
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr. , 17 July 2023
Sec. Pediatric Infectious Diseases
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1163103
 May Albarrak1
May Albarrak1 Mona Al Dabbagh2
Mona Al Dabbagh2 Hilal Al Hashami3
Hilal Al Hashami3 Omar Alzomor4
Omar Alzomor4 Ghassan Ghatasheh5
Ghassan Ghatasheh5 Nervana Habashy6
Nervana Habashy6 Ashraf Hassanien7
Ashraf Hassanien7 Andrés Pérez-López8,9*
Andrés Pérez-López8,9*
Urinary tract infections (UTIs) are common healthcare-associated and community-acquired bacterial infections in children. Data on pediatric UTIs in the Gulf Cooperation Council (GCC) region (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates) have not been collated. Our aim is to review the published literature on the risk factors, etiology, antimicrobial susceptibility, and treatment of pediatric (aged <18 years) UTIs from healthcare and community settings in the GCC countries.
Urinary tract infections (UTIs) are common in children (1–3). Up to 11% of children have had a UTI by 16 years of age, with higher infection rates in girls than boys (4–7). The diagnosis, prevalence and risk factors for UTIs may be stratified by patient sex or age, or the presence of underlying anatomical anomalies [such as vesicoureteral reflux (VUR)] that can lead to the recurrence of infection (1, 8). Awareness of the current risk factors for pediatric UTIs and factors contributing to recurrent UTIs can improve the clinical outcome of children with UTIs.
Uropathogenic Escherichia coli accounts for 80%–90% of pediatric UTIs (9). Resistance to common antibiotics used to treat UTIs, such as ampicillin and trimethoprim-sulfamethoxazole, is high among E. coli urinary isolates from children in the Gulf Cooperation Council (GCC) region [Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates (UAE)] (10). Furthermore, isolates producing extended-spectrum β-lactamases (ESBLs) exhibit not only resistance to third- and fourth-generation cephalosporins and monobactams but also cross-resistance to other antibiotic classes, such as aminoglycosides and fluoroquinolones, are increasingly collected in GCC countries (10).
The challenges of managing pediatric UTIs in the GCC region have not been documented in a single article. Therefore, this review will collate data on risk factors, pathogens, resistance phenotypes, and antimicrobial management practices for pediatric UTIs within the region. Our objective is to provide a comprehensive assessment of the current knowledge on pediatric UTIs to improve diagnostic accuracy and help clinicians make rational therapeutic choices for UTIs, to improve the health of children in the region.
This review evaluated relevant studies published between 1st January 2011 and 31st March 2022 on the PubMed and Google Scholar databases. We excluded non-English language articles, case reports, letters, books, editorials, notes, and conference abstracts.
The primary search terms were “urinary tract infection” and “pediatric”, followed by secondary terms relating to the review topics (shown in Supplementary Table S1). A free text search in title and abstract fields was also performed. Study methodology information and relevant study data were extracted from each article by two independent reviewers. Study information and findings not presented in-text are presented in Supplementary Tables S2–S4. Study data that were omitted from Tables 1, 2 or Supplementary Tables S2–S4 were not available in that publication.
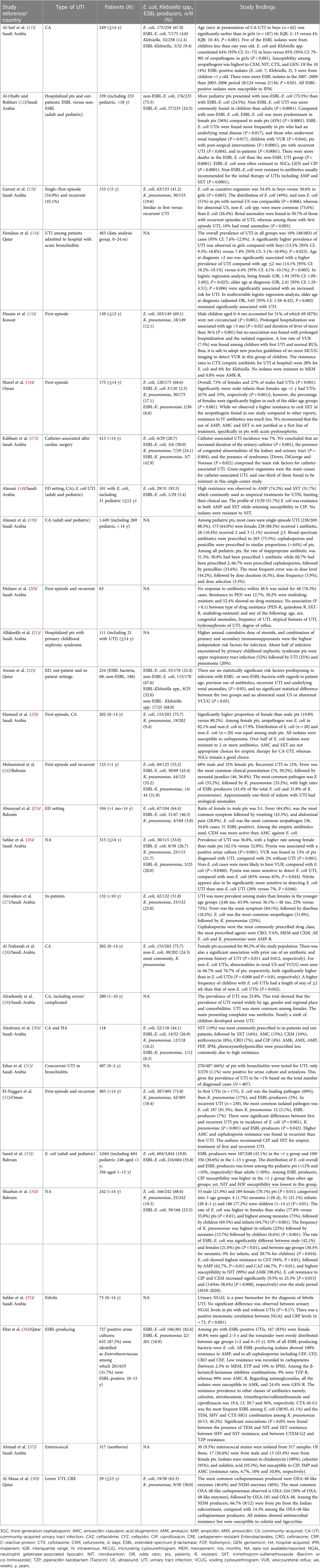
Table 1. Summary table of study findings on pediatric UTIs in the GCC countries (2011–2022).
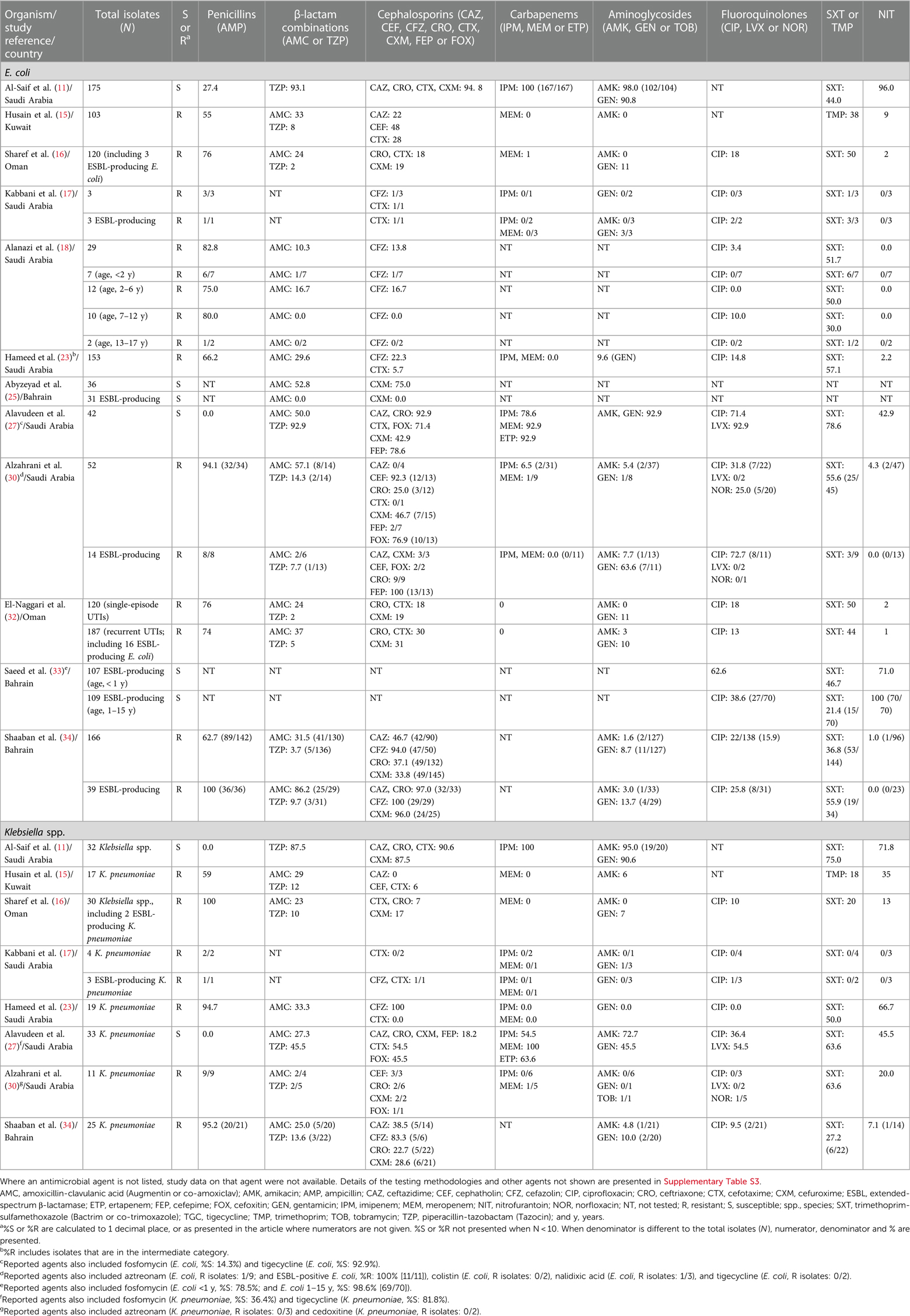
Table 2. Antimicrobial susceptibility or resistance among Escherichia coli, Klebsiella spp., and ESBL-producing isolates from pediatric UTIs in the GCC countries (2011–2022).
Following initial identification and screening of publication titles, 38 full-text articles remained (Bahrain, 4; Kuwait, 1; Oman, 4; Qatar, 5; Saudi Arabia, 23; and the UAE, 1). Nine articles (Oman, 2; Qatar, 1; Saudi Arabia, 5; and the UAE, 1) were excluded for not differentiating data for extraction.
The final GCC study number totaled 28: 24 retrospective studies (11–34) and 4 cross-sectional studies (35–38) (Supplementary Table S4). One set of clinical guidelines (39) was included. Four studies included adult patient data (adult ages defined as >12 years (18), >15 years (19), >15 years (33) and >18 years (12):), presented separately from pediatric patients (Supplementary Table S4).
The Saudi Pediatric Infectious Diseases Society (SPIDS) guidelines on community-acquired UTI (CA-UTI) recommend transurethral catheterization for collecting urine from infants and non-toilet-trained children to minimize bacterial contamination from the skin (39). Catheterization was used in 15 of all 28 studies (53.6%) (Supplementary Table S2) (11, 13, 14, 16, 17, 22, 24, 26–28, 30–32, 36, 38) and specified for younger children (≤2 years) in 5 studies (13, 26, 28, 36, 38). One study reported catheterization use for most patients aged <2 years and midstream collection for most aged >2 years (Supplementary Table S2) (13). In the community setting, clean catch samples may be preferred to catheterization (16). Clean catch urine was used in 13 of all studies (46.4%) (11, 13, 16, 18, 19, 22, 25–27, 30, 33, 35, 38) and suprapubic aspiration in 8 (28.6%) (17, 22, 24, 26, 28, 30, 32, 36). Urinary bag collection [not recommended by SPIDS (39)] was used in three studies (10.7%) (11, 30, 37) and excluded in three (10.7%) (13, 24, 28). Seven studies (25.0%) omitted the method of urine collection (12, 15, 20, 21, 23, 29, 34).
SPIDS defines UTI as significant bacteriuria in a symptomatic patient (febrile and/or with urinary symptoms) and recurrent UTI as ≥2 episodes of symptomatic UTI within 12 months (39). Their threshold for significant bacteriuria in colony-forming units (CFU) ranges from any number for suprapubic aspiration to ≥100,000 CFU/ml for clean catch urine. The American Association of Pediatrics (AAP) threshold is 50,000 CFU/ml for catheterization in febrile infants aged 2–24 months (40).
Positive pyuria by urine microscopy was an inclusion criterion of two studies (Supplementary Table S2) (15, 28) and was recorded in 25.6%–92.6% of patients (16, 23, 24, 26, 28). One study found an independent association between pyuria and positive urine culture (P = 0.001) (Table 1) (26). Pyuria (P = 0.044) and nitrite (P = 0.046) were significantly sensitive to detect E. coli UTI, compared with non-E. coli UTI (Table 1) (26).
SPIDS advocates renal and bladder ultrasonography as a safe, noninvasive procedure for the detection of abnormalities and renal infections in preference to micturating or voiding cystourethrogram (MCUG or VCUG) (39). Renal ultrasound was performed for 66.4%–91.3% of patients, and abnormal findings were recorded in 11.4%–51.0% (Supplementary Table S4) (13, 15, 22, 24, 28). Overall, 11.5% (104/901) of patients across seven studies had VUR (Supplementary Table S4) (13, 15, 20, 22, 24, 26, 27). Following MCUG, VUR was detected in 13.0% of patients with a first UTI and 23.1% with recurrent UTI (Supplementary Table S4) (15). Among patients with ESBL-producing uropathogens, 42.9% had VUR (22). Children with their first UTI and normal renal ultrasound were less likely to have VUR and were recommended not to undergo MCUG (Table 1) (15).
The predominant symptom was fever (50.3%–86.6%), with a regional prevalence of 60.7% (784/1,292) (Supplementary Table S4) (15, 16, 23–25, 27, 32). Fever was more common in children aged ≤2 years (16, 24) in two studies, and first vs. recurrent UTI [50.3% and 24.8%, respectively (P < 0.001)] (Supplementary Table S4) (32). Two studies included only febrile children (14, 35).
Other common symptoms (>20% of each study cohort) were urinary frequency, urgency or dysuria, nausea, vomiting, and abdominal pain (Supplementary Table S4) (15, 16, 25). Nausea and/or vomiting rates were higher in patients aged ≤2 years (P = 0.002), whereas rates of abdominal pain and urinary symptoms were higher in older children [2–14 years (P < 0.001)] (16). In addition, nausea and/or vomiting and abdominal pain were significantly more common in first vs. recurrent UTI (P < 0.001) (Supplementary Table S4) (32).
Blood C-reactive protein (>5 mg/L) did not significantly change with patient age (16) or between recurring and first-episode UTI (32). SPIDS advises against routinely obtaining these laboratory parameters in children >3 months with suspected UTI who otherwise appear healthy (39).
The prevalence of pediatric UTI across four studies including adults was 18.6%–68.7% (12, 18, 19, 33). In three studies, UTI was more common among younger patients aged <2 years (13, 15, 20), whereas two studies found a higher rate of UTI in patients aged 1–14 years (25, 34). Univariate and multivariate analyses showed that CA-UTI was associated with ages 1–6 years (29).
Overall, 65.0% (2,550/3,924) of UTI patients were girls. More girls than boys had a UTI in 15 studies (Supplementary Table S4) (11, 12, 14, 19, 22, 23, 25, 26, 28–30, 32, 34, 36, 38); the difference was statistically significant in three studies (one including adults) (Supplementary Table S4) (12, 14, 34). Conversely, more boys had UTIs in seven studies (13, 15, 17, 20, 24, 27, 37), with younger patients (<5 years) (13, 24, 37) or higher rates of UTIs in younger males (<48 months) and older females (overall, 48 months to 14 years) [15 (not significant), 16 (P < 0.001), 27 (P = 0.001)]. Boys presented with CA-UTI at a significantly younger age than girls (Table 1) (11).
In other studies, being uncircumcised was associated with UTI (7, 41). In the current review, only three studies examined circumcision (13, 15, 23). In one study, most boys aged <6 months with a first UTI were uncircumcised (87%) (Table 1) (15). The circumcision rate was 67.5% among patients aged <14 years (23), whereas, in the other study, UTIs were more common in younger patients (<2 years), even in circumcised males (13).
Female sex (P = 0.018), antibiotic use (P = 0.015) and VUR (P = 0.019) were associated with UTI (26). Prolonged hospitalization (>7 days) was associated with age <3 months (P = 0.02) and duration of fever of >36 h (P = 0.001), but not with the isolated uropathogen (Table 1) (15).
Patient comorbidities (such as hydronephrosis and congenital abnormalities) were associated with UTI (P = 0.05) (29). UTI among patients with acute bronchiolitis was associated with female sex (P = 0.025) and age >2 months (P = 0.006) (Table 1) (14). In another study of bronchiolitis, the youngest patients (<3 months) were more likely to be tested for a UTI (P < 0.0001) (31).
Following cardiac surgery, 7.0% of patients had UTIs (all catheter-associated) (17). Prolonged urinary catheterization, the presence of congenital abnormalities of the kidney and urinary tract, and Down, DiGeorge, and Noonan syndromes were associated with UTI (Table 1) (17).
Compared with E. coli, non-E. coli UTIs were associated with hospitalization >7 days (P = 0.042), male sex (P < 0.0001), younger age [<4 years (P = 0.01)], prior use of antibiotics (P = 0.011), or history of UTI (P = 0.012) (Table 1) (28). Significantly higher rates of abnormalities, such as VUR, were found with non-E. coli UTIs (Table 1) (13, 26, 28). It is noteworthy that renal and bladder imaging methods are recommended for febrile UTIs caused by non-E. coli species (39). The percentages of E. coli (49%) and non-E. coli (51%) in patients with normal ultrasound were comparable (Table 1) (13).
One study of adults and children in Saudi Arabia found that significantly more UTI patients had non-ESBL-producing than ESBL-producing E. coli, and ESBL-producing E. coli were associated with VUR in children (P = 0.044) (Table 1) (12). The percentage of ESBL-producing E. coli was higher in male than female patients (P < 0.01); in neonates than older children and infants (P = 0.016) (34); and in recurrent than first UTIs (32). In contrast, no association was found between ESBL- or non-ESBL-producing bacteria and patient sex, age group, previous use of antibiotics, recurrent UTI, abnormal renal ultrasound, or abnormal VCUG in CA-UTI (Table 1) (22). Antibiotic use prior to hospital admission was recorded for 29.7% (28) and 40.6% (22) of patients (of which 27.2% had ESBL-producing bacteria) (22).
The prevalence of recurrent UTI was 28.5% (542/1,900) (Supplementary Table S4) (13, 15, 19, 20, 22, 24, 28, 29, 32). The rate of renal anomalies was higher in recurrent (50.7%) than single-episode UTI [10% (P < 0.005)] (13). In univariate and multivariate analyses, younger patient age (<6 years) and male sex, but not comorbidities (such as congenital abnormalities and immune disorders), were significantly associated with severe/complicated CA-UTI (defined as UTI which required hospitalization, presented with pyelonephritis, or recurrent UTI <30 days after initial diagnosis) (29).
E. coli was predominant (26.1%–100% of isolates), with a regional prevalence of 64.9% (1,898 E. coli among 2,925 uropathogens) (11, 13, 16–18, 22–28, 30, 32–34). ESBL-producing uropathogens were documented in 15 studies (Supplementary Table S4) (11, 12, 16–18, 22–26, 30, 32–34, 36). The regional prevalence of ESBL-producing E. coli and K. pneumoniae was 25.0% (480 of 1,918 E. coli) and 19.8% (37 of 187 K. pneumoniae), respectively (11, 12, 16–18, 22, 24–26, 30, 32–34). Half of all ESBL-producing uropathogens from CA-UTIs were isolated from children aged <1 year and more ESBL-producers were isolated in 2007–2009 than 2003–2006 (P = 0.05) (Table 1) (11).
Klebsiella spp. (predominantly Klebsiella pneumoniae) were the second most common uropathogens (3.8%–35.2% of isolates), with a regional prevalence for K. pneumoniae of 13.8% (377 isolates among 2,723 uropathogens) (11, 13, 17, 22–25, 27, 30).
Other isolated uropathogens included Pseudomonas aeruginosa, Proteus mirabilis, Enterococcus spp., and Enterobacter spp. (Supplementary Table S4) (11, 15, 17, 18, 22–27, 30, 32, 34, 37).
Resistance among E. coli was highest to ampicillin (62.7%–82.8%) and cefazolin (94.0%) in Bahrain and Saudi Arabia (Table 2) (18, 34). Cefotaxime resistance was 28% in Kuwait (15) among E. coli, and cefuroxime resistance in Bahrain increased significantly from 2018 to 2020 (Table 1) (34). More than 90% of E. coli isolated from in-patients were susceptible to ertapenem and meropenem (27). In Oman, meropenem resistance was higher among non-E. coli than E. coli (including ESBL-producing isolates) (P < 0.001) for recurrent UTIs (32).
More than 96% of ESBL-producing E. coli from children in Bahrain (Table 2) (34) and all ESBL-producing isolates (83% E. coli) from Qatar were resistant to ceftriaxone (Table 1) (36).
Among all K. pneumoniae, >90% of isolates were susceptible to cefotaxime, ceftriaxone, and meropenem (Table 2) (11, 15, 16, 23, 27). Overall resistance to ampicillin (which is commonly used to treat UTI caused by E. faecalis) was 26.9% among enterococci (37).
Resistance to trimethoprim-sulfamethoxazole among urinary E. coli was 36.8%–55.6% in Saudi Arabia (16, 18, 30, 32, 34), whereas low resistance (≤9%) or high susceptibility (>90%) was reported to amikacin, gentamicin, levofloxacin, nitrofurantoin or tigecycline in Bahrain, Kuwait, Oman, and Saudi Arabia (15, 16, 18, 27, 30, 34). In Bahrain, ciprofloxacin resistance in E. coli increased significantly from 2018 to 2020 (Table 1) (34). Colistin and nitrofurantoin resistance was higher in non-E. coli than E. coli (including ESBL-producing isolates) from recurrent UTIs (P < 0.001) (32).
No ESBL-producing isolates (E. coli, 83%) from Qatar were resistant to amikacin, with higher resistance to nitrofurantoin (13.0%), gentamicin (24.4%), and trimethoprim-sulfamethoxazole (59.7%) (Table 1) (36). Susceptibility among ESBL-producing E. coli from Bahrain was highest to nitrofurantoin and fosfomycin (71.0%–100%) (Table 2) (33). All carbapenem-resistant urinary Enterobacterales were resistant to ciprofloxacin, and susceptible to colistin and tigecycline (38).
Among K. pneumoniae, >90% of isolates were susceptible to the tested aminoglycosides (Table 2) (11, 15, 16, 23, 27). The susceptibility of K. pneumoniae to trimethoprim-sulfamethoxazole was 63.6% (27). Among enterococci from newborns, the lowest resistance was to ciprofloxacin (6.7%) (37).
Multidrug resistance [defined by the authors as resistance to ≥3 antimicrobial classes in the testing panel (Supplementary Table S3)], was found in 10.3% of E. coli (18). Another study found no significant association between age group, patient sex or congenital anomalies (including VUR) in pediatric UTI patients and urinary isolates exhibiting multidrug resistance (overall rate, 30.2%) (Table 1) (20). Their study determined a higher rate of multidrug resistance in recurrent vs. first episode UTIs (50.0% and 22.7%, respectively) (20).
Most pediatric ESBL-producing E. coli isolates (61.1%) harbored the blaCTX−M−G1 gene, whereas 46.2% of ESBL-producing K. pneumoniae carried blaSHV, blaTEM and blaCTX−M−G1 genes (Table 1) (36). The distribution of individual ESBL genes did not correlate with patient age (36).
Similar findings were demonstrated by a study in Qatar of pediatric ESBL-producing E. coli and K. pneumoniae (52.2% of isolates were urinary) (42). CTX-M group 1 enzymes (CTX-M-15, 87.8%) were the most prevalent ESBL enzymes and all isolates were resistant to ceftriaxone (42).
A study of carbapenem-resistant Enterobacterales (63.3% E. coli; 30% K. pneumoniae) in Qatar revealed that carbapenem resistance was largely attributed to a limited number of OXA-48-like and NDM carbapenemases, suggesting that certain international high-risk clones associated with other carbapenemase genes such as blaKPC-type, have not spread locally (38).
For CA-UTI, SPIDS recommends first-line oral amoxicillin-clavulanic acid, cephalexin, cefuroxime, or cefprozil (39). The Qatar Ministry of Public Health (MOPH) recommends amoxicillin-clavulanic acid or a third-generation cephalosporin (3GC) as an empiric oral therapy, and gentamicin, amoxicillin-clavulanic acid, or ceftriaxone as empiric intravenous (IV) therapy (43). For infants and children hospitalized with a CA-UTI, an IV parenteral 3GC (such as ceftriaxone) is recommended (39). In-patients were mostly prescribed a 3GC (23), and patients hospitalized with a first UTI were given cefotaxime as empiric therapy before uropathogen susceptibilities were confirmed (15).
For in-patients with previous UTIs caused by ESBL-producing uropathogens, and in those who have been recently exposed to cephalosporins, gentamicin should be considered (39). Aminoglycoside therapy in combination with ceftriaxone may be indicated in critically ill patients and in those whose clinical condition worsens after starting the first-line antimicrobial therapy (39). A similar proportion of patients with ESBL-producing bacteria received IV antibiotics as in-patients or oral antibiotics as out-patients (27.8% and 26.1%, respectively) (22).
In the emergency department, most pediatric patients received a broad-spectrum antibiotic for CA-UTI (75.5%), mostly a cephalosporin (43.5%) or penicillin (44.2%), namely amoxicillin-clavulanic acid (29.4%) or cefprozil (23.0%) (Supplementary Table S4) (19). In a tertiary hospital, ceftriaxone (29.5%), vancomycin (25.0%), and meropenem (20.5%) were predominantly prescribed (27). In the in-patient and out-patient departments, nitrofurantoin (19%), trimethoprim-sulfamethoxazole (16%), and amoxicillin-clavulanic acid (15%) were mostly prescribed (Table 1) (30).
The evidence presented in this review indicates limited published data from the UAE and a lack of studies on HA-UTIs. Also, most studies specified a patient age of <14 years, while four studies included patients aged 14–18 years (12, 18, 19, 33). GCC data are lacking on predictors of treatment failure; clinical outcomes; epidemiological data on multidrug resistance; complicated UTI in addition to the implication of prophylaxis on resistance rates; and the correlation of antimicrobial resistance rates with previous antimicrobial use. Further studies are also warranted to monitor the trends in rates of resistance phenotypes and antimicrobial resistance over time.
Fever was the predominant symptom of pediatric UTI in the GCC countries. UTIs were more prevalent in girls, overall, and in boys aged <5 years. The predominant uropathogen was E. coli (including ESBL-producing isolates). ESBL-producing uropathogens are an established cause of UTI in the region, whereas CRE organisms (predominantly E. coli, followed by K. pneumoniae) are emerging (38). Guidelines on pediatric UTI from the neighboring region of Asia also found a higher incidence of UTI in boys than girls of a younger age (≤3 months) (44).
Existing data suggest that ampicillin and trimethoprim-sulfamethoxazole are not recommended empiric agents for pediatric UTIs in the GCC region due to high resistance rates (18, 33, 34, 39). Furthermore, our review found that 3GCs are commonly prescribed in GCC countries for the empirical treatment of children with pyelonephritis that required hospitalization, despite high regional 3GC resistance (15, 39, 43). Of note is that 3GC resistance in our region is mainly attributed to CTX-M-type ESBL enzymes that exhibit higher in vitro activity against cefotaxime and ceftriaxone than other oxyimino-cephalosporins (36, 42). Nevertheless, observational studies have not observed significant differences in clinical response and outcome in ESBL UTI between patients started on 3GC and those initially receiving effective agents, and between UTI caused by resistant and susceptible strains in patients started on 3GC, suggesting that cefotaxime or ceftriaxone are reasonable empirical choices until antimicrobial susceptibility testing results are available (45–47).
Empirical use of aminoglycosides due to the high prevalence of uropathogens resistant to 3GC has been proposed in Kuwait (15). Gentamicin is recommended by SPIDS and Qatar MOPH, particularly in patients recently exposed to cephalosporins (39, 43). However, the prevalence of gentamicin resistance among ESBL-producing uropathogens, especially E. coli, is >20% in these countries (30, 36). Therefore, amikacin, which is increasingly used in many countries as a carbapenem-sparing option, may be a suitable option given the low amikacin resistance rates among ESBL-producing uropathogens in the GCC region, particularly with MIC ≤4 mg/L (15, 48–51). Empirical treatment with carbapenems (meropenem if aged <3 months or ertapenem if aged >3 months) should be reserved for critically ill children, particularly those having a previous UTI caused by, or other risk factors for, ESBL-producing uropathogens. Alternatively, ceftazidime-avibactam, a novel cephalosporin/β-lactamase inhibitor combination that inactivates ESBL and OXA-48-type enzymes, could be considered a treatment option for ESBL pyelonephritis (52).
The treatment of UTIs caused by carbapenemase-producing uropathogens in our region is challenging. Although aztreonam is stable against NDM and 3GC against OXA-48 enzymes, none of these agents can be empirically used to treat UTI caused by NDM and OXA-48 producers as most isolates in our region co-produce CTX-M-type ESBL (38). It could be speculated that susceptibility to aztreonam might be restored by adding avibactam, making aztreonam-avibactam or ceftazidime-avibactam combined with aztreonam, theoretically appealing alternatives for pyelonephritis caused by NDM producers. Ceftazidime-avibactam and meropenem, for strains with meropenem MIC <8 mg/L, could be considered to treat pyelonephritis caused by OXA-48 producers (53, 54). Finally, oral nitrofurantoin or fosfomycin can be used to treat uncomplicated lower UTI caused by ESBL and carbapenemase-producing E. coli in our region.
In conclusion, our review showed that UTIs are increasingly caused by antimicrobial-resistant uropathogens in the pediatric population of GCC countries. Further epidemiological and clinical studies are needed to optimize diagnostic and antimicrobial stewardship strategies in pediatric UTIs in the GCC region.
All authors were involved in data interpretation, as well as drafting and reviewing the manuscript. All authors read and approved the final submitted version.
This work is funded by Pfizer. Medical writing support was provided by Neera Hobson, Wendy Hartley, and Wendy Wilkinson of Micron Research Ltd. (Ely, UK), and was funded by Pfizer.
NH and AH are employees of Pfizer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1163103/full#supplementary-material
1. Foxman B, Brown P. Epidemiology of urinary tract infections: transmission and risk factors, incidence, and costs. Infect Dis Clin North Am. (2003) 17:227–41. doi: 10.1016/s0891-5520(03)00005-9
2. Saleem Z, Godman B, Hassali MA, Hashmi FK, Azhar F, Rehman IU. Point prevalence surveys of health-care-associated infections: a systematic review. Pathog Glob Health. (2019) 113:191–205. doi: 10.1080/20477724.2019.1632070
3. Zhu C, Wang DQ, Zi H, Huang Q, Gu JM, Li LY, et al. Epidemiological trends of urinary tract infections, urolithiasis and benign prostatic hyperplasia in 203 countries and territories from 1990 to 2019. Mil Med Res. (2021) 8:64. doi: 10.1186/s40779-021-00359-8
4. Hellström A, Hanson E, Hansson S, Hjälmås K, Jodal U. Association between urinary symptoms at 7 years old and previous urinary tract infection. Arch Dis Child. (1991) 66:232–4. doi: 10.1136/adc.66.2.232
5. Coulthard MG, Lambert HJ, Keir MJ. Occurrence of renal scars in children after their first referral for urinary tract infection. Br Med J. (1997) 315:918–9. doi: 10.1136/bmj.315.7113.918
6. Mårild S, Jodal U. Incidence rate of first-time symptomatic urinary tract infection in children under 6 years of age. Acta Paediatr. (1998) 87:549–52. doi: 10.1111/j.1651-2227.1998.tb01502.x
7. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. (2008) 27:302–8. doi: 10.1097/INF.0b013e31815e4122
8. Tullus K, Shaikh N. Urinary tract infections in children. Lancet. (2020) 395:1659–68. doi: 10.1016/S0140-6736(20)30676-0
9. Leung AK, Wong AH, Leung AA, Hon KL. Urinary tract infection in children. Recent Pat Inflamm Allergy Drug Discov. (2019) 13:2–18. doi: 10.2174/1872213X13666181228154940
10. Bryce A, Hay AD, Lane IF, Thornton HV, Wootton M, Costelloe C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: systematic review and meta-analysis. Br Med J. (2016) 352:i939. doi: 10.1016/j.clp.2014.10.003
11. Al-Saif MA, Al-Abdi SY, Samara JT, Al-Rahman NG, Mousa TA, Alabdulbaqi MA, et al. Antibiotic sensitivity pattern of common community-acquired uropathogens in children in a Saudi tertiary care hospital. Saudi Med J. (2012) 33:565–7.22588821
12. Al-Otaibi FE, Bukhari EE. Clinical and laboratory profiles of urinary tract infections caused by extended-spectrum beta-lactamase-producing Escherichia coli in a tertiary care center in central Saudi Arabia. Saudi Med J. (2013) 34:171–6.23396464
13. Garout WA, Kurdi HS, Shilli AH, Kari JA. Urinary tract infection in children younger than 5 years: etiology and associated urological anomalies. Saudi Med J. (2015) 36:497–501. doi: 10.15537/smj.2015.4.10770
14. Hendaus MA, Alhammadi AH, Khalifa MS, Muneer E, Chandra P. Risk of urinary tract infection in infants and children with acute bronchiolitis. Paediatr Child Health. (2015) 20:e25–9. doi: 10.1093/pch/20.5.e25
15. Husain EH, Al-Saleem T, Marwan Y, Al-Jalahma M, Al-Kandari F. Management of pediatric urinary tract infections in Kuwait: current practices and practicality of new guidelines. Kuwait Med J. (2015) 47:139–43.
16. Sharef SW, El-Naggari M, Al-Nabhani D, Al Sawai A, Al Muharrmi Z, Elnour I. Incidence of antibiotics resistance among uropathogens in omani children presenting with a single episode of urinary tract infection. J Infect Public Health. (2015) 8:458–65. doi: 10.1016/j.jiph.2015.01.005
17. Kabbani MS, Ismail SR, Fatima A, Shafi R, Idris JA, Mehmood A, et al. Urinary tract infection in children after cardiac surgery: incidence, causes, risk factors and outcomes in a single-center study. J Infect Public Health. (2016) 9:600–10. doi: 10.1016/j.jiph.2015.12.017
18. Alanazi MQ, Alqahtani FY, Aleanizy FS. An evaluation of E. coli in urinary tract infection in emergency department at KAMC in Riyadh, Saudi Arabia: retrospective study. Ann Clin Microbiol Antimicrob. (2018) 17:3. doi: 10.1186/s12941-018-0255-z
19. Alanazi MQ. An evaluation of community-acquired urinary tract infection and appropriateness of treatment in an emergency department in Saudi Arabia. Ther Clin Risk Manag. (2018) 14:2363–73. doi: 10.2147/TCRM.S178855
20. Hisham D, Safdar OY, Shalaby M, Sabbahi M, Ashgar M, Shafi R, et al. Evaluating antimicrobial resistance patterns of the etiological agents of urinary tract infections. Australasian Med J. (2018) 11:96–106. doi: 10.21767/AMJ.2018.3310
21. Alfakeekh K, Azar M, Al Sowailmi B, Alsulaiman S, Al Makdob S, Omair A, et al. Immunosuppressive burden and risk factors of infection in primary childhood nephrotic syndrome. J Infect Public Health. (2019) 12:90–4. doi: 10.1016/j.jiph.2018.09.006
22. Awean GZ, Salameh K, Elmohamed H, Alshmayt H, Omer MR. Prevalence of ESBL urinary tract infection in children. J Adv Pediatr Child Health. (2019) 2:004–7. doi: 10.29328/journal.japch.1001004
23. Hameed T, Al Nafeesah A, Chishti S, Al Shaalan M, Al Fakeeh K. Community-acquired urinary tract infections in children: resistance patterns of uropathogens in a tertiary care center in Saudi Arabia. Int J Pediatr Adolesc Med. (2019) 6:51–4. doi: 10.1016/j.ijpam.2019.02.010
24. Mohammed D, Isa HM, Nasser AA. Urinary tract infections in infants: etiology and associated urological anomalies. Bahrain Med Bull. (2019) 41:25–8.
25. Abuzeyad FH, Ashraf MK, Ebrahim A, Ullah S, Yaqub M, Shoaib M, et al. Clinical presentation, culture and sensitivity pattern of urinary tract infection. Bahrain Med Bull. (2020) 42:20–3.
26. Safdar O, Marouf A, Sait R, Bayazeed L, Silawi R, Mustafa LH, et al. Urine analysis sensitivity and specificity for paediatric urinary tract infections. Australasian Med J. (2020) 13(12):330–7. doi: 10.35841/1836-1935.13.12.330-337
27. Alavudeen SS, Asiri AA, Fageeh SA, Aljarie AA, Iqbal MJ, Khan NA, et al. Evaluation of antibiotic prescribing practices and antimicrobial sensitivity patterns in urinary tract related infectious diseases in pediatric patients. Front Pediatr. (2021) 9:740106. doi: 10.3389/fped.2021.740106
28. Al Nafeesah A, Al Fakeeh K, Chishti S, Hameed T. E. coli versus non-E. coli urinary tract infections in children: a study from a large tertiary care center in Saudi Arabia. Int J Pediatr Adolesc Med. (2022) 9:46–8. doi: 10.1016/j.ijpam.2021.05.002
29. Alrasheedy M, Abousada HJ, Abdulhaq MM, Alsayed RA, Alghamdi KA, Alghamdi FD, et al. Prevalence of urinary tract infection in children in the kingdom of Saudi Arabia. Arch Ital Urol Androl. (2021) 93:206–10. doi: 10.4081/aiua.2021.2.206
30. Alzahrani MA, Sadoma HHM, Mathew S, Alghamdi S, Malik JA, Anwar S. Retrospective analysis of antimicrobial susceptibility of uropathogens isolated from pediatric patients in tertiary hospital at Al-Baha region, Saudi Arabia. Healthcare (Basel). (2021) 9:1564. doi: 10.3390/healthcare9111564
31. Edun TR, Aldibasi O, Jamil SF. Urinary tract infection in children with bronchiolitis: is it worth testing everyone? Cureus. (2021) 13:e15485. doi: 10.7759/cureus.15485
32. El-Naggari M, Al-Mulaabed S, Rabah F, Idrees AB, Al Muharrmi Z, El Nour I. Urinary tract infection in omani children: etiology and antimicrobial resistance. A comparison between first episode and recurrent infection. J Adv Microbiol. (2021) 21:51–62. doi: 10.9734/jamb/2021/v21i130319
33. Saeed NK, Al Khawaja S, Al-Biltagi M. Antimicrobial susceptibilities of urinary extended-spectrum β-lactamase Escherichia coli to randomized. Oman Med J. (2021) 36:e314. doi: 10.5001/omj.2021.95
34. Shaaban OA, Mahmoud NA, Zeidan AA, Kumar N, Finan AC. Prevalence and resistance patterns of pediatric urinary tract infections in Bahrain. Cureus. (2021) 13(12):e20859. doi: 10.7759/cureus.20859
35. Safdar OY, Shalaby MA, Toffaha WM, Turki AA, Toffaha WM, Ghunaim AH. Neutrophil gelatinase-associated lipocalin as an early marker for the diagnosis of urinary tract infections in Saudi children. J Nephrol Ther. (2015) 5:1–4. doi: 10.4172/2161-0959.1000221
36. Eltai NO, Al Thani AA, Al-Ansari K, Deshmukh AS, Wehedy E, Al-Hadidi S, et al. Molecular characterization of extended spectrum β-lactamases Enterobacteriaceae causing lower urinary tract infection among pediatric population. Antimicrob Resist Infect Control. (2018) 7:90. doi: 10.1186/s13756-018-0381-6
37. Ahmad S, Alotaibi HA, Alkhaibari SH, Alshahrani BM. Enterococcal urinary tract infection in newborns at a pediatric hospital in Saudi Arabia. Dhaka Univ J Pharmaceut Sci. (2020) 19:119–24. doi: 10.3329/dujps.v19i2.50626
38. Al Mana H, Sundararaju S, Tsui CK, Pérez-López A, Yassine H, Al Thani A, et al. Whole-genome sequencing for molecular characterization of carbapenem-resistant Enterobacteriaceae causing lower urinary tract infection among pediatric patients. Antibiotics (Basel). (2021) 10:972. doi: 10.3390/antibiotics10080972
39. Albarrak M, Alzomor O, Almaghrabi R, Alsubaie S, Alghamdi F, Bajouda A, et al. Diagnosis and management of community-acquired urinary tract infection in infants and children: clinical guidelines endorsed by the Saudi pediatric infectious diseases society (SPIDS). Int J Pediatr Adolesc Med. (2021) 8:57–67. doi: 10.1016/j.ijpam.2021.03.001
40. Subcommittee on Urinary Tract Infection. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2–24 months of age. Pediatrics. (2016) 138:e20163026. doi: 10.1542/peds.2016-3026
41. Singh-Grewal D, Macdessi J, Craig J. Circumcision for the prevention of urinary tract infection in boys: a systematic review of randomized trials and observational studies. Arch Dis Child. (2005) 90:853–8. doi: 10.1136/adc.2004.049353
42. Pérez-López A, Sundararaju S, Al-Mana H, Tsui KM, Hasan MR, Suleiman M, et al. Molecular characterization of extended-spectrum β-lactamase–producing Escherichia coli and Klebsiella pneumoniae among the pediatric population in Qatar. Front Microbiol. (2020) 11:581711. doi: 10.3389/fmicb.2020.581711
43. Ministry of Public Health Qatar. National clinical guideline: the diagnosis and management of urinary tract infections in children (2019). Available at: https://www.moph.gov.qa/_layouts/download.aspx?SourceUrl=/Admin/Lists/ClinicalGuidelinesAttachments/Attachments/67/The%20Diagnosis%20and%20Management%20of%20Urinary%20Tract%20Infections%20in%20Children.pdf (Accessed April 20, 2022).
44. Yang SS, Tsai JD, Kanematsu A, Han CH. Asian guidelines for urinary tract infection in children. J Infect Chemother. (2021) 27:1543–54. doi: 10.1016/j.jiac.2021.07.014
45. Dasgupta-Tsinikas S, Zangwill KM, Nielsen K, Lee R, Friedlander S, Donovan SM, et al. Treatment and epidemiology of third-generation cephalosporin-resistant urinary tract infections. Pediatrics. (2022) 150:e2021051468. doi: 10.1542/peds.2021-051468
46. Wang ME, Lee V, Greenhow TL, Beck J, Bendel-Stenzel M, Hames N, et al. Clinical response to discordant therapy in third-generation cephalosporin-resistant UTIs. Pediatrics. (2020) 145:e20191608. doi: 10.1542/peds.2019-1608
47. Vazouras K, Hsia Y, Folgori L, Bielicki J, Aguadisch E, Bamford A, et al. Treatment and outcomes of children with febrile urinary tract infection due to extended spectrum beta-lactamase-producing bacteria in Europe: TOO CUTE study. Pediatr Infect Dis J. (2020) 39:1081–7. doi: 10.1097/INF.0000000000002838
48. Lob SH, Nicolle LE, Hoban DJ, Kazmierczak KM, Badal RE, Sahm DF. Susceptibility patterns and ESBL rates of Escherichia coli from urinary tract infections in Canada and the United States, SMART 2010−2014. Diagn Microbiol Infect Dis. (2016) 85:459–65. doi: 10.1016/j.diagmicrobio.2016.04.022
49. Madhi F, Jung C, Timsit S, Levy C, Biscardi S, Lorrot M, et al. Febrile urinary-tract infection due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in children: a French prospective multicenter study. PLoS One. (2018) 13:e0190910. doi: 10.1371/journal.pone.0190910
50. Demir M, Kazanasmaz H. Uropathogens and antibiotic resistance in the community and hospital-induced urinary tract infected children. J Glob Antimicrob Resist. (2020) 20:68–73. doi: 10.1016/j.jgar.2019.07.019
51. Mana HA, Sundararaju S, Eltai NO, Al-Hadidi SH, Hasan MR, Tang P, et al. Low-level amikacin resistance induced by AAC(6′)-ib and AAC(6′)-ib-cr in extended-spectrum β-lactamase (ESBL)-producing enterobacterales isolated from urine in children. J Glob Antimicrob Resist. (2021) 26:42–4. doi: 10.1016/j.jgar.2021.04.026
52. Bassetti M, Peghin M, Mesini A, Castagnola E. Optimal management of complicated infections in the pediatric patient: the role and utility of ceftazidime/avibactam. Infect Drug Resist. (2020) 13:1763–73. doi: 10.2147/IDR.S209264
53. Aguilera-Alonso D, Escosa-García L, Saavedra-Lozano J, Cercenado E, Baquero-Artigao F. Carbapenem-resistant gram-negative bacterial infections in children. Antimicrob Agents Chemother. (2020) 64:e02183–19. doi: 10.1128/AAC.02183-19
Keywords: urinary tract infection, pediatric, Gulf Cooperation Council (GCC), antimicrobial susceptibility, antimicrobial resistance
Citation: Albarrak M, Al Dabbagh M, Al Hashami H, Alzomor O, Ghatasheh G, Habashy N, Hassanien A and Pérez-López A (2023) Urinary tract infections in children from the Gulf Cooperation Council countries: a literature review (2011–2022). Front. Pediatr. 11:1163103. doi: 10.3389/fped.2023.1163103
Received: 10 February 2023; Accepted: 22 June 2023;
Published: 17 July 2023.
Edited by:
Nopporn Apiwattanakul, Mahidol University, ThailandReviewed by:
Elisabeth Adderson, St. Jude Children’s Research Hospital, United States© 2023 Albarrak, Al Dabbagh, Al Hashami, Alzomor, Ghatasheh, Habashy, Hassanien and Pérez-López. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrés Pérez-López YXBlcmV6bG9wZXpAc2lkcmEub3Jn
Abbreviations 3GC, third-generation cephalosporin; CA, community-acquired; CA-UTI, community-acquired urinary tract infection; CFU, colony forming units; CRE, carbapenem-resistant Enterobacterales; ESBL, extended-spectrum β-lactamase; HA, hospital-acquired; HA-UTI, hospital-acquired UTI; IV, intravenous; MCUG, micturating cystourethrogram; SPIDS, Saudi Pediatric Infectious Diseases Society; UAE, United Arab Emirates; UTI, urinary tract infection; VCUG, voiding cystourethrogram; VUR, vesicoureteral reflux.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.