 N. Mand
N. Mand C. Donath
C. Donath A. Leonhardt1
A. Leonhardt1 M. Kömhoff
M. Kömhoff- 1Pediatric Intensive Care, Department of Pediatrics, Philipps-University Marburg, Marburg, Germany
- 2Pediatric Nephrology, Department of Pediatrics, Philipps-University Marburg, Marburg, Germany
Rhabdomyolysis is a challenging condition in pediatric emergency departments (PED): It ranges from asymptomatic illness with isolated elevation of creatine kinase (CK) levels to a life-threatening condition associated with extreme elevations in CK, electrolyte imbalances, circulatory failure (CF), acute kidney injury (AKI), and multi-organ disease. Most common causes of rhabdomyolysis are viral myositis and trauma, hereditary metabolic myopathies must be considered when facing rhabdomyolysis in early childhood. We report two cases of severe rhabdomyolysis with CF in our PED, thereby summarizing first-line management of rhabdomyolysis.
Introduction
Rhabdomyolysis (RM) is characterized by (skeletal) muscle necrosis and subsequent release of its intracellular contents including serum creatine kinase (CK), myoglobin, potassium, and phosphorus into the blood (1). This occurs either due to direct muscle cell membrane damage or as a result of cellular energy depletion (2, 3). In the pediatric population, two thirds of all cases are caused by viral myositis and trauma. Other typical causes include metabolic disorders, exercise, and drug overdose (1, 3, 4).
More than 25,000 pediatric and adult cases are reported annually in the US (5). The exact incidence of pediatric RM is unknown, with many mild cases probably going unrecognized (2, 6).
In adults, RM is defined as a clinical syndrome of acute muscle weakness, myalgia, and muscle swelling combined with a CK of >1,000 IU/L or higher than five times the upper limit of normal in the absence of significant elevations of brain or cardiac CK fractions (1, 7). There is a wide variation in the clinical presentation of RM (8). The level of CK, however, does not predict the severity of symptoms (4).
The most common symptoms in childhood are myalgia, weakness, and fever, up to one-third present with convulsions and/or reduced consciousness, while dark urine is rather rare (1, 4, 9). Infants and young children may present with nonspecific symptoms such as vomiting or apathy (9), thus making RM a challenging diagnosis in pediatric emergency departments (PED). Severe complications include electrolyte imbalances, circulatory failure (CF), disseminated intravascular coagulation, and hepatic dysfunction (8). Up to 10% of the patients develop acute kidney injury (AKI) (1, 4). A weak correlation between peak CK values and the incidence of AKI has been reported (10). In the absence of other significant risk factors such as sepsis the risk to develop AKI starts to increase above CK levels of 15.000 IU/L (10).
We report two cases of severe rhabdomyolysis with CF in our PED developing AKI necessitating renal replacement therapy further on.
Case presentations
Case 1
A previously healthy 4-year-old boy was introduced with malaise, fever, airway infection until 3 days ago, and myalgia. His mother reported increasing weakness, unwillingness to walk, decreasing diuresis and acute somnolence on the day of presentation. In the PED he showed signs of decompensated hypovolemic shock [CRT 4 s, HR 100 bpm, BP 72/28 (58) mmHg, GCS 10, Temp. 34.4°C]. Thus, 20 ml/kg crystalloids were infused manually within five minutes, and another 40 ml/kg crystalloids within the first hour on the PICU. The boy improved transiently. Capillary POCT analysis showed metabolic acidosis and hyperkalemia (pH 7.12, potassium 10.2 mmol/L, lactate 7.4 mmol/L, Hb 16.4 g/dl). Approximately 3 h after admission the patient went into ventricular tachycardia (VT) which was terminated with calcium gluconate within 2 min. Laboratory results confirmed hyperkalemia of 8 mmol/L and a CK > 100,000 U/L. Beyond that, inflammation markers were slightly, while liver enzymes were markedly elevated (AST 4,328 U/L), clotting was normal. Despite extensive conservative measures to treat hyperkalemia (bicarbonate, albuterol, and insulin-glucose-infusion) three more episodes of VT occurred. Therefore, continuous veno-venous hemofiltration (CVVH: Filter: FX50, Fresenius Medical Care, Bad Homburg, Germany; initial settings: bloodflow 60 ml/min, dialysis 2,500 ml/h) was initiated (serum creatinine at this point 0.65 mg/dl, urea 77 mg/dl, phosphate 3.2 mmol/L). In addition, catecholamine therapy with epinephrine, dopamine, and norepinephrine was begun due to persisting cardio-circulatory failure despite ongoing volume substitution with normal saline, human albumin, and fresh frozen plasma. The patient was intubated and pressure-controlled ventilated with NO due to developing clinical and radiological signs of ARDS (see Figure 1) (min. PaO2/FiO2 60; OI max. 38, max. PEEP 16 cm H2O, max. driving pressure 21 cm H2O). Sedation was initiated with midazolam and ketamine and sustained with midazolam and fentanyl. Broadband antibiotics were started.
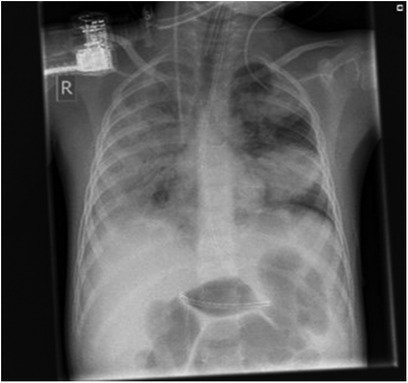
Figure 1. X ray case 1, twelve hours after admission.
During the following days, the boy's respiration and circulation stabilized while diuresis ceased on day 2. CK and myoglobin continued to increase till day 5 (max. CK 734,098 U/L, max. myoglobin 142,121 U/L, see Figure 2), and electrolytes normalized during CVVHDF. There were no further episodes of VT. Starting from day 4, catecholamines were slowly tapered, and respiratory weaning was begun. Initial hepatic dysfunction (max. AST 13,913 U/L on day 5) and intravascular coagulation normalized gradually. The boy was extubated on day 8, CVVHDF was discontinued on day 12 (max. serum creatinine 3.3 mg/dl), and he was then transferred to the pediatric ward. Intermittent HD was terminated on day 20 and retention parameters remained normal. With tailored exercise multiple times daily muscle weakness in arms and legs slowly decreased. The boy was discharged from the hospital on day 27, CK still being mildly elevated (791 U/L).
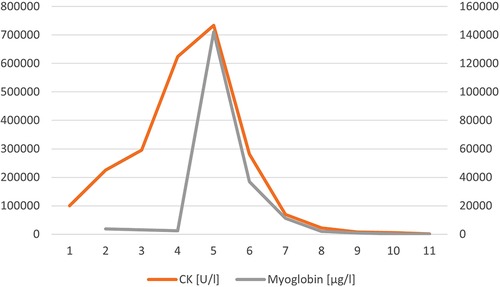
Figure 2. CK and myoglobin in case 1.
Influenza A was identified as the cause of this severe rhabdomyolysis via PCR-testing. Further extensive testing for other viruses, bacteria, drug toxins, and metabolic myopathies remained negative.
So far, the boy did not redevelop any other RM episode. Being 8 years now, renal function is normal, he has no cognitive or motoric impairments, and he is attending a regular school and is playing soccer several times a week.
Case 2
An 11-month-old male infant with a known motor development delay but otherwise healthy was admitted to the PED with recurrent vomiting over the last two days. No fever was reported, but mild diarrhea, and increasingly dry diapers. Physical examination revealed an ubiquitous sensitivity to touch and signs of a hypovolemic shock [HR 156 bpm, BP 112/66 (87) mmHg, RR 64 pm, Temp. 36.5°C, GCS 11]. Arterial POCT analysis revealed normokalemia with respiratory compensated metabolic acidosis (pH 7.4, pCO2 28 mmHg, HCO3 17.5 mmol/L, BE −5.5 mmol/L, potassium 4.9 mmol/L). Laboratory results showed markedly elevated CK and liver enzymes (CK 343,030 U/L, AST 9,365 U/L, see Figure 3). Despite volume substitution with 50 ml/kg crystalloids and normal saline anuria persisted and continuous veno-venous hemofiltration (CVVH: Filter: FX40, Fresenius Medical Care; initial settings: bloodflow 60 ml/min, dialysis 2,500 ml/h) was started on day 2 when CK was peaking (max. 556,386 U/L). Additionally, alkalinization of urine was achieved with bicarbonate. Serum creatinine, urea, and electrolytes stayed normal throughout the hospital stay, while CK and myoglobin decreased gradually. CVVHF was discontinued on day 12 when adequate diuresis was re-established. During recovery, CK-levels dropped markedly, but did not normalize completely. The patient was discharged with slightly elevated CK (1,673 U/L) on day 17; subsequently, CK levels peaked maximally 1,500 U/L during febrile disease. A metabolic myopathy was suspected and genetic alterations consistent with compound heterozygeous, pathogenic mutations in LPIN1, causing acute, recurrent rhabdomyolysis (OMIM #268200) were detected in the patient and his parents: Sequencing of DNA from the patient and his parents revealed a pathogenic splice site mutation (c.2513 + 1G > A) in the patient and his mother but none in the father. Due to the high degree of suspicion of a second mutation in LPIN1 in the patient and hence possibly also in his father, mRNA sequencing from RNA isolated from paternal fibroblast were performed. This approach revealed that exon 3 of LPIN1 was reduced by approximately 50%, resulting from a cryptic splice site mutation in LPIN1. Importantly, in the second child of the family who carries the maternal mutation, mRNA sequencing excluded a splicing defect. A third child was conceived without mutation in LPIN1 following preimplantation genetic diagnosis.
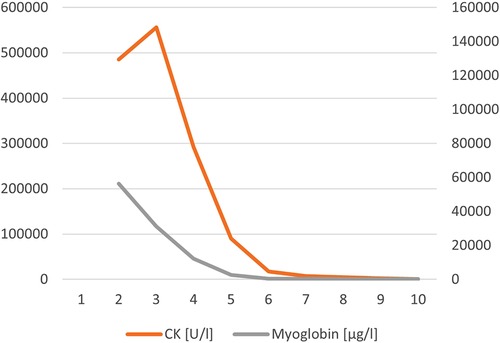
Figure 3. CK and myoglobin in case 2
Children bearing bi-allelic mutations in LPIN1 which encodes an enzyme important in the pathway of triglyceride and phospholipid biosynthesis, are prone to recurrent bouts of rhabdomyolysis especially in states of catabolic stress but sometimes also without overt precipitating factors (11). The parents were instructed to administer an oral carbohydrate-electrolyte-rehydration-solution whenever fever or fasting occurred. At 2.5 years of age, while on holiday, another episode with rapid deterioration occurred in our patient resulting in cardiac arrest. Due to massive spasms of the masseter, airway securement was not possible. The boy died after 60 min of unsuccessful cardiopulmonary resuscitation.
Discussion
Rhabdomyolysis in children has a broad spectrum of causes and severity and is potentially life-threatening. The heterogeneity of its symptoms makes it a challenging condition to diagnose and treat in the PED (2, 4).
Besides trauma, infections are the main cause of rhabdomyolysis in children, with mycoplasma spp. and different viruses such as influenza, enteroviruses, and SARS-CoV-2 being known triggers (1, 4, 12, 13). In our first case, influenza A was identified, which is the most common viral trigger for RM (1). Influenza-associated myositis is mostly a benign complication and typically occurs, when symptoms of influenza are about to resolve (14). A progression into RM should be suspected if muscle pain is worsening or severe enough to discourage walking (see Table 1) (14, 15). The classic triad of RM-symptoms including muscle pain, weakness, and dark urine is rarely seen in children (1, 4, 9). Especially infants and young children present atypically with fever, vomiting, and convulsions, thus being at risk of being misdiagnosed as simple gastroenteritis or, if symptoms are more severe, an intracranial infection (9). In our second case gastroenteritis causing hypovolemic shock was suspected initially. Routine laboratory results revealed markedly elevated CK and liver enzymes, thus prompting investigations for a hereditary metabolic myopathy. Any episode of severe RM, especially in infants or recurrent episodes of RM triggered by minimal exercise at any age should be a reason to suspect hereditary diseases (9, 16, 17). Genetic causes of RM include metabolic muscle disorders (e.g., fatty acid metabolism disorders or abnormal glycogen storage), mitochondrial disorders, disorders of intramuscular calcium release, and muscular dystrophies (16, 18). With autosomal-recessive mutations in the LPIN1 gene causing intracellular energy deficiency with severe RM episodes poor prognosis and high mortality have been reported (16–18). As a frequent cause of early-onset RM LPIN1-mutation was detected in our second case subsequently.
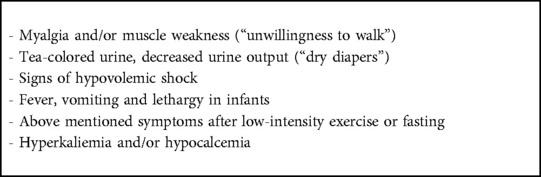
Table 1. Clinical suspicion for rhabdomyolysis (“red flags”) that should prompt evaluation of CK.
In both patients lethargy and severe hypovolemia were the leading symptoms prompting initial therapy. Significantly elevated CK, myoglobin and liver enzymes were detected in routine laboratory results. In one patient POCT analysis revealed typical electrolyte disbalances thus determining the subsequent therapeutic approach. The pathological hallmark of RM is necrosis of muscle cells due to an insult to the cell's membrane or cellular energy depletion (2). This is contrary to myositis, where the muscle is inflamed but cell walls remain intact. Compromised cell integrity leads to the leakage of cellular contents into the circulatory system and energy deficiency on electrolyte transporters (e.g., Na+/Ca2+ or Na+/K+ exchanger) leads to massive shifting of electrolytes (2, 8). Initially, serum levels of potassium and phosphate increase as these components are released from the cells, and serum concentrations of calcium are decreased as calcium moves into the cells aggravating the destruction of cell membranes (2, 8). Intracellular proteins (CK, myoglobin, lactate dehydrogenase (LDH), aminotransferase (AST), aldolase) are released into the bloodstream (6, 8). CK typically rises within 12 h of the onset of muscle injury, peaks within 1–3 days, and declines 3–5 days after the cessation of muscle injury (8). Unlike haemoglobin, which is avidly bound by haptoglobin, myoglobin levels rapidly exceed the unspecific protein-binding capacity of plasma, resulting in a dark red-brown colored urine and precipitation in the glomerular filter, thus facilitating AKI (6, 10).
AKI is a major mortality factor in children with or without RM (10, 19). Children with AKI as a component of multisystem failure have a much higher mortality rate than children with intrinsic renal disease (20, 21). In critically ill children severe AKI occurs in up to 15% (21, 22). Reported incidence in children with RM highly varies, rates between 5% and 42% have been described (1, 10, 23). Sequestration of water in injured muscles initiates volume depletion (10, 24). Clinical findings like dry mucous membrane, decreased skin turgor, sunken anterior fontanelle, tachycardia, or hemoconcentration should prompt fluid therapy, as AKI is more likely to develop in the presence of dehydration (10, 25). In addition, precipitating myoglobin and myoglobin-mediated tubular cytotoxicity, renal vasoconstriction/hypoperfusion as a result of circulatory impairment and consequent metabolic acidosis is probably contributing to AKI (25). Positive urinary heme dipstick results are an earlier indicator of potential AKI than creatinine and urea might be (1, 10), CK-levels being an indicator for AKI only in adult traumatic RM (4, 26). Attempts to remove myoglobin via extracorporeal therapy before AKI has established were successful in case reports (27, 28), but its benefits could not be clearly confirmed in large trials (10). This notion is supported by a recently published trial describing the effects of high cutoff vs. conventional renal replacement therapy in 70 adults with AKI and rhabdomyolysis. Even though myoglobin clearance with continuous veno-venous hemodialysis using high cutoff dialyzer was significantly higher compared to control, there was no clinical benefit and ICU-mortality was even significantly higher in the “high cutoff” group (29).
Hence, irrespective of the underlying aetiology, the main therapeutic intervention in rhabdomyolysis is the aggressive administration of intravenous fluid to avoid circulatory failure (CF) and AKI (see Table 2) (4). In children with recognized shock volume resuscitation with one or more early fluid boluses of 10 ml/kg crystalloids have to be performed, up to 60 ml/kg might be needed in the first hour of treatment (30). Reassessments after each bolus are aimed at early recognition of circulatory improvement or signs of fluid overload and cardiac failure (30). Severely volume-depleted children might need up to 100 ml/kg fluids within the first 8 h of presentation (30). As long as kidney function is intact, volume therapy after resolution of hypovolemic shock is aimed at a high urine output to dilute and eliminate the heme protein; diuretics are applied in states of volume overload (24, 28).
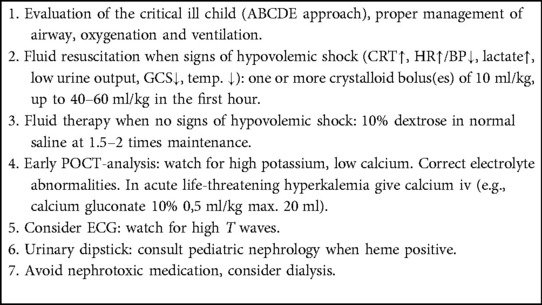
Table 2. Rhabdomyolysis treatment in the PED.
There is conflicting evidence on use of mannitol and sodium bicarbonates to alkalinize the urine (24). Myoglobin excretion is enhanced at a urine pH of 8.0 (31). However, studies in children are lacking (1, 24). Sodium bicarbonate (1 mmol/kg IV, repeat as necessary) should be used in the presence of hyperkalemia and metabolic acidosis (pH < 7.2), though, the effect is slow (30). In life-threatening hyperkalemia intravenous calcium (e.g., calcium gluconate 10% 0.5 ml/kg, max. 20 ml) is administered, the effect occurring within minutes and lasting for up to an hour. Insulin-glucose-infusion and nebulized beta-agonists are additional conservative measures to decrease potassium levels (30). Hyperkalemia as the first “red flag” of increased cell turnover can be easily detected in POCT analyses but may not be present initially. ECG abnormalities such as high-amplitude T waves can precede hyperkalemia, especially in hereditary myoglobinuria and should prompt aggressive treatment without delay. Progression to critical hyperkalemia initiates cardiac dysrhythmias and possibly cardiac arrest (2, 8, 17). Other potentially lethal electrolyte disturbance such as hypocalcemia or severe metabolic acidosis should be corrected as early as possible (4, 24).
In hereditary metabolic disorders, such as in autosomal recessive recurrent myoglobinuria caused by gene mutations in LPIN1 (OMIM *605518) presented by case 2, the intramuscular energy deficiency that is associated with RM is effectively treated by hyperhydration and energy supply, using high-concentration glucose-solutions next to crystalloids (32). Consequently, parents should be instructed to maintain a high caloric intake in situations with increased energy demand (32, 33). Concomitantly, dexamethasone can be successfully added in the standard treatment (33).
Conclusion
Rhabdomyolysis can present as a life-threatening condition in the pediatric emergency department. Patients with a history of myalgia and/or muscle weakness, a decreased urinary output or with signs of hypovolemic shock should prompt an evaluation for CK. Hyperkalemia as the first “red flag” of RM can be easily detected in POCT analyses, which should be performed early in every critical patient. Urinary dipstick is an easily available and non-invasive screening test for the identification of patients who need monitoring of renal function (1, 34). In children, rhabdomyolysis is most commonly caused by viral disease or trauma (1). Nevertheless, genetic disorders such as hereditary metabolic myopathies have to be excluded especially if the first episode occurs in early childhood or in subjects with extremely elevated CK values (18). Until the establishment of a genetic diagnosis, which is critical because of the high risk of recurrence, and upon confirmation of a genetic diagnosis, respectively, sufficient administration of carbohydrates and fluids in myoglobulin precipitating conditions (febrile disease, fasting, strenuous exercise) is potentially lifesaving.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
Conceptualisation: NM, MK. Original draft preparation: NM. Review and editing: CD, AL, SW, MK. Supervision: MK. All authors contributed to the article and approved the submitted version.
Funding
Open Access funding provided by the Open Access Publishing Fund of Philipps-Universität Marburg with support of the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mannix R, Tan ML, Wright R, Baskin M. Acute pediatric rhabdomyolysis: causes and rates of renal failure. Pediatrics. (2006) 118(5):2119–25. doi: 10.1542/peds.2006-1352
2. Szugye HS. Pediatric rhabdomyolysis. Pediatr Rev. (2020) 41(6):265–75. doi: 10.1542/pir.2018-0300
3. Torres PA, Helmstetter JA, Kaye AM, Kaye AD. Rhabdomyolysis: pathogenesis, diagnosis, and treatment. Ochsner J. (2015) 15(1):58–69.25829882
4. Chen CY, Lin YR, Zhao LL, Yang WC, Chang YJ, Wu KH, Wu HP. Clinical spectrum of rhabdomyolysis presented to pediatric emergency department. BMC Pediatr. (2013) 13:134. doi: 10.1186/1471-2431-13-134
6. Zutt R, van der Kooi AJ, Linthorst GE, Wanders RJA, de Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. (2014) 24(8):651–9. doi: 10.1016/j.nmd.2014.05.005
7. Stahl K, Rastelli E, Schoser B. A systematic review on the definition of rhabdomyolysis. J Neurol. (2020) 267(4):877–82. doi: 10.1007/s00415-019-09185-4
8. Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: rhabdomyolysis – an overview for clinicians. Crit Care. (2005) 9(2):158–69. doi: 10.1186/cc2978
9. Yao Z, Yuan P, Hong S, Li M, Jiang L Clinical features of acute rhabdomyolysis in 55 pediatric patients. Front Pediatr. (2020) 8:539. doi: 10.3389/fped.2020.00539
10. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. (2009) 361(1):62–72. doi: 10.1056/NEJMra0801327
11. Zeharia A, Shaag A, Houtkooper RH, Hindi T, de Lonlay P, Erez G, et al. Mutations in LPIN1 cause recurrent acute myoglobinuria in childhood. Am J Hum Genet. (2008) 83(4):489–94. doi: 10.1016/j.ajhg.2008.09.002
12. Kontou M, Kakleas K, Kimioni V, Georgiadi D, Spoulou V, Michos A. Rhabdomyolysis and coronavirus disease-2019 in children: a case report and review of the literature. Pediatr Investig. (2022) 6(2):135–9. doi: 10.1002/ped4.12320
13. Soliman A, Bisht S, Jeyamurugan K, Blasundaram P, Basak R. Severe rhabdomyolysis in a pediatric patient after coxsackie B virus infection without acute renal failure: a case report. Cureus. (2020) 12(2):e7126. doi: 10.7759/cureus.7126
14. Agyeman P, Duppenthaler A, Heininger U, Aebi C. Influenza-associated myositis in children. Infection. (2004) 32(4):199–203. doi: 10.1007/s15010-004-4003-2
15. Skellett SC, Dhesi R. Myositis, rhabdomyolysis and compartment syndrome complicating influenza A in a child. BMJ Case Rep. (2009) 2009. doi: 10.1136/bcr.07.2009.2099
16. Scalco RS, Gardiner AR, Pitceathly RDS, Znoteli E, Becker J, Holton JL, et al. Rhabdomyolysis: a genetic perspective. Orphanet J Rare Dis. (2015) 10:51. doi: 10.1186/s13023-015-0264-3
17. Bergounioux J, Brassier A, Rambaud C, Bustarret O, Michot C, Hubert L, et al. Fatal rhabdomyolysis in 2 children with LPIN1 mutations. J Pediatr. (2012) 160(6):1052–4. doi: 10.1016/j.jpeds.2012.02.033
18. Michot C, Hubert L, Brivet M, De Meirleir L, Valayannopoulos V, Müller-Felber W, et al. LPIN1 Gene mutations: a major cause of severe rhabdomyolysis in early childhood. Hum Mutat. (2010) 31(7):E1564–73. doi: 10.1002/humu.21282
19. Andreoli SP. Management of acute kidney injury in children: a guide for pediatricians. Paediatr Drugs. (2008) 10(6):379–90. doi: 10.2165/0148581-200810060-00005
20. Lameire N, Van Biesen W, Vanholder R. Epidemiology of acute kidney injury in children worldwide, including developing countries. Pediatr Nephrol. (2017) 32(8):1301–14. doi: 10.1007/s00467-016-3433-2
21. Kaddourah A, Basu R, Goldstein S, Sutherland S. Oliguria and acute kidney injury in critically ill children: implications for diagnosis and outcomes*. Pediatr Crit Care Med. (2019) 20(4) 332–339. doi: 10.1097/PCC.0000000000001866
22. Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL. Epidemiology of acute kidney injury in critically ill children and young adults. N Engl J Med. (2017) 376(1):11–20. doi: 10.1056/NEJMoa1611391
23. Watemberg N, Leshner RL, Armstrong BA, Lerman-Sagie T. Acute pediatric rhabdomyolysis. J Child Neurol. (2000) 15(4):222–7. doi: 10.1177/088307380001500404
24. Elsayed EF, Reilly RF. Rhabdomyolysis: a review, with emphasis on the pediatric population. Pediatr Nephrol. (2010) 25(1):7–18. doi: 10.1007/s00467-009-1223-9
25. Watanabe T. Rhabdomyolysis and acute renal failure in children. Pediatr Nephrol. (2001) 16(12):1072–5. doi: 10.1007/s004670100030
26. Safari S, Yousefifard M, Hashemi B, Baratloo A, Forouzanfar MM, Rahmati F, et al. The value of serum creatine kinase in predicting the risk of rhabdomyolysis-induced acute kidney injury: a systematic review and meta-analysis. Clin Exp Nephrol. (2016) 20(2):153–61. doi: 10.1007/s10157-015-1204-1
27. Rauch S, Borgato A, Gruber E, Leggieri C, Bock M, Seraglio PME. Case report: prevention of rhabdomyolysis-associated acute kidney injury by extracorporeal blood purification with cytosorb®. Front Pediatr. (2021) 9:801807. doi: 10.3389/fped.2021.801807
28. Hui WF, Hon KL, Lun KS, Leung KKY, Cheung WL, Leung AKC. Successful treatment of rhabdomyolysis-associated acute kidney injury with haemoadsorption and continuous renal replacement therapy. Case Rep Pediatr. (2021) 2021:2148024. doi: 10.1155/2021/2148024
29. Weidhase L, de Fallois J, Haußig E, Kaiser T, Mende M, Petros S. Myoglobin clearance with continuous veno-venous hemodialysis using high cutoff dialyzer versus continuous veno-venous hemodiafiltration using high-flux dialyzer: a prospective randomized controlled trial. Crit Care. (2020) 24(1):644. doi: 10.1186/s13054-020-03366-8
30. Van de Voorde P, Turner NM, Djakow J, de Lucas N, Martinez-Mejias A, Biarent D, et al. European resuscitation council guidelines 2021: paediatric life support. Resuscitation. (2021) 161:327–87. doi: 10.1016/j.resuscitation.2021.02.015
31. Zager RA. Studies of mechanisms and protective maneuvers in myoglobinuric acute renal injury. Lab Invest. (1989) 60(5):619–29.2716281
32. Pichler K, Scholl-Buergi S, Birnbacher R, Freilinger M, Straub S, Brunner J, et al. A novel therapeutic approach for LPIN1 mutation-associated rhabdomyolysis–the Austrian experience. Muscle Nerve. (2015) 52(3):437–9. doi: 10.1002/mus.24749
33. Summerlin ML, Regier DS, Fraser JL, Chapman KA, Kafashzadeh D, Billington C, et al. Use of dexamethasone in idiopathic, acute pediatric rhabdomyolysis. Am J Med Genet A. (2021) 185(2):500–7. doi: 10.1002/ajmg.a.62000
Keywords: rhabdomyolysis, hereditary metabolic disease, LPIN1 mutation, circulatory failure, acute kidney injury (AKI)
Citation: Mand N, Donath C, Leonhardt A, Weber S and Kömhoff M (2023) Case report: Rhabdomyolysis in children in acute and chronic disease—a challenging condition in pediatric emergency medicine. Front. Pediatr. 11:1070465. doi: 10.3389/fped.2023.1070465
Received: 14 October 2022; Accepted: 17 February 2023;
Published: 9 March 2023.
Edited by:
Emmanuel Schneck, University of Giessen, GermanyReviewed by:
Christoph Neuhäuser, Independent Researcher, Hüttenberg, GermanyHolger Hauch, Justus Liebig University, Germany
© 2023 Mand, Donath, Leonhardt, Weber and Kömhoff. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: N. Mand mandn@staff.uni-marburg.de
Specialty Section: This article was submitted to General Pediatrics and Pediatric Emergency Care, a section of the journal Frontiers in Pediatrics