
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr., 28 September 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.983367
This article is part of the Research TopicAdvances of Health Care Transition for Patients with Childhood-onset Chronic Diseases: International Perspectives, Volume IIView all 17 articles
 Jiro Takeuchi1
Jiro Takeuchi1 Yoshitoki Yanagimoto2
Yoshitoki Yanagimoto2 Yuki Sato3
Yuki Sato3 Ryota Ochiai4
Ryota Ochiai4 Akinori Moriichi3
Akinori Moriichi3 Yuko Ishizaki5*
Yuko Ishizaki5* Takeo Nakayama6
Takeo Nakayama6Objective: We inspected efficacious interventions to improve the transition readiness of adolescent and young adult patients with childhood-onset chronic illnesses using the Transition Readiness Assessment Questionnaire (TRAQ).
Methods: Our narrative review was conducted on randomized control studies assessed with TRAQ for outcome measurement before and after the interventions. We included all patients with chronic diseases. We searched eight electronic database(s): Allied and Complementary Medicine Database (AMED) Allied and Complementary Medicine, BioSciences Information Service of Biological Abstracts (BIOSIS) Previews, Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Library, Embase, Ichu-shi, Medline, and Web of Science. The text words for the search of data sources were as follows: “(“transition readiness assessment questionnaire” OR TRAQ) AND 2011/01:2022/06[DP] AND (clinical AND trial OR clinical trials OR clinical trial OR random* OR random allocation).” More studies were identified from the references in our reported study. This data set was independently cross-checked by two reviewers.
Results: We identified 261 reports and collected three articles. The target diseases were type-1 diabetes, congenital heart disease, cystic fibrosis, and inflammatory bowel disease. All the studies excluded patients with intellectual disabilities. The age of the participants was distributed between 12 and 20 years. Nurse-provided web-based intervention of transition readiness was constructed using digital resources in two studies. The intervention ranged from 6 to 18 months. All the interventions were efficacious in improving transition readiness assessed with TRAQ scores, except for the self-advocacy score.
Conclusions: We obtained three randomized control studies with TRAQ for outcome measurement. In two studies, web-based and nurse-led organized interventions were shown to improve transition readiness.
There is a growing concern about what medical care should be for adolescent and young adult patients with childhood-onset chronic diseases around the world. American Academy of Pediatrics, jointly with the American Academy of Family Physicians and American College of Physicians – American Society of Internal Medicine issued a Consensus Statement on Health Care Transitions for Young Adults with Special Health Care Needs in 1992 (1). While most young adults with special health care needs are able to become adults, many patients with severe medical conditions and disabilities — which limit their ability to function and result in complicated social, emotional, or behavioral sequelae — experience difficulty while transitioning from child to adult health care systems (1). Transition readiness is associated with independent self-care behaviors and patient quality of life, in addition to the appropriate shift to adult health care systems. The specific methodology for the transition is summarized in Six Core Elements (2). However, it has not been clarified as to what kind of interventions are effective in promoting self-care skills in adolescents and young adults with chronic diseases. In order to evaluate the efficacy of interventions aimed at transition to adult health care systems, it may be appropriate to examine the transition readiness status by interventions. At the moment, there are 10 kinds of tools to assess transition readiness. Among them, the Transition Readiness Assessment Questionnaire (TRAQ) (3) and TRxANSITION (4) have been verified for enough reliability and validity. Moreover, TRAQ, developed in 2011 (5, 6), has acquired internal validity, construct validity, and internal consistency (7). A higher TRAQ score indicates knowledge of the disease, skill, self-efficacy, positive outlook toward the future, and health-related quality of life (8–11). Conversely, a lower TRAQ score indicates non-adherence to drug therapy (12). In this study, we tried to review high-quality interventional research using the TRAQ for the outcome measurement to identify efficacious interventions and thus improve transition readiness for patients with childhood-onset chronic disease. We targeted randomized controlled studies for high-quality interventional research to avoid selection bias and confounding bias. The aspects to be addressed in this narrative review are as follows: participants, intervention, control, and outcome. We confirmed that increasing the score between the intervention group and control group allows for assessment of the quality of transition readiness. Therefore, employing efficacious interventions can improve the outcomes of the patients.
All randomized control trials assessed with the TRAQ before and after the intervention were included. Our narrative review was conducted by partially following the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols 2020 (PRISMA 2020) as a guide for the systematic review and meta-analysis protocol (13).
We established eligibility criteria and exclusion criteria before the identification and selection of studies. The eligibility criteria are as follows: (1) research papers and not protocols or reviews and (2) studies assessed with TRAQ. The exclusion criteria are as follows: (1) non-intervention studies and (2) non-randomized studies.
We included all patients who were diagnosed with childhood-onset chronic illness.
On 18 June 2022, we searched eight electronic databases: Allied and Complementary Medicine Database (AMED) (14), BioSciences Information Service of Biological Abstracts (BIOSIS) Previews (15), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (16), the Cochrane Library (17), Embase (18), Ichu-shi (in Japanese) (19), Medline (20), and Web of Science (21) for articles from 1st January 2011 to 30th June 2022. The text words used for the search were as follows: “(“transition readiness assessment questionnaire” OR TRAQ) AND (clinical AND trial OR clinical trials OR clinical trial OR random* OR random allocation) AND 2011/01:2022/06[DP].” We checked the updates to all the databases through 30 June 2022. Additionally, more studies were identified from the references in our past reports. No limitation was imposed with regard to language. Publication type was limited to research papers of any length.
First, we identified eligible studies through electronic searches and excluded duplicates. Second, we identified eligible studies and excluded duplicates of the same study by referring to the study title. Third, two reviewers (JT and YY) independently checked the reports at the title/abstract level and identified potentially relevant studies among the research assessed with TRAQ. Fourth, we assessed the studies and decided whether to include them based on the same eligibility criteria as the aspects of the randomized intervention. Any disagreements were resolved by an additional reviewer (YI).
Characteristics of the studies, patients, interventions, and outcome measures were collected from each included study. Characteristics of the studies were established as columns in one table, and characteristics of the patients, interventions, and outcome measures were established as columns in another table.
One reviewer (JT) put the above data as variables into a data set in MS Excel. This data set was independently cross-checked by another reviewer (YY). They consulted with an additional reviewer (YI) regarding the variables with missing information. If we could not solve a problem, we employed expert opinion.
This narrative review does not require ethical approval. The data used here are neither individual nor private.
We searched eight database records identified (n = 261) from the following: no study from AMED, 90 studies from BIOSIS Previews, 4 studies from CINAHL, 92 studies from the Cochrane Library, 35 studies from Embase, 10 studies from Ichu-shi (Japanese), 15 studies from Medline, and 15 studies from Web of Science. After removing the duplicates, 147 studies were identified. After checking the reports at the title and abstract level, 47 studies were identified as potentially relevant. The excluded 100 studies were deemed to focus on other research themes. Of the remaining 47 studies, 11 studies were without an abstract or only included an abstract; 10 only included protocols; 3 were reviews; 10 included other questionnaires and not TRAQ; 5 were without intervention, and the last 6 were without randomization; therefore, we excluded these 45 studies. Finally, we included two randomized control studies (22, 23) in our review. An additional study (24) was identified from the references of our previous report (25). Overall, our study included three randomized control studies. The characteristics of the studies are presented in Table 1. All the reports are original articles in English. The collected data are presented in Table 2.
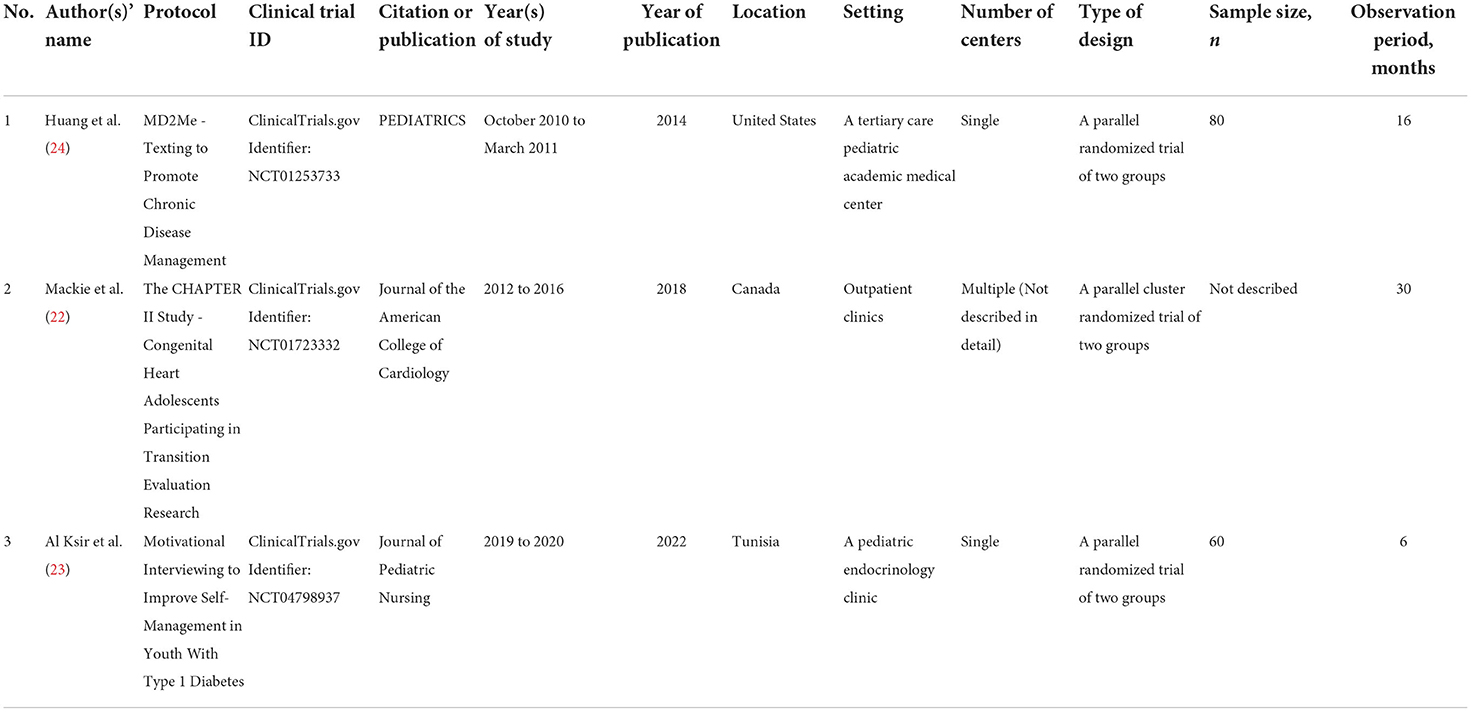
Table 1. Characteristics of studies.
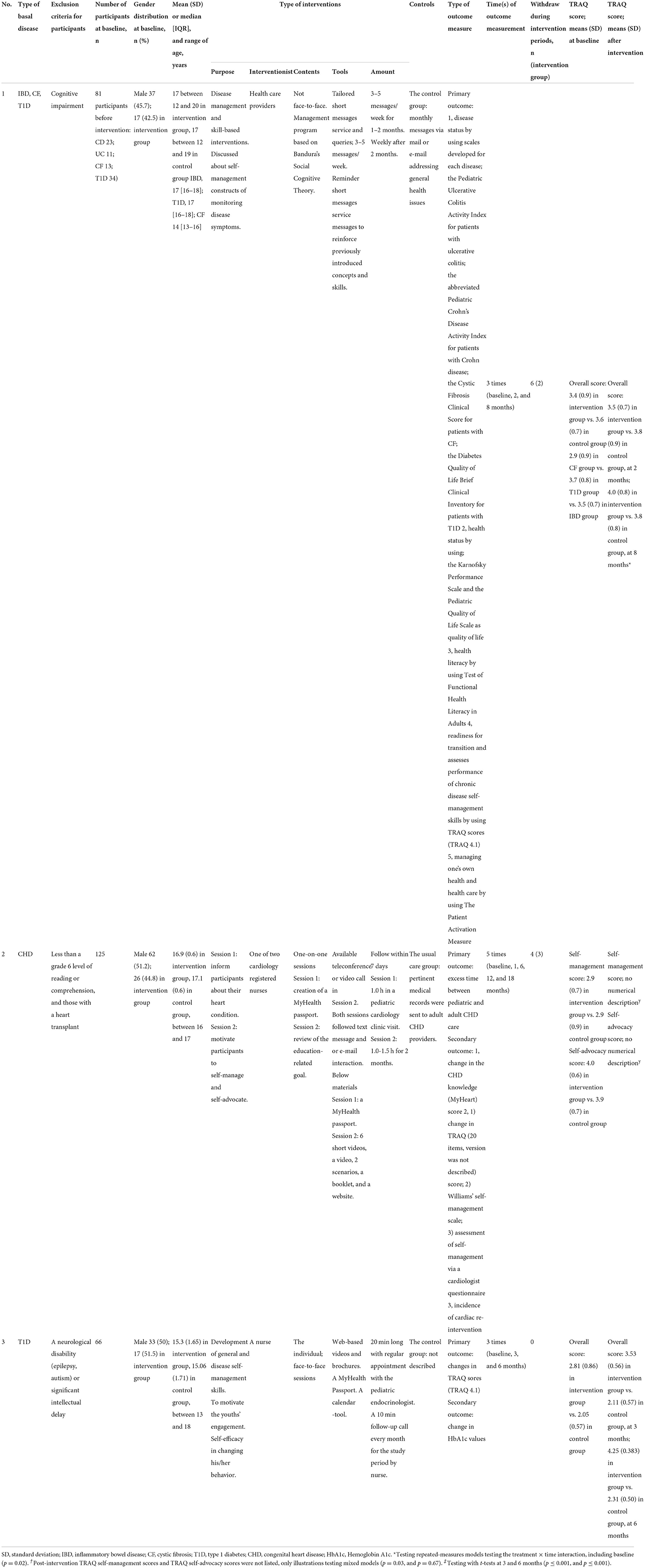
Table 2. Characteristics of study patients, interventions, and outcome.
The target diseases were type-1 diabetes in two studies, congenital heart disease in one study, cystic fibrosis in one study, and inflammatory bowel disease in one study. All the studies excluded intellectual disability. The subjects ranged in age from 12 to 20 years, with the mean or median age in each study ranging from 15 to 17 years.
In one study (24), the health care provider provided web-based and mobile phone-text-delivered disease management and skill-based interventions. The intervention was an 8-month technology-based disease management program based on Bandura's Social Cognitive Theory.
In the second study (22), nurses provided two nurse-led face-to-face sessions. The sessions comprised individualized 60-min educational sessions: Session 1 was created using the MyHealth Passport app (26). Session 2 reviewed the education-related goals including discussion, role-play, and reviews, with the same materials [short videos, video, scenarios, booklet (27), and website (28)], followed by a text message or e-mail interaction within 7 days.
In the third study (23), a nurse provided two face-to-face structured motivational interviews based on training manuals (29, 30). The sessions were conducted as 20-min face-to-face sessions and 10-min follow-up calls every month.
Contents of interventions were provided by digital resources in two studies. The length of the interventions ranged from 6 to 18 months in all studies.
Usual care was provided in the control groups in two studies; however, the remaining study did not describe the process followed.
The number of outcome types was five, five, and two in each study, respectively. All the outcomes were employed as a means to assess the TRAQ. The outcomes included disease status in all the studies. The outcomes of the two studies included health literacy or disease knowledge, which are not included in the TRAQ. All the interventions were efficacious at 6, 8, and 18 months, except for the self-advocacy score as evaluated by the TRAQ scores.
The mean TRAQ score at baseline was around 2.9 points, ranging from 2.05 to 3.7 in all three studies (22–24). Each chronic disease was shown in the same study (24), with a mean TRAQ score (SD) of 3.7 (0.8) points for patients with type-1 diabetes, 3.5 (0.7) points for patients with inflammatory bowel disease, and 2.9 (0.9) points for patients with cystic fibrosis.
The intervention in the overall TRAQ score showed a 0.6-point increase in the mean of the intervention group compared with a 0.2-point increase for the control group during 8 months for patients with inflammatory bowel disease, cystic fibrosis, and type-1 diabetes (24).
The intervention in the TRAQ self-management score did not have a numerical description but showed a significant increase in the graphic figure during 18 months among patients with congenital heart disease (23). The usual care in the TRAQ self-management score for patients with congenital heart disease did not have a numerical description but showed a significant increase in the graphic figure during 12 months; however, it did not show a significant increase in the graphic figure at 18 months (23). Neither the intervention nor usual care in the TRAQ self-advocacy score for patients with congenital heart diseases have a numerical description and did not show a significant increase in the graphic figure during 18 months (23).
The intervention in the overall TRAQ score showed an increase of 1.44 points in the mean of the intervention group compared with 0.26 points in that of the control group during 6 months among patients with type-1 diabetes (22).
The TRAQ is one of the best assessment tools (5), as it has cross-cultural validity and has thus been translated into many languages (25, 31–35). In our search results, three randomized control trial articles were assessed with the TRAQ. The developer of TRAQ recommends using the mean when it comes to a representative value. However, the authors of the study (24) instructed that acquiring four points or more as a TRAQ summary score can be regarded as starting to acquire the necessary disease management skills.
The target diseases were, of course, chronic illnesses, as the age for starting transition is related to the specific disease. In fact, the mean age in patients with type-1 diabetes was approximately 15 years, and that for patients with congenital heart disease was around 17 years. These differences mean that patients with a younger-onset disease tend to have a later starting transition than patients with an older-onset disease, as patients with a younger-onset disease are not adequately prepared for the transfer to adult care.
Before the discussion of interventions and assessment, we summarize the interventions and assessment, particularly related to the TRAQ for the three studies: In the first study, there was a 2-month intensive web-based and text-delivered disease management and skill-based intervention followed by a 6-month review period, with disease management and self-efficacy assessed with TRAQ (24). In the second, there were nurse-led face-to-face sessions in the intervention, with periods between the end of pediatrics and the beginning of adult medicine as the primary outcome, and change in the congenital heart disease knowledge in the TRAQ as the secondary outcome (22). In the third, 20-min face-to-face sessions were conducted as intervention, with changes in the TRAQ score as the primary outcome, and changes in hemoglobin A1c as the secondary outcome (23).
The intervention tools were applied with digital online devices for intervention staff to communicate with patients in two studies. A nurse was employed for intervention because nurses can work in both pediatrics and adult medicine. They additionally provide medical care for patients with chronic diseases. Nurses can improve the TRAQ scores of patients with nurses' independent support. On the other hand, medical social workers participate in connecting patients with social resources or the local society for transition readiness (2, 36, 37). We could not find a study in which a medical social worker led the intervention, and we hope such a randomized control trial study will be conducted with TRAQ in the future.
Patients with younger-onset disease tended to have lower mean TRAQ scores in the order of highest scores to lowest scores (24). These results indicated that patients with younger-onset diseases tend to have lower scores than patients with older-onset diseases. Sato et al. reported the TRAQ score (SD) for each chronic disease — 4.2 (0.6) points for patients with kidney disease, 3.3 (1.0) points for patients with congenital heart disease (25), and 4.2 (0.5) points for patients with other diseases (mainly rheumatoid disease) — assessed with the Japanese TRAQ. Thus, we should intensively intervene in patients with younger-onset diseases.
The intervention group showed a 0.6-point increase in the mean of the overall TRAQ score compared with the 0.2-point increase for the control group during 8 months among patients with inflammatory bowel disease, cystic fibrosis, and type-1 diabetes (24). The intervention group showed an increase of 1.44 points in the mean intervention group compared with 0.26 points in that of the control group during 8 months among patients with type-1 diabetes (22). After all, the longer the intervention was continued, the more efficacy was shown. In 2015, a Cochrane review reported that intervention made improvements in transition readiness, but it had low evidence (38). However, we collected novel evidence on transition readiness (22, 23).
Parental knowledge and parent-child discussions about transition are associated with higher TRAQ scores (9). Transition readiness requires intelligence. The three studies indicated some role of intelligence in the exclusion criteria. However, the TRAQ is one of the outcomes that assess transition readiness. However, the TRAQ has some limitations in terms of transition readiness. For instance, the TRAQ scores are not associated with appropriate consultation with medical experts for adults (3). Deliberateness would be required to increase appropriate consultations. Besides, while transitional intervention improves knowledge and transition readiness, it is unclear whether it improves the quality of life (39). We recommend the use of general quality of life scales as well as disease-specific scales for condition assessment (40–42). Disease-specified TRAQ can assess a disease-specific issue (43–45). The status or events of the disease can also be used to assess disease-specific issues from the current studies (22, 23). We require multiple assessments in practice (9, 46). Disease-specific evaluation tools are also recommended based on these results (24).
We try to provide patients with an opportunity to communicate with their guardians and health providers for their transition readiness through TRAQ. Such communication gives them an idea of how to deal with their disease.
In conclusion, both face-to-face and web-based interventions were shown to have the potential to improve transition readiness, as assessed by TRAQ. Nurses were considered to be key players in face-to-face interventions. All three studies intervened with the subjects repeatedly, suggesting that continuous support is efficacious.
YS, YI, RO, and TN contributed to the conception of the study. JT substantially contributed to designing, searching databases, and drafting the article. JT, YY, AM, and YI contributed to the review of reports. JT, YY, YS, AM, YI, RO, and TN contributed to the critical revision of the article. All authors read and approved the final manuscript.
JT received a grant for research from Japan Health Academy, the public interest foundation. YI received a grant for research activities from Chugai Pharmaceutical Co., Ltd.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American American Academy of Pediatrics American American Academy of Family Physicians American American College of Physicians-American Society of Internal Medicine. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics. (2002) 110:1304–6. doi: 10.1542/peds.110.S3.1304
2. Got transition. Six core elements of health care transition (2022). Available online at: https://www.gottransition.org/six-core-elements/ (accessed June 27, 2022).
3. Jensen PT, Paul GV, LaCount S, Peng J, Spencer CH, Higgins GC, et al. Assessment of transition readiness in adolescents and young adults with chronic health conditions. Pediatr Rheumatol Online J. (2017) 15:70. doi: 10.1186/s12969-017-0197-6
4. Ferris ME, Harward DH, Bickford K, Layton JB, Ferris MT, Hogan SL, et al. A clinical tool to measure the components of health-care transition from pediatric care to adult care: the UNC TR(x)ANSITION scale. Ren Fail. (2012) 34:744–53. doi: 10.3109/0886022X.2012.678171
5. Sawicki GS, Lukens-Bull K, Yin X, Demars N, Huang IC, Livingood W, et al. Measuring the transition readiness of youth with special healthcare needs: validation of the TRA–Transition Readiness Assessment Questionnaire. J Pediatr Psychol. (2011) 36:160–71. doi: 10.1093/jpepsy/jsp128
6. Wood DL, Sawicki GS, Miller MD, Smotherman C, Lukens-Bull K, Livingood WC, et al. The Transition Readiness Assessment Questionnaire (TRAQ): its factor structure, reliability, and validity. Acad Pediatr. (2014) 14:415–22. doi: 10.1016/j.acap.2014.03.008
7. Zhang LF, Ho JS, Kennedy SE. A systematic review of the psychometric properties of transition readiness assessment tools in adolescents with chronic disease. BMC Pediatr. (2014) 14:4. doi: 10.1186/1471-2431-14-4
8. Carlsen K, Haddad N, Gordon J, Phan BL, Pittman N, Benkov K, et al. Self-efficacy and resilience are useful predictors of transition readiness scores in adolescents with inflammatory bowel diseases. Inflamm Bowel Dis. (2017) 23:341–6. doi: 10.1097/MIB.0000000000001038
9. Stewart KT, Chahal N, Kovacs AH, Manlhiot C, Jelen A, Collins T, et al. Readiness for transition to adult health care for young adolescents with congenital heart disease. Pediatr Cardiol. (2017) 38:778–86. doi: 10.1007/s00246-017-1580-2
10. Pereira Júnior ADC, Castilho ECD, Borges TL, Santos PLD, Carvalho AMP, Miasso AI. An integrative review of non-pharmacological therapeutic interventions in children with mental health problems. Compr Child Adolesc Nurs. (2020) 43:245–59. doi: 10.1080/24694193.2019.1621961
11. Corsello A, Pugliese D, Bracci F, Knafelz D, Papadatou B, Aloi M, et al. Transition of inflammatory bowel disease patients from pediatric to adult care: an observational study on a joint-visits approach. Ital J Pediatr. (2021) 47:18. doi: 10.1186/s13052-021-00977-x
12. Rosen D, Annunziato R, Colombel JF, Dubinsky M, Benkov K. Transition of inflammatory bowel disease care: assessment of transition readiness factors and disease outcomes in a young adult population. Inflamm Bowel Dis. (2016) 22:702–8. doi: 10.1097/MIB.0000000000000633
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Walters K. AMED Allied and complementary medicine (2022). Available online at: https://www.wolterskluwer.com/ja-jp/solutions/ovid/amed-allied-and-complementary-medicine-12 (accessed June 30, 2022).
15. EBISCO. Biosis previews (2022). Available online at: https://www.ebsco.com/products/research-databases/biosis-previews (accessed June 30, 2022).
16. Science Direct. CINAHL (2022). Available online at: https://www.sciencedirect.com/topics/nursing-and-health-professions/cinahl (accessed June 30, 2022).
17. Cochrane Library. Cochrane library (2022). Available online at: https://www.cochranelibrary.com/ (accessed June 30, 2022).
18. Embase. Embase (2022). Available online at: https://www.embase.com/ (accessed June 30, 2022).
19. Ichu-shi Web. Ichu-shi web (in Japanese) (2022). Available online at: https://search.jamas.or.jp/search (accessed June 30, 2022).
20. Proquest. MEDLINE (2022). Available online at: https://www.proquest.com/medline/ (accessed June 30, 2022).
21. Web of Science. Web of science (2022). Available online at: https://www.webofscience.com/wos/woscc/basic-search (accessed June 30, 2022).
22. Mackie AS, Rempel GR, Kovacs AH, Kaufman M, Rankin KN, Jelen A, et al. Transition intervention for adolescents with congenital heart disease. J Am Coll Cardiol. (2018) 71:1768–77. doi: 10.1016/j.jacc.2018.02.043
23. Al Ksir K, Wood DL, Hasni Y, Sahli J, Quinn M, Ghardallou M. Motivational interviewing to improve self-management in youth with type 1 diabetes: a randomized clinical trial transition of care for adolescents from paediatric services to adult health services. J Pediatr Nurs. (2022) 66:e116–e121. doi: 10.1016/j.pedn.2022.05.001
24. Huang S, Terrones L, Tompane T, Dillon L, Pian M, Gottschalk M, et al. Preparing adolescents with chronic disease for transition to adult care: a technology program. Pediatrics. (2014) 133:e1639–46. doi: 10.1542/peds.2013-2830
25. Sato Y, Ochiai R, Ishizaki Y, Nishida T, Miura K, Taki A, et al. Validation of the Japanese transition readiness assessment questionnaire. Pediatr Int. (2020) 62:221–8. doi: 10.1111/ped.14086
26. Kaufman M. MyHealth Passport (2012). Available online at: https://www.sickkids.ca/myhealthpassport (accessed August 23, 2022).
27. Mackie A, Robert C, Rempel G, Magill-Evans J, Heggie P, Buchanan K. When You're 18—A Healthcare Transition Guide for Young Adults (Canadian edition) (2012). Edmonton, Alberta, Canada: University of Alberta, Department of Pediatrics. Available online at: http://fcrc.albertahealthservices.ca/transition/resources/When-You-Are-18.pdf (accessed August 23, 2022).
28. University of Florida. Jacksonville health and transition Services (JaxHATS) (2017). Available online at: http://hscj.ufl.edu/jaxhats/ (accessed August 23, 2022).
29. Rollnick S, Miller WR, Butler C. Motivational interviewing in health care: Helping patients change behavior (2008). Guilford Press. Available online at: https://casaa.unm.edu/mimanuals.html (accessed August 23, 2022).
30. The University of New Mexico. Motivational interviewing and therapist manuals (2022). Available online at: https://casaa.unm.edu/mimanuals.html (accessed August 23, 2022).
31. De Cunto CL, Eymann A, Britos ML, González F, Roizen M, Rodríguez Celin ML, et al. Cross-cultural adaptation of the Transition Readiness Assessment Questionnaire to Argentinian Spanish. Arch Argent Pediatr. (2017) 115:181–7. doi: 10.5546/aap.2017.eng.181
32. Kiziler E, Yildiz D, Eren Fidanci B. Validation of Transition Readiness Assessment Questionnaire in Turkish adolescents with diabetes. Balkan Med J. (2018) 35:93–100.
33. Perica MS, Mayer M, Bukovac LT. Readiness for transition–Croatian version and pilot evaluation of the transition readiness assessment questionnaire (TRAQ) in rheumatologic patients. Ann Rheum Dis. (2019) 78:1349–50. doi: 10.1016/j.jped.2017.12.013
34. Culen C, Herle M, König M, Hemberger SH, Seferagic S, Talaska C, et al. Be on TRAQ-cross-cultural adaptation of the Transition Readiness Assessment Questionnaire (TRAQ 5.0) and pilot testing of the German version (TRAQ-GV-15). J Transit Med. (2019) 1:1. doi: 10.1515/jtm-2018-0005
35. Chapados P, Aramideh J, Lamore K, Dumont É, Lugasi T, Clermont MJ, et al. Getting ready for transition to adult care: tool validation and multi-informant strategy using the Transition Readiness Assessment Questionnaire in pediatrics. Child Care Health Dev. (2021) 47:645–53. doi: 10.1111/cch.12872
36. Andrade DM, Bassett AS, Bercovici E, Borlot F, Bui E, Camfield P, et al. Epilepsy: transition from pediatric to adult care. Recommendations of the Ontario epilepsy implementation task force. Epilepsia. (2017) 58:1502–17. doi: 10.1111/epi.13832
37. Gray WN, Holbrook E, Dykes D, Morgan PJ, Saeed SA, Denson LA. Improving IBD Transition, self-management, and disease Outcomes with an in-clinic transition coordinator. J Pediatr Gastroenterol Nutr. (2019) 69:194–9. doi: 10.1097/MPG.0000000000002350
38. Campbell F, Biggs K, Aldiss SK, Neill PM, Clowes M, McDonagh J, et al. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst Rev. (2016) 29:CD009794. doi: 10.1002/14651858.CD009794.pub2
39. Levy BB, Song JZ, Luong D, Perrier L, Bayley MT, Andrew G, et al. Transitional care interventions for youth with disabilities: a systematic review. Pediatrics. (2020) 146:e20200187. doi: 10.1542/peds.2020-0187
40. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. (1993) 118:622–9. doi: 10.7326/0003-4819-118-8-199304150-00009
41. Queiroz DM, Amorim MH, Zandonade E, Miotto MH. Quality of life of children and adolescents with cancer: revision of studies literature that used the Pediatric Quality of Life Inventory. Invest Educ Enferm. (2015) 33:343–54. doi: 10.17533/udea.iee.v33n2a17
42. Varni JW, Seid M, Kurtin PS. PedsQL 40: reliability and validity of the Pediatric Quality of Life Inventory version 40 generic core scales in healthy and patient populations. Med Care. (2001) 39:800–12.
43. Johnson K, Rocque B, Hopson B, Barnes K, Omoike OE, Wood D. The reliability and validity of a newly developed spina bifida-specific Transition Readiness Assessment Questionnaire: Transition Readiness Assessment Questionnaire-supplement (TRAQ-SB). J Pediatr Rehabil Med. (2019) 12:415–22. doi: 10.3233/PRM-180599
44. Clark SJ, Beimer NJ, Gebremariam A, Fletcher LL, Patel AD, Carbone L, et al. Validation of EpiTRAQ, a transition readiness assessment tool for adolescents and young adults with epilepsy. Epilepsia Open. (2020) 5:487–95. doi: 10.1002/epi4.12427
45. Patel N, Klamer B, Davis S, Nahata L. Patient-parent perceptions of transition readiness in Turner syndrome and associated factors. Clin Endocrinol (Oxf). (2022) 96:155–64. doi: 10.1111/cen.14584
Keywords: adolescent, chronic disease, intervention, randomized controlled trial (RCT), review, transition readiness, questionnaires, young adult
Citation: Takeuchi J, Yanagimoto Y, Sato Y, Ochiai R, Moriichi A, Ishizaki Y and Nakayama T (2022) Efficacious interventions for improving the transition readiness of adolescents and young adult patients with chronic illness: A narrative review of randomized control trials assessed with the transition readiness assessment questionnaire. Front. Pediatr. 10:983367. doi: 10.3389/fped.2022.983367
Received: 30 June 2022; Accepted: 05 September 2022;
Published: 28 September 2022.
Edited by:
Maria Immacolata Spagnuolo, Federico II University Hospital, ItalyReviewed by:
Betsy Hopson, University of Alabama at Birmingham, United StatesCopyright © 2022 Takeuchi, Yanagimoto, Sato, Ochiai, Moriichi, Ishizaki and Nakayama. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuko Ishizaki, aXNoaXpha3lAdGFraWkua211LmFjLmpw
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.