 Bekalu Getnet Kassa*
Bekalu Getnet Kassa* Nhial Char Lul
Nhial Char Lul
- Department of Midwifery, College of Health Science, Debre Tabor University, Debre Tabor, Ethiopia
Background: The World Health Organization's Expanded Immunization Program was established in 1974 and aimed to provide vaccines to children all over the world. Since the inception of this program, numerous initiatives and campaigns have been launched, and millions of children around the world have been saved from death. Many vaccine-preventable diseases, however, remain prevalent in developing countries. This is because most of those countries have low immunization coverage for an unknown number of reasons. As a result, the goal of this study was to examine missed opportunities for immunization among children aged 0 to 11 months.
Methods: A cross-sectional survey was carried out from May to August 2022. A structured questionnaire was used to collect data, and the sample was chosen using a simple random sampling technique. Before being entered into the Epidata and exported to the Statistical Package for Social Science for analysis, the data were checked for consistency and completeness. The statistical significance was determined using binary and multiple logistic regression analyses. The statistical level of significance was established at p ≤ 0.05.
Result: In this study, 49.1% of immunization opportunities were missed. Education status [AOR = 2.45, 95% CI = 2.14, 4.22], rural residence [AOR = 4.32, 95% CI = 3.11, 6.38], and perception of caretakers [AOR = 2.13, 95% CI = 1.89, 4.07] were associated with the missed opportunity of immunization.
Conclusion: When compared to previous studies, the proportion of missed immunization opportunities was high in this study. The healthcare staff should be applying the multi-dose vial policy, which is recommended by the World Health Organization to increase the services. The doses for BCG and measles should be minimized to lower doses per vial in order to conduct immunization without having to wait for enough children and without worrying about vaccine waste. All infants who visit the hospital should be linked to immunization services.
Background
By the age of 9 to 12 months, children in Ethiopia are considered completely vaccinated if they have obtained one dose of Bacillus Calmette Guerin (BCG), three doses of DPT, three doses of polio vaccines, and one dose of measles vaccination (1, 2). A missed opportunity for vaccination (MOV) refers to any contact with health services by an individual (child or person of any age) who is eligible for vaccination (e.g., unvaccinated or partially vaccinated and free of contraindications to vaccination), which does not result in the person receiving one or more of the vaccine doses for which he or she is eligible (3–5).
Diseases covered by the Expanded Program on Immunization (EPI) are highly contagious and account for more than half of all child morbidity and mortality (6). Every year, over nineteen million children miss out on the benefits of complete vaccination, and many receive no vaccines at all, which results in >1 million deaths each year. Nearly 30% of deaths among under-5-year-old children are caused by vaccine-preventable diseases (7).
An increase in global immunization coverage would save 1.5 million lives (8). Despite a significant increase in immunization services in Africa, many children remain unvaccinated or under-vaccinated (9). Routine immunization performance in the African Region has stalled for the majority of vaccine-delivered antigens over the last decade.
The country with the second-highest proportion of unvaccinated children, after Nigeria, is Ethiopia, where vaccine coverage was reported to be 75% in 2020 (3). To minimize such problems, the World Health Organization recommended a multi-dose vial policy across each country to fulfill the criteria of the multi-dose vial policy (10). In absolute figures, the majority of deaths are still attributable to a small number of conditions that can be avoided using existing interventions through vaccinations (11).
Ethiopia, one of the ten nations with the highest global non-vaccination prevalence, is below the WHO target of vaccine coverage. Morbidity and mortality from diseases that can be prevented by vaccination are still high, with diarrheal illnesses, respiratory infections, and tuberculosis ranking among the top five killers of young children (12). The infant mortality rate stood at 47, and the mortality of under 5-year-old children was 59 per thousand live births in Ethiopia (1). Vaccination, the most cost-effective measure for public health, has protected children around the world from common illnesses (13). Several factors have been identified as contributing to missed opportunities such as antenatal care visits, residence, educational status, high fertility rates, place of delivery, perceived health care support, wealth index, occupational status, religious affiliation, mothers’ awareness of vaccination, and parity (5, 7, 14–16). As a result, further studies are required to determine the main factors for missed opportunities for immunization.
Methods
Study area
The study was conducted at the Debre Tabor Comprehensive and Specialized Hospital located in Debre Tabor town, south Gondar zone, Amhara National Regional State, Ethiopia, which is 667 kilometers north of Addis Ababa, the capital city of Ethiopia. The hospital has been offering preventive, delivery, and curative healthcare services to approximately 2.7 million people. It serves as a teaching hospital for Debre Tabor University's College of Health Sciences.
Study design and period
A facility-based cross-sectional study was carried out from May to August 2022.
Population
All infants aged between 0 and 11 months were the source populations. Infants aged 0 to 11 months who visited Debre Tabor Comprehensive Specialized Hospital during the study period were the sampled population. All infants aged 0 to 11 months who were seriously ill or hospitalized were excluded.
Sample size determination and sampling procedures
The required sample size for this study was determined using the following assumptions: desired precision (d) = 5%, confidence level = 95% (Zα/2 = ±1.96 value), and prevalence of missed opportunity of 28.8% (17). As a result, with a 10% non-response rate, the final sample size was 346. A simple random sampling technique was employed to select 346 study participants who fulfilled the inclusion criteria from the source population. The sample size was then determined by drawing a sample randomly by the lottery method from each visit until the desired sample size was gotten.
Study variables
Dependent variable: Missed opportunity for vaccination (Yes/No).
Independent variable: Maternal educational status, false contraindication for vaccination, health workers' practice and knowledge, side effects of vaccination, marital status, attitude towards immunization, occupational status (employment), place of delivery, parity, age, sex, religion, ethnicity, and residence.
Operational definitions
Missed opportunities for Vaccination: A missed opportunity for vaccination (MOV) refers to any contact with health services by an individual (child or person of any age) who is eligible for vaccination (e.g., unvaccinated or partially vaccinated and free of contraindications to vaccination), which does not result in the person receiving one or more of the vaccine doses for which he or she is eligible (3–5).
Eligible child: A child whose age is 0 to 11 months and who needs immunization without any contradiction.
Fully immunized: A child who had completed vaccination against eight EPI-targeted diseases according to the standard vaccination schedule of the Ministry of Health of Ethiopia (1).
Perception of caretakers: The perception of caretakers was measured by comparing mean score responses to seven perception-assessing parameters (immunization is beneficial, childhood vaccines are safe, mothers should take their children for immunization, immunizations are provided free of charge, immunization can cause infertility later in life, the government promotes immunization for selfish interest, and local preparation can serve as a substitute for immunization). Those with scores at or below the mean were classified as having “no or poor perception” while those with scores above the mean were categorized as having “yes or good perception” (18).
Data collection procedure and tools
A structured questionnaire was developed following a thorough review of the literature and a consideration of the local situation. It was first written in English and then translated into Amharic, the local language. Data were gathered through face-to-face interviews with a pre-tested and structured questionnaire. Two midwives with diploma degrees were used as data collectors, one degree midwives serving as supervisor.
Data quality controls
Pre-testing was done, technical training was given to data collectors and supervisors, and a data collection tool was created after a review of the pertinent literature. On a daily basis, the supervisors and principal investigators checked the data for completeness, accuracy, and clarity. Then the necessary correction was made according to the aims of the study. The necessary correction was made in accordance with the study's objectives. Throughout the period of data collection, the principal investigator and supervisor conducted daily ongoing checks to ensure the accuracy of the data.
Data processing, analysis, and presentation
Data were cleaned, coded, and entered into the Epidata version 4.0 before being transferred to SPSS version 20 for analysis. To summarize the data, a descriptive analysis was performed. A binary logistic regression analysis was performed to determine the association between independent and outcome variables. All predictor variables with p ≤ 0.2 were entered into multivariable logistic regression analysis; a significant association based on p ≤ 0.05 and an adjusted odd ratio (AOR) with 95% CI were identified. The results are presented in the form of texts and tables.
Results
Socio-Demographic characteristics of participants
Three hundred and forty-six children aged 0 to 11 months, who visited a health facility during the study period, were included, with a 100% response rate. Out of 346 children, 115 (33.2%) were younger than 45 days and 182 (56.6%) were between 45 days and 9 months. There were 194 (56.1%) male children and 152 (43.9%) female children among the included infants. Three hundred and twenty-seven (94.5%) of the babies were born in hospitals. The purpose of children's visits to the health facility was for treatment of sickness 129 (37.3%), vaccination 174 (50.3%), and other purposes 43 (12.4%). Concerning the age of the caregiver, 26 (7.5%) were under the age of 18, 183 (52.9%) were between the ages of 18 and 35, and 137 (39.1%) were over 35. Regarding the educational status of caregivers, 129 (37.3%) had no formal education, 112 (15.3%) completed primary education, 53 (15.3%) completed secondary education, and the remaining 52 (15.0%) completed college level or higher. Approximately 206 (59.5%) caregivers were from urban areas, and the remaining 140 (40.5%) were from rural catchment areas. In terms of religion, there were 314 orthodox Christians (90.8%), 26 Muslims (7.5%), and 6 Protestants (1.7%) (see Table 1).
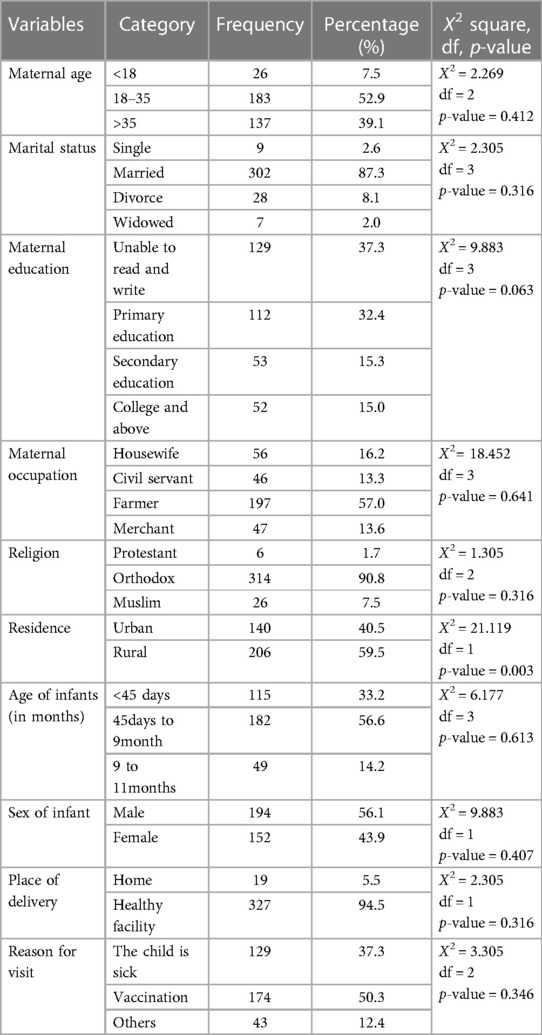
Table 1. Socio-demographic related characteristics of the respondents for missed opportunities for vaccination, 2022.
Knowledge and perception of caretakers on immunization
Regarding vaccine-preventable diseases, the assessment of caretakers' knowledge revealed that 95 (27.5%) of them were unaware of any of the ten vaccine-preventable diseases, while 165 (46.7%) of them knew about one to two vaccine-preventable diseases and 25 (7.2%) knew about six to nine vaccine-preventable diseases. Two hundred and thirty-seven (68.5%) caregivers indicated that the goal of vaccination is to prevent diseases, 67 (19.4%) of them said that children grow up healthy, and 133 (9.5%) of them said that vaccination can treat diseases (see Table 2).
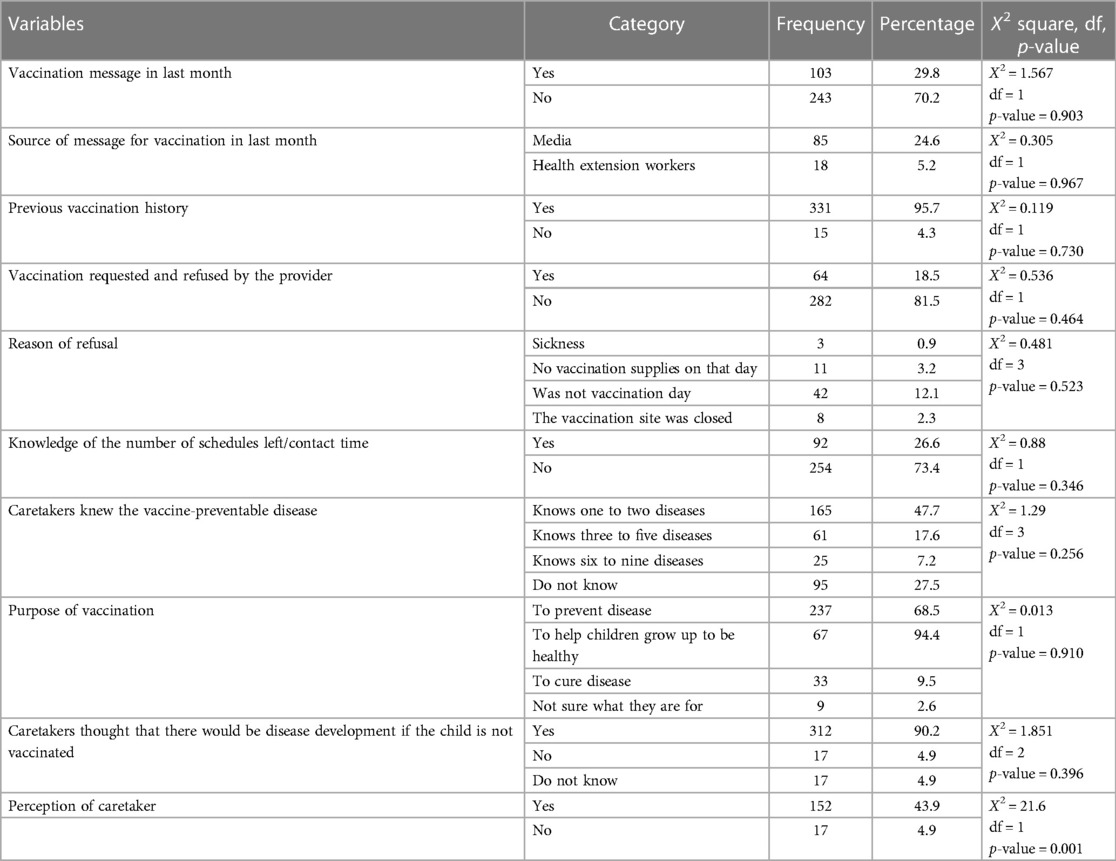
Table 2. Knowledge and perception of caretakers for missed opportunities for vaccination, 2022.
The magnitude of missed opportunities for immunization
Among all study participants, the magnitude of the missed opportunity for immunization among infants was 49.1% with a 95% CI (43.7 to 52.9%). Major vaccines with a high missed opportunity were OPV 0 (35%), BCG (37.9%), and measles (31.1%), and the major reason for immunization for missed vaccines was due to the absence of an adequate number of children to conduct immunization sessions, which was approximately 81.2%.
Factors associated with missed opportunities for immunization
Age of infants, age of caretaker, maternal education, residence, stock out of vaccine session, vaccination message, knowledge contact time, perception, and purpose of the visit were found to be candidate variables for multivariable logistic regression analysis.
Multivariable logistic regression analysis revealed that residence, maternal education, and perception about immunization were associated with missed opportunities for immunization at p-values ≤ 0.05.
Mothers who resided in rural areas were 4.32 times more likely to have missed opportunities than their counterparts (AOR = 4.32, 95% CI: 3.11, 6.38).
Mothers who are unable to read or write are twice as likely than their counterparts to miss immunization opportunities (AOR = 2.45, 95% CI: 2.14, 4.22).
Maternal perception towards immunization is another factor that affects missed opportunities. Mothers who had negative perceptions were two times more likely to have missed opportunities for immunization when compared to their counterparts (AOR = 2.13, 95% CI: 1.89, 4.07) (see Table 3).
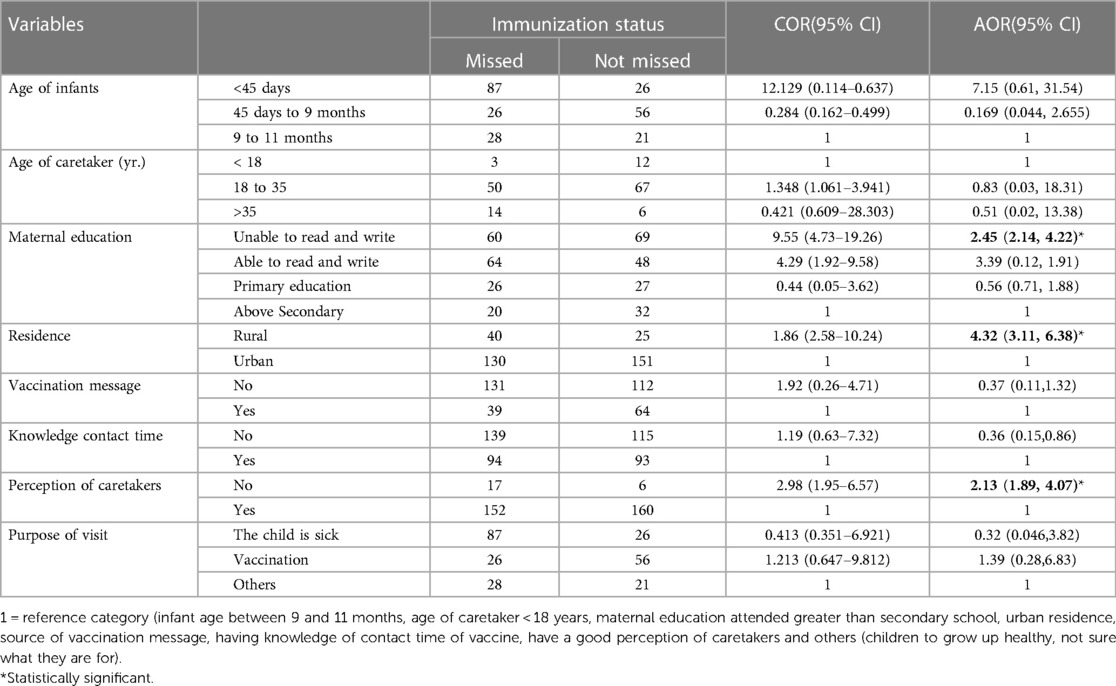
Table 3. Multivariable analysis for factors associated with missed opportunities for vaccination, 2022.
Discussion
The purpose of this research was to find out how common missed opportunities for immunization are and what factors contribute to them in the study area. In this research, the proportion of missed opportunities for immunization was 49.1%. The findings were consistent with vaccine assessments missed in Chad (51%) (19) and Gurage zone, Ethiopia (49.1%) (20). This could be due to similarities in the nature of the study, the study design, the study population, and the healthcare infrastructure.
This study is significantly greater than the cross-sectional research conducted in the Sidama zone (28.8%) (14), Jimma hospital (28.8%) (17), Ambo, central Ethiopia (23.7%) (16), Kenya (16.2%) (21), Timor Leste (41%) (22), Nigeria (32.8%) (23), and South Africa (14.1) (24). However, the finding is also less than the research done in the East Gojjam Zone, Ethiopia (74.9%), South Sudan (56.5%), Mozambique (76%), Malawi (66%), Kenya (75%), and Burkina Faso (76%) (15, 19, 25–27). This might be a result of a lack of infrastructure for access to healthcare facilities. Furthermore, this finding might also differ from others due to socioeconomics, study area, and study period differences.
Additionally, we attempted to evaluate factors that might contribute to missed opportunities for immunization. The results show that maternal educational status, place of residence, and caregivers’ attitudes toward the vaccine all had statistically significant correlations with missed opportunities for immunization among infants in the age range of 0 to 11 months.
Children born to mothers whose level of education is low were more likely to be unvaccinated compared with their counterparts. It was supported by research done in the Ilorin metropolis (28), South Africa (24), Mozambique (29), and the East Gojjam Zone, Ethiopia (25). The possible reason for more missed opportunities could be a lack of knowledge about the benefits of vaccines for their children. On the other hand, the level of education itself affects access to immunization messages since they could not read reliable information and even appointment dates from cards. However, maternal education is not consistently associated with missed opportunities for immunization. This is similar to the research done in Saudi Arabia (24).
Place of residence was another factor that affected the use of immunization among infants. We found that children who lived in rural areas were more likely to miss opportunities for immunization compared with urban ones. This is consistent with the findings of the study conducted in Nigeria, which revealed that long-distance walking was the major reason for missed opportunities for the vaccine (30). This could be due to the accessibility of the vaccine location, which could be the cause of more missed opportunities for immunization.
The proportion of missed opportunities for immunization was associated with caregiver perceptions. Caregivers with a negative perception about the about the side effects of vaccines is twice more likely to have for missed opportunities for immunization compared to their counterparts. This is similar to previous studies done in southern Ethiopia and Uganda (14, 31). The possible explanation could be that mothers who are concerned about vaccine side effects either refuse or postpone immunizations.
The limitation of this study was its lack of generalizability due to its single setting and institutional basis. Recall biases are another limitation of this study. In this study, we did not use a standard for measuring missed opportunities for immunization, and we used a Qualitative approach that could not address the “why” questions in detail.
Conclusion
The proportion of missed opportunities for immunization was 49.1%, which is high. Low level of education, rural residence, and perception of caretakers were factors affecting missed opportunities for immunization. There should be a system in place to provide mothers and caregivers with information and education about immunization services for their children.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Debre Tabor University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
BG and NC contributed to the design of the study, conceptualization validation, visualization, methodology, and analysis and interpretation of findings, as well as writing the original draft and revising the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The author would like to acknowledge Debre Tabor University for ethical clearance and technical support, as well as the study participants, data collectors, and supervisors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, adjusted odd ratio; BCG, bacillus calmette guerin; CI, confidence interval; DTCSH, debre tabor comprehensive and specialized hospital; EPI, expanded program on immunization; SPSS, statistical package for social science; WHO, world health organization.
References
1. Tamirat KS, Sisay MM. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health. (2019) 19(1):1–7. doi: 10.1186/s12889-019-7356-2
2. Idris IO, Ayeni GO, Adebisi YA. Why are missed opportunities for immunisation and immunisation defaulting among children indistinguishable? Ann Med Surg. (2022) 80(July):10–3. doi: 10.1016/j.amsu.2022.104268
3. Federal Ministry of Health Ethiopia(FMoH). Ethiopia National expanded program on immunization, comprehensive multi—year plan 2016–2020. World Health Organization. (2015):1–115.
4. WHO. Reducing Missed Opportunities for Vaccination (MOV). Who. 2021. p. 1. Available at: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization%0Ahttps://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/integration/linking-with-other-health-interventions/v
5. Jacob N, Coetzee D. Missed opportunities for immunisation in health facilities in Cape Town, South Africa. South African Med J. (2015) 105(11):917–21. doi: 10.7196/SAMJ.2015.v105i11.10194
6. Ethiopian Public Health Institute (EPHI), ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report. 2021. 1–207 p. Available at: https://dhsprogram.com/pubs/pdf/FR363/FR363.pdf
7. Tefera YA, Wagner AL, Mekonen EB, Carlson BF, Boulton ML. Predictors and barriers to full vaccination among children in Ethiopia. Vaccines (Basel). (2018) 6(2):1–11. doi: 10.3390/vaccines6020022
8. Unicef. GIVS: Global Immunization Vision and Strategy, 2006-2015. Givs. 2005;12–3. Available at: http://www.who.int/immunization/givs/GIVS_strategies.pdf?ua=1%5Cnhttp://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Global+Immunization+Vision+and+Strategy+2006+?+2015#2
9. Wiysonge CS, Uthman OA, Ndumbe PM, Hussey GD. Individual and contextual factors associated with low childhood immunisation coverage in sub-saharan Africa: a multilevel analysis. PLoS One. (2012) 7(5. doi: 10.1371/journal.pone.0037905
10. World Health Organization. Handling of Multi Dose Vaccine Vials (MDVP) after opening. 2014;14. Available at: http://www.who.int/immunization_standards/vaccine_quality/PQ_vaccine_list_en/en/index.html
11. Porth JM, Wagner AL, Tefera YA, Boulton ML. Childhood immunization in Ethiopia: accuracy of maternal recall compared to vaccination cards. Vaccines (Basel). (2019) 7(2):1–12. doi: 10.3390/vaccines7020048
12. UNICEF. UNICEF Immunization Roadmap 2018–2030. United Nations Child Fund (UNICEF). 2018;1–56. Available at: www.unicef.org
13. Obi Daniel E, Olaiya Abiodun P, Omoniyi Ayeni G, Victor Ojo O, Biar Anyieth J, Michael Olagbegi O. Factors contributing to missed opportunities and incomplete vaccination of children: a focus on mothers in rumbek centre county of lakes state South Sudan. World J Public Heal. (2019) 4(3):47. doi: 10.11648/j.wjph.20190403.11
14. Negussie A, Kassahun W, Assegid S, Hagan AK. Factors associated with incomplete childhood immunization in arbegona district, southern Ethiopia: a case—control study. BMC Public Health. (2016) 16(1):1–9. doi: 10.1186/s12889-015-2678-1
15. Submitted AD, The IN, Fulfilment P, The OF, Of D, Of M, et al. Prevelance and Factors Associated With Missed Opportunity for Immunization in Children Attending Paediatric Outpatient Clinic At Juba Teaching Hospital. 2012;(January).
16. Etana B, Deressa W. Factors associated with complete immunization coverage in children aged 12-23 months in ambo woreda, central Ethiopia. BMC Public Health. (2012) 12(1):1. Available at: BMC Public Health. doi: 10.1186/1471-2458-12-566
17. Girma S, Tekelemariam S. Missed opportunities for immunization in jimma hospital. Ethiop J Health Sci. (2000) 10(2. doi: 10.4314/ejhs.v26i2.6
18. Adedire EB, Ajumobi O, Bolu O, Nguku P, Ajayi I. Maternal knowledge, attitude, and perception about childhood routine immunization program in atakumosa-west local government area, Osun state, southwestern Nigeria. Pan Afr Med J. (2021) 40(Supp 1):8. doi: 10.11604/pamj.supp.2021.40.1.30876
19. Ogbuanu IU, Li AJ, Anya BPM, Tamadji M, Chirwa G, Chiwaya KW, et al. Can vaccination coverage be improved by reducing missed opportunities for vaccination? Findings from assessments in Chad and Malawi using the new WHO methodology. PLoS One. (2019) 14(1):1–19. doi: 10.1371/journal.pone.0210648
20. Assefa M. Magnitude of Missed Opportunities on Infants Under One Year Routine Immunization Services and Associated Year Routine Immunization Services and Associated Factors in Wolikte Healthcenter, Gurage Zone,. 2015;(July):72).
21. Odera-Ojwang P. Prevalence and factors associated with missed opportunities for immunization among children below 60 months at siaya county referral hospital. J Public …. (2016) 3(April):194–203. Available at: http://www.academicjournals.org/article/article1379427155_Abdulraheemet al.pdf
22. Li AJ, Sudath T, Peiris R, Sanderson C, Lochlainn LN, Mausiry M, et al. Opportunities to improve vaccination coverage in a country with a fledgling health system: findings from an assessment of missed opportunities for vaccination among health center attendees—timor leste, 2016. Vaccine. (2019) 37(31):4281–90. doi: 10.1016/j.vaccine.2019.06.041
23. Fatiregun AA, Lochlainn LN, Kaboré L, Dosumu M, Isere E, Olaoye I, et al. Missed opportunities for vaccination among children aged 0-23 months visiting health facilities in a southwest state of Nigeria, December 2019. PLoS One. (2021) 16(8 August):1–21. doi: 10.1371/journal.pone.0252798
24. Nimir E, Hospital T, Dawria A, Mohieldin A, Alshehk F, Tutu ZO. Missed opportunities of immunisation among children below 24 months visited elmak nimir teaching hospital, Sudan 2016. International Journal of Vaccines and Immunization. (2017) 2(3):33–7. doi: 10.25141/2475-6326-2017-3.0033
25. Muluneh F, Wubetu M, Abate A. Missed opportunity for routine immunization and its associated factors in gozamen district health centers, northwestern Ethiopia. Glob Pediatr Heal. (2020) 7. doi: 10.1177/2333794X20981306
26. Magadzire BP, Joao G, Bechtel R, Matsinhe G, Nic Lochlainn L, Ogbuanu IU. Reducing missed opportunities for vaccination in Mozambique: findings from a cross-sectional assessment conducted in 2017. BMJ Open. (2021) 11(12):1–10. doi: 10.1136/bmjopen-2020-047297
27. Kaboré L, Meda B, Médah I, Shendale S, Nic Lochlainn L, Sanderson C, et al. Assessment of missed opportunities for vaccination (MOV) in Burkina Faso using the world health Organization's Revised MOV strategy: findings and strategic considerations to improve routine childhood immunization coverage. Vaccine. (2020) 38(48):7603–11. doi: 10.1016/j.vaccine.2020.10.021
28. Aderibigbe SA, Ameen HA, Bolarinwa OA. Determinants of missed opportunities for immunization among under-five children in Ilorin metropolis. Trop J Health Sci. (2009) 24(March):18–23.
29. Jani JV, De Schacht C, Jani IV, Bjune G. Risk factors for incomplete vaccination and missed opportunity for immunization in rural Mozambique. BMC Public Health. (2008) 8:1–7. doi: 10.1186/1471-2458-8-1
30. Abdulraheem IS, Onajole AT, Jimoh AA, Oladipo AR. Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children. J Public Health Epidemiol. (2011) 3(4):194–203.
Keywords: missed opportunities, immunization, vaccine, dropout, Ethiopia
Citation: Kassa BG and Lul NC (2023) Missed opportunities for immunization among children 0 to 11 months of age that were attended to at debre tabor comprehensive specialized hospital, south gondar zone, Ethiopia. Front. Pediatr. 11:1169328. doi: 10.3389/fped.2023.1169328
Received: 19 February 2023; Accepted: 11 April 2023;
Published: 27 April 2023.
Edited by:
Ana Afonso, Nova University of Lisbon, PortugalReviewed by:
Imtiaz Hussain, Aga Khan University, PakistanKimberly Bonner, Centers for Disease Control and Prevention (CDC), United States
Bilkis Banu, Northern University, Bangladesh
© 2023 Kassa and Lul. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bekalu Getnet Kassa YmVrYWx1Z2V0bmV0OTQ3QGdtYWlsLmNvbQ==