 Mark Belletrutti
Mark Belletrutti Mihir Bhatt2
Mihir Bhatt2- 1BC Children’s Hospital, Oncology/Hematology/BMT, University of British Columbia, Vancouver, BC, Canada
- 2McMaster Children’s Hospital, Hematology/Oncology, McMaster University, Hamilton, ON, Canada
The introduction of emicizumab into the treatment regime of persons with hemophilia A has dramatically reduced frequency of bleeding in patients with and without inhibitors. However, in children with Hemophilia A (CwHA) who require surgical or other invasive procedures, additional treatment with factor replacement or other hemostatic agents may still be needed to prevent intraoperative or postoperative bleeding. This review will look at the reported outcomes in CwHA on emicizumab who have had surgery and propose recommendations for the best perioperative management of major and minor procedures.
Introduction
Hemophilia A is a congenital deficiency of clotting factor VIII (FVIII) due to the presence of mutations on the FVIII gene. It is an X-linked disorder primarily affecting males and results in a lifelong bleeding tendency. Frequent, seemingly unprovoked bleeding into joints and muscles as well as potentially life-threatening bleeding into vital areas (such as the central nervous system) can lead to significant long-term complications (1). The mainstay of treatment is FVIII replacement using purified factor concentrates. In many areas of the world, prophylactic FVIII replacement to prevent bleeding is the standard of care, especially in children (2, 3). While effective at preventing most bleeding episodes, FVIII prophylaxis comes with considerable challenges in the pediatric population, including development of inhibitors as well as need for venous access, which often requires surgically implanted catheters to support the frequency of regular prophylactic intravenous infusions (4).
In up to 30% of previously untreated children, the development of FVIII neutralizing autoantibodies (inhibitors) renders FVIII replacement ineffective (5–7) and requires eradication of the inhibitor through immune tolerance induction treatment (8). Until eradication, episodic bleeding is treated with alternative agents that bypass the FVIII step in coagulation (BPA)(activated prothrombin complex concentrates [aPCCs], recombinant factor VIIa [rFVIIa]) (9–11) which, unfortunately, have suboptimal and unpredictable efficacy. This leads to increased bleeding episodes, increased morbidity and mortality, and decreased quality of life (12, 13).
Emicizumab (Hemlibra®, Roche, USA) is a bispecific humanized monoclonal antibody engineered to bring activated factor IX and factor X together allowing activation of factor X thus mimicking the action of missing FVIII in persons with hemophilia A (14). Restoration of FVIII function with emicizumab results in activity at 10%–20% equivalency of endogenous FVIII (15, 16) and converts an individual from a severe bleeding phenotype to a mild phenotype. Emicizumab has shown efficacy in bleed prevention in both adolescents/adults and children with Hemophilia A with and without inhibitors (17–20) and has the added benefit of subcutaneous administration, removing the need for venous access. This has led to widespread adoption of emicizumab as prophylaxis therapy in many countries (21).
Many children with Hemophilia A require surgical procedures throughout their lifetime, often because of their disease. In addition, routine procedures such as dental extraction or tonsillectomy can also lead to excessive bleeding if not managed appropriately. Coordination between the Hemophilia Treatment Center and surgical teams is essential to ensure proper treatment can be given prior to, during, and after surgery to minimize bleeding complications. This remains the standard approach in the emicizumab era as additional factor replacement or treatment with other hemostatic agents may still be needed. To date, no standard guidelines exist to guide clinicians on what the best practice is for preparing children with Hemophilia A on emicizumab for surgery. However, data on surgical outcome from the seminal clinical trials and from published real-world experience can guide clinicians on how to manage their patients. This review will appraise the data from these publications and present recommendations for laboratory testing, treatment for major and minor procedures. Additional unanswered questions will also be discussed.
Methods
A PubMed search using the terms “emicizumab AND surgery” was conducted. Relevant journal articles were selected, and reference lists reviewed for additional publications. All articles containing pediatric patients 0–18 years of age where data could be easily extracted were included. Articles with only adult patients or where pediatric data could not be easily separated or interpreted were excluded.
Major and minor surgical procedures were defined based on Santogostino et al. (22) Minor surgery was defined as an invasive procedure involving manipulation of only skin, mucous membranes, or superficial connective tissue. Major surgery was defined as an invasive procedure which included one or more of the following: entering a body cavity, crossing a mesenchymal barrier, opening a fascial plane, removing an organ, or operatively altering the normal anatomy.
Post-operative bleeding definitions were based on the HAVEN studies (23) and were defined as bleeding that occurred after surgery and felt to be “due to the surgery/procedure.” A treated bleed was defined as a bleed that was directly followed by the administration of a FVIII concentrate or rFVIIa, irrespective of the time between the treatment and preceding bleed.
Review of published data
Search of the literature revealed 1 post-hoc analysis of HAVEN 1–4 studies (23), 1 phase IV study which enrolled 11 children (14 total patients) (24), and 13 pediatric case series or case reports.
Summary of HAVEN studies 1–4
During the 4 HAVEN trials, 126 patients underwent 233 surgical procedures including 215 minor procedures (115 patients, 64 patients with inhibitors) and 18 major surgeries (18 patients, 10 patients with inhibitors). Overall, 141/215 minor procedures (65.6%) received no pre-operative FVIII or rFVIIa and 128 of these procedures (85.8%) did not require post-operative FVIII or rFVIIa. In the major surgeries, 15 patients (83.3%) received additional FVIII or rFVIIa treatment and 12 patients had no postoperative bleeding. Having an inhibitor vs. no inhibitor had no effect on rate of postoperative bleeding, nor did receipt of pre-operative FVIII or rFVIIa (23).
The two most common minor procedures were dental (62 procedures; 29 extractions, 15 endodontic procedures, 7 dental implants) and central line procedures (29 removals, 7 placements). Of the 40 procedures performed without prophylactic FVIII or rFVIIa, 13 (32.5%) were associated with post-operative bleeds, 9 (27.5%) of which were treated and 4 of which did not require factor concentrate. Prophylactic FVIII or rFVIIa was administered in 22 dental procedures; 11 (50%) of these procedures had associated post-operative bleeds, 5 (22.7%) of which were treated and 6 were untreated bleeds. Antifibrinolytic agents were given in 32 procedures either as an adjunctive or as the singular hemostatic agent. Seventeen patients received antifibrinolytic therapy as the sole hemostatic agent; 10 of these procedures were not associated with a bleed.
Of the 36 central line procedures, 35 occurred in FVIII inhibitor patients. The one patient without inhibitors did not receive prophylactic factor nor did they have postoperative bleeding. Nine procedures were managed with prophylactic FVIII or rFVIIa, 2 of which required further treatment for bleeding. The 27 procedures that did not receive prophylactic FVIII or rFVIIa had 1 treated bleed and 1 untreated bleed. Antifiribrinolytic agents were given as the only treatment in 12 central line procedures and 8/12 had no bleeding complications.
While specific pediatric data was not separately reported, data from the 88 FVIII inhibitor patients enrolled in HAVEN 2 showed that 43 had a central line and 21 underwent central line removal. In this cohort, 17 had no prophylactic rFVIIa, and 1 patient had a treated postoperative bleed. Four patients received preoperative rFVIIa and none had postoperative bleeding. Specifics on other pediatric procedures were not reported (18).
Overall, minor surgery was well-tolerated with low rates of bleeding regardless of whether prophylactic infusions were given. A similar pattern was seen in the pediatric patients in these studies although analysis was limited and not specific for this age group.
Phase IV study
A phase IV, multicentre, open-label study of emicizumab prophylaxis in persons with hemophilia A with or without FVIII inhibitors undergoing minor surgery was conducted from June 2018 to March 2020. The mean age of patients who participated in the trial was 11 (range: 5–22). Patients receiving emicizumab who were scheduled to undergo minor surgery within 60 days of enrolment and were planned to receive emicizumab for ≳1 month following surgery were eligible to participate in this study. The primary objective was to compare the percentage of participants who required FVIII or rFVIIa for surgery-related bleeding until discharge from surgery to those who did not require FVIII or rFVIIa, and to report the occurrence of bleeding and FVIII or rFVIIa use after discharge. Perioperative administration of FVIII, rFVIIa and antifibrinolytics was at the discretion of the treating physician (24).
Overall, 14 patients enrolled in this study with 13 undergoing minor surgical procedures (11 were children). Minor procedures performed in this study included CVAD removal (n = 11) and simple dental extractions (n = 2). Only 3/14 participants did not have FVIII inhibitors. rFVIIa was administered intra-operatively in three minor surgeries, although only one was for treatment of an intraoperative bleed. Post-operative bleeding occurred in three participants, two of whom received rFVIIa intraoperatively; all three patients received post-operative rFVIIa. The study was terminated early due to low enrollment and limited variety of surgical procedures.
Of the 11 patients who underwent central line removal, bleeding occurred in 2; 1 postoperative bleed and 1 intra-operative bleed. Both received intra and post-operative rFVIIa. One additional patient undergoing central line removal received rFVIIa immediately prior to surgery (and was classified as receiving intra-operative factor) and had no postoperative bleeding. The 8 other central removals did not receive preoperative or intra-operative FVIII or rFVIIa and had no postoperative bleeding. Both dental extractions had postoperative bleeding although only 1 was a treated bleed.
Early termination due to few patients undergoing minor surgeries and low enrollment numbers limited the generalizability of this study. Conclusions were difficult to draw in this small study although the results were similar to those reported in the HAVEN studies and other cohort studies. Most pediatric patients in this study tolerated central line removals without the need for preoperative or intraoperative FVIII or rFVIIa replacement. The authors still advised clinical judgment as the major deciding factor for when to give preoperative or intraoperative factor and to continue to coordinate surgical care with expert clinicians in hemophilia care.
Case series and reports
Thirteen publications reported surgical approaches and outcomes in CwHA. Similar to previous publications, the most common minor surgical procedure was central line removal or insertion (82 patients, 79 removals, 3 insertions, Table 1). Post-operative bleeding was minimal and occurred at the same rate regardless of administration of prophylactic FVIII or rFVIIa or no preoperative factor. The most common bleeding complications were hematoma development and bleeding from the surgical site (25–39).

Table 1. Reports of Central Venous Access Device (CVAD) surgeries in CwHA on emicizumab.
Twenty-one additional minor surgical procedures were reported and are described in Table 2. The majority of these procedures (15/21) were performed with pre-operative FVIII or rFVIIa administration and resulted in minimal bleeding. Four of these procedures also received planned FVIII or rFVIIa post-operatively and reported no bleeding.
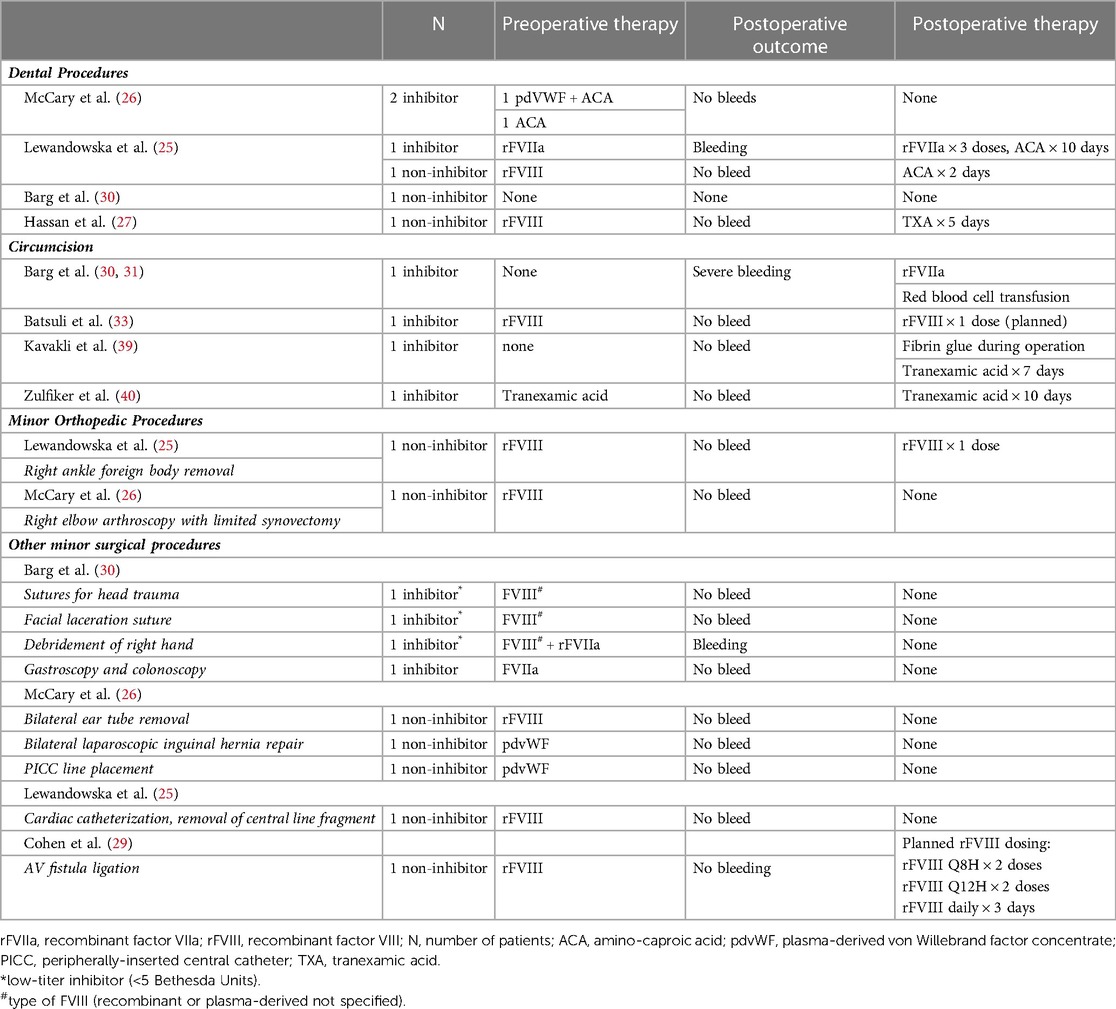
Table 2. Reports of other minor surgical procedures in CwHA on emicizumab.
Four circumcision procedures were reported and all 4 had different perioperative treatment regimens including prolonged antifibrinolytic treatment with or without fibrin glue (2 patients, no postoperative bleeding) (32), rFVIII preoperative with 1 planned dose postoperative (1 patient, no postoperative bleeding) (33), and no preoperative treatment (1 patient, major postoperative bleeding requiring rFVIIa and packed red blood cell transfusion) (31).
Five publications reported 8 major procedures (4 orthopedic procedures, 2 ventriculo-peritoneal shunt revisions, 1 cleft palate repair) and are described in Table 3. All patients who underwent major surgery received prophylactic and prolonged postoperative FVIII or rFVIIa and all reported good outcomes with no intraoperative or postoperative bleeding (25–27, 29, 30, 34).

Table 3. Reports of major surgical procedures in CwHA on emicizumab.
Discussion
Emicizumab, a bispecific monoclonal antibody which mimics the action of factor VIII has improved bleeding outcomes for patients with severe Hemophilia A. Its evolution has impacted the way providers manage patients with and without inhibitors; many have shifted away from routine use of factor VIII bypassing agents for patients with inhibitors. Data regarding surgical management and outcomes continues to evolve. The incorporation of emicizumab as prophylaxis for CwHA with or without inhibitors has represented a major shift in therapy. The experience around surgery for these children continues to evolve.
This review captured 103 minor surgeries that were reported in children on emicizumab prophylaxis. Nearly half (46.6%) of the procedures did not utilize pre-operative factor. Of the 48 surgeries that did not utilize additional hemostatic factor, 6 (12.5%) were associated with post-operative bleeds, one of which was major, requiring a red blood cell transfusion. Of the remaining 55 surgeries that utilized pre-operative factor prophylaxis, 6 (10.9%) also had post-operative bleeding.
The data demonstrates that many minor surgeries in children may be safely done with no additional factor prophylaxis or with one pre-operative factor dose. These included common minor surgeries such as dental extractions and central line removal, although the latter will likely decrease in incidence as more CwHA switch to emicizumab and no longer require regular venous access for factor prophylaxis or, in the case of inhibitor development, immune tolerance induction. Bleeding appeared to be similar between pre-treated and untreated patients. Management of post-operative bleeds varied between studies and included observation only and treatment with 1 dose of additional factor with or without adjunctive therapies such as antifibrinolytics.
Potential limitations of this review include possible publication bias such as case reports of surgery with bleeding complications being less likely to be published, and patients with a high clinical bleeding tendency not being included in surgery studies. We think these limitations are likely of low probability given that emicizumab was first used in patients with Hemophilia A with inhibitors which tend to have the highest bleeding tendency and these higher risk patients comprise the majority of the HAVEN study patients (23) and those reported in the case series (25–36).
While conclusions are limited based on available data, care needs to be taken in infants potentially owing to developmental differences in hemostasis (31), and possibly different metabolism or clearance of emicizumab. Further data should be forthcoming once the results of the ongoing HAVEN 7 study are reported (37). In this age group, until more information is known, provision of prophylactic factor and probably post-operative factor should be administered in situations where surgery is required.
For older children, what is the right approach? Should prophylactic factor be given prior to minor surgical procedures? Is it safe to not give prophylactic factor and instead observe postoperatively and give factor only if significant bleeding? Both approaches seem to be safe and without significant adverse events. These decisions require expertise from the hemophilia treatment team and close collaboration with the surgical team to create an optimal plan for each patient. The individual bleeding risk of the patient based on past bleeding pattern, FVIII inhibitor status, other medical conditions that may delay wound healing, and concomitant medical diagnoses also need to be considered when assessing risk of operative bleeding (25).
Giving prophylactic factor preoperatively could result in less factor required postoperatively, and emicizumab may provide enough FVIII equivalent levels to allow for adequate wound healing without re-bleeding. However, it will still be challenging to come up with strict guidelines as each minor surgery type may have different bleeding risks and many minor surgical procedures have minimal reported outcome data based on current publications.
The picture is clearer in major surgery and a similar approach as is done in patients with mild hemophilia should be the norm, namely a low threshold for additional factor replacement to ensure FVIII levels close to 80%–100% especially during surgery and in the immediate postoperative period. One possible advantage of emicizumab that we have observed in these situations is that additional factor administration post-operatively can likely be stopped earlier than in the past given the FVIII-equivalent levels emicizumab provides.
Identifying an appropriate perioperative hemostatic agent is important for optimizing hemostasis in patients on emicizumab undergoing major surgery especially as patients with active inhibitors should only receive rFVIIa due to the observed thrombotic complications in patients who received aPCC (17). This is a situation where laboratory monitoring (when available) to determine the presence or absence of an inhibitor in patients with a past history of inhibitors could be useful to determine appropriate factor replacement choice. Additional high-level laboratory monitoring such as thrombin generation assays may also be considered to assess bleeding and thrombosis risk, however this assay is often restricted to highly specialized centers and not widely available. Using such strategies could be considered especially for highly complex major surgeries and would require discussion, collaboration and forward planning with the Hemophilia, Laboratory Medicine, and Surgical teams. If patients have not been exposed to FVIII in a long time before surgery and they received FVIII replacement during and after surgery, testing for emergence of a new or previous inhibitor should be done to guide future factor therapy.
With the widespread adoption of emicizumab worldwide, a new cohort of CwHA who have had none or minimal factor exposure is expected to grow. This “factor naive” group will present different challenges when faced with surgery, especially when deciding on supplemental FVIII. Should the approach to surgery be similar to the decisions around factor administration in children with mild hemophilia A? One difference is that unlike mild HA patients who can sometimes use desmopressin as a way to increase their baseline FVIII level, in severe HA patients on emicizumab, additional factor administration before and possible following surgery will need to be considered if higher FVIII levels are needed for the surgical procedure.
One other major shift expected with widespread adoption of emicizumab is reduction in central line procedures as fewer patients opt for regular FVIII replacement as their prophylaxis regimen and fewer patients opt for immune tolerance induction therapy for inhibitor eradication. This likely means that there will be fewer pediatric surgery procedures overall but will also mean a shift in the type of surgical procedures seen in CwHA to more what is commonly seen in the pediatric age groups namely trauma-related surgeries, emergency procedures, otolaryngology procedures such as tonsillectomy, adenoidectomy and myringotomy tube placement, and repair of congenital malformations. More data and experience with these types of procedures will need to be collected to understand the best approaches to safely performing these surgeries with minimal to no bleeding. Likely, many of these types of surgeries would be classified as major surgery and hence require additional FVIII coverage.
Development of specific surgical guidelines is difficult given the variety of surgical procedures and their different bleeding risks. However, the following approach is suggested:
1. Close collaboration between the surgical team and hemophilia clinicians involved in the care of the child with hemophilia A.
2. Identify the bleeding risk for the specific procedure.
3. Consider if the FVIII equivalent levels provided by emicizumab are sufficient for this procedure to occur without bleeding or if additional FVIII is required to increase levels desired.
4. Consider if a dose of FVIII or rFVIIa preoperatively would greatly reduce the chance of needing multiple doses of replacement postoperatively.
5. For CwHA with inhibitors, consider rFVIIa only [given the reported serious adverse events with aPCC and emicizumab (17)] unless no inhibitor is detected prior to surgery. In this case, dosing with FVIII could be done but only under supervision of the Hemophilia care team.
6. Consider specialized laboratory testing to help guide therapy in complex major surgeries. Coordination and forward planning with surgical teams, laboratory, and the Hemophilia care team is essential in this case.
7. Be prepared and have a plan in case of bleeding.
8. Prepare parents for the possibility of a bleeding emergency after discharge with clear plans on when to present for re-evaluation.
Conclusion
The use of emicizumab as prophylaxis for CwHA has revolutionized hemophilia A care. Understanding the safest approaches to major and minor surgeries in children is important to minimize bleeding complications during and after surgery. While no specific guidelines exist for how to best manage surgeries in the pediatric population, recent publications have shown that most minor procedures can be safely completed without factor prophylaxis pre-procedure. While some procedures may necessitate the use of prophylactic factor pre-operatively, both approaches seem to result in mild or no postoperative bleeding for almost all minor procedures. Major surgeries still require ongoing factor administration postoperatively and duration of postoperative factor should continue to be guided by desired FVIII levels based on days since surgery occurred. One benefit of emicizumab is that less postoperative factor may be needed given the FVIII equivalent levels reached with emicizumab. Ongoing collaboration between the surgical teams, laboratory, and Hemophilia care team remains crucial. Further understanding of surgical outcomes for CwHA on emicizumab in trauma surgery, repair of congenital malformations and other common pediatric surgeries will need to continue. Collection of these outcomes through pre-planned national or international registries would be the best way to further this understanding.
Author contributions
MBe performed main literature search and manuscript structure. MBe, MBh and NS all equally contributed to writing of manuscript and final edits. All authors contributed to the article and approved the submitted version.
Conflict of interest
MBe: Advisory Board attendee with Roche Canada, Sanofi Canada, Bayer Canada, Octapharma Canada; invited speaker for Roche Canada, Octapharma Canada. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Srivastava A, Santagostino E, Dougall A, Kitchen S, Sutherland M, Pipe SW, et al. WFH Guidelines for the management of hemophilia, 3rd edition. Haemophilia. (2020) 26(Suppl 6):1–158. doi: 10.1111/hae.14046
2. Manco-Johnson MJ, Abshire TC, Shapiro AD, Riske B, Hacker MR, Kilcoyne R, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. (2007) 357(6):535–44. doi: 10.1056/NEJMoa067659
3. Fischer K, Collins PW, Ozelo MC, Srivastava A, Young G, Blanchette VS. When and how to start prophylaxis in boys with severe hemophilia without inhibitors: communication from the SSC of the ISTH. J Thromb Haemost. (2016) 14(5):1105–9. doi: 10.1111/jth.13298
4. Van Dijk K, Van Der Bom JG, Bax KNMA, Van Der Zee DC, Van Den Berg MH. Use of implantable venous access devices in children with severe hemophilia: benefits and burden. Haematologica. (2004) 89(2):189–94. doi: 10.3324/%25x
5. Gouw SC, van den Berg HM, Fischer K, Auerswald G, Carcao M, Chalmers E, et al. Intensity of factor VIII treatment and inhibitor development in children with severe hemophilia A: the RODIN study. Blood. (2013) 121:4046–55. doi: 10.1182/blood-2012-09-457036
6. Gouw SC, van der Bom JG, Auerswald G, Ettinghausen CE, Tedgård U, van den Berg HM. Recombinant versus plasma-derived factor VIII products and the development of inhibitors in previously untreated patients with severe hemophilia A: the CANAL cohort study. Blood. (2007) 109:4693–7. doi: 10.1182/blood-2006-11-056317
7. Calvez T, Chambost H, Claeyssens-Donadel S, d’Oiron R, Goulet V, Guillet B, et al. Recombinant factor VIII products and inhibitor development in previously untreated boys with severe hemophilia A. Blood. (2014) 124(23):3398–408. doi: 10.1182/blood-2014-07-586347
8. Hay CRM, DiMichele DM. The principal results of the international immune tolerance study: a randomized dose comparison. Blood. (2012) 119:1335–44. doi: 10.1182/blood-2011-08-369132
9. Antunes SV, Tangada S, Stasyshyn O, Mamonov V, Phillips J, Guzman-Becerra N, et al. Randomized comparison of prophylaxis and on-demand regimens with FEIBA NF in the treatment of haemophilia A and B with inhibitors. Haemophilia. (2014) 20:65–72. doi: 10.1111/hae.12246
10. Konkle BA, Ebbesen LS, Erhardtsen E, Bianco RP, Lissitchkov T, Rusen L, et al. Randomized, prospective clinical trial of recombinant factor VIIa for secondary prophylaxis in hemophilia patients with inhibitors. J Thromb Haemost. (2007) 5(9):1904–13. doi: 10.1111/j.1538-7836.2007.02663.x
11. Leissinger C, Gringeri A, Antmen B, Berntorp E, Biasoli C, Carpenter S, et al. Anti-inhibitor coagulant complex prophylaxis in hemophilia with inhibitors. N Engl J Med. (2011) 365(18):1684–92. doi: 10.1056/NEJMoa1104435
12. D’Angiolella LS, Cortesi PA, Rocino A, Coppola A, Hassan HJ, Giampaolo A, et al. The socioeconomic burden of patients affected by hemophilia with inhibitors. Eur J Haematol. (2018) 101(4):435–56. doi: 10.1111/ejh.13108
13. Walsh CE, Soucie JM, Miller CH, United States Hemophilia Treatment Center Network. Impact of inhibitors on hemophilia A mortality in the United States. Am J Hematol. (2015) 90(5):400–5. doi: 10.1002/ajh.23957
14. Kitazawa T, Igawa T, Sampei Z, Muto A, Kojima T, Soeda T, et al. A bispecific antibody to factors IXa and X restores factor VIII hemostatic activity in a hemophilia A model. Nat Med. (2012) 18:1570–4. doi: 10.1038/nm.2942
15. Donners AAMT, Rademaker CMA, Bevers LAH, Huitema ADR, Schutgens REG, Egberts TCG, et al. Pharmacokinetics and associated efficacy of emicizumab in humans: a systematic review. Clin Pharmacokinet. (2021) 60(11):1395–406. doi: 10.1007/s40262-021-01042-w
16. Kizilocak H, Marquez-Casas E, Malvar J, Carmona R, Young G. Determining the approximate factor VIII level of patients with severe haemophilia A on emicizumab using in vivo global haemostasis assays. Haemophilia. (2021) 27(5):730–5. doi: 10.1111/hae.14359
17. Oldenburg J, Mahlangu JN, Kim B, Schmitt C, Callaghan MU, Young G, et al. Emicizumab prophylaxis in hemophilia A with inhibitors. N Engl J Med. (2017) 377(9):809–18. doi: 10.1056/NEJMoa1703068
18. Young G, Liesner R, Chang T, Sidonio R, Oldenburg J, Jiménez-Yuste V, et al. A multicenter, open-label phase 3 study of emicizumab prophylaxis in children with hemophilia A with inhibitors. Blood. (2019) 134:2127–38. doi: 10.1182/blood.2019001869
19. Mahlangu J, Oldenburg J, Paz-Priel I, Negrier C, Niggli M, Mancuso ME, et al. Emicizumab prophylaxis in patients who have hemophilia A without inhibitors. N Engl J Med. (2018) 379(9):811–22. doi: 10.1056/NEJMoa1803550
20. Pipe SW, Shima M, Lehle M, Shapiro A, Chebon S, Fukutake K, et al. Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): a multicentre, open-label, non-randomised phase 3 study. Lancet Haematol. (2019) 6(6):e295–305. doi: 10.1016/S2352-3026(19)30054-7
21. Mahlangu J, Iorio A, Kenet G. Emicizumab state-of-the-art update. Haemophilia. (2022) 28(Suppl 4):103–10. doi: 10.1111/hae.14524
22. Santagostino E, Lentz SR, Misgav M, Brand B, Chowdary P, Savic A, et al. Safety and efficacy of turoctocog alfa (NovoEight ®) during surgery in patients with haemophilia A: results from the multinational guardian TM clinical trials. Haemophilia. (2015) 21:34–40. doi: 10.1111/hae.12518
23. Kruse-Jarres R, Peyvandi F, Oldenburg J, Chang T, Chebon S, Doral MY, et al. Surgical outcomes in people with hemophilia A taking emicizumab prophylaxis: experience from the HAVEN 1-4 studies. Blood Adv. (2022) 6(24):6140–50. doi: 10.1182/bloodadvances.2022007458
24. Escobar M, Dunn A, Quon D, Trzaskoma B, Lee L, Ko RH, et al. A phase IV, multicentre, open-label study of emicizumab prophylaxis in people with haemophilia A with or without FVIII inhibitors undergoing minor surgical procedures. Haemophilia. (2022) 28(4):e105–8. doi: 10.1111/hae.14574
25. Lewandowska M, Randall N, Bakeer N, Maahs J, Sagar J, Greist A, et al. Management of people with haemophilia A undergoing surgery while receiving emicizumab prophylaxis: real-world experience from a large comprehensive treatment centre in the US. Haemophilia. (2021) 27(1):90–9. doi: 10.1111/hae.14212
26. McCary I, Guelcher C, Kuhn J, Butler R, Massey G, Guerrera MF, et al. Real-world use of emicizumab in patients with haemophilia A: bleeding outcomes and surgical procedures. Haemophilia. (2020) 26(4):631–6. doi: 10.1111/hae.14005
27. Hassan E, Motwani J. Management and outcomes of paediatric patients on emicizumab prophylaxis undergoing surgical procedures: experience from a large haemophilia centre in the UK. Haemophilia. (2021) 27(5):e620–3. doi: 10.1111/hae.14358
28. Swan D, Paran S, Nolan B. Port removal in patients receiving emicizumab prophylaxis: a single centre experience and review of the literature. Haemophilia. (2022) 28(1):42–5. doi: 10.1111/hae.14459
29. Cohen CT, Diaz R. Emicizumab in pediatric hemophilia: bleeding and surgical outcomes from a single-center retrospective study. Pediatr Blood Cancer. (2021) 68(11):e29325. doi: 10.1002/pbc.29325
30. Barg AA, Livnat T, Budnik I, Avishai E, Brutman-Barazani T, Tamarin I, et al. Emicizumab treatment and monitoring in a paediatric cohort: real-world data. Br J Haematol. (2020) 191(2):282–90. doi: 10.1111/bjh.16964
31. Barg AA, Avishai E, Budnik I, Levy-Mendelovich S, Barazani TB, Kenet G, et al. Emicizumab prophylaxis among infants and toddlers with severe hemophilia A and inhibitors-a single-center cohort. Pediatr Blood Cancer. (2019) 66(11):e27886. doi: 10.1002/pbc.27886
32. Jiménez-Yuste V, Rodríguez-Merchán EC, Matsushita T, Holme PA. Concomitant use of bypassing agents with emicizumab for people with haemophilia A and inhibitors undergoing surgery. Haemophilia. (2021) 27(4):519–30. doi: 10.1111/hae.14322
33. Batsuli G, Zimowski KL, Tickle K, Meeks SL, Sidonio RF Jr. Immune tolerance induction in paediatric patients with haemophilia A and inhibitors receiving emicizumab prophylaxis. Haemophilia. (2019) 25(5):789–96. doi: 10.1111/hae.13819
34. Lefèvre CR, Jaffré A, Pontis A, Nedelec-Gac F, Guéret P, Gouin-Thibault I, et al. Management of a high-risk surgery with emicizumab and factor VIII in a child with a severe hemophilia A and inhibitor. TH Open. (2021) 5(2):e163–5. doi: 10.1055/s-0041-1728667
35. Zimowski KL, Batsuli GM, Reding MT, Rana J, Callaghan MU, Tickle K, et al. Maintaining perioperative hemostasis in patients with severe hemophilia A and inhibitors receiving emicizumab prophylaxis. Blood. (2018) 132:635–635. doi: 10.1182/blood-2018-99-115089
36. Lockhart M, Tardy-Poncet B, Montmartin A, Noyel P, Thouvenin S, Berger C. Surgery with emicizumab prophylaxis for two paediatric patients with severe haemophilia A with inhibitors. Pediatr Blood Cancer. (2021) 68(7):e29041. doi: 10.1002/pbc.29041
37. A study to evaluate the efficacy, safety, pharmacokinetics, and pharmacodynamics of subcutaneous emicizumab in participants from birth to 12 months of age with hemophilia A without inhibitors. ClinicalTrials.gov. (2023). Available at: https://clinicaltrials.gov/ct2/show/NCT04431726
38. Badle SGD, Taylor A, Sibson K, Mathias M, Liesner R. Surgical experience with emicizumab: a single centre experience with central venous access device removal. Res Pract Thromb Haemost. (2021) 4(S1):584–5. doi: 10.1002/rth2.12393
39. Kavakli K, Balkan C, Karadas N, Erdener A. Circumcision operation without using by-passing agents in patient with high responder inhibitor while he was in weekly emicizumab prophylaxis. Haemophilia. (2020) 26(S2):89. doi: 10.1111/hae.13911
Keywords: hemophilia A, emicizumab, surgery, bleeding, pediatric
Citation: Belletrutti M, Bhatt M and Samji N (2023) Management of children with hemophilia A on emicizumab who need surgery. Front. Pediatr. 11:1155853. doi: 10.3389/fped.2023.1155853
Received: 31 January 2023; Accepted: 14 March 2023;
Published: 4 April 2023.
Edited by:
Birgit Knoechel, Dana–Farber Cancer Institute, United StatesReviewed by:
Juan Carlos Núñez-Enríquez, Instituto Mexicano del Seguro Social, MexicoMartin Olivieri, LMU Munich University Hospital, Germany
© 2023 Belletrutti, Bhatt and Samji. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mark Belletrutti bWFyay5iZWxsZXRydXR0aUBjdy5iYy5jYQ==
Specialty Section: This article was submitted to Pediatric Hematology and Hematological Malignancies, a section of the journal Frontiers in Pediatrics