
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 27 February 2023
Sec. Pediatric Cardiology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1044352
This article is part of the Research Topic Kawasaki Disease: An Ongoing Enigma Tangled With the Appearance of MIS-C View all 8 articles
 Michaela Semeraro1,2*
Michaela Semeraro1,2* Pierre Pinson2,3
Pierre Pinson2,3 Margaux Populaire1Mourad Dellagi2,3
Margaux Populaire1Mourad Dellagi2,3 Mehdi Oualha2,3,4Nathanael Beeker2,3Hélène Chappuy2,3,4,5and on behalf of AP-HP/Universities/INSERM COVID-19 research collaboration and AP-HP COVID CDR Initiative†
Mehdi Oualha2,3,4Nathanael Beeker2,3Hélène Chappuy2,3,4,5and on behalf of AP-HP/Universities/INSERM COVID-19 research collaboration and AP-HP COVID CDR Initiative†
Background: The clinical characteristics, disease progression and outcome in children affected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection appear significantly milder compared to older individuals. Nevertheless, the trends in hospitalization and clinical characteristics in the pediatric population seem to be different over time across the different epidemic waves.
Objective: Our aim was to understand the impact of the different COVID-19 variants in the pediatric population hospitalized in the Pediatric Departments of the Public Hospital in the Greater Paris area by the analysis performed with the Assistance Publique-Hopitaux de Paris (AP-HP) Health Data Warehouse.
Methods: This is a retrospective cohort study including 9,163 patients under 18 years of age, hospitalized from 1 March 2020 to 22 March 2022, in the Paris area, with confirmed infection by SARS-CoV-2. Three mutually exclusive groups with decreasing severity (Pediatric Inflammatory Multisystem Syndrome (PIMS), symptomatic infection, mild or asymptomatic infection) were defined and described regarding demography, medical history, complication of the SARS-CoV-2 infection, and treatment during admission. Temporal evolution was described by defining three successive waves (March–September 2020, October 2020–October 2021, and November 2021–March 2022) corresponding to the emergence of the successive variants.
Results: In the study period, 9,163 pediatric patients with SARS-CoV-2 infection were hospitalized in 21 AP-HP hospitals. The number of patients with SARS-CoV-2 infection increased over time for each wave of the pandemic (the mean number of patients per month during the first wave was 332, 322 during the 2nd, and 595 during the third wave). In the medical history, the most associated concomitant disease was chronic respiratory disease. Patients hospitalized during the third wave presented a higher incidence of pulmonary involvement (10.2% compared to 7% and 6.5% during the first and second waves, respectively). The highest incidence of PIMS was observed during the first and second waves (4.2% in the first and second waves compared to 2.3% in the 3rd wave).
Discussion: This analysis highlighted the high incidence of hospitalized children in the Greater Paris Area during the third wave of SARS-CoV-2 pandemic corresponding to the Omicron Covid-19 variant, which is probably an expression of a concomitant SARS-CoV-2, while a decreased incidence of PIMS complication was observed during the same period.
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic was declared by the World Health Organization on 11 March 2020. Since this time, several waves of infections related to specific variants of the SARS-CoV-2 have emerged. These variants are due to the virus's acquired additional advantageous mutations, potentially altering transmissibility, severity, and escape from natural or vaccine-derived immunity.
Compared to adults, SARS-CoV-2 infection in the children population presented different characteristics and courses (1–3). First data from China suggested that pediatric COVID-19 infections might be less severe than cases in adults, and children might experience different symptoms than adults (4).
In this regard, specific characteristics and consequences of the pandemic in young patients have been described. First of all, since the beginning of the pandemic, several countries reported cases of a rare Pediatric Inflammatory Multisystem Syndrome temporally associated with SARS-CoV-2 (PIMS-TS) also named Multisystem Inflammatory Syndrome in Children (MIS-C), characterized by Kawasaki-like symptoms and toxic shock syndrome (5–7).
The impact of the variants on the clinical courses in adult patients is well known (i.e., the Omicron-variant surge has been characterized by a mild severity of the disease compared to the Delta variant infection (8)), but little is known about the different patterns of clinical characteristics and outcomes in pediatric patients according to the different surges of infection.
The aim of this study was to understand the impact of the COVID-19 variants in the pediatric population presenting with SARS-CoV2 infection hospitalized in the Public Hospitals of the Paris metropolitan area over the different surges of the pandemic and particularly during the last Omicron variant.
The Assistance Publique–Hôpitaux de Paris (AP-HP) is the largest hospital entity in Europe, with 39 hospitals (22,474 beds) mainly located in the Greater Paris area.
This retrospective cohort study was conducted using the Assistance Publique-Hopitaux de Paris (AP-HP) Health Data Warehouse (Entrepôt de Données de Santé (EDS), https://eds.aphp.fr/; AP-HP Covid Clinical Data Warehouse (CDW)). This data warehouse contains electronic health records (EHRs) of all inpatients from the 39 greater Paris university hospitals. The clinical data repository has received authorization from the French Data Protection Authority (Commission Nationale de l'Informatique et des Libertés, number 1980120).
As such, the members of the AP-HP Covid CDW initiative contributed to the design and implementation of the database but did not participate in the analysis or writing of this report. A complete listing of members can be found at https://eds.aphp.fr/covid-19.
This analysis follows recommendations provided by the Reporting of Studies Conducted Using Observational Routinely Collected Health Data Statement (9).
This study was approved by the institutional review board (N° CSE: CSE 20–48_COVIDPed; AP-HP CDW Scientific and Ethics Committee number IRB00011591) of the scientific and ethical committee of the AP-HP. All subjects included in this study were informed about the reuse of their data for research, and subjects who objected to the reuse of their data were excluded from this study in accordance with French legislation.
We retrospectively retrieved the data of all patients with COVID-19 infection hospitalized in one of the AP-HP hospitals between March 2020 and March 2022 from the EDS-COVID database.
Inclusion criteria were:
1. Full hospitalization in one of the AP-HP pediatric departments between 1 March 2020 and 22 March 2022.
2. SARS-CoV-2 positive diagnosis and/or PIMS diagnosis according to the International Classification of Diseases (ICD-10 code) related to the hospitalization or positive SARS-CoV2 PCR test between 5 days prior to the start of the hospitalization and 15 days after.
3. Minor patient (<18 years old) at the time of hospitalization.
Comorbidities were extracted from ICD-10 codes used during the previous hospitalizations of each patient if available. Outcomes and treatments during hospitalization were obtained from the current hospitalization codes (ICD-10 and technical treatment French codification-CCAM). PIMS outcome code screening was extended up to 28 days after the start of hospitalization considering the delay between SARS-CoV-2 infection and PIMS described in the literature (10). Correspondence between variables and codes is presented in Supplementary Material Table S2.
Age at admission, sex, intensive care unit (ICU) admission, and death during hospitalization were obtained from the hospital administrative data.
Data are presented as mean (standard deviation) and numbers (%).
The study population comprised three retrospective cohorts:
Cohort 1: Patients who had their first SARS-CoV-2 infections or PIMS between March 2020 to September 2020 corresponding to the emergent first historical variant cohort.
Cohort 2: Patients hospitalized during the second wave, October 2020 to October 2021, including the emergent Delta and Alpha/Beta/Gamma variant cohorts in addition to the cohort of patients without a determined variant type.
Cohort 3: Patients hospitalized during the third wave, November 2021 to February 2022, corresponding to the Delta and Omicron variant cohorts and patients with a non-determined variant.
For the analysis of the population, we defined three mutually excluded groups with decreasing severity. The first group was represented by pediatric patients with PIMS diagnosis or acute myocarditis. The second group was represented by pediatric patients with a principal diagnosis of SARS-CoV-2 infection, and the third group was defined by a positive PCR test or secondary diagnosis of SARS-CoV2, referred to as clinically mild or asymptomatic infection group.
To assess the differences between waves, we performed chi-squared tests, first on the PIMS distribution within the population, then on the symptomatic SARS-CoV2 within the population, with a significance level of 5%. For each cohort, we performed chi-squared or one-way ANOVA test when appropriate, to compare covariates across waves.
A total of 9,163 pediatric patients hospitalized across 21 APHP hospitals with SARS-CoV-2 infection were included between March 2020 and March 2022: 2,325 patients were included in cohort 1 (mean number of patients detected per month: 332), 3,861 were included in cohort 2 (mean number of patients detected per month: 322), and 2,977 in cohort 3 (mean number of patients detected per month: 595).
Variant genotyping was automatically assigned to the historical variant for the forst wave period, while was available (the varian genotyping for 787 patients (9%) of the patients detected during the second and third waves (Figure 1). In more detail, in the second cohort, 92 patients presented with the emergent Delta variant cohort, 986 presented with the first historical variant cohort, and 176 patients presented with the Alpha/Beta/Gamma variant while the variant was not available for 2,607 patients. In the third cohort, 411 presented with the Omicron variant and 108 the Delta variant. The rest of the cohort was made up of patients with a non-determined variant.
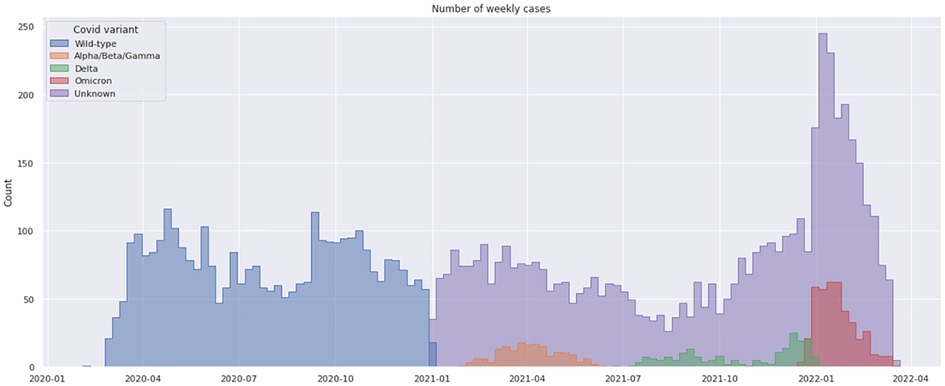
Figure 1. Weekly distribution of SARS-CoV2 cases variant genotyping in children hospitalized in the public hospital in the greater Paris area (AP-HP) from march 2020 to march 2022.The blue and violet bars represent the number of cases; the orange, green, and red bars represent the alpha-beta-gamma, delta, and omicron detected genotyping, respectively. For the first wave period (March 2020- Dec 2020) the genotyping was assigned to the historical variant (wild type).
Distribution according to age group is detailed in Table 1. Children between the age of 28 days and 5 years were the most represented in all periods. During the first wave, the least represented age group was patients younger than 28 days old (13.8%), whereas the proportion of this group increased during the other two surges (17.6% and 15.6%, respectively). Globally, the average patient's age decreased throughout the pandemic.
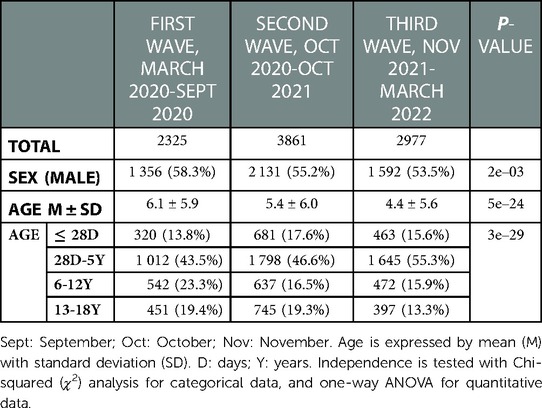
Table 1. Demography of the pediatric population analyzed.
Characteristics of the three study groups are described in tables 2 to 4.
For study group 1, we collected data for PIMS and isolated myocarditis (PIMS/M) occurring after SARS-Cov2 infection (PIMS/M group) (Table 2). Focusing on this group, we observed that the highest number of these complications were registered during the first and second waves (incidence of 4.2%, 4.2%, and 2.4%, respectively, p = 3e-4). The PIMS/M patients were mostly within the age group of 5 to 12 years in all the three periods.
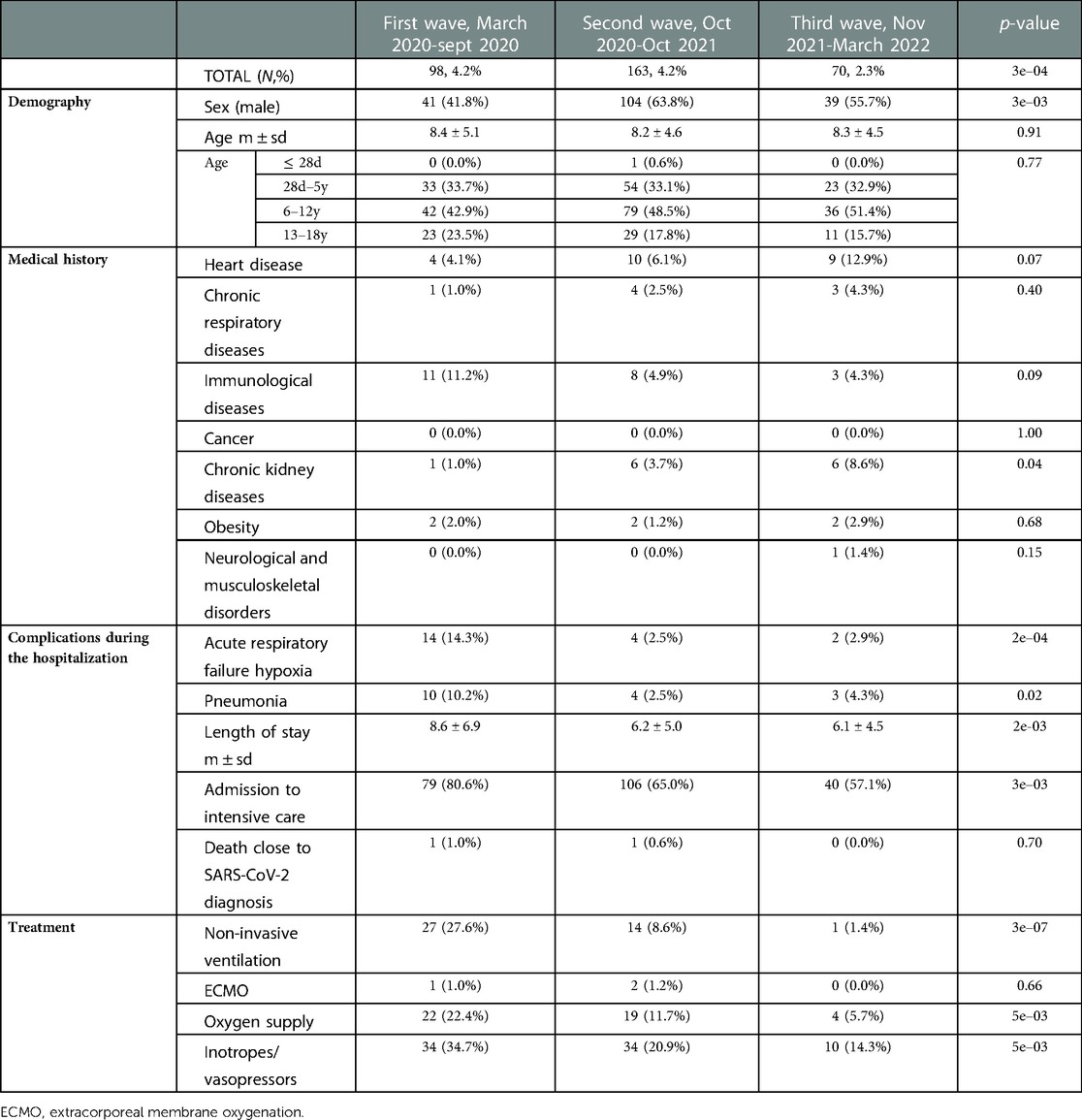
Table 2. Characteristics of pediatric patients hospitalized with pediatric inflammatory multisystem syndrome (PIMS) or acute myocarditis after SARS-Cov2 infection.
The analysis of the clinical characteristics of this group of patients showed that respiratory distress occurred mostly during the first wave (14.3%) compared to the 2 other periods (2.5 and 2.9%, respectively). The third wave was characterized by a lower resort to active respiratory treatments (ventilator support, oxygen support, etc.) compared to the previous surges (i.e., non-invasive ventilation utilized for 27.6% of the patients during the first wave compared to 1.4% during the third wave). Only 57.1% of these patients were admitted to the intensive care (IC) department during the third wave while 80.6% and 65% were hospitalized in the IC unit during the first and second waves, respectively. The percentage of patients who needed inotrope support during the last SARS-Cov2 wave amounted to 14.3% compared to 34.7% of patients during the first wave.
The most represented underlying comorbidities in the personal medical history of pediatric patients presenting PIMS/M were immunologic diseases and cardiac diseases during the first wave (11.2% and 4.1%, respectively), while during the second and third waves, underlying cardiac diseases were the most represented comorbidities (6.1% and 12.9%, respectively), followed by immunologic diseases during the second wave (4.9%) and chronic kidney disease during the third wave (8.6%). Interestingly, during the third wave, the incidence of PIMS/M patients with a history of respiratory diseases increased compared to the other periods (4.3% vs. 1% and 2.5%).
Only two patients hospitalized in one of the AP-HP hospitals presenting PIMS/M died during the pandemic (during the first and second waves).
The number of patients hospitalized with a primary diagnosis of SARS-CoV2 infection (group 2) increased over time as 132 (5.6%), 308 (7.9%), and 442 (14.8%) patients were detected in the three periods of the pandemic (p = 1e-25), however, the specific respiratory symptoms decreased as well as admission to the intensive care department (Table 3).
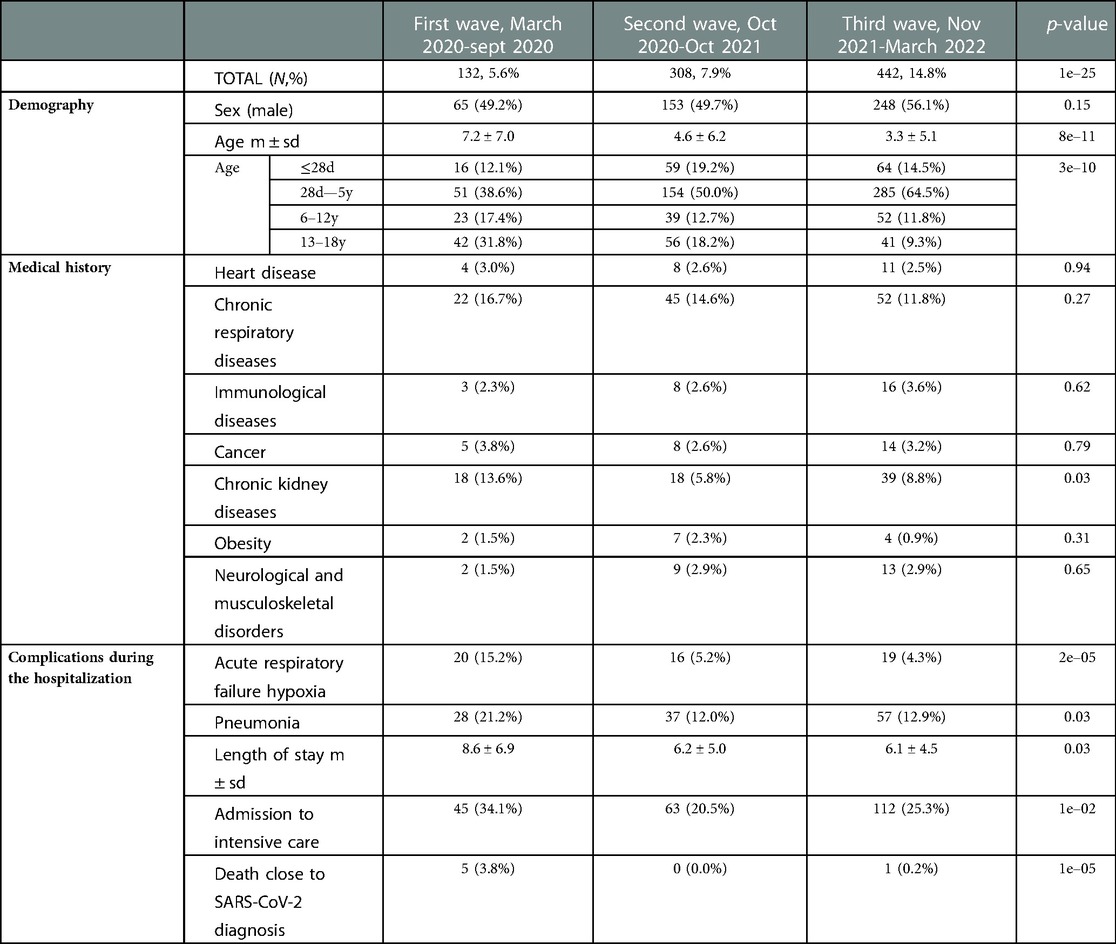
Table 3. Characteristics of pediatric patients hospitalized with a principal diagnosis of SARS-CoV-2 infection.
The most represented cohort was pediatric patients with mild or asymptomatic SARS-CoV-2 infection. This third group was homogenously well represented in all the periods (Table 4). As in symptomatic SARS-Cov2 patients, most of the patients detected in this group were between the age of 28 days to 5 years old in the three periods. The proportional number of patients in this age group increased over time.
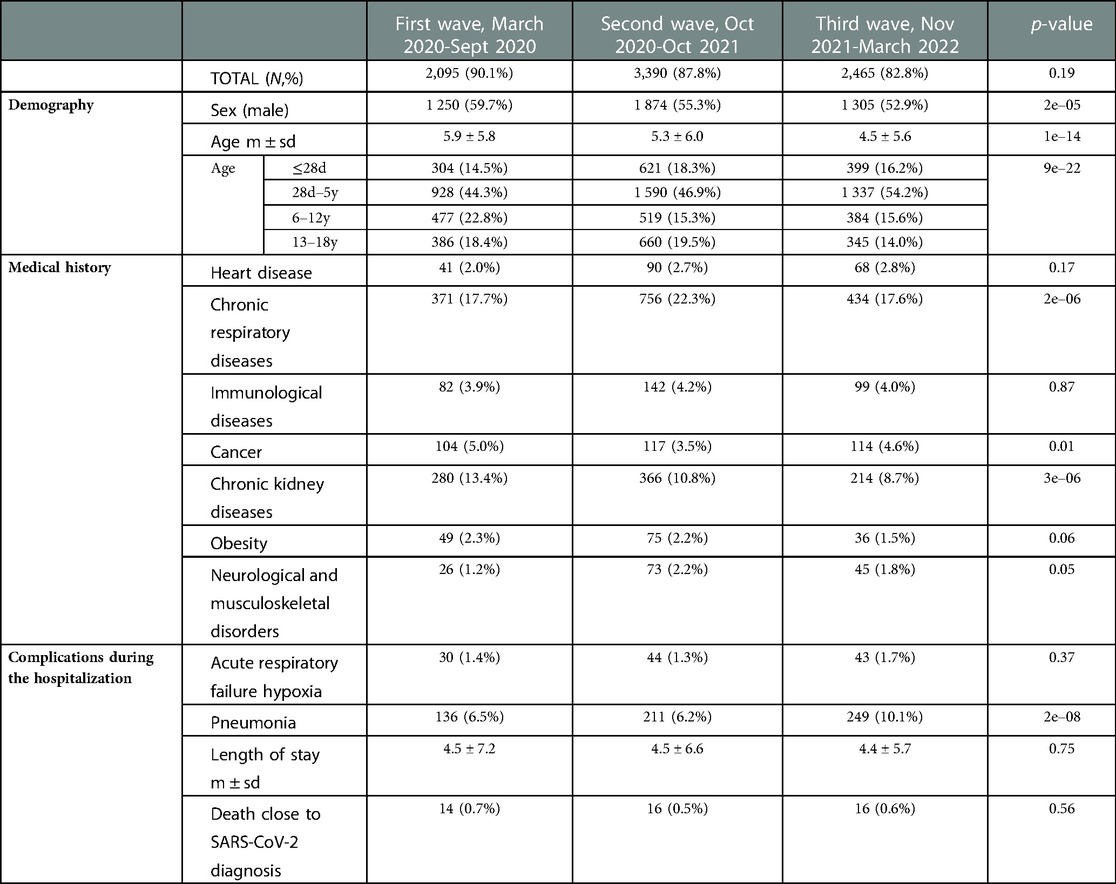
Table 4. Characteristics of pediatric patients hospitalized with mild or asymptomatic SARS-CoV-2 infection..
The analysis of the patients with symptomatic or mildly symptomatic or asymptomatic SARS-Cov2 infection (groups 2 and 3) showed that 51 patients died within 5 days after the dismission. These deaths are likely due to other concurrent illnesses not related to the SARS-COv2 infection..
Despite the different clinical presentations of the SARS-CoV-2 infection, the incidence of concomitant diseases was similar in the symptomatic and mild or asymptomatic infected patients with higher involvement in patients with previous respiratory or chronic kidney diseases (Tables 3, 4).
Considering the whole population of SARS-Cov2 hospitalized pediatric patients (groups 2 and 3), the concomitant occurrence of pneumonia was higher during the third wave (10.2% during the third wave compared to 7% and 6.5% in the first and second waves).
To our knowledge, this study is one of the largest multicenter retrospective COVID-19 pediatric studies to date on more than 9,100 hospitalized pediatric patients presenting SARS-Cov2 infection in France. Using the AP-HP Covid Clinical Data Warehouse allowed an in-depth analysis of the clinical characteristics of these patients according to the period of hospitalization and the SARS-Cov2 variant identification, if available. The aim of this study was to characterize the impact of the SARS-Cov2 infection on the hospitalized pediatric population in the Great Paris area among the three different waves and, consequently, if possible, to analyze the link with the different subsequent SARS-Cov2 variants.
The greater Paris area has experienced five SARS-Cov2 infection surges (11): from March to May 2020, from September to November 2020, from March to May 2021, from July to September 2021, and from December 2021 to January 2022. For our analysis, we preferred to merge the periods characterized by a predominant SARS-Cov2 variant in order to better compare the impact and clinical characteristics in the pediatric population.
The spread of SARS-CoV-2 infection in the pediatric population, and in more detail, the incidence of the Omicron variant has been previously reported in the literature. Data from a pediatrics cohort in the United States suggested that hospitalization for symptomatic SARS-CoV-2 infection increased with the emergence of the Omicron variant, particularly in younger children (12). In another large cohort of pediatric patients in the United States (7,201 infected children), the incidence of SARS-COV2 with the Omicron variant predominated in children under the age of 5 years old (13). The REACT-1 cohort in England found a significantly higher incidence of the Sars-Cov2 Omicron infection in children (5 to 17 years old) compared to the previous variant infections (14).
Parts of these results are similar to our analysis where pediatric patients, less than 5 years old, are highly represented in the last period of the pandemic (71% of the 2,977 patients hospitalized during the third wave). The role of the incoming SARS-Cov2 vaccination for older children during the third wave is to be taken into account considering the higher incidence in very young patients (15).
In our study, the total number of pediatric patients hospitalized for symptomatic SARS-Cov2 infection increased over time (442 in the third wave vs. 132 and 308 in the first and second wave) with lung involvement, especially during the first period (21.2%). Nevertheless, considering the entire pediatric cohort (groups 2 and 3), a higher incidence of pulmonary involvement was observed during the third wave. Concomitant seasonal virus infections have to be considered in the analysis of the Omicron SARS-Cov2 infected pediatric patients (16) since SARS-CoV2 infection has similar symptoms to winter respiratory viruses. However, in our cohort, the symptoms could originate from several viruses without the possibility of attribution to SARS-Cov2. On the other hand, a recent study underlined that children without previous SARS-Cov2 immunization could present a more severe Omicron variant Covid-19 disease than children with previous immunization (17).
Interestingly, the analysis of the medical records showed that chronic respiratory diseases (i.e., asthma) were associated with a higher incidence of SARS-CoV2 infection. The association of chronic kidney diseases with SARS-Cov2 infection is probably due to a selection bias in patients in an exclusive hospital setting. Further studies need to focus on this population in order to state if chronic kidney disease patients are exposed to a higher risk of infection.
Pediatric Inflammatory Multisystem Syndrome correlated to SARS-Cov2 infection is an exclusive complication of COVID-19 infection in the pediatric population (18). These patients have been already well-characterized in the literature (19, 20). In our analysis, we showed that pediatric patients presenting PIMS or acute myocarditis following SARS-Cov2 infection were well represented in the three periods with higher incidence during the first and the second wave. Interestingly, in accordance with our results, a German study comparing the incidence of PIMS over the pandemic and the incidence of the different variants revealed a lower occurrence of PIMS correlating with the Omicron variant of SARS-COV2 infection (21). This is also concordant with other results from studies performed in the United Kingdom (22), Denmark (23), and Australia (24) which also found a lower incidence of PIMS during the dominant Omicron variant of SARS-CoV-2. This is probably due to the viral antigen changes and the subsequent host immune-inflammatory pathway activations. Further investigations is needed to complete these analyses since this complication could occur with a variable delay from the time of infection. Nevertheless, the diagnosis and management of PIMS patients improved over time and this is probably a significant reason why the severity of the disease seems to be less important during the last wave.
Several limitations of this study should be noted since some variables were not available in the database for the analysis, and potential inaccuracies can be present in the electronic health records. Although these findings should be interpreted with caution, this study illustrated the impact of the SARS-Cov2 infection on the hospitalized pediatric population providing valuable information on the characteristics and frequency over time. The robustness of the data analyzed rests on one of the largest multicenter retrospective SARS-Cov2 pediatric studies. Further analysis is needed to improve our knowledge of the new emerging variants and to monitor the frequency of reinfection.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by N° CSE: CSE 20-48_COVIDPed; AP-HP CDW Scientific and Ethics Committee number IRB00011591. The authors have the necessary regulatory agreements (n° 1980120) to use the patient data from the National Commission on Informatics and Liberty (CNIL), aimed at ensuring the application of data privacy laws.
MS: primary author, designed the study plan; analysis of the data, writing the bulk of the manuscript. PP, MD, and NB: AP-HP Covid Clinical Data Warehouse extraction and analysis, statistical analysis, image acquisition, and image edition. MP: drafted the manuscript, and contributed to the analysis of the data. MO and HC: critical revision of the manuscript, contributed to the analysis of the data, and designed the study plan. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1044352/full#supplementary-material.
1. Parkar S, Pethani A, Zehra SMEJ, Khan F, Kazi Z, Hilal K, et al. Epidemiological, clinical, and radiological comparison of adult and pediatric features in COVID-19: a scoping review. J Pak Med Assoc. (2022) 72(2):305–11. doi: 10.47391/JPMA.3269
2. Zhu F, Ang JY. COVID-19 Infection in children: diagnosis and management. Curr Infect Dis Rep. (2022) 24(4):51–62. doi: 10.1007/s11908-022-00779-0
3. CDC COVID-19 Response Team. Coronavirus disease 2019 in children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69(14):422–6. doi: 10.15585/mmwr.mm6914e4
4. Kelvin AA, Halperin S. COVID-19 in children: the link in the transmission chain. Lancet Infect Dis. (2020) 20(6):633–4. doi: 10.1016/S1473-3099(20)30236-X
5. Flood J, Shingleton J, Bennett E, Walker B, Amin-Chowdhury Z, Oligbu G, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS): prospective, national surveillance, United Kingdom and Ireland, 2020. Lancet Reg Health Eur. (2021) 3:100075. doi: 10.1016/j.lanepe.2021.100075
6. Payne AB, Gilani Z, Godfred-Cato S, Belay ED, Feldstein LR, Patel MM, et al. Incidence of multisystem inflammatory syndrome in children among US persons infected with SARS-CoV-2. JAMA Netw Open. (2021) 4(6):e2116420. doi: 10.1001/jamanetworkopen.2021.16420
7. Guenver C, Oualha M, Levy C, Antona D, Madhi F, Toubiana J, et al. Educational setting and SARS-CoV-2 transmission among children with multisystem inflammatory syndrome: a French national surveillance system. Front Pediatr. (2021) 9:745364. doi: 10.3389/fped.2021.745364
8. Taylor CA, Whitaker M, Anglin O, Milucky J, Patel K, Pham H, et al. COVID-19-Associated hospitalizations among adults during SARS-CoV-2 Delta and omicron variant predominance, by race/ethnicity and vaccination Status - COVID-NET, 14 states, July 2021-January 2022. MMWR Morb Mortal Wkly Rep. (2022) 71(12):466–73. doi: 10.15585/mmwr.mm7112e2
9. Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. The REporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. (2015) 12(10):e1001885. doi: 10.1371/journal.pmed.1001885
10. Jiang L, Tang K, Levin M, Irfan O, Morris SK, Wilson K, et al. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis. (2020) 20(11):e276–88. doi: 10.1016/S1473-3099(20)30651-4
11. Dinh A, Dahmane L, Dahoumane M, Masingue X, Jourdain P, Lescure FX. Impact of omicron surge in community setting in greater Paris area. Clin Microbiol Infect. (2022) 28(6):897–9. doi: 10.1016/j.cmi.2022.02.015
12. Wang L, Berger NA, Kaelber DC, Davis PB, Volkow ND, Xu R. Comparison of outcomes from COVID infection in pediatric and adult patients before and after the emergence of omicron. medRxiv. (2022). doi: 10.1101/2021.12.30.21268495
13. Wang L, Berger NA, Kaelber DC, Davis PB, Volkow ND, Xu R. COVID Infection severity in children under 5 years old before and after omicron emergence in the US. medRxiv. (2022. doi: 10.1101/2022.01.12.22269179
14. Elliott P, Eales O, Bodinier B, Tang D, Wang H, Jonnerby J, et al. Dynamics of a national omicron SARS-CoV-2 epidemic during January 2022 in England. Nat Commun. (2022) 13(1):4500. doi: 10.1038/s41467-022-32121-6
15. Infectious Diseases CO. COVID-19 Vaccines in infants, children, and adolescents. Pediatrics. (2022). 150(3):e2022058700. doi: 10.1542/peds.2022-058700
16. Fratty IS, Reznik-Balter S, Nemet I, Atari N, Kliker L, Sherbany H, et al. Outbreak of influenza and other respiratory viruses in hospitalized patients alongside the SARS-CoV-2 pandemic. Front Microbiol. (2022) 13:902476. doi: 10.3389/fmicb.2022.902476
17. Edward PR, Lorenzo-Redondo R, Reyna ME, Simons LM, Hultquist JF, Patel AB, et al. Severity of illness caused by severe acute respiratory syndrome coronavirus 2 variants of concern in children: a single-center retrospective cohort study. J Pediatric Infect Dis Soc. (2022):piac068. doi: 10.1101/2021.10.23.21265402
18. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. (2020) 324(3):259–69. doi: 10.1001/jama.2020.10369
19. Harwood R, Allin B, Jones CE, Whittaker E, Ramnarayan P, Ramanan AV, et al. A national consensus management pathway for paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): results of a national delphi process. Lancet Child Adolesc Health. (2021) 5(2):133–41. doi: 10.1016/S2352-4642(20)30304-7
20. Davies P, Evans C, Kanthimathinathan HK, Lillie J, Brierley J, Waters G, et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health. (2020) 4(9):669–77. doi: 10.1016/S2352-4642(20)30215-7
21. Sorg AL, Schönfeld V, Siedler A, Hufnagel M, Doenhardt M, Diffloth N, et al. SARS-CoV-2 variants and the risk of pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 among children in Germany. Infection. (2022):1–7. doi: 10.1007/s15010-022-01908-6
22. Cohen JM, Carter MJ, Cheung CR. Ladhani S, for the evelina paediatric inflammatory multisystem syndrome temporally related to SARS-CoV-2 (PIMS-TS) study group. Lower risk of multisystem inflammatory syndrome in children with the Delta and omicron variants of severe acute respiratory syndrome coronavirus 2. Clin Infect Dis. (2022) 76(3):e518–e21. doi: 10.1093/cid/ciac553
23. Holm M, Espenhain L, Glenthøj J, Schmidt LS, Nordly SB, Hartling UB, et al. Risk and phenotype of multisystem inflammatory syndrome in vaccinated and unvaccinated danish children before and during the omicron wave. JAMA Pediatr. (2022) 176(8):821. doi: 10.1001/jamapediatrics.2022.2206
Keywords: data warehouse, SARS-CoV-2, children, PIMS, MIS-C multisystem inflammatory syndrome in children, hospitalized child
Citation: Semeraro M, Pinson P, Populaire M, Dellagi M, Oualha M, Beeker N and Chappuy H (2023) Analysis of the impact of the SARS-CoV-2 infection on the pediatric population hospitalized during the pandemic in the Greater Paris University Hospitals. Front. Pediatr. 11:1044352. doi: 10.3389/fped.2023.1044352
Received: 14 September 2022; Accepted: 31 January 2023;
Published: 27 February 2023.
Edited by:
Andras Bratincsak, University of Hawaii, United StatesReviewed by:
Luca Pierantoni, Sant'Orsola-Malpighi Polyclinic, Italy© 2023 Semeraro, Pinson, Populaire, Dellagi, Oualha, Beeker and Chappuy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michaela Semeraro bWljaGFlbGEuc2VtZXJhcm9AYXBocC5mcg==
†Data used in preparation of this article were obtained from the AP-HP Covid Clinical Data Warehouse (CDW). As such, the members of the AP-HP Covid CDW initiative contributed to the design and implementation of the database but did not participate in analysis or writing of this report. A complete listing of members can be found at: https://eds.aphp.fr/covid-19 and in
Specialty Section: This article was submitted to Pediatric Cardiology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.