
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 17 March 2023
Sec. Neonatology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1090701
This article is part of the Research TopicRespiratory Management of Extremely Preterm Infants: Volume 2View all 5 articles
 Mari Oma Ohnstad1,2*
Mari Oma Ohnstad1,2* Hans Jørgen Stensvold3
Hans Jørgen Stensvold3 Are Hugo Pripp4,5Christine Raaen Tvedt1Lars-Petter Jelsness-Jørgensen1,6,7Henriette Astrup8Beate Horsberg Eriksen9,10Mai Linn Lunnay11Khalaf Mreihil12
Are Hugo Pripp4,5Christine Raaen Tvedt1Lars-Petter Jelsness-Jørgensen1,6,7Henriette Astrup8Beate Horsberg Eriksen9,10Mai Linn Lunnay11Khalaf Mreihil12 Tanja Pedersen13
Tanja Pedersen13 Siren Irene Rettedal14,15Terje Reidar Selberg16
Siren Irene Rettedal14,15Terje Reidar Selberg16 Rønnaug Solberg17,18Ragnhild Støen19,20
Rønnaug Solberg17,18Ragnhild Støen19,20 Arild Erland Rønnestad2,3,21
Arild Erland Rønnestad2,3,21 on behalf of the Norwegian Neonatal Network
on behalf of the Norwegian Neonatal Network
Objective: The objective was to explore whether high workloads in neonatal intensive care units were associated with short-term respiratory outcomes of extremely premature (EP) infants born <26 weeks of gestational age.
Methods: This was a population-based study using data from the Norwegian Neonatal Network supplemented by data extracted from the medical records of EP infants <26 weeks GA born from 2013 to 2018. To describe the unit workloads, measurements of daily patient volume and unit acuity at each NICU were used. The effect of weekend and summer holiday was also explored.
Results: We analyzed 316 first planned extubation attempts. There were no associations between unit workloads and the duration of mechanical ventilation until each infant’s first extubation or the outcomes of these attempts. Additionally, there were no weekend or summer holiday effects on the outcomes explored. Workloads did not affect the causes of reintubation for infants who failed their first extubation attempt.
Conclusion: Our finding that there was no association between the organizational factors explored and short-term respiratory outcomes can be interpreted as indicating resilience in Norwegian neonatal intensive care units.
Neonatal intensive care units (NICUs) provide care for some of the most vulnerable patients admitted to hospitals, and all admissions to Norwegian NICUs are essentially emergencies (1).
In Norway, the vast majority of extremely premature (EP) infants who are born alive between 23 and 26 weeks of gestational age (GA) receive transitional assistance, mainly with respiratory support. Those who respond positively are admitted to a NICU immediately after birth. Survival rates decrease with decreasing GA, and the smallest babies require treatment in the NICU for weeks or months (2).
The risk of neonatal mortality and morbidity has been shown to increase with increased workloads and decreased staff ratios (3–5). Moreover, NICUs differ from adult and pediatric intensive care units, which exclusively treat intensive care patients, as NICUs treat patients with varied resource needs, from highly intensive care to nearly normal maternity care (6). This creates challenges regarding unit staffing (7). Synnes et al. linked intraventricular hemorrhage to unit characteristics, suggesting that practices in NICUs with higher patient volumes and those with higher neonatologist-to-house staff ratios result in a lower incidence of severe intraventricular hemorrhage (8). In a study from Canada, greater resource use in the unit at the time of admission was associated with a higher risk of neonatal morbidity in very premature infants (9). Furthermore, weekends and holidays have been identified as times when staffing in hospitals tends to be lower, and several researchers have noted associations between weekend admissions and worse patient outcomes (10–12).
For most EP infants <26 weeks GA, mechanical ventilation (MV) is required for survival (13, 14). However, MV itself is associated with complications (15, 16), and the optimal timing of extubation is one of many challenges for clinicians (17). Close and continuous observation and monitoring, as well as clinical assessment, are essential to decide whether and why MV is needed and to prevent prolonged MV treatment or failure of an extubation attempt (18). Moreover, the post-extubation period is considered a time during which the EP infant <26 weeks GA requires special attention and management to prevent reintubation.
It is unknown whether a high unit workload affects the duration of MV until the first extubation attempt and the first extubation outcome. The main objective of this study was to explore whether high workloads in NICUs influenced timing of first planned extubation attempts or affected extubation success. We examined the association of unit workloads and the effects of weekends or summer holiday with the duration of MV until the first extubation attempt and the outcome of the first extubation attempt. As many EP infants <26 weeks GA are reintubated after their first extubation attempt (19), we explored whether high workloads in the NICUs affected respiratory morbidity for the infants reintubated within 72 h after the extubation attempt. Therefore, our secondary objective was to assess the association of unit workloads and the effects of weekends or summer holiday with indicators of respiratory morbidity before and shortly after reintubation.
This population-based cross-sectional study included infants born at 220 through 256 weeks GA and admitted to a Norwegian NICU between January 1, 2013, and December 31, 2018. The population being explored represent a subgroup of EP infants, as we included infants born before 26 weeks GA. Eligible infants were identified in the Norwegian Neonatal Network (NNN) database. An informational letter describing the purpose of the study was distributed to the infants’ mothers and included an opt-out alternative. Infants were enrolled in the study if the mother did not indicate a desire to opt out within four weeks.
We examined data from the NNN supplemented by data extracted from medical records. Data on all patients admitted to any Norwegian NICU (n = 20) are collected daily by trained staff and entered into the NNN’s electronic registration platform. The NNN contains anthropometric and demographic data and detailed data on resuscitation, treatment modalities, treatment procedures, diagnoses, outcome parameters, and status at discharge.
From the NNN, we extracted perinatal variables, which included antenatal steroids, delivery method and plurality, and demographic variables, such as GA, sex, birth weight, and weight at GA. In addition, the Clinical Risk Index for Babies (CRIB II) and Apgar scores at 5 min were included as variables describing illness severity and general condition at birth. Furthermore, we extracted delivery room variables, which included endotracheal intubation and surfactant administration. From the medical records, we extracted data on MV settings and blood gas samples.
Unit workloads were calculated based on variables extracted from the NNN database for each day during the six years studied. To describe the workloads, measurements of daily patient volume and unit acuity at each participating NICU were derived and used as follows.
The patient volume of a given NICU on a given day was defined as “the number of all infants staying in the unit,” not only those born below 26 weeks GA and included in our study. Unit acuity was defined as the “intensity of nursing care needed by the patients” in a given NICU on a given day and was calculated based on daily resource registration in the NNN (shown in Figure 1). Each day, patient care and individual treatment procedures are recorded in the NNN database. Patients are classified into five levels, similar to the Vermont Oxford Network researcher’s classification (20). Levels 1 and 2 represent patients with low acuity who require basic monitoring and care. Level 3 represents patients receiving breathing assistance with nasal continuous airway pressure and often drug therapy. These infants require frequent monitoring. Level 4 typically represents patients on MV requiring continuous monitoring, and Level 5 represents patients requiring the highest level of intensive care treatment and surveillance. The coding accuracy for the patient classification variable is considered high, as each hospitalized newborn is registered in the NNN each day, and there is little room for individual interpretation of each newborn’s clinical condition. The total acuity in one NICU for each day was calculated based on an estimation of the need for nursing, as described elsewhere (7). Patient volume and unit acuity were calculated for each day in the study period and defined as a low, normal, or high unit workload based on standard deviations. We also extracted the number of patients admitted and discharged each day, as these patients often require more resources. Furthermore, unit workloads were explored at three time points that are considered important in an EP infant’s course of treatment:
(i) the infant’s day of birth,
(ii) the day of the first extubation attempt, and
(iii) the week after the first extubation attempt.
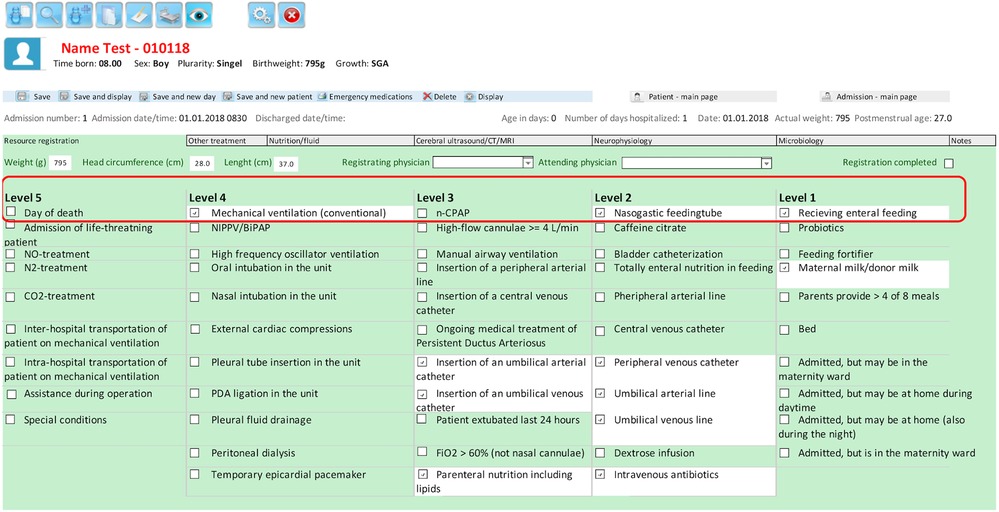
Figure 1. Screenshot of part of the daily resource registration form in the Norwegian neonatal network database (the patient classification system, with levels 1–5). This form was translated into English from Norwegian.
Moreover, if the infant was reintubated, the workload on the day of reintubation was explored. We chose to explore the unit workload on the infant’s day of birth (DOB), as the DOB is considered important related to prior research about the importance of the golden hour, suggesting that interventions performed in the first minutes after birth may have long-term consequences in addition to short-term effects on the rate and quality of survival of EP infants (21, 22).
To distinguish weekdays from weekends, weekends were defined as Saturdays and Sundays, as this is the most common weekend definition in “off-shift” research (23). Summer days were defined from July to August, as this is the most common period for annual leave among Norwegian healthcare professionals.
The primary outcomes were the duration of MV until the first planned extubation attempt and the outcome of this attempt. Extubation success was defined as no reintubation within 72 h.
Secondary outcomes were causes of reintubation and short-term respiratory morbidity of the infants reintubated within 72 h. The causes of reintubation and variables relevant to the ventilation treatment provided six hours before and after the reintubation event were extracted from the medical records to enable a description of short-term respiratory morbidity. The pre-reintubation variables extracted included the mode of non-invasive ventilation, such as positive end-expiratory pressure, and fraction of inspired oxygen (FiO2) administered. The post-reintubation variables included ventilator modes and settings, such as peak inspiratory pressure, mean positive airway pressure, and FiO2. In addition, blood gas variables before and after reintubation were extracted.
Data were expressed as means with 95% confidence intervals or standard deviations (SDs), medians with 25th and 75th percentiles (the interquartile range), or numbers with proportions (%). For patient volume and unit acuity, z-scores for each NICU were calculated for the total of the six years studied because stratified analyses did not show a distinctive change in patient volume or unit acuity over these years. Z-scores were calculated as the association between each day’s patient volume and unit acuity as measured by standard deviations from the mean. According to this, each day was defined as normal if the z-score was ±1 SD, high if the z-score was >+1 SD, and low if the z-score was <−1 SD. Depending on the variable distribution, we examined unadjusted associations between the outcome and exposure variables using Kruskal–Wallis and logistic regression analyses with unit workloads as independent variables. In the regression analysis, days with low patient volume or low unit acuity were used as the reference groups. All statistical analyses were performed using Stata/MP (2019, Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). The threshold for statistical significance was set at p < 0.05.
Of 482 infants with GA <26 weeks admitted to a NICU during the study period, 43 (9%) infants were excluded, as the mother’s address could not be verified or the mother chose to opt out. Additionally, 10 (2%) infants were excluded because they had never been intubated during admission. Furthermore, 102 (21%) infants who died prior to the first extubation attempt, and 11 (2%) who had an identified accidental extubation were excluded. In the final analysis, 316 first extubation attempts were included (Figure 2). The first extubation attempts were performed in 11 different Norwegian NICUs. Table 1 presents the characteristics of the study population.
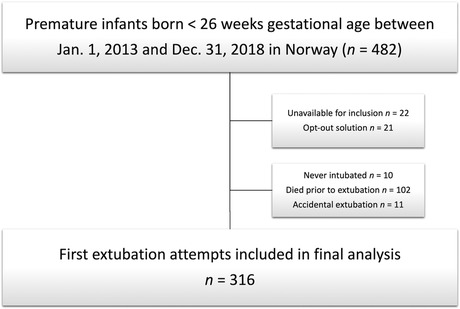
Figure 2. Flowchart of included infants.
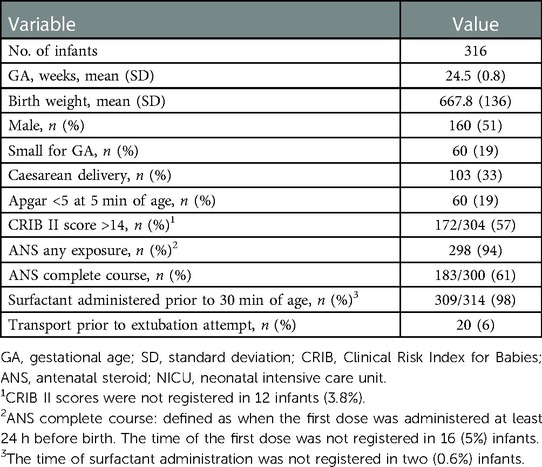
Table 1. Characteristics of the study population.
The associations between the exposure variables and primary outcomes are presented in Table 2. Most of the infants had their first extubation attempt on a day categorized by normal patient volume and normal unit acuity. There was no statistical difference in the outcomes if the infant was extubated on a day with low, normal, or high patient volume or unit acuity. Additionally, there was no association between patient volume and unit acuity in the week after the first extubation attempt with the duration of MV or extubation success (data not shown).
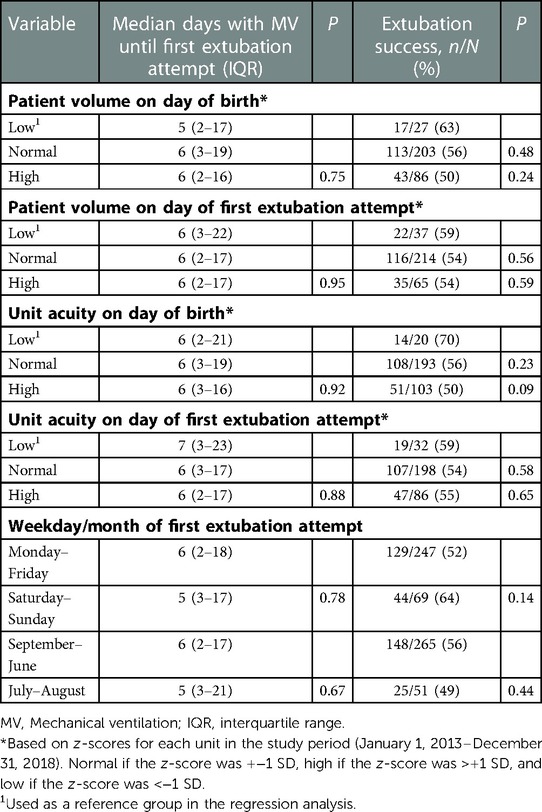
Table 2. The association of patient volume, unit acuity, and weekdays with duration of mechanical ventilation and extubation success, n = 316.
We found that 86 (27%) infants were extubated on days classified as high workload (acuity), while 32 (10%) were extubated on days classified as low workload (acuity) (data not shown).
There were 247 (78%) infants who had their first extubation attempt on a weekday, while 69 (22%) experienced their first attempt on a weekend. Extubation was more often attempted on weekdays compared to Sundays (with a factor of 1.4–1.9, p ≤ 0.01–0.03). Moreover, 51 (16%) infants had their first extubation attempt on a day categorized as a summer holiday. There was no statistical difference in the duration of MV or extubation success between weekdays and weekends, and no statistical difference in these outcomes if it was a summer holiday compared with other days during the year.
A total of 143 (45%) infants experienced reintubation within 72 h after the first extubation attempt, as described elsewhere (24). The documented causes of reintubation are presented in Table 3. The analyses showed no statistical associations between causes of reintubation and weekends, summer holidays, or unit workloads. For the reintubated infants, the short-term respiratory morbidity and associations with the unit workloads are presented in Table 4. There were borderline significant higher pre-reintubation FiO2 between days with a high patient volume and days with a low patient volume, and higher post-reintubation pCO2 on days with a normal patient volume compared with those with a low patient volume. No other differences in the pre- and post-reintubation variables were found. Analyses of differences in unit acuity on the day of reintubation revealed similar results.
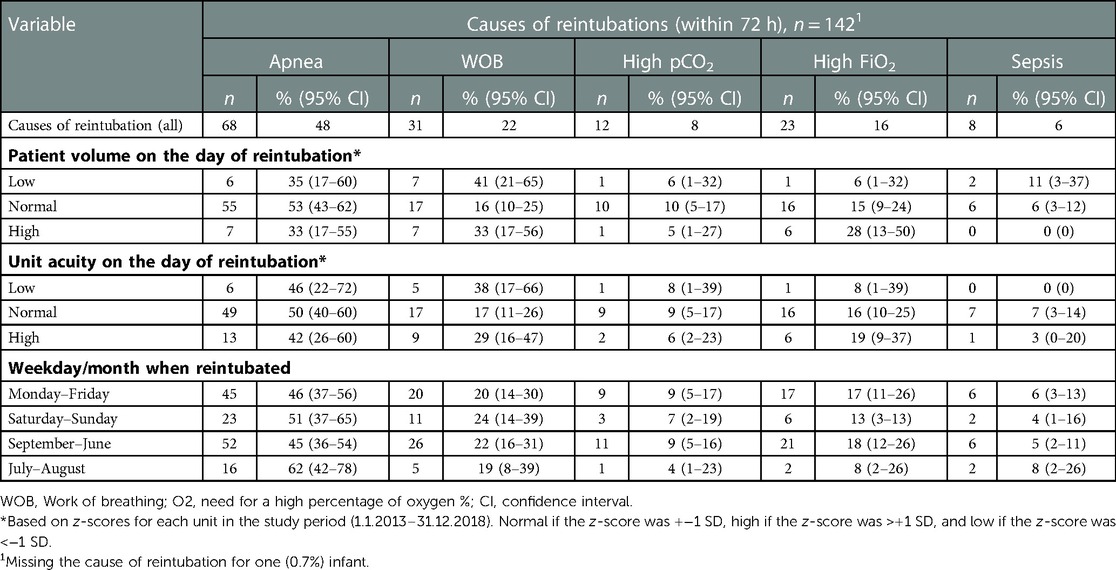
Table 3. Causes of reintubation and associations with patient volume, unit acuity, and the weekday the infant was reintubated.
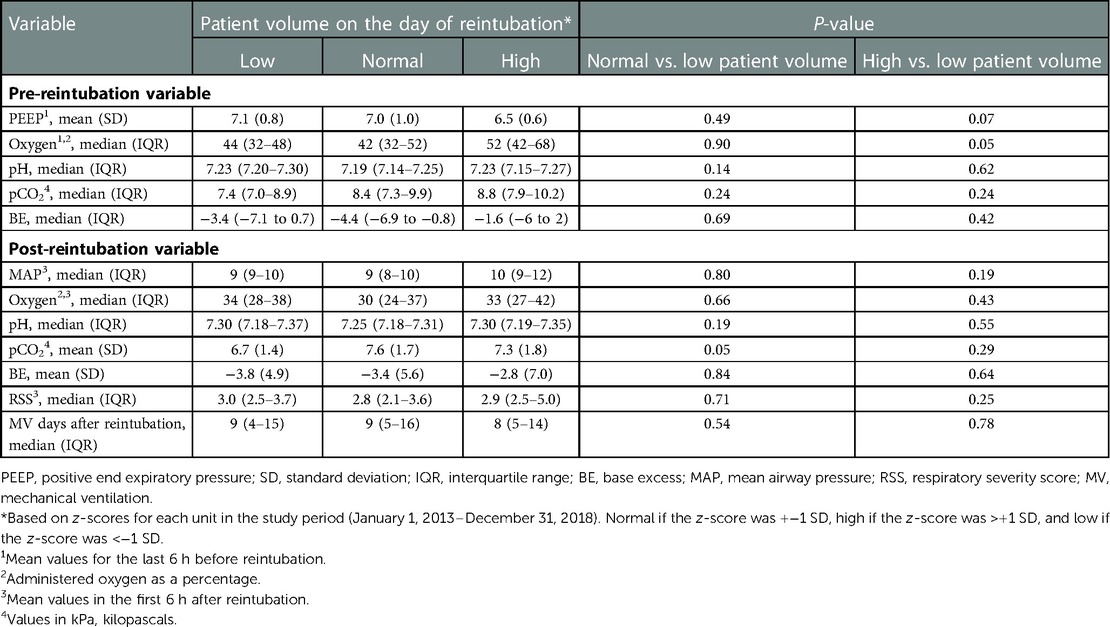
Table 4. Indicators of short-term respiratory morbidity for infants reintubated and associations with patient volume, n = 143.
The results from all pre- and post-reintubation variables explored are provided in Supplementary Tables S1 (patient volume) and S2 (unit acuity).
In this national cohort of EP infants <26 weeks GA, unit workloads, weekdays, or summer holiday did not affect the duration of MV until the first extubation attempt or the outcome of the extubation attempt. In addition, for infants reintubated within 72 h, the organizational factors explored did not affect the causes of reintubation or the indicators of respiratory morbidity before or after reintubation. To our knowledge, this is the first study exploring NICU characteristics and outcomes related to the first extubation attempt among EP infants <26 weeks GA.
The results indicating that workload does not affect extubation outcome and reasons for reintubation due not take into account that some NICUs might have a high workload as their “normal” compared to others. High workload (+1 SD) describe approximately the 85th percentile of workloads in each NICU. It is also possible that there might be a non-linear effect on care from workloads. Both low and high workloads might have a positive or negative effect on care. Extreme high workloads could invoke resilience as emergency procedures supplying more personnel.
Our data suggest that clinicians might be more inclined to extubate on days with high workload since 27% were extubated in the 15% of the days with the highest workload. Interestingly, the outcome of the extubation attempt was not influenced by workload.
Our results may have two potential interpretations. First, the results could suggest that the level of standard staffing (or short-term increased staffing) in Norwegian NICUs is sufficient, regardless of fluctuations in patient volume, unit acuity, weekends, and summer holiday. Alternatively, respiratory care of the most vulnerable infants <26 weeks GA might be the least affected and most protected when workload is high. One might speculate that tight and continuous observation and monitoring of EP infants <26 weeks GA on MV is resilient to fluctuations in workloads in the NICU. Resilience in healthcare has been defined as “the capacity to adapt to challenges and changes at different system levels, to maintain high quality care” (25). Resilience at the clinical level (micro level) could have potential negative consequences in other aims of care in the NICU. Resilience at the level of the NICU (meso level) might include increasing staff on short notice. Possible negative consequences of this could be increased personnel burnout and turnover. Resilience at hospital level (macro level) would be sufficient standard staffing for high workload days, with its financial consequences. Our data does not differentiate level of resilience and potential unwanted consequences.
Our database did not include the actual number of healthcare professionals on call in each participating unit on each day. It also did not include the hours actually worked by physicians and nurses. For instance, individual healthcare personnel might make an extra effort to compensate for the higher unit workload and work overtime if needed. The nursing overtime ratio and unit occupancy have been associated with medical incidents, nosocomial infections, and unplanned extubation events (26–28).
The results of our study indicate that healthcare personnel in Norwegian NICUs were able to deliver high-quality short-term respiratory care independent of unit workloads. However, we speculate whether resources used to maintain high quality in fundamental short-term outcomes aimed at airways and breathing could have come at the expense of attention to other important assignments. Tubbs-Cooley et al. determined that high workloads of NICU nurses were significantly associated with missed nursing care, e.g., missed hourly intravenous site assessments, oral feedings, and parental involvement (29). Hence, the long-term consequences of higher workloads and missed care for infants, parents, and healthcare professionals are uncertain.
Our finding that there was no weekend or summer holiday association is comparable to the results of a large cohort study from the National Institute of Child Health and Human Development Neonatal Research Network database. They found little effect on the risks of death and morbidity among very low birth weight infants born on weekends or during the months of July and August (30). However, our study identified fewer extubation attempts on weekends compared to weekdays. This finding may indicate that extubation attempts were postponed from the weekends and that available staffing on weekends might influence judgments related to the timing of extubation. A lower tendency to extubate on weekends could be a contributing factor to prolonged duration of MV. Over the last decades, the weekend effect has been analyzed and discussed in several studies in both adult and maternal-neonatal settings (31–35). Still, the weekend phenomenon is not yet fully understood, emphasizing the need for further studies exploring actual weekend staffing in relation to respiratory neonatal outcomes.
Furthermore, in this study we have explored several indicators of short-term respiratory morbidity for the infants who were reintubated within 72 h after the extubation attempt. Our results did not indicate that infants reintubated on days with high workload was sicker or needed higher level of respiratory support compared with infants reintubated on days with normal or low workloads. However, we found a borderline significant higher pre-reintubation FiO2 that could be implied as an indicator of infant stress related to a busy unit. Nevertheless, these results must be interpreted with caution with respect to possible confounders, whereas both patient factors and differences in extubation practice among units could influence these results. The choice and management of the post-extubation therapy might be of importance when it comes to extubation success. In a previous publication exploring predictors of successful extubation carried out on the exact same population we showed that all of these infants were predominantly treated with nasal continuous positive airway pressure immediately after extubation (24).
Our study has certain limitations. First, we included patients treated in 11 different NICUs in Norway and were unable to collect the existing staffing levels, seniority, and experience levels of staff present in the unit on each day. In addition, Norwegian NICUs are small resulting in lack of statistical power to control for cluster effects. Second, we were unable to describe fluctuations in workloads during the day. Previous studies have identified higher odds of mortality for infants admitted to the NICU at night compared to the daytime (36). However, a recent study examining overnight extubation was not able to identify differences in success rates between day and night shifts (37). Future studies investigating unit workloads in relation to actual staffing levels and healthcare experiences are needed to further explore the complex contexts of the first extubation events among EP infants <26 weeks GA. Still, there is a lack of a standard method for modeling unit workloads, and the description of a workload effect depends on several factors, including its measure and definition. We considered two measures of unit workload: patient volume and unit acuity. Our calculations were based on z-scores for the total of six years examined. Furthermore, unit acuity may be a more meaningful measure of workloads, as a higher patient volume with relatively few infants at the highest patient levels places different requests on a unit compared with lower patient volumes with a relatively high number of infants demanding intensive care treatment.
The strength of this study is the prospective collection of data on a daily basis by the NNN and the inclusion of a large population-based sample of EP infants <26 weeks GA. The completeness of the variables allowed us to explore unit workloads on days perceived as critical in these vulnerable infants’ courses of treatment in the NICU. Several neonatal networks (e.g., the Vermont Oxford Network, Neonatal Research Network, Italian Neonatal Network, and others) collect data on an individual infant level, and research into the treatment and outcomes of premature infants has expanded, partially due to these large multicenter databases (38). However, few studies using data from neonatal databases address features of the environment where neonatal care takes place, e.g., the unit workload.
In conclusion, we found that there was no association between unit workloads and weekday/summer holiday with the duration of MV until the first extubation attempt and the result of the attempt. The data, containing daily registered measures of acuity for each infant, made it possible to calculate objective indicators of NICU workloads in addition to patient volume. Our results may suggest that the potential threat to short-term respiratory morbidity associated with total patient burden is alleviated by resilience. Further research is needed to examine potential negative consequences for infants and staff in the NICU.
The datasets presented in this article are not readily available because they contain information that could compromise the privacy of research participants. The data that support the findings of this study are available from the corresponding author, MOO, upon reasonable request. Requests to access the datasets should be directed to mari.oma.ohnstad@ldh.no
This population-based study which included infants born before 26 weeks GA was reviewed and approved by Regional Committee for Medical and Health Research Ethics (REC North) (approval number: 2018/1346). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
MOO conceptualized and designed the study; contributed to the data acquisition, database preparation, statistical analyses, and interpretation of the results; and wrote the initial and subsequent drafts of the manuscript. HJS contributed to the study design, data acquisition, statistical analyses, interpretation of the results, and drafting of the manuscript. AHP, CRT, and LPJJ co-supervised the study and contributed to the study design, statistical analyses, interpretation of the results, and critical revision of the manuscript. HA, BHE, MLL, KM, TP, SIR, TRS, RSo, and RSt contributed to the data acquisition, interpretation of the results, and critical revision of the manuscript. AER conceptualized, designed, and supervised the study; contributed to data acquisition, statistical analyses, and interpretation of the results; and drafted the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by Lovisenberg Diaconal University College grant number 1125.
The authors wish to thank the staff, patients, and families in the participating Norwegian NICUs. In addition, the authors wish to thank all dedicated members of the NNN who contributed to quality control, and special thanks are offered to Lina Merete Mæland Knudsen and Kristin Wasland for offering their valuable help with the data collection and ensuring the quality of the data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1090701/full#supplementary-material.
1. Rønnestad A, Stensvold HJ, Knudsen LMM. Norsk nyfødtmedisinsk kvalitetsregister, Årsrapport for 2020. Oslo: Oslo University Hospital (2021) (In Norwegian).
2. Myrhaug HT, Brurberg KG, Hov L, Markestad T. Survival and impairment of extremely premature infants: a meta-analysis. Pediatrics. (2019) 143(2):1–12. doi: 10.1542/peds.2018-0933
3. Callaghan LA. Infant to staff ratios and risk of mortality in very low birthweight infants. Arch Dis Child Fetal Neonatal Ed. (2003) 88(2):94F–97. doi: 10.1136/fn.88.2.F94
4. Sherenian M, Profit J, Schmidt B, Suh S, Xiao R, Zupancic JAF, et al. Nurse-to-patient ratios and neonatal outcomes: a brief systematic review. Neonatology. (2013) 104(3):179–83. doi: 10.1159/000353458
5. Watson SI, Arulampalam W, Petrou S, Marlow N, Morgan AS, Draper E, et al. The effects of a one-to-one nurse-to-patient ratio on the mortality rate in neonatal intensive care: a retrospective, longitudinal, population-based study. Arch Dis Child Fetal Neonatal Ed. (2016) 101(3):F195–200. doi: 10.1136/archdischild-2015-309435
6. Gagliardi L, Corchia C, Bellù R, Coscia A, Zangrandi A, Zanini R. What we talk about when we talk about NICUs: infants’ acuity and nurse staffing. J Matern Fetal Neonatal Med. (2016) 29(18):2934–9. doi: 10.3109/14767058.2015.1109618
7. Ohnstad MO, Solberg MT. Patient acuity and nurse staffing challenges in Norwegian neonatal intensive care units. J Nurs Manag. (2017) 25(7):569–76. doi: 10.1111/jonm.12495
8. Synnes AR, Macnab YC, Qiu Z, Ohlsson A, Gustafson P, Dean CB, et al. Neonatal intensive care unit characteristics affect the incidence of severe intraventricular hemorrhage. Med Care. (2006) 44(8):754–9. doi: 10.1097/01.mlr.0000218780.16064.df
9. Shah PS, Mirea L, Ng E, Solimano A, Lee SK, Canadian Neonatal N. Association of unit size, resource utilization and occupancy with outcomes of preterm infants. J Perinatol. (2015) 12:1–8. doi: 10.1038/jp.2015.4
10. Hamilton KESC, Redshaw ME, Tarnow-Mordi W. Nurse staffing in relation to risk-adjusted mortality in neonatal care. Arch Dis Child Fetal Neonatal Ed. (2007) 92(2):99–103. doi: 10.1136/adc.2006.102988
11. Aylin P. Making sense of the evidence for the “weekend effect”. Br Med J. (2015) 351(September):17–8. doi: 10.1136/bmj.h4652
12. Bell C, Redelmeier D. Mortality among patients admitted to hospitals on weekends compared with weekdays. N Engl J Med. (2001) 345(9):663–8. doi: 10.1056/NEJMsa003376
13. Stensvold HJ, Klingenberg C, Stoen R, Moster D, Braekke K, Guthe HJ, et al. Neonatal morbidity and 1-year survival of extremely preterm infants. Pediatrics. (2017) 139(3):e20161821. doi: 10.1542/peds.2016-1821
14. Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal outcomes of extremely preterm infants from the NICHD. Pediatrics. (2010) 126(3):443–56. doi: 10.1542/peds.2009-2959
15. Choi YB, Lee J, Park J, Jun YH. Impact of prolonged mechanical ventilation in very low birth weight infants: results from a national cohort study. J Pediatr. (2018) 194:34–39.e3. doi: 10.1016/j.jpeds.2017.10.042
16. Jensen EA, DeMauro SB, Kornhauser M, Aghai ZH, Greenspan JS, Dysart KC. Effects of multiple ventilation courses and duration of mechanical ventilation on respiratory outcomes in extremely low-birth-weight infants. JAMA Pediatr. (2015) 169(11):1011–7. doi: 10.1001/jamapediatrics.2015.2401
17. Shalish W, Keszler M, Davis PG, Sant’Anna GM. Decision to extubate extremely preterm infants: art, science or gamble? Arch Dis Child Fetal Neonatal Ed. (2022) 107(1):105–12. doi: 10.1136/archdischild-2020-321282
18. Joseph RA. Prolonged mechanical ventilation: challenges to nurses and outcome in extremely preterm babies. Crit Care Nurse. (2015) 35(4):58–66. doi: 10.4037/ccn2015396
19. Ohnstad MO, Stensvold HJ, Tvedt CR, Rønnestad AE. Duration of mechanical ventilation and extubation success among extremely premature infants. Neonatology. (2021) 118(1):90–7. doi: 10.1159/000513329
20. Rogowski JA, Staiger DO, Patrick TE, Horbar JD, Kenny MJ, Lake ET. Nurse staffing in neonatal intensive care units in the United States. Res Nurs Health. (2016) 38(5):333–41. doi: 10.1002/nur.21674
21. Vento M, Cheung PY, Aguar M. The first golden minutes of the extremely-low-gestational-age neonate: a gentle approach. Neonatology. (2009) 95(4):286–98. doi: 10.1159/000178770
22. Barrington KJ. Management during the first 72 h of age of the periviable infant: an evidence-based review. Semin Perinatol. (2014) 38(1):17–24. doi: 10.1053/j.semperi.2013.07.004
23. de Cordova PB, Phibbs CS, Bartel AP, Stone PW. Twenty-four/seven: a mixed-method systematic review of the off-shift literature. J Adv Nurs. (2012) 68(7):1454–68. doi: 10.1111/j.1365-2648.2012.05976.x
24. Ohnstad MO, Stensvold HJ, Pripp AH, Tvedt CR, Jelsness-Jørgensen LP, Astrup H, et al. Predictors of extubation success: a population-based study of neonates below a gestational age of 26 weeks. BMJ Paediatr Open. (2022) 6(1):e001542. doi: 10.1136/bmjpo-2022-001542
25. Wiig S, Aase K, Billett S, Canfield C, Røise O, Njå O, et al. Defining the boundaries and operational concepts of resilience in the resilience in healthcare research program. BMC Health Serv Res. (2020) 20(1):1–9. doi: 10.1186/s12913-020-05224-3
26. Beltempo M, Lacroix G, Cabot M, Blais R, Piedboeuf B. Association of nursing overtime, nurse staffing and unit occupancy with medical incidents and outcomes of very preterm infants. J Perinatol. (2018) 2:1–6. doi: 10.1038/jp.2017.146
27. Beltempo M, Blais R, Lacroix G, Cabot M, Piedboeuf B. Association of nursing overtime, nurse staffing, and unit occupancy with health care-associated infections in the NICU. Am J Perinatol. (2017) 34(10):996–1002. doi: 10.1055/s-0037-1601459
28. Le Blanc G, Jabbour E, Patel S, Kazantseva O, Zeid M, Olivier F, et al. Organizational risk factors and clinical impacts of unplanned extubation in the NICU. J Pediatr. (2022) 249:14–21.e5. doi: 10.1016/j.jpeds.2022.06.012
29. Tubbs-Cooley HL, Mara CA, Carle AC, Mark BA, Pickler RH. Association of nurse workload with missed nursing care in the neonatal intensive care unit. JAMA Pediatr. (2019) 173(1):44–51. doi: 10.1001/jamapediatrics.2018.3619
30. Bell EF, Hansen NI, Morriss FH, Stoll BJ, Ambalavanan N, Gould JB, et al. Impact of timing of birth and resident duty-hour restrictions on outcomes for small preterm infants. Pediatrics. (2010) 126(2):222–31. doi: 10.1542/peds.2010-0456
31. Pauls L, Johnson-Paben R, McGready J, Murphy J, Pronovost P, Wu C. The weekend effect in hospitalized patients: a meta-analysis. J Hosp Med. (2017) 12(9):760–6. doi: 10.12788/jhm.2815
32. Kim S, Selya AS. Weekend delivery and maternal–neonatal adverse outcomes in low-risk pregnancies in the United States: a population-based analysis of 3-million live births. Birth. (2022) 49(3):549–58. doi: 10.1111/birt.12626
33. Rodrigo F G-M, Cruz L G, Henríquez G G, Martí L U, Rodríguez S R, García-Alix A, et al. Variations in the number of births by day of the week, and morbidity and mortality in very-low-birth-weight infants. J Pediatr (Rio J). (2019) 95(1):41–7. doi: 10.1016/j.jped.2017.10.006
34. Snowden JM, Kozhimannil KB, Muoto I, Caughey AB, McConnell KJ. A “busy day” effect on perinatal complications of delivery on weekends: a retrospective cohort study. BMJ Qual Saf. (2017) 26(1):1–9. doi: 10.1136/bmjqs-2016-005257
35. Gould JB, Qin C, Marks AR, Chavez G. Neonatal mortality in weekend vs weekday births. J Am Med Assoc. (2003) 289(22):2958–62. doi: 10.1001/jama.289.22.2958
36. Lee SK, Lee DSC, Andrews WL, Baboolal R, Pendray M, Stewart S. Higher mortality rates among inborn infants admitted to neonatal intensive care units at night. J Pediatr. (2003) 143(5):592–7. doi: 10.1067/S0022-3476(03)00367-6
37. Guy B, Dye ME, Richards L, Guthrie SO, Hatch LD. Association of time of day and extubation success in very low birthweight infants: a multicenter cohort study. J Perinatol. (2021) 41(10):2532–6. doi: 10.1038/s41372-021-01168-6
Keywords: extremely premature infants (EP infants), extubation, workload, weekend effect, resillience, mechanical ventilatioin
Citation: Ohnstad MO, Stensvold HJ, Pripp AH, Tvedt CR, Jelsness-Jørgensen L-P, Astrup H, Eriksen BH, Lunnay ML, Mreihil K, Pedersen T, Rettedal SI, Selberg TR, Solberg R, Støen R and Rønnestad AE (2023) Associations between unit workloads and outcomes of first extubation attempts in extremely premature infants below a gestational age of 26 weeks. Front. Pediatr. 11:1090701. doi: 10.3389/fped.2023.1090701
Received: 5 November 2022; Accepted: 27 February 2023;
Published: 17 March 2023.
Edited by:
Letizia Capasso, Federico II University Hospital, ItalyReviewed by:
Daniel Dirnberger, Alfred I. duPont Hospital for Children, United States© 2023 Ohnstad, Stensvold, Pripp, Tvedt, Jelsness-Jørgensen, Astrup, Eriksen, Lunnay, Mreihil, Pedersen, Rettedal, Selberg, Solberg, Støen and Rønnestad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mari Oma Ohnstad bWFyaS5vbWEub2huc3RhZEBsZGgubm8=
Specialty Section: This article was submitted to Neonatology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.