 weeks (CGA) at infection (P < .01), fetal growth restriction (FGR) (P = .04), and proven pathogen-related BSI vs. CoNS-related BSI (P < .01). There were no differences in severe morbidity and mortality between proven and possible CoNS BSIs. In possible BSI, S. epidermidis was associated with a lower risk of severe morbidity than other CoNS (P < .01), notably S. capitis and S. haemolyticus.
Conclusions: In BSIs in the NICU, severe morbidity/mortality was associated with low CGA at infection, FGR, and proven pathogen-related BSIs. When only one blood culture was positive, severe morbidity/mortality were less frequent if it grew with S. epidermidis compared to other CoNS. Further studies to help distinguish real CoNS BSIs from contaminations are needed.
Study registration: ClinicalTrials.gov (NCT02598609).
Introduction
Neonates have a high risk of adverse events during their hospitalization in intensive care units (NICUs). Health care-associated infections (HAIs) are the most frequent adverse event in care (1). Extremely preterm neonates are particularly susceptible to HAIs, with a reported incidence around 40% (2, 3). Many studies have demonstrated the association between HAI risk and preterm birth or low birth weight (4–8).
Health care-associated primary bloodstream infections (BSIs), as defined by the US Centers for Disease Control and Prevention (9), are infections acquired at least 2 calendar days after admission and are BSIs that are not secondary to an infection at another body site. Because all BSIs in this study are primary and health-care associated, we will for simplicity's sake refer to them simply as BSI. Health care-associated primary BSIs account for more than half the proven neonatal HAIs (around 57%) (10) and are often associated with a central line (4, 11). Blood cultures remain the mainstay for the diagnosis of these BSI. Nonetheless, proven BSIs are often underestimated in neonates, especially in premature patients, due to blood sampling difficulties and their small intravascular blood volume. The blood volume sampled is often limited, and drawing blood for only one culture before starting antibiotic therapy is frequent.
In low birth weight neonates, sepsis is associated with a higher risk of mortality and morbidity, such as adverse neurodevelopmental outcomes and bronchopulmonary dysplasia, more ventilator days, and extended lengths of stay (6, 12–14).
The organisms involved in BSIs have been extensively described in developed countries: coagulase-negative staphylococci (CoNS) are responsible for 21% to 78% of HAIs, followed by Gram-negative bacilli (15%–33%), Staphylococcus aureus (8%–17%), Enterococcus spp. (3%–16%), and fungi (4%–12%) (6, 15–20). Nonetheless, the outcomes related to BSIs in NICU patients have not been fully described according to the organism involved and the patients’ characteristics. Studies have shown higher morbidity and mortality associated with Gram-negative compared to Gram-positive sepsis (6, 21, 22). Among preterm neonates, however, several studies have shown that CoNS BSI may also be associated with significant morbidity (12, 23, 24).
The SEPREVEN trial (25) was a stepped-wedge randomized controlled trial that evaluated the impact of an educational program on the rate of adverse events in NICUs. The main result of this trial was that a multiprofessional safety-promoting program in NICUs reduced the rate of adverse events. HAIs accounted for one of the most frequent categories of adverse events, and the trial collected outcomes related to these infections. The primary objective of this ancillary analysis was to identify factors associated with severe morbidity and mortality related to HAI BSI in neonates receiving intensive care. The secondary objectives were to describe the BSIs: the organisms involved and the risk factors associated with persistent HAI BSI.
Materials and methods
Study design and population
This was an ancillary study of the SEPREVEN trial (25), which took place between November 23, 2015, and November 2, 2017, in 12 French NICUs. Patients included in this study were hospitalized in one of the 12 participating NICUs for more than 2 days, with a corrected gestational age (GA) ≤ 42 weeks on admission, whose parents, after information, did not oppose use of their data, and who had one or more BSIs in the NICU during the SEPREVEN 20-month study period. We excluded cases where blood cultures grew two or more different commensal organisms or an unknown organism and cases where one blood culture grew a CoNS with a treatment that lasted less than 5 days.
Data collection and definitions
Health-care associated primary BSIs were defined according to the Centers for Disease Control and Prevention 2015 definition as laboratory-confirmed BSIs that were not secondary to an infection at another body site (9). We included all health care associated primary BSIs in the study and, among them, we distinguished central line-associated BSI (CLABSI), according to the US Centers for Disease Control and Prevention 2015 definition: a laboratory-confirmed BSI with an eligible central line in place for more than two consecutive calendar days and on the date of event or the day before (9).
For descriptive purposes, we distinguished three types of BSIs: (i) BSIs with one blood culture growing a recognized bacterial or fungal pathogen (proven pathogen-related BSI); (ii) BSIs with clinical symptoms of infection and two or more blood cultures collected on separate occasions growing the same common commensal organism such as coagulase-negative staphylococci (proven commensal-related BSI); and iii) BSIs with only one blood culture growing a common commensal organism with clinical symptoms or signs compatible with infection and at least 5 days of antibiotic treatment (possible commensal-related BSI) (9). Because only one blood culture is often drawn before starting antibiotic treatment in neonates, we considered possible BSIs (6).
We included all health care associated primary BSIs in the study and we distinguished central line-associated BSI (CLABSI), according to the US Centers for Disease Control and Prevention 2015 definition: a laboratory-confirmed BSI with an eligible central line in place for more than two consecutive calendar days and on the date of event or the day before (9).
For each BSI, a physician, using a specific questionnaire, prospectively collected the following data: the patient's clinical characteristics and bacteriological data (clinical symptoms, organism involved, number and timing of blood samples, resistance status for Gram-negative bacilli and S. aureus, time to positivity of blood culture). Patient's overall characteristics were collected prospectively within the SEPREVEN trial data collection.
Early removal of a central line was defined as removal on the day or day after antibiotic treatment started; all other cases were late removal or no removal. Persistent bacteremia was defined by a blood culture positive for the same organism after at least one day of antibiotic treatment.
Outcomes
The physician prospectively graded the BSI consequences, according to the MCC MERP classification for medical error (26). Morbidity related to BSI was considered moderate if the consequence was only an antibiotic prescription (with or without use of noninvasive ventilation), or severe if the consequence included any of the following: a life-saving procedure (intubation, vasopressor drugs, chest compressions, or inhaled nitric oxide) and/or an extended length of stay in the hospital, and/or possible permanent damage (such as cystic periventricular leukomalacia), and/or contribution to death (26). Only the most severe consequence was collected.
Analyses
Data are presented as medians [interquartile ranges, IQR] or means ± standard deviations (SD) for quantitative (continuous) variables and as numbers (percentages) for categorical variables. To compare characteristics between groups, we used Student t- or Mann-Whitney tests for quantitative variables and chi-square/Fisher exact tests for qualitative variables, as appropriate. To identify factors associated with severe morbidity/mortality and those associated with persistent bacteremia after initiation of antibiotic therapy, we conducted univariate and multivariate analyses using a mixed effect logistic regression model, with center and patient levels as random effects. The factors we studied were gestational age at birth, corrected gestational age at infection, sex, birth weight, type of BSI, FGR at birth (yes/no), time to positivity of blood culture, CLABSI, and catheter removal (early/late).
Factors associated with persistent bacteremia after initiation of antibiotic therapy were sought among the following: gestational age at birth, birth weight, sex, postnatal age at first positive blood culture (in days), time to positivity of blood culture (< or ≥ 12 h and < or ≥ 24 h), early removal of central line (yes/no), type of BSI, and presence of central line on the date of persistent positive blood culture (yes/no). Factors associated with the outcome at a P-value < .20 in the univariate analysis were entered into the multivariate analysis. We then applied a backwards stepwise approach to retain factors significant at the P < .05 level until we obtained a final model for each outcome.
The association between severe morbidity/mortality and the organism involved was studied for each type of BSI. All analyses were conducted with Stata software (v 16). A P-value of.05 was considered significant.
Ethics
The SEPREVEN study was approved by the National Data Protection Authority (CNIL no 915263) and the relevant ethics committees (Consultative Committee on the Treatment of Data on Personal Health for research Purposes, France CCTIRS no 15327, and the Committee for the Protection of People Participating in Biomedical Research CPP Ile-de-France III, France, no ID RCB: 2014-A01751-46). The trial registration number was NCT 02598609. Parents were informed of data collection for the SEPREVEN study and did not oppose the use of their newborn's data.
Results
Population
Among 6,099 patients included in the SEPREVEN cohort, 572 BSIs were collected in 506 patients. After 15 BSIs were excluded, the final study population comprised 557 BSIs in 494 patients (Figure 1). Table 1 presents the characteristics of the patients and the BSIs.
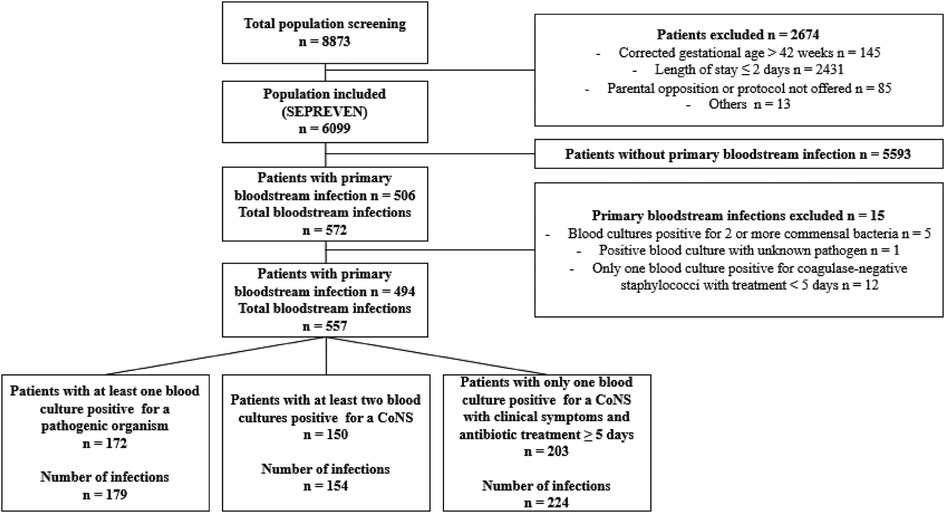
Figure 1. Flow chart. SEPREVEN, Study on preventing adverse events in neonates; CoNS, Coagulase negative staphylococci.
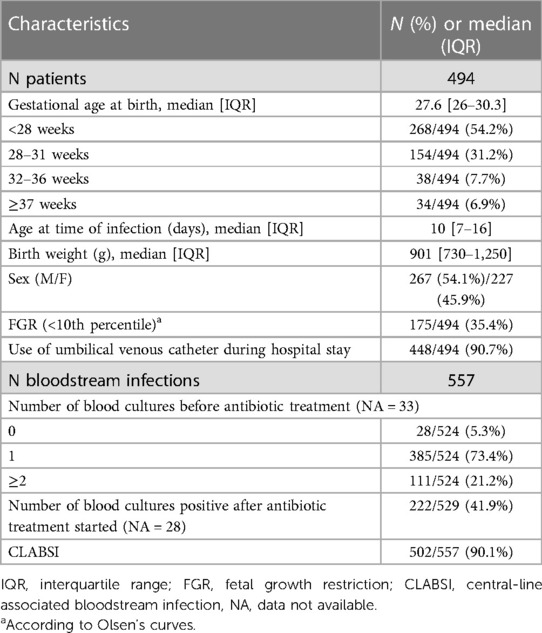
Table 1. Characteristics of patients and bloodstream infections.
Microbiological description
Common commensal organisms accounted for 378/557 BSIs (67.8%) and were mainly CoNS: 154/557 proven BSIs (27.6%) and 224/557 possible BSIs (40.2%). Recognized bacterial or fungal pathogens accounted for 179/557 (32.1%) BSIs (Table 2).
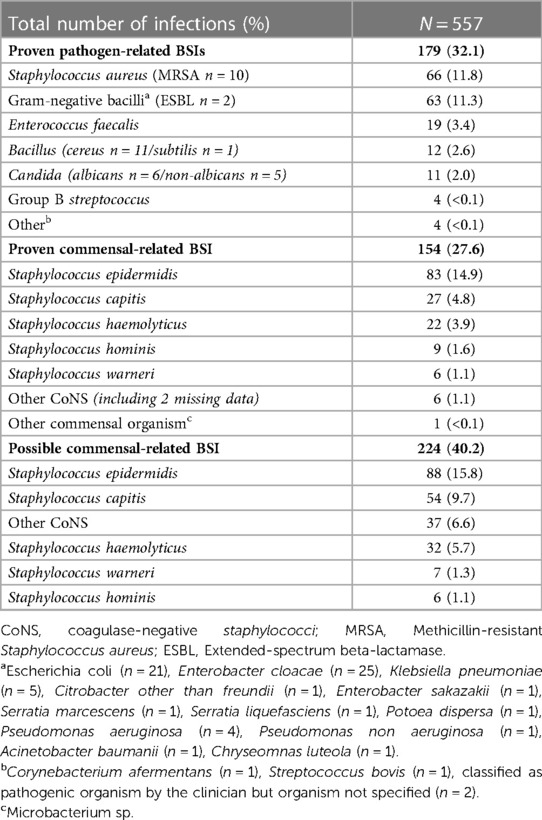
Table 2. Microbiological description of organisms involved in primary health care-associated bloodstream infections in the SEPREVEN cohort.
Among possible commensal-related BSIs, ≥ 2 blood cultures were collected in only 32/224 (15.5%) cases.
Morbidity and mortality after BSIs
Overall, moderate morbidity was found in 409/557 (73.4%) cases of BSI and severe morbidity/mortality in 148/557 (26.6%). The severe consequence was death in 35/557 (6.3%) BSIs, a life-saving treatment in 100/557 (17.9%) BSIs, an extended length of stay in 10/557 (1.8%), and possible permanent damage in 3/557 (0.5%).
Factors associated with severe morbidity/mortality
Factors significantly associated with severe morbidity/mortality in the univariate analysis were a GA <28 weeks compared to 28–32 weeks (P = .02), a corrected GA <28 weeks at infection (P = .03), a birth weight <1,000 g (P = .02), and a recognized pathogen isolated in blood cultures (P = .03) (Table 3). In the multivariate analysis, factors independently associated with severe morbidity/mortality were a corrected GA <28 weeks at infection (P < .01), FGR (P = .04), and a proven pathogen-related BSI (vs. a proven or possible commensal-related BSI (P < .01) (Table 4). Concerning mortality alone in multivariate analysis, a corrected GA <28 weeks at infection (P = .04) and a proven pathogen-related BSI (P = .03) were significantly associated with mortality.
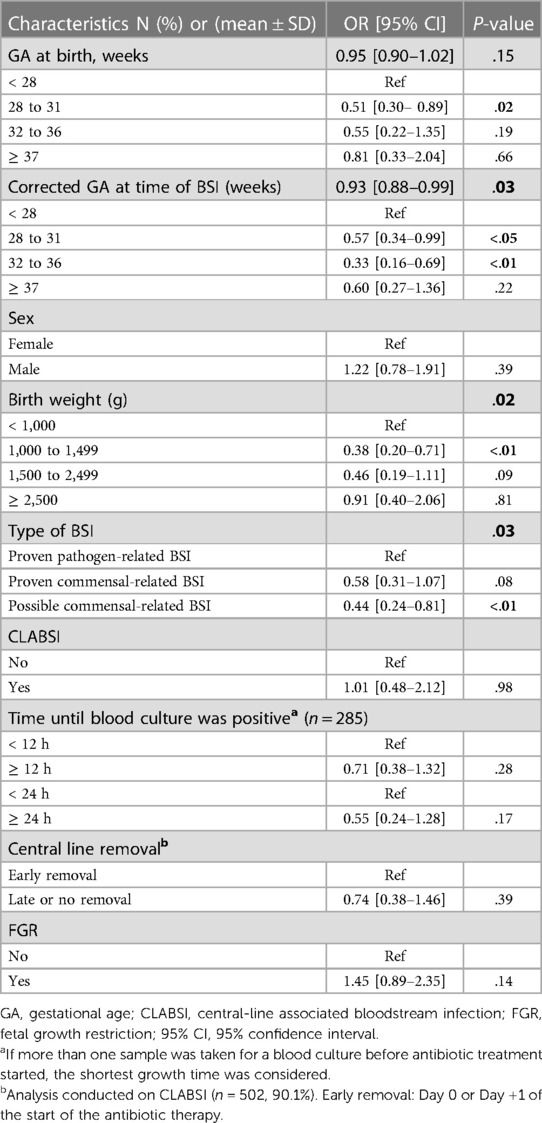
Table 3. Univariate analysis of factors associated with severe morbidity/mortality after health care-associated primary bloodstream infections.
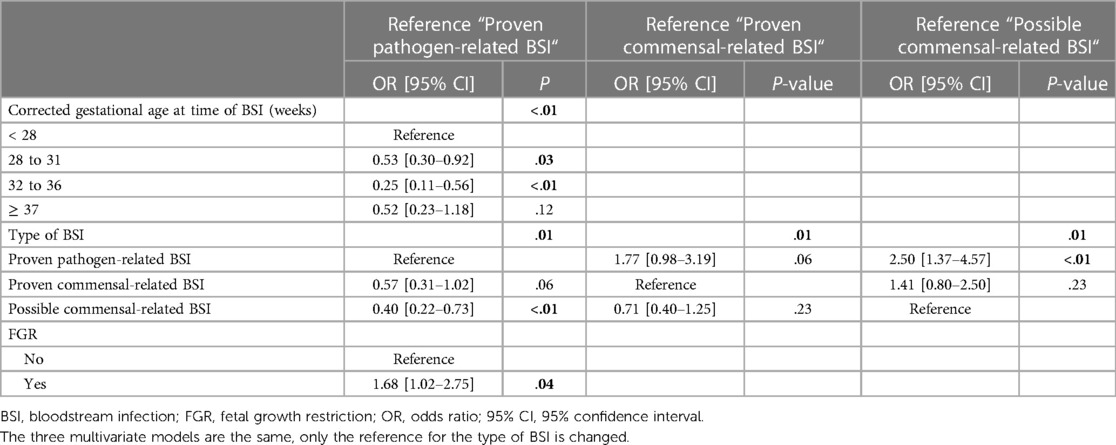
Table 4. Multivariate analysis of factors associated with severe morbidity/mortality of primary health care-associated bloodstream infections.
Morbidity and mortality by type of organism
Among proven BSIs, risk of severe morbidity/mortality was similar among the different CoNS species (P = 0.23) and similar among the different bacterial or fungal pathogens (P = 0.64). A possible BSI with only one blood culture growing S. epidermidis was significantly associated with a lower risk of severe morbidity/mortality compared to the other CoNS (P < 0.01) (Table 5).
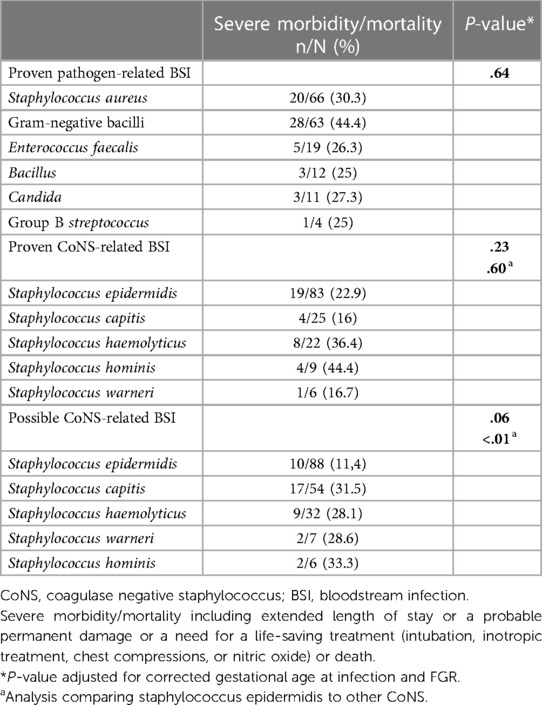
Table 5. Clinical consequences of primary health care-associated bloodstream infections by organism.
When considering only mortality, there was no significant difference among the different pathogens (P = 0.68) and among the different CoNS species in proven BSI (P = 0.97), respectively.
Factors associated with persistent bacteremia
Among the 529 infections with available data about blood cultures after initiation of antibiotic treatment, bacteremia persisted in 222/529 (42.0%) cases. In multivariate analysis, after adjustment for corrected GA at infection and FGR, the only factor significantly associated with persistent bacteremia was the type of BSI: there was a higher risk of persistent bacteremia in proven CoNS-related BSI (OR, 7.22; 95% CI, 2.68–19.46], P < .01) and a lower risk of persistent bacteremia in possible CoNS-related BSI (OR, 0.22; 95% CI, 0.09–0.47], P < .01) compared to proven pathogen-related BSI. Early removal of the central line was not associated with a significant difference in the persistence of bacteremia (OR, 0.60; 95% CI, 0.22–1.61], P = 0.31).
Discussion
This large prospective multicenter study including more than 500 BSIs in 12 NICUs reports both short-term and discharge outcomes. Because of the exhaustive and prospective multicenter data collection for the SEPREVEN trial, it offers a good overview of these particular infections for all GAs combined.
Among the 6,099 neonates included in the SEPREVEN trial, 8.1% presented a HAI primary BSI, with a risk inversely related to GA at birth. An original feature of our study was to distinguish primary BSI from other types of late-onset sepsis associated with specific locations. The incidence of all types of late-onset sepsis in our cohort was 18%, which is consistent with the literature (3, 27). Microbiological distribution in this cohort was also consistent with the literature, with a large predominance of CoNS, followed by S. aureus. and Gram-negative bacilli (6, 15–19). The largest share of CoNS species were S. epidermidis (45.2%), followed by S. capitis (21.8%) and S. haemolyticus (14.2%), again consistent with previous reports (20, 28).
The main result of our study was that severe infection-related morbidity/mortality was associated with a corrected GA <28 weeks at the time of infection, FGR at birth, and proven pathogen-related BSI. This study thus confirms the role of immaturity and growth restriction in neonatal outcomes in BSIs. It shows that risks factors of severity are not different in primary BSIs compared to late onset sepsis considered globally. This study also confirmed a higher risk of severe morbidity/mortality in BSI due to recognized pathogens compared to CoNS. Several studies in the literature have previously shown higher mortality in BSI with Gram-negative bacilli and fungi compared to Gram-positive bacteria (6, 21, 22). Our study also confirmed the considerable burden of CoNS BSIs, with severe morbidity found in 22.7% of cases, in line with the literature (29, 30). Our study found a low overall mortality rate (6.2%), little different from the rates found in the literature around 7% (7, 19), our large proportion of commensal-related BSI probably explained this result.
An original aspect of our study was its comparison of outcomes by CoNS species. We found that when only one blood culture was positive for S. epidermidis, neonates had a lower risk of severe morbidity than with other CoNS. This result raises two questions: is contamination responsible when only a single blood culture is taken and is positive? And does pathogenicity differ between CoNS species? To distinguish possible contaminants from true CoNS infections without underestimating the number of BSIs, we included CoNS infections with only one positive blood culture using criteria described in the literature (6) (one CoNS-growing blood culture with clinical symptoms and antibiotic treatment ≥ 5 days). In BSIs with only one positive blood culture, clinicians face a dilemma: whether to treat what might be a true BSI in a vulnerable patient or to protect her/him from possibly unnecessary antibiotic therapy (31). Taking samples for two blood cultures reduces the number of diagnoses of CoNS sepsis and thus the use of antibiotics (32).
Drawing culture samples from neonates, and especially very low birth weight neonates, can be technically difficult. In more than 2/3 of BSI cases, only one blood culture was available before antibiotic prescription: 385/557 (69%) regardless of the organism involved, and 168/224 (81.2%) in possible commensal-related BSI. If two blood samples had been collected for culture before antibiotic administration in all the cases, it would clearly have been easier to distinguish between real BSI and contamination.
The lack of a significant difference in morbidity/mortality in our study between neonates with a proven CoNS infection and those with possible CoNS infection suggests that many of the possible CoNS infections were true BSIs. Thus, other factors must be able to distinguish contaminants from true BSI. Time until the first culture is positive is likely to be the first clue in differentiating a contaminated sample from true BSI (33). When only one culture was positive for S. epidermidis, that time to positivity always exceeded 24 h. The second factor might be the particular CoNS species identified. The finding of similar rates of severe outcomes in proven and possible CoNS BSI for all CoNS species except S. epidermidis is interesting. S. capitis BSIs have been shown to be associated with higher morbidity in the literature than other CoNS infections (34). We might hypothesize that when only one blood culture is positive for a CoNS other than S. epidermidis (that is, for S. capitis or haemolyticus), it was more likely to be a true BSI than one positive for S. epidermidis.
Another interesting finding in our cohort was that removing the catheter at an early stage of infection did not appear to protect patients from severe morbidity/mortality. Removing the central catheter in cases of infection is controversial (35–37). An indication bias might exist in our cohort since one indication for removing the catheter could well be the patient's more severe symptoms. This might thus be a confounding factor with more severe infections in the early removal group. The Infectious Diseases Society of America (IDSA) recommends for both children and adults that the catheter be removed in cases of severe sepsis, suppurative thrombophlebitis, endocarditis, infections due to specific organisms (for instance, S. aureus, P. aeruginosa, or fungi), and when BSI continues despite 72 h of effective antimicrobial therapy (38). On the one hand, clinicians may feel reluctant to remove the catheter in neonates because of the difficulty in obtaining another venous access and the risk of bacterial dissemination at removal. On the other hand, possible severe consequences of BSI in this vulnerable population may motivate an early treatment and removal of the source of infection. Although our study might have lacked the power to reach a conclusion on this question, it does not support early removal of the catheter outside the severe situations described in adult guidelines.
In our study, cultures remained positive after starting antibiotic treatment more often for proven CoNS-related BSI than for proven pathogen-related BSI. This could be due to the ability of CoNS to form biofilms on medical devices such as central lines, thus providing a permanent source and continuous seeding of bacteria into the bloodstream (39, 40). Another explanation, however, might be the slow bactericidal activity of the vancomycin used to treat CoNS infections and the possible variability in vancomycin serum levels in patients. Finally, this finding could be due to the existence of contaminations in the possible commensal-related BSIs.
We had a higher proportion of persistent bacteremia in our cohort compared to other cohorts, which found persistence rates between 12% and 25% but it might be due to the large definition we took of persistent bacteremia (41–43).
Our study has several limitations. First, despite the high number of infections, we might have lacked power to distinguish differences in outcomes according to the organism responsible. Second, connecting clinical consequences, such as prolonged length of stay to a BSI episode can be difficult, as numerous factors may influence this length of stay. Clinicians were asked to report consequences prospectively after the infection, but assigning consequences to infections and not to prematurity or other conditions can be difficult and could have resulted in imprecision in our data. Nonetheless, these consequences were reported by senior physicians with experience in neonatal intensive care. Third, we lacked detailed data on type and doses of antibiotics used, and the appropriateness of antibiotic therapy could have influenced clinical outcomes. Fourth, blood sampling practices could have varied among participating NICUs, and we know that the volume of blood and the number of cultures are important for identifying BSIs. However, before starting the inclusions in the SEPREVEN trial, blood sample practices before antibiotic treatment were standardized in the participating units, by informing and encouraging health care professionals to collect two separate blood samples for culture, of a volume ≥ 1 ml. Finally, the educational program conducted during the SEPREVEN trial might have modified the incidence of CLABSI. However, it seems unlikely that this intervention changed the microbiological distribution or outcomes related to BSI that we report here.
Conclusion
Independent factors associated with severe morbidity/mortality related to the health care-associated primary BSIs were a corrected GA <28 weeks at infection, a recognized pathogen causing the BSI, and FGR at birth. There were no differences in severe morbidity and mortality between proven and possible CoNS BSIs. When only one blood culture was positive, severe morbidity/mortality were less frequent if it grew with S. epidermidis compared to other CoNS. Further studies to help distinguish real CoNS BSIs from contaminations are needed, along with data on pathogenicity according to the organism involved and patients' characteristics.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Consultative Committee on the Treatment of Data on Personal Health for research Purposes, France CCTIRS no 15,327, and the Committee for the Protection of People Participating in Biomedical Research CPP Ile-de-France III, France, no ID RCB: 2014-A01751-46. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements. Written informed consent was not obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
LC, MT, MJ, RL, VB, FD, RC contributed to conception and design of the study. LC, VB, FD, MC, NL, MRB and PB helped with data collection. RL and EA performed the statistical analysis. MJ wrote the first draft of the manuscript. MT and LC wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Solidarity and Health Ministry, France, grant no 13-0401
Acknowledgments
On behalf of the Study on Epidemiology and PRevention of adverse EVEnts in Neonates (SEPREVEN) investigators: LC, Dominique Astruc, VB, Leila Marcus, Laurent Beghin, Stephane Le Bouedec, Bernard Guillois, Radia Remichi, Faiza Harbi, Xavier Durrmeyer, Florence Casagrande, Nolwenn Lesaché, Darina Todorova, Ali Bilal, Damien Olivier, Audrey Reynaud, Cécile Jacquin, Jean-Christophe Roze, RL, Claude Danan, Camille Jung, FD, EA. We thank Jo Ann Cahn for English language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1170863/full#supplementary-material.
References
1. Sharek PJ, Horbar JD, Mason W, Bisarya H, Thurm CW, Suresh G, et al. Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool to identify harm in north American NICUs. Pediatrics. (2006) 118(4):1332–40. doi: 10.1542/peds.2006-0565
2. Greenberg RG, Kandefer S, Do BT, Smith PB, Stoll BJ, Bell EF, et al. Late-onset sepsis in extremely premature infants: 2000-2011. Pediatr Infect Dis J Août. (2017) 36(8):774–9. doi: 10.1097/INF.0000000000001570
3. Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA. (2015) 314(10):1039–51. doi: 10.1001/jama.2015.10244
4. Perlman SE, Saiman L, Larson EL. Risk factors for late-onset health care-associated bloodstream infections in patients in neonatal intensive care units. Am J Infect Control avr. (2007) 35(3):177–82. doi: 10.1016/j.ajic.2006.01.002
5. Bizzarro MJ, Raskind C, Baltimore RS, Gallagher PG. Seventy-five years of neonatal sepsis at Yale: 1928-2003. Pediatrics. (2005) 116(3):595–602. doi: 10.1542/peds.2005-0552
6. Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD neonatal research network. Pediatrics Août. (2002) 110(2 Pt 1):285–91. doi: 10.1542/peds.110.2.285
7. Tsai MH, Hsu JF, Chu SM, Lien R, Huang HR, Chiang MC, et al. Incidence, clinical characteristics and risk factors for adverse outcome in neonates with late-onset sepsis. Pediatr Infect Dis J. (2014) 33(1):e7–13. doi: 10.1097/INF.0b013e3182a72ee0
8. Tröger B, Göpel W, Faust K, Müller T, Jorch G, Felderhoff-Müser U, et al. Risk for late-onset blood-culture proven sepsis in very-low-birth weight infants born small for gestational age: a large multicenter study from the German neonatal network. Pediatr Infect Dis J. (2014) 33(3):238–43. doi: 10.1097/INF.0000000000000031
9. BSI | PSC | NHSN | CDC. 2021 [cité 24 janv 2022]. Disponible sur: https://www.cdc.gov/nhsn/psc/bsi/index.html
10. Zingg W, Hopkins S, Gayet-Ageron A, Holmes A, Sharland M, Suetens C, et al. Health-care-associated infections in neonates, children, and adolescents: an analysis of paediatric data from the European centre for disease prevention and control point-prevalence survey. Lancet Infect Dis. (2017) 17(4):381–9. doi: 10.1016/S1473-3099(16)30517-5
11. Auriti C, Maccallini A, Di Liso G, Di Ciommo V, Ronchetti MP, Orzalesi M. Risk factors for nosocomial infections in a neonatal intensive-care unit. J Hosp Infect. (2003) 53(1):25–30. doi: 10.1053/jhin.2002.1341
12. Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA. (2004) 292(19):2357–65. doi: 10.1001/jama.292.19.2357
13. Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. (2018) 6(3):223–30. doi: 10.1016/S2213-2600(18)30063-8
14. Fanaroff AA, Korones SB, Wright LL, Verter J, Poland RL, Bauer CR, et al. Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. The national institute of child health and human development neonatal research network. Pediatr Infect Dis J. (1998) 17(7):593–8. doi: 10.1097/00006454-199807000-00004
15. Tsai MH, Chu SM, Lee CW, Hsu JF, Huang HR, Chiang MC, et al. Recurrent late-onset sepsis in the neonatal intensive care unit: incidence, clinical characteristics and risk factors. Clin Microbiol Infect. (2014) 20(11):O928–35. doi: 10.1111/1469-0691.12661
16. Bizzarro MJ, Shabanova V, Baltimore RS, Dembry LM, Ehrenkranz RA, Gallagher PG. Neonatal sepsis 2004-2013: the rise and fall of coagulase-negative staphylococci. J Pediatr. (2015) 166(5):1193–9. doi: 10.1016/j.jpeds.2015.02.009
17. Boghossian NS, Page GP, Bell EF, Stoll BJ, Murray JC, Cotten CM, et al. Late-Onset sepsis in very low birth weight infants from singleton and multiple gestation births. J Pediatr. (2013) 162(6):1120–1124.e1. doi: 10.1016/j.jpeds.2012.11.089
18. Vergnano S, Menson E, Kennea N, Embleton N, Russell AB, Watts T, et al. Neonatal infections in England: the NeonIN surveillance network. Arch Dis Child Fetal Neonatal Ed. (2011) 96(1):F9–14. doi: 10.1136/adc.2009.178798
19. Berardi A, Sforza F, Baroni L, Spada C, Ambretti S, Biasucci G, et al. Epidemiology and complications of late-onset sepsis: an Italian area-based study. PLoS One. (2019) 14(11):e0225407. doi: 10.1371/journal.pone.0225407
20. Hira V, Sluijter M, Estevão S, Horst-Kreft D, Ott A, de Groot R, et al. Clinical and molecular epidemiologic characteristics of coagulase-negative staphylococcal bloodstream infections in intensive care neonates. Pediatr Infect Dis J. (2007) 26(7):607–12. doi: 10.1097/INF.0b013e318060cc03
21. Benjamin DK, DeLong E, Cotten CM, Garges HP, Steinbach WJ, Clark RH. Mortality following blood culture in premature infants: increased with gram-negative bacteremia and candidemia, but not gram-positive bacteremia. J Perinatol. (2004) 24(3):175–80. doi: 10.1038/sj.jp.7211068
22. Shah J, Jefferies AL, Yoon EW, Lee SK, Shah PS, et al. Canadian Neonatal Network. Risk factors and outcomes of late-onset bacterial sepsis in preterm neonates born at < 32 Weeks’ gestation. Am J Perinatol. (2015) 32(7):675–82. doi: 10.1055/s-0034-1393936
23. Marchant EA, Boyce GK, Sadarangani M, Lavoie PM. Neonatal sepsis due to coagulase-negative staphylococci. Clin Dev Immunol. (2013) 2013:586076. doi: 10.1155/2013/586076
24. Dong Y, Speer CP, Glaser K. Beyond sepsis: staphylococcus epidermidis is an underestimated but significant contributor to neonatal morbidity. Virulence. (2018) 9(1):621–33. doi: 10.1080/21505594.2017.1419117
25. Caeymaex L, Astruc D, Biran V, Marcus L, Flamein F, Le Bouedec S, et al. An educational programme in neonatal intensive care units (SEPREVEN): a stepped-wedge, cluster-randomised controlled trial. Lancet. (2022) 399(10322):384–92. doi: 10.1016/S0140-6736(21)01899-7
26. National Coordinating Council for Medication Error Reporting and Prevention. Taxonomy of medication errors. http://www.nccmerp.org/pdf/indexBW2001-06-12.pdf NCC MERP. (cité 26 mars 2022). Disponible sur: https://www.nccmerp.org/file/2
27. Shane AL, Sánchez PJ, Stoll BJ. Neonatal sepsis. Lancet. (2017) 390(10104):1770–80. doi: 10.1016/S0140-6736(17)31002-4
28. Decalonne M, Dos Santos S, Gimenes R, Goube F, Abadie G, Aberrane S, et al. Staphylococcus capitis isolated from bloodstream infections: a nationwide 3-month survey in 38 neonatal intensive care units. Eur J Clin Microbiol Infect Dis. (2020) 39(11):2185–94. doi: 10.1007/s10096-020-03925-5
29. Anderson-Berry A, Brinton B, Lyden E, Faix RG. Risk factors associated with development of persistent coagulase-negative staphylococci bacteremia in the neonate and associated short-term and discharge morbidities. Neonatology. (2011) 99(1):23–31. doi: 10.1159/000292567
30. Cantey JB, Anderson KR, Kalagiri RR, Mallett LH. Morbidity and mortality of coagulase-negative staphylococcal sepsis in very-low-birth-weight infants. World J Pediatr. (2018) 14(3):269–73. doi: 10.1007/s12519-018-0145-7
31. Cotten CM. Adverse consequences of neonatal antibiotic exposure. Curr Opin Pediatr. (2016) 28(2):141–9. doi: 10.1097/MOP.0000000000000338
32. Struthers S, Underhill H, Albersheim S, Greenberg D, Dobson S. A comparison of two versus one blood culture in the diagnosis and treatment of coagulase-negative staphylococcus in the neonatal intensive care unit. J Perinatol. (2002) 22(7):547–9. doi: 10.1038/sj.jp.7210792
33. Huggard D, Powell J, Kirkham C, Power L, O’Connell NH, Philip RK. Time to positivity (TTP) of neonatal blood cultures: a trend analysis over a decade from Ireland. J Matern Fetal Neonatal Med. (2021) 34(5):780–6. doi: 10.1080/14767058.2019.1617687
34. Ben Said M, Hays S, Bonfils M, Jourdes E, Rasigade JP, Laurent F, et al. Late-onset sepsis due to Staphylococcus capitis “neonatalis” in low-birthweight infants: a new entity? J Hosp Infect. (2016) 94(1):95–8. doi: 10.1016/j.jhin.2016.06.008
35. Tsai MH, Hsu JF, Lien R, Huang HR, Chiang CC, Chu SM, et al. Catheter management in neonates with bloodstream infection and a percutaneously inserted central venous catheter in situ: removal or not? Am J Infect Control. (2012) 40(1):59–64. doi: 10.1016/j.ajic.2011.04.051
36. Karlowicz MG, Furigay PJ, Croitoru DP, Buescher ES. Central venous catheter removal versus in situ treatment in neonates with coagulase-negative staphylococcal bacteremia. Pediatr Infect Dis J. (2002) 21(1):22–7. doi: 10.1097/00006454-200201000-00005
37. Vasudevan C, Oddie SJ, McGuire W. Early removal versus expectant management of central venous catheters in neonates with bloodstream infection. Cochrane Database Syst Rev. (2016) 4(4):CD008436. doi: 10.1002/14651858.CD008436.pub3
38. Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases society of America. Clin Infect Dis. (2009) 49(1):1–45. doi: 10.1086/599376
39. Otto M. Staphylococcal biofilms. Microbiol Spectr. (2018) 6(4):10.1128/microbiolspec.GPP3-0023-2018. doi: 10.1128/microbiolspec.GPP3-0023-2018
40. Cheung GYC, Otto M. Understanding the significance of Staphylococcus epidermidis bacteremia in babies and children. Curr Opin Infect Dis. (2010) 23(3):208–16. doi: 10.1097/QCO.0b013e328337fecb
41. Bellou V, Gkentzi D, Giormezis N, Vervenioti A, Spiliopoulou I, Dimitriou G. Persistent coagulase-negative staphylococcal bacteremia in neonates: clinical, microbiological characteristics and changes within a decade. Antibiotics (Basel). (2022) 11(6):765. doi: 10.3390/antibiotics11060765
42. Furuichi M, Miyairi I. Risk factors for persistent bacteremia in infants with catheter-related bloodstream infection due to coagulase-negative Staphylococcus in the neonatal intensive care unit. J Infect Chemother déc. (2016) 22(12):785–9. doi: 10.1016/j.jiac.2016.08.011
Keywords: bloodstream infections, newborn, outcomes, coagulase-negative staphylococci, preterm
Citation: Jaloustre M, Cohen R, Biran V, Decobert F, Layese R, Audureau E, Le Saché N, Chevallier M, Boukhris MR, Bolot P, Caeymaex L and Tauzin M (2023) Determinants of morbidity and mortality related to health care-associated primary bloodstream infections in neonatal intensive care units: a prospective cohort study from the SEPREVEN trial. Front. Pediatr. 11:1170863. doi: 10.3389/fped.2023.1170863
Received: 21 February 2023; Accepted: 10 May 2023;
Published: 31 May 2023.
Edited by:
Diego Gazzolo, Chieti, ItalyReviewed by:
Cinzia Auriti, Bambino Gesù Children's Hospital (IRCCS), ItalyTuuli Metsvaht, University of Tartu, Estonia
© 2023 Jaloustre, Cohen, Biran, Decobert, Layese, Audureau, Le Saché, Chevallier, Boukhris, Bolot, Caeymaex, Tauzin and with SEPREVEN study Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manon Tauzin bWFub24udGF1emluQGNoaWNyZXRlaWwuZnI=
†These authors have contributed equally to this work and share last authorship
‡Study Group team members are listed in the Acknowledgments