
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr. , 02 August 2023
Sec. Pediatric Cardiology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1137853
 Sophie Quennelle1,2,3*Damien Bonnet1,3
Sophie Quennelle1,2,3*Damien Bonnet1,3
Diastolic dysfunction refers to a structural or functional abnormality of the left ventricle, resulting in impaired filling of the heart. Severe diastolic dysfunction can lead to congestive heart failure even when the left ventricle systolic function is normal. Heart failure with preserved ejection fraction (HFpEF) accounts for nearly half of the hospitalizations for acute heart failure in the adult population but the clinical recognition and understanding of HFpEF in children is poor. The condition is certainly much less frequent than in the adult population but the confirmatory diagnosis of diastolic dysfunction in children is also challenging. The underlying causes of HFpEF in children are diverse and differ from the main cause in adults. This review addresses the underlying causes and prognostic factors of HFpEF in children. We describe the pulmonary hypertension profiles associated with this cardiac condition. We discuss diagnosis difficulties in clinical practice, and we provide a simplified diagnostic algorithm for HFpEF in children.
Left Ventricular (LV) diastolic function plays an important role in determining the kinetics and quality of ventricular filling and thereby also the stroke volume. It can be defined as the capacity of the heart to relax and distend during diastoles leading to fulfilling of the LV chamber up to an appropriate telediastolic volume. Diastolic dysfunction is defined by the incapacity of the ventricle to fill in even if the atrial pressure is normal. Diastolic dysfunction might be due to a prolonged relaxation or/and an increased stiffness of the ventricle (1). The normal functioning of the left ventricle during diastole involves the relaxation of its walls, allowing for the ventricle to expand and accommodate incoming blood. This is facilitated by the normal functioning of muscle cells within the ventricle, which contract during systole and then relax during diastole. However, in diastolic dysfunction, the relaxation of the ventricular walls is impaired or slowed, resulting in decreased filling of the left ventricle. At a cellular level, relaxation of the left ventricle during diastole is enabled by the detachment of actin-myosin cross bridges, which occurs after calcium uptake by the sarcoplasmic reticulum, leading to a decrease in cellular tension. It is the main protein that's modulates myocyte stiffness. Additionally, the increased stiffness of the ventricular walls, due to conditions such as fibrosis or hypertrophy, can also contribute to diastolic dysfunction by limiting the ventricle's ability to expand and accommodate blood. Chamber stiffness is primarily determined by the stiffness properties of the sarcomeres, the interstitial space, and LV chamber geometry and wall thickness (1). Another component that influences LV filling and diastolic pressures is elastic recoil. Early diastolic recoil, is the ability of the left ventricle to “snap back” into its relaxed state, it contributes to the quick decrease in LV pressure during isovolumic relaxation time (IVRT). In diastolic dysfunction, this recoil may be delayed or reduced, further impeding the ventricle's ability to fill with blood during diastole. Titin plays an important role in LV expansion. It is an elastic protein that assembles sarcomere unity and acts as an elastic spring that is squeezed during systole and recoils during diastole (2). Left atrial pressure, is closely related to LV pressure and is used as a surrogate marker of LV filling pressures. During diastole, when the LV is filling with blood, the pressure within the LV pressure increases. This increased pressure is then transmitted backwards into the left atrium, resulting in an increase in left atrial pressure. Therefore, in conditions where LV diastolic function is impaired, there is an associated increase in LAP, reflecting the elevated filling pressures within the LV.
Today, the commonly used definition is heart failure with a left ventricle ejection fraction (LVEF) >50% associated with evidence of spontaneous or provokable increased left ventricle (LV) filling pressures (2). There is a thin line between HFpEF and diastolic dysfunction as patients with LV diastolic dysfunction are often asymptomatic at rest but experience limitations during exercise. Clinical presentations of HFpEF rank from acute heart failure to shortness of breath during effort. While adults are able to describe the onset or worsening of shortness of breath after having experienced well-tolerated efforts in the past, poor exercise tolerance in a child could be difficult to identify.
LV diastolic dysfunction has been well studied and described in adults as HFpEF accounts for at least half the patients diagnosed with heart failure (3). Risk factors in adults include age, obesity, hypertension, coronary artery disease and diabetes mellitus (4, 5). However, comprehensive studies were conducted on elderly diabetic and hypertensive patients (6–8) and do not reflect diastolic dysfunction epidemiology and physiopathology in the pediatric population. Indeed, insights on the epidemiology and causes of HFpEF in children are scarce. There are few studies that evaluated the LV diastolic function in children (9–11) and diastolic function screening is challenging in routine pediatric cardiologist's evaluation (12). As a consequence, HFpEF prevalence in children is unknown and probably underestimated. Pan et al. (10) reported 421 children suffering from diastolic heart failure. This large cohort was collected between 2004 and 2014 at the Children's Hospital of Chongqing Medical University. Among a series of 3,907 pediatric hospitalizations in a cardiology department that were retrospectively reviewed, only 18 patients were considered as having HFpEF (0.5%) (11).
HFpEF is a heterogeneous group of diseases characterized by symptoms of heart failure due to increase in myocardial stiffness. The physiology and cellular mechanism of HFpEF depends on the cause and involves, among other things, cardiac hypertrophy and fibrosis (13), intrinsic myocardial dysfunction (14) impaired calcium handling (15), titin stiffening (16), inflammatory state (17), large and small vessels disease (18).
In restrictive cardiomyopathy (RCM), LV wall thickness is more often within normal limits and for Gewillig the pathophysiology of RCM is related to myocyte abnormality such as myocyte hypertrophy, enlarged, irregular and hyperchromatic myocyte nuclei (19). Genetic disorders leading to intracellular accumulation of substances such as Anderson Fabry disease (20), Danon disease (21), iron overload cardiomyopathy (22) are examples of myocyte induced restrictive physiology.
In the study of Lombardi et al. (23), a linear correlation between aortic elasticity and LV diastolic function was observed, which raises the hypothesis that, just like in the elderly population, aortic vascular stiffness leads to LV diastolic dysfunction. Indeed, with increased vascular stiffness, the systolic pulse wave velocity is increased and, thus, the reflected wave returns to the heart earlier, during late systole increasing late systolic afterload, which affects thick-thin myofilament interactions and crossbridge dissociation, leading to impaired relaxation.
Interstitial myocardial fibrosis also plays a role in the pathogenesis of the LV diastolic dysfunction as it increases ventricular rigidity and compromise the stretching capability of the myofibrils (24). Collagen is a key component of the myocardial extracellular environment, and increased collagen deposition alters myocardium viscoelasticity, impairing relaxation, diastolic recoil, and passive stiffness (25). Fibrosis is a common endpoint of myocardium pathologic processes such as chronic ischemic heart disease of myocarditis.
The causes of LV diastolic dysfunction in children differs substantially from the classical risk factors identified in adults, intrinsic myocytes abnormality seems to be the leading cause of diastolic dysfunction in children. Primary cardiomyopathies are diseases of the heart muscle in which the myocardial dysfunction appears in the absence of systemic comorbidities, valvular or congenital heart disease (26). Hypertrophic, dilated, and restrictive cardiomyopathies are primary cardiomyopathies that can lead to diastolic dysfunction. There are two major clinical categories of LV diastolic dysfunction in children: congenital, related to a genetic or metabolic disorder and acquired i.e., secondary to another cause (27). In this review, we choose not to describe transitory diastolic dysfunction related to congenital heart defect as it almost always resolves after cardiac surgery.
Dilated cardiomyopathy (DCM) is defined by the presence of a dilated LV with systolic dysfunction without any hemodynamic, physiological, ischemic or anatomic cause (28). DCM accounts for around 50% of the pediatric cardiomyopathy cases (26). Patients suffering from DCM present at first heart failure with reduced ejection fraction, but progression of cell death and extension of fibrosis of the LV often lead to diastolic dysfunction. Occurrence of diastolic dysfunction with elevated filling pressures is associated with poor prognosis in these conditions (29).
Hypertrophic cardiomyopathy (HCM) is defined by an hypertrophied and non-dilated ventricle in the absence of a hemodynamic cause of wall thickening, excluding physiological hypertrophy (secondary to physical activity) and pathological hypertrophy (secondary to aortic coarctation, aortic valvular stenosis, hypertension) (28). HCM is the second most common pediatric cardiomyopathy (40% of patients) (26). Diastolic function impairment is common and of variable severity. Impaired calcium handling, myocyte hypertrophy and disarray, ischemia and fibrosis are the etiologies of diastolic dysfunction (30).
Diastolic dysfunction has been described mainly in children suffering from restrictive cardiomyopathy, accounting for less than 5% of pediatric cardiomyopathy cases (19, 26). Leading mutations associated with restrictive cardiomyopathy are MYH7, TNNI3, TNNT2, MYL2, and DES (31). Restrictive cardiomyopathies may also be secondary to systemic diseases including infiltrative disorder, collagen-vascular diseases (9), neoplastic process (32), thoracic irradiation and chemotherapy, bone marrow transplantation (26, 32, 33), and endomyocardial disease with or without eosinophilia resulting in fibrosis of the endocardium. Left heart obstruction such as coarctation and aortic stenosis can result in restrictive physiology of the left ventricle that persists after repair (18, 34, 35). The common mechanism in these cardiomyopathies is the increasing myocardial stiffness, which decreases compliance.
LV diastolic dysfunction has been described in patients with aortic coarctation or aortic stenosis (18, 23, 24, 35) even after successful repair. In the study of Moskowitz et al. (35), altered LV relaxation was found in children with successful coarctation repair and late diastolic filling pressures were influenced by LV mass suggesting that hypertrophy rather than increased afterload is the primary determinant of the impaired LV diastolic function.
Some extrinsic factors have also been described in children such as inflammatory diseases: acute myocarditis (36), Kawasaki shock syndrome (37), and more recently Multisystem Inflammatory Syndrome in Children (MISC) due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (38). Graft rejection is also a cause of LV diastolic dysfunction in pediatric heart recipients (39, 40). Myocardial edema secondary to the inflammation causes the impaired ventricular compliance.
Transient LV diastolic dysfunction can be observed in acute contexts such as tachycardia, during the early post-operative period or during sepsis. It is important to note that at birth (during the first 7 days/the first two months for preterms) the diastolic properties of the LV are significantly impaired without pathological significance.
As for adults, renal insufficiency (41–44) and obesity are risk factors for diastolic dysfunction (45, 46). Restrictive physiology of the left ventricle has also been described in infants of mothers with gestational diabetes (47–49). Other acquired conditions include deposition diseases that reduce ventricular compliance (e.g., iron infiltration) (22).
In some cases, diastolic dysfunction may not cause any symptoms and may only be suspected during a routine echocardiography. In other cases, it can cause symptoms such as shortness of breath, atypical asthma, and syncope. The clinical signs that may suggest the presence of diastolic dysfunction include increased jugular venous pressure, hepatomegaly, oedema and ascites (19). Lack of appetite, fatigue and infection susceptibility are markers of heart failure exacerbation. Electrocardiogram (EKG) findings are generally not specific for diastolic dysfunction. Electric signs of left atrial enlargement, biatrial hypertrophy, abnormal Q wave or pseudoinfarct pattern, repolarization abnormalities such as the T wave notched or biphasic can be noted (19). Chest x-ray can show pulmonary venous congestion, and, depending on the underlying cardiac condition, cardiomegaly (19). These symptoms are not specific and may be related to left ventricular systolic dysfunction which makes the diagnosis even more difficult.
Group 2 pulmonary hypertension includes PH associated with left heart disease including HFpEF, heart failure with reduce ejection fraction, valvular heart diseases and congenital heart diseases. Despite similar hemodynamic profiles, there are significant disparities between these patients' groups in terms of comorbidities and clinical phenotypes (50). The hemodynamic definition of group 2 PH was proposed during the 6th World Symposium on PH as a mean pulmonary artery pressure of >20 mm Hg and a pulmonary artery wedge pressure of >15 mm Hg (51). HFpEF associated with PH can be subdivided into isolated postcapillary pulmonary hypertension (IPH) and combined postcapillary and precapillary pulmonary hypertension (CPH). The diagnosis is based on the pulmonary vascular resistance (PVR) measurement during RHC: <3 Wood units (WU) for IPH or ≥3 WU for CPH. This distinction is crucial since it influences therapeutic strategies (52). The pathophysiologic mechanisms in HFpEF associated with PH have been well described in adults. Abnormal relaxation and increased stiffness of the LV lead to an increase in LV and left atrial pressure (53). Left atrial elevated pressures expose the lung pulmonary veins to elevation in pressure (54) and cause the stress failure of the alveolar-capillary junction resulting in pulmonary edema and inflammation. Inflammatory mediators increase endothelin-1 depression and decrease nitric oxide and natriuretic peptide activity. The fibroblast proliferation is activated and leads to the occlusion of the lumen and thickening of the alveolar septa (55). This structural remodeling associated with lung edema compresses small lung arterioles and induces precapillary PH. Thus, with progress of the diastolic disease PH can evolve from a postcapillary to a combined PH (pre and postcapillary). The pulmonary hemodynamic profiles in HFpEF have received little attention but the development of PH with elevated pulmonary vascular resistance in HFpEF is recognized as an important contributor to morbidity and mortality. PH profiles has not yet been studied in pediatrics HFpEF patients but PH has been well described in children suffering from RCM as a relevant proportion of them developed CPH unresponsing to vasodilator testing and precluding them from orthotopic heart transplantation (56). Up to half of the RCM children have PH at diagnosis (57) it is a factor of poor prognosis and therapeutic solution are scares (58).
The clinical recognition and understanding of heart failure with preserved ejection fraction in children is poor. This might be because it is a rare condition but also because the diagnosis of diastolic dysfunction in children is difficult in clinical practice. The symptoms may be subtle and can vary depending on the severity of the condition. The consensual definition of HFpEF is the presence of signs and symptoms of heart failure, a LV ejection fraction >50% associated with evidence of spontaneous or provokable increased LV filling pressure (3).
The gold standard to characterize LV relaxation is cardiac catheterization. A high-fidelity catheter placed into the LV measure simultaneously LV volumes and pressure. The LV pressure-volume loops reflects the filling and contractile properties of the ventricle (5). The commonly measured parameters are (1) Time constant of relaxation (tau or τ) that reflects the rate of decline of LV pressure during the isovolumic relaxation period (IVRT). Normal duration of tau is 30–40 ms (1). (2) Pulmonary capillary wedge pressure (PCWP) is the pressure measured in the pulmonary artery during diastole, which reflects the pressure in the left atrium and left ventricle. (3) Left ventricular end-diastolic pressure (LVEDP) is the pressure measured directly within the left ventricle at the end of diastole. Also, rapid saline loading during RHC can be used to assess the response of the LV and further elucidate the pathophysiology of heart failure (59). Indeed, an increase in PCWP in response to an increased afterload may suggest that diastolic dysfunction is related to increased ventricular stiffness.
Because of its invasive nature, technical complexity, and cost, heart catheterization is impractical for the routine evaluation of the LV filling pressures that are almost always estimated by transthoracic echocardiography (TTE). The H2FPEF (60) and the HFA–PEFF diagnostic algorithm (61) have been proposed to evaluate LV filling pressure in adults but precise thresholds are missing in the pediatric population (12). Indeed, in children, tachycardia and pediatric particularities make Doppler measurements challenging and adults cut-off values for these various parameters are inappropriate (62). Former studies attempted to determine specific TTE parameters to facilitate LV End Diastolic Pressure (LVEDP) estimation (63, 64). Dragulescu and al. found that the mitral E wave deceleration time (DT) (153 ± 23 ms in control patient vs. 97 ± 27 ms in RCM patients) and the mitral lateral peak early diastolic tissue velocity (normal if >11 cm/s) were the most discriminating parameters (12). Peak late diastolic mitral velocities (A) vary significantly throughout childhood, this impacts the peak early to late diastolic filling velocity (E/A) ratio and this parameter should not be considered without taking into account the patient's age (65). In contrast, the isovolumic relaxation time appeared stable with age which makes it an excellent parameter in children. Sasaki and al. compared the echocardiographic findings of 9 RCM patients with 27 controls and concluded that the left atrial size distinguished patients with and without diastolic dysfunction with the least overlap as the indexed left atrial area was significantly larger in RCM group: median 22.8 cm2/m2 (range 16.9–28.6) vs. 10.3 cm2/m2 (range 8.3–12.3) in the control group (66). By providing quantitative analysis of LV longitudinal function speckle tracking-derived global longitudinal strain (GLS) is accurate in early detection of subclinical alterations in LV longitudinal function (63). There is not clear threshold for normal GLS in children (64). In the study of McAree and al (67), it appears that patients suffering from MISC presented a lower mean GLS than controls (−20.4 (±2.8) vs. −22.0 (±1.9).
The B-type natriuretic peptide (BNP) and its pro-hormone NT-proBNP (N-terminal pro-B-type natriuretic peptide) are produced by the ventricles in response to increased pressure or volume loads. It is typically released when the myocytes are stretched or under stress (68) NT-proBNP levels can be elevated in children with left ventricular diastolic dysfunction because the increased pressure or volume in the heart leads to the release of NT-proBNP. Higher levels of NT-proBNP can therefore be a marker of diastolic dysfunction and may be used to help diagnose this condition. However, NT-proBNP levels are dependent on age and, to a lesser extent, on gender in the pediatric population. In the review of Nir et al. (69), the data from four studies which included patients who had NT-proBNP dosage for other reasons than heart failure was concatenated, taking the 95th percentile as the upper limit for normal. They proposed the normal NT-proBNP threshold for age (reported in Table 1). Inspired by H2FPEF (60) and the HFA–PEFF diagnostic algorithm (61) that is used in adults, we propose a stepwise diagnosis approach that is a compilation of published criteria (Table 1). Another pertinent biomarker is aldosterone, indeed, in the study of Masutani and al (11). the aldosterone/BNP ratio was markedly higher in HFpEF patients than in HFrEF patients (38 ± 63 vs. 1.7 ± 1.9, P < 0.05) and “ROC curve analysis showed that an aldosterone/ BNP ratio of 10.3 or higher best predicted HFpEF [area under the curve (AUC) = 0.89], with a sensitivity of 0.67 and specificity of 1.0.”.
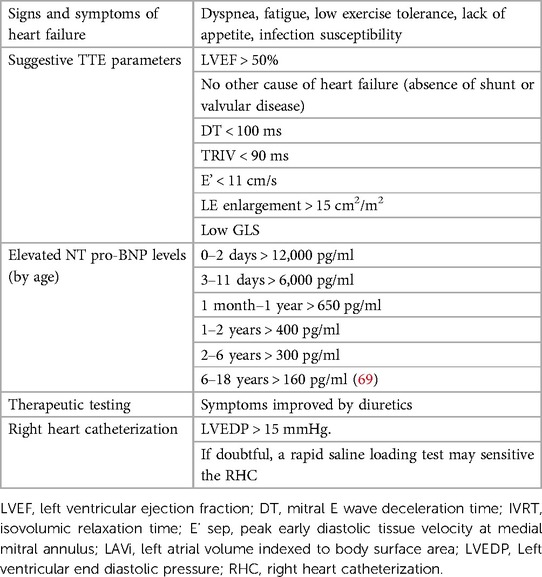
Table 1. Stepwise diagnosis approach for HFpEF in children.
Cardiac magnetic resonance imaging (CMRI) is a non-invasive imaging modality that can provide valuable information about the structure and function of the heart. By providing details about myocardial phenotype such as the localization of the myocardial hypertrophy (septal or apical) in HCM or the specific myocardial composition such as the presence of fibrosis, edema, fat, iron overload (by T2* imaging) in patients with hemochromatosis (70) CMRI is helpful to access the etiology of HFpEF. CMRI allows myocardial tissue characterization and fibrosis extension which makes it the modality of choice in diagnosing and following up cardiomyopathies. Indeed, the administration of intravenous gadolinium based contrast is the gold standard to locate and quantify the extension of the myocardial fibrosis (71). In the absence of focal LGE, T1 relaxation times and extracellular volume evaluation confirm the diagnosis of diffuse fibrosis (72). The extend of myocardial fibrosis estimated by late gadolinium enhancement (LGE) significantly correlates with the degree of diastolic dysfunction (25). Quantification of fibrosis, maximum wall thickness, and LV mass are markers of risk for sudden cardiac death that can be obtained by CMRI. Another important feature of CMRI is its ability to provide information on blood flow patterns in the heart. The analysis of LV filling velocity and volume flow, of the volumetric assessment of LV and of left atrium makes CMRI an highly accurate and reproducible noninvasive technique for the assessment of diastolic function (73). The wave intensity represents the energy flux per unit area that is carried by waves traveling in the cardiovascular network and derived from CMRI flow data (74). There are two main wave patterns during systole: the forward compression wave at systolic ejection (FCW) and the forward expansion wave (FEW) at end systole. The FCW/FEW ratio was significantly lower in patients suffering from HFpEF as peak FCW was lower in patients with LV diastolic dysfunction. CMRI is helpful in assessing graft function in pediatric heart transplant recipient (75).
The clinical course of children with diastolic dysfunction varies depending on the underlying cardiac condition. Global prognosis of HFpEF in children is uncertain especially since this term refers to a heterogeneous group of patients. There is limited literature on the prognosis of HFpEF in children beyond the phenotypes of HCM and RCM. No well-defined predictors exist for determining survival after diagnosis but it appears that RCM prognosis is grim due to the risk of sudden death and progression of pulmonary hypertension leading to early transplantation (76), younger age at diagnosis, repeated admissions for heart failure, diuretic use and isolated RCM phenotype are risk factors for death (76, 77). In the National Heart, Lung, and Blood Institute (NHLBI) Pediatric Cardiomyopathy Registry, children with RCM who had congestive heart failure and a lower fractional shortening Z score at diagnosis had the worst prognosis. The occurrence of LV diastolic dysfunction in patients with dilated cardiomyopathy is a marker of poor prognosis (29, 78) but there are no specific studies in children. Masutani et al. (11) compared the clinical course of 18 children suffering from HFpEF to 22 children suffering from HF with reduced EF (HFrEF) and observed that the heart failure mortality rate was significantly lower in the HFpEF than in the HFrEF patients (22% vs. 41%). Future works should focus on patients with isolated left ventricular diastolic dysfunction (and preserved ejection fraction) to define the pertinent predictor of outcome.
It is important for children with left ventricular diastolic dysfunction to receive timely and appropriate treatment to help prevent any long-term complications. To date, there is no pharmaceutical drug facilitating myocardial relaxation or improving ventricular compliance. Also, pharmaceutical treatment for HFpEF in children is extrapolated from adult clinical trials. Lifestyle management in children includes fighting against obesity and poor diet, blood pressure control and physical activity. Medical management strategies include diuretics to relieve symptoms of congestive heart failure. In adults' patients, the precise monitoring of the pulmonary pressures through a device, the CardioMEMS Heart Sensor, allows for efficient diuretic titration and has proven its benefit in reducing hospitalization for heart failure in patients suffering from HFpEF (79, 80). Beta Blockers may be useful as they increase diastolic duration by slowing down the heart rate (81). Spironolactone appears to improve prognosis in obese and diabetic adult patients suffering from HFpEF (15, 82) but these results are not transferable to pediatric patients. Angiotensin-converting enzyme inhibitors and sartans are prescribed with the intention to treat and prevent both systolic and diastolic dysfunction in the case of cardiomyopathies and after aortic coarctation repair but there is no evidence of efficacy of this treatment on the diastolic function. Empagliflozin and sacubitril/valsartan (83) have shown promising results in adults but data on children are not available yet. To date, no therapeutic trial has shown any benefit in treating patients suffering from HFpEF associated with PH with pulmonary arterial hypertension-approved therapies (84). In patients suffering from post-capillary PH and heart failure symptoms, the atrial flow regulator, an interatrial shunt device that recently became available proved to be efficient on symptoms and secure including in the pediatric population (85–87).
HFpEF is a rare and probably under-diagnosed condition in children. It can be caused by a variety of underlying conditions. Clinical presentation is not specific, and the diagnosis may be difficult. We proposed a diagnosis algorithm easy to use in clinical practice. Prognosis depends on the cause, but the appearance of associated hypertension marks a turning point in the evolution of the disease. Specific treatments are limited.
SQ: analysis and interpretation of the literature, writing original draft. DB: supervision, critical revision, validation of the final version of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CMRI, cardiac magnetic resonance imaging; CPH, combined postcapillary and precapillary pulmonary; FCW, forward compression wave; FEW, forward expansion wave; DT, mitral E wave deceleration time; HCM, hypertrophic cardiomyopathy; DCM, dilated cardiomyopathy; HFpEF, heart failure with preserved ejection fraction; IPH, isolated postcapillary pulmonary hypertension; IVRT, isovolumic relaxation time; LV, left ventricle; LVEDP, left ventricular end diastolic pressure; MISC, Multisystem Inflammatory Syndrome in Children; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PH, pulmonary hypertension; PVR, pulmonary vascular resistance; RCM, restrictive cardiomyopathy; TTE, transthoracic echocardiography.
1. Nagueh SF. Left ventricular diastolic function. JACC Cardiovasc Imaging. (2020) 13(1):228–44. doi: 10.1016/j.jcmg.2018.10.038
2. Fukuda N, Terui T, Ishiwata S, Kurihara S. Titin-based regulations of diastolic and systolic functions of mammalian cardiac muscle. J Mol Cell Cardiol. (2010) 48(5):876–81. doi: 10.1016/j.yjmcc.2009.11.013
3. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2022) 145(18):e895–1032. doi: 10.1161/CIR.0000000000001063Circulation
4. Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. (2017) 14(10):591–602. doi: 10.1038/nrcardio.2017.65
5. Nagueh SF. Heart failure with preserved ejection fraction: insights into diagnosis and pathophysiology. Cardiovasc Res. (2021) 117(4):999–1014. doi: 10.1093/cvr/cvaa228
6. Mishra S, Kass DA. Cellular and molecular pathobiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. (2021) 18(6):400–23. doi: 10.1038/s41569-020-00480-6
7. Gevaert AB, Boen JRA, Segers VF, Van Craenenbroeck EM. Heart failure with preserved ejection fraction: a review of cardiac and noncardiac pathophysiology. Front Physiol. (2019) 10:638. doi: 10.3389/fphys.2019.00638
8. Arques S, Quennelle F, Roux E. Accuracy of peak mitral e-wave velocity in the diagnosis of heart failure with preserved ejection fraction in older patients with acute dyspnea. Ann Cardiol Angeiol. (2021) 70(5):281–5. doi: 10.1016/j.ancard.2021.05.008
9. Das BB, Taylor AL, Yetman AT. Left ventricular diastolic dysfunction in children and young adults with marfan syndrome. Pediatr Cardiol. (2006) 27(2):256–8. doi: 10.1007/s00246-005-1139-5
10. Pan B, Hu D, Sun H, Lv T, Xu W, Tian J. Pediatric diastolic heart failure: clinical features description of 421 cases. Front Pediatr. (2022) 10:846408. doi: 10.3389/fped.2022.846408
11. Masutani S, Saiki H, Kurishima C, Ishido H, Tamura M, Senzaki H. Heart failure with preserved ejection fraction in children: hormonal imbalance between aldosterone and brain natriuretic peptide. Circ J. (2013) 77(9):2375–82. doi: 10.1253/circj.CJ-12-1271
12. Dragulescu A, Mertens L, Friedberg MK. Interpretation of left ventricular diastolic dysfunction in children with cardiomyopathy by echocardiography: problems and limitations. Circ Cardiovasc Imaging. (2013) 6(2):254–61. doi: 10.1161/CIRCIMAGING.112.000175
13. Nakamura M, Sadoshima J. Mechanisms of physiological and pathological cardiac hypertrophy. Nat Rev Cardiol. (2018) 15(7):387–407. doi: 10.1038/s41569-018-0007-y
14. Rapezzi C, Aimo A, Barison A, Emdin M, Porcari A, Linhart A, et al. Restrictive cardiomyopathy: definition and diagnosis. Eur Heart J. (2022) 43(45):4679–93. doi: 10.1093/eurheartj/ehac543
15. Cohen JB, Schrauben SJ, Zhao L, Basso MD, Cvijic ME, Li Z, et al. Clinical phenogroups in heart failure with preserved ejection fraction. JACC Heart Failure. (2020) 8(3):172–84. doi: 10.1016/j.jchf.2019.09.009
16. Zile MR, Baicu CF, Ikonomidis J, Stroud RE, Nietert PJ, Bradshaw AD, et al. Myocardial stiffness in patients with heart failure and a preserved ejection fraction: contributions of collagen and titin. Circulation. (2015) 131(14):1247–59. doi: 10.1161/CIRCULATIONAHA.114.013215
17. Murdoch CE. Endothelial NADPH oxidase-2 promotes interstitial cardiac fibrosis and diastolic dysfunction through proinflammatory effects and endothelial-mesenchymal transition. J Am Coll Cardiol. (2014) 63(24):8. doi: 10.1016/j.jacc.2014.02.572
18. Dusenbery SM, Jerosch-Herold M, Rickers C, Colan SD, Geva T, Newburger JW, et al. Myocardial extracellular remodeling is associated with ventricular diastolic dysfunction in children and young adults with congenital aortic stenosis. J Am Coll Cardiol. (2014) 63(17):1778–85. doi: 10.1016/j.jacc.2013.11.066
19. Gewillig M, Mertens L, Moerman P, Dumoulin M. Idiopathic restrictive cardiomyopathy in childhood: a diastolic disorder characterized by delayed relaxation. Eur Heart J. (1996) 17(9):1413–20. doi: 10.1093/oxfordjournals.eurheartj.a015076
20. Zarate YA, Hopkin RJ. Lysosomal storage disease 3 fabry’s disease. Lancet. (2008) 372(9647):1427–35. doi: 10.1016/S0140-6736(08)61589-5
21. Yang Z, McMahon CJ, Smith LR, Bersola J, Adesina AM, Breinholt JP, et al. Danon disease as an underrecognized cause of hypertrophic cardiomyopathy in children. Circulation. (2005) 112(11):1612–7. doi: 10.1161/CIRCULATIONAHA.105.546481
22. Murphy CJ, Oudit GY. Iron-overload cardiomyopathy: pathophysiology, diagnosis, and treatment. J Card Fail. (2010) 16(11):888–900. doi: 10.1016/j.cardfail.2010.05.009
23. Lombardi KC, Northrup V, McNamara RL, Sugeng L, Weismann CG. Aortic stiffness and left ventricular diastolic function in children following early repair of aortic coarctation. Am J Cardiol. (2013) 112(11):1828–33. doi: 10.1016/j.amjcard.2013.07.052
24. Florianczyk T, Werner B. Assessment of left ventricular diastolic function in children after successful repair of aortic coarctation. Clin Res Cardiol. (2011) 100(6):493–9. doi: 10.1007/s00392-010-0272-1
25. Moreo A, Ambrosio G, De Chiara B, Pu M, Tran T, Mauri F, et al. Influence of myocardial fibrosis on left ventricular diastolic function: non-invasive assessment by CMR and ECHO. Circ Cardiovasc Imaging. (2009) 2(6):437–43. doi: 10.1161/CIRCIMAGING.108.838367
26. Choudhry S, Puri K, Denfield SW. An update on pediatric cardiomyopathy. Curr Treat Options Cardio Med. (2019) 21(8):36. doi: 10.1007/s11936-019-0739-y
27. Knudson JD, Cabrera AG. The pathophysiology of heart failure in children: the basics. CCR. (2016) 12(2):99–103. doi: 10.2174/1573403X12666151119164525
28. Lipshultz SE, Law YM, Asante-Korang A, Austin ED, Dipchand AI, Everitt MD, et al. Cardiomyopathy in children: classification and diagnosis: a scientific statement from the American heart association. Circulation. (2019) 140(1):e9–e68 doi: 10.1161/CIR.0000000000000682
29. Reichart D, Magnussen C, Zeller T, Blankenberg S. Dilated cardiomyopathy: from epidemiologic to genetic phenotypes: a translational review of current literature. J Intern Med. (2019) 286(4):362–72. doi: 10.1111/joim.12944
30. Menon SC, Eidem BW, Dearani JA, Ommen SR, Ackerman MJ, Miller D. Diastolic dysfunction and its histopathological correlation in obstructive hypertrophic cardiomyopathy in children and adolescents. J Am Soc Echocardiogr. (2009) 22(12):1327–34. doi: 10.1016/j.echo.2009.08.014
31. Hershberger RE. Genetic evaluation of cardiomyopathy: a clinical practice resource of the American college of medical genetics and genomics (ACMG). Genet Med. (2018) 20(9):11. doi: 10.1038/s41436-018-0039-z
32. Minotti G, Reggiardo G, Camilli M, Salvatorelli E, Menna P. From cardiac anthracycline accumulation to real-life risk for early diastolic dysfunction. JACC CardioOncology. (2022) 4(1):139–40. doi: 10.1016/j.jaccao.2021.12.002
33. Dorup I, Levitt G, Sullivan I, Sorensen K. Prospective longitudinal assessment of late anthracycline cardiotoxicity after childhood cancer: the role of diastolic function. Heart. (2004) 90(10):1214–6. doi: 10.1136/hrt.2003.027516
34. Tede NH, Child JS. Diastolic dysfunction in patients with congenital heart disease. Cardiol Clin. (2000) 18(3):491–9. doi: 10.1016/S0733-8651(05)70157-0
35. Moskowitz WB, Schieken RM, Mosteller M, Bossano R. Altered systolic and diastolic function in children after “successful” repair of coarctation of the aorta. Am Heart J. (1990) 120(1):103–9. doi: 10.1016/0002-8703(90)90166-U
36. Shin JH, Choi HJ. Heart failure with preserved ejection fraction in children without congenital heart disease. J Cardiovasc Dis Diagn. (2018) S2:004. doi: 10.4172/2329-9517.S2-004
37. Selamet Tierney ES, Newburger JW, Graham D, Baker A, Fulton DR, Colan SD. Diastolic function in children with kawasaki disease. Int J Cardiol. (2011) 148(3):309–12. doi: 10.1016/j.ijcard.2009.11.014
38. Matsubara D, Kauffman HL, Wang Y, Calderon-Anyosa R, Nadaraj S, Elias MD, et al. Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J Am Coll Cardiol. (2020) 76(17):1947–61. doi: 10.1016/j.jacc.2020.08.056
39. Putzer GJB, Cooper D, Keehn C, Asante-Korang A, Boucek MM, Boucek RJ. An improved echocardiographic rejection-surveillance strategy following pediatric heart transplantation. J Heart Lung Transplant. (2000) 19(12):1166–74. doi: 10.1016/S1053-2498(00)00214-X
40. Asante-Korang A, Fickey M, Boucek MM, Boucek RJ. Diastolic performance assessed by tissue Doppler after pediatric heart transplantation. J Heart Lung Transplant. (2004) 23(7):865–72. doi: 10.1016/j.healun.2003.08.004
41. Ten Harkel ADJ, Cransberg K, Van Osch-Gevers M, Nauta J. Diastolic dysfunction in paediatric patients on peritoneal dialysis and after renal transplantation. Nephrol Dial Transplant. (2009) 24(6):1987–91. doi: 10.1093/ndt/gfp049
42. Schoenmaker NJ, Kuipers IM, van der Lee JH, Tromp WF, van Dyck M, Gewillig M, et al. Diastolic dysfunction measured by tissue Doppler imaging in children with end-stage renal disease: a report of the RICH-Q study. Cardiol Young. (2014) 24(2):236–44. doi: 10.1017/S1047951113000188
43. Mitsnefes MM. Cardiovascular disease in children with chronic kidney disease. J Am Soc Nephrol. (2012) 23(4):578–85. doi: 10.1681/ASN.2011111115
44. Mitsnefes MM, Kimball TR, Border WL, Witt SA, Glascock BJ, Khoury PR, et al. Impaired left ventricular diastolic function in children with chronic renal failure. Kidney Int. (2004) 65(4):1461–6. doi: 10.1111/j.1523-1755.2004.00525.x
45. Bartkowiak J, Spitzer E, Kurmann R, Zürcher F, Krähenmann P, Garcia-Ruiz V, et al. The impact of obesity on left ventricular hypertrophy and diastolic dysfunction in children and adolescents. Sci Rep. (2021) 11(1):13022. doi: 10.1038/s41598-021-92463-x
46. Saiedi SAE, Mira MF, Sharaf SA, Musaddar MMA, Kaffas RMHE, AbdelMassih AF, et al. Left ventricular diastolic dysfunction without left ventricular hypertrophy in obese children and adolescents: a tissue Doppler imaging and cardiac troponin I study. Cardiol Young. (2018) 28(1):76–84. doi: 10.1017/S1047951117001627
47. Kozák-Bárány A, Jokinen E, Kero P, Tuominen J, Rönnemaa T, Välimäki I. Impaired left ventricular diastolic function in newborn infants of mothers with pregestational or gestational diabetes with good glycemic control. Early Hum Dev. (2004) 77(1):13–22. doi: 10.1016/j.earlhumdev.2003.11.006
48. Mehta S, Nuamah I, Kalhan S. Altered diastolic function in asymptomatic infants of mothers with gestational diabetes. Diabetes. (1991) 40(Supplement_2):56–60. doi: 10.2337/diab.40.2.S56
49. Zablah JE, Gruber D, Stoffels G, Cabezas EG, Hayes DA. Subclinical decrease in myocardial function in asymptomatic infants of diabetic mothers: a tissue Doppler study. Pediatr Cardiol. (2017) 38(4):801–6. doi: 10.1007/s00246-017-1584-y
50. Guazzi M, Ghio S, Adir Y. Pulmonary hypertension in HFpEF and HFrEF: jACC review topic of the week. J Am Coll Cardiol. (2020) 76(9):1102–11. doi: 10.1016/j.jacc.2020.06.069
51. Galiè N, McLaughlin VV, Rubin LJ, Simonneau G. An overview of the 6th world symposium on pulmonary hypertension. Eur Respir J. (2019) 53(1):1802148. doi: 10.1183/13993003.02148-2018
52. Inampudi C, Silverman D, Simon MA, Leary PJ, Sharma K, Houston BA, et al. Pulmonary hypertension in the context of heart failure with preserved ejection fraction. Chest. (2021) 160(6):2232–46. doi: 10.1016/j.chest.2021.08.039
53. Røe ÅT, Aronsen JM, Skårdal K, Hamdani N, Linke WA, Danielsen HE, et al. Increased passive stiffness promotes diastolic dysfunction despite improved Ca2 + handling during left ventricular concentric hypertrophy. Cardiovasc Res. (2017) 113(10):1161–72. doi: 10.1093/cvr/cvx087
54. Inciardi RM, Rossi A, Bergamini C, Benfari G, Maffeis C, Greco C, et al. Mitral regurgitation, left atrial structural and functional remodelling and the effect on pulmonary haemodynamics. Eur J Heart Fail. (2020) 22(3):499–506. doi: 10.1002/ejhf.1677
55. Obokata M, Kane GC, Reddy YNV, Melenovsky V, Olson TP, Jarolim P, et al. The neurohormonal basis of pulmonary hypertension in heart failure with preserved ejection fraction. Eur Heart J. (2019) 40(45):3707–17. doi: 10.1093/eurheartj/ehz626
56. Ditaranto R, Caponetti AG, Ferrara V, Parisi V, Minnucci M, Chiti C, et al. Pediatric restrictive cardiomyopathies. Front Pediatr. (2022) 9:745365. doi: 10.3389/fped.2021.745365
57. Weller RJ, Weintraub R, Addonizio LJ, Chrisant MRK, Gersony WM, Hsu DT. Outcome of idiopathic restrictive cardiomyopathy in children. Am J Cardiol. (2002) 90(5):501–6. doi: 10.1016/S0002-9149(02)02522-5
58. Schlein J, Riebandt J, Laufer G, Zimpfer D. Reversal of pulmonary hypertension in paediatric patients with restrictive cardiomyopathy. Interact Cardiovasc Thorac Surg. (2021) 33(5):834–6. doi: 10.1093/icvts/ivab163
59. Fujimoto N, Borlaug BA, Lewis GD, Hastings JL, Shafer KM, Bhella PS, et al. Hemodynamic responses to rapid saline loading: the impact of age, sex, and heart failure. Circulation. (2013) 127(1):55–62. doi: 10.1161/CIRCULATIONAHA.112.111302
60. Reddy YNV, Carter RE, Obokata M, Redfield MM, Borlaug BA. A simple, evidence-based approach to help guide diagnosis of heart failure with preserved ejection fraction. Circulation. (2018) 138(9):861–70. doi: 10.1161/CIRCULATIONAHA.118.034646
61. Pieske B, Tschöpe C, de Boer RA, Fraser AG, Anker SD, Donal E, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the heart failure association (HFA) of the European society of cardiology (ESC). Eur Heart J. (2019) 40(40):3297–317. doi: 10.1093/eurheartj/ehz641
62. Recher M, Botte A, Baudelet JB, Leteurtre S, Godart F. Évaluation de la fonction diastolique du ventricule gauche en réanimation pédiatrique : quelles indications, quels paramètres mesurer? Levy B, Voicu S, editors. Méd Intensive Réa. (2019) 28(2):144–56. doi: 10.3166/rea-2019-0088
63. Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese society of echocardiography. J Am Soc Echocardiogr. (2011) 24(3):277–313. doi: 10.1016/j.echo.2011.01.015
64. Galderisi M, Cosyns B, Edvardsen T, Cardim N, Delgado V, Di Salvo G, et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: an expert consensus document of the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging. (2017) 18(12):1301–10. doi: 10.1093/ehjci/jex244
65. Eidem BW, McMahon CJ, Cohen RR, Wu J, Finkelshteyn I, Kovalchin JP, et al. Impact of cardiac growth on Doppler tissue imaging velocities: a study in healthy children. J Am Soc Echocardiogr. (2004) 17(3):212–21. doi: 10.1016/j.echo.2003.12.005
66. Sasaki N, Garcia M, Ko HH, Sharma S, Parness IA, Srivastava S. Applicability of published guidelines for assessment of left ventricular diastolic function in adults to children with restrictive cardiomyopathy: an observational study. Pediatr Cardiol. (2015) 36(2):386–92. doi: 10.1007/s00246-014-1018-z
67. McAree D, Hauck A, Arzu J, Carr M, Acevedo J, Patel AB, et al. Clinical predictors of subacute myocardial dysfunction in multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19. Pediatr Cardiol. (2022). 1–12. doi: 10.1007/s00246-022-03021-9. [Epub ahead of print].36260103
68. Cowie MR, Mendez GF. BNP And congestive heart failure. Prog Cardiovasc Dis. (2002) 44(4):293–321. doi: 10.1053/pcad.2002.24599
69. Nir A, Lindinger A, Rauh M, Bar-Oz B, Laer S, Schwachtgen L, et al. NT-Pro-B-type natriuretic peptide in infants and children: reference values based on combined data from four studies. Pediatr Cardiol. (2009) 30(1):3–8. doi: 10.1007/s00246-008-9258-4
70. Treibel TA, White SK, Moon JC. Myocardial tissue characterization: histological and pathophysiological correlation. Curr Cardiovasc Imaging Rep. (2014) 7(3):9254. doi: 10.1007/s12410-013-9254-9
71. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the society for cardiovascular magnetic resonance (SCMR) endorsed by the European association for cardiovascular imaging (EACVI). J Cardiovasc Magn Reson. (2017) 19(1):75. doi: 10.1186/s12968-017-0389-8
72. Rao S, Tseng SY, Pednekar A, Siddiqui S, Kocaoglu M, Fares M, et al. Myocardial parametric mapping by cardiac magnetic resonance imaging in pediatric cardiology and congenital heart disease. Circ Cardiovasc Imaging. (2022) 15(1):e012242. doi: 10.1161/CIRCIMAGING.120.012242
73. Paelinck BP, Lamb HJ, Bax JJ, Van der Wall EE, de Roos A. Assessment of diastolic function by cardiovascular magnetic resonance. Am Heart J. (2002) 144(2):198–205. doi: 10.1067/mhj.2002.123316
74. Ntsinjana HN, Chung R, Ciliberti P, Muthurangu V, Schievano S, Marek J, et al. Utility of cardiovascular magnetic resonance-derived wave intensity analysis as a marker of ventricular function in children with heart failure and normal ejection fraction. Front Pediatr. (2017) 5:65. doi: 10.3389/fped.2017.00065
75. Belay W, Godown J, Chan KC, Bearl DW, George-Durrett K, Slaughter JC, et al. Cardiac magnetic resonance diastolic indices correlate with ventricular filling pressures in pediatric heart transplant recipients. Pediatr Transplant. (2022):e14332. doi: 10.1111/petr.14332
76. Webber SA, Lipshultz SE, Sleeper LA, Lu M, Wilkinson JD, Addonizio LJ, et al. Outcomes of restrictive cardiomyopathy in childhood and the influence of phenotype: a report from the pediatric cardiomyopathy registry. Circulation. (2012) 126(10):1237–44. doi: 10.1161/CIRCULATIONAHA.112.104638
77. Wittekind SG, Ryan TD, Gao Z, Zafar F, Czosek RJ, Chin CW, et al. Contemporary outcomes of pediatric restrictive cardiomyopathy: a single-center experience. Pediatr Cardiol. (2019) 40(4):694–704. doi: 10.1007/s00246-018-2043-0
78. Dujardin KS, Tei C, Yeo TC, Hodge DO, Rossi A, Seward JB. Prognostic value of a Doppler index combining systolic and diastolic performance in idiopathic-dilated cardiomyopathy. Am J Cardiol. (1998) 82(9):1071–6. doi: 10.1016/S0002-9149(98)00559-1
79. Adamson PB, Abraham WT, Bourge RC, Costanzo MR, Hasan A, Yadav C, et al. Wireless pulmonary artery pressure monitoring guides management to reduce decompensation in heart failure with preserved ejection fraction. Circ Heart Fail. (2014) 7(6):935–44. doi: 10.1161/CIRCHEARTFAILURE.113.001229
80. Heywood JT, Jermyn R, Shavelle D, Abraham WT, Bhimaraj A, Bhatt K, et al. Impact of practice-based management of pulmonary artery pressures in 2000 patients implanted with the CardioMEMS sensor. Circulation. (2017) 135(16):1509–17. doi: 10.1161/CIRCULATIONAHA.116.026184
81. Rai P, Okhomina VI, Kang G, Akil N, Towbin JA, Hankins JS, et al. The effects of cardio-selective beta blockade on diastolic dysfunction in children with sickle cell disease. Haematol. (2022) 108(2):594–8. doi: 10.3324/haematol.2022.281428
82. Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. (2014) 370(15):1383–92. doi: 10.1056/NEJMoa1313731
83. Effect of Empagliflozin on Worsening Heart Failure Events in Patients With Heart Failure and Preserved Ejection Fraction: EMPEROR-Preserved Trial. Available at: https://www.ahajournals.org/doi/epub/10.1161/CIRCULATIONAHA.121.056824 (Cited July 6, 2022).
84. Vachiéry JL, Tedford RJ, Rosenkranz S, Palazzini M, Lang I, Guazzi M, et al. Pulmonary hypertension due to left heart disease. Eur Respir J. (2019) 53(1):1801897. doi: 10.1183/13993003.01897-2018
85. Paitazoglou C, Bergmann MW, Özdemir R, Pfister R, Bartunek J, Kilic T, et al. One-year results of the first-in-man study investigating the atrial flow regulator for left atrial shunting in symptomatic heart failure patients: the PRELIEVE study. Eur J Heart Fail. (2021) 23(5):800–10. doi: 10.1002/ejhf.2119
86. Paitazoglou C, Bergmann MW. The atrial flow regulator: current overview on technique and first experience. Ther Adv Cardiovasc Dis. (2020) 14:1753944720919577. doi: 10.1177/1753944720919577
Keywords: heart failure with preserved ejection fraction, diastolic heart failure, pediatric, child, cardiomyopathy, pulmonary hypertension
Citation: Quennelle S and Bonnet D (2023) Pediatric heart failure with preserved ejection fraction, a review. Front. Pediatr. 11:1137853. doi: 10.3389/fped.2023.1137853
Received: 4 January 2023; Accepted: 5 July 2023;
Published: 2 August 2023.
Edited by:
Giorgia Grutter, Bambino Gesù Children's Hospital (IRCCS), ItalyReviewed by:
Nancy Halnon,Mattel Children's Hospital and David Geffen School of Medicine at UCLA, United States© 2023 Quennelle and Bonnet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Quennelle Sophie sophie.quennelle@aphp.fr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.