 Qiongzhang Xia1
Qiongzhang Xia1 Tongshuai Kuang
Tongshuai Kuang Xiaokun Lin
Xiaokun Lin- 1Department of Pediatric Surgery, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, China
- 2Wenzhou Key Laboratory of Children Genitourinary Diseases, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, China
Objectives: Testicular tumors in the intra-abdominal undescended testis are rare in children, and their management remains challenging. The aim was to present a case report and review of the literature about diagnosis and treatment of testicular tumors arising from undescended intra-abdominal testis in children.
Methods: In this study, we retrospectively analyzed the clinical records of a 1-year-old male patient admitted to pediatric surgery in March 2022 with a testicular tumor originating in the intra-abdominal undescended testis. Furthermore, medical literature published in English during the last three decades was systematically searched through the databases of Medline, PubMed, and Google Scholar.
Results: The patient underwent laparoscopic orchiopexy and tumor excision. The operation was uneventful, and the patient recovered well without complications. An 8-month follow-up showed no recurrence of the teratoma after postoperative pathology. The literature search resulted in the retrieval of 16 non-duplicate articles, and 16 patients were included in this review. The cases included six cases of left cryptorchidism and 10 cases of right cryptorchidism, with an average age of 15.3 months. The largest transverse diameter of the tumors ranged from 1.8 to 12.5 cm, with an average tumor length of 6.7 cm. All patients underwent surgical treatment, including three cases of laparoscopic orchiectomy, a sole case of a conversion of inguinal incision to laparotomy and orchiectomy, and 12 cases of laparotomy and orchiectomy. Postoperative pathology revealed 12 cases of mature teratoma, two cases of immature teratoma, one case of yolk sac tumor, and a single case of embryonic carcinoma combined with yolk sac tumor. 11 patients were followed up, and one of them recurred.
Conclusion: Abdominal ultrasound (US) or abdominal computer tomography (CT) should be performed in cases of undescended testis suspected to have testicular tumors on clinical findings. The most common type of intra-abdominal testicular tumor is mature teratomas. Early diagnosis and prompt surgical intervention resulted in an excellent outcome.
Introduction
Undescended testis also called cryptorchidism, is the most common reproductive congenital anomaly in pediatric urology (1). Undescended testis is one of the few known risk factors for testicular tumor (2). The undescended testis increases the risk of testicular tumor 3.7–7.5 times (3). The relative risk to develop testicular tumor for boys who had orchidopexy before puberty ranged from 2.02–2.35, while between 5.06 and 6.24 in those who underwent orchidopexy after puberty (4). Pediatric testicular tumors are rare and represent 1%–2% of all pediatric solid tumors, with an incidence of 0.5–2.0 per 100,000 children (5). Most pre-pubertal testicular tumors are benign compared to post-pubertal tumors, which are 75% malignant (6). The relationship between undescended testis and testicular tumors remains unclear. The causes of children with undescended testicles that have tumors and the timing of tumor development remain unknown. We present a rare testicular tumor from an undescended testis treated with laparoscopic orchiopexy and excision. The patient had cryptorchidism without tumor in the preliminary stages, but a testicular tumor suddenly appeared during follow-up, a finding that has not been documented in the medical literature.
Materials and methods
Case presentation
A 1-year-old boy, born with a non-palpable undescended testis on the right side, was admitted to our hospital. Four months ago, the first ultrasound (US) examination revealed a nonpalpable undescended testis in the abdomen near the internal ring and no mass was found in the testis. The preoperative ultrasound showed that the testis was still in the abdomen near the internal ring. The US simultaneously showed a hyperechoic mass of approximately 3 mm in the testis (Figure 1A). However, a contrast-enhanced computer tomography (CT) scan showed no mass.
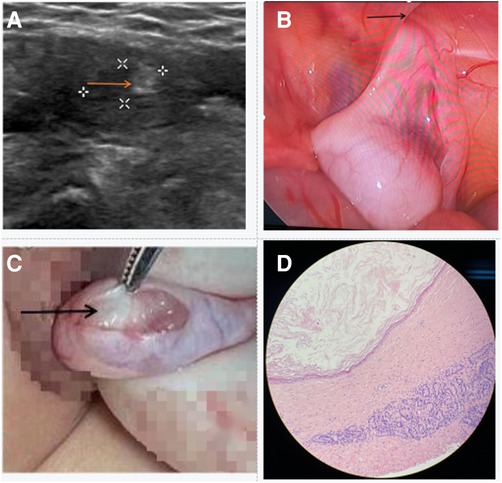
Figure 1. Perioperative data of the patient. (A) The US shows hyperechoic changes in undescended testis (see arrow). (B) The testicle was located in the abdomen, above the internal ring (see arrow). (C) The well-defined, white solid mass was seen in the testicle (see arrow). (D) The postoperative pathological examination suggested benign mature teratoma.
Furthermore, blood routines and coagulation tests were normal. Serum tumor marker analyses also showed no abnormalities: Alpha-fetoprotein (4.62 ng/ml), β- hCG (<0.1 mIU/ml). It was necessary for the child to undergo laparoscopic surgery. During the operation, we discovered that the right testicle was within a few centimeters of the internal ring but that there was no visible tumor (Figure 1B). Using a small incision in the middle of the right scrotum, the testis was pulled out through the inguinal canal. A hard mass could be palpated in the upper pole of the testis. The tunica albuginea was dissected by taking appropriate precautions and the testicular tumor were exposed (Figure 1C). We performed testis-sparing surgery. The specimen was sent for rapidly frozen histopathology, and the report suggested a mature teratoma of the testis (Figure 1D). The testis was fixed in the scrotum and the skin was sutured. The patient recovered uneventfully and was discharged on the second postoperative day. After eight months of follow-up, the patient showed no evidence of recurrence and testicular atrophy.
Literature review
Medical literature published in English during from 1990 to 01-01 to 2022-12-31 was systematically searched through the databases of Medline, PubMed, and Google Scholar. The publication type was limited to article, case report and case series. The main search terms were set as “testicular tumor”, “undescended testis”, and “non-palpable testis”. After excluding patients older than 14 years of age and those children's cases without full-text articles, a total of 16 cases were retrieved from English literatures. Clinical data were counted, including age, clinical manifestations, location, preoperative examination, tumor diameter, surgical method, pathological diagnosis, follow-up time, and recurrence. The clinical characteristics of the patients are shown in Table 1. The details are described in Table 2 (7–22). The onset time was from newborn to five years old, with an average age of 15.3 months. 87.5% of the cases were children under three years; another 12.5% were children between three and five years old. The patients underwent imaging evaluation, including US or CT or magnetic resonance imaging (MRI), during the preoperative period. A total of 13 patients underwent US examination, but only one patient didn't find the testicular tumor. There were multiple variations in the reported US morphologic properties, including a solid, cystic, or mixed mass. The cases consisted of six patients with unilateral left and 10 with unilateral right. Only 1/4 of the cases had obvious clinical symptoms, mainly abdominal pain (three cases) and abdominal mass with pain (one case), and the remaining 3/4 of the cases had no clinical symptoms before imaging examination. The largest transverse diameter of the tumors ranged from 1.8 cm to 12.5 cm, with an average tumor length of 6.7 cm. All patients underwent surgical treatment, including three cases of laparoscopic orchiectomy, a sole case of a conversion of inguinal incision to laparotomy and orchiectomy, and 12 cases of laparotomy and orchiectomy. No case was treated with testis-sparing surgery. Postoperative pathology revealed 12 cases of mature teratoma, two cases of immature teratoma, one case of yolk sac tumor, and a single case of embryonic carcinoma combined with yolk sac tumor. Both immature teratomas were grade 1. One patients relapsed 3 months later, and underwent tumor re-excising, then received chemotherapy with BEP protocol, which included bleomycin, etoposide, and cisplatin. Another patient didn't undergo additional treatment. The patient with embryonic carcinoma combined with yolk sac tumor received one cycle of chemotherapy with bleomycin, etoposide and cisplatinum. The patient with a stage III yolk sac tumor received the first cycle of JEB therapy (which included carboplatin, etoposide and bleomycin) and subsequent PEB therapy consisted of cisplatin, etoposide and bleomycin). Three-month to three-year follow-ups were conducted on 11 cases, and recurrence was noted in only one patient.
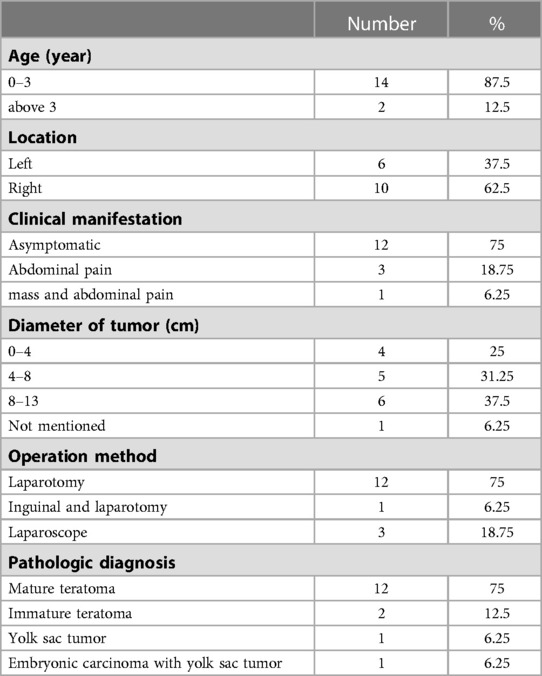
Table 1. Summary of clinical characteristics based on the literature.
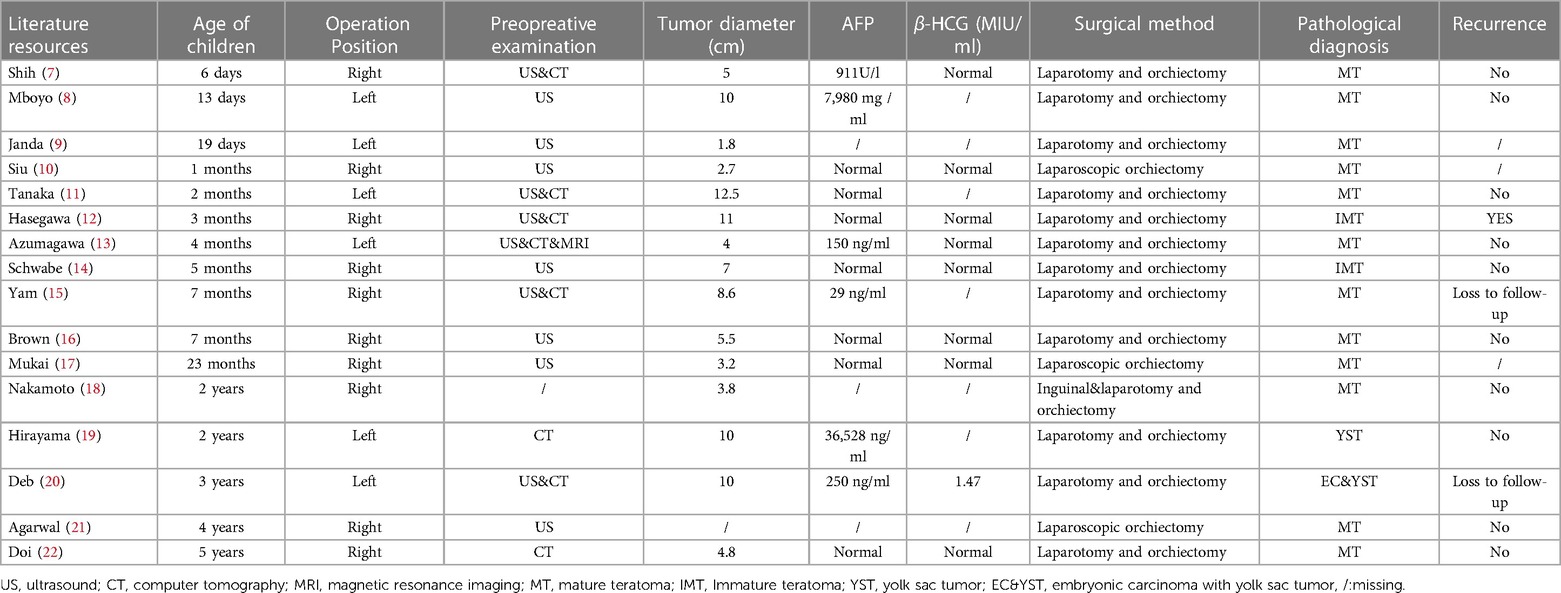
Table 2. Clinical features of 16 patients based on the literature.
Discussion
Studies have found that 20% of undescended testis were non-palpable, and 25%–40% were non-palpable intraabdominal testes (23, 24).Undescended testis had an incidence of 1%–3% in full-term male newborns and about 0.8% at one year of life. It is estimated that undescended testis cause around 10% of all testicular tumors, with the risk being higher for testicles in the abdomen (25). However, the molecular mechanism behind the development of malignancy and failed testicular descent remains unknown. Testicular tumors in children are rare in clinics, the most common of which are teratomas found in pre-pubertal children (26). However, intra-abdominal testicular tumor originating in the abdominal cavity is even rarer. Based on the literature review, non-palpable intraabdominal testis with testicular tumor are more commonly observed in children under two years old. When the intra-abdominal testicular tumor is located above the inner ring, it may prevent the testicle from descending properly into the scrotum (17).
A typical clinical presentation is absent in patients with undescended testis or testicular tumors. Most patients were hospitalized for cryptorchidism, and testicular tumors were discovered unexpectedly during the preoperative ultrasound. Clinical symptoms are less apparent when the patient is young, even asymptomatic. This may be due to the children's inability to express symptoms and the fact that symptoms are ignored, leading to late detection. Cryptorchidism with testicular tumors has only been diagnosed in a few patients due to abdominal mass or abdominal pain. Testicular tumors in the abdominal cavity are difficult to detect without imaging examination. The abdominal US is sensitive to testicular tumors, with hyperechoic changes often indicating tumors. An abdominal CT examination plays a vital role in confirming an intraperitoneal undescended testis with testicular tumor (27).
The most common use of this procedure is a follow-up examination after the tumor is discovered to clarify diagnoses and determine whether it has metastasized. However, some testicular tumors were too small to be detected on abdominal CT. In the reported case, only an undescended testis was found in the abdominal cavity at diagnosis and the abdominal US did not indicate a tumor. On abdominal CT, however, there was no sign of a testicular tumor four months later, even though the abdominal US showed a testicular tumor in the undescended testis. The preoperative diagnostic work-up includes imaging data and blood samples for tumor markers such as AFP, β-HCG, and CA-125 (28). An auxiliary examination was used to identify the type of tumor before surgery, but postoperative pathology determined the final diagnosis. Testicular tumors with undescended testis have many histologies, including benign types, such as teratomas, and some malignant types, such as yolk sac tumors and seminomas. There were 17 children in review of literature, 15 with teratomas (13 mature and two immature), one child with a yolk sac tumor, and a child with an embryonic carcinoma combined with a yolk sac tumor.
Surgical resection is critical for the treatment of patients with undescended testis and testicular tumors. A frozen-section biopsy performed during surgery may determine the best surgical procedure. The preservation of gonad function and mass resection are crucial for children whose tumors are benign. Testis-sparing surgery is applied to benign tumors and a microscopically negative resection margin (R0) must be guaranteed (29). Radical surgical excision is recommended if the tumor is malignant. However, there is still controversy concerning the use of retroperitoneal lymph node dissection (RPLND) (30). RPLND are often used in children with elevated or rising AFP levels and/or retroperitoneal lymphadenopathy (31). Following surgery, the patient received chemotherapy or radiotherapy, as necessary. The surgical approach is also determined by the size of the intraperitoneal testicular tumor. There are few reports in the literature on surgical methods, and most focus on open surgical methods. Laparotomy is recommended if the tumor size is larger than 3 cm, or the nature of the tumor cannot be determined before the operation. Based on the literature review, 12 cases (75%) performed laparotomy. Our experience suggests that laparoscopic surgery might be viable if the tumor is small, especially smaller than 1 cm. Following laparoscopic orchiopexy and tumor excision, there was no recurrence and no testicular atrophy during the follow-up period.
In conclusion, abdominal US or abdominal CT should be performed in cases of undescended testis suspected to have testicular tumors on clinical findings. The most common type of intra-abdominal testicular tumor is mature teratomas. Early diagnosis and prompt surgical intervention resulted in an excellent outcome.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
XL and HZ conceived and designed the study that led to the submission, acquired data, and played an important role in interpreting the results. QX and TK wrote the paper and perform the analysis with constructive discussions. All authors contributed to the article and approved the submitted version.
Acknowledgment
We would like to thank our colleagues from the Department of Pediatric Surgery, for their assistance
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Morgan JT, Robbins AK, Mateson AB, Sawamoto K, Tomatsu S, Gray DR, et al. Regional variation in androgen receptor expression and biomechanical properties may contribute to cryptorchidism susceptibility in the LE/orl rat. Front Endocrinol (Lausanne). (2018) 9:738. doi: 10.3389/fendo.2018.00738
2. Gurney JK, McGlynn KA, Stanley J, Merriman T, Signal V, Shaw C, et al. Risk factors for cryptorchidism. Nat Rev Urol. (2017) 14(9):534–48. doi: 10.1038/nrurol.2017.90
3. Komarowska MD, Hermanowicz A, Debek W. Putting the pieces together: cryptorchidism—do we know everything. J Pediatr Endocrinol Metab. (2015) 28(11-12):1247–56. doi: 10.1515/jpem-2015-0098
4. Echeverría Sepúlveda MP, Yankovic Barceló F, Lopez Egaña PJ. The undescended testis in children and adolescents. Part 1: pathophysiology, classification, and fertility- and cancer-related controversies. Pediatr Surg Int. (2022) 38(6):781–7. doi: 10.1007/s00383-022-05110-5
5. Hermann AL, L'Herminé-Coulomb A, Irtan S, Audry G, Cardoen L, Brisse HJ, et al. Imaging of pediatric testicular and para-testicular tumors: a pictural review. Cancers (Basel). (2022) 14(13):3180. doi: 10.3390/cancers14133180
6. Jarvis H, Cost NG, Saltzman AF. Testicular tumors in the pediatric patient. Semin Pediatr Surg. (2021) 30(4):151079. doi: 10.1016/j.sempedsurg.2021.151079
7. Shih HH, Teng RJ, Yau KI, Lin HH, Hsieh FJ, Chen CC. Mature teratoma arising from an intra-abdominal undescended testis presenting as a fetal abdominal mass. Ultrasound Obstet Gynecol. (1997) 10(3):209–11. doi: 10.1046/j.1469-0705.1997.10030209.x
8. Mboyo A, Foulet A, Hocine S, Cheve MT, Plat M, Weil D. Teratoma in an undescended testis detected prenatally. J Urol. (1997) 158(1):200–1. doi: 10.1097/00005392-199707000-00071
9. Janda GM, Najdzionek JS, Kozielski R, Greenfield SP, Williot PE. Early prenatal detection of an intra-abdominal cryptorchid testicular teratoma. Urology. (2014) 83(1):214–6. doi: 10.1016/j.urology.2013.08.013
10. Siu SS, Leung TN, Leung TY, Ng SW, Yeung CK, Lau TK. Prenatal diagnosis of intra-abdominal mature testicular teratoma. J Ultrasound Med. (2001) 20(11):1257–60. doi: 10.7863/jum.2001.20.11.1257
11. Tanaka N, Yoneda A, Fukuzawa M. Mature teratoma arising from an intraabdominal testis in a 2-month-old boy: case report and review of intraabdominal testicular tumors in children. J Pediatr Surg. (2009) 44(6):E15–8. doi: 10.1016/j.jpedsurg.2009.03.021
12. Hasegawa T, Maeda K, Kamata N, Okita Y. A case of immature teratoma originating in intra-abdominal undescended testis in a 3-month-old infant. Pediatr Surg Int. (2006) 22(6):570–2. doi: 10.1007/s00383-006-1694-8
13. Azumagawa K, Mimaki T, Tanoue H, Mino M. Mature teratoma arising from intra-abdominal contralateral undescended testis in an infant: a case report. Eur J Pediatr. (1993) 152(11):893–5. doi: 10.1007/BF01957524
14. Schwabe J, Francke A, Gerharz CD, Willnow U, Schneider DT, Nürnberger W. Immature teratoma arising from an intra-abdominal testis in a 5-month-old boy. Med Pediatr Oncol. (2000) 35(2):140–1. doi: 10.1002/1096-911X(200008)35:2%3C140::AID-MPO13%3E3.0.CO;2-S
15. Yam B, Georgiou NA, Khullar P, Coren CV, Katz DS. Radiology-Pathology conference: mature teratoma arising from an intra-abdominal undescended testis in a 7-month-old infant. Clin Imaging. (2010) 34(6):466–71. doi: 10.1016/j.clinimag.2010.03.005
16. Brown IR, Dunlap HJ, Nizalik E, Schillinger JF. A child with an intra-abdominal testicular teratoma: a case report and review of prepubertal cryptorchid germ cell tumors. Urology. (1995) 46(6):863–6. doi: 10.1016/S0090-4295(99)80359-8
17. Mukai M, Takamatsu H, Noguchi H, Tahara H. Intra-abdominal testis with mature teratoma. Pediatr Surg Int. (1998) 13(2-3):204–5. doi: 10.1007/s003830050293
18. Nakamoto T, Igawa M, Ueda M, Yasumoto H, Usui T. A case of testicular teratoma located in the opposite side of the upper abdominal wall. Int J Urol. (1994) 1(2):187–8. doi: 10.1111/j.1442-2042.1994.tb00034.x
19. Hirayama Y, Kubota M, Imamura M, Imai C, Okuyama N, Tsukada M, et al. A 2-year-old boy with a stage III yolk sac tumor occurring in an intra-abdominal retained testis. J Pediatr Surg. (2009) 44(12):2395–8. doi: 10.1016/j.jpedsurg.2009.08.024
20. Deb M, Alexander B, Das K. Embryonal carcinoma in a cryptorchid testis of a 3-year old. Pediatr Surg Int. (2010) 26(2):233–5. doi: 10.1007/s00383-009-2528-2
21. Agarwal P, Bagdi RK. Testicular tumour in non-palpable undescended testis: a rare presentation and laparoscopic management in a 4-year-old. J Minim Access Surg. (2016) 12(2):167–9. doi: 10.4103/0972-9941.178520
22. Doi O, Itoh F, Aoyama K. Mature teratoma arising in intraabdominal undescended testis in an infant with previous inguinal exploration: case report and review of intraabdominal testicular tumors in children. J Pediatr Surg. (2002) 37(8):1236–8. doi: 10.1053/jpsu.2002.34492
23. Berger C, Haid B, Becker T, Koen M, Roesch J, Oswald J. Nonpalpable testes: ultrasound and contralateral testicular hypertrophy predict the surgical access, avoiding unnecessary laparoscopy. J Pediatr Urol. (2018) 14(2):163.e1–e7. doi: 10.1016/j.jpurol.2017.10.010
24. Tsujihata M, Miyake O, Yoshimura K, Kakimoto K, Matsumiya K, Takahara S, et al. Laparoscopic diagnosis and treatment of nonpalpable testis. Int J Urol. (2001) 8(12):692–6. doi: 10.1046/j.1442-2042.2001.00397.x
25. Sembiring M, Sihombing B. Intraabdominal mass in adult men with unilateral UDT revealed as seminoma: a case report. Urol Case Rep. (2021) 39:101806. doi: 10.1016/j.eucr.2021.101806
26. Wu D, Shen N, Lin X, Chen X. Prepubertal testicular tumors in China: a 10-year experience with 67 cases. Pediatr Surg Int. (2018) 34(12):1339–43. doi: 10.1007/s00383-018-4366-6
27. Wang SQ, Ren FY, Wang JH, Ren ZH, Jin ZG, Xu Y, et al. Diagnostic value of multislice spiral computed tomography (CT) combined with CT angiography for intra-abdominal undescended testis secondary seminomas. Cancer Imaging. (2019) 19(1):24. doi: 10.1186/s40644-019-0210-z
28. Lin X, Wu D, Zheng N, Xia Q, Han Y. Gonadal germ cell tumors in children: a retrospective review of a 10-year single-center experience. Medicine. (2017) 96(26):e7386. doi: 10.1097/MD.0000000000007386
29. Stein R, Quaedackers J, Bhat NR, Dogan HS, Nijman RJM, Rawashdeh YF, et al. EAU-ESPU pediatric urology guidelines on testicular tumors in prepubertal boys. J Pediatr Urol. (2021) 17(4):529–33. doi: 10.1016/j.jpurol.2021.06.006
30. Masterson TA, Cary C, Foster RS. Current controversies on the role of lymphadenectomy for testicular cancer for the journal: urologic oncology: seminars and original investigations for the special seminars section on the role of lymphadenectomy for urologic cancers. Urol Oncol. (2021) 39(10):698–703. doi: 10.1016/j.urolonc.2018.12.021
Keywords: testicular tumor, undescended testis, cryptorchidism, teratoma, orchiopexy
Citation: Xia Q, Kuang T, Lin X and Zhang H (2023) Testicular tumor arising from an intra-abdominal undescended testis in a 1-year-old child: a case report and literature review. Front. Pediatr. 11:1142157. doi: 10.3389/fped.2023.1142157
Received: 11 January 2023; Accepted: 17 April 2023;
Published: 17 May 2023.
Edited by:
Peter Vajda, University of Pécs, HungaryReviewed by:
Sameh Shehata, Alexandria University, EgyptMarta Diana Komarowska, Medical Univeristy of Bialystok, Poland
© 2023 Xia, Kuang, Lin and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaokun Lin bGlueGsyMDAwQDE2My5jb20= Hua Zhang bWFpbHhoQDE2My5jb20=