 Shangqin Long
Shangqin Long Liren Zhang3,†
Liren Zhang3,†- 1Department of Obstetrics and Gynecology, The First Affiliated Hospital of Dalian Medical University, Dalian, China
- 2Department of Obstetrics and Gynecology, Dalian City Third People's Hospital, Dalian, China
- 3Department of Urology, Dalian City Third People's Hospital, Dalian, China
Objectives: Positive antiphospholipid antibodies (aPLs) and chronic hypertension (CH) in pregnancy are important causes of maternal and neonatal morbidity and mortality. However, there are no relevant studies on the treatment of aPL-positive pregnant women with CH. This study aimed to determine the effect of low-dose aspirin (LDA) plus low-molecular-weight heparin (LMWH) on maternal and perinatal outcomes in persistently aPL-positive pregnant women with CH.
Methods: This study was performed at the First Affiliated Hospital of Dalian Medical University in Liaoning, China, from January 2018 to December 2021. Pregnant women diagnosed CH and persistently positive aPL who had no autoimmune disease such as systemic lupus erythematosus, antiphospholipid syndrome were recruited and divided into control group (LDA and LWMH were not used), LDA group (LDA was used) and LDA plus LMWH group (both LDA and LMWH were used) according to whether they use LDA and/or LMWH. A total of 81 patients were enrolled, including 40 patients in the control group, 19 patients in the LDA group, and 22 patients in the LDA plus LMWH group. The maternal and perinatal outcomes of LDA plus LMWH therapy were analysed.
Results: Compared with control group, the rate of severe preeclampsia in LDA group (65.00% vs. 31.58%, p = 0.016) and LDA plus LMWH group (65.00% vs. 36.36%, p = 0.030) had a statistically significant reduction. Compared with control group, the rate of fetal loss in LDA group (35.00% vs. 10.53%, p = 0.014) and LDA plus LMWH group (35.00% vs. 0.00%, p = 0.002) had a statistically significant reduction. Compared with control group, the rate of live birth in LDA group (65.00% vs. 89.74%, p = 0.048) and LDA plus LMWH group (65.00% vs. 100.00%, p = 0.002) had a statistically significant increased. Compared withcontrol group, the incidence of early-onset preeclampsia (47.50% vs. 36.84%, p = 0.008) and early-onset severe preeclampsia (47.50% vs. 13.64%, p = 0.001) in the LDA plus LMWH group decreased and were statistically different. Furthermore, we also found that LDA or LDA plus LMWH hadn't increase the rate of blood loss and placental abruption.
Conclusion: Both LDA and LDA combined with LMWH could decrease the incidence of severe preeclampsia, decrease the rate of foetal loss, increase the rate of live birth. However, LDA plus LWMH could reduce and delay the onset of severe preeclampsia, prolong the gestational age and increase the rate of full-term delivery, improve the maternal and perinatal outcomes.
1. Introduction
Hypertensive disorders are the most common medical complication of pregnancy and represent one of the major global causes of maternal and perinatal morbidity and mortality (1, 2). Recently, the principal international boards of obstetrics and gynaecology reached a consensus on the diagnostic criteria, wherein HDP is considered a group of diseases that coexist with pregnancy and elevated blood pressure, including gestational hypertension (pregnancy-induced hypertension, chronic hypertension [CH] complicating pregnancy), preeclampsia (PE; preeclampsia de novo, superimposed preeclampsia on CH) and eclampsia (3, 4). CH refers to hypertension (> 140/90 mmHg) before pregnancy or before 20 weeks of gestation and persisting>12 weeks after delivery (5). According to the existing literature, CH complicates 1% to 2% of pregnancies and constitutes the highest risk factor, among maternal characteristics and medical history, for the development of PE. A recent study showed that severe PE occurs in about 20% of women with CH, and the risk of preterm delivery is 5 to 6 times higher in women with CH superimposed with PE compared with those without PE (5).
aPLs are a group of autoantibodies against a variety of negatively charged phospholipids, including lupus anticoagulant (LA), anticardiolipin antibodies (aCL), anti-β2 glycoprotein-I antibodies (anti-β2 GPI), anti-phosphatidylserine (aPS), anti-phosphatidylinositol (API), anti-phosphatidylethanolamine (APE) etc. (6, 7), A recent study proposed the inclusion of LA, aCL and anti-β2 GPI antibodies in the laboratory diagnosis of APS (8). Most studies have shown that patients with PE have a high rate of aPL positivity than the general population (9). Among them, patients with aPL positivity have a higher risk of early-onset severe PE (9). Duckitt K et al. found that women with aPLs have an almost ten-fold increased risk of PE (10). A recent study reported that women with these antibodies are at higher risk of recurrent miscarriage, stillbirth, and other pregnancy-associated morbidities, including PE, a pregnancy disorder of maternal high blood pressure and systemic endothelial activation (11). The current guidelines recommend the use of LDA to prevent PE in pregnant women with CH in the first trimester (12). However, aPL-positive pregnant women are treated with a combination of LMWH and LDA, with a success rate of approximately 75% (13). As we all known, CH and APS are both vascular disorders and renal involvement of antiphospholipid antibodies. Malignant hypertension is a hallmark of APS-nephropathy. Several studies have elaborated the reasons why chronic hypertension is associated with aPL (14). Some studies demonstrated that circulating levels of aPL in pregnant women with CH are greater compared to normotensive women (15). In addition, some researchers have listed CH as a clinical feature associated with the presence of aPLs (16). With the improvement and standardization of technologies, aPLs are being identified in an increasing number of women with CH. However, there are no relevant studies regarding the treatment of aPL positivity and CH in pregnancy.
Moreover, there are limited studies and no clear guidelines for the prevention of complications among aPL-positive pregnant women with CH. Therefore, the present study mainly explored the effect of LDA combined with LMWH on pregnancy outcomes in aPL-positive women with CH.
2. Material and methods
2.1. Study cohort
This study included persistently aPL-positive pregnant women with CH who had no autoimmune disease such as systemic lupus erythematosus, antiphospholipid syndrome, myasthenia gravis or pernicious anaemia and delivered in the First Affiliated Hospital of Dalian Medical University in Liaoning, China, from January 2018 to December 2021. The data collection began after obtaining approval from the Ethics Committee of The First Affiliated Hospital of Dalian Medical University. Pregnant women with CH who were positive for aPLs (LA, aCL, and/or anti-β2-GPI) were included, while patients with incomplete medical records and those who were lost to follow-up were excluded from this study. If a woman had more than one pregnancy, we considered only the first index pregnancy for them. The flowchart of patient enrolment is shown in Figure 1.
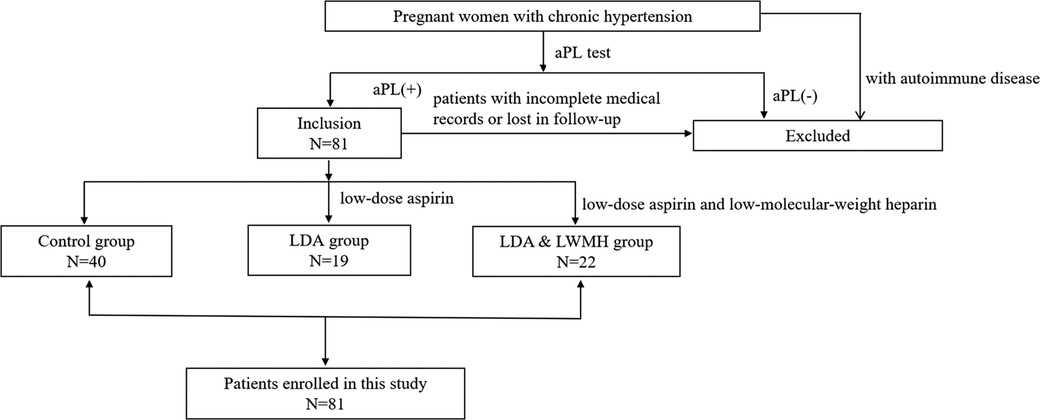
Figure 1. Patient enrolment.
2.2. Data collection
Data were collected from the medical records of the patients. Data on the general maternal characteristics (including age, BMI, blood pressure and pre-pregnancy complications, such as chronic kidney disease, diabetes mellitus, hypothyroidism etc.) were recorded to assess baseline uniformity. The primary outcomes of this study included maternal outcomes (PE, early-onset PE, severe PE, early-onset severe PE, eclampsia, thrombocytopenia, HELLP syndrome, oligoamnios, placental abruption, premature rupture of membranes, heart failure and postpartum hemorrhage, among other outcomes), and perinatal outcomes (gestational age, baby birth weight, foetal loss, prematurity, caesarean delivery and foetal growth restriction [FGR], among other outcomes). At discharge, clinical diagnosis was determined according to Table 1.
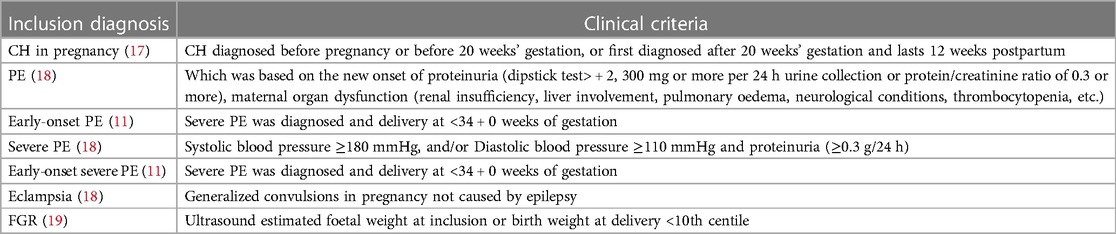
Table 1. Inclusion diagnosis and criteria at discharge.
2.3. Statistical analysis
Data were analysed using IBM SPSS Statistics® 26. The unpaired t-test was used for quantitative data to evaluate differences between two groups with normal distribution and the relation between two parameters. The x2 test was used to evaluate qualitative data. The Mann-Whitney U test was used for variables with an abnormal distribution.
3. Results
3.1. Basic clinical data
Between January 2018 and December 2021, a total of 524 pregnant women were diagnosed with chronic hypertension in our hospital, and 34 patients had autoimmune diseases, we ruled them out. A total of 490 patients were enrolled. In these 490 patients, only 184 patients were screened for aPL, the examination rate was 37.55%. In these 184 patients, 81 women were aPL positive with an interval of more than 12 weeks. the rate of aPL positive in pregnant patients with chronic hypertension was 44.02%. In these 81 patients enrolled, 19 were treated with low-dose aspirin and were included in the LDA group, 22 were treated with low-dose aspirin and low-molecular-weight heparin and were included in the LDA plus LMWH group, and 40 women who were not treated with aspirin or LMWH were allocated to the control group. The basic clinical date between the three group, including age, BMI, blood pressure stage and pre-pregnancy complications, were not significantly different (Table 2). Further, we compared the maternal and perinatal outcomes in the three groups.
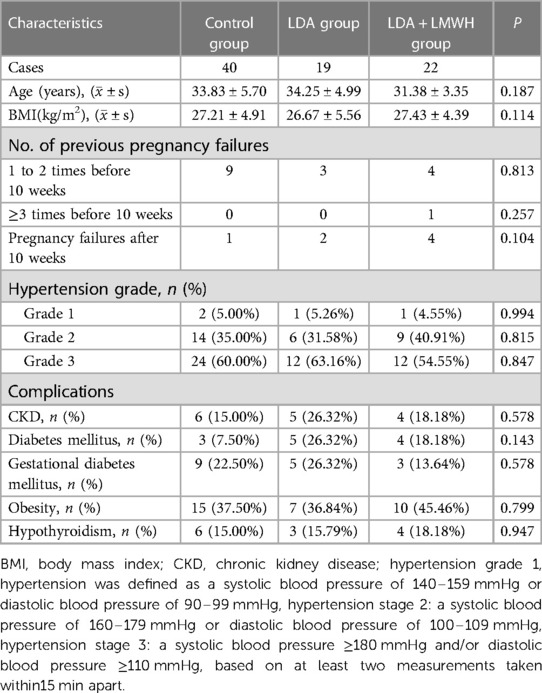
Table 2. Basic clinical data of the three groups.
3.2. Maternal and perinatal outcomes in the three groups
In this study, we found that in aPL-positive pregnant women with CH, both LDA or LDA in combination with LWMH can reduce the rate of severe preeclampsia, reduce fetal loss rates, increase live birth rates and average birth weight. Furthermore, the use of LDA combined with LMWH can reduce the incidence of early-onset preeclampsia and early-onset severe preeclampsia. The use of LDA plus LMWH can increase the gestational age and full-term delivery rates. Suggesting that in patients with aPL-positive pregnancy with chronic hypertension, LDA alone is not enough for avoiding the early-onset preeclampsia and early-onset severe preeclampsia. It is recommended that aPL should be screened in pregnant patients with chronic hypertension, once abnormal aPL results are found, LDA and LMWH should be added promptly.
In maternal outcomes, we found that compared with the control group, the rate of severe preeclampsia in LDA group (65.00% vs. 31.58%, p = 0.016) and LDA plus LMWH group (65.00% vs. 36.36%, p = 0.030) had a statistically significant reduction. However, when compared with the LDA group, there were no significant differences in the incidence of severe preeclampsia in LDA plus LMWH group. compared with the control group, the incidence of early-onset preeclampsia (47.50% vs. 36.84%, p = 0.008) and early-onset severe preeclampsia (47.50% vs. 13.64%, p = 0.001) in pregnant women in the LDA plus LMWH group decreased and were statistically different. However, when compared with the control group, the incidence of early-onset preeclampsia and early-onset severe preeclampsia in the LDA group had no statistically significant difference. Moreover, the incidence of thrombocytopenia, HELLP syndrome, oligoamnios, placental abruption, rupture of membranes, heart failure and postpartum haemorrhage were not statistically significant in LDA group and LDA plus LMWH group when compared with control group (Table 3).
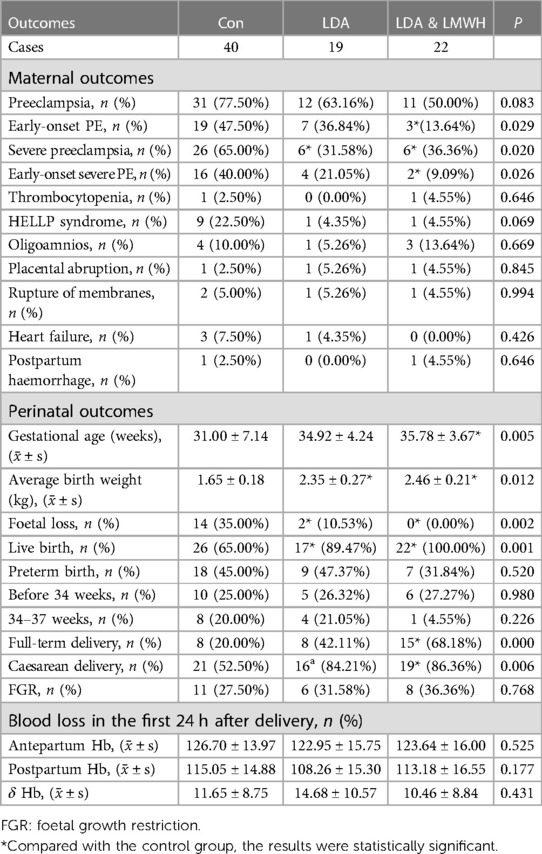
Table 3. Maternal and perinatal outcomes of patients in the three groups.
In perinatal outcomes, we found that compared with the control group, the rate of fetal loss in LDA group (35.00% vs. 10.53%, p = 0.014) and LDA plus LMWH group (35.00% vs. 0.00%, p = 0.002) had a statistically significant reduction, However, when compared with the LDA group, there were no significant differences in the incidence of the rate of fetal loss. Compared with control group, the rate of live birth in LDA group (65.00% vs. 89.74%, p = 0.048) and LDA plus LMWH group (65.00% vs. 100.00%, p = 0.002) had a statistically significant increased. Compared with control group, the average birth weight in LDA group (1.65 ± 0.18 vs. 2.35 ± 0.27, P = 0.016) and LDA plus LMWH group (1.65 ± 0.18 vs. 2.46 ± 0.21, P = 0.007) had a statistically significant increased. However, when compared with the LDA group, there were no significant differences in the rate of fetal loss and the rate of live birth. Compared with control group, the gestational age (31.00 ± 7.14 vs. 35.78 ± 3.67, P = 0.024) and the rate of full-term delivery (20.00% vs. 68.18%, p = 0.001) in pregnant women in the LDA plus LMWH group decreased and were statistically different. However, when compared with the control group, the incidence of gestational age and the rate of full-term delivery in the LDA group had no statistically significant difference. However, there were no significant differences were observed in the incidence of preterm birth, caesarean delivery and FGR between the three groups (Table 3).
Furthermore, we found that there had no significant difference in blood loss and placental abruption between the three groups.
4. Discussion
In the present study, we assessed the maternal and perinatal outcomes in 81 patients aiming to determine the effect of LDA and LDA combined with LMWH in aPL-positive pregnant women with CH. We observed that both LDA and LDA combined with LMWH could reduce the rate of foetal loss and increase the average birth weight compared to control group. Furthermore, LDA combined with LMWH could reduce the rates of early-onset PE and early-onset severe PE in aPL-positive pregnant women with CH and improve maternal and perinatal outcomes.
It is known that the presence of aPLs is associated with a hypercoagulable state, referring to an abnormally increased tendency toward blood clotting (20). Maternal aPL positivity has been associated with the development of placental insufficiency, characterised by abnormal uteroplacental vascular function, resulting in serious pregnancy complications, including PE and FGR, which are major causes of maternal and foetal mortality and morbidity (21). Aspirin can suppress the production of thromboxane, leading to an inhibition of platelet aggregation, thereby producing an antithrombotic effect due to the inactivation of cyclooxygenase (COX)-1 and COX-2 enzymes (22, 23). LMWH possesses anti-inflammatory and antithrombotic properties (24). A recent study proved that LMWH prevents metabolic and immunological disorders causing placental inflammation, thereby reducing pregnancy complications (25). Initially, LDA and LMWH were considered an effective and safe treatment of aPL- positive women (26).
In this study, we found that there had no significant differences in the rate of preeclampsia in both LDA group and LDA plus LMWH group compared with control group. Our study also observed that both LDA and LDA combined with LMWH could reduce the rate of severe preeclampsia, furthermore, the use of LDA combined with LMWH can reduce the incidence of early-onset preeclampsia and early-onset severe preeclampsia in aPL-positive pregnant women with CH, however, there had no significant differences in the rate of early-onset preeclampsia and early-onset severe preeclampsia in LDA group when compared with control group. Therefore, we concluded that LDA could reduce the incidence of severe preeclampsia to a certain extent, however, LDA plus LMWH can delay the onset of severe preeclampsia and improve the perinatal outcomes in aPL-positive pregnant women with CH. Similarly, other studies reported that LAD combined with LMWH improved maternal outcomes in pregnant women with CH (27, 28). Poon LC et al. reported that LDA did not reduce the incidence of preterm PE in women with CH (28). similarly, Lu C et al. reported that aspirin therapy alone did not demonstrate a significant statistical difference in placenta-mediated pregnancy complications compared to placebo among women with aPL positivity (27). The study by other researchers also showed that the combination of LDA and LMWH can reduce the occurrence of preeclampsia, which is similar to this study (29, 30). Nevertheless, for the first time, the present study observed that LDA combined with LMWH could reduce the rate of early-onset preeclampsia and early-onset severe preeclampsia in aPL-positive pregnant women with CH.
In this study, we observed that both LDA and LDA combined with LMWH could reduce the rate of foetal loss and increase the rate of live birth and the foetal average birth weight compared to control group. However, there was no significant difference between these perinatal outcomes with the use of LDA plus LMWH vs. aspirin monotherapy. Therefore, we concluded that LDA or LDA plus LMWH could improve the perinatal outcomes to a certain extent. Similarly, previous studies have reported that, compared with the placebo group, LDA combined with LMWH reduced the rate of miscarriage, increased neonatal weight and improved perinatal outcomes in aPL-positive pregnant women (31–33). Other studies reported that LAD combined with LMWH improved perinatal outcomes in pregnant women with CH (34). Shi T et al. conducted a study on the prevention of maternal outcomes and found that LDA combined with LMWH could reduce the rate of foetal loss and improve the live birth rate in aPL-positive pregnant women (32). On the other hand, in aPL-positive pregnant women with CH, we found that LDA combined with LMWH could reduce the rate of foetal loss, prolong the gestational age, increase the average birth weight and the rate of full-term delivery, however, LDA alone had no statistically significant effect ongestational age and foetal average birth weight. This finding is consistent with those reported in a recent systematic review (13).
Finally, this study showed that treatment with LDA or LDA combined with LMWH does not increase the risk of postpartum haemorrhage and placental abruption, similar to that reported in many previous studies (35, 36).
Although this study is the first-ever synopsis to highlight the roles of both LDA and LDA combined with LMWH in improving maternal and perinatal outcomes, certain limitations should be noted. Due to the limited sample size, more large-scale prospective studies are required to confirm the conclusions of our study. In addition, we only conducted experimental verification at the level of clinical expression. In the future, more in-depth fundamental investigations will be required to evaluate and confirm the precise mechanism of LDA and LDA combined with LMWH on aPL-positive pregnant women with CH.
5. Conclusion
We observed that both LDA and LDA combined with LMWH could decrease the incidence of severe preeclampsia, decrease the rate of foetal loss, increase the rate of live birth and increase the average birth weight. However, LDA plus LWMH could reduce and delay the onset of severe preeclampsia, prolong the gestational age and increase the rate of full-term delivery, improve the maternal and perinatal outcomes.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SL and LZ contributed to this article equally. All authors are responsible for the study design, data collection, analysis and revision of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We extend our appreciation to the patients who participated in this study. We also thank Bullet Edits Limited for the linguistic editing of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nzelu D, Dumitrascu-Biris D, Hunt KF, Cordina M, Kametas NA. Pregnancy outcomes in women with previous gestational hypertension: a cohort study to guide counselling and management. Pregnancy Hypertens. (2018) 12:12194–200. doi: 10.1016/j.preghy.2017.10.011
2. Reddy M, Fenn S, Rolnik DL, Mol BW, da Silva Costa F, Wallace EM, et al. The impact of the definition of preeclampsia on disease diagnosis and outcomes: a retrospective cohort study. Am J Obstet Gynecol. (2021) 224(2):217.e211–217.e211. doi: 10.1016/j.ajog.2020.08.019
3. Poon LC, Magee LA, Verlohren S, Shennan A, von Dadelszen P, Sheiner E, et al. A literature review and best practice advice for second and third trimester risk stratification, monitoring, and management of pre-eclampsia: compiled by the pregnancy and non-communicable diseases committee of FIGO (the international federation of gynecology and obstetrics). Int J Gynaecol Obstet. (2021) 154(Suppl 1):3–31. doi: 10.1002/ijgo.13763
4. Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, et al. Hypertensive disorders of pregnancy: iSSHP classification, diagnosis, and management recommendations for international practice. Hypertension. (2018) 72(1):24–43. doi: 10.1161/HYPERTENSIONAHA.117.10803
5. Panaitescu AM, Syngelaki A, Prodan N, Akolekar R, Nicolaides KH. Chronic hypertension and adverse pregnancy outcome: a cohort study. Ultrasound Obstet Gynecol. (2017) 50(2):228–35. doi: 10.1002/uog.17493
6. Tonello M, Bison E, Cattini MG, Pontara E, Iaccarino L, Denas G, et al. Anti-phosphatidyl-serine/prothrombin antibodies (aPS/PT) in isolated lupus anticoagulant (LA): is their presence linked to dual test positivity? Clin Chem Lab Med. (2021) 59(12):1950–3. doi: 10.1515/cclm-2021-0692
7. Fialová L, Mikulíková L, Matous-Malbohan I, Benesová O, Zwinger A. Prevalence of various antiphospholipid antibodies in pregnant women. Physiol Res. (2000) 49(3):299–305. PMID: 11043916.
8. Schreiber K, Hunt BJ. Managing antiphospholipid syndrome in pregnancy. Thromb Res. (2019) 181(Suppl 1):S41–s46. doi: 10.1016/S0049-3848(19)30366-4
9. Branch DW, Andres R, Digre KB, Rote NS, Scott JR. The association of antiphospholipid antibodies with severe preeclampsia. Obstet Gynecol. (1989) 73(4):541–5. PMID: 2494618.2494618
10. Duckitt K, Harrington D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. Br Med J. (2005) 330(7491):565. doi: 10.1136/bmj.38380.674340.E0
11. Alijotas-Reig J, Esteve-Valverde E, Anunciación-Llunell A, Marques-Soares J, Pardos-Gea J, Pathogenesis M-MF. Diagnosis and management of obstetric antiphospholipid syndrome: a comprehensive review. J Clin Med. (2022) 11(3):675. doi: 10.3390/jcm11030675
12. Tsakiridis I, Giouleka S, Arvanitaki A, Giannakoulas G, Papazisis G, Mamopoulos A, et al. Gestational hypertension and preeclampsia: an overview of national and international guidelines. Obstet Gynecol Surv. (2021) 76(10):613–33. doi: 10.1097/OGX.0000000000000942
13. Li X, Shopit A, Wang J. Biochemical and clinical predictors in pregnant women with antiphospholipid syndrome and systemic lupus erythematosus: comprehensive update. Arch Gynecol Obstet. (2021) 304(5):1153–60. doi: 10.1007/s00404-021-06178-5
14. Silver RK, Peaceman AM, Adams DM. Understanding prostaglandin metabolites and platelet-activating factor in the pathophysiology and treatment of the antiphospholipid syndrome. Clin Perinatol. (1995) 22(2):357–73. doi: 10.1016/S0095-5108(18)30288-4
15. el-Roeiy A, Myers SA, Gleicher N. The relationship between autoantibodies and intrauterine growth retardation in hypertensive disorders of pregnancy. Am J Obstet Gynecol. (1991) 164(5 Pt 1):1253–61. doi: 10.1016/0002-9378(91)90695-N
16. Branch DW, Silver RM, Blackwell JL, Reading JC, Scott JR. Outcome of treated pregnancies in women with antiphospholipid syndrome: an update of the Utah experience. Obstet Gynecol. (1992) 80(4):614–20. PMID: 1407882.1407882
17. ACOG, Alex Vidaeff M. MPH., Jimmy Espinoza M MSc., Hyagriv Simhan M, Christian M, Pettker M. ACOG Practice bulletin No. 203: chronic hypertension in pregnancy. Obstet Gynecol. (2019) 133(1):e26–50. doi: 10.1097/01.AOG.0000559202.88943.30
18. Jimmy Espinoza M MSc., Alex Vidaeff M. MPH., Christian M, Pettker M, Hyagriv Simhan M. Gestational hypertension and preeclampsia: aCOG practice bulletin, number 222. Obstet Gynecol. (2020) 135(6):e237–60. doi: 10.1097/AOG.0000000000003891
19. Tranquilli AL, Dekker G, Magee L, Roberts J, Sibai BM, Steyn W, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: a revised statement from the ISSHP. Pregnancy Hypertens. (2014) 4(2):97–104. doi: 10.1016/j.preghy.2014.02.001
20. Harris EN, Gharavi AE, Boey ML, Patel BM, Mackworth-Young CG, Loizou S, et al. Anticardiolipin antibodies: detection by radioimmunoassay and association with thrombosis in systemic lupus erythematosus. Lancet. (1983) 2(8361):1211–4. doi: 10.1016/S0140-6736(83)91267-9
21. Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN maternal mortality estimation inter-agency group. Lancet. (2016) 387(10017):462–74. doi: 10.1016/S0140-6736(15)00838-7
22. Vane JR, Botting RM. The mechanism of action of aspirin. Thromb Res. (2003) 110(5-6):255–8. doi: 10.1016/S0049-3848(03)00379-7
23. Tóth L, Muszbek L, Komáromi I. Mechanism of the irreversible inhibition of human cyclooxygenase-1 by aspirin as predicted by QM/MM calculations. J Mol Graph Model. (2013) 40:4099–109. doi: 10.1016/j.jmgm.2012.12.013
24. Litov L, Petkov P, Rangelov M, Ilieva N, Lilkova E, Todorova N, et al. Molecular mechanism of the anti-inflammatory action of heparin. Int J Mol Sci. (2021) 22(19):10730. doi: 10.3390/ijms221910730
25. Beksac MS, Tanacan A, Ozten G, Cakar AN. Low-dose low-molecular-weight heparin prophylaxis against obstetrical complications in pregnancies with metabolic and immunological disorder-associated placental inflammation. J Matern Fetal Neonatal Med. (2022) 35(8):1546–53. doi: 10.1080/14767058.2020.1760834
26. Hamulyák EN, Scheres LJ, Marijnen MC, Goddijn M, Middeldorp S. Aspirin or heparin or both for improving pregnancy outcomes in women with persistent antiphospholipid antibodies and recurrent pregnancy loss. Cochrane Database Syst Rev. (2020) 5(5):Cd012852. doi: 10.1002/14651858.CD12852.pub2
27. Lu C, Liu Y, Jiang HL. Aspirin or heparin or both in the treatment of recurrent spontaneous abortion in women with antiphospholipid antibody syndrome: a meta-analysis of randomized controlled trials. J Matern Fetal Neonatal Med. (2019) 32(8):1299–311. doi: 10.1080/14767058.2017.1404979
28. Poon LC, Wright D, Rolnik DL, Syngelaki A, Delgado JL, Tsokaki T, et al. Aspirin for evidence-based preeclampsia prevention trial: effect of aspirin in prevention of preterm preeclampsia in subgroups of women according to their characteristics and medical and obstetrical history. Am J Obstet Gynecol. (2017) 217(5):585.e581–e585. doi: 10.1016/j.ajog.2017.07.038
29. Cruz-Lemini M, Vázquez JC, Ullmo J, Llurba E. Low-molecular-weight heparin for prevention of preeclampsia and other placenta-mediated complications: a systematic review and meta-analysis. Am J Obstet Gynecol. (2022) 226(2s):S1126–S1144.e1117. doi: 10.1016/j.ajog.2020.11.006
30. Wu C, Li L, Zhang J, Song Y. Efficacy and safety of low-dose aspirin combined with low-molecular-weight heparin in treatment of preeclampsia: a meta-analysis and systematic review. Arch Med Sci. (2022) 18(6):1525–34. doi: 10.5114/aoms/136518
31. Yu X, He L. Aspirin and heparin in the treatment of recurrent spontaneous abortion associated with antiphospholipid antibody syndrome: a systematic review and meta-analysis. Exp Ther Med. (2021) 21(1):57. doi: 10.3892/etm.2020.9489
32. Shi T, Gu ZD, Diao QZ. Meta-analysis on aspirin combined with low-molecular-weight heparin for improving the live birth rate in patients with antiphospholipid syndrome and its correlation with d-dimer levels. Medicine (Baltimore). (2021) 100(25):e26264. doi: 10.1097/MD.0000000000026264
33. Baiazid L, Hraib M. Effects of low-dose aspirin and heparin on the pregnancy outcome in women with antiphospholipid syndrome. Ann Med Surg (London). (2022) 83:83104807. doi: 10.1016/j.amsu.2022.104807
34. Liu YH, Zhang YS, Chen JY, Wang ZJ, Liu YX, Li JQ, et al. Comparative effectiveness of prophylactic strategies for preeclampsia: a network meta-analysis of randomized controlled trials. Am J Obstet Gynecol. (2022) 23(22):819–25. doi: 10.1016/j.ajog.2022.10.014
35. Zhang Y, Shen F, Yang W, Wang J, Zhou J, Chen Y. Effects of low-molecular-weight heparin and aspirin in recurrent pre-eclampsia: a stratified cohort study. Int J Gynaecol Obstet. (2021) 154(2):337–42. doi: 10.1002/ijgo.13535
Keywords: chronic hypertension, low-dose aspirin, low-molecular-weight heparin, antiphospholipid antibody, pregnant women
Citation: Long S, Zhang L, Li X, He Y, Wen X, Xu N, Li X and Wang J (2023) Maternal and perinatal outcomes of low-dose aspirin plus low-molecular-weight heparin therapy on antiphospholipid antibody-positive pregnant women with chronic hypertension. Front. Pediatr. 11:1148547. doi: 10.3389/fped.2023.1148547
Received: 23 January 2023; Accepted: 11 April 2023;
Published: 5 May 2023.
Edited by:
Giada Crescioli, University of Florence, ItalyReviewed by:
Jamilya Khizroeva, I.M. Sechenov First Moscow State Medical University, RussiaAlessandra Bettiol, University of Florence, Italy
© 2023 Long, Zhang, Li, He, Wen, Xu, Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jingmin Wang d2ptMjEwMjA0QDEyNi5jb20=
†These authors have contributed equally to this work