
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Pediatr. , 02 June 2023
Sec. Pediatric Critical Care
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1127633
 Sara Malone1*
Sara Malone1* Jocelyn Rivera2
Jocelyn Rivera2 Maria Puerto-Torres3
Maria Puerto-Torres3 Kim Prewitt4
Kim Prewitt4 Firas Sakaan3
Firas Sakaan3 Lara Counts1
Lara Counts1 Zebin Al Zebin5Anita V. Arias3Parthasarathi Bhattacharyya6
Zebin Al Zebin5Anita V. Arias3Parthasarathi Bhattacharyya6 Sanjeeva Gunasekera7Sherry Johnson3Joyce Kambugu8
Sanjeeva Gunasekera7Sherry Johnson3Joyce Kambugu8 Erica C. Kaye3
Erica C. Kaye3 Belinda Mandrell3Jennifer W. Mack9
Belinda Mandrell3Jennifer W. Mack9 Jennifer McArthur3Alejandra Mendez10
Jennifer McArthur3Alejandra Mendez10 Lisa Morrissey9
Lisa Morrissey9 Rana Sharara-Chami11,12Jennifer Snaman9Elizabeth Sniderman13
Rana Sharara-Chami11,12Jennifer Snaman9Elizabeth Sniderman13 Douglas A. Luke4
Douglas A. Luke4 Dylan E. Graetz3
Dylan E. Graetz3 Asya Agulnik3
Asya Agulnik3
Background: As implementation science in global health continues to evolve, there is a need for valid and reliable measures that consider diverse linguistic and cultural contexts. A standardized, reproducible process for multilingual measure development may improve accessibility and validity by participants in global health settings. To address this need, we propose a rigorous methodology for multilingual measurement development. We use the example of a novel measure of multi-professional team communication quality, a determinant of implementation efforts.
Methods: The development and translation of this novel bilingual measure is comprised of seven steps. In this paper, we describe a measure developed in English and Spanish, however, this approach is not language specific. Participants are engaged throughout the process: first, an interprofessional panel of experts and second, through cognitive interviewing for measure refinement. The steps of measure development included: (1) literature review to identify previous measures of team communication; (2) development of an initial measure by the expert panel; (3) cognitive interviewing in a phased approach with the first language (English); (4): formal, forward-backward translation process with attention to colloquialisms and regional differences in languages; (5) cognitive interviewing repeated in the second language (Spanish); (6) language synthesis to refine both instruments and unify feedback; and (7) final review of the refined measure by the expert panel.
Results: A draft measure to assess quality of multi-professional team communication was developed in Spanish and English, consisting of 52 questions in 7 domains. This measure is now ready for psychometric testing.
Conclusions: This seven-step, rigorous process of multilingual measure development can be used in a variety of linguistic and resource settings. This method ensures development of valid and reliable tools to collect data from a wide range of participants, including those who have historically been excluded due to language barriers. Use of this method will increase both rigor and accessibility of measurement in implementation science and advance equity in research and practice.
Implementation science is becoming increasingly used in global health (1, 2). As a result, implementation research efforts must ask how current implementation science theories, measures, and models can, or cannot, be applied to global settings (2). For example, some frameworks, such as the Consolidated Framework for Implementation Research requires extension for application in low- and middle-income countries (3). There is a need to develop reliable and pragmatic measures of implementation determinants, processes, and outcomes that can be utilized across these diverse cultural and linguistic contexts.
Measurement of constructs and outcomes has been recognized as important for research in implementation science and to assist practitioners outside of the research context (4). Implementation measures are often developed for single studies and may lack rigorous evaluation to ensure reliability and validity (5, 6), limiting comparison between studies and resulting in multiple measures that have not been tested in different settings. Prior outlines of instrument development have not detailed the processes by which we should pay attention to cultural and linguistic needs within this process (7). Additionally, most measures have limited global applicability and are only useful in certain settings due to measure development in a high-income context. To advance implementation research, it is vital to construct measures that are pragmatic and valid in a variety of settings (4).
Similarly, few tools have been designed or evaluated for use in multiple languages. Existing multilingual measures have not been co-developed, but instead translated in multiple iterations without a standardized process. For example, three commonly used brief measures of implementation outcomes have been translated only after initial development and testing (8, 9). While this strategy is valid, it adds additional work and does not allow for either simultaneous refinement of both measures or up-front research in multiple linguistic settings. Translation without appropriate systematic consideration of linguistic and cultural differences can result in measures that are assessing different concepts, potentially limiting knowledge accumulation across global settings. Finally, translation after development of the initial instrument risks creation of an instrument that does not include all relevant constructs across different cultures. There is also currently no standard process to guide measure translation and reporting, which may have implications for measure quality.
To address current gaps in guidance for development of high-quality measures for use in research and practice, this paper does two things. First, we outline a 7-step method for multilingual measure development and subsequent translation. Second, we describe the use of this method through the development of a new measure that assesses the quality of multi-professional team communication in clinical settings.
This 7-step method allows for rigorous development of new measures that are useful in a variety of contexts and have linguistic validity (10, 11), which should then be refined through psychometric testing. This method has two main benefits for the field of implementation science: first, it allows for research in multiple settings that do not share a primary language, and second, it helps develop consistent and clear definitions for implementation science constructs. Ultimately, this approach allows constructs to be compared across studies and settings. Additionally, this paper provides guidance for measure translation, which represents best practices even for measures that are not being co-developed.
The measure described in this study was developed to assess multi-professional communication quality within the context of pediatric oncology. Hospitalized pediatric oncology patients are at high risk of clinical deterioration (12, 13) and require excellent interdisciplinary communication to provide high-quality care. During clinical patient deteriorations, team members must alert one another to concerns, come together to consider etiologies and strategize about medical interventions, and then implement interventions, all in a coordinated and rapid manner. Previous studies have reported that effective interdisciplinary communication is a fundamental component of quality care and a priority to improve outcomes in pediatric oncology (14) and intensive care (15–17). Effective communication between clinical teams improves clinical outcomes of hospitalized patients (18), whereas lack of effective team communication contributes to a delayed response to critically ill patients (19, 20). Additionally, multi-professional team communication and processes have been identified as important determinants of implementation and sustainment of evidence-based care (3, 21, 22).
Multiple studies have demonstrated the importance of high-quality interdisciplinary communication in childhood cancer care globally, where hospitals face variability in resources to provide acute medical care– specifically, staff, equipment, and systems of care (23). However, there is currently no reliable and validated measure of the quality of interdisciplinary (different medical specialties) and multi-professional (different professions, like nurses and physicians) communication applicable to clinical settings of variable resource-levels. While there is a clear need for effective interventions to optimize interdisciplinary communication to improve patient care (24, 25), lack of reliable and valid assessment tools makes development and evaluation of such interventions challenging, especially across different practice settings. There is an urgent need for a measurement tool that provides a reliable assessment of communication and collaboration quality in clinical settings to improve patient care globally (25).
To develop CritCom, an expert panel was assembled, including 21 experts from 9 countries with expertise in pediatric oncology medicine, critical care medicine, interdisciplinary communication, and measure development. These individuals represented different disciplines associated with critical care communication, global regions, economic and cultural backgrounds (Table 1). Panelists assisted with the development and refinement of the CritCom measure based on the literature research and their expertise in measurement, clinical care, and/or communication. This process was conducted in English and Spanish. While this could be conducted in any language, these two were selected because of its relationship to our previous work primarily focused in Latin America (14, 26).
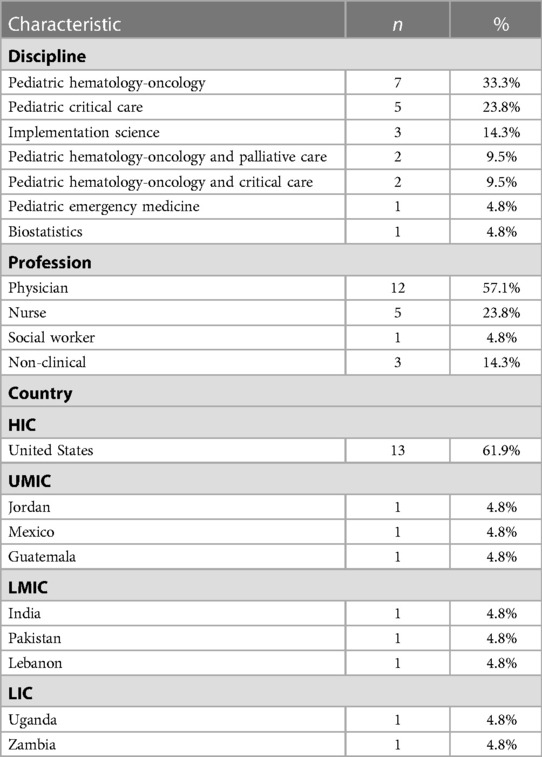
Table 1. Expert panel demographics (n = 21).
After an initial measure was drafted, cognitive interviews (detailed below) were conducted in both English and Spanish. Participants were recruited via an email to a wide network of global health workers to voluntarily participate in virtual interviews to analyze the preliminary survey, emphasizing its objective related to interdisciplinary communication. Thirty-six individuals from 15 countries participated in cognitive interviews. These individuals were clinicians in Pediatric Oncology or Critical Care Medicine and included both nurses and physicians practicing in hospitals with a variety of resource-levels (Table 2).
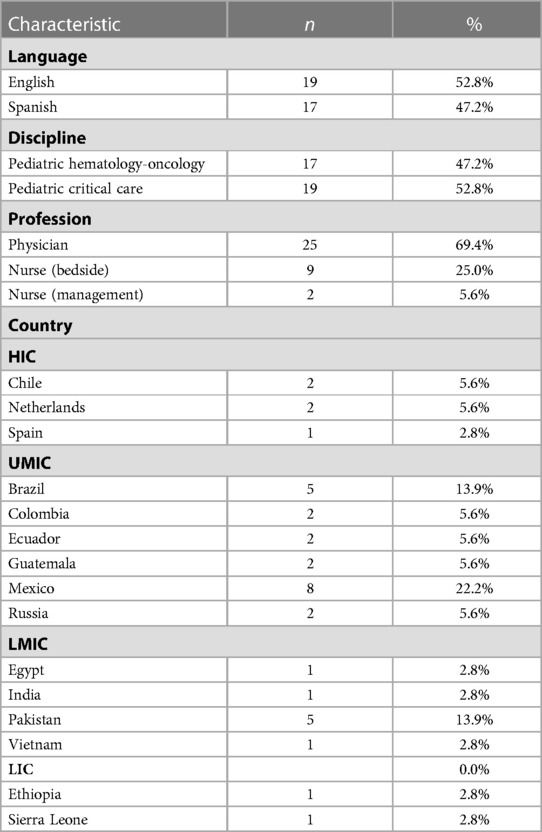
Table 2. Demographics for cognitive interviews (n = 36).
Below are the seven steps we recommend for multilingual measurement development (Figure 1). Additionally, we describe how these steps were operationalized for CritCom measurement development.
Step 1: literature review
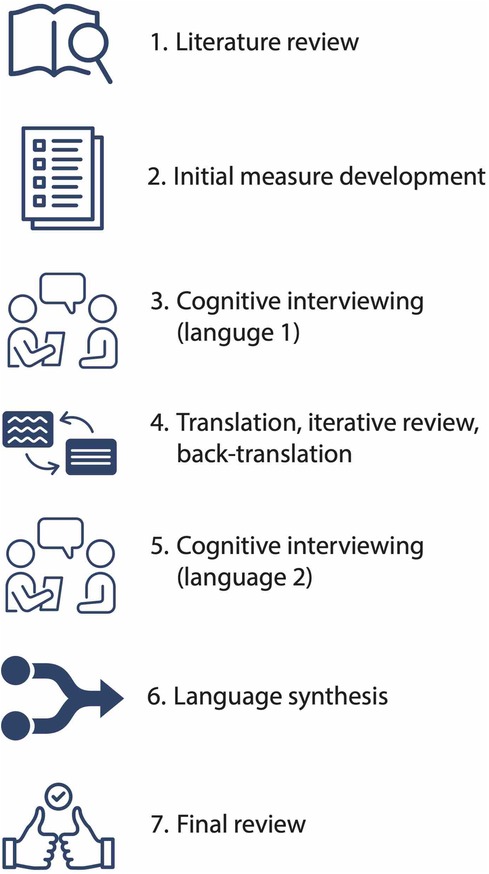
Figure 1. Seven step process for bilingual measurement development methods.
A thorough literature review can help ensure that there is a need for a new measurement tool by offering a comprehensive understanding of what is available in a specific area. Additionally, a comprehensive and systematic literature review can be used for preliminary item identification.
To develop CritCom, we conducted a literature search to identify existing tools assessing teamwork and communication, focusing on quantitative measurement articles. The concepts were searched using the keywords “interdisciplinary communication,” “interprofessional communication,” “nurse-doctor communication,” “evaluation of teamwork,” and “communication in critical care.” This literature search failed to identify a single measure of quality of interdisciplinary communication around patient deterioration; however, it identified multiple studies that informed our subsequent measure development process (Table 3). Measurement tools identified by this search were used to build a database of question items and domains which were reviewed by the expert panel to verify that they address all relevant aspects of team communication.
Step 2: initial measure development
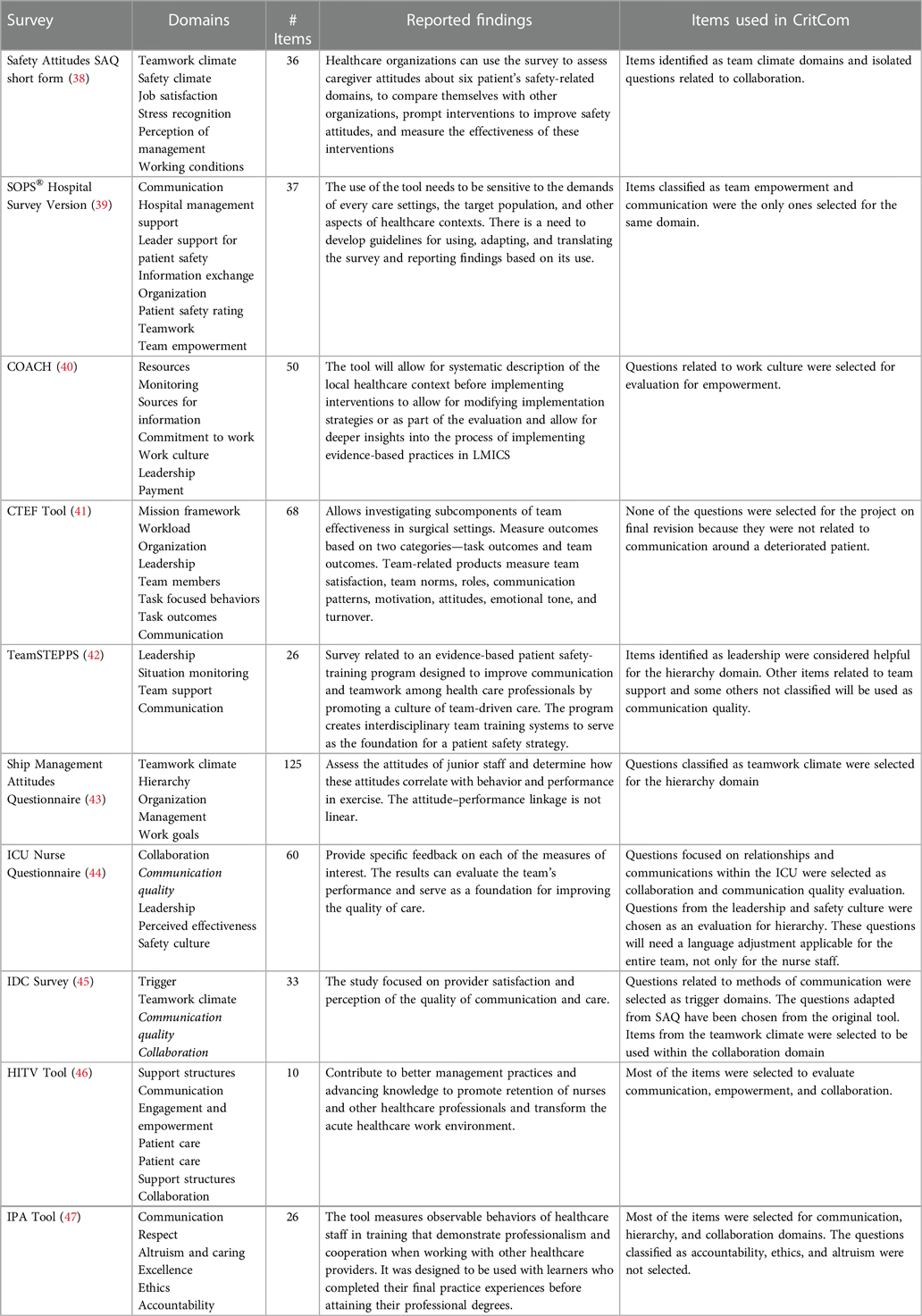
Table 3. Existing tools and domains.
The literature review in step 1 serves to identify if there is prior work that can inform measure development. If so, these existing measures can be incorporated as appropriate. However, for content areas where there is no prior work, other strategies should be considered for rigorous measurement development. For example, concept mapping has been used as a valid strategy for item and domain generation (27).
To draft the initial CritCom measure, the expert panel participated in a series of working meetings to identify and define independent domains of interprofessional communication quality. They then reviewed all question items that had been extracted during literature review of existing published tools and mapped these to the identified domains. This was done through group discussion and electronic survey to reach consensus. Because of the extent of prior work and already established items identified during literature review, concept mapping was not used to draft items for this measure. The survey asked individuals to rate each potential survey item on importance and clarity. Following this, the expert panel met and reviewed the results, choosing the items that were rated as the most important and clear to include in the initial measure. Items were removed for a variety of reasons including concerns about clarity, importance, and to delete duplicate concepts. Ultimately, this process resulted in a draft measure that underwent iterative rounds of review by listed collaborators to ensure both content validity and cultural sensitivity.
Step 3: cognitive interviewing (first instrument language-English)
Cognitive interviewing is an established method to assist with identification of problematic survey items while establishing face validity (28). Participants are asked to both complete the draft measure and answer questions about how they interpreted items, what they found difficult to answer, and what concepts they think the items are capturing (29). Cognitive interviewing is typically done via semi-structured interviews with a representative sample of future users of the tool.
Since the goal of developing CritCom was to administer it in English and Spanish, we first completed cognitive interviewing in English, followed by translation, then repeated the same process in Spanish (see Step 5). We consider this a best practice for two reasons: first, this ensures clarity in both languages and second, this reduces the potential for conflicting edits between languages. For our English-language cognitive interviewing, the sampled target participants included English-speaking intensive care unit and ward nurses and physicians from centers located in different countries and various resource levels.
A standard semi structured cognitive interview guide was developed (Supplementary Material S1) and updated with each round of interviewing. These interviews were virtually conducted over Zoom (by SM, KP, JR) with audio and cameras enabled to facilitate the interview. This allowed for better simulation of in-person interviews and improved communication. Participants were interviewed in phases of 3–5 interviews at a time, after which the core team (JR, SM, AsA, MPT, KP) met to adjust both the measure and the interview guide. Feedback by participants was used to adjust CritCom wording to optimize clarity and ensure appropriate comprehension of each survey item. A total of 19 English-speaking participants from 9 countries were interviewed (Table 2). This included native and non-native English speakers, as we anticipated that many participants taking the survey in English would not be native English speakers. This process allowed for iterative revisions of the measure to ensure comprehension and face validity. Interviews were stopped when no further changes were needed for the English version of the initial items.
Step 4: translation
A formal, thorough translation process is needed for measures intended to be delivered in multiple languages. Using forward-backward translation is a standard approach (30). This process involves translation to the second language, and then translation back to the original language by a different individual or group to compare with the original version. However, even within languages there are regional and dialect differences impacting the interpretation of survey items across and within different countries and regions. Appropriate attention must be paid to these differences and their potential implications for item interpretation and construct definitions. To best address these, our method emphasizes using translators with different dialects from different regions speaking the same language, and then reconciling language differences to achieve linguistic validity.
In our study, survey questions were first translated from English to Spanish through a professional translation company, then iteratively reviewed by five bilingual members of the research team (JR, MPT, HMT, AnA, AsA) from five different countries (Mexico, Puerto Rico, Chile, Colombia, USA). Collaborators reviewed the translation for colloquial syntax, comprehension, cultural relevance, and questions were modified as needed to enhance cultural and linguistic validity. This process allowed the team to account for regional differences and resolve them in a way that was most generalizable to all Spanish speakers regardless of origin.
Developing conceptually equivalent surveys is challenging. We faced challenges related to regionalism, education background, preferences for more or less formal phrases, and English words/terms for which there is no exact Spanish equivalent (e.g., “speak up” and “actionable”). We selected the final translations to maximize: (i) the consistency of the Spanish translation with the intent of the English version; (ii) clarity; and (iii) similarities in understanding between regions (31).
Step 5: cognitive interviewing (second instrument language-spanish)
As described above, cognitive interviewing ensures that the measure is understandable to participants in each language. This must be done in every language to identify items that may be problematic in that language. These steps should be repeated as necessary for all desired language-versions for measure co-development.
A second round of cognitive interviewing was repeated using the Spanish version of CritCom with native Spanish-speaking participants, using a similar process as described in Step 3. The English-language cognitive interview script was translated into Spanish using a similar process as described above; specific questions were added to target survey items that were challenging to translate in Step 4. Bilingual, native Spanish speaking members of the research team (JR, MPT) conducted cognitive interviews with participants from 6 Spanish-speaking countries from Mexico, Central and South America, representing the same target participant demographic as Step 3. Interviews were stopped after 17 participants, when saturation was reached and no further changes were recommended. Like in Step 3, interviews were conducted in phases. After each round of 3–5 interviews, the core team met (JR, SM, AsA, MPT, KP) to review feedback and edit the tool as needed. When change was made to the measure, back-translation to English was done to ensure that the intent of the questions remained intact. Input on this process was provided by native Spanish and English speakers to ensure that final questions were appropriate in both languages.
Step 6. Language Synthesis
A final review of the items must be completed to confirm that the items are still the same across languages. A unique benefit of this co-design process is the ability to use the second language (Spanish) to confirm face validity and further refine the original English language measure.
Translation to and cognitive interviewing with the Spanish-language measure identified additional wording that was unclear in the English tool and both measures were adjusted based on feedback (e.g., speak up vs. “alzar la voz”; speak up is translated as “raise your voice” in Spanish, which is not the intended meaning and would represent a completely different interpretation). This opportunity for synthesis between feedback derived from evaluating both language-versions is a unique benefit of co-development of multilingual measures.
Step 7: final review
Following the described structured method for development including cognitive interviewing and synthesis of feedback, the bilingual measure confirmed content, face, and linguistic validity. In a final step, the English and Spanish versions of the instrument were reviewed by the entire expert panel. No further edits were made to the instrument at this step; this review served as a final confirmation that the two versions were identical, clear to all individuals, and achieved the initial objectives for this measure. To ensure measure reliability and validity, further psychometric testing is required. However, this provides a rigorously developed draft measure for pilot testing.
Figure 2 presents the steps as used for CritCom with a timeline for the process and Figure 3 highlights how questions were added and dropped from the measure at each step.
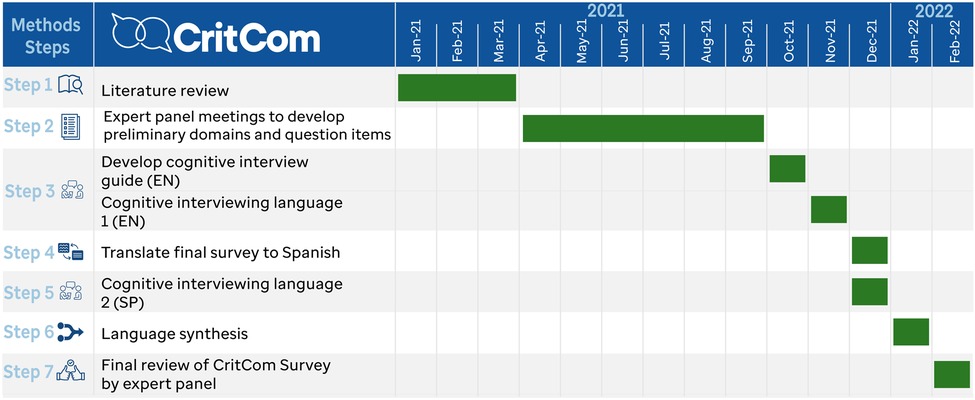
Figure 2. Timeline for CritCom development.

Figure 3. Flow diagram of CritCom items.
The literature review (Step 1) resulted in 421 questions from 10 unique previously developed measures in related areas. After initial review by the expert panel (Step 2), 105 questions related to relevant domains of interprofessional communication were selected. Expert panel members were asked to identify the most important and clear items for the assessment, resulting in 59 items that were further reviewed for importance and clarity. After removing low-rated items, the draft instrument had 52 items across 7 domains (Table 4). The domains highlight the content of communication, the style in which it was delivered, and aspects about the team and organizational context that promote or hinder high quality communication. The items were all phrased to inquire, on a Likert scale from almost never to almost always, a clinician's perception of different aspects of communication in their unit. For example, one item under actionable communication asked if during shift changes, staff exchange all essential patient information.”
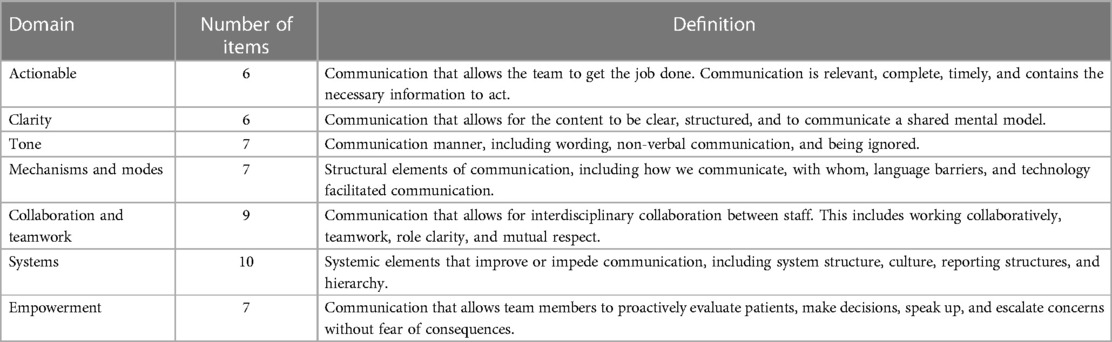
Table 4. Selected preliminary domains and definitions.
A total of 36 English and Spanish-speaking individuals from 15 countries were interviewed during this process (Table 2). This included 25 doctors and 11 nurses from both Pediatric Hematology-Oncology and Critical Care programs. Cognitive interviews were conducted in rounds, where 2–4 individuals were interviewed prior to the research team reviewing interview notes and making edits to the tool. The English interviews were conducted in 8 rounds, with edits made after each round except the last. The Spanish interviews were conducted in 5 rounds, with edits being made in a similar fashion. All interviews were conducted in individual's native language and were recorded on Zoom, with interviews lasting 15–60 min. Participants were able to identify language and content changes needed to improve the measure (Table 5). As described above, following the Spanish cognitive interviews, feedback in both languages was synthesized (Step 6).
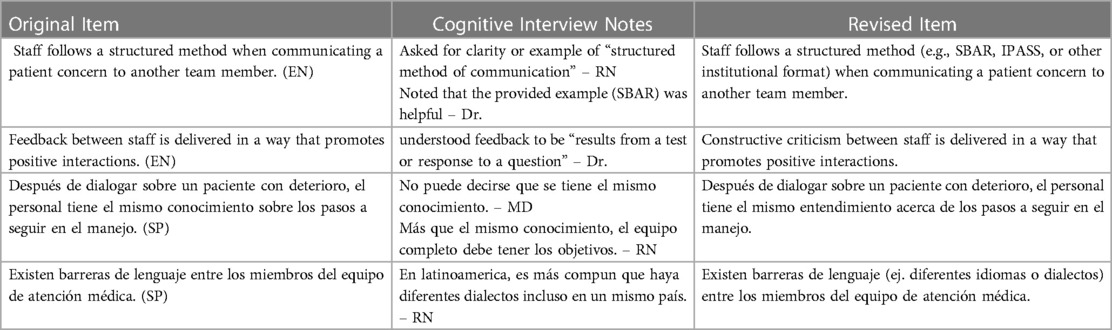
Table 5. Examples of items refined during cognitive interview process.
After the final round of cognitive interviewing and language synthesis, the measure had 52 items across 7 domains in the draft CritCom instrument. This measure was reviewed by the expert panel (Step 7) resulting in no further changes. This resulted in a measure with content, face, and linguistic validity to evaluate aspects of quality communication among healthcare professionals from the perspective of in both English and Spanish speaking individuals practicing in hospitals with a range of resource-levels. This measure is now ready to pilot to remove poor performing items and evaluate the proposed domain structure through psychometric testing.
This paper details a novel method for simultaneous measurement co-development in multiple languages, resulting in a draft measure that has content, face, and linguistic validity. We accomplished this through engagement of interdisciplinary, multi-professional experts in clinical care, measurement development, and communication. The 7-step process described is both rigorous and inclusive while maintaining efficiency, and it advances measurement development in two important ways. First, this method ensures that created measures have strong face and linguistic validity and that they are pragmatic for researchers and practitioners in a variety of practices and linguistic settings. Second, this method addresses concerns of health equity in implementation science (32, 33) by facilitating development of multilingual measures that can be utilized across a variety of participant populations, including those who have been previously excluded due to language barriers.
Measure development using this method requires broad considerations about the target populations and settings. To assure linguistic validity, special considerations must be given to the variety of dialects and regional variation that may influence the translation and comprehension of the new measure. Additionally, phrasing of related components that may be difficult to interpret for participants answering the survey in a non-native language (as is common in global health research), such as the instructions, must be considered. Finally, measures that are intended for a variety of audiences must consider the literacy levels and experiences of all individuals who may complete the measure. These challenges are best assessed through cognitive interviewing that is inclusive and comprehensive of the target participant population discipline, profession, and language (34–36). Measure development without these considerations can have potential problems, including inaccurate measurement of a construct and systematic misrepresentation of specific participant groups.
This process, while useful, also has a few challenges that must be considered. The proposed method requires a multilingual team, including individuals from different regional settings. To conduct the cognitive interviews, it is necessary to engage a network of willing participants, which can only be fostered through appropriate community engagement in research. Intentional engagement is especially important for expanding implementation science in a global health context and emphasizing inclusion beyond individuals in high income countries (1). Committing to this process is also relatively time intensive, which means that it must be planned for and considered well before a final measure is needed.
Even after considering these challenges, we believe there are several best practices described in this 7-step process that promote rigorous methodology for measurement development in implementation science. First, translation, review, and back-translation should be conducted by multiple bilingual native speakers to reconcile regional differences in phrasing and context. Additionally, cognitive interviewing should be conducted serially and prior to pilot testing a new measure. This allows improvements in any language to be incorporated before any psychometric testing. Additionally, this process allows for problematic items to be identified and improved in all versions of the measure, with each language informing the others. Discussions about cultural adaptation occur during this process, thereby avoiding the need for multiple future revisions (37). The synthesis step used to align feedback between languages facilitates development of a more robust and useful measure due to the need to clearly articulate concepts in both languages. Components of the co-development process can also be applied for rigorous translation of existing measures, for which standardized guidance does not exist in the literature.
Following the process described, the CritCom measure will undergo psychometric testing, focusing on evaluating the 7-domain structure and shortening through removal of poorly performing items via reliability assessment and confirmatory factor analysis. This will be done through administering the survey to a group of participants, collecting data, and conducting quantitate analyses concurrently in English and Spanish. Ultimately, this process will result in a measure that can reliably and validly assess the quality of interprofessional communication with a focus on pediatric cancer settings. We expect CritCom to be ultimately used in future research to understand how team communication is implicated in the system of healthcare delivery, both as a determinant for implementation and sustainability and as an outcome to measure the impact of interventions on team communication within complex clinical systems.
We described a 7-step stakeholder-engaged process which results in the development of measures with content, face, and linguistic validity and allows researchers and practitioners to measure clearly articulated and defined constructs in multiple languages. This methodology can inform the development of a broad range of measures, responding to concerns regarding the need for more rigorous measure development in implementation science. This work also responds to an important need in global health for tools that can be administered in multilingual contexts. Finally, this approach highlights how measures can be pragmatically developed for use across a wide range of settings, promoting inclusivity and equity in implementation science.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants was not required to participate in this study in accordance with the national legislation and the institutional requirements.
SM, JR, MP, KP, DL, DG, AsA participated in design of the work. SM, JR, MPT, KP, FS participated in data collection. LC participated in editing, formatting, and reference management. ZAZ, AnA, PB, SG, SJ, JK, EK, BM, JMa, JMc, AM, LM, RS, JS, ES participated in on the expert panel, assisted with measurement design, and reviewed all work products. MP, AnA, JR, AsA assisted with translation and review of multilingual documents. SM, JR, MP, KP, AsA collaborated in drafting the manuscript. All authors contributed to the article and approved the submitted version.
This project was supported in part by the St. Jude-Washington University in St. Louis joint implementation sciences collaboration, the National Cancer Institute (P50CA244431), and the American Lebanese Syrian Associated Charities (ALSAC/St. Jude Children's Research Hospital). The findings and conclusions in this paper are those of the authors and do not necessarily represent the official positions of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We would like to acknowledge all the help of everyone who participated on our expert panel and cognitive interviewing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1127633/full#supplementary-material.
1. Bartels SM, Haider S, Williams CR, Mazumder Y, Ibisomi L, Alonge O, et al. Diversifying implementation science: a global perspective. Glob Health Sci Pract. (2022) 10:e2100757. doi: 10.9745/GHSP-D-21-00757
2. Alonge O, Rodriguez DC, Brandes N, Geng E, Reveiz L, Peters DH. How is implementation research applied to advance health in low-income and middle-income countries? BMJ Glob Health. (2019) 4:e001257. doi: 10.1136/BMJGH-2018-001257
3. Means AR, Kemp CG, Gwayi-Chore MC, Gimbel S, Soi C, Sherr K, et al. Evaluating and optimizing the consolidated framework for implementation research (CFIR) for use in low- and middle-income countries: a systematic review. Implement Sci. (2020) 15:1–19. doi: 10.1186/S13012-020-0977-0/TABLES/3
4. Lewis CC, Mettert KD, Stanick CF, Halko HM, Nolen EA, Powell BJ, et al. The psychometric and pragmatic evidence rating scale (PAPERS) for measure development and evaluation. Implement Res Pract. (2021) 2:263348952110373. doi: 10.1177/26334895211037391
5. Rabin BA, Purcell P, Naveed S, Moser RP, Henton MD, Proctor EK, et al. Advancing the application, quality and harmonization of implementation science measures. Implement Sci. (2012) 7:1–11. doi: 10.1186/1748-5908-7-119/TABLES/2
6. Lewis CC, Weiner BJ, Stanick C, Fischer SM. Advancing implementation science through measure development and evaluation: a study protocol. Implement Sci. (2015) 10:1–10. doi: 10.1186/S13012-015-0287-0/FIGURES/2
7. Martinez RG, Lewis CC, Weiner BJ. Instrumentation issues in implementation science. Implement Sci. (2014) 9:1–9. doi: 10.1186/S13012-014-0118-8/TABLES/1
8. Weiner BJ, Lewis CC, Stanick C, Powell BJ, Dorsey CN, Clary AS, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. (2017) 12:1–12. doi: 10.1186/S13012-017-0635-3/TABLES/3
9. Kien C, Griebler U, Schultes M-T, Thaler KJ, Stamm T. Psychometric testing of the German versions of three implementation outcome measures. Glob Implement Res Appl. (2021) 1(3):183–94. doi: 10.1007/S43477-021-00019-Y
10. Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. (2005) 8:94–104. doi: 10.1111/J.1524-4733.2005.04054.X
11. Huang YP, Chen B, Ping P, Wang HX, Hu K, Zhang T, et al. The premature ejaculation diagnostic tool (PEDT): linguistic validity of the Chinese version. J Sex Med. (2014) 11:2232–8. doi: 10.1111/JSM.12612
12. Ceppi F, Antillon F, Pacheco C, Sullivan CE, Lam CG, Howard SC, et al. Supportive medical care for children with acute lymphoblastic leukemia in low- and middle-income countries. Expert Rev Hematol. (2015) 8:613–26. doi: 10.1586/17474086.2015.1049594
13. Agulnik A, Méndez Aceituno A, Mora Robles LN, Forbes PW, Soberanis Vasquez DJ, Mack R, et al. Validation of a pediatric early warning system for hospitalized pediatric oncology patients in a resource-limited setting. Cancer. (2017) 123:4903–13. doi: 10.1002/CNCR.30951
14. Graetz D, Kaye EC, Garza M, Ferrara G, Rodriguez M, Soberanis Vásquez DJ, et al. Qualitative study of pediatric early warning systems’ impact on interdisciplinary communication in two pediatric oncology hospitals with varying resources. JCO Glob Oncol. (2020) 6:1079–86. doi: 10.1200/GO.20.00163
15. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anesthesiology Scandinavica. (2008) 53:143–51. doi: 10.1111/j.1399-6576.2008.01717.x
16. Reader TW, Flin R, Mearns K, Cuthbertson BH. Developing a team performance framework for the intensive care unit. Crit Care Med. (2009) 37:1787–93. doi: 10.1097/CCM.0B013E31819F0451
17. Reader TW, Flin R, Mearns K, Cuthbertson BH. Interdisciplinary communication in the intensive care unit. Br J Anaesth. (2007) 98:347–52. doi: 10.1093/BJA/AEL372
18. Carron T, Rawlinson C, Arditi C, Cohidon C, Hong QN, Pluye P, et al. An overview of reviews on interprofessional collaboration in primary care: effectiveness. Int J Integr Care. (2021) 21:31. doi: 10.5334/ijic.5588
19. Gluyas H. Effective communication and teamwork promotes patient safety. Nurs Stand. (2015) 29:50–7. doi: 10.7748/ns.29.49.50.e10042
20. Sridhar S, Schmid A, Biziyaremye F, Hodge S, Patient N, Wilson K. Implementation of a pediatric early warning score to improve communication and nursing empowerment in a rural district hospital in Rwanda. Glob Health Sci Pract. (2020) 8:838–45. doi: 10.9745/GHSP-D-20-00075
21. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:1–15. doi: 10.1186/1748-5908-4-50/TABLES/1
22. Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. (2013) 8:1–11. doi: 10.1186/1748-5908-8-35/TABLES/1
23. Muttalib F, González-Dambrauskas S, Lee JH, Steere M, Agulnik A, Murthy S, et al. Pediatric emergency and critical care resources and infrastructure in resource-limited settings: a multicountry survey. Crit Care Med. (2021) 49:671–81. doi: 10.1097/CCM.0000000000004769
24. Hailu FB, Worku Kassahun C, Woldie Kerie M. Perceived nurse—physician communication in patient care and associated factors in public hospitals of jimma zone, south west Ethiopia: cross sectional study. PLoS One. (2016) 11. doi: 10.1371/JOURNAL.PONE.0162264
25. Busari JO, Moll FM, Duits AJ. Understanding the impact of interprofessional collaboration on the quality of care: a case report from a small-scale resource limited health care environment. J Multidiscip Healthc. (2017) 10:227. doi: 10.2147/JMDH.S140042
26. Agulnik A, Gonzalez Ruiz A, Muniz-Talavera H, Carrillo AK, Cárdenas A, Puerto-Torres MF, et al. Model for regional collaboration: successful strategy to implement a pediatric early warning system in 36 pediatric oncology centers in Latin America. Cancer. (2022) 128:4004–16. doi: 10.1002/CNCR.34427
27. Malone S, Prewitt K, Hackett R, Lin JC, McKay V, Walsh-Bailey C, et al. The clinical sustainability assessment tool: measuring organizational capacity to promote sustainability in healthcare. Implement Sci Commun. (2021) 2:77. doi: 10.1186/S43058-021-00181-2
28. Peterson CH, Peterson NA, Powell KG. Cognitive interviewing for item development: validity evidence based on content and response processes. Meas Eval Couns Dev. (2017) 50:217–23. doi: 10.1080/07481756.2017.1339564
29. Miller K, Mont D, Maitland A, Altman B, Madans J. Results of a cross-national structured cognitive interviewing protocol to test measures of disability. Qual Quant. (2011) 45:801–15. doi: 10.1007/S11135-010-9370-4
30. Koller M, Kantzer V, Mear I, Zarzar K, Martin M, Greimel E, et al. The process of reconciliation: evaluation of guidelines for translating quality-of-life questionnaires. Expert Rev Pharmacoecon Outcomes Res. (2012) 12:189–97. doi: 10.1586/ERP.11.102
31. Kwan CM, Napoles AM, Chou J, Seligman HK. Development of a conceptually equivalent Chinese-language translation of the US household food security survey module for Chinese immigrants to the USA. Public Health Nutr. (2014) 18:242–50. doi: 10.1017/S1368980014000160
32. Shelton RC, Adsul P, Oh A. Recommendations for addressing structural racism in implementation science: a call to the field. Ethn Dis. (2021) 31:357–64. doi: 10.18865/ED.31.S1.357
33. Brownson RC, Kumanyika SK, Kreuter MW, Haire-Joshu D. Implementation science should give higher priority to health equity. Implement Sci. (2021) 16(1):1–16. doi: 10.1186/S13012-021-01097-0
34. Willis GB, Miller K. Cross-cultural cognitive interviewing: seeking comparability and enhancing understanding. Field Methods. (2011) 23:331–41. doi: 10.1177/1525822X11416092
35. García AA. Cognitive interviews to test and refine questionnaires. Public Health Nurs. (2011) 28:444–50. doi: 10.1111/J.1525-1446.2010.00938.X
36. Irwin DE, Varni JW, Yeatts K, DeWalt DA. Cognitive interviewing methodology in the development of a pediatric item bank: a patient reported outcomes measurement information system (PROMIS) study. Health Qual Life Outcomes. (2009) 7:3. doi: 10.1186/1477-7525-7-3
37. Baumann AA, Cabassa LJ. Reframing implementation science to address inequities in healthcare delivery. BMC Health Serv Res. (2020) 20:1–9. doi: 10.1186/S12913-020-4975-3/TABLES/1
38. Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. (2006) 6:44. doi: 10.1186/1472-6963-6-44
39. Waterson P, Carman E-M, Manser T, Hammer A. Hospital survey on patient safety culture (HSPSC): a systematic review of the psychometric properties of 62 international studies. BMJ Open. (2019) 9:e026896. doi: 10.1136/bmjopen-2018-026896
40. Bergström A, Skeen S, Duc DM, Blandon EZ, Estabrooks C, Gustavsson P, et al. Health system context and implementation of evidence-based practices-development and validation of the context assessment for community health (COACH) tool for low- and middle-income settings. Implement Sci. (2015) 10:120. doi: 10.1186/s13012-015-0305-2
41. Essens P, Vogelaar A, Mylle J, Blendell C, Paris C, Halpin S, et al. Military command team effectiveness: Model and instrument for assessment and improvement (L’efficacite des Equipes de Commandement Militaires: un Modele et un Instrument Pour L’evaluation et L’amelioration). (2005). https://apps.dtic.mil/sti/citations/ADA437898
42. Mayer CM, Cluff L, Lin WT, Willis TS, Stafford RE, Williams C, et al. Evaluating efforts to optimize TeamSTEPPS implementation in surgical and pediatric intensive care units. Jt Comm J Qual Patient Saf. (2011) 37:365–74. doi: 10.1016/s1553-7250(11)37047-x
43. Röttger S, Vetter S, Kowalski JT. Ship management attitudes and their relation to behavior and performance. Hum Factors. (2013) 55:659–71. doi: 10.1177/0018720812461271
44. Shortell SM, Zimmerman JE, Rousseau DM, Gillies RR, Wagner DP, Draper EA, et al. The performance of intensive care units: does good management make a difference? Med Care. (1994) 32:508–25. doi: 10.1097/00005650-199405000-00009
45. Graetz DE, Chen Y, Devidas M, Antillon-Klussmann F, Fu L, Quintero K, et al. Interdisciplinary care of pediatric oncology patients in Central America and the Caribbean. Cancer. (2020) 127:508–25. doi: 10.1002/cncr.33339
46. Upenieks VV, Lee EA, Flanagan ME, Doebbeling BN. Healthcare team vitality instrument (HTVI): developing a tool assessing healthcare team functioning. J Adv Nurs. (2010) 66:168–76. doi: 10.1111/j.1365-2648.2009.05137.x
Keywords: measurement, implementation science, communication, health equity, bilingual
Citation: Malone S, Rivera J, Puerto-Torres M, Prewitt K, Sakaan F, Counts L, Al Zebin Z, Arias AV, Bhattacharyya P, Gunasekera S, Johnson S, Kambugu J, Kaye EC, Mandrell B, Mack JW, McArthur J, Mendez A, Morrissey L, Sharara-Chami R, Snaman J, Sniderman E, Luke DA, Graetz DE and Agulnik A (2023) A new measure for multi-professional medical team communication: design and methodology for multilingual measurement development. Front. Pediatr. 11:1127633. doi: 10.3389/fped.2023.1127633
Received: 6 March 2023; Accepted: 9 May 2023;
Published: 2 June 2023.
Edited by:
Roberto Manuel Jabornisky, Universidad Nacional del Nordeste, ArgentinaReviewed by:
Jana Pressler, University of Nebraska Medical Center, United States© 2023 Malone, Rivera, Puerto-Torres, Prewitt, Sakaan, Counts, Al Zebin, Arias, Bhattacharyya, Gunasekera, Johnson, Kambugu, Kaye, Mandrell, Mack, McArthur, Mendez, Morrissey, Sharara-Chami, Snaman, Sniderman, Luke, Graetz and Agulnik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara Malone c2FyYS5tYWxvbmVAd3VzdGwuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.