 Empar Lurbe1,2*
Empar Lurbe1,2* Giuseppe Mancia3
Giuseppe Mancia3 Javier Calpe4
Javier Calpe4 Dorota Drożdż5
Dorota Drożdż5 Serap Erdine6
Serap Erdine6 Fernando Fernandez-Aranda1,7,8
Fernando Fernandez-Aranda1,7,8 Adamos Hadjipanayis9,10*
Adamos Hadjipanayis9,10* Peter F. Hoyer11
Peter F. Hoyer11 Augustina Jankauskiene12
Augustina Jankauskiene12 Susana Jiménez-Murcia1,7,8
Susana Jiménez-Murcia1,7,8 Mieczysław Litwin13
Mieczysław Litwin13 Artur Mazur14
Artur Mazur14 Denes Pall15,16
Denes Pall15,16 Tomas Seeman17,18
Tomas Seeman17,18 Manish D. Sinha19
Manish D. Sinha19 Giacomo Simonetti20
Giacomo Simonetti20 Stella Stabouli21
Stella Stabouli21 Elke Wühl22*
Elke Wühl22*
- 1CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Madrid, Spain
- 2Department of Pediatric, Consorcio Hospital General, University of Valencia, Valencia, Spain
- 3University of Milano-Bicocca, Milan, Italy
- 4Analog Devices, Inc., Paterna, Spain
- 5Department of Pediatric Nephrology and Hypertension, Pediatric Institute, Jagiellonian University Medical College, Kraków, Poland
- 6Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, Istanbul, Turkey
- 7University Hospital of Bellvitge-IDIBELL, Barcelona, Spain
- 8Department of Clinical Sciences, University of Barcelona, Barcelona, Spain
- 9School of Medicine, European University Cyprus, Nicosia, Cyprus
- 10Department of Paediatrics, Larnaca General Hospital, Larnaca, Cyprus
- 11Department of Pediatrics II, University Hospital Essen, Essen, Germany
- 12Pediatric Center, Institute of Clinical Medicine, Vilnius University, Vilnius, Lithuania
- 13Department of Nephrology, Kidney Transplantation and Hypertension, The Children's Memorial Health Institute, Warsaw, Poland
- 14Institute of Medical Sciences, Medical College, Rzeszów University, Rzeszow, Poland
- 15Department of Medical Clinical Pharmacology, University of Debrecen, Debrecen, Hungary
- 16Department of Medicine, University of Debrecen, Debrecen, Hungary
- 17Division of Pediatric Nephrology, University Children’s Hospital, Charles University, Prague, Czechia
- 18Department of Pediatrics, University Hospital Ostrava, Ostrava, Czechia
- 19Department of Paediatric Nephrology, Evelina London Children's Hospital, Guy's and St Thomas’ NHS Foundation Trust, London, United Kingdom
- 20Institute of Pediatrics of Southern Switzerland, Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland
- 211st Department of Pediatrics, Aristotle University of Thessaloniki, Hippokratio General Hospital of Thessaloniki, Thessaloniki, Greece
- 22Division of Pediatric Nephrology, Center for Pediatrics and Adolescent Medicine, Heidelberg University Hospital, Heidelberg, Germany
The joint statement is a synergistic action between HyperChildNET and the European Academy of Pediatrics about the diagnosis and management of hypertension in youth, based on the European Society of Hypertension Guidelines published in 2016 with the aim to improve its implementation. The first and most important requirement for the diagnosis and management of hypertension is an accurate measurement of office blood pressure that is currently recommended for screening, diagnosis, and management of high blood pressure in children and adolescents. Blood pressure levels should be screened in all children starting from the age of 3 years. In those children with risk factors for high blood pressure, it should be measured at each medical visit and may start before the age of 3 years. Twenty-four-hour ambulatory blood pressure monitoring is increasingly recognized as an important source of information as it can detect alterations in circadian and short-term blood pressure variations and identify specific phenotypes such as nocturnal hypertension or non-dipping pattern, morning blood pressure surge, white coat and masked hypertension with prognostic significance. At present, home BP measurements are generally regarded as useful and complementary to office and 24-h ambulatory blood pressure for the evaluation of the effectiveness and safety of antihypertensive treatment and furthermore remains more accessible in primary care than 24-h ambulatory blood pressure. A grading system of the clinical evidence is included.
Introduction
The joint statement is a synergistic action between HyperChildNET and the European Academy of Pediatrics about the diagnosis and management of hypertension in youth, based on the European Society of Hypertension Guidelines published in 2016 with the aim to improve its implementation. The grading system of the clinical evidence reads as follows:
A. Recommendations are based on randomized trials (or systematic reviews of trials) with high levels of internal validity and statistical precision, provided that the trial results can be directly applied to the patients because of similar clinical characteristics and outcomes have clinical relevance.
B. Recommendations are based on randomized trials, systematic reviews, or prespecified subgroup analyses that have lower levels of precision, or need to extrapolate from studies in different populations or using validated intermediate/surrogate outcomes.
C. Recommendations are based on trials that have lower levels of internal validity and/or precision, trials for which non validated surrogate outcomes were used, or results from observational studies.
D. Recommendations are based on expert opinion alone.
The first and most important requirement for the diagnosis and management of hypertension (HTN) is an accurate measurement of office blood pressure (BP), because in adults, studies on HTN as a cardiovascular risk factor and randomized trials on the beneficial effects of antihypertensive treatment have both been obtained via office BP measurements (1). However, although conventional office BP measurement represents the standard BP measurement method, in adults out-of-office BP (24-h ambulatory and home BP) has been shown to offer additional advantages, such as a more accurate identification of the BP phenotype, a more accurate prognostic value and a greater BP reproducibility (2–4). Some of these advantages have been confirmed in children, for which reason multiple measurements away from the office setting are increasingly recommended as a useful addition to office measurement in HTN guidelines for adults as well as for children (5).
Blood pressure measurements
Office blood pressure
Essential information
Office BP measurement is currently recommended for screening, diagnosis, and management of high BP in children and adolescents. In cohort studies, high office BP in childhood tracks through adulthood and associates with the presence of subclinical cardiovascular damage (6–8). BP levels should be screened in all children starting from the age of 3 years at well-child visits (Figure 1A). In case of children with risk factors for high BP, office BP should be measured at each medical visit and may start before the age of 3 years (Figure 1B) (9–12). Several studies have shown high variability and low reproducibility of office BP measurements during childhood and adolescence (13). Thus, for the diagnosis of HTN, office BP should be measured on at least 3 different occasions with intervals between visits depending on individual child's BP elevation (10–12) (Figure 1C).
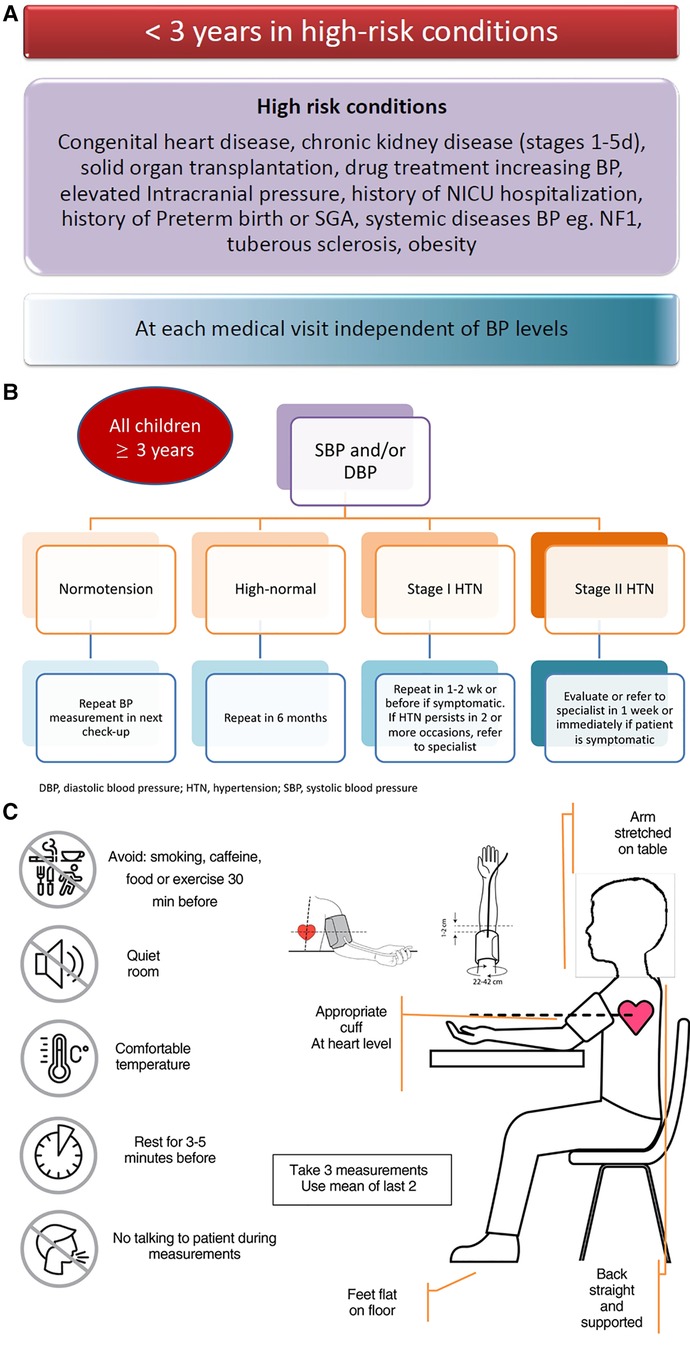
Figure 1. (A-C) Algorithm for frequency of office BP measurement and methodology.
Present challenges
Although office BP has been the basis for the management of HTN in children and adolescents some important challenges remain to be solved:
• Lack of reference values. Very limited reference data are available with oscillometric devices (14). The largest normative BP database (National High Blood Pressure Education Program or NHBPEP) is based on auscultatory measurements (15–17). Discrepancies between oscillometric BP monitors and auscultatory-based devices may occur due to observer error with auscultation or to worse performance of oscillometric devices (10). Oscillometric devices may provide significantly higher systolic BP values. Although, the overestimation of systolic BP is less when validated devices for children are used, the difference is still significant (18).
• Validated devices and appropriate cuff sizes to fit the child´s arm circumference especially for neonates and infants are limited (19, 20).
• Goals of Treatment. There are no validated office BP thresholds for treatment based on protection against cardiovascular or renal hard outcomes. In children with primary HTN the recommended office BP target for treatment is a BP < 95th percentile, although BP values < 90th percentile may be preferable because of the increasing evidence from cohort and multicenter studies that cardiovascular risk is increased at office BP levels >90th percentile (6–8, 21). The recommended BP targets in children with chronic kidney disease (CKD) are <75th percentile if there is no proteinuria and <50th percentile with proteinuria. These targets are based on extrapolation of the results of the ESCAPE trial, a multicentre randomized controlled trial that used ambulatory blood pressure monitoring (ABPM) targets to evaluate the effect of strict BP control on CKD progression (10, 22).
• Ambiguity regarding office BP interpretation and management decisions. Differences in guidelines among various societies, as well as gaps in knowledge lead to ambiguity regarding office BP interpretation and management decisions. A more protocolized approach and further insight into the reasons for variation in physicianś interpretations could help standardize practice (10–12).
• Advances in the ability to identify, evaluate, and care for neonates with HTN. Important gaps need to be addressed to improve the management of neonatal HTN. While no large studies exist, published data of BP percentiles for neonates are available (15, 23–25).
In the following materials we present advantages and limitations of office blood pressure (Table 1), methodology for office blood pressure measurement (Box 1), recommendations for high blood pressure screening at the office (Table 2), common mistakes during office blood pressure measurement (Table 3) and Interpretation of office blood pressure (Table 4).

Table 1. Advantages and limitations of office blood pressure.
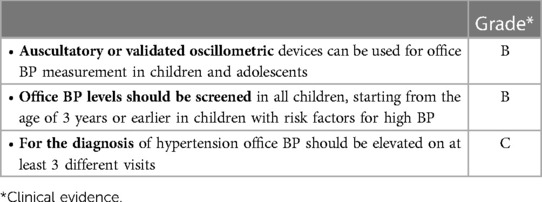
Table 2. Recommendations for high blood pressure screening at the office.
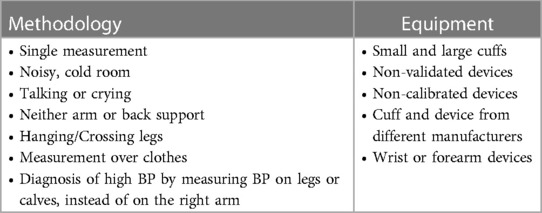
Table 3. Common mistakes during office blood pressure measurement.
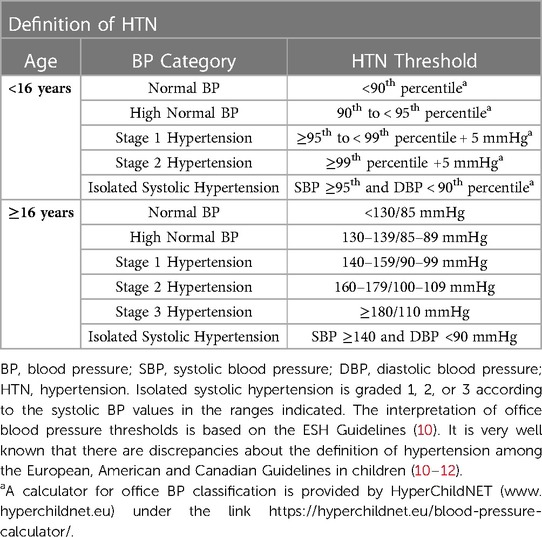
Table 4. Interpretation of office blood pressure.
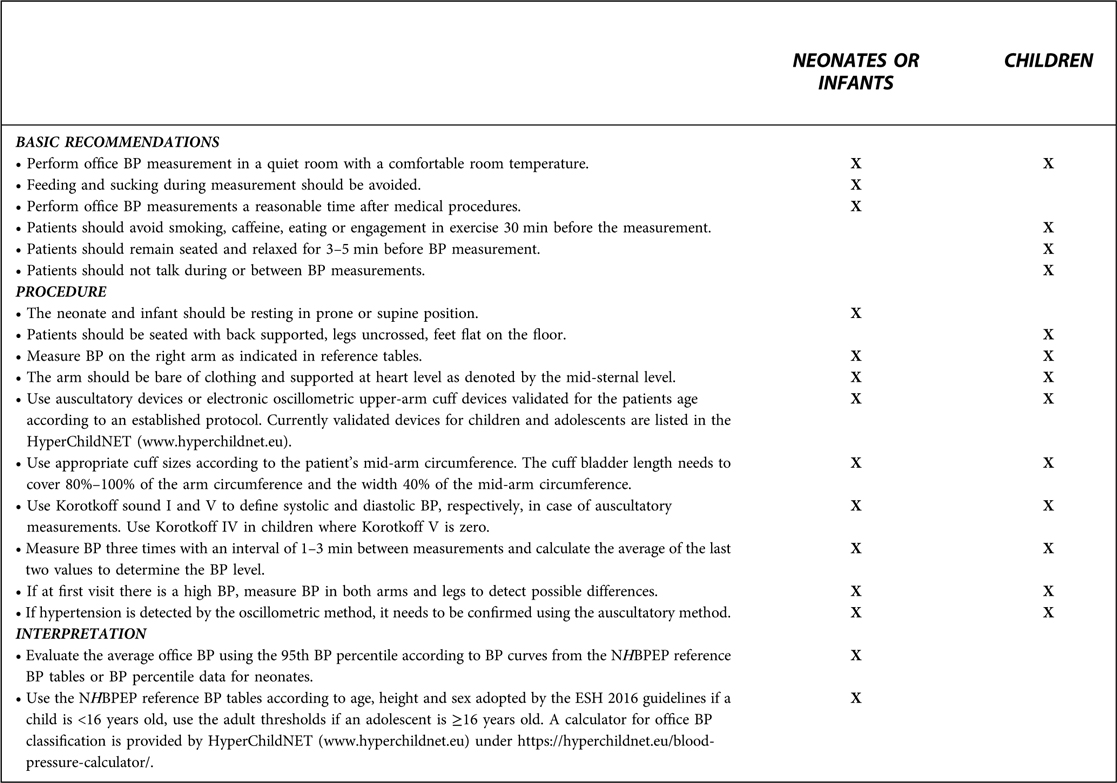
BOX 1. Methodology for office blood pressure measurement.
Out of office blood pressure
Twenty-four hour ambulatory blood pressure monitoring
Essential information
Twenty-four-hour (24-h) ABPM is increasingly recognized as an important source of information and is regarded as an established tool for the diagnosis of HTN in children and adolescents in several guidelines (10–12, 26). Reproducibility of BP measurement is of fundamental importance for an accurate identification of an individual BP level in absence and during treatment and 24-h mean BP values are indisputably more reproducible than office BP values. Limitations of office BP measurements such as within visit BP variability, the white coat effect, and the observer bias can be avoided by ABPM (10–12, 26, 27). ABPM can detect alterations in circadian and short-term BP variations and identify specific phenotypes such as nocturnal HTN or non-dipping pattern, morning BP surge, white coat and masked HTN (10–12, 26–28) with prognostic significance. In adults, ABPM shows a closer association with HTN outcomes than office BP, and the joint use of the two BP values increases the predictive ability for cardiovascular outcomes (4, 10, 11).
Present challenges
Although use of 24-h ABPM in children is now widespread, some important challenges remain to be solved:
• Lack of reference values for the non-European White Caucasian population. The most widely used data were published by Wühl and co-workers (29) as age and sex, and height and sex specific reference values from 5 years of age or 120 cm height. As for office BP, the 95th 24-h mean systolic and diastolic BP percentiles are used as HTN thresholds in children and younger adolescents. However, whether to use percentiles or fixed cut-off BP values to diagnose HTN in adolescents is a matter of debate (30, 31). Currently, the 95th percentile is used as a HTN threshold as long as the values are inferior to the accepted criteria for adults (10). This avoids the paradoxical situation in which an adolescent may meet criteria for HTN set by adult guidelines but not by paediatric guidelines. Considering the intraindividual differences between office and ABPM, it is inaccurate to derive reference values for ambulatory BP by extrapolation from office BP values (27).
• Significance and persistence of white coat hypertension (WCH) and masked hypertension (MH). The clinical relevance of WCH and MH in children and adolescents is a matter of debate because: (a) in young people studies on the relationship of these conditions with clinical outcomes are unfeasible (b) whether WCH and MH are associated with more frequent or severe HTN-mediated organ damage (HMOD) has been addressed in only few studies (32, 33) and (c) persistence of these conditions has not been well analysed in prospective studies. Additional difficulties derive from physiological changes of BP due to growth, maturation or pathological changes (34).
• Validated devices and cuff size to fit the individuaĺs arm circumference according to the device instructions (19).
• Goals of Treatment. There is an ongoing debate on which should be the BP targets for treatment in children younger than 16 years. In children with primary HTN without HMOD, achievement of BP values < 95th percentile may be acceptable and has the advantage of aligning with the cut-off for diagnosis of HTN. In the presence of HMOD or secondary HTN, BP values < 90th percentile are probably preferable. Children with CKD, without proteinuria, should be targeted to a 24-h MAP <75th while in children with CKD and proteinuria, the 24-h BP target should be <50th percentile (10, 22).
• Clinical trials. There is a strong need for clinical trials on 24-h ABPM, to facilitate the assessment of efficacy of antihypertensive treatment strategies and their impact on daily life BP, BP phenotypes and BP variability in children. In clinical practice 24-h ABPM increases the accuracy of HTN diagnosis in children and improves the power of clinical trials in pediatric HTN (10, 35).
• Ambiguity regarding 24-h ABPM interpretation and management decisions. Differences in guidelines among various societies, as well as gaps in knowledge lead to ambiguity regarding 24-h ABPM interpretation and management decisions. A more protocolized approach and further insight into the reasons for variation in physicianś interpretations could help standardise practice (10–12, 36).
In the following materials we present indications for 24-h ambulatory blood pressure monitoring (Table 5), advantages and limitations of 24-h ambulatory blood pressure monitoring vs. office blood pressure (Table 6), methodology for 24-h ambulatory blood pressure monitoring (Box 2), interpretation of 24-h ambulatory blood pressure monitoring (Table 7), blood pressure phenotypes according to office and ambulatory blood pressure monitoring (Table 8).
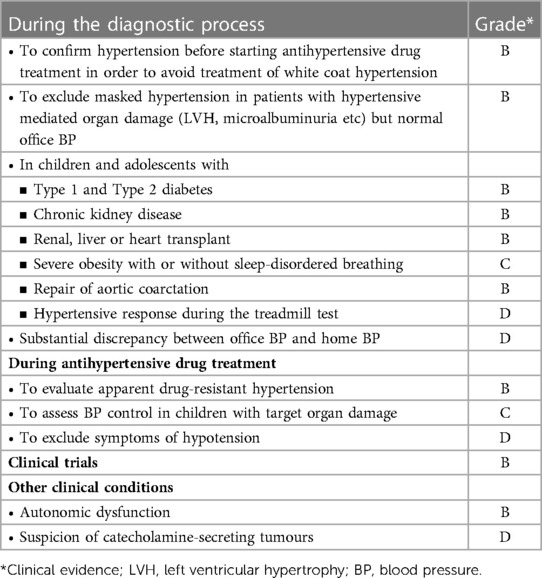
Table 5. Indications for 24-h ambulatory blood pressure monitoring.
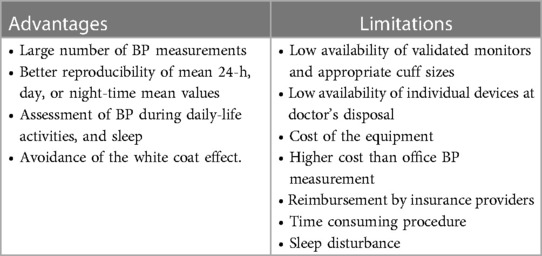
Table 6. Advantages and limitations of 24-h ambulatory blood pressure monitoring vs. office blood pressure.
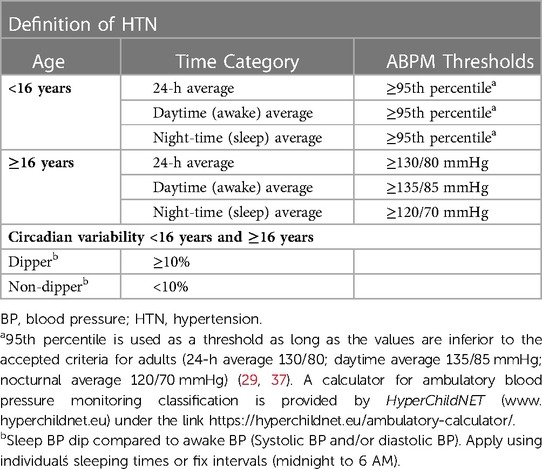
Table 7. Interpretation of 24-h ambulatory blood pressure monitoring.
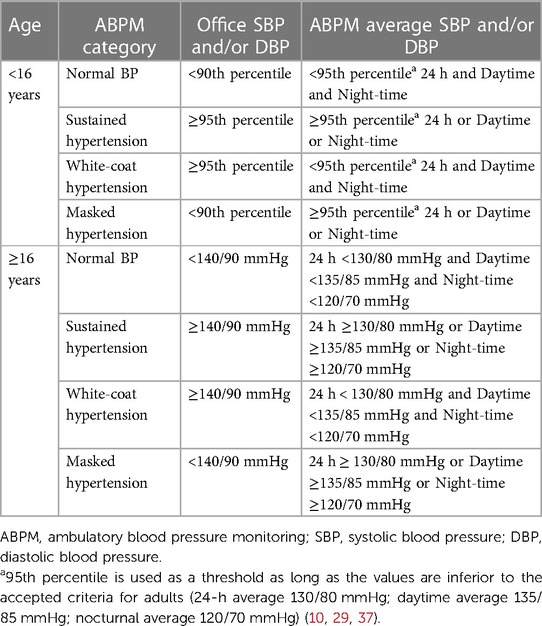
Table 8. Blood pressure phenotypes according to office and ambulatory blood pressure monitoring.
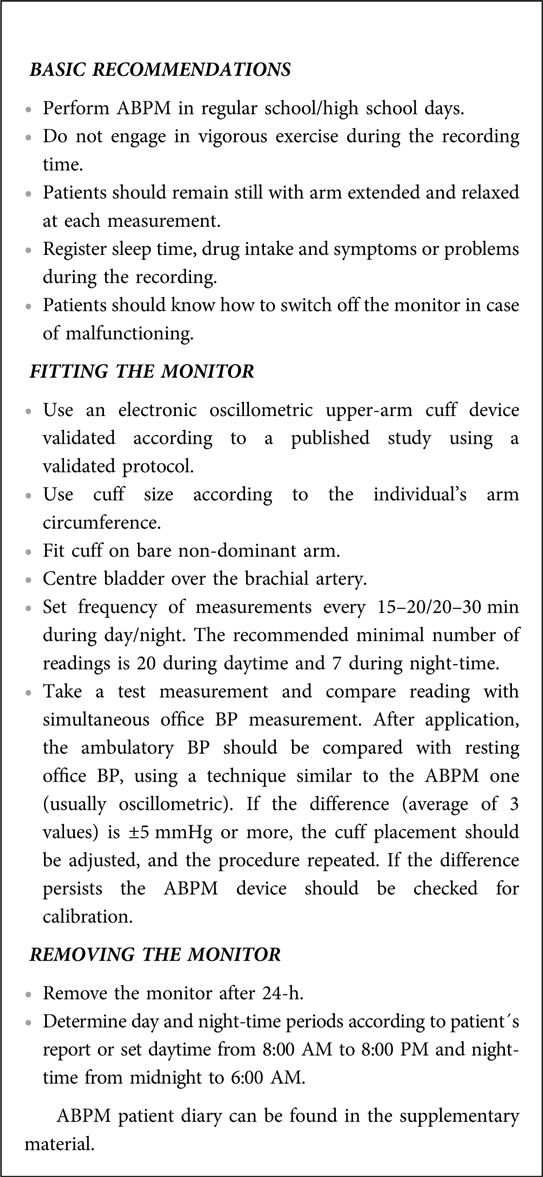
BOX 2. Methodology for 24-h ambulatory blood pressure monitoring.
Home blood pressure
Essential information
Home BP (HBP) allows multiple BP measurements away from the office setting, with the advantage of providing measurements on multiple days at rest and away from a potentially stressful environment. Like ABPM home BP values are more reproducible than the office BP values (10, 37). Based on data collected in adults, other ABPM advantages are likely to hold also for home BP. However, at present no data on Home BP advantages for the diagnosis of HTN are available in children while home BP measurements are generally regarded as useful and complementary to office and 24-h ABPM for the evaluation of the effectiveness and safety of antihypertensive treatment (10, 38). Overall, home BP will remain more accessible in primary care than ABPM.
Present challenges
Although studies have shown that in children it is feasible to obtain repeated BP measurements within the family environment, there are some challenges and uncertainties:
• Lack of reference values. The most widely used data originate from the relatively small Arsakeion School study which provides percentiles tables according to sex and a height of 120 cm and above (39).
• The relationship between HBP and preclinical hypertensive mediated organ damage is limited. Very limited evidence exists on the association of HBP with organ damage in children. Studies comparing this association with the association of HMOD with office and 24-h ABPM measurements are needed (10, 40, 41).
• The variability of HBP monitoring might induce anxiety in some children and their parents, resulting in too frequent measurements. This can be avoided by careful training (10, 37).
• Accuracy of the result BP data can be misreported or unreported by parents, relatives, or children themselves. This can be avoided by using devices with automated memory (37).
• The role of HBP in children remains controversial, mainly due to limited evidence of its clinical utility in the young population (10, 11, 38, 41). Relevant research questions on the practical application of HBPM in children should be addressed in future studies
• Telemedicine using automatic devices with data transmission may improve the role of HBP.
In the following materials we present advantages and limitations of home blood pressure (Table 9) and methodology and interpretation for home blood pressure (Box 3).

Table 9. Advantages and limitations of home blood pressure.
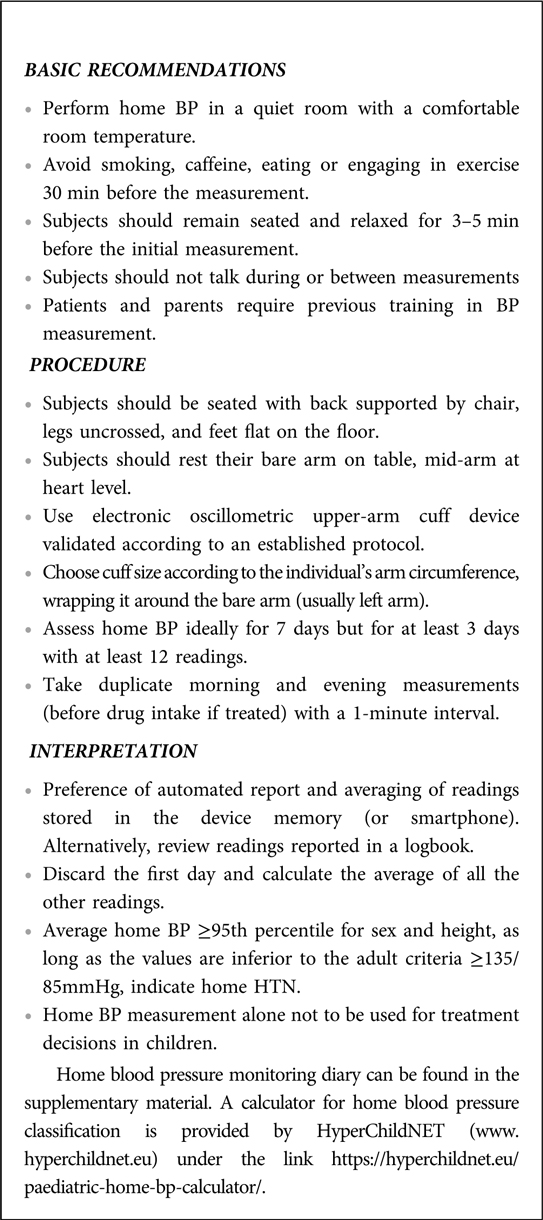
BOX 3. Methodology and interpretation for home blood pressure.
Conclusion
The first and most important requirement for the diagnosis and management of hypertension is an accurate measurement of office blood pressure. Out-of-office blood pressure measurements in youth is now widely and increasingly recognized as an important source of information. Twenty-four-hour ambulatory blood pressure is regarded as an established tool for the diagnosis of hypertension in children and adolescents with well-known recommendations. Gaps in knowledge lead to ambiguity regarding interpretation and management decisions with relevant research questions on the practical application. Action is required to be addressed in future studies.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Acknowledgments
Chapter 1 “How to correctly measure blood pressure in children and adolescents” and Chapter 2 “How to manage high blood pressure in children and adolescents” of the JOINT STATEMENT FOR ASSESSING AND MANAGING HIGH BLOOD PRESSURE IN CHILDREN AND ADOLESCENTS are based upon the work of the COST Action HyperChildNET (CA19115), with the support of COST (European Cooperation in Science and Technology).
Conflict of interest
JC was employed by Analog Devices, Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1140357/full#supplementary-material.
DATA SHEET 1
Hyperchildnet ABPM patient diary.
DATA SHEET 2
Hyperchildnet HBPM patient diary.
References
1. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 Practice guidelines for the management of arterial hypertension of the European society of hypertension and the European society of cardiology. J Hypertens. (2018) 36:2284–309. doi: 10.1097/HJH.0000000000001961
2. Redon J, Lurbe E. Ambulatory blood pressure monitoring is ready to replace clinic blood pressure in the diagnosis of hypertension: con side of the argument. Hypertension. (2014) 64:1169–74; discussion 1174. doi: 10.1161/HYPERTENSIONAHA.114.03883
3. Head GA. Ambulatory blood pressure monitoring is ready to replace clinic blood pressure in the diagnosis of hypertension: pro side of the argument. Hypertension. (2014) 64(6):1175–81; discussion 1181. doi: 10.1161/HYPERTENSIONAHA.114.03882
4. Mancia G, Facchetti R, Seravalle G, Cuspidi C, Corrao G, Grassi G. Adding home and/or ambulatory blood pressure to office blood pressure for cardiovascular risk prediction. Hypertension. (2021) 77:640–9. doi: 10.1161/HYPERTENSIONAHA.120.16303
5. Falkner B, Lurbe E. Primary hypertension beginning in childhood and risk for future cardiovascular disease. J Pediatr. (2021) 238:16–25. doi: 10.1016/j.jpeds.2021.08.008
6. Juhola J, Magnussen CG, Berenson GS, Venn A, Burns TL, Sabin MA, et al. Combined effects of child and adult elevated blood pressure on subclinical atherosclerosis: the international childhood cardiovascular cohort consortium. Circulation. (2013) 128:217–24. doi: 10.1161/CIRCULATIONAHA.113.001614
7. Yang L, Magnussen CG, Yang L, Bovet P, Xi B. Elevated blood pressure in childhood or adolescence and cardiovascular outcomes in adulthood: a systematic review. Hypertension. (2020) 75:948–55. doi: 10.1161/HYPERTENSIONAHA.119.14168
8. Urbina EM, Mendizábal B, Becker RC, Daniels SR, Falkner BE, Hamdani G, et al. Association of blood pressure level with left ventricular mass in adolescents. Hypertension. (2019) 74:590–6. doi: 10.1161/HYPERTENSIONAHA.119.13027
9. Falkner B, Lurbe E. The USPSTF call to inaction on blood pressure screening in children and adolescents. Pediatr Nephrol. (2021) 36:1327–9. doi: 10.1007/s00467-021-04926-y
10. Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A, Erdine S, Hirth A, et al. 2016 European society of hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. (2016) 34:1887–920. doi: 10.1097/HJH.0000000000001039
11. Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. (2017) 140:e20171904. doi: 10.1542/peds.2017-1904
12. Rabi DM, McBrien KA, Sapir-Pichhadze R, Nakhla M, Ahmed SB, Dumanski SM, et al. Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. (2020) 36:596–624. doi: 10.1016/j.cjca.2020.02.086
13. Sun J, Steffen LM, Ma C, Liang Y, Xi B. Definition of pediatric hypertension: are blood pressure measurements on three separate occasions necessary? Hypertens Res. (2017) 40:496–503. doi: 10.1038/hr.2016.179
14. Neuhauser HK, Thamm M, Ellert U, Hense HW, Rosario AS. Blood pressure percentiles by age and height from nonoverweight children and adolescents in Germany. Pediatrics. (2011) 127:e978–88. doi: 10.1542/peds.2010-1290
15. Report of the second task force on blood pressure control in children. Task force on blood pressure control in children. National heart, lung, and blood institute, Bethesda, Maryland. Pediatrics. (1987) 79:1–25. doi: 10.1542/peds.79.1.1
16. Update on the 1987 task force report on high blood pressure in children and adolescents: a working group report from the national high blood pressure education program. National high blood pressure education program working group on hypertension control in children and adolescents. Pediatrics. (1996) 98:649–58. doi: 10.1542/peds.98.4.649
17. National High Blood Pressure Education Program Working Group on High Blood Pressure in Clhildren and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. (2004) 114(2 Suppl 4th Report):555–76.15286277
18. Duncombe SL, Voss C, Harris KC. Oscillometric and auscultatory blood pressure measurement methods in children: a systematic review and meta-analysis. Jypertens. (2017) 35:213–24. doi: 10.1097/HJH.0000000000001178
19. Stabouli S, Chainoglu C, Evripidou K, Simao C, Antza C, Petrou P, et al. Comparison of validation protocols for blood pressure measuring devices in children and adolescents. Front Cardiovasc Med. (2022) 9:1001878. doi: 10.3389/fcvm.2022.1001878
20. Dionne JM, Bremner SA, Baygani SK, Batton B, Ergenekon E, Bhatt-Mehta V, et al. Method of blood pressure measurement in neonates and infants: a systematic review and analysis. J Pediatr. (2020) 221:23–31.e5. doi: 10.1016/j.jpeds.2020.02.072
21. Price JJ, Urbina EM, Carlin K, Becker R, Daniels SR, Falkner BE, et al. Cardiovascular risk factors and target organ damage in adolescents: the SHIP AHOY study. Pediatrics. (2022) 149:e2021054201. doi: 10.1542/peds.2021-054201
22. ESCAPE Trial Group; Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, Zurowska A, et al. Strict blood-pressure control and progression of renal failure in children. N Engl J Med. (2009) 361:1639–50. doi: 10.1056/NEJMoa0902066
23. Dionne JM, Abitbol CL, Flynn JT. Hypertension in infancy: diagnosis, management and outcome. Pediatr Nephrol. (2012) 27:17–32. Erratum in: Pediatr Nephrol. 2012;27:159-60. doi: 10.1007/s00467-010-1755-z
24. Park MK, Menard SM. Normative oscillometric blood pressure values in the first 5 years in an office setting. Am J Dis Child. (1989) 143:860–4. doi: 10.1001/archpedi.1989.02150190110034
25. Starr MC, Flynn JT. Neonatal hypertension: cases, causes, and clinical approach. Pediatr Nephrol. (2019) 34:787–99. Erratum in: Pediatr Nephrol. 2019;34:1637. doi: 10.1007/s00467-018-3977-4
26. Flynn JT, Urbina EM, Brady TM, Baker-Smith C, Daniels SR, Hayman LL, et al. Ambulatory blood pressure monitoring in children and adolescents: 2022 update: a scientific statement from the American heart association. Hypertension. (2022) 79:e114–24. doi: 10.1161/HYP.0000000000000215
27. Lurbe E, Redon J, Alvarez J, Grau-Pérez M, Martinez F, Mancia G. Insights from matched office and ambulatory blood pressure in youth: clinical relevance. Hypertension. (2022) 79:1237–46. doi: 10.1161/HYPERTENSIONAHA.122.18993
28. Lurbe E, Redon J, Kesani A, Pascual JM, Tacons J, Alvarez V, et al. Increase in nocturnal blood pressure and progression to microalbuminuria in type 1 diabetes. N Engl J Med. (2002) 347:797–805. doi: 10.1056/NEJMoa013410
29. Wühl E, Witte K, Soergel M, Mehls O, Schaefer F, German Working Group on Pediatric Hypertension. Distribution of 24-h ambulatory blood pressure in children: normalized reference values and role of body dimensions. J Hypertens. (2002) 20:1995–2007. doi: 10.1097/00004872-200210000-00019
30. Merchant K, Shah PP, Singer P, Castellanos L, Sethna CB. Comparison of pediatric and adult ambulatory blood pressure monitoring criteria for the diagnosis of hypertension and detection of left ventricular hypertrophy in adolescents. J Pediatr. (2021) 230:161–6. doi: 10.1016/j.jpeds.2020.11.003
31. Campbell JF, Shah S, Srivaths P, Acosta AA. Reclassification of adolescent hypertension by ambulatory blood pressure monitoring using adult norms and association with left ventricular hypertrophy. J Clin Hypertens. (2021) 23:265–71. doi: 10.1111/jch.14156
32. Stabouli S, Kotsis V, Toumanidis S, Papamichael C, Constantopoulos A, Zakopoulos N. White-coat and masked hypertension in children: association with target-organ damage. Pediatr Nephrol. (2005) 20:1151–5. doi: 10.1007/s00467-005-1979-5
33. Lurbe E, Torro I, Alvarez V, Nawrot T, Paya R, Redon J, et al. Prevalence, persistence, and clinical significance of masked hypertension in youth. Hypertension. (2005) 45:493–8. doi: 10.1161/01.HYP.0000160320.39303.ab
34. Lurbe E, Thijs L, Torro MI, Alvarez J, Staessen JA, Redon J. Sexual dimorphism in the transition from masked to sustained hypertension in healthy youths. Hypertension. (2013) 62:410–4. doi: 10.1161/HYPERTENSIONAHA.113.01549
35. Gimpel C, Wühl E, Arbeiter K, Drozdz D, Trivelli A, Charbit M, et al. Superior consistency of ambulatory blood pressure monitoring in children: implications for clinical trials. J Hypertens. (2009) 27:1568–74. doi: 10.1097/HJH.0b013e32832cb2a8
36. Mitsnefes M, Flynn JT, Brady T, Baker-Smith C, Daniels SR, Hayman LL, et al. Pediatric ambulatory blood pressure classification: the case for a change. Hypertension. (2021) 78:1206–10. doi: 10.1161/HYPERTENSIONAHA.121.18138
37. Stergiou GS, Palatini P, Parati G, O'Brien E, Januszewicz A, Lurbe E, et al. 2021 European society of hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens. (2021) 39:1293–302. doi: 10.1097/HJH.0000000000002843
38. Stergiou GS, Bountzona I, Alamara C, Vazeou A, Kollias A, Ntineri A. Reproducibility of office and out-of-office blood pressure measurements in children: implications for clinical practice and research. Hypertension. (2021) 77:993–1000. doi: 10.1161/HYPERTENSIONAHA.120.16531
39. Stergiou GS, Yiannes NG, Rarra VC, Panagiotakos DB. Home blood pressure normalcy in children and adolescents: the arsakeion school study. J Hypertens. (2007) 25:1375–9. doi: 10.1097/HJH.0b013e328122d3fc
40. Stergiou G, Stambolliu E, Bountzona I, Ntineri A, Kollias A, Vazeou A, et al. Home blood pressure monitoring in children and adolescents: systematic review of evidence on clinical utility. Curr Hypertens Rep. (2019) 21:64. doi: 10.1007/s11906-019-0967-2
Keywords: adolescents, blood pressure, children, hypertension, monitoring
Citation: Lurbe E, Mancia G, Calpe J, Drożdż D, Erdine S, Fernandez-Aranda F, Hadjipanayis A, Hoyer PF, Jankauskiene A, Jiménez-Murcia S, Litwin M, Mazur A, Pall D, Seeman T, Sinha MD, Simonetti G, Stabouli S and Wühl E (2023) Joint statement for assessing and managing high blood pressure in children and adolescents: Chapter 1. How to correctly measure blood pressure in children and adolescents. Front. Pediatr. 11:1140357. doi: 10.3389/fped.2023.1140357
Received: 8 January 2023; Accepted: 13 March 2023;
Published: 11 April 2023.
Edited by:
Ruan Kruger, North-West University, South AfricaReviewed by:
Rachel Climie, University of Tasmania, AustraliaIbrahim F. Shatat, Sidra Medicine, Qatar
Elaine Urbina, Cincinnati Children's Hospital Medical Center, United States
Joshua Alex Samuels, University of Texas Health Science Center at Houston, United States
© 2023 Lurbe, Mancia, Calpe, Drożdż, Erdine, Fernandez-Aranda, Hadjipanayis, Hoyer, Jankauskiene, Jiménez-Murcia, Litwin, Mazur, Pall, Seeman, Sinha, Simonetti, Stabouli and Wühl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Empar Lurbe ZW1wYXIubHVyYmVAdXYuZXM= Elke Wühl ZWxrZS53dWVobEBtZWQudW5pLmhlaWRlbGJlcmcuZGU= Adamos Hadjipanayis YWRhbW9zQHBhaWRpYXRyb3MuY29t
Specialty Section: This article was submitted to General Pediatrics and Pediatric Emergency Care, a section of the journal Frontiers in Pediatrics