 Guangchao Tian
Guangchao Tian Bingtao Guo*
Bingtao Guo*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 21 March 2023
Sec. Pediatric Urology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1103200
This article is part of the Research Topic Recent Advances in Hypospadiology View all 6 articles
Objective: The objective of this study was to investigate the influencing factors of multiple urethrocutaneous fistula (UF) after urethroplasty in children with hypospadias.
Methods: The clinical data of 195 children with UF after urethroplasty treated surgically in the Third Affiliated Hospital of Zhengzhou University from August 2015 to August 2022 were retrospectively analyzed and divided into the single UF group (n = 134) and the multiple UF group (n = 61) according to whether multiple UF occurred after urethroplasty. The possible correlated factors were collected and compared between the two groups, including hypospadias degree, length of formed urethra, time of urethroplasty, pre-urethroplasty weight, age at urethroplasty, urethroplasty style, season of urethroplasty, the first fistula repair method, season of the first fistula repair, diameter of the largest fistula of the first fistula repair, time of the first fistula repair surgery, and other 13 factors.
Results: By univariate analysis, statistically significant differences were found between the two groups in age at urethroplasty, length of the formed urethra, method of urinary drainage after urethroplasty, whether or not purulent urethral drainage after first fistula repair was present, the first fistula repair method, and diameter of the largest fistula of the first fistula repair (P < 0.05). After multifactorial analysis, the independent risk factors associated with multiple UF after urethroplasty were determined to be use of a vesicostomy tube as the urinary drainage method after urethroplasty (P < 0.05, OR = 6.574, 95% CI: 2.720–15.891) and the presence of purulent urethral drainage after first fistula repair (P < 0.05, OR = 2.723, 95% CI: 1.214–6.109).
Conclusions: A catheter as the drainage method after urethroplasty is an independent protective factor for multiple urethrocutaneous fistula, and the existence of purulent urethral secretions after the first fistula repair is an independent risk factor.
Hypospadias is the most common congenital malformation of male external genitalia, and its incidence is significantly different in different regions worldwide (1–4). The cause of hypospadias is not clear, and most scholars believe that it is the result of the comprehensive influence of multiple factors, so it is impossible to achieve targeted prevention. In addition, the diagnosis and surgical treatment of fetal hypospadias have obvious limitations, so postnatal surgery is the only solution for it (5, 6). With the development of pediatric anesthesia and surgical instruments in recent years, the operation of hypospadias in children has become mature. However, the postoperative complications cannot be completely avoided. Urethrocutaneous fistula (UF) is one of the common short-term complications after urethroplasty in children with hypospadias. The incidence of UF has decreased to some extent in recent years, but it is still much higher than other complications. The high incidence of UF and the high possibility of recurrence after the first fistula repair are still key problems to be solved in pediatric urology. The purpose of this study was to explore the influencing factors of multiple UF after urethroplasty in children with hypospadias.
We conducted a retrospective case–control study using our hospital's clinical data on patients with UF after urethroplasty from August 2015 to August 2022, which was approved by the Ethics Committee of the Third Affiliated Hospital of Zhengzhou University. The exclusion criteria were as follows: (1) complicated with DSD (disorder of sexual development); (2) initial surgery such as penile straightening or urethroplasty was performed in other hospital; (3) initial surgery was performed in our hospital, and complications such as UF were treated in other hospital; (4) history of application of sex hormones such as chorionic gonadotropin and testosterone undecanoate within 3 months before urethroplasty (7); (5) complicated with urethral stricture when UF occurred for the first time; (6) the fistula was located in the thin ventral tissue of distal part of the glans, and the connecting tissue between the fistula and the external orifice of the urethra was cut directly, without glansplasty; (7) incomplete data.
The clinical data of 195 children with UF after urethroplasty meeting the inclusion criteria were collected. These cases were divided into the single UF group (n = 134) and the multiple UF group (n = 61) according to whether multiple UF occurred after urethroplasty (Table 1). Twenty-four factors related to multiple UF were collected: degree of hypospadias (I, II, III, IV) (8), urinary comorbidities (cryptorchidism, hydrocele concurrenting, etc.), length of formed urethra, time of urethroplasty, pre-urethroplasty weight, age of urethroplasty, urethroplasty style [staged operation (one-stage penile straightening and two-stage Snodgrass), Snodgrass, Duckett and Duplay, Snodgrass and Ducket, Koyanagi, Duckett], season of urethroplasty (spring, summer, autumn, winter), the presence of purulent urethral drainage after urethroplasty, existing usage of analgesics or sedatives after urethroplasty, method of urinary drainage after urethroplasty, time of removal of catheter after urethroplasty, time of removal of penile dressing after urethroplasty, the first fistula repair method, season of the first fistula repair, diameter of the largest fistula of the first fistula repair, time of the first fistula repair surgery, weight of the first fistula repair surgery, interval time between urethroplasty and the first fistula repair surgery, number of UF of the first fistula repair, the presence of purulent urethral drainage after first fistula repair, existing usage of analgesics or sedatives after the first fistula repair, time of removal of catheter after the first fistula repair, and time of removal of penile dressing after the first fistula repair.
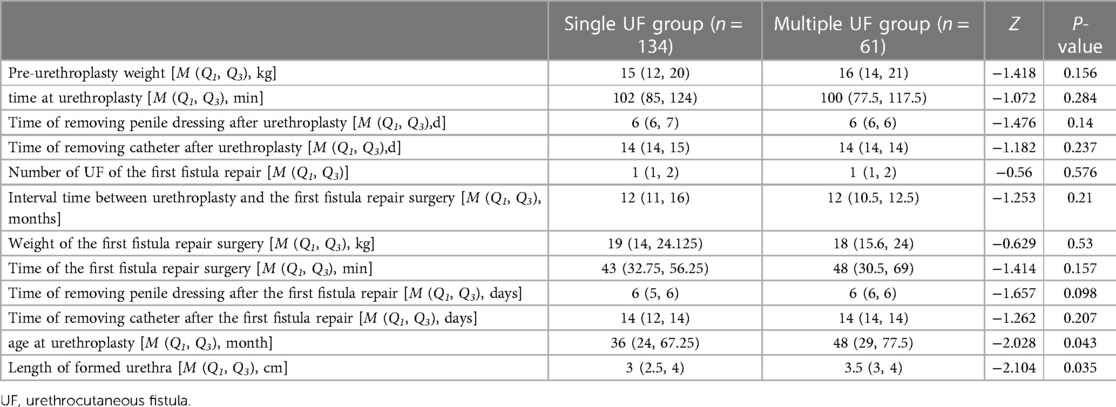
Table 1. Demographic characteristics of the single UF group and multiple UF group.
Multivariate logistic regression analysis was used to analyze the influencing factors significantly correlated with multiple UF after urethroplasty in children with hypospadias. The Shapiro–Wilk test was used to test the normality of quantitative data. Continuous variables were represented as medians and interquartile ranges [M (Q1, Q3)] if non-normally distributed. The 12 continuous variables in this study were non-normal distribution and analyzed by the Wilcoxon rank-sum test on both sides. Qualitative data were analyzed by the χ2-test and represented as frequencies and percentages [n (%)] on both groups. Statistical analyses were performed using SPSS v.25 software. Statistical significance was set at P < 0.05.
None of the 195 children with UF were complicated with urethral diverticulum in this study. A total of 134 children with single UF were cured after one time of fistula repair. Among the 61 children with multiple UF, 39 cases were cured after two times of fistula repair, 21 cases were cured after three times of fistula repair, and 1 case was cured after four times of fistula repair.
By univariate regression analysis, statistically significant differences were found between the single UF group and the multiple UF group in age at urethroplasty, length of the formed urethra, method of urinary drainage after urethroplasty, the presence of purulent urethral drainage after first fistula repair, the first fistula repair method, and the diameter of the largest fistula of the first fistula repair (P < 0.05) (Table 2).
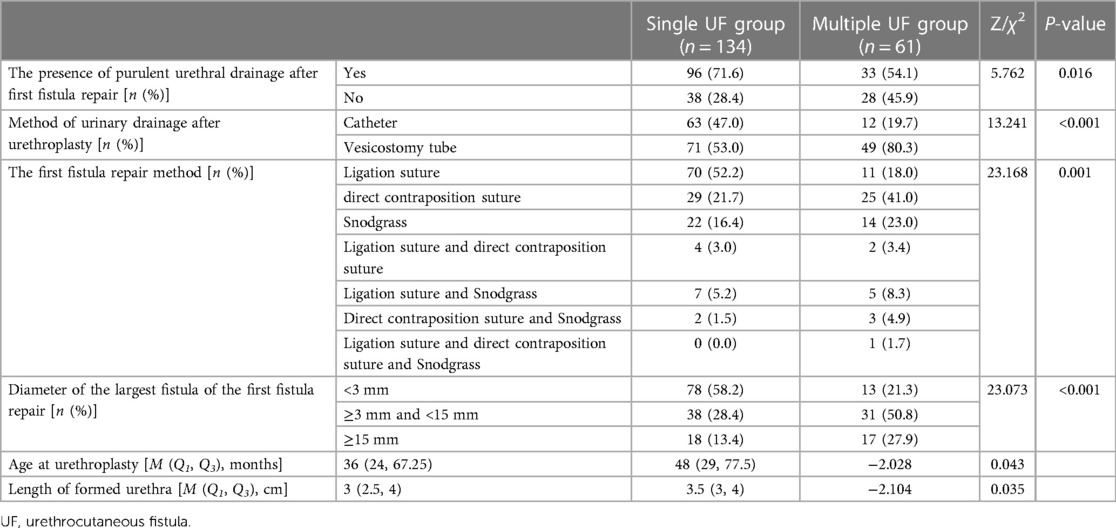
Table 2. Univariate regression analysis of multiple UF after urethroplasty.
The statistically significant factors calculated by the univariate regression analysis were added in the multivariate logistic regression analysis. The results showed that the factors related to multiple UF after urethroplasty were method of urinary drainage after urethroplasty and the presence of purulent urethral drainage after first fistula repair (P < 0.05)(Table 3).
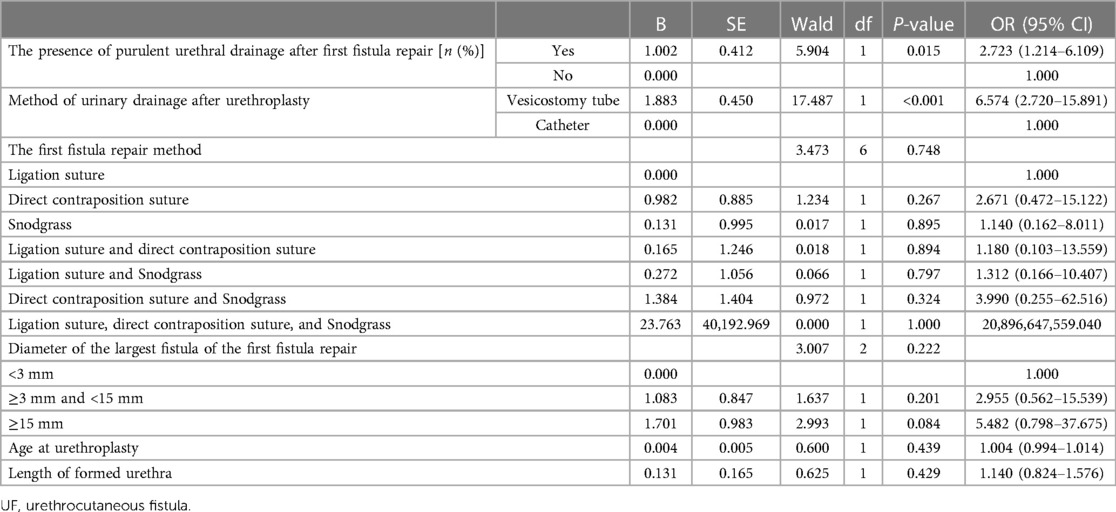
Table 3. Multivariate logistic regression analysis of multiple UF after urethroplasty.
UF is one of the most common complications after urethroplasty in children with hypospadias. At present, there are many studies on the incidence of the first UF, but there are few on the incidence of recurrent UF after the first fistula repair. The multiple UF incidence reported by Abdullaev et al., Yassin et al., and Aldaqadossi et al. are 19%, 22.3%, and 4.4%, respectively (9–11). However, the sample size in their studies on multiple UF was small, including 63 cases in Abdullaev et al. and 67 cases in Yassin et al., and only 45 cases in Aldaqadossi et al., all of which are retrospective studies, so the conclusions are not completely reliable. In our study, 195 children with UF who met the criteria were enrolled, of which 134 cases had no recurrence after the first fistula repair and 61 cases had recurrence after the first fistula repair. The incidence of multiple UF in our study was slightly higher than others, which may be related to the differences in the sample inclusion criteria, surgeon's surgical techniques, surgical methods, and sample size.
The formation of UF after urethroplasty is related to many factors, such as the surgical experience of surgeons, urethroplasty style, method of urinary drainage after urethroplasty, length of the formed urethra, infection at the operation site, dysvascularization of formed urethral tissue, necrosis and inactivation of skin flap, and hypoplasia of glans (12, 13). There are many studies on the influencing factors of the initial UF but few on the multiple UF. Hypospadias degree, length of formed urethra, and the type of material used to cover the fistula are determined to be related to the recurrence of UF (9, 11). Our study suggests the vesicostomy tube as a method of urinary drainage after urethroplasty and the existence of purulent urethral secretions after the first fistula repair will lead to multiple UF. It is controversial to use a catheter or a vesicostomy tube to drain urine after urethroplasty or the fistula repair surgery currently (14). The results of our study support the conclusion that catheter is the better way for urine drainage, and the accumulation of surgical experience of surgeons is also of certain significance for the prevention of UF occurrence after urethroplasty (15). However, our study does not take into account the accumulation of surgical experience of surgeons, which makes the conclusions of this study not rigorous to a certain extent. This study is a retrospective case–control study, which cannot completely eliminate the influence of confounding factors such as the accumulation of surgical experience of surgeons, so it needs to be verified by a prospective follow-up research study regarding multiple UF. Purulent urethral secretion is caused by bacterial infection in the tissue of operation site after urethroplasty or fistula repair surgery, which will cause necrosis of the skin flap tissue cell in the microenvironment of bacteria, pus, and inflammatory factors, and then cause the first and multiple UFs.
The local application of the growth factor and prolonging the indwelling time of a catheter is sometimes used to treat acicular UF in clinics. Surgery is still the main method to treat acicular UF because of the lack of reliable research support. Srivastava et al. divided UF into two types according to its diameter. UF with a diameter smaller than 2 mm was repaired by direct contraposition suture, and that bigger than 2 mm was repaired by transferring a skin flap from other sites (16). In the traditional method, the superficial skin tissue of the penis around the large UF is dissociated, and then a local propulsive flap is formed to suture the fistula. In the traditional method, the blood supply of the penile skin tissue around the UF is always poor because the microvessels present there are likely to have been destroyed by electrocoagulation during urethroplasty or first fistula repair surgery (17). We evaluated the diameter, location, number of UF, and blood supply of the penis skin tissue around the UF, and then adopted a comprehensive method to repair the first or multiple UF. The key step of our comprehensive method to prevent recurrence of UF was to cover the repaired UF using the tissue with good blood supply (such as testicular sheath and dartos fascia) (18). The tissue conditions around the UF of children who have experienced fistula repair surgery multiple times are always very poor, which is also an important reason why children with UF will still recur after repeated fistula repair (8). Carmignani used microscope magnification technology to achieve the tight suture of UF and protect the microvessels, so as to reduce the recurrence of UF (19). For children with multiple UF whose local blood supply around UF is poor, and the adjacent tissue that can be used for skin flap to repair UF is nearly exhausted, some scholars use biosynthetic materials (such as Integra®, bladder mucosal acellular matrix, and intestinal mucosal acellular matrix) to repair (20–22). Both the microscope magnification technology and the biosynthetic materials can be used as an alternative method to repair the multiple UF whose local blood supply and adjacent tissue that can be used for the skin flap is poor.
Our study shows that a catheter used as the drainage method after urethroplasty is an independent protective factor for multiple UF, and the existence of purulent urethral secretions after the first fistula repair is an independent risk factor. In addition, multiple factors such as UF diameter, number, local blood supply around UF, and adjacent tissue conditions should be comprehensively considered when repairing multiple UF.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
GT designed the main purposes and methods of this study. GT wrote the article and BG revised the article. LZ participated in the index design and preliminary statistical analysis. GT, BG, and LZ participated in the data collection and critically reviewed the content of the article. All authors contributed to the article and approved the submitted version.
We thank all our colleagues from the Department of Pediatric Urology of the Third Affiliated Hospital of Zhengzhou University, for their support of our project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ságodi L, Kiss A, Kiss-Tóth E, Barkai L. Prevalence and possible causes of hypospadias. Orv Hetil. (2014) 155(25):978–85. doi: 10.1556/OH.2014.29858
2. Nordenvall AS, Frisén L, Nordenström A, Lichtenstein P, Nordenskjöld A. Population based nationwide study of hypospadias in Sweden, 1973 to 2009: incidence and risk factors. J Urol. (2014) 191(3):783–9. doi: 10.1016/j.juro.2013.09.058
3. Li Y, Mao M, Dai L, Li K, Li X, Zhou G, et al. Time trends and geographic variations in the prevalence of hypospadias in China. Birth Defects Res A Clin Mol Teratol. (2012) 94(1):36–41. doi: 10.1002/bdra.22854
4. Loane M, Dolk H, Kelly A, Teljeur C, Greenlees R, Densem J. Paper 4: EUROCAT statistical monitoring: identification and investigation of ten year trends of congenital anomalies in Europe. Birth Defects Res A Clin Mol Teratol. (2011) 91(Suppl 1):S31–43. doi: 10.1002/bdra.20778
5. Rocheleau CM, Romitti PA, Dennis LK. Pesticides and hypospadias: a meta-analysis. J Pediatr Urol. (2009) 5(1):17–24. doi: 10.1016/j.jpurol.2008.08.006
6. Nassar N, Abeywardana P, Barker A, Bower C. Parental occupational exposure to potential endocrine disrupting chemicals and risk of hypospadias in infants. Occup Environ Med. (2010) 67(9):585–9. doi: 10.1136/oem.2009.048272
7. Netto JM, Ferrarez CE, Schindler Leal AA, Tucci S, Gomes CA, Barroso U. Hormone therapy in hypospadias surgery: a systematic review. J Pediatr Urol. (2013) 9(6 Pt B):971–9. doi: 10.1016/j.jpurol.2013.03.009
8. Browne D. Congenital deformities of mechanical origin: (section for the study of disease in children). Proc R Soc Med. (1936) 29(11):1409–31. doi: 10.1136/bmj.1.3935.1182
9. Abdullaev Z, Agzamkhodjaev S, Chung JM, Lee SD. Risk factors for fistula recurrence after urethrocutaneous fistulectomy in children with hypospadias. Turk J Urol. (2021) 47(3):237–41. doi: 10.5152/tud.2020.20323
10. Yassin T, Bahaaeldin KH, Husein A, Minawi HE. Assessment and management of urethrocutaneous fistula developing after hypospadias repair. Ann Pediatr Surg. (2011) 7(2):88–93. doi: 10.1097/01.XPS.0000397066.98404.82
11. Aldaqadossi HA, Eladawy M, Shaker H, Kotb Y, Azazy S. Tunica vaginalis graft for recurrent urethrocutaneous fistula repair after hypospadias surgery. Int J Urol. (2020) 27(9):726–30. doi: 10.1111/iju.14287
12. Cimador M, Vallasciani S, Manzoni G, Rigamonti W, De Grazia E, Castagnetti M. Failed hypospadias in paediatric patients. Nat Rev Urol. (2013) 10(11):657–66. doi: 10.1038/nrurol.2013.164
13. Bush NC, Villanueva C, Snodgrass W. Glans size is an independent risk factor for urethroplasty complications after hypospadias repair. J Pediatr Urol. (2015) 11(6):355. doi: 10.1016/j.jpurol.2015.05.029
14. Redman JF. Results of undiverted simple closure of 51 urethrocutaneous fistulas in boys. Urology. (1993) 41(4):369–71. doi: 10.1016/0090-4295(93)90599-6
15. Han WW, Zhang WP, Sun N, Bai JW, Liu RX, Tian J. Study on learning curve of hypospadias among pediatric urologists. Contin Med Educ. (2016) 30(3):51–2. doi: 10.3969/j.issn.1004-6763.2016.03.032
16. Srivastava RK, Tandale MS, Panse N, Gupta A, Sahane P. Management of urethrocutaneous fistula after hypospadias surgery—an experience of thirty-five cases. Indian J Plast Surg. (2011) 44(1):98–103. doi: 10.4103/0970-0358.81456
17. Ochi T, Seo S, Yazaki Y, Okawada M, Doi T, Miyano G. Traction-assisted dissection with soft tissue coverage is effective for repairing recurrent urethrocutaneous fistula following hypospadias surgery. Pediatr Surg Int. (2015) 31(2):203–7. doi: 10.1007/s00383-014-3652-1
18. Ren ZT, Zhang WP. Research progress of urethral coverage in hypospadias repair. J Clin Ped Sur. (2021) 21(1):30–5. doi: 10.3760/cma.j.cn101785-202009034-006
19. Carmignani G, Belgrano E, Gaboardi F, Farina FP. Microsurgical one-stage repair of hypospadias with a rectangular transverse dorsal preputial vascularized skin flap. J Microsurg. (1982) 3(4):222–7. doi: 10.1002/micr.1920030406
20. Casal-Beloy I, Somoza Argibay I, García González M, García-Novoa MA, Míguez Fortes LM, Dargallo Carbonell T. Dermal regeneration sheet Integra® in management of recurrent urethrocutaneous fistula after hypospadias surgery. J Pediatr Urol. (2019) 15(6):634. doi: 10.1016/j.jpurol.2019.10.002
21. Chan YY, Bury MI, Yura EM, Hofer MD, Cheng EY, Sharma AK. The current state of tissue engineering in the management of hypospadias. Nat Rev Urol. (2020) 17(3):162–75. doi: 10.1038/s41585-020-0281-4
Keywords: hypospadias/SU, hypospadias/CO, urethrocutaneous fistula, multiple fistula, complications, risk factors
Citation: Tian G, Guo B and Zhang L (2023) Analysis of influencing factors of multiple urethrocutaneous fistula after urethroplasty in children with hypospadias. Front. Pediatr. 11:1103200. doi: 10.3389/fped.2023.1103200
Received: 20 November 2022; Accepted: 1 March 2023;
Published: 21 March 2023.
Edited by:
Nicolas Fernandez, Seattle Children's Hospital, United StatesReviewed by:
Cristina Dominguez, Fundación Santa Fe de Bogotá, Colombia© 2023 Tian, Guo and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bingtao Guo Z2J0d2luQDE2My5jb20=
Specialty Section: This article was submitted to Pediatric Urology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.