 Adugna Negussie Gudeta1
Adugna Negussie Gudeta1 Carin Andrén Aronsson1
Carin Andrén Aronsson1 Bayissa Bekele Binagdie2Alemayehu Girma3
Bayissa Bekele Binagdie2Alemayehu Girma3 Daniel Agardh1*
Daniel Agardh1*
- 1Unit of Diabetes and Celiac Disease, Department of Clinical Sciences, Clinical Research Center, Lund University, Malmö, Sweden
- 2Adama Public Health Referral and Research Laboratory Center, Adama, Ethiopia
- 3Department of Pediatrics, Adama Hospital Medical College, Adama, Ethiopia
Background: The prevalence of celiac disease in the general population is mainly unknown in most of sub-Saharan African countries. The aim of this study was to determine the incidence of celiac disease autoimmunity (CDA) and its associations with latent Mycobacterium tuberculosis (LMTB) and Helicobacter pylori (HP) infections in Ethiopian children aged 4 years in an HLA genotyped cohort study.
Methods: Of 1,389 recruited children between 2018 and 2022, 1,046 (75.3%) had been screened at least twice for celiac disease between the ages of 2 and 4 years using a tissue transglutaminase autoantibody (tTGA) ELISA kit. Tissue TGA-positive children were retested using radio-binding assays. CDA was defined as persistent-confirmed tTGA positivity in two consecutive samples. Associations of CDA with LMTB and HP were tested in a subpopulation of 752 children born to mothers who were previously tested for LMTB with IFN-γ and anti-HP antibodies in samples collected at a mean age of 49.3 ± 5.3 months.
Results: Screening detected 38 out of 1,046 (3.6%) IgA-tTGA-positive children. Ten (1.0%) were confirmed to be positive, with six (0.6%) children diagnosed with CDA. The incidence of CDA at 4 years of age was 1.2 per 1,000 person-years. LMTB was found in 4 of 6 (66.7%) mothers with CDA children compared with 340 of 734 (46.3%) mothers of children without CDA (p = 0.424), while HP was found in 3 of 6 (50.0%) CDA children compared with 315 of 746 (42.2%) children without CDA (p = 0.702).
Conclusion: The incidence of CDA in Ethiopian children is lower than the pooled global incidence. Neither LMTB nor HP infections are associated with CD in Ethiopian children.
Introduction
Celiac disease (CD) prevalence varies globally depending on the distribution of the HLA-DQ2 and HLA-DQ8 haplotypes and wheat consumption in the general population (1). The increase in incidence observed in many countries over the past few decades can be attributed to either increased awareness of the disease or as a result of changes in the environment (2). However, due to limited access to diagnostic testing and the diverse clinical manifestation, CD is most likely underestimated in many developing countries (1, 3). Serological tests are widely used in the diagnosis of CD. Tissue transglutaminase autoantibody (tTGA) is considered the best serological screening marker for CD since it has high sensitivity (78%–100%) and specificity (90%–100%) (4) and tTGA levels correlate with intestinal mucosal damage (5).
CD may develop at any age but has a peak incidence occurring in early childhood and a second peak in the third decade of life (6). Similar to many other autoimmune diseases, females are predominantly affected (7, 8). CD has a wide range of symptoms that make the disease difficult to diagnose in a clinical setting. In fact, population-based studies show that the majority of individuals with CD are diagnosed only through screenings (9). Despite the fact that the global prevalence of CD is believed to be around 1.4% (1), the true frequency of CD is mainly unknown in most countries around the world (10).
Although environmental factors like gluten and HLA-DQ2 or DQ8 are associated with CD, the actual etiology of CD is still unknown (11). The rising incidence supports the role of environmental risk factors, including exposure to microorganisms that may cause an inflammatory response in the small intestine. Latent Mycobacterium tuberculosis (LMTB) and Helicobacter pylori (HP) are common bacterial infections that affect humans globally. The occurrences of these two chronic infections are higher in developing countries, countries with low socioeconomic wealth, and in densely populated areas. There are numerous ways in which autoimmune diseases are brought on by pathogenic microorganisms. The molecular mimicry between microbial antigens and host proteins is one of the etiological paradoxes in the onset of autoimmune diseases. Studies indicate that TB-reactive T-cells can potentially be recognized as self-antigen, and this cross-reactive epitope may trigger autoimmune responses. A number of previous studies have shown that rheumatoid arthritis, multiple sclerosis, and other chronic inflammatory diseases are widespread in tuberculosis-endemic areas (12). On the other hand, studies from Karelia in Russia and Finland indicate that people living in deprived socioeconomic situations and lower hygienic conditions are at a lower risk of type 1 diabetes and CD, supporting the hygiene hypothesis that exposures to chronic infections and parasites may be protective from autoimmune diseases (13).
Ethiopia is one of the few endemic countries in the world where both HP and LMTB are two highly prevalent and clinically silent infections, whereas CD is still considered a rare disease (14, 15). Several previous studies on LMTB and HP have confirmed a prevalence as high as 50% for both infections in different regions of the country (16, 17). In a recent study on adult Ethiopian woman, we found a 0.05% seroprevalence of celiac disease autoimmunity (CDA) (15). It is hypothesized that differences in prevalence could indicate that low-grade infections might protect from autoimmune diseases, further supporting the hygiene hypothesis as demonstrated in the Russian Karelian and Finnish studies (13). Furthermore, previous studies indicate that HP infections are inversely associated with CD (18, 19). However, there is a paucity of studies from Ethiopian testing on the incidence of CDA and associations with LMTB and HP. The aim of the present study was to provide new insight into the incidence of CD and its associations with LMTB and HP infection in Ethiopian children.
Materials and methods
Study population
The Traditional Ethiopian Food (TEF) project is a longitudinal, observational prospective screening study that follows up a birth cohort at three health facilities in Adama, Oromia, Ethiopia's largest regional state. The purpose is to assess the incidence and prevalence of CD study in relation to genetic and environmental factors, e.g., dietary patterns, nutritional conditions, and exposure to infectious diseases. As of April in 2018, 1,389 participants were recruited for a 4-year follow-up. Annual screening for CD began from 2 years of age (Figure 1). Baseline data were collected during first recruitments for female participants and after delivery by 6 weeks for infants and then followed up at 9, 18, 24, 36, and 48 months for CD. At each visit, trained clinical nurses filled out a questionnaire regarding the participant's feeding practices, clinical information, medications, and growth metrics provided by the legal guardian as previously described (Supplementary Table S1) (20, 21). As of June 2022, 1,256 (90.4%) children had been screened at least once for tTGA using a commercial ELISA, of whom 1,046 (83.4%) had at least two serological tTGA measurements at median age of 49.3 (interquartile range, 47.5–53.3) months. Among the 1,046 recruited children, 752 children had mothers who had been screened for LMTB findings and children themselves screened for HP at a mean age of 49.3 ± 5.3 months.
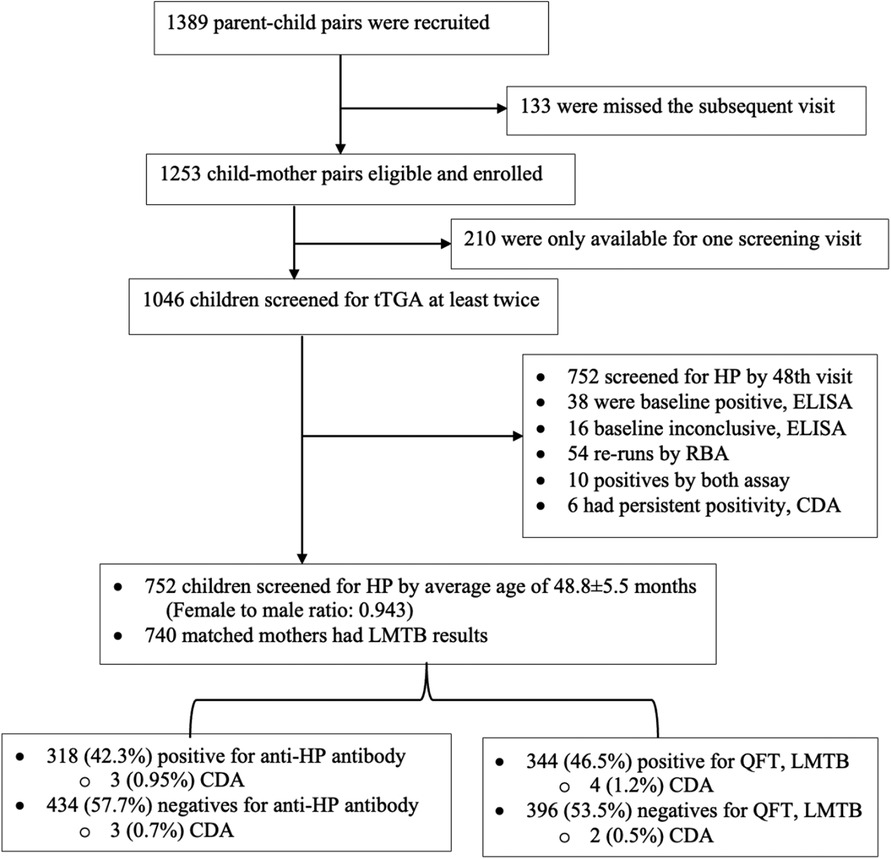
Figure 1. Flow chart of study participants.
Screening for CDA
Baseline screening for CDA started at 2 years of age by measuring IgA-neoepitopes against tTGA as previously described (AESKULISA tTg-A New generation, AESKU DIAGNOSTICS GmbH & Co. KG Mikroforum Ring 2 55234 Wendelsheim, Germany) (22–24). Antibody levels were expressed in U/ml. The cutoff level chosen for the present study was 18 U/ml for IgA anti-tTGA according to receiver operating characteristic curves. A range between 12 and 18 U/ml was considered as the borderline positivity region. Children who were tTGA-positive at baseline were retested for both IgA-tTGA and IgG-tTGA using radioligand-binding assays (RBAs) as previously described (25). tTGA levels were expressed in U/ml, calculated from standard curves. Samples above the highest calibrator range were diluted as appropriate and reassayed. Children who were persistent-confirmed tTGA-positive in two consecutive samples were defined as having CDA and referred to a pediatrician for clinical follow-up (26). The decision whether to refer the child to the tertiary hospital for an upper endoscopy and intestinal biopsy to confirm diagnosis of CD was taken by the pediatrician.
Screening for LMTB and HP infections
Data on LMTB and related sociodemographic factors were collected during prenatal care and after delivery from mothers in the integrated Pregnancy-TB cohort. LMTB was confirmed by measuring IFN-γ using ELISA according to the QFT-Plus protocol (27). The present analysis included 752 children for data on the colonization of HP and mother–child pairs for LMTB exposure. HP infection was examined in the leftover serum samples from the birth cohort that were maintained in the repository. All serum samples collected at an average age of 4 years were analyzed for anti-HP antibody by using the commercially available ELISA (IBL International GmbH, Hamburg, Germany) method as previously described (28).
Statistical analysis
The data were analyzed using a statistical software package for Social Science, IBM SPSS, version 27. Descriptive statistics, namely, mean, percentages, frequency, and standard deviation, were calculated. The distribution of the parameters was evaluated using the Shapiro–Wilk test. Student's t test was used for comparison of two groups with a normal distribution; the Mann–Whitney U test was used for comparison of two groups with no normally distributed parameters. The chi-square test was used for comparison of categorical data. The binary logistic regression analysis was used to see the relation between dependent variables and independent variables. Spearman's and Fisher's correlation analyses were used to examine the correlations between metric variables. A p-value <0.05 and a width of 95% CI was considered to be statistically significant.
Results
Sociodemographic characteristics of the study population
Of the 1,389 mother–child pairs who were invited to take part in the 4-year follow-up, 1,256 underwent at least one IgA-tTGA test, of whom 1,046 were tested at least twice starting at two years of age. Of the 1,046 children, 752 were tested for HP. Of these, 740 matched mothers had been checked for LMTB findings and had complete data for analysis were included. The mean follow-up was 50.0 (IQR, 47.5–53.3) months (Table 2).
Incidence of CDA
A total of 2,433 serum samples from 1,046 children were assessed for IgA-tTGA ELISA. Of the 1,046 (3.6%) children, 38 tested baseline positive, while 16 (1.5%) were borderline positive. Ten children were confirmed to be tTGA-positive with RBA and six of those children were persistent-confirmed tTGA-positive. Detailed information about the six children with CDA is given in Supplementary Table S2. Three children were identified at 24 months of age and the remaining three at 36 months, with an equal number of boys and girls affected by CDA (1:1, p = 0.401) (Table 1). The prevalence of CDA estimated at 0.6% (6/1046) (95% CI 0.23–1.28) and incidence of CDA by age four years was 1.2 per 1,000 person-years. One CDA child had an IgA-tTG level >10 times the upper limit of normal (ULN) supporting the diagnosis of CD. The other five CDA children had persistent elevated IgA-tTG levels that could indicate CD but were yet to be confirmed histologically. Five of the six CDA children carried any of the HLA-DQ2 and/or DQ8 haplotypes, with the exception of one child who had a sequencing failure during the HLA genotyping (Table 1). Most children were asymptomatic and there was no difference in anthropometrics between the two groups (Tables 2, 3).
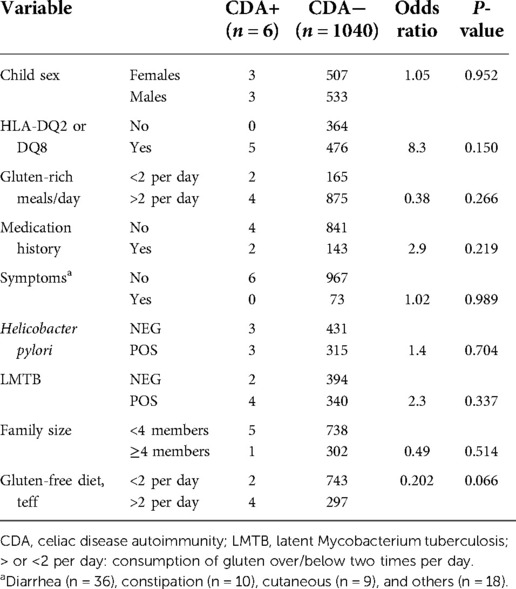
Table 1. Observed factors in children with and without CDA.
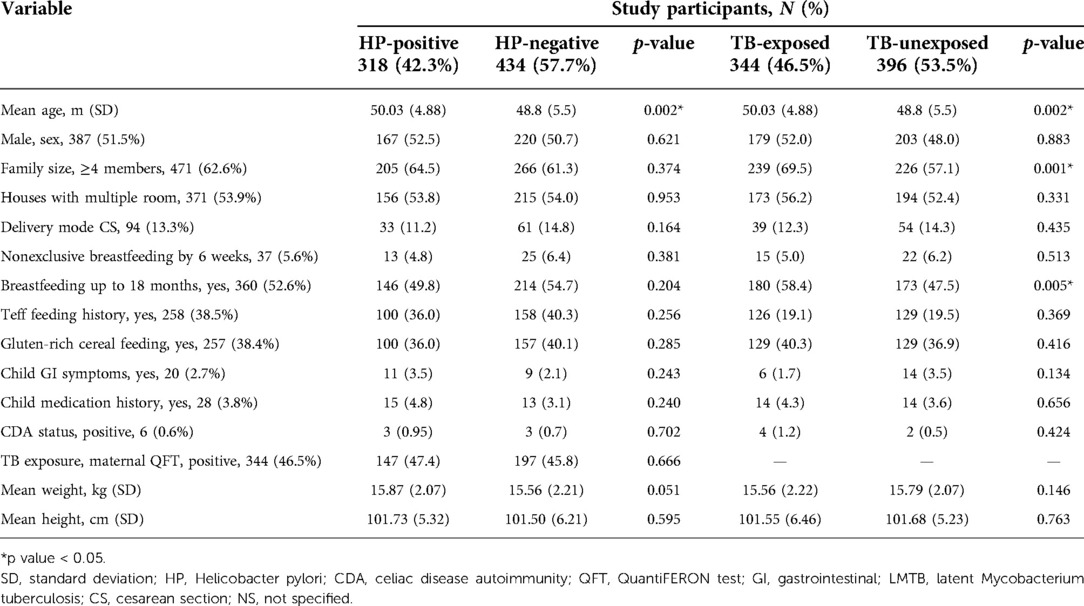
Table 2. Characteristics of study population stratified by HP (n = 752) and LMTB (n = 740).

Table 3. Anthropometrics of children with and without CDA by age.
Associations of LMTB and HP with incidence of CDA
Complete LMTB-related data was obtained from 740 mothers whose children had also been tested for anti-HP antibodies. Of these, 344 (46.5%) had LMTB and found in 4/6 (66.7%) mothers to CDA children compared with 340/734 (46.3%) mothers of children without CDA (p = 0.424) (Table 1). Among the 752 children of mothers with LMTB also screened for HP at a mean age of 50.0 ± 4.9 months, 318/752 (42.3%) were HP-positive (Table 2). Three of the six children with CDA (50.0%) were HP-positive compared with 315/746 (42.2%) without CDA (p = 0.702).
Diet and anthropometric characteristics of the study participants
Overall, 4.4%, 9.2%, and 5.9% of the children in this study were wasted, stunted, and underweight, respectively, by 4 years of age. The majority of children were fed with teff and gluten-rich, wheat, or barley grains on a regular basis. Two or more serving portions per day of teff or gluten-rich foods did not increase the risk of developing CDA. At the 6-week study visit, the majority (94%) had been exclusively breastfed. Up until the age of 18 months, nearly half of the mothers breastfed their children, but history of breastfeeding was not found to be associated with CDA.
Discussion
This prospective birth cohort study found a 0.6% prevalence of CDA in the screening of Ethiopian children up to 4 years of age and a corresponding incidence of 1.2 per 1,000 person-years. This is lower than the pooled global seroprevalence of CDA, which varied from 1.1% (Africa) to 1.4% (Oceania and North America) (29), but corresponded to the prevalence of CD reported from Egypt (0.5%) (30), Libya (0.8%) (31), Tunisia (0.6%) (32), and Western Europe (0.6%) (29). This finding of importance further refutes the devoid of CD in sub-Saharan Africa along with case reports from Sudan (33), Djibouti (34), and Ethiopia (14). In a previous study, we estimated the prevalence of tTGA positivity in Ethiopian adult women to be 0.05% (15). Compared to the adult population, the CDA prevalence in the present pediatric cohort increased 12 times. The discrepancy between the two cohorts cannot be explained by methodological reasons since the same assays were used to assess tTGA. We speculate that the reasons for this increase in the prevalence between the two cohorts can be attributed to changes in exposure environmental factors such as infections, adoption of a more western lifestyle, increase of wheat consumption, and a rise in exports of teff injera (35, 36).
First, we noticed during the follow-up screening that many children had transient tTGA levels and seroconverted to tTGA negativity. Although the reason some children seroconvert to tTGA negativity while others progress to developing CD remains unknown, the phenomenon of fluctuating tTGA levels has been described in several previous longitudinal birth cohort studies (37, 38). In this population, we anticipated that most parents in the research area often use injera or flat bread as dietary bases. Teff is an important food grain in Ethiopia, a cereal that lacks T-cell stimulatory peptides and is gluten-free (39). It seems that eating foods free of gluten, such as teff, reduces tTGA levels. This is supported by research findings on the extent of tTGA after a gluten-free diet (40).
Alternatively, falsely tTGA-positive results may have occurred due to the poor diagnostic performance of the assays. A sequential testing approach was employed for initial screening with the highly sensitive ELISA assay ASKULISA, followed by the more specific RBA, a previously used assay in several screenings for CD. It was believed that ELISA tests would be more easily accessible and fairly priced in the setting where the research was conducted and will be used in future clinical screenings. Our findings indicate that ELISA identified more positive results than RBA, which is in line with our previous studies demonstrating that ELISA had lower specificity but equivalent sensitivity to RBA (22, 23, 41). In addition, we found that HLA-DQ2 and/or DQ8 were presented in all CDA-positive children, with an exception of one child whose sequencing phase failed during the genetic analysis. It was shown that the risk of CD for children carrying HLA risk genotypes is eight times higher than children with nonrisk HLA genotypes (42).
Second, we tested if the incidence of CDA was associated with two silent chronic infections—LMTB and HP. Although the exposure of LMTB among Ethiopian mother–child pairs was alarmingly high, there was no association found with CDA incidence in this cohort. This is in contrast to a previous study that found noticeably higher prevalence rates of LMTB in CD patients (43, 44). Autoimmune disorders are more common in groups that have been exposed to tuberculosis and developed resistance to it, and less common in populations that have not (45). In addition, we found that 42.3% of Ethiopian children were HP-positive by 4 years of age. Earlier research showed that the prevalence of HP colonization in the Ethiopian population has decreased from 64.4% to 42.9% between 1990 and 2017 (46). Despite this high but decreasing prevalence, we found no association with CDA incidence in this cohort. However, this contrasts to previous research showing inverse association between lower incidence of infections and increased risk of autoimmune disease (47, 48). The finding is also in contrast to previous studies indicating that HP infection would protect against CD (19). Reasons for inconsistent results between this current study and previous studies might be due to statistical power, sociodemographic differences, research design, diagnostic techniques, and the geographic settings. Moreover, compared to Sweden, the prevalence of HP infection is higher in Ethiopian children, whereas as the opposite seems to be true for CD (49).
The strength is the prospective study design of Ethiopian children enrolled from the general population to a 4-year longitudinal follow-up. This allows for monitoring children from birth and collecting information prior to the onset of CDA without recall bias. Furthermore, the strict definition of CDA, i.e., being persistent tTGA-positive in two consecutive samples collected 1 year apart, in addition to carrying HLA risk genotypes from previous HLA genotyping of the entire cohort (20), most likely excluded many false tTGA-positive individuals, In addition, it allowed us to conclude that the lower incidence of CDA in the present cohort was not dependent on a skewed HLA population. Another strength was the unbiased data collected from mother–child pairs of two highly prevalent chronic infections. However, this study did have a few limitations. For instance, diet-related data were qualitative in nature since data collection was mainly based on parent feedback and not free from recall bias. Since the study was conducted in only a single city of the region of Oromia, it was not representative of the entire region of the country. Another limitation was lack of testing for endomysial autoantibodies and limited access to upper endoscopy for intestinal biopsy to confirm the diagnosis of CD according to the ESPGHAN criteria in children with CDA, which is a common problem in many developing countries like the situation in Ethiopia. Finally, TB exposure in children was based on the information recalled by their mothers either before or after birth.
Conclusion
The incidence of CDA in Ethiopian children from the Oromia region appears to be higher than that of adults but lower than the pooled global incidence. Exposures to LMTB or childhood HP infections are not associated with incidence of CDA at age 4 years. Therefore, the reason for this increase in prevalence remains to be explored. It is recommended that the current study be expanded to include a larger geographic area of the country, allowing for the regional mapping of CD.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The Armauer Hansen Research Institute (AHRI) (P028/ 17), the Faculty of Medicine at Lund University in Lund, Sweden (Pro. No. 2017/3), and the National Ethical Review Board of Ethiopia (Ref.No.3.10/16/2018) all provided their approval to the study. Written informed consent was obtained before study participants were enrolled. Under the guidelines set forth by the Ethiopian Ministry of Health, blood samples were taken by trained healthcare workers who participated in routine medical deliveries. The screening results were kept confidential and were only shared with the pediatricians in the study team who would be using them for additional diagnosis and care. All children who tested positive were taken to the pediatric clinic for consultation with a GI expert.
Author contributions
ANG and DA contributed to the conceptualization of the article. ANG, DA, CAA, AG, and BBB contributed to the investigation. ANG and DA contributed to the methodology, validation, analysis, and data curation. DA and CAA contributed to the supervision, project administration, and resource and funding acquisition. ANG wrote the original draft of the article. DA carried out critical manuscript revision and approval. All authors contributed to the article and approved the submitted version.
Funding
This research was aided by the funds provided by the Swedish Research Council, Swedish Celiac Disease Foundation, Håkanssons Stiftelse, and Pålssons Stiftelse.
Acknowledgments
The authors thank the Lund-Adama research team, Adama Referral Laboratory and Public Health Research center staff, AHRI, Oromia regional Health Bureau, laboratory and clinical staffs at research facilities, the CRC laboratory, study participants and their families, as well as the project's financial supporters. The pregnancy-TB study team; Per Björkman, Fregenet Tesfaye, and John Köng Walles, from the integrated cohort contributed the data on LMTB. The authors gratefully thank the members of the team who collected the biological samples and clinical data, as well as Anne Müller from the University of Zurich's Institute of Molecular Cancer Research provided the study kit for H. pylori. Finally, the authors thank Sarah Austin-Gonzalez for English proofreading of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.999287/full#supplementary-material.
References
1. Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2018) 16(6):823–36. doi: 10.1016/j.cgh.2017.06.037
2. Lebwohl B, Rubio-Tapia A. Epidemiology, presentation, and diagnosis of celiac disease. Gastroenterology. (2021) 160(1):63–75. doi: 10.1053/j.gastro.2020.06.098
3. Prescott SL, Smith P, Tang M, Palmer DJ, Sinn J, Huntley SJ, et al. The importance of early complementary feeding in the development of oral tolerance: concerns and controversies. Pediatr Allergy Immunol. (2008) 19(5):375–80. doi: 10.1111/j.1399-3038.2008.00718.x
4. Giersiepen K, Lelgemann M, Stuhldreher N, Ronfani L, Husby S, Koletzko S, et al. Accuracy of diagnostic antibody tests for coeliac disease in children: summary of an evidence report. J Pediatr Gastroenterol Nutr. (2012) 54(2):229–41. doi: 10.1097/MPG.0b013e318216f2e5
5. Malamisura M, Colantuono R, Salvati VM, Croce R, D’Adamo G, Passaro T, et al. Current ESPGHAN guidelines for celiac disease in pediatric age. Tertiary care center experience: a proposal for further simplification. Transl Med UniSa. (2019) 20(4):13–8. PMID: 31850247; PMCID: PMC6910143
6. Gujral N, Freeman HJ, Thomson ABRR. Celiac disease: prevalence, diagnosis, pathogenesis and treatment. World J Gastroenterol. (2012) 18(42):6036–59. doi: 10.3748/wjg.v18.i42.6036
7. King JA, Jeong J, Underwood FE, Quan J, Panaccione N, Windsor JW, et al. Incidence of celiac disease is increasing over time: a systematic review and meta-analysis. Am J Gastroenterol. (2020) 115(4):507–25. doi: 10.14309/ajg.0000000000000523
8. Jansson-Knodell CL, Hujoel IA, West CP, Taneja V, Prokop LJ, Rubio-Tapia A, et al. Sex difference in celiac disease in undiagnosed populations: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2018) 17(10):1954–68. doi: 10.1016/j.cgh.2018.11.013
9. Tommasini A, Not T, Kiren V, Baldas V, Santon D, Trevisiol C, et al. Mass screening for coeliac disease using antihuman transglutaminase antibody assay. Arch Dis Child. (2004) 89(6):512–5. doi: 10.1136/adc.2003.029603
10. Barada K, Abu Daya H, Rostami K, Catassi C. Celiac disease in the developing world. Gastrointest Endosc Clin N Am. (2012) 22(4):773–96. doi: 10.1016/j.giec.2012.07.002
11. Lázár-Molnár E, Snyder M. The role of human leukocyte antigen in celiac disease diagnostics. Clin Lab Med. (2018) 38(4):655–68. doi: 10.1016/j.cll.2018.07.007
12. Chodisetti SB, Rai PK, Gowthaman U, Pahari S, Agrewala JN. Potential T cell epitopes of Mycobacterium tuberculosis that can instigate molecular mimicry against host: implications in autoimmune pathogenesis. BMC Immunol. (2012) 21:13. doi: 10.1186/1471-2172-13-13
13. Kondrashova A, Mustalahti K, Kaukinen K, Viskari H, Volodicheva V, Haapala AM, et al. Lower economic status and inferior hygienic environment may protect against celiac disease. Ann Med. (2008) 40(3):223–31. doi: 10.1080/07853890701678689
14. Habtamu A, Kebede T. Celiac disease, a rare cause of malabsorption syndrome in children; the first case report in an Ethiopian children. Ethiop Med J. (2018) 56(2):181–3.
15. Gudeta A N, Brundin C, Muleta Feyissa D, Tolera Balcha T, Agardh D. Prevalence of celiac disease autoimmunity in Ethiopian pregnant women: a cross sectional study from the Oromia region. Int J Celiac Dis. (2019) 7(3):74–7. doi: 10.12691/ijcd-7-3-1
16. Chekesa B, Gumi B, Chanyalew M, Zewude A, Ameni G. Prevalence of latent tuberculosis infection and associated risk factors in prison in East Wollega Zone of western Ethiopia. PLoS One. (2020) 15(5):1–11. doi: 10.1371/journal.pone.0233314
17. Teklu T, Legesse M, Medhin G, Zewude A, Chanyalew M, Zewdie M, et al. Latent tuberculosis infection and associated risk indicators in pastoral communities in southern Ethiopia: a community based cross-sectional study. BMC Public Health. (2018) 18(1):1–9. doi: 10.1186/s12889-018-5149-7
18. Narang M, Puri AS, Sachdeva S, Singh J, Kumar A, Saran RK. Celiac disease and Helicobacter pylori infection in children: is there any association? J Gastroenterol Hepatol. (2017) 32(6):1178–82. doi: 10.1111/jgh.13654
19. Lebwohl B, Blaser MJ, Ludvigsson JF, Green PHR, Rundle A, Sonnenberg A, et al. Decreased risk of celiac disease in patients with Helicobacter pylori colonization. Am J Epidemiol. (2013) 178(12):1721–30. doi: 10.1093/aje/kwt234
20. Gudeta AN, Ramelius A, Balcha TT, Girma A, Ilonen J, Agardh D. Distribution of HLA-DQ risk genotypes for celiac disease in Ethiopian children. HLA. (2020) 96(6):681–7. doi: 10.1111/tan.14119
21. Gudeta AN, Andrén Aronsson C, Balcha TT, Agardh D. Complementary feeding habits in children under the age of 2 years living in the city of Adama in the Oromia region in central Ethiopia: traditional Ethiopian food study. Front Nutr. (2021) 8:1–7. doi: 10.3389/fnut.2021.672462
22. Venugopal G, Mechenro J, Makharia G, Singh A, Pugazhendhi S, Balamurugan R, et al. Sequential testing with different tissue transglutaminase antibodies, a new approach for diagnosis of celiac disease. Indian J Gastroenterol. (2017) 36(6):481–6. doi: 10.1007/s12664-017-0803-z
23. Lerner A, Jeremias P, Neidhöfer S, Matthias T. Antibodies against neo-epitope tTg complexed to gliadin are different and more reliable then anti-tTg for the diagnosis of pediatric celiac disease. J Immunol Methods. (2016) 429:15–20. doi: 10.1016/j.jim.2015.12.006
24. Agardh D, Matthias T, Wusterhausen P, Neidhöfer S, Heller A, Lerner A. Antibodies against neo-epitope of microbial and human transglutaminase complexes as biomarkers of childhood celiac disease. Clin Exp Immunol. (2020) 199(3):294–302. doi: 10.1111/cei.13394
25. Agardh D, Dahlbom I, Daniels T, Lörinc E, Ivarsson SA, Lernmark A, et al. Autoantibodies against soluble and immobilized human recombinant tissue transglutaminase in children with celiac disease. J Pediatr Gastroenterol Nutr. (2005) 41(3):322–7. doi: 10.1097/01.mpg.0000174845.90668.fa
26. Björck S, Brundin C, Lörinc E, Lynch KF, Agardh D. Screening detects a high proportion of celiac disease in young HLA-genotyped children. J Pediatr Gastroenterol Nutr. (2010) 50(1):49–53. doi: 10.1097/MPG.0b013e3181b477a6
27. Walles JK, Tesfaye F, Jansson M, Balcha TT, Winqvist N, Kefeni M, et al. Performance of QuantiFERON-TB gold plus for detection of latent tuberculosis infection in pregnant women living in a tuberculosis- and HIV-endemic setting. PLoS One. (2018) 13(4):e0193589. doi: 10.1371/journal.pone.0193589
28. Deshpande N, Lalitha P, Krishna Das SR, Jethani J, Pillai RM, Robin A, et al. Helicobacter pylori IgG antibodies in aqueous humor and serum of subjects with primary open angle and pseudo-exfoliation glaucoma in a South Indian population. J Glaucoma. (2008) 17(8):605–10. doi: 10.1097/IJG.0b013e318166f00b
29. Makharia GK, Chauhan A, Singh P, Ahuja V. Review article: epidemiology of coeliac disease. Aliment Pharmacol Ther. (2022) 56(Suppl 1):S3–S17. doi: 10.1111/apt.16787
30. Abu-Zekry M, Kryszak D, Diab M, Catassi C, Fasano A. Prevalence of celiac disease in Egyptian children disputes the east west agriculture-dependent spread of the disease. J Pediatr Gastroenterol Nutr. (2008) 47(2):136–40. doi: 10.1097/MPG.0b013e31815ce5d1
31. Alarida K, Harown J, Ahmaida A, Marinelli L, Venturini C, Kodermaz G, et al. Coeliac disease in Libyan children: a screening study based on the rapid determination of anti-transglutaminase antibodies. Dig Liver Dis. (2011) 43(9):688–91. doi: 10.1016/j.dld.2011.01.002
32. Fethia B, Nabil S, Mohsen H, Hamouda S. Prevalence of celiac disease in Tunisian blood donors. Gastroenterol Clin Biol. (2006) 30(1):33–6. doi: 10.1016/S0399-8320(06)73075-5
33. Ageep AK. Celiac disease in the Red Sea state of Sudan. Trop Gastroenterol. (2012) 3(2):118–22. doi: 10.7869/tg.2012.28
34. Ibrahima D, Thierry C. Celiac disease: a challenging disease uneasy to diagnose in sub-Saharan Africa. J Gastroenterol Hepatol Res. (2013) 2(8):753–6. doi: 10.6051/j.issn.2224-3992.2013.02.327
35. Abeje A, Desalegn T, Abebe E. Review on economics of teff in Ethiopia. Open Acc Biostat Bioinform. (2019) 2(3):OABB.000539. doi: 10.31031/OABB.2018.02.000539
36. Tadele E, Hibistu T. Spatial production distribution, economic viability and value chain features of teff in Ethiopia: systematic review. Cogent Econ Financ. (2022) 10:2020484. doi: 10.1080/23322039.2021.2020484
37. Auricchio R, Mandile R, Del Vecchio MR, Scapaticci S, Galatola M, Maglio M, et al. Progression of celiac disease in children with antibodies against tissue transglutaminase and normal duodenal architecture. Gastroenterology. (2019) 157(2):413–20. doi: 10.1053/j.gastro.2019.04.004
38. Castellaneta S, Piccinno E, Oliva M, Cristofori F, Vendemiale M, Ortolani F, et al. High rate of spontaneous normalization of celiac serology in a cohort of 446 children with type 1 diabetes: a prospective study. Diabetes Care. (2015) 38(5):760–6. doi: 10.2337/dc14-2890
39. Hopman E, Dekking L, Blokland ML, Wuisman M, Zuijderduin W, Koning F, et al. Tef in the diet of celiac patients in The Netherlands. Scand J Gastroenterol. (2008) 43(3):277–82. doi: 10.1080/00365520701714871
40. Hota D, Bhalla K, Nanda S, Gupta A, Mehra S. Beneficial effects of gluten free diet on IgA tissue transglutaminase levels and various growth parameters in celiac disease patients. J Fam Med Prim Care. (2019) 8:823–7. doi: 10.4103/jfmpc.jfmpc_56_19
41. Agardh D, Carlsson A, Lynch K, Axelsson I, Lernmark Å, Ivarsson SA. Using radioligand-binding assays to measure tissue transglutaminase autoantibodies in young children. Acta Paediatr Int J Paediatr. (2004) 93(8):1046–51. doi: 10.1111/j.1651-2227.2004.tb02716.x
42. Ludvigsson JF, Murray JA. Epidemiology of celiac disease. Gastroenterol Clin North Am. (2019) 48:1–18. doi: 10.1016/j.gtc.2018.09.004
43. Ludvigsson JF, Wahlstrom J, Grunewald J, Ekbom A, Montgomery SM. Coeliac disease and risk of tuberculosis: a population-based cohort study. Thorax. (2006) 62(1):23–8. doi: 10.1136/thx.2006.059451
44. Shapira Y, Agmon-Levin N, Shoenfeld Y. Mycobacterium tuberculosis, autoimmunity, and vitamin D. Clin Rev Allergy Immunol. (2010) 38:169–77. doi: 10.1007/s12016-009-8150-1
45. Williams H. Coeliac syndrome due to tuberculous enteritis. Med J Aust. (1952) 2(11):388–9. doi: 10.5694/j.1326-5377.1963.tb23110.x
46. Melese A, Genet C, Zeleke B, Andualem T. Helicobacter pylori infections in Ethiopia; prevalence and associated factors: a systematic review and meta-analysis. BMC Gastroenterol. (2019) 19(1):8. doi: 10.1186/s12876-018-0927-3
47. Okada H, Kuhn C, Feillet H, Bach JF. The “hygiene hypothesis” for autoimmune and allergic diseases: an update. Clin Exp Immunol. (2010) 160(1):1–9. doi: 10.1111/j.1365-2249.2010.04139.x
48. Bach JF. The hygiene hypothesis in autoimmunity: the role of pathogens and commensals. Nat Rev Immunol. (2018) 18(2):105–20. doi: 10.1038/nri.2017.111
Keywords: autoimmunity, celiac disease, children, cohort, Ethiopia, incidence, HLA
Citation: Gudeta AN, Andrén Aronsson C, Binagdie BB, Girma A and Agardh D (2022) Incidence of celiac disease autoimmunity and associations with maternal tuberculosis and pediatric Helicobacter pylori infections in 4-year-old Ethiopian children followed up in an HLA genotyped birth cohort. Front. Pediatr. 10:999287. doi: 10.3389/fped.2022.999287
Received: 20 July 2022; Accepted: 28 September 2022;
Published: 26 October 2022.
Edited by:
Rita Désirée Jores, Azienda Socio Sanitario Cagliari, ItalyReviewed by:
Sofia Kröger, Tampere University Hospital, FinlandMara Corpino, Ospedale G. Brotzu, Italy
© 2022 Gudeta, Andrén Aronsson, Binagdie, Girma and Agardh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Agardh ZGFuaWVsLmFnYXJkaEBtZWQubHUuc2U=
Specialty Section: This article was submitted to Pediatric Gastroenterology, Hepatology and Nutrition, a section of the journal Frontiers in Pediatrics