
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 25 January 2023
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.994882
 Franziska Köhler-Dauner1*
Franziska Köhler-Dauner1* Inka Mayer1
Inka Mayer1 Melissa Hitzler2
Melissa Hitzler2 Alexander Karabatsiakis3Lynn Matits2,4Alexandra M. Bach2Katharina Rost1
Alexander Karabatsiakis3Lynn Matits2,4Alexandra M. Bach2Katharina Rost1 Jörg M. Fegert1
Jörg M. Fegert1 Iris-Tatjana Kolassa2Ute Ziegenhain1
Iris-Tatjana Kolassa2Ute Ziegenhain1
The quality of maternal caregiving is an important factor in the healthy development of a child. One consequence of prolonged insensitive and atypical maternal interaction behavior (e.g., withdrawing from interactions with the child and role-reversal, i.e., the takeover of the parental role or parts of it by the child) in mother-child-dyads can cause alteration of the child's stress response system. Higher salivary cortisol concentrations were reported in infants and toddlers directly after negative interactions with their parents. However, no study to date has examined the association between atypical maternal interaction behavior and hair cortisol concentrations (HCC) in infants. Here, we studied the association of maternal interaction behavior with HCC of the child. Mother-child dyads (N = 112) participated in the longitudinal study My Childhood—Your Childhood. The AMBIANCE scale and its subscales were used to assess atypical maternal interaction behavior during the Strange Situation Procedure. Chronic stress levels in the child were assessed by HCC of 3 cm hair strands at the age of 12 months. Maternal educational level (operationalized in highest education level) served as a control variable. Robust multiple linear regression analyses revealed that role/boundary confusion was associated with HCC, i.e., the higher atypical interaction behavior of the mother the higher the HCC in the children. By measuring hair cortisol in this study, it is possible to determine the average long-term activity of the child's stress response system.Thus, atypical maternal interaction behavior could be a risk factor for persistent stress in children, contributing to a higher risk for negative health outcomes in later life. The results of this study highlight the importance of early intervention programs that focus on the relationship between mother and child.
The family environment is a crucial influencing factor for the healthy development of a child (1, 2). Particularly, the interaction of parents and other caregivers with the infant has a major impact on child development such as attachment representation (3–6), receptive language development (7), emotion regulation (8, 9) or the risk for mental disorders later in life (10, 11). Indeed, atypical maternal behavior such as withdrawing from interactions with the child or role-reversal, which means the takeover of the parental role or parts of it by the child was linked to disorganized attachment patterns among infants and toddlers (5, 6, 12, 13). The kindergarten-aged children showed poorer receptive and expressive language skills when their mothers behavior was more intrusive (7). A longitudinal study indicated that especially young adults with less responsive parents in childhood reported dissociative symptoms compared to children with more responsive parents (10). Moreover, low quality of parental interaction behavior in childhood was associated with physical diseases such as inflammatory bowel disease (14), asthma, respiratory infections (15–17), migraine (17, 18), and allergies (15).
A paternal lack of sensitive and appropriate responses to the child's emotions and behaviors is a chronic psychosocial stressor and might chronically stimulate the hypothalamic-pituitary-adrenal (HPA) axis and lead to a release of cortisol from the adrenal cortex into the bloodstream (19–22). Indeed, chronic psychosocial stress has been linked to allostatic overload of the body's stress response systems and an increased risk of physical and mental disorders (23). Smeekens and colleagues (24) found a stronger increase in 5-year-olds' salivary cortisol concentrations following a negatively attributed interaction with parents. Particularly children with low ego resilience, i.e., a decreased ability to cope appropriately with stress, displayed a stronger stress response in negative interactions with their parents (24). Furthermore, in a sample of mothers with a post-partum anxiety disorder a correlation between the mother's stress level during pregnancy and the baby's cortisol response has been reported (25).
An important factor contributing to elevated mental stress levels and cortisol levels in adulthood is experiencing abuse and neglect during childhood. It has been assumed that intergenerational transmission of childhood maltreatment (CM) experiences from the mother to her child is found because appropriate regulatory and coping strategies were not developed (26). Another impact of CM on the next generation, considering the findings of Zietlow and colleagues (25), could also be an atypically increased salivary cortisol concentration and reactivity of the child as a consequence of the Face-to-Face-Still-Face paradigm (FFSF). Furthermore, maternal HCC has been associated with infant salivary cortisol levels when the mothers were more intrusive and had lower positive engagement synchrony in the interaction with their infants (27). Thus, there appears to be an interrelation between the stress response systems of mother and child.
Negative interactions between mother and child occur as a chronic stressor. Therefore, the child's brain might be exposed to chronically elevated levels of cortisol, which may result in increased HCC in the child (19, 21). A study looking at chronic biological stress levels of parents and preschoolers found a moderation of the association between parental and child HCC by emotion regulation skills of the child (28). Meaning, children with good emotion regulation abilities were not as affected by intergenerational transmission effects of chronic stress. Furthermore, such children showed less strong associations between parental financial status and HCC. In contrast, children with less developed emotion regulation were found to have an increased HCC, which was negatively associated with the socioeconomic status (SES) of the family. Vaghri and colleagues (29) also found a stable negative correlation between HCC in children and parental education levels. This might be due to the exposure to various social stressors because of lower financial resources. Thus, consideration of those variables in the context of cortisol research is important.
To conclude, atypical maternal interaction patterns with the child can act as psychosocial stressors negatively affecting its development as well as mental and physical health in later life. However, to our knowledge, no study so far investigated the relationship between atypical maternal behavior and the child's neuroendocrine stress response measured via HCC. The aim of this study was to fill this gap. We hypothesized that higher atypical maternal interaction behavior (operationalized by the Atypical Maternal Behavior Instrument for Assessment and Classification [AMBIANCE] (30); would be positively associated with higher HCC of infants.
Within the project TransGen, mother and infant dyads were investigated longitudinaly starting from birth. The recruitment took place in the women's hospital of the University hospital of Ulm shortly after parturition. The study was financially supported by the German Federal Ministry of Education and Research BMBF and approved by the local Ethics Committee of Ulm.
The recruitment of mother-child-dyads (N = 533) started in October 2013 within 1 to 6 days after parturition (timepoint t0). Mothers with twins were not recruited for the study. At t0, mothers provided written informed consent before participating in the study. They then took part in an initial screening interview. CM load was assessed using the Childhood Trauma Questionnaire [CTQ, (31)] including emotional, physical and sexual abuse as well as physical and emotional neglect. All mother–child-dyads were invited at three sequential time points: 3 months (t1), 12 months (t2), and 24 to 36 months after birth (t3). The following data regarding the Atypical Maternal Behavior Instrument for Assessment and Classification (AMBIANCE) scale (30) and HCC of infants were assessed at t2. Likewise, depressive symptomatology was assessed with the Brief Symptom Inventory [BSI, (32)]. For data collection, all mother-child-dyads were invited from 10 a.m. to 1 p.m. to the Department of Child and Adolescent Psychiatry/Psychotherapy at the Ulm University Hospital. During their visit, mothers and children were first asked to listen to a calming digital lullaby (episode 1). Afterwards, all mother-infant-dyads performed the Strange Situation Procedure, for which the AMBIANCE was than later coded.
In total, N = 112 mother-child-dyads participated at both time points t0 and t2. One person had to be excluded from the sample due to taking cortisone medication. The average age of participating mothers was M = 34 years (SD = 5), ranging from 21 to 45 years. Considering educational qualifications (measured as an ordinal variable with a range from 2 = “lowest school education level” to 5 = “highest school education level”), 71.9% of all mothers reported a high school diploma, whereas 21.6% had a secondary school diploma, and 6.6% had a lower secondary diploma as the highest education certificate. The mean T-value measured with the BSI at time point t2 was M = 46.71 (SD = 8.42). n = 6 of the mothers from this study reported depressive symptoms in the conspicuous range with T > 60. The average age of all infants was M = 53.22 weeks (SD = 5.25) with their ages ranging from 44 to 78 weeks. Almost half of all infants (48.2%) were males.
All Strange Situation Procedure sessions were videotaped to analyze the quality of maternal interactive behavior between the mother and her infant using the AMBIANCE (30). Lyons-Ruth and colleagues (33) based the development of the AMBIANCE instrument on Main and Hesse's theory, which explains the frightened, frightening, and dissociated parental behavior (34, 35). Therefore, they considered profound disruptions in mother-child interactions and emotional as well as physical withdrawal behaviors as anomalous parental behavior of mothers during the interactions with their children (36). The AMBIANCE is a coding system that assesses disrupted maternal behaviours on five dimensions on a 7-point scale: (1) affective communication errors, (2) role/boundary confusion, (3) disorganized/ disoriented behaviors, (4) negative/intrusive behavior, and (5) withdrawal. For a final assessment, an overall score of the general level of disruption is determined. This score is based on the displayed level of intensity and frequency of disrupted behaviors during the recorded mother-child-interaction, whereby a level of disrupted communication of up to 4 is considered “not-disrupted” and a level of 5–7 is considered “disrupted”. A single coder, who was trained by and reliable according to the original developers of the AMBIANCE, scored all play sessions blinded to the data sets of the mother-infant-dyads (30).
At t2, hair strands of mothers and their children were collected from the posterior vertex region of the scull, preferably cut as close as possible to the scalp. Following the recommendations of the Society of Hair Testing, two to three hair strands with a diameter of at least 3 mm were collected to have sufficient hair material for the subsequent biolaboratory analyses (37, 38). Under sterile conditions, the hair samples were wrapped with aluminium foil and stored at −20°C until preanalytical processing. Preprocessing of all hair samples was performed in the laboratory of Ulm University. To avoid contamination of the hair with skin moisture, hair samples were processed using laboratory gloves. Hair strands of the same subject were pooled. From the proximal end, hair strands were cut into 3 cm long segments to assess HCC of the last 3 months prior to sampling. According to a study by de Kruijff and colleagues (39) childrens hair grows approx. 1 cm/month already at this age. Hair segments were then placed into cryotubes with a standardized hair weight (range 4–6 mg) per sample. Samples were shipped to the laboratory of Prof. Dr. Kirschbaum at the Technical University of Dresden in Germany for analysis. With reference to the protocol of Gao and colleagues (40), every 3 cm hair segment was washed with isopropanol twice and dried for at least 12 h under a stream of nitrogen gas. Subsequently, cortisol was extracted by placing the same non-pulverized hair segment in a methanol solution at room temperature overnight. The supernatant which remained after centrifugation (10,000 rpm for 2 min) was used, while the methanol was evaporated at 65°C under a constant nitrogen stream. All dried samples were then resuspended in 150 μl double-distilled water. Mass spectrometry-analysis of HCC was conducted using a Shimadzu HPLC system (Shimadzu, Canby, OR) coupled to an ABSciex API 5,000 Turbo ion-spray triple quadruple platform (AB Sciex, Foster City, CA) as reported previously (38).
Data were analyzed using R version 4.2.1 (41) and p-values ≤ 0.05 were considered as significant. Due to the skewed distributions of HCC data, the natural logarithm was applied and logarithmized data were used in further analyses. In advance, boxplots were used to identify potential outliers. Three potential outliers were identified (at least > 2 SD). The outliers showed no physiological or medical reason for exclusion. However, adding or removing these data points did not change the pattern of results and they were therefore retained in the analyses.
For multiple regression models, assumptions of linear regression were checked visually using scatter plots, standardized residuals, and leverages (to check for linearity as well as for outliers) and P-P plots (to check for normal distribution of the residuals). The tolerance and variance inflation factor values were used to check for multicollinearity.
Due to skewness and outliers in HCC data, the use of traditional parametric methods was considered inappropriate. Thus robust multiple linear regression models [R package: robust, (42)], with HC4 estimators for heteroscedasticity were calculated to test the second hypothesis. Due to theoretical overlap and intercorrelation of the AMBIANCE subscales with the AMBIANCE global score, two separate robust regression models were calculated. We used AIC and BIC for model selection to distinguish among a set of possible models describing the relationship between HCC and the AMBIANCE global score (model 1), and respectively the five AMBIANCE subscales (model 2). The two models with the best model-to-data fit were selected for analysis. For all analyses, maternal age and education level (categorical variable: high school diploma, secondary school diploma, lower secondary diploma) and child's sex were considered as additional covariates. The best fit for model 1 included the AMBIANCE global score and mother's education as covariate. The best fit for model 2, regarding the AMBIANCE subscales included: role/boundary confusion, negative/intrusive behavior and mother's education as covariates.
The descriptive statistics of the AMBIANCE global score, its subscales and HCC are provided in Table 1.
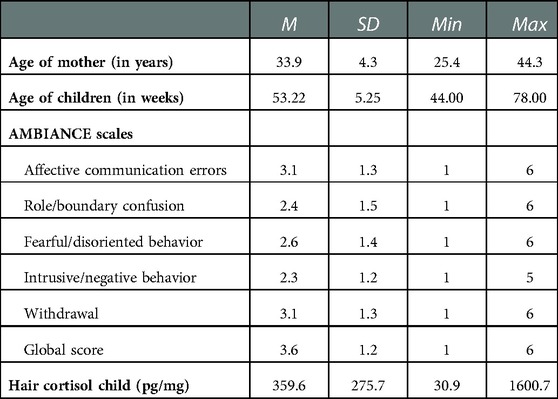
Table 1. Descriptive statistics of AMBIANCE subscales, AMBIANCE global score, and child's hair cortisol for N = 111 mother-child-dyads.
The results of the two multiple linear regression models are shown in Tables 2, 3 and illustrated in Figures 1, 2.
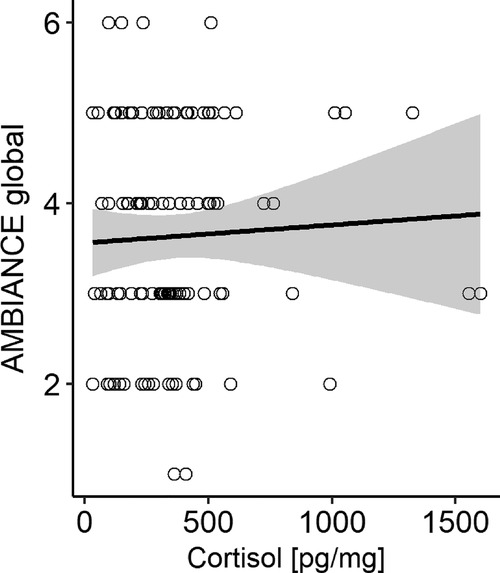
Figure 1. Scatterplot with HCC raw data for robust regression model including AMBIANCE global score as predictor. Grey areas depict the 95% confidence interval.
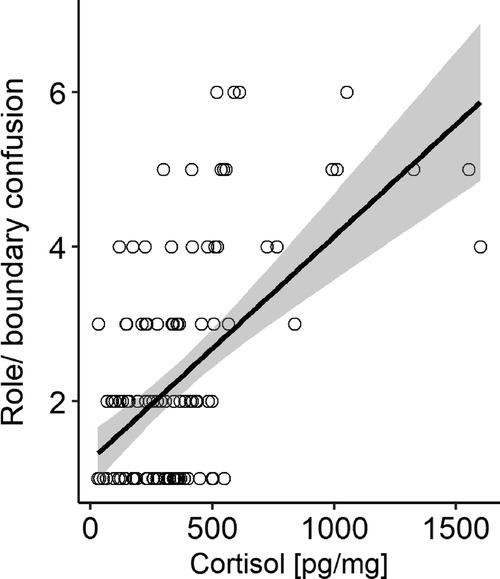
Figure 2. Scatterplot with HCC (pg/mg) raw data for robust regression model including AMBIANCE scale role/boundary confusion as predictor. Grey areas depict the 95% confidence interval.
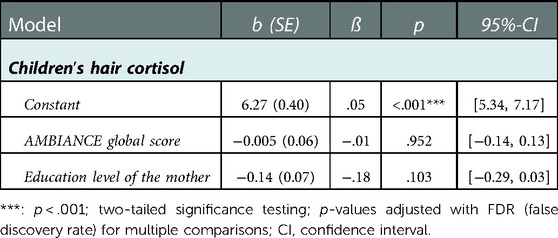
Table 2. Results of robust multiple linear regression with AMBIANCE global score as predictor for child's hair cortisol level and maternal education as covariate.
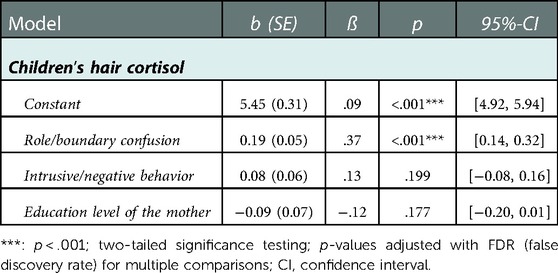
Table 3. Results of robust multiple linear regression with AMBIANCE subscales role/boundary confusion and intrusive/negative behavior as predictors for child's hair cortisol level and maternal education.
In the first model, the AMBIANCE global score was a predictor, while mother's education level was entered as a covariate: the overall model fit was not significant [F(2,108) = 1.92, p = .152], i.e., the model did not explain the data better than a simple overall mean model. This was also reflected in the explained variance of childrens' HCC levels which was only around 4%.
In Model 2, the subscales of the AMBIANCE “role reversal” and “intrusive/negative behavior” were entered as predictors for infants HCC, while mother's education was included as a covariate. The overall model was significant [F(3,107) = 12.21, p < .001] and explained 24% of the variance. Only the factor “role/boundary confusion” (p < .001) significantly predicted infants HCC.
This study investigated the association of various atypical maternal interaction patterns (as measured with the AMBIANCE global score and its subscales) with the children's HCC one year after birth. While the AMBIANCE global score was not associated with infant's HCC, the subscale “role/boundary confusion” in the AMBIANCE, was associated positively with higher HCC in children, i.e., the more inappropriate mother's behaviour in this subscale, the higher the HCC of the child. Therefore, this type of atypical maternal behavior might be a psychosocial stressor in early childhood linked to an altered cortisol secretion, endangering childrens mental and biological development and health. However, other explanations are equally plausible as the behaviour of mothers and the HCC of children could be influenced by a third unknown variable such as biological factors [e.g., higher levels of inflammation due to shared environment such as diet, living context (living close to busy streets with high levels of pollution, lack of green space), a pro-inflammatory diet, etc.] which might translate in atypical maternal interaction behaviour and higher HCC in children. Unfortunately, we did not directly assess the level of inflammation in our sample and cannot completely rule out inflammation as one factor underlying this association.
The association between more role confusing maternal behavior and higher HCC in children might indicate that this form of atypical interaction of the mother represents a psychosocial stressor that contributes (at least partially) to an increased biological stress response in the child. As HCC is a measure of chronic stress hormone accumulation over the last three months, this might suggest that these behaviors of the mother were not exclusively displayed in the artificial examination situation but are displayed regularly in everyday life. This interpretation could be in line with previous studies, which showed a correlation between inadequate interaction as well as cortisol levels of the mother in saliva and hair with the salivary cortisol of the child (24, 27).
Role reversal is described as the transfer of parental roles and functions to the child that should be addressed/fulfilled by the mother's partners or friends (43). More specifically, this means that children take over the care of the mother's needs (44). Macfie and colleagues (44) consider this a major risk for healthy child development. Indeed, if role reversal is present it can lead to the development of various psychopathologies later in life (45, 46). Parents with adverse childhood experiences are particularly prone to this kind of atypical interaction as they often show difficulities maintaining functioning relationships with peers (47). Thus, they try to meet their needs with the help of their child and seek the missing emotional support within this relationship. In the long run, if the mother's demands exceed the child's psychosocial and emotional resources, this can impede the child's psychosocial and emotional development (44). Hence our results emphasize atypical maternal interaction patterns, especially role reversal, as a critical psychosocial stressor presumably contributing to elevated stress levels in children. Consequently, this might partially contribute to permanently altered HCC and possibly also to higher inflammation levels in children. This influence seems to be stronger than the influence of maternal education as this factor was not significant in the regression models.
We observed no correlation of maternal age with any AMBIANCE score in the present study. In contrast, previous studies observed that the children of older mothers had on average lower HCC levels (48). Similarly, while previous studies found an influence of education on HCC of children (28), we observed no such association.
In contrast to our hypotheses, the subscales withdrawal, fearful/disoriented behavior and the global score of the AMBIANCE were not significantly correlated with HCC and were no significant predictors for infant's HCC. However, in a study by Khoury and colleagues (49), a correlation was found between maternal HCC and specifically increased withdrawal behavior but only when the mother also reported increased severity in depressive symptoms. It is possible that withdrawal behaviors represent a particular variation in the interaction, as Khoury et al. (49) found that only in individuals with severe depression there was a significant correlation between withdrawal behaviors and maternal HCC. In addition, the other subtypes of atypical interaction (e.g., role/boundary confusion) might induce stronger psychosocial and biological stress responses in the child and interfere more with its emotional regulation as compared to withdrawal or fearful/disoriented behavior, as there might be more intrusive/erratic behavior displayed by the mother than in passive withdrawal. In contrast, if mothers show inappropriate externalizing or unpredictable behavior towards their child, a withdrawal by the mother might be experienced as a short-time relief. As a consequence, the child could reorient without being confronted with repeated potential stressful interactions.
Our study cohort comprised predominantly healthy women in the postpartum period, living mostly in a committed relationship, with a high level of education, and relatively high socioeconomic status. Atypical maternal interaction behavior in our healthy community sample was comparably low, and—given the relatively high SES, this distribution might underestimate the effect sizes of atypical interactions on HCC. An intentional oversampling of at-risk mothers could be a solution in future studies. Therefore it should be kept in mind when applying the results to other cohorts and contexts that the generalizability might be limited. Nevertheless, social desirability effects were avoided in the classification of the interactions as this was based on external raters and not on self-assessment by the mothers themselves. In future studies additional relevant factors should be considered such as children's and parents’ level of inflammation and environmental factors contributing to a pro-inflammatory state in the body as these factors might have an influence on cortisol. In addition, breastfeeding should be considered in future studies, as findings from previous studies show that breastfeeding is associated with lower cortisol levels in children [e.g., (50)].
We found inappropriate parenting behavior, more specifically role/boundary confusion, to be associated with higher HCC in the children. By measuring hair cortisol in this study, it was possible to determine the average long-term activity of the child's stress response system, therefore the increased HCC might indicate an increased state of allostatic load in the affected children, which might create a higher risk of mental and physical problems later in life. Future studies on the impact of maternal parenting behavior on HCC should assess additional relevant factors for allostatic load, such as inflammatory processes in the course of child development. For instance, it should be investigated whether more inflammation in the mother is associated with more maternal role reversal and whether role/boundary confusion and/or inflammation or the interplay of both can explain the increased risk for mental and physical illness later in life. The findings of this study highlight the importance of early intervention programs that focus on the early interaction between mother and child. However, before too far-reaching conclusions are drawn on the implications of the observed findings for interventions, the results should be replicated in future studies with at risk families.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee of Ulm University. The patients/participants provided their written informed consent to participate in this study.
FKD, IM, MH, LM, KR and AK: analyzed and interpreted the data regarding the effect of maternal attachment behavior on mother and child's hair cortisol concentration. MH: preprocessed childrens hair samples and revised the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
The study was funded by the Federal Ministry of Education and Research (Grant no. 01KR1304A) (BMBF, 2013-2016, additional interim funding 2017). A. M. Bach and M. Hitzler were supported by a scholarship of the Konrad Adenauer Foundation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AMBIANCE, atypical maternal behavior instrument for assessment and classification; CM, childhood maltreatment; DV, dependent variable; HCC, hair cortisol concentration; HPA, hypothalamic-pituitary-adrenal; IV, independent variable; PSS14, perceived stress questionnaire-14; PSSQ, psychosocial support questionnaire; SES, socioeconomic status.
1. Bornstein MH. Parenting infants. In: Bornstein MH, editors. Handbook of parenting. Mahwah: Lawrence Erlbaum Associates (2002). p. 3–43.
2. Schroeder VM, Kelley ML. Family environment and parent-child relationships as related to executive functioning in children. Early Child Dev Care. (2010) 180(10):1285–98. doi: 10.1080/03004430902981512
3. De Wolff MS, van IJzendoorn MH. Sensitivity and attachment: a meta-analysis on parental antecedents of infant attachment. Child Dev. (1997) 68:571–91. doi: 10.1111/j.1467-8624.1997.tb04218.x
4. Korja R, Ahlqvist-Björkroth S, Savonlahti E, Stolt S, Haataja L, Lapinleimu H, et al. Relations between maternal attachment representations and the quality of mother-infant interaction in preterm and full-term infants. Infant Behavior and Development. (2010) 33(3):330–6. doi: 10.1016/j.infbeh.2010.03.010
5. Moran G, Forbes L, Evans E, Tarabulsy GM, Madigan S. Both maternal sensitivity and atypical maternal behavior independently predict attachment security and disorganization in adolescent mother–infant relationships. Infant Behav Dev. (2008) 31(2):321–5. doi: 10.1016/j.infbeh.2007.12.012
6. Forbes LM, Evans EM, Moran G, Pederson DR. Change in atypical maternal behavior predicts change in attachment disorganization from 12 to 24 months in a high-risk sample. Child Dev. (2007) 78(3):955–71. doi: 10.1111/j.1467-8624.2007.01043.x
7. Conway LJ, Levickis PA, Smith J, Mensah F, Wake M, Reilly S. Maternal communicative behaviours and interaction quality as predictors of language development: findings from a community-based study of slow-to-talk toddlers. Int J Lang Comm Disorders. (2018) 53(2):339–54. doi: 10.1111/1460-6984.12352
8. Easterbrooks MA, Bureau J-F, Lyons-Ruth K. Developmental correlates and predictors of emotional availability in mother–child interaction: a longitudinal study from infancy to middle childhood. Dev Psychopathol. (2012) 24(1):65–78. doi: 10.1017/S0954579411000666
9. Gianino AA, Tronick EZ. The mutual regulation model: the infant's Self and interactive regulation and coping and defensive capacities. In: Field TM, McCabe PM, editors. Schneiderman N, editors. Stress and coping across development. Hillsdale: Lawrence Erlbaum Associates, Inc (1988). p. 47–68.
10. Dutra L, Bureau JF, Holmes B, Lyubchik A, Lyons-Ruth K. Quality of early care and childhood trauma: a prospective study of developmental pathways to dissociation. J Nerv Ment Dis. (2009) 197(6):383. doi: 10.1097/NMD.0b013e3181a653b7
11. Hohm E, Laucht M, Zohsel K, Schmidt MH, Esser G, Brandeis D, et al. Resilienz und ressourcen im verlauf der entwicklung. Kindheit und Entwicklung. (2017) 26(4):230–90. doi: 10.1026/0942-5403/a000236
12. Lecompte V, Moss E. Disorganized and controlling patterns of attachment, role reversal, and caregiving helplessness: links to adolescents’ externalizing problems. Am J Orthopsychiatry. (2014) 84(5):581–9. doi: 10.1037/ort0000017
13. Madigan S, Voci S, Benoit D. Stability of atypical caregiver behaviors over six years and associations with disorganized infant–caregiver attachment. Attach Hum Dev. (2011) 13:237–52. doi: 10.1080/14616734.2011.562410
14. Agostini A, Rizzello F, Ravegnani G, Gionchetti P, Tambasco R, Ercolani M, et al. Parental bonding and inflammatory bowel disease. Psychosomatics. (2010) 51(1):14–21. doi: 10.1016/s0033-3182(10)70654-x
15. Jacobs MA, Spilken AZ, Norman MM, Anderson L, Rosenheim E. Perception of faulty parent-child relationships and illness behavior. J Consult Clin Psychol. (1972) 39(1):49–55. doi: 10.1037/h0033176
16. Johnson SB, Riley AW, Granger DA, Riis J. The science of early life toxic stress for pediatric practice and advocacy. Pediatrics. (2013) 131(2):319–27. doi: 10.1542/peds.2012-0469
17. Pless IB, Roghmann KJ. Chronic illness and its consequences: observations based on three epidemiologic surveys. J Pediatr. (1971) 79(3):351–9. doi: 10.1016/S0022-3476(71)80141-5
18. Siniatchkin M, Darabaneanu S, Gerber-Von Müller G, Niederberger U, Petermann F, Schulte IE, et al. Kinder mit migräne und asthma: zur rolle der eltern-kind-interaktion. Kindheit Und Entwicklung. (2010) 19(1):27–35. doi: 10.1026/0942-5403/a000005
19. Clark ELM, Jiao Y, Sandoval K, Biringen Z. Neurobiological implications of parent–child emotional availability: a review. Brain Sci. (2021) 11(8):1016. doi: 10.3390/brainsci11081016
20. Frodl T, O’Keane V. How does the brain deal with cumulative stress? A review with focus on developmental stress, HPA axis function and hippocampal structure in humans. Neurobiol Dis. (2013) 52:24–37. doi: 10.1016/j.nbd.2012.03.012
21. Gunnar M, Talge NM. Neuroendocrine measures in developmental research. In: Schmidt LA, Segalowitz SJ, editors. Developmental psychophysiology: Theory, systems, and methods. Published online by Cambridge University Press (2008). p. 343–64.
22. Wesarg C, Van Den Akker AL, Oei NYL, Hoeve M, Wiers RW. Identifying pathways from early adversity to psychopathology: a review on dysregulated HPA axis functioning and impaired self-regulation in early childhood. Eur J Dev Psychol. (2020) 17(6):808–27. doi: 10.1080/17405629.2020.1748594
23. Hitzler M, Karabatsiakis A, Kolassa IT. Biomolecular vulnerability factors of mental disorders; influence of chronic and traumatic stress on the immune system, free radicals and mitochondria. Psychotherapeut. (2019) 64(4):329–49. doi: 10.1007/s00278-019-0366-9
24. Smeekens S, Marianne Riksen-Walraven J, Van Bakel HJ. Cortisol reactions in five-year-olds to parent–child interaction: the moderating role of ego-resiliency. J Child Psychol Psychiatry. (2007) 48(7):649–56. doi: 10.1111/j.1469-7610.2007.01753.x
25. Zietlow AL, Nonnenmacher N, Reck C, Ditzen B, Müller M. Emotional stress during pregnancy–associations with maternal anxiety disorders, infant cortisol reactivity, and mother–child interaction at pre-school age. Front Psychol. (2019) 10:2179. doi: 10.3389/fpsyg.2019.02179
26. Köhler-Dauner F, Clemens V, Hildebrand K, Ziegenhain U, Fegert JM. The interplay between maternal childhood maltreatment, parental coping strategies as well as endangered parenting behavior during the current SARS-CoV-2 pandemic. Dev Child Welf. (2021) 3(2):71–84. doi: 10.1177/2F25161032211014899
27. Tarullo AR, John AMS, Meyer JS. Chronic stress in the mother-infant dyad: maternal hair cortisol, infant salivary cortisol and interactional synchrony. Infant Behav Dev. (2017) 47:92–102. doi: 10.1016/2Fj.infbeh.2017.03.007
28. Kao K, Tuladhar CT, Meyer JS, Tarullo AR. Emotion regulation moderates the association between parent and child hair cortisol concentrations. Dev Psychobiol. (2019) 61(7):1064–78. doi: 10.1002/dev.21850
29. Vaghri Z, Guhn M, Weinberg J, Grunau RE, Yu W, Hertzman C. Hair cortisol reflects socio-economic factors and hair zinc in preschoolers. Psychoneuroendocrinology. (2013) 38(3):331–40. doi: 10.1016/2Fj.psyneuen.2012.06.009
30. Bronfman E, Madigan S, Lyons-Ruth K. Atypical maternal behavior instrument for assessment and classifcation (AMBIANCE). Manual for coding disrupted affective communication. Cambridge: Department of Psychiatry, Harvard Medical School; 1992–2009 (Unpublished manual).
31. Bader K, Hänny C, Schäfer V, Neuckel A, Kuhl C. Childhood trauma questionnaire-psychometrische eigenschaften einer deutschsprachigen version. Z Klin Psychol Psychother. (2009) 38(4):223–30. doi: 10.1026/1616-3443.38.4.223
32. Derogatis LR. Brief Symptom Inventory (BSI), administration, scoring, and procedures manual. 3rd ed. Minneapolis: National Computer Services (1993).
33. Lyons-Ruth K, Bronfman E, Parsons E. Maternal frightened, frightening, or atypical behavior and disorganized infant attachment patterns. In: Vondra J, Barnett D, editors. Atypical patterns of infant attachment. Monographs of the society for research in child development, Vol. 64. Wiley (1999). p. 67–96.
34. Hesse E, Main M. Second-generation effects of unresolved trauma in non-maltreating parents: dissociated, frightened, and threatening parental behavior. Psychoanal Inq. (1999) 19(4):481–540. doi: 10.1080/07351699909534265
35. Main M, Hesse E. Parents’ unresolved traumatic experiences are related to infant disorganized attachment status: is frightened and/or frightening parental behavior the linking mechanism? In: Greenberg M, Cicchetti D, Cummings E, editors. Attachment in the preschool years: theory, research, and intervention. Chicago: University of Chicago Press (1990). p. 161–82.
36. Grienenberger J, Kelly K, Slade A. Maternal reflective functioning, mother-infant affective communication, and infant attachment: exploring the link between mental states and observed caregiving behavior in the intergenerational transmission of attachment. Attachment Hum Dev. (2005) 7:299–311. doi: 10.1080/14616730500245963
37. Cooper GAA, Kronstrand R, Kintz P. Society of hair testing guidelines for drug testing in hair. Forensic Sci Int. (2012) 218(1-3):20–4. doi: 10.1016/j.forsciint.2011.10.024
38. Schury K, Koenig AM, Isele D, Hulbert AL, Krause S, Umlauft , et al. Alterations of hair cortisol and dehydroepiandrosterone in mother-infant-dyads with maternal childhood maltreatment. BMC Psychiatry. (2017) 17(1):213. doi: 10.1186/s12888-017-1367-2
39. de Kruijff I, Noppe G, Kieviet N, Choenni V, Lambregtse-van den Berg MP, Begijn DG, et al. LC-MS/MS-based reference intervals for hair cortisol in healthy children. Psychoneuroendocrinology. (2020) 112:104539. doi: 10.1016/j.psyneuen.2019.104539
40. Gao W, Stalder T, Foley P, Rauh M, Deng H, Kirschbaum C. Quantitative analysis of steroid hormones in human hair using a column-switching LC-APCI-MS/MS assay. J Chromatogr B Analyt Technol Biomed Life Sci. (2013) 928:1–8. doi: 10.1016/j.jchromb.2013.03.008
41. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2019).
42. Wang J, Zamar R, Marazzi A, Yohai V, Salibian-Barrera M, Maronna R, et al. Package ‘robust’. (2022). https://cran.r-project.org/web/packages/robust/robust.pdf
43. Macfie J, Fitzpatrick KL, Rivas EM, Cox MJ. Independent influences upon mother–toddler role reversal: infant–mother attachment disorganization and role reversal in mother's Childhood. Attach Hum Dev. (2008) 10(1):29–39. doi: 10.1080/14616730701868589
44. Macfie J, Brumariu LE, Lyons-Ruth K. Parent–child role-confusion: a critical review of an emerging concept. Dev Rev. (2015) 36:34–57. doi: 10.1016/j.dr.2015.01.002
45. Shaffer A, Egeland B. Intergenerational transmission of familial boundary dissolution: observations and psychosocial outcomes in adolescence. Fam Relat. (2011) 60(3):290–302. doi: 10.1111/j.1741-3729.2011.00653.x
46. Obsuth I, Hennighausen K, Brumariu LE, Lyons-Ruth K. Disorganized behavior in adolescent–parent interaction: relations to attachment state of mind, partner abuse, and psychopathology. Child Dev. (2014) 85(1):370–87. doi: 10.1111/cdev.12113
47. Sroufe LA, Rutter M. The domain of developmental psychopathology. Child Dev. (1984) 55(1):17–29. doi: 10.2307/1129832
48. Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, Ottaviani E, et al. Inflamm-aging: an evolutionary perspective on immunosenescence. Ann N Y Acad Sci. (2000) 908(1):244–54. doi: 10.1111/j.1749-6632.2000.tb06651.x
49. Khoury JE, Bosquet Enlow M, Patwa MC, Lyons-Ruth K. Hair cortisol in pregnancy interacts with maternal depressive symptoms to predict maternal disrupted interaction with her infant at 4 months. Dev Psychobiol. (2020) 62(6):768–82. doi: 10.1002/dev.21950
Keywords: mother-child interaction, chronic stress, endocrine stress response, hair cortisol concentrations (HCC), intergenerational transmission
Citation: Köhler-Dauner F, Mayer I, Hitzler M, Karabatsiakis A, Matits L, Bach AM, Rost K, Fegert JM, Kolassa I and Ziegenhain U (2023) Atypical maternal interaction is associated with elevated levels of hair cortisol in children. Front. Pediatr. 10:994882. doi: 10.3389/fped.2022.994882
Received: 15 July 2022; Accepted: 7 December 2022;
Published: 25 January 2023.
Edited by:
George Paltoglou, National and Kapodistrian University of Athens, GreeceReviewed by:
Andrea De Giacomo, University of Bari Aldo Moro, Italy© 2023 Köhler-Dauner, Mayer, Hitzler, Karabatsiakis, Matits, Bach, Rost, Fegert, Kolassa and Ziegenhain. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franziska Köhler-Dauner ZnJhbnppc2thLmtvZWhsZXItZGF1bmVyQHVuaWtsaW5pay11bG0uZGU=
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.