
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 30 May 2023
Sec. Pediatric Hematology and Hematological Malignancies
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1166176
This article is part of the Research TopicDiagnosis and Therapy Pediatric Hematological Malignancies - Recent ProgressView all 5 articles
 Bárbara Ochoa-Fernández1*
Bárbara Ochoa-Fernández1* Víctor Galán-Gómez1
Víctor Galán-Gómez1 Pilar Guerra-García1,2
Pilar Guerra-García1,2 Sonsoles Sanromán1,2Isabel Martínez1
Sonsoles Sanromán1,2Isabel Martínez1 David Bueno1,2
David Bueno1,2 Yasmina Mozo1Luisa Sisinni1
Yasmina Mozo1Luisa Sisinni1 Itsaso Losantos1Berta González1,2
Itsaso Losantos1Berta González1,2 Antonio Pérez-Martínez1,2
Antonio Pérez-Martínez1,2
Objectives: This study aimed to evaluate the characteristics and outcomes of infant patients with leukemia.
Methods: A retrospective analysis was conducted in a cohort of 39 patients diagnosed with infant leukemia from 1990 to 2020 who underwent treatment at the pediatric hemato-oncology department of a tertiary hospital in Madrid, Spain.
Results: Of the 588 diagnosed cases of childhood leukemia, 39 (6.6%) cases were infant leukemia. The 5-year event-free survival and the 5-year overall survival were 43.6% (SE 4.1) and 46.5% (SD 24.08), respectively. In a univariate analysis, a younger age at diagnosis was associated with poorer outcomes (p = 0.027), as was induction failure (p = 0.0024). Patients treated with hematopoietic stem cell transplantation had better outcomes than non-transplanted patients (p = 0.001); however, the group comparisons that exclude patients who were unable to undergo transplantation due to refractoriness/relapse or death during treatment showed no significant differences.
Conclusions: The main risk factors that affected survival in our study were an age younger than 6 months and a poor response to induction therapy. It is important to identify poor prognostic factors in this population in order to seek different approaches that could improve outcomes.
Acute leukemia is the most common malignancy diagnosed in children. Although survival rates have greatly increased over time, infant leukemia (IL) remains a challenge, and therapeutic improvements are needed.
The term “infant leukemia” refers to acute leukemia diagnosed before the first year of life and represents a distinctive subgroup of patients with particular clinical and biological characteristics. Infant leukemia is a rare disease, with an estimated incidence of 45 cases per million in the United States, equivalent to 175 cases per year (1, 2). During the recent decades, infant leukemia comprised 5.5% of the cases of childhood leukemia in Spain, amounting to 186 cases (3). Within the infant group, leukemia is the second most common cancer after neuroblastoma and accounts for 16.4% of infant malignancies (4).
The particularities of infant leukemia include a female predominance (in contrast to male predominance in older children) and an increased incidence rate of acute myeloblastic leukemia (AML), a rate approximately twice that for older children, in whom there is a clear predominance of acute lymphoblastic leukemia (ALL). Clinically, the onset of infant leukemia tends to present with more aggressive features, including higher white blood cell (WBC) counts, hepatosplenomegaly, involvement of the central nervous system (CNS), and skin infiltration (5).
In terms of genetics, KMT2A or the lysine methyltransferase 2A gene (previously known as mixed-lineage leukemia, MLL) rearrangements are a primary characteristic of infant leukemia. KMT2A rearrangements (KMT2A-r) are balanced chromosomal translocations that appear in 5% of cases of childhood leukemia (80% of infant ALL cases and 50% of infant AML cases) (2). KMT2-r in ALL is associated with CD10 negativity and co-expression of myeloid antigens. KMT2A-r also confers different prognostic connotations between infant ALL and AML. The presence of KMT2A-r in ALL is associated with poor outcomes (6).
Although the long-term event-free survival (EFS) rates for childhood leukemia are near 80%, the prognosis for infants diagnosed with leukemia is unfavorable, and the treatment of this high-risk patient group remains a major challenge despite the use of intensified standard therapies (4, 6). The indication for hematopoietic stem cell transplantation (HSCT) is restricted to specific subgroups with risk factors of poor prognosis and is controversial in terms of efficacy and potential for acute and late toxicity (7).
The objective of this retrospective descriptive study is to reflect the experience of a single tertiary center over the past three decades.
We retrospectively analyzed a cohort of 39 patients diagnosed with infant leukemia from 1990 to 2020, who underwent treatment at the pediatric hemato-oncology department of a tertiary hospital in Madrid, Spain.
Infant leukemia was defined as acute leukemia diagnosed during the first year of life. The leukemia diagnosis was based on cytomorphology, immunophenotyping, cytogenetics (karyotype and fluorescence in situ hybridization, FISH), and molecular biology of bone marrow aspirate.
The variables that were analyzed included patients’ characteristics, such as age, sex, initial signs and symptoms, laboratory findings at diagnosis, CNS involvement, immunophenotype, HSCT, relapse, and follow-up (Table 1). Data were collected from the medical records of the hospital.

Table 1. Summary of the patients’ characteristics.
Patients with ALL were initially treated within the protocol from the Spanish Cooperative Group SHOP/ALL (1990–2016) and according to the INTERFANT-06 protocol since 2018 (8, 9). Patients with AML were treated within the SHOP/AML protocols at the beginning of the cohort study (1990–2014) and within the NOPHO-DBH AML 2012 trial since 2018.
This retrospective data collection study was approved by the ethics committee of University Hospital La Paz (Code PI-4575), and written informed consent to participate in this study was obtained from the parents/legal guardians.
Qualitative data are presented with absolute and relative frequencies. Quantitative data are presented as mean ± standard deviation (SD) if they followed normality and as median and interquartile ranges if not. Normality was studied employing the Kolmogorov–Smirnov test. The association between qualitative variables was analyzed with the χ2 test or Fisher's exact test.
Survival was determined by the 5-year overall survival (OS) rate, employing a Kaplan–Meier analysis. EFS was defined as the time from diagnosis to relapse or death from any cause. Transplant-related mortality (TRM) was defined as death after HSCT without disease progression or relapse. We performed a survival analysis employing a Kaplan–Meier estimator (log-rank tests were employed to compare the survival functions by groups) and Cox regression (to obtain the risks associated with the significant variables).
Differences were considered statistically significant at p ≤ 0.05, with a 95% confidence interval. The statistical analysis was conducted with the SAS 9.3 software (SAS Institute, Cary, NC, United States).
A total of 588 patients were diagnosed with childhood leukemia during this period. Of these, 39 (6.6%) were diagnosed with infant leukemia (patients’ demographics are summarized in Table 1). Due to the long period of the study, we divided it into two groups: an early period (from 1990 to 2005) and a late period (from 2006 to 2020) (Table 2).
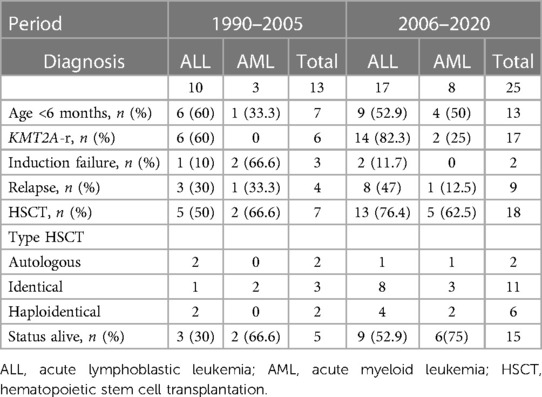
Table 2. Evolution of characteristics over the years.
There were 24 (61.5%) girls and 15 (38.5%) boys, with a mean age at diagnosis of 5.5 months (SD 3.5). A total of 27 (69%) patients were diagnosed with ALL, 11 (28%) with AML, and 1 patient with mixed-phenotype acute leukemia. At diagnosis, 12 (30.8%) patients had hyperleukocytosis >300,000 cells/mm3, 22 (59.5%) harbored KMT2A-r, and 2 (5.1%) had CNS involvement. Induction failure and relapse occurred in 6 (15.3%) and 14 (35.9%) patients, respectively. The median duration of the first remission before relapse was 4 (3.1–8.4) months.
A total of 26 (66.6%) patients underwent HSCT (Supplementary Table 1), 24 (92.3%) after achieving the first complete remission, 4 (15.4%) of them with autologous SCT. With a median follow-up of 15 months, the 5-year EFS and 5-year OS were 43.6% (SE 4.1) and 46.5% (SE 24.08), respectively. In a univariate analysis, a younger age at diagnosis was associated with poorer outcomes (p = 0.027), as was the failure to achieve remission after induction therapy (p = 0.0024) (Table 3). In our series, the patients who underwent HSCT had better outcomes than the non-transplanted patients (p = 0.001); however, group comparison taking into account the criteria for not performing HSCT did not show differences (see Table 4). TRM was 31.6%, and relapse after HSCT occurred in 7 (17.9%) patients.
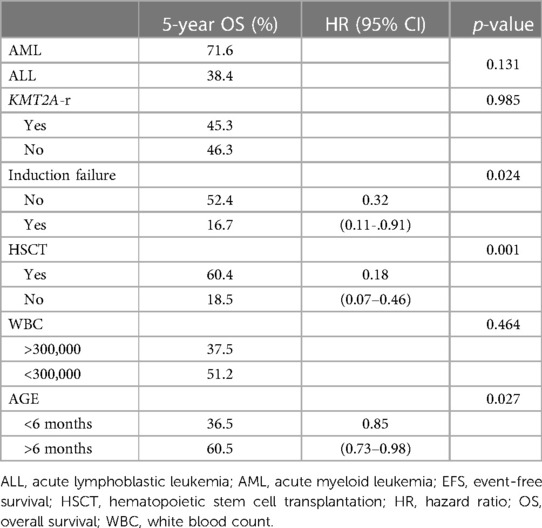
Table 3. Univariate analysis of prognostic factors.
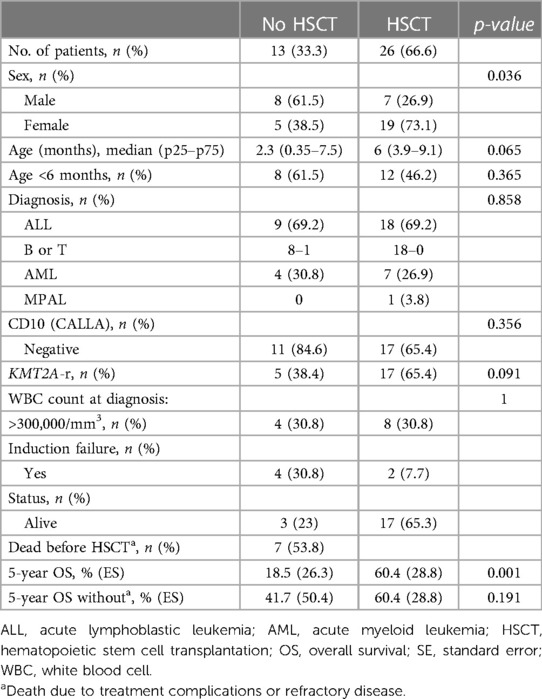
Table 4. Comparison between transplanted and non-transplanted patients.
For the ALL patients in the first period (1990–2005), the 5-year EFS and 5-year OS were the same at 30% (SE 14.5), and in the late period (2006–2020), the 5-year EFS and 5-year OS were 41.2 (SE 11.9) and 44.2 (SE 13.3), respectively.
For AML patients in the first period, the 5-year EFS and 5-year OS were the same at 66.7% (SE 27.2) and in the late period were 62.5 (SE 17.1) and 75 (SE 15.3), respectively. There was no statistically significant difference in EFS or OS between the early and late cohorts.
Although childhood leukemia is more frequently observed in male patients, infant leukemia is more common among females, a fact that is consistent in our study. Although sex does not appear to influence the outcomes in our study and other studies (6), recent results from the Children's Oncology Group (COG) describe better outcomes for girls with infant ALL (10).
The age at diagnosis was younger than 6 months in 20 (51.2%) patients, of whom 60% died. A younger age at diagnosis was associated with a poorer prognosis, which coincides with the findings of previous studies that established an age younger than 6 months as one of the main factors of poor prognosis in infant leukemia (8, 9).
Patients with infant leukemia usually have hepatosplenomegaly and extramedullary involvement. A physical examination revealed that 71% of our patients had hepatosplenomegaly and 7% presented skin infiltration, which was more frequent in patients with AML (27% vs. 15%). CNS involvement occurs more frequently in infant leukemia than in childhood leukemia; however, our findings differ from previous studies, with only 5.1% of CNS involvement at diagnosis, in contrast to results from the COG group (16.4%) (11) and the INTERFANT-06 protocol (16%) (8).
Phenotypically, infant ALL is often an early B-cell precursor and is associated with CD10 negativity and co-expression of myeloid antigens, which has been linked with these types of leukemia being resistant to standard ALL-based therapy (6, 12). Our cohort had a predominance of pro-B ALL, with 71.8% having CD10 negativity; however, this lack of CD10 antigen was not associated with worse outcomes.
The T-cell phenotype is associated with the worst outcome (13); in our cohort, only one patient had T-cell leukemia and died of progression 6 months after diagnosis.
AML accounted for 28% of the cases in this study. As in infant ALL, infant AML presents with relatively high WBC counts, hepatosplenomegaly, and CNS involvement. Unlike ALL, however, there is frequent skin infiltration (5). In our cohort, these characteristics were more frequent in ALL except for skin infiltration, which was more frequent in AML, at 27.3% (the comparison between ALL and AML is shown in Supplementary Table 2).
A total of 74% of our patients with ALL harbored KMT2A-r, while only 18.2% of those with AML had KMT2A-r. Our findings were similar to those reported in ALL, but with a lower incidence in AML, in which KMT2A-r is typically around 50% (8, 11, 14).
In our cohort, KMT2-r was not associated with poorer outcomes in either ALL or AML. The possible explanations for this are the small size of our sample; also, during the first decade of our study (1990s), cytogenetic techniques could give rise to more false negatives, as well as the fact that many of the patients without KMT2A-r had other factors described as poor prognosis (2), 80% of them were very young patients of age <6 months at diagnosis. In addition, this group included one patient with T-ALL and another with mixed-phenotype acute leukemia.
Treating infant ALL is challenging. Three major cooperative groups (INTERFANT, COG, and JPLSG—Japanese pediatric leukemia study group) (8, 11, 15) are conducting specific clinical trials to improve infant ALL treatment (2) and have reported several independent prognostic factors for infant ALL, including KMT2A-r, age, WBC count at diagnosis, and a poor prednisone response on day 8 (2).
In our patients with ALL, induction failure and relapse occurred in 15% and 36%, respectively. The median duration of first remission before relapse was 4 months. These results are consistent with larger studies that suggest that almost half of all infants with ALL will relapse, with most relapses occurring early (median of 10 months) (8, 9).
The 5-year OS in our ALL patients was 38.4% (SE 10), an abysmal result compared with the current outcomes reporting for IL. These results have been different over time, with 30% OS in the first period of the cohort (ES 14.5), when patients were treated in pediatric ALL protocols that are not specific for infants, and in general, there were fewer therapeutic options to improve the results (Table 2). In the second period, the results have improved, obtaining an OS of 44.2% (SE 13.3), a result similar to what is currently reported (8).
Outcomes for infants with AML are comparable with those of older children with similar cytogenetic features. Given the similar prognosis and therapeutic response, infants are generally treated with the same clinical trial protocols as older children (16). Induction failure and relapse occurred in 27% and 18% of our cohort with AML, respectively, and the median duration of the first remission before relapse was 10 months. In the early period of our cohort where the 5-year OS was 66.7% (ES 27.2) and in the late period 75% (ES 15.3), we see considerably better results than in ALL, as what has been reported in other series, and also an improvement in the most recent results.
The role of HSCT in infant leukemia is controversial. Regardless of diagnosis, HSCT in this vulnerable age group can prove difficult (16). For AML, HSCT indications are similar to those for older patients and are based on molecular features and therapeutic responses. A consolidative HSCT plays an important role for pediatric patients with high-risk AML, and this potential transplant benefit is extrapolated to infants, although large series of infants have not been examined (5).
The role of HSCT in infant ALL is less clear. An HSCT indication during the first complete remission has not yet been uniformly established for this age group, with the most high-risk infants in European and Japanese (but not US) protocols being stratified to HSCT according to the age at diagnosis, WBC counts above 300 × 109/L, and a poor prednisone response (17).
In our cohort, 26 (66.6%) patients underwent HSCT, of which 24 (92.3%) during their first complete remission (Figure 1). We saw an evolution from the first period when, according to local protocols, some patients underwent autologous HSCT as a consolidation treatment, a practice that has decreased in the most recent period (Table 2). On the other hand, we see an increase in the use of haploidentical HSCT, according to what has been reported in our country with the acquisition of experience and graft manipulation techniques in the recent decades (18). The 5-year OS for the patients who underwent HSCT was 60.4% vs. 18.5% for the non-transplanted patients, similar to that reported in INTERFANT-99 (a 4-year disease-free survival of 50% for HSCT vs. 37% for chemotherapy alone) (9). However, group comparisons that excluded the patients who were unable to undergo transplantation due to refractoriness/relapse or death during treatment showed no statistically significant differences between the HSCT and the non-HSCT groups (Table 4). TRM was 31.6%, consistent with the substantially higher risk of TRM reported for infants compared with older children (17).
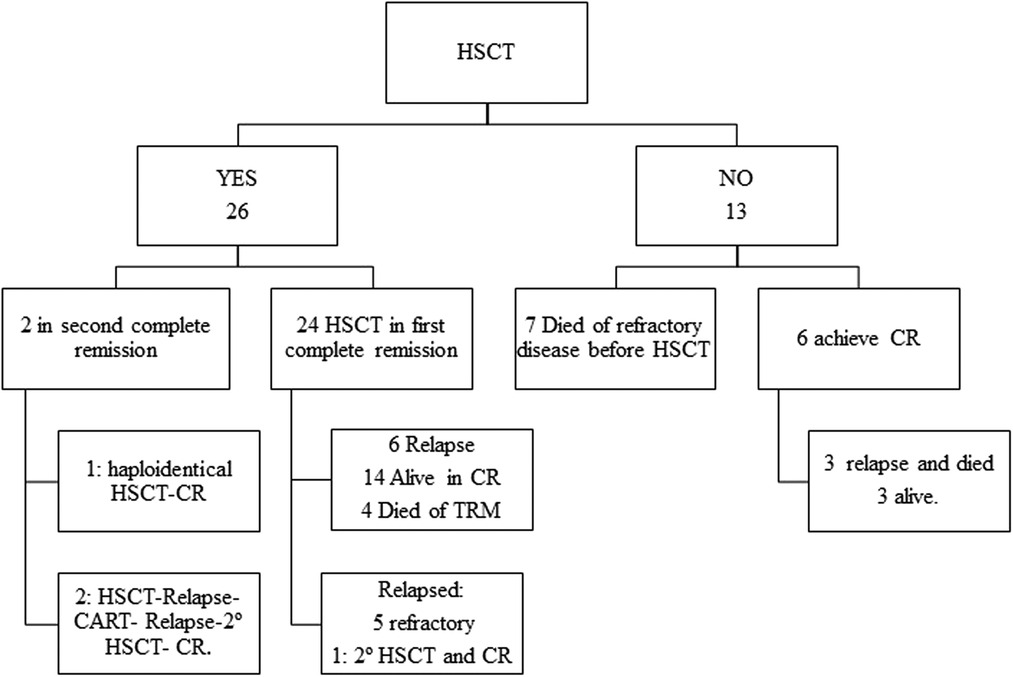
Figure 1. Follow-up of transplanted patients. CR, complete remission; HSCT, Hematopoietic stem cell transplantation; TRM, transplant-related mortality.
It is important to note that this study included various conditioning regimens and a variety of donor sources, which makes it difficult to evaluate the true benefit of a particular transplantation approach. HSCT is currently recommended for high-risk patients, although the occurrence of relapse after HSCT is also common (15, 19). In our study, 17.9% of the patients relapsed after HSCT.
Advances in molecularly targeted therapies and immunotherapy present promising opportunities for potential improvements. The incorporation of novel treatments in this young population suggests the possibility of reducing the toxicity and late effects associated with classical cytotoxic chemotherapy and HSCT (16).
Chimeric antigen receptor (CAR) T-cell therapies have shown exciting promise for pediatric patients with relapsed/refractory leukemia. Although antigen targets for ALL (CD19, CD22) and AML (CD33, CD123) could be useful for treating infant leukemia (20, 21), there are limitations to their use, including the development of lineage switching as an escape mechanism, especially in cells with KMT2A-r, in addition to the difficulty of apheresis and the subsequent manufacturing of CAR-T cells in infants (22, 23). In our cohort, one patient underwent CAR-T-cell therapy in 2020. This patient received CAR-T cells after a post-HSCT relapse; however, 9 months after administering the CAR-T cells, the patient experienced an isolated extramedullary relapse and underwent a second HSCT using a haploidentical donor, after which the patient remained in complete remission (24).
With a median follow-up of 15 months, the 5-year EFS and 5-year OS were 43.6% and 46.5%, respectively, similar to the results published in other series of infant leukemia (5, 25, 26). The closeness between EFS and OS reflects the difficulty of rescuing patients who relapse.
We can see the improvement in the results in our cohort from the 1990s to the present (Figure 2). This is a reflection of the implementation of new therapeutic strategies, the advance in the knowledge of the biology of IL and, in turn, the gain in expertise in the treatment of such vulnerable patients.

Figure 2. Overall survival between earlier versus later period of time.
Our results suggest that HSCT is a good and efficient option for treating selected patients. However, there remains a major issue in deciding which patients should undergo transplantation. More studies with larger patient groups are needed to re-evaluate the eligibility criteria for HSCT in this patient group.
The main risk factors that affected survival in our study were an age younger than 6 months and a poor response to induction therapy. There were no differences in the patients with KMT2A-r compared with the results reported by other studies.
Sensitivity to the initial therapy and good response at the end of the induction therapy were the determining factors that improved survival in our cohort, which are independent of other factors.
It is important to continue stratifying the treatment according to the factors that confer a poorer prognosis so as to improve the results for infant patients, whose condition does not behave like childhood leukemia and therefore does not respond to the same treatments.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the ethics committee of University Hospital La Paz (Code PI-4575).
BO-F, AP-M, VG-G, and BG contributed to the conception and design of the study. BO-F organized the database and wrote the first draft of the manuscript. IL performed the statistical analysis. VG-G, PG-G, LS, DB, YM, IM, and SS wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported in part by the National Health Service of Spain, Instituto de Salud Carlos III (ISCIII), FONDOS FEDER grant (FIS) PI18/01301, and the CRIS Cancer Foundation (http://criscancer.org)
We are indebted to all the patients who agreed to participate in this study, as well as to the hospital personnel involved in the study for their support and for the data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1166176/full#supplementary-material.
1. Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, et al. SEER cancer statistics review, 1975–2017. Bethesda, MD: National Cancer Institute (2017).
2. Brown P, Pieters R, Biondi A. How I treat infant leukemia. Blood. (2019) 133:205–14. doi: 10.1182/blood-2018-04-785980
3. Cañete Nieto A, Pardo Romaguera E, Muñoz López A, Valero Poveda S, Porta Cebolla S, Barreda Reines MS, et al. Cáncer infantil en España. Estadísticas 1980–2021. Registro Español de Tumores Infantiles (RETI-SEHOP). Valencia: Universitat de València (2022). Available at: https://www.uv.es/rnti/pdfs/Informe_RETI-SEHOP_1980-2021.pdf.
4. Kaatsch P. Epidemiology of childhood cancer. Cancer Treat Rev. (2010) 36:277–85. doi: 10.1016/j.ctrv.2010.02.003
5. Zweidler-McKay PA, Hilden JM. The ABCs of infant leukemia. Curr Probl Pediatr Adolesc Health Care. (2008) 38:78–94. doi: 10.1016/j.cppeds.2007.12.001
6. Brown P. Treatment of infant leukemias: challenge and promise. Hematol Am Soc Hematol Educ Progr. (2013) 2013:596–600. doi: 10.1182/asheducation-2013.1.596
7. Takachi T, Watanabe T, Miyamura T, Moriya Saito A, Deguchi T, Hori T, et al. Hematopoietic stem cell transplantation for infants with high-risk KMT2A gene-rearranged acute lymphoblastic leukemia. Blood Adv. (2021) 5:3891–9. doi: 10.1182/bloodadvances.2020004157
8. Pieters R, De Lorenzo P, Ancliffe P, Aversa LA, Brethon B, Biondi A, et al. Outcome of infants younger than 1 year with acute lymphoblastic leukemia treated with the interfant-06 protocol: results from an international phase III randomized study. J Clin Oncol. (2019) 37:2246–56. doi: 10.1200/JCO.19.00261
9. Pieters R, Schrappe M, De Lorenzo P, Hann I, De Rossi G, Felice M, et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (interfant-99): an observational study and a multicentre randomised trial. Lancet. (2007) 370:240–50. doi: 10.1016/S0140-6736(07)61126-X
10. Guest EM, Kairalla JA, Hilden JM, Dreyer ZE, Carroll AJ, Heerema NA, et al. Outstanding outcomes in infants with KMT2A-germline acute lymphoblastic leukemia treated with chemotherapy alone: results of the children’s oncology group AALL0631 trial. Haematologica. (2022) 107:1205–8. doi: 10.3324/haematol.2021.280146
11. Hilden JM, Dinndorf PA, Meerbaum SO, Sather H, Villaluna D, Heerema NA, et al. Analysis of prognostic factors of acute lymphoblastic leukemia in infants: report on CCG 1953 from the Children’s Oncology Group. Blood. (2006) 108:441–51. doi: 10.1182/blood-2005-07-3011
12. Pieters R, den Boer ML, Durian M, Janka G, Schmiegelow K, Kaspers GJ, et al. Relation between age, immunophenotype and in vitro drug resistance in 395 children with acute lymphoblastic leukemia—implications for treatment of infants. Leukemia. (1998) 12:1344–8. doi: 10.1038/sj.leu.2401129
13. Sison EAR, Brown P. Does hematopoietic stem cell transplantation benefit infants with acute leukemia? Hematol Am Soc Hematol Educ Progr. (2013) 2013:601–4. doi: 10.1182/asheducation-2013.1.601
14. Harrison CJ, Hills RK, Moorman AV, Grimwade DJ, Hann I, Webb DKH, et al. Cytogenetics of childhood acute myeloid leukemia: United Kingdom medical research council treatment trials AML 10 and 12. J Clin Oncol. (2010) 28:2674–81. doi: 10.1200/JCO.2009.24.8997
15. Tomizawa D, Miyamura T, Imamura T, Watanabe T, Moriya Saito A, Ogawa A, et al. A risk-stratified therapy for infants with acute lymphoblastic leukemia: a report from the JPLSG MLL-10 trial. Blood. (2020) 136:1813–23. doi: 10.1182/blood.2019004741
16. Ibrahimova A, Pommert L, Breese EH. Acute leukemia in infants. Curr Oncol Rep. (2021) 23:27. doi: 10.1007/s11912-021-01021-1
17. Balduzzi A, Buechner J, Ifversen M, Dalle J-H, Colita AM, Bierings M. Acute lymphoblastic leukaemia in the youngest: haematopoietic stem cell transplantation and beyond. Front Pediatr. (2022) 10:807992. doi: 10.3389/fped.2022.807992
18. Ochoa-Fernández B, Galán-Gómez V, Mestre C, González-Vicent M, Pascual A, Alonso L, et al. Haploidentical hematopoietic stem cell transplantation in pediatric and adolescent patients: a study of the Spanish hematopoietic stem cell transplantation group (GETH). Med Clin (Barc). (2022) 159:411–9. doi: 10.1016/j.medcli.2022.01.009
19. Tomizawa D, Miyamura T, Koh K, Ishii E. Acute lymphoblastic leukemia in infants: a quarter century of nationwide efforts in Japan. Pediatr Int. (2022) 64:e14935. doi: 10.1111/ped.14935
20. Britten O, Ragusa D, Tosi S, Kamel YM. MLL-rearranged acute leukemia with t(4;11)(q21;q23)-current treatment options. Is there a role for CAR-T cell therapy? Cells. (2019) 8:1–22. doi: 10.3390/cells8111341
21. Gardner R, Wu D, Cherian S, Fang M, Hanafi L-A, Finney O, et al. Acquisition of a CD19-negative myeloid phenotype allows immune escape of MLL-rearranged B-ALL from CD19 CAR-T-cell therapy. Blood. (2016) 127:2406–10. doi: 10.1182/blood-2015-08-665547
22. Moskop A, Pommert L, Baggott C, Prabhu S, Pacenta HL, Phillips CL, et al. Real-world use of tisagenlecleucel in infant acute lymphoblastic leukemia. Blood Adv. (2022) 6:4251–55. doi: 10.1182/bloodadvances.2021006393
23. Pasquini MC, Hu Z-H, Curran K, Laetsch T, Locke F, Rouce R, et al. Real-world evidence of tisagenlecleucel for pediatric acute lymphoblastic leukemia and non-Hodgkin lymphoma. Blood Adv. (2020) 4:5414–24. doi: 10.1182/bloodadvances.2020003092
24. Ghorashian S, Jacoby E, De Moerloose B, Rives S, Bonney D, Shenton G, et al. Tisagenlecleucel therapy for relapsed or refractory B-cell acute lymphoblastic leukaemia in infants and children younger than 3 years of age at screening: an international, multicentre, retrospective cohort study. Lancet Haematol. (2022) 9:e766–75. doi: 10.1016/S2352-3026(22)00225-3
25. Yaman-Bajin İ, Aytaç S, Kuşkonmaz B, Uçkan-çetinkaya D, Ünal Ş, Gümrük F, et al. Infant lymphoblastic leukemia: a single centers 10 year experience. Turk J Pediatr. (2019) 61:325–9. doi: 10.24953/turkjped.2019.03.002
Keywords: infant leukemia, acute lymphoblastic leukemia, acute myeloid leukemia, KMT2A rearrangement, hematopoietic stem cell transplantation, infant leukemia
Citation: Ochoa-Fernández B, Galán-Gómez V, Guerra-García P, Sanromán S, Martínez I, Bueno D, Mozo Y, Sisinni L, Losantos I, González B and Pérez-Martínez A (2023) Younger age and induction failure predict outcomes in infant leukemia: 30 years of experience in a tertiary center. Front. Pediatr. 11:1166176. doi: 10.3389/fped.2023.1166176
Received: 14 February 2023; Accepted: 24 April 2023;
Published: 30 May 2023.
Edited by:
Joanna Zawitkowska, Medical University of Lublin, PolandReviewed by:
Joanna Trelińska, Medical University of Lodz, Poland© 2023 Ochoa-Fernández, Galán-Gómez, Guerra-García, Sanromán, Martínez, Bueno, Mozo, Sisinni, Losantos, González and Pérez-Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bárbara Ochoa-Fernández YmFyYmFyYW9jaG9hZkBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.