 Junming Huo
Junming Huo Song Chen
Song Chen Jing Li
Jing Li Chengjun Liu
Chengjun Liu- Department of Critical Care Medicine, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, China International Science and Technology Cooperation Base of Child Development and Critical Disorders, Chongqing Key Laboratory of Pediatrics, Children’s Hospital of Chongqing Medical University, Chongqing, China
Objective: To investigate the clinical features, diagnosis and treatment methods and prognosis of retroperitoneal Kaposiform hemangioendothelioma (R-KHE) in children.
Methods: The clinical data of an infant with R-KHE was retrospectively analyzed. Literature on R-KHE in pediatrics were retrieved in databases including Wanfang, CNKI and PubMed as of April 2022.
Results: A 1 month and 6 days female infant with R-KHE was reported. After the diagnosis was confirmed by biopsy and pathological examination, the patient was treated by interventional embolization, and a combined therapy with glucocorticoid, vincristine, sirolimus and propranolol. The patient has been followed up for 1 year and 2 months, and is still alive with tumor. Through literature search, a total of 15 children, together with the case in our report, were included. The main manifestations were diversity among those patients. 14 cases have combined Kasabach-Merritt phenomenon (KMP). 6 cases accepted surgery plus drug therapy. 4 cases accepted only surgery, and 4 cases only accepted drug therapy. While drug therapy plus radiotherapy were employed to 1 case. Improvement was observed in 11 cases, with significantly reduced tumor and survival with tumor. Tumor disappeared completely in 2 cases. While 2 cases suffered death.
Conclusion: R-KHE has diverse clinical presentations and non-specificity in symptoms and imaging examinations, and most cases accompanied with KMP. Methods for R-KHE treatment include surgical resection, interventional embolization and drug therapy. Close attention needs to be paid to the adverse reactions of the drug during the course of treatment.
1. Introduction
Kaposiform hemangioendothelioma (KHE) is a rare vascular tumor with an estimated incidence of 0.91/100,000 (1). It often involves the dermis and extends to the subcutaneous tissue. It is characterized by moderate malignancy and local aggression, and the risk of death in KHE patients is often associated with the Kasabach-Merritt phenomenon (KMP), which occurs in 42%–71% of KHE cases (2–5). KMP is characterized by profound thrombocytopenia, microangiopathic anemia and hypofibrinogenemia. Compared with superficial lesions, Retroperitoneal KHE(R-KHE) has a higher incidence of KMP (2), which means that patients with R-KHE will have a higher mortality rate. It is difficult to diagnose R-KHE, and missed diagnosis or misdiagnosis is inevitable since it has diverse clinical presentations and nonspecific symptoms, and shows no specific manifestations in routine auxiliary examinations, and most of the patients cannot tolerate surgical biopsy due to their critical condition. In addition, the optimal treatment for KHE is to be determined though there are various drugs, including glucocorticoids, vincristine (VCR), interferon alfa and sirolimus, either alone or in combination, being used. Given the challenges in diagnosis and treatment of R-KHE, we report a 1-month-old girl with R-KHE, with a review of the literature on R-KHE, in the hope of providing relevant experience in diagnosis and treatment for future clinical work.
2. Materials and methods
2.1. Clinical data
The patient was a 1 month and 6 days female infant who was admitted to the hospital on March 6, 2021 with “abdominal distension for 20 days, skin petechiae and ecchymoses for 14 days and aggravation for 2 days”. The patient had progressive abdominal distension. Physical examination on admission revealed that the patient had pale complexion and lips, slightly swollen face, trunk and perineum, and scattered petechiae and ecchymoses all over the body, especially on the right waist. As to the auxiliary examinations, the findings of abdominal color Doppler ultrasound on March 7, 2021 included: (1) slightly enlarged liver, but no obvious abnormality in its internal structure; (2) immobile biliary sludge in the gallbladder; and (3) a medium-large amount of peritoneal effusion with cloudy components. Blood test at admission showed: WBC 8.48X109/L, RBC 1.52 × 1012/L, Hb 53 g/L, PLT 5X109/L, and coagulation factors ATTP > 150 s, PT > 150 s, fibrinogen 0.5 g/L, FDP 62.6 mg/L, and D-dimer 12.5 ng/L. CT scan of abdomen on March 11, 2021 showed in Figure 1. Treatment: anti-infection; hemostasis; repeated infusion of platelets, fresh frozen plasma (FFP), cryoprecipitate and red blood cell suspension (RBCS); invasive mechanical ventilation; methylprednisolone + gamma globulin + plasma exchange. On March 12, the patient underwent exploratory laparotomy, retroperitoneal hematoma removal, tissue biopsy and abdominal drainage. Findings during these operations included: dark red hematoma was seen from the right retroperitoneum up to the perirenal space and down to the ileocecal junction in the right lower abdomen; hemorrhage in the mesentery of the colon and the small intestine, with obvious swelling; canal stenosis due to compression by right colon hematoma; and 300 ml blood lose during the operation without obvious bleeding site found. The pathological findings of the biopsy on March 17 indicated R-KHE (Figure 2). After the diagnosis confirmed by the biopsy, the patient was treated with dexamethasone (1 mg/kg, bid) and sirolimus (0.15 mg, bid). After which and in a gradual manner, the patient's hemoglobin and platelet levels became stabilized, and the thoracic and abdominal drainage decreased, with no obvious active bleeding. Fibrinogen fluctuated between 0.6–0.9 g/L during treatment, and gradually rise to normal about 2 weeks after treatment. On April 10, the patient was in a stable condition and was discharged from the hospital with prescriptions of sirolimus and prednisone. The patient was again admitted to the hospital and stayed for chemotherapy with VCR from June 22 to 28. From September 27 to October 26, 2021, the patient was hospitalized again due to intestinal perforation, during which, treatments performed included anti-infection, ileal perforation repair, and abdominal abscess incision and drainage. After discharge, the use of oral drugs was discontinued by the family members without authorization due to their concerns about the side effects of sirolimus and prednisone. The patient was hospitalized from January 16 to 30, 2022 due to severe thrombocytopenia, the patient underwent three times of chemotherapy with VCR, once a week. The abdominal MRI on January 23 was shown in Figure 3. Interventional embolization under the guidance of digital subtraction angiography (DSA) was performed under general anesthesia after comprehensive consideration on January 26. After interventional embolization, platelets of the children gradually return to normal. Oral administrations of sirolimus, prednisone and propranolol were continued for the patient after discharged. The patient received regular outpatient follow-ups. As the platelets gradually stabilized, corticosteroid was gradually reduced within about 5 weeks, and the concentration of sirolimus trough concentration was monitored and maintained at 10–15 ng/ml. Sulfonamide was used to prevent Pneumocystitis Carinii Pneumonia during treatment, and the results of abdominal CT on March 1, 2022 was shown in Figure 4.
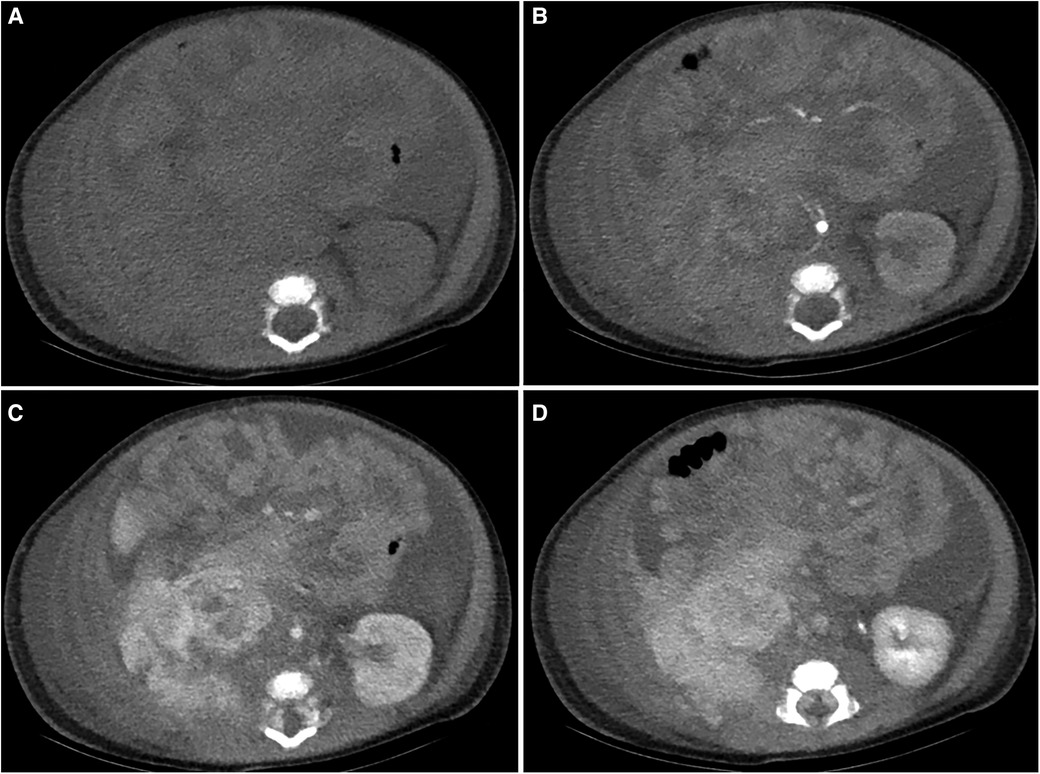
Figure 1. Abdominal CT results of this patient at the first visit. Plain scan (A) indicated a large amount of fluid-density shadow in the abdominal cavity, blurred right-sided retroperitoneal perirenal layers with an iso-low density change. Contrast enhanced scan [(B) arterial phase, (C) venous phase, (D) delayed phase] indicated there was inhomogeneous enhancement in the perirenal lesions.
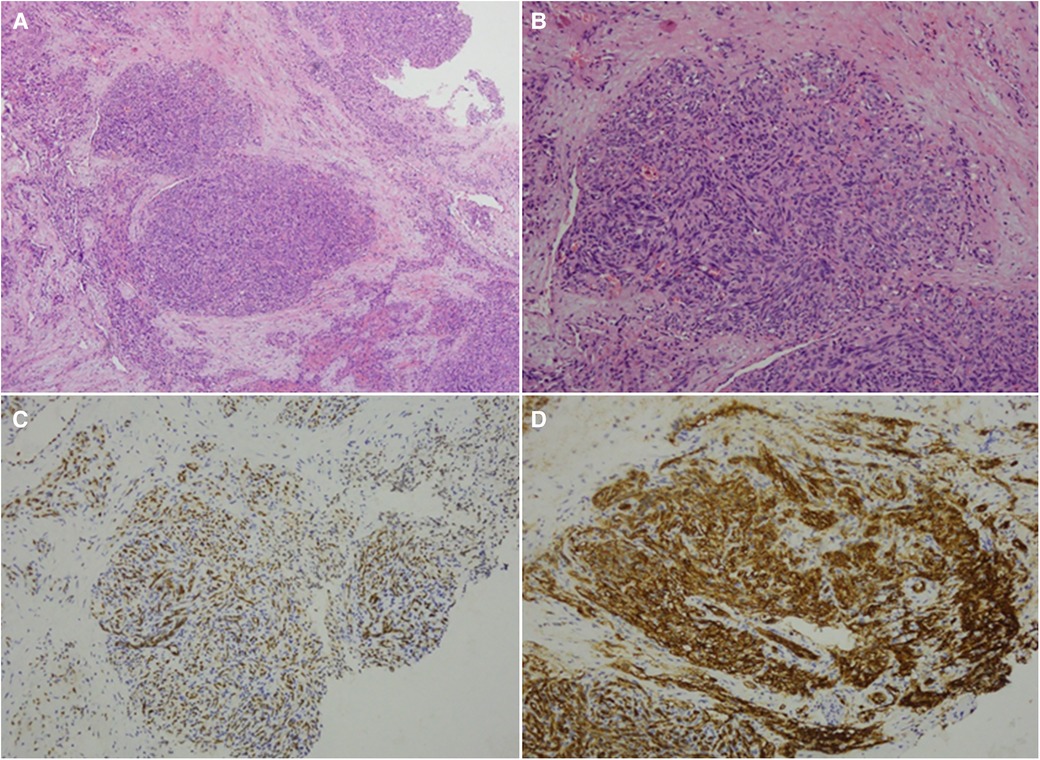
Figure 2. Biopsy results of the patient. Biopsy showed multifocal proliferation of cleft-like hyperplasia of small blood vessels and densely arranged spindle-shaped epithelioid cells, with red blood cells seen in the intercellular clefts [(A) hematoxylin and eosin, ×40; (B) hematoxylin and eosin, ×100]. Immunohistochemistry: FLI-1(+) [(C), ×100], CD31(+) [(D), ×100], CD34 (+), D2-40 partially (+), REG (+), Glut-1 (-), HHV8 (-), Ki67 hotspot 40% (+). The biopsy indicated (retroperitoneal) KHE.
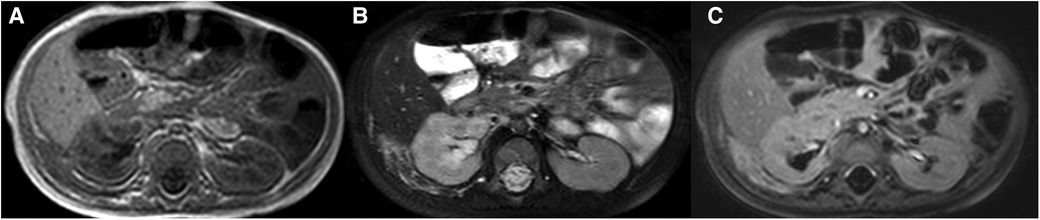
Figure 3. Re-examination by abdominal MRI after 10 months of treatment. The images showed that the lesion of the right kidney was significantly reduced, increased T2 signals, and there was enhancement when with contrast [(A) T1WI, (B) T2WI, (C) contrast-enhanced T2WI].
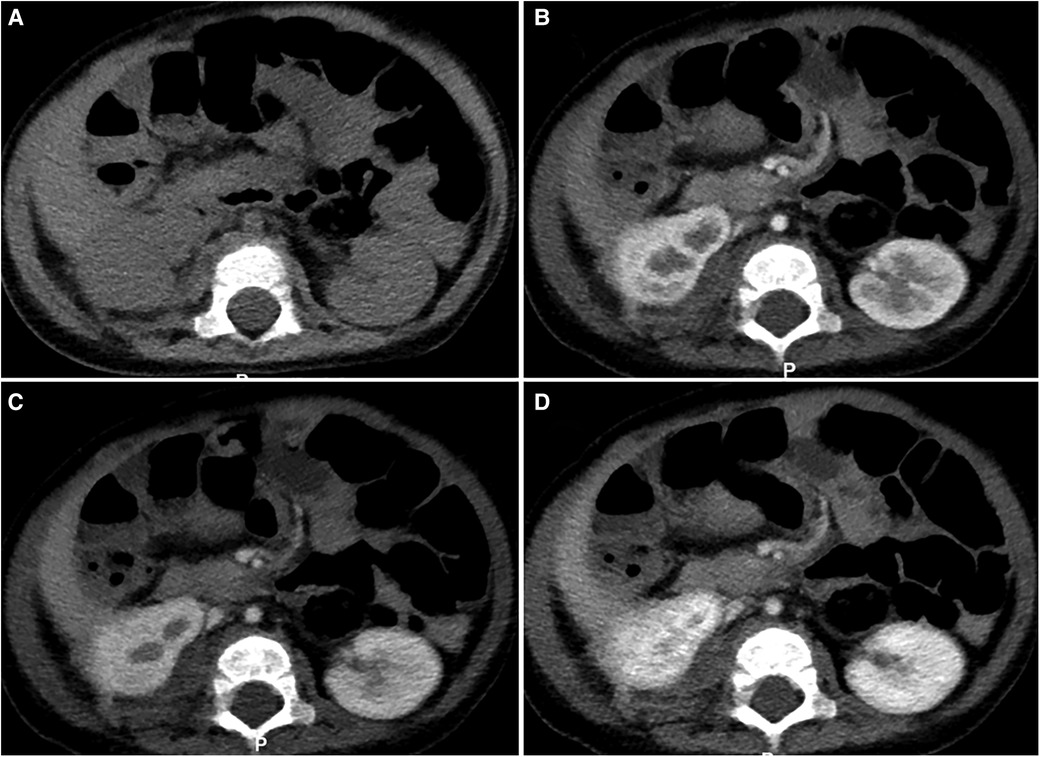
Figure 4. Abdominal CT results of this patient after 11 + months of treatment. The images [(A) plain scan, (B) arterial phase, (C) venous phase, (D) delayed phase] indicated the original peri-renal lesions were significantly reduced, the contour of the right kidney tended to be normal with a few residual lesions, and a little enhancement was seen with contrast.
2.2. Review of the literature
The scope of published literature research was databases including Wanfang, CNKI, and PubMed by March 2022. Key words included Kaposiform hemangioendothelioma (KHE), retroperitoneal Kaposiform hemangioendothelioma (R-KHE), and KMP. After excluding adult cases and those children's cases without full-text articles, a total of 14 cases of R-KHE were retrieved from Chinese and English literatures (6–16).
3. Results
3.1. Prognosis of the patient
As informed by the follow-up phone calls for 1 year and 2 months, the patient was in good growth and development. The retroperitoneal tumor was significantly smaller as shown by subsequent CT scan, and follow-up tests indicated normal platelet and coagulation functions.
3.2. Literature analysis
Together with the case in this report, there are 15 cases of R-KHE in children, as shown in Table 1. The male to female ratio was 12:3, age ranged from 7d to 36 months. Twelve cases underwent biopsy, all 15 cases have clinical symptoms and positive signs, and 14 cases have combined KMP. The main manifestations were abdominal mass in 3 cases, jaundice in 7 cases, abdominal distension and skin purpura in 2 cases, vomiting in 2 cases, and walking instability in 1 case. Auxiliary examinations: 5 cases underwent MRI, and 9 cases underwent abdominal CT. Treatment methods: surgery plus drug therapy for 6 cases, only surgery for 4 cases, only drug therapy for 4 cases, and drug therapy plus radiotherapy for 1 case. Clinical outcomes (Table 2): improvement was observed in 11 cases, with significantly reduced tumor and survival with tumor; complete disappearance of tumor and full clinical recovery in 2 cases; and death in 2 cases.
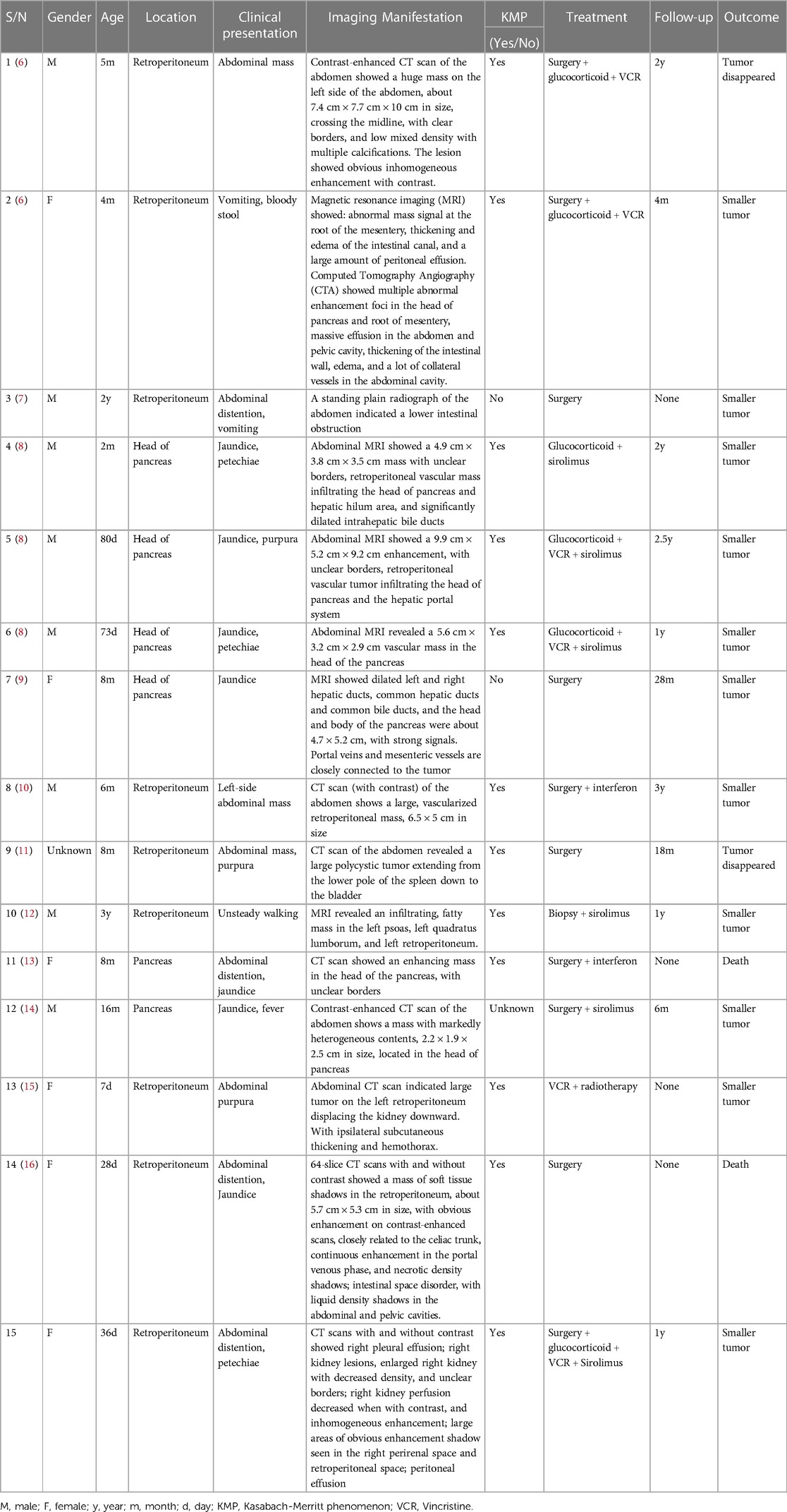
Table 1. General information of R-KHE in children reported in literature review and our case .
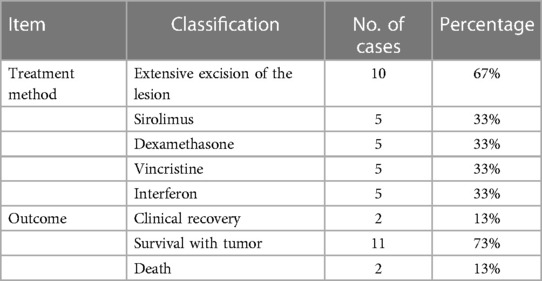
Table 2. Analysis of treatment methods and follow-up outcomes of 15 cases.
4. Discussion
Kaposiform hemangioendothelioma (KHE) is an aggressive tumor that resembles Kaposi's sarcoma (KS) in histology, and most KHE cases manifested in infancy and childhood (4). First reported by Zukerberg in 1993, it was classified as a “locally aggressive or borderline vascular tumor” by the International Society for the Study of Vascular Anomalies (ISSVA) in 2014. According to the morphology of the tumor, Ji et al. (2) divided the tumor into superficial type (limited to the skin and subcutaneous soft tissue, without invading muscle and bone, without invading chest and abdominal cavity), mixed type (involving skin and subcutaneous, deep muscle, bone or joint at the same time) and deep type (involving deep muscle, bone or joint, without skin manifestations). Of which the mixed type was the most common, that's about 63 percent. And only 10% located in the retroperitoneum (4). KHE is one of the main tumors that cause the KMP in infants and young children. Associated with severe (consumption) thrombocytopenia, anemia, secondary fibrinogen reduction and coagulation factor consumption and other clinical presentations, KMP is featured by rapid onset, rapid progression and high mortality (17). R-KHE has diverse clinical presentations and non-specific symptoms and imaging examinations, and often accompanied by KMP. Thus, it has some difficulty in R-KHE diagnosis.
The tumor in our case was located in the retroperitoneum, with severe thrombocytopenia, severe anemia, and coagulation dysfunction when she was admitted to the hospital. Initially we considered it a bleeding disorder caused by some internal disease: immune thrombocytopenia (ITP) or thrombotic thrombocytopenia (TTP)? The patient received glucocorticoid therapy, high-dose gamma globulin pulse therapy, and plasma exchange therapy, but the symptoms showed no improvement. A multidisciplinary consultation was organized, which recommended exploratory laparotomy after infusion of platelets and improvement of coagulation. The subsequent pathological biopsy suggested KHE. Based on this definitive diagnosis, oral administration of sirolimus and dexamethasone was prescribed for the patient.
The incidence of R-KHE is low, and most of the reports are single case study. Both the clinical presentations and auxiliary examinations are non-specific. The diagnosis is mostly based on pathological biopsy, and there are no standard treatment protocols. Most R-KHE in previous reports occurred in the pancreas, and the common clinical presentations include abdominal pain and jaundice. The lesion of our case was in the kidney, with abdominal distension and skin petechiae as the main manifestations. The common auxiliary examinations for R-KHE include abdominal contrast-enhanced CT scan, contrast-enhanced MRI (18), and biopsy. Among them, CT scan is quicker and has better performance in evaluating tumor size and degree of infiltration, but it is insufficient on specificity. MRI is more valuable for diagnosing vascular tumors, but it may be too time-consuming to perform in some critical cases (19). Pathological diagnosis, as the gold standard for the diagnosis of KHE, still has the disadvantage that some patients in critical condition cannot tolerate surgical biopsy. Among all 15 cases, there were 9 cases underwent abdominal contrast-enhanced CT scan, which showed retroperitoneal mass or diffuse low-density shadow, and enhancement when with contrast; 5 cases underwent abdominal contrast-enhanced MRI, with high and low signals on T1-weighted images and high signals on T2-weighted images, and inhomogeneous enhancement after contrast applied; 12 cases underwent surgical biopsy to confirm the diagnosis. It is feasible to perform ultrasound or CT-guided biopsy on KHE patients, which has been reported in previous literature (20). Case 10 was performed by CT-guided puncture biopsy, and the final diagnosis was confirmed. Our case was treated by exploratory laparotomy, because we didn't know the cause of the disease at beginning. Considering the critical status of the patient, we had chosen exploratory laparotomy to stop bleeding, remove hematoma, and make a definite diagnosis.
There are several options for the treatment of KHE, including drug therapy, surgery and arterial embolization. In clinical practice, a combined therapy is often preferred due to the limited efficacy of a single regimen (21). Most cases of KMP occur in infants younger than 6 months, in whom, there may be organ compression as the tumor increasing, accompanied with formation of large hematoma and severe thrombocytopenia. Platelet transfusions can exacerbate this phenomenon and should be avoided if possible. Platelets are given only when the patient has life-threatening bleeding or is preparing for biopsy or tumor resection (21). Most deaths are due to bleeding in vital organs. The mortality could be higher if the tumor is located in the retroperitoneum. Because most R-KHE cases are accompanied by severe thrombocytopenia and coagulation dysfunction, some patients cannot tolerate surgical treatment, but when the patient has life-threatening bleeding, it is proper to consider surgical excision or biopsy after the patient has been treated with platelets and fresh frozen plasma. Among the 15 cases in this study, 10 children received extensive resection of the lesions, which was supplemented by postoperative drug treatment, and 8 of them recovered well after surgery, with rapid recovery of platelet and coagulation functions. The significant reduction in tumor volume may account for the rapid normalization of platelet counts and disappearance of residual lesions. Interventional embolization under the guidance of digital subtraction angiography (DSA) is also an important therapeutic method when the lesions are extensive, unresectable, ineffective in drug therapy, or the coagulation function is not improved and continues to deteriorate (22). Its advantage is that it has a rapid effect. Through embolization of the blood supplying artery, the tumor is ischemia, degeneration, necrosis, shrinkage, and the capture and destruction of platelets in the tumor are reduced (22). In our case, the disease relapsed, and platelets decreased significantly. Interventional embolization was performed to the patient, and platelets gradually returned to normal along with drug therapies.
Despite the multiple drug options for KMP treatment, the reported efficacy varies greatly. Main drugs used in clinical practice include VCR, steroids, sirolimus and propranolol (21). The Expert Consensus on KMP Treatment formulated by Drolet et al. recommended a glucocorticoid + VCR therapy as the initial treatment for KHE patients with KMP (17). Among the cases reported in this study, 6 children were treated with glucocorticoid combined with VCR, and good curative effects were found in all of them. Recent retrospective clinical studies have found that sirolimus has shown good effects in the treatment of KHE, even in patients that being resistant to steroid, combined with KMP and showing no response to VCR, and the effects are long-lasting (23). The six children received oral sirolimus treatment, and the treatment achieved good effects. The dosage is: sirolimus [0.08 mg/kg, orally, twice a day, to maintain the plasma drug concentration at 10–15 ng/ml]. In most cases, the drug takes effect in 5 to 10 days, and the drug concentration in plasma reaches a stable level in 3 to 4 weeks (23). If the drug treatment is effective, the platelet level will increase significantly in a short period of time, the coagulation function will also be significantly improved; and in some patients bloody pleural effusion or peritoneal effusion will also be reduced. Recent studies (24) have shown that short-term prednisolone combined with sirolimus is superior to sirolimus monotherapy in improving the signs and symptoms of KMP-active KHE. In our case, sirolimus combined with prednisone was treated orally after discharge, and the patient gradually decreased and stopped prednisone treatment about 5 weeks after platelet stabilization during follow-up. However, improper feeding method, severe vomiting and jaundice will affect the absorption and effectiveness of sirolimus, so close monitoring of its plasmatic concentration is the key to achieving good therapeutic effects (25). As reported in literature, the short-term toxic side effects of sirolimus mainly include immunosuppression, elevated transaminases, hyperlipidemia, mucositis, and delayed vaccination (25). The patient in this study developed intestinal perforation and complications of intestinal infection 6 months after oral sirolimus treatment, but improved after active anti-infection and surgical treatment. Therefore, we need to monitor closely during treatment and be alert to the side effects of sirolimus. In our case, family members of the patient stopped sirolimus by themselves, which resulted in relapse. Therefore, it is important to strengthen the education of the family members in the process of diagnosis and treatment.
Together with the cases in the literature and our study, we conclude the following revelations: (1) R-KHE occurs in very young patients, mostly in infants of 1 to 4 months old, and R-KHE is often accompanied with KMP; (2) R-KHE shall be distinguished from solid retroperitoneal tumors and hematological tumors, such as idiopathic thrombocytopenic purpura; (3) the clinical presentations of R-KHE are diverse, mainly including abdominal distension, abdominal mass, jaundice, skin petechiae and ecchymoses. The symptoms are nonspecific; (4) Imaging manifestations of R-KHE: CT scan without contrast showed mass or diffuse low-density shadows in the retroperitoneum, and the lesions were obviously enhanced when with contrast, and some were accompanied by peritoneal effusion. Contrast-enhanced MRI may also be used to assist diagnosis; (5) for patients with above symptoms and imaging manifestations, if with accompanied KMP and the condition is critical, surgical biopsy can be performed after improvement of coagulation and infusion of platelets. If biopsy is not feasible due to the condition, clinical judgement could be made based on previous diagnosis and treatment experience, and diagnostic treatment with drugs could be performed; (6) if the effect of single drug therapy is unsatisfactory, a combination therapy could be considered.
5. Conclusion
The clinical presentations of R-KHE are diverse and non-specific, most of which are associated with KMP, with rapid onset, rapid progression, and high mortality. Therefore, we should be wary of this disease in children with severe thrombocytopenia, anemia, severe coagulation dysfunction combined with intra-abdominal hemorrhage. Intervention-guided needle biopsy can be performed, It can also be treated with surgery if the condition permits. But, if the patient is in a critical condition and cannot tolerate surgery, a comprehensive judgment shall be made with combined consideration of the medical history, and diagnostic treatment with drugs could be performed. At present, sirolimus shows good outcomes in KHE treatment, but the plasmatic concentration should be monitored during medication, and attention should be paid to the side effects. If the treatment effect is not good, a combination with other drugs should be considered.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Children's Hospital of Chongqing Medical University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
JMH is the principal author and contributed to data collection, clinical follow-up, and drafted the manuscript. JMH and SC contributed to the literature retravel and selection. JMH, SC, JL and CJL contributed to the study conception and revised the manuscript critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Acknowledgments
Thanks for the cooperation of all departments in the progress of treatment.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ji Y, Chen S, Yang K, Xia C, Li L. Kaposiform hemangioendothelioma: current knowledge and future perspectives. Orphanet J Rare Dis. (2020) 15(1):39. doi: 10.1186/s13023-020-1320-1
2. Ji Y, Yang K, Peng S, Chen S, Xiang B, Xu Z, et al. Kaposiform haemangioendothelioma: clinical features, complications and risk factors for Kasabach-Merritt phenomenon. Br J Dermatol. (2018) 179(2):457–63. doi: 10.1111/bjd.16601
3. Lyons LL, North PE, Mac-Moune Lai F, Stoler MH, Folpe AL, Weiss SW. Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol. (2004) 28(5):559–68. doi: 10.1097/00000478-200405000-00001
4. Croteau SE, Liang MG, Kozakewich HP, Alomari AI, Fishman SJ, Mulliken JB, et al. Kaposiform hemangioendothelioma: atypical features and risks of Kasabach-Merritt phenomenon in 107 referrals. J Pediatr. (2013) 162(1):142–7. doi: 10.1016/j.jpeds.2012.06.044
5. Harbers VEM, van der Salm N, Pegge SAH, van der Vleuten CJM, Verhoeven BH, Vrancken S, et al. Effective low-dose sirolimus regimen for kaposiform haemangioendothelioma with Kasabach-Merritt phenomenon in young infants. Br J Clin Pharmacol. (2022) 88(6):2769–81. doi: 10.1111/bcp.15202
6. Li K, Xiao X, Dong K, Yao W, Wang Z. Experience in treatment of retroperitoneal kaposiform hemangioendothelioma. J Clin Pediatr Surg. (2014) 13(1):55–7. doi: 10.3969/j.issn.1671-6353.2014.01.016
7. Guan J, Wu L. A case report of abdominal Kaposiform emangioendothelioma and literature review. J Qiqihar Med Univ. (2018) 39(19):2355–57. doi: 10.3969/j.issn.1002-1256.2018.19.052
8. Yao W, Li K, Wang Z, Dong K, Zheng S. Retroperitoneal kaposiform hemangioendothelioma complicated by kasabach-merritt phenomenon and obstructive jaundice: a retrospective series of 3 patients treated with sirolimus. Pediatr Dermatol. (2020) 37(4):677–80. doi: 10.1111/pde.14157
9. Wang X, Xiong Q. Pancreatic hemangioendothelioma, an extremely rare vascular anomaly in children: a case report and literature review. Oncol Lett. (2015) 10(2):793–97. doi: 10.3892/ol.2015.3270
10. Harper L, Michel JL, Enjolras O, Raynaud-Mounet N, Rivière JP, Heigele T, et al. Successful management of a retroperitoneal kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon using alpha-interferon. Eur J Pediatr Surg. (2006) 16(5):369–72. doi: 10.1055/s-2006-924615
11. Brasanac D, Janic D, Boricic I, Jovanovic N, Dokmanovic L. Retroperitoneal kaposiform hemangioendothelioma with tufted angioma-like features in an infant with Kasabach-Merritt syndrome. Pathol Int. (2003) 53(9):627–31. doi: 10.1046/j.1440-1827.2003.01518.x
12. Iacobas I, Simon ML, Amir T, Gribbin CE, McPartland TG, Kaufman MR, et al. Decreased vascularization of retroperitoneal kaposiform hemangioendothelioma induced by treatment with sirolimus explains relief of symptoms. Clin Imaging. (2015) 39(3):529–32. doi: 10.1016/j.clinimag.2015.01.003
13. Mathew D, Mahomed N. Pancreatic kaposiform hemangioendothelioma complicated by Kasabach-Merritt phenomenon: a rare entity. SA J Radiol. (2019) 23(1):1760. doi: 10.4102/sajr.v23i1.1760
14. Wang C, Li Y, Xiang B, Li F, Chen S, Li L, et al. Successful management of pancreatic kaposiform hemangioendothelioma with sirolimus: case report and literature review. Pancreas. (2017) 46(5):e39–41. doi: 10.1097/mpa.0000000000000801
15. Takemura R, Wada Y. Large abdominal purpura of neonatal retroperitoneal kaposiform hemangioendothelioma. Clin Case Rep. (2021) 9(8):e04600. doi: 10.1002/ccr3.4600
16. Xu Q, Ding D, Luo Z, Zhang S, Yan X, Wang H, et al. A case of neonatal mesenteric Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon. Chin J Pediatr. (2021) 59(2):139–41. doi: 10.3760/cma.j.cn112140-20200820-00813
17. Drolet BA, Trenor CC 3rd, Brandão LR, Chiu YE, Chun RH, Dasgupta R, et al. Consensus-derived practice standards plan for complicated Kaposiform hemangioendothelioma. J Pediatr. (2013) 163(1):285–91. doi: 10.1016/j.jpeds.2013.03.080
18. Hu PA, Zhou ZR. Clinical and imaging features of Kaposiform hemangioendothelioma. Br J Radiol. (2018) 91(1086):20170798. doi: 10.1259/bjr.20170798
19. Peng S, Xia C, Yang K, Chen S, Ji Y. Kaposiform haemangioendothelioma: magnetic resonance imaging features in 64 cases. BMC Pediatr. (2021) 21(1):107. doi: 10.1186/s12887-021-02573-8
20. Shen W, Cui J, Chen J, Zou J, Xiaoying Z. Treating kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon by intralesional injection of absolute ethanol. J Craniofac Surg. (2014) 25(6):2188–91. doi: 10.1097/scs.0000000000001145
21. Schmid I, Klenk AK, Sparber-Sauer M, Koscielniak E, Maxwell R, Häberle B. Kaposiform hemangioendothelioma in children: a benign vascular tumor with multiple treatment options. World J Pediatr. (2018) 14(4):322–29. doi: 10.1007/s12519-018-0171-5
22. Brill R, Uller W, Huf V, Müller-Wille R, Schmid I, Pohl A, et al. Additive value of transarterial embolization to systemic sirolimus treatment in kaposiform hemangioendothelioma. Int J Cancer. (2021) 148(9):2345–51. doi: 10.1002/ijc.33406
23. Wang Z, Li K, Dong K, Xiao X, Zheng S. Refractory Kasabach-Merritt phenomenon successfully treated with sirolimus, and a mini-review of the published work. J Dermatol. (2015) 42(4):401–4. doi: 10.1111/1346-8138.12797
24. Ji Y, Chen S, Zhou J, Yang K, Zhang X, Xiang B, et al. Sirolimus plus prednisolone vs sirolimus monotherapy for kaposiform hemangioendothelioma: a randomized clinical trial. Blood. (2022) 139(11):1619–30. doi: 10.1182/blood.2021014027
Keywords: kaposiform hemangioendothelioma, retroperitoneal, kasabach-Merritt phenomenon, pediatric, literature review
Citation: Huo J, Chen S, Li J and Liu C (2023) Retroperitoneal kaposiform hemangioendothelioma with kasabach-merritt phenomenon in children: A case report and review of the literature. Front. Pediatr. 11:1138689. doi: 10.3389/fped.2023.1138689
Received: 6 January 2023; Accepted: 28 February 2023;
Published: 17 March 2023.
Edited by:
Wang Zuopeng, Fudan University, China© 2023 Huo, Chen, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chengjun Liu bGl1Y3dkQDE2My5jb20=
Specialty Section: This article was submitted to Pediatric Critical Care, a section of the journal Frontiers in Pediatrics