 Laura F. Niño-Serna
Laura F. Niño-Serna Eliana López-Barón
Eliana López-Barón Isabel Cristina Maya Ángel1
Isabel Cristina Maya Ángel1- 1Department of Pediatrics, Hospital Pablo Tobón Uribe, Medellín, Colombia
- 2Pediatric Critical Care Unit, Hospital Pablo Tobón Uribe, Medellín, Colombia
Objective: COVID-19 infections have shown a different behavior in children than in adults. The objective of this study was to describe the clinical characteristics and severity of SARS-CoV-2 infection in pediatric patients seen at a reference hospital in Colombia.
Method: A descriptive, observational study in patients under the age of 18 years with a positive test for SARS-CoV-2 infection (RT-PCR or antigen) between April 2020 and March 2021. Multiple variables were studied, including demographic data, clinical characteristics, lab measurements, treatments administered, intensive care unit admission, and mortality.
Results: A total of 361 patients were included of whom 196 (54%) were males. The median age was 3 years. Of all the patients, 65 (18%) were asymptomatic. The majority of patients had no comorbidities (n = 225, 76%). In those who were symptomatic (n = 296, 82%), the most frequent complaints were fever (n = 178, 60%), nasal congestion (n = 164, 55%) and cough (n = 149, 50%). Chest x-rays were normal in 73 patients (50%). When abnormalities were found, interstitial (29%) and alveolar (12%) patterns were the most prevalent. One hundred and fifty-seven children (53%) required general ward hospitalization, and 24 patients (8%) required pediatric intensive care admission. The global mortality was 0.8% (3 patients).
Conclusions: The majority of cases were asymptomatic or mild. However, a significant percentage of patients required general ward admission, and some even required intensive care. The main symptom of COVID-19 infections in newborns was apnea. A second COVID-19 RT-PCR may be necessary to detect infections in critically ill patients with a high clinical suspicion of the disease if an initial test was negative.
Introduction
In December 2019, an outbreak of severe acute respiratory syndrome coronavirus infection was described in Wuhan, China. As of March 2020, a global pandemic had been declared. A wide array of disease manifestations has been observed, ranging from no symptoms at all to serious respiratory distress and even death. Adults, especially the elderly, have suffered the greatest impact of this disease (1). At the time of writing, the World Health Organization (WHO) had confirmed over 500 million cases worldwide, with almost 6 million deaths attributed directly to COVID-19 infection (2). In Latin America, around 56 million cases and more than 1.2 million deaths have been reported (3). In Colombia, an upper-middle-income country, around 6 million cases and more than 100,000 deaths had been reported as of February 2022 (4). Of all the positive cases in Colombia up to February 2022, 11% were reported in people under the age of 19 (5).
The reported pediatric COVID-19-related deaths have been higher in low and middle-income countries (91.5%) compared to high-income countries (8.5%), with an excess of deaths in Latin America (6). In South America, there are economic, social, and health disparities. Previous studies have shown that certain traits of poor countries have a direct impact on COVID-19 outcomes. This includes low socioeconomic status, overcrowding, higher use of public transportation, absence of potable water, and informal work (7). As a result of the worst scenarios experimented on by infected adults, healthcare services, including pediatric ones, were rearranged to meet the increasing requirements of that age group (8). This came to destabilize vulnerable health systems in which lack of government support, excessive centralization, inequities, and inadequate access were already historical. As a consequence, the pandemic became a major challenge (9).
As the pandemic has progressed, several papers have provided a better understanding of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This includes a glimpse into its pathophysiology, immune response, treatments, as well as the spectrum of manifestations in the pediatric population, in whom the disease has been less severe. Previous studies carried out in countries with limited resources are mainly focused on the characteristics of the multisystem inflammatory syndrome in children (MIS-C) due to its particular specificity for this age group (10–13). Therefore, case series not related to MIS-C are lacking.
The objective of this study was to describe the clinical and imaging characteristics of the infection, the use of specific diagnostic tests and the severity of the SARS-CoV-2 infection in patients admitted to a reference pediatric hospital in Colombia, an upper-middle-income country in Latin America.
Methods
A descriptive, observational study was carried out at a tertiary care hospital in Medellín, Colombia. The Hospital is a high complexity reference center, with 78 pediatric hospital beds and 27 pediatric and neonatal intensive care beds. Around 928 patients per month (11,139 during the study period) were seen in the emergency department and 2,928 were admitted during the study period.
Population
Children under 18 years of age who had a positive test for SARS-CoV-2 [real-time reverse transcription-polymerase chain reaction (RT-PCR) or COVID-19 antigen] and were treated in one of our hospital services: ambulatory care, pediatric emergency room (ER), hospitalization ward, or pediatric intensive care unit (PICU) between April 2020 and March 2021 were included.
COVID-Protocol Attention in the Institution
The institutional protocol for diagnosing SARS-CoV-2 infection was based on RT-PCR. Indications for testing included at least one of the following: respiratory distress, odynophagia, asthenia, anosmia, hypogeusia, runny nose, or fever. If a positive result was available, then no further workup was carried out. In hospitalized patients, if the initial test was negative, then a second RT-PCR test 48–72 h was done. Patients transferred from other institutions were also tested if a previous test was negative; no mattered if was either antigen or RT-PCR. Also, RT-PCR was customary in patients who had surgery or as part of a stem cell transplantation protocol.
Data Collection
The medical charts were reviewed and the data was registered on an Excel form previously designed for this purpose with the following variables: age, sex; clinical variables such as the onset of symptoms, presenting symptoms of the disease, epidemiological contact, comorbidities, area of care (hospital ward, ER, PICU, ambulatory care); complications like multisystem inflammatory syndrome in children (MIS-C), PICU admission, and respiratory failure; lab and diagnostic test results; treatment received during hospitalization (pharmacological treatment, mechanical ventilation, vasopressor support, dialysis); length of hospital and PICU stay; and outcome at discharge: death or recovery.
Statistical Analysis
A descriptive analysis was performed. Qualitative variables are presented as frequencies and proportions. For quantitative variables, normality was assessed using the Shapiro-Wilk test and they are reported as median or mean with interquartile range (IQR) or standard deviation (SD). The data were processed on SPSS version 20 (SPSS Inc. Chicago, IL, USA). The study was approved by the institution's ethics committee and did not require informed consent because of the national statements.
Results
Demographic and Epidemiological Characteristics
A total of 361 patients were included. The median age was 3 years (IQR 1–10 years). Seven patients were newborns (2%). The demographic characteristics of all the patients are reported in Table 1. In Figure 1 we present a flowchart of the included patients.
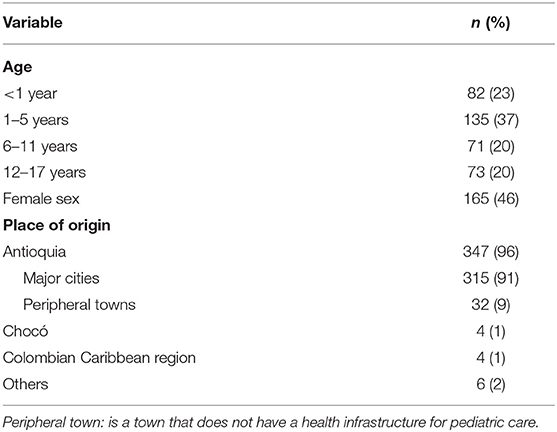
Table 1. Demographic characteristics of all the patients.
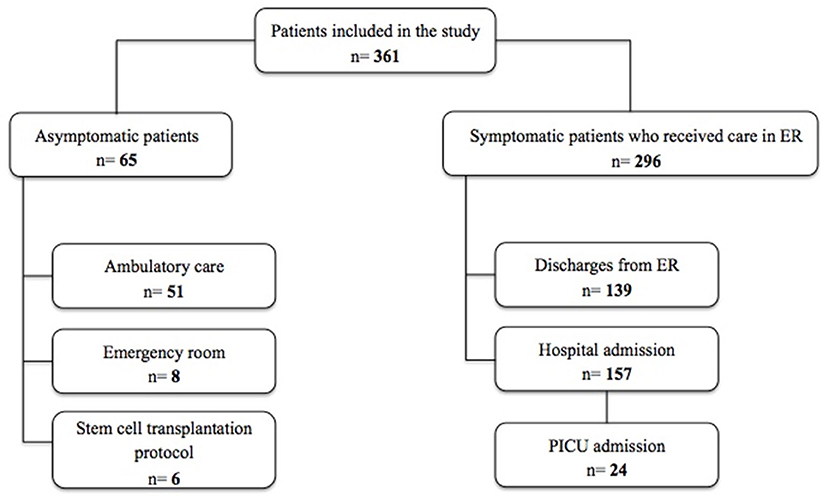
Figure 1. Flowchart of the included patients.
Clinical Characteristics
Out of all the patients, 65 (18%) were asymptomatic. The vast majority were tested because of positive close contact, 51(79%) were outpatients and eight (12%) received attention in the ER. Also, six patients (9%) underwent testing as a part of the stem cell transplantation protocol.
The bulk of the sample, 269 (82%), was composed of symptomatic patients, and all received pediatric medical care. Of these, 157 (53%) patients were hospitalized. Most of the children admitted to ER were 2 years old or younger (n = 159, 52%); the youngest was 7 days old and the oldest was 17 years old. The longest time that elapsed between the onset of symptoms and consultation was 20 days, in one patient. Table 2 shows the characteristics of the symptomatic patients.
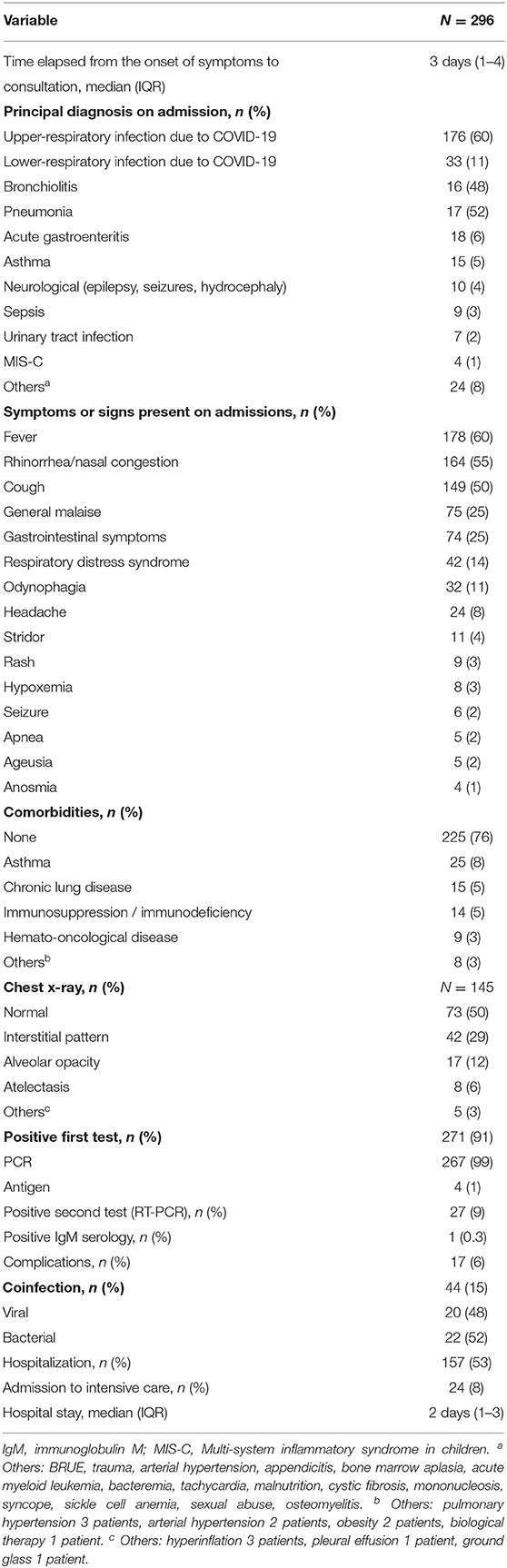
Table 2. Characteristics of patients with COVID-19 symptoms.
The main diagnosis on admission was directly related to SARS-CoV-2 infection in 213 patients (72%) and included: upper-respiratory infection (common cold, pharyngitis, sinusitis, or laryngitis), lower-respiratory infection (bronchiolitis and pneumonia) and MIS-C. In 83 patients (28%) the reason for admission was another non-COVID-related diagnosis and a test was performed as a part of the institutional protocol. The most frequent symptoms were fever in 60%, rhinorrhea in 55%, and cough in 50% of the cases (Table 2). Of all the patients treated, 9 (3%) had MIS-C and were treated with immunoglobulin infusions and high-dose steroids. Another form of presentation was apnea, characteristic of newborns (n = 4/5, 80%). None of these patients had other viruses detected, like respiratory syncytial virus (RSV) or influenza. If asymptomatic cases and those with mild respiratory infections are grouped, they add up to 204 (57%).
SARS-CoV-2 infection was diagnosed with an initial positive test in 271 cases (92%); the remaining 25 patients (8%) required a second RT-PCR test to confirm the diagnosis. Of those initially negative, 23 were RT-PCR and 2 were antigen tests.
Coinfections were detected in 42 patients (14%); 20 children (48%) had an associated viral infection, 9 (45%) due to RSV, 5 (25%) due to influenza; 4 (20%) due to both, RSV and influenza. One patient had cytomegalovirus infection, and another had Epstein-Barr virus. Twenty-two patients (52%) had bacterial coinfections. The isolated microorganisms were E. coli, E. cloacae, P. mirabilis, Staphylococcus aureus, S. epidermidis, Salmonella, S. agalactiae, E. faecalis, Pseudomonas aeruginosa, Clostridium difficile and Candida parapsilosis. Mycoplasma pneumoniae was found in 5 of 28 (18%) patients.
Table 3 describes the results of laboratory tests. A C-reactive protein (CRP) >10 mg/dl was found in 28/169 patients (16%), neutropenia was reported in 30/180 patients (16%) and moderate thrombocytopenia (<100,000) was found in 12 patients (7%).
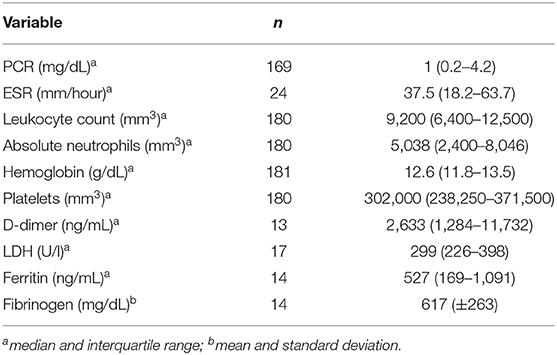
Table 3. Laboratory tests performed on patients with COVID-19 infection.
Two patients (0.5%) were suspected of having healthcare-associated COVID-19 infection after 14 days of hospitalization for a different cause, one for aplastic anemia and another undergoing bone marrow transplantation due to leukemia.
The global mortality for the entire cohort was 0.8% (3 patients). Two patients died of septic shock and multiple organ dysfunction: a healthy 4-year-old with Staphylococcus aureus infection and a newborn with suspected immunodeficiency with Candida parapsilosis infection. The third child, a 5-year-old with cerebral palsy and epileptic encephalopathy, was receiving palliative care and died of respiratory failure. In this case, no other etiological agent other than SARS-CoV-2 was identified.
Intensive Care
Of the 296 symptomatic patients, 24 (8%) were admitted to the PICU or the neonatal care unit with a positive test for COVID-19. Only in six patients (25%), the cause of admission was related to COVID-19. The median length of stay in intensive care was 4 days (IQR 3–6 days). Of the patients that were admitted to the PICU, seven (29%) had a false negative initial test, five RT-PCR tests, and two antigen tests. Table 4 describes the characteristics of the patients admitted to the PICU.
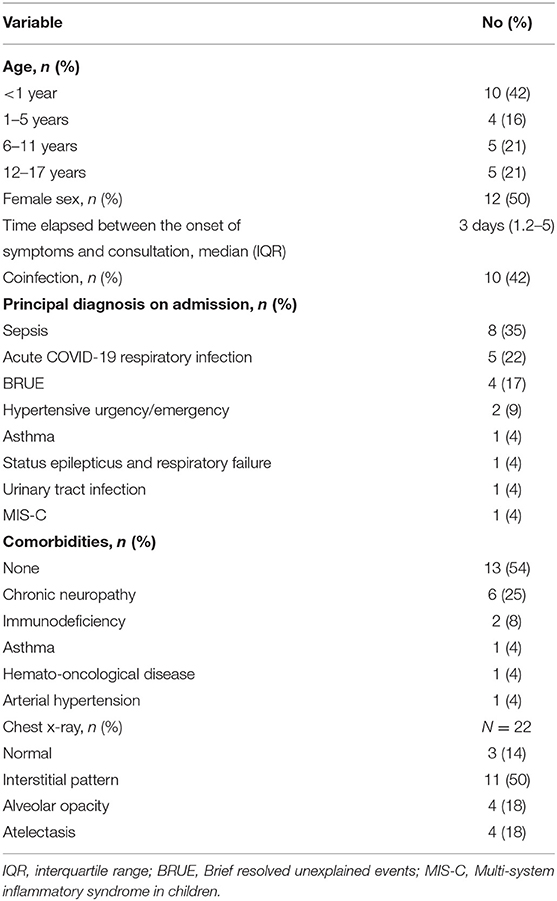
Table 4. Characteristics of patients admitted to the pediatric intensive care unit.
The treatment received in the intensive care unit was as follows: invasive or non-invasive mechanical ventilation in 9 patients (38%), including two patients who required prone positioning, with a median duration of 3 days (IQR 1.5–16 days). Three patients required a high flow cannula. Seven (78%) patients who required mechanical ventilation had bacterial coinfection. Four patients (15%) received vasopressor support, and three patients (11%) received renal replacement therapy. Chest x-rays characteristics of those admitted to the intensive care unit are reported in Table 4.
Discussion
This study describes the demographic, diagnostic, clinical, and imaging characteristics of 361 patients under the age of 18 years diagnosed with SARS-CoV-2 infection at a tertiary care hospital in an upper-middle-income Latin American country. The majority of cases were either symptomatic or mild. We found a highly variable clinical and radiological presentation, perhaps a reflection of the diverse geographical and economical background of the population studied. Additionally, the diagnostic protocol carried out in our institution was successful in detecting false-negative cases, thus possibly preventing in-hospital infections.
The burden placed on health services during the COVID-19 pandemic substantially affected the care of pediatric patients. Given the fact of higher complications and mortality rates, infrastructure and human resources were redirected towards adults' attention. Evidence suggests that children suffered a drop in quality and delays in healthcare access (14). Moreover, as described by Kitano et al. (6) these differences may have been accentuated in low and middle-income countries, which further deepened the gap between nations concerning diagnosis, progression, and follow-up. This disparity is exemplified in mortality rates 35 times higher than those seen in high-income countries (0.43 vs. 0.012). Furthermore, there is an inverse relationship between PICU admissions and income so that access to these units is truncated in countries with limited resources (6).
Latin America is an example of the negative effects that lack of resources and a faulty healthcare structure had on the outcomes of this global emergency. Before the pandemic, most Latin American countries did not have the bare minimum recommended facilities to take care of patients as recommended by the WHO: at least 2.9 hospital beds per 1,000 inhabitants. For instance, Colombia and Peru had 1.6 and Ecuador 1.5. Similarly, only Argentina and Brazil met the essential critical care bed requirement of 6 per 100,000 inhabitants. Moreover, qualified human resources for critically ill patients in Latin America are scarce (9). Therefore, when available means were heavily shifted towards adult care, the already deficient pediatric infrastructure suffered a shortage of hospital and PICU beds. Our institution, aware of the situation caused by the pandemic, had to reduce pediatric critical care beds by 26% and general hospital beds by 22%. In 2020, there was a considerable reduction in pediatric admissions to hospitalization wards and pediatric intensive care units. A phenomenon registered throughout Latin America, mainly evidenced by lower admissions due to lower respiratory tract infections (15).
No less important were the effects of the pandemic on the global health of children and the socioeconomic factors that influence them. In the years 2020-2021 in Colombia, there was a notable decrease in morbidity and mortality due to respiratory diseases. On the other hand, child malnutrition increased significantly after lockdowns were lifted, evidencing low employment rates and high rates of informal work in the region and the country (9, 16). In this series, only 4% of patients lived in peripheral rural areas even if infection rates were similar to those of cities. This is a reflection of the limited access those populations have to the country's health system.
A notable difference from other studies was the prevalence between age groups. While in other studies, the infection was more prevalent in children over 6 years old, in this series we observed more cases in infants under 2 years old (52%). This age distribution could be explained by a selection bias in which parents of younger children seek medical attention in the ER worried about potentially worst outcomes and because the access to ambulatory care is difficult.
Although this study was carried out in a tertiary care center, the occurrence of comorbidities was low and 76% of patients did not have any comorbidity. Data from other studies are inconsistent in this regard. Li et al. (17) results are aligned with our findings whereas others report a greater proportion of comorbidities, for instance, studies from Peru (42%), Argentina (53.9%), and Brazil (38.9%) (18–20).
Every study reviewed, and ours, show that COVID-19 symptoms are similar to and indistinguishable from those of other common viral diseases affecting preschoolers and school-age children and comprise: fever, respiratory and gastrointestinal complaints (18, 19, 21–23). In this series, most patients suffered from acute upper respiratory infection, with a few cases of pneumonia and hypoxemia. Also, of all the patients admitted to the PICU, only 25% had a diagnosis directly related to COVID-19, unlike the clinical presentation in adults (24, 25).
In these series, the majority of patients had mild symptoms or were asymptomatic; just 6% had pneumonia and 5% had bronchiolitis, which explains the lower frequency of hypoxemia at the moment of ER admission. A similar trend was found by Rodriguéz-Portilla et al. (18). For many reasons and hypotheses, the severe COVID-19-pneumonia experienced by adults is very rare in children (26).
The largest Colombian study was carried out by Bolaños-Almeida (27). The records of around fifty thousand patients under 18 years with COVID-19 were reviewed. Hospital admissions only represented around 2.8% of cases, whereas PICU admissions were even lower, with <1% requiring intensive care, similar to another population-based study in Chile, where hospitalization in patients with COVID-19 was 2% (28). These data are not comparable to our results given the type of studies, but they give us a broader picture of the behavior of the disease in the pediatric population. Half of our patients required admission. This high figure could be explained by the nature of our institution and the complexity of our patients, as well as our center's protocols for care and follow-up. Ferraro et al. (19) in a single-center study in Argentina, found even higher admissions rates with a tally of 74.8%.
The performance of the diagnostic tests for COVID-19 infection, either antigen or RT-PCR, seems to be variable. Specifically, sensitivity is greatly influenced by the time elapsed since the onset of symptoms and the nasal swabbing (29). Moreover, significant false-negative rates and discordance between different RT-PCR have been described, although not in children (30, 31). In our case, 8% of tests were initially negative and this was even higher in PICU patients (29%). We believe that this is not negligible because COVID-19 infections are significantly contagious and entail confinements in affected patients. Thus, we hypothesize that a second test may be necessary to rule out or confirm the infection in critically ill patients with high clinical suspicion of COVID-19.
Hospital-acquired COVID-19 infections were rare (0.5%) and at a rate lower than previously estimated. For instance, Hendler et al. (20) found a frequency of 7.9% of nosocomial infections. We strongly believe that our diagnostic strategy contributed to these numbers. Since symptomatic patients were required to have two negative RT-PCRs for COVID-19, 48–72 h apart, for isolation measures to be lifted, the probability of hospital contagions was significantly lowered.
We found that 3% of patients suffered from MIS-C. Similar results have been reported in the series from Australia (1.3%) and Argentina (4.6%). On the other hand, a Peruvian study found higher rates of severe disease with 16.8% affected with MIS-C (18, 19, 32). Compared with other studies, our PICU admission rate (8%) was similar to that described by Ferraro et al. (18–20, 32, 33) (6.8%) and is rather average. PICU admissions figures range from 0.5 up to 28%.
A striking finding was that previously healthy patients were the ones mainly admitted to the PICU, although this has also been described in previous studies (10, 18). Besides, SARS-CoV-2 severe respiratory disease is rare in children when compared to adults and in our cohort was present in only 9 patients, 77% of whom had previous ailments.
A common complaint in neonates was apnea (80%), which prompted admission to the neonatal intensive care unit. These patients did not have a viral co-infection that frequently causes this symptom. This granted a greater risk in this population whit confirmed COVID-19 infection, a finding not described in other series (34). Regarding respiratory coinfection, the study by Wu et al. (35) reported similar germs but in different proportions; Mycoplasma infection being the most frequent in that series and RSV in ours.
Deaths were rare with an estimate of 0.8% and resembled those of most studies (19, 27, 36, 37). Patients with chronic illnesses such as pulmonary disease, immunodeficiencies, congenital heart disease, or neurological disease are more susceptible to death (22, 23, 38). Higher mortality rates have been reported and probably are explained by healthcare access constraints in the studied populations (18, 20).
Positive imaging findings were scarce in our series and general x-rays did not disclose abnormalities, except for patients in the PICU where pathological findings were the norm. Studies that have evaluated radiological variables differ somehow. Investigations carried out in Latin America and Spain found that peribronchial thickening, ground-glass opacities, consolidation, and vascular thickening were frequent (39, 40).
Patients were treated with immunomodulators, steroids and immunoglobulin, when severe infection or MIS-C ensued. In those cases with a diagnosis of asthma exacerbation, steroids were used. There are no other approved treatments for SARS-CoV-2 in Colombia.
An important limitation of this study is that being retrospective, we were sometimes unable to retrieve information for some variables. In addition, the study was conducted at a local and national reference center, which allows for selection bias, especially for critically ill patients.
In summary, this study provides insights into COVID-19 infection in children cared for at a high complexity hospital. By and large, the disease is mostly mild. However, a substantial number of patients required hospital or PICU admission. Therefore, specific arrangements should be implemented in these settings to confront the pandemic.
Finally, we found that, after an initially negative result, a second COVID-19 RT-PCR may be necessary to detect the infection in critically ill patients with a high clinical suspicion of the disease. This strategy may lower the rate of nosocomial infections.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Investigaciones y ética en Investigaciones del Hospital Pablo Tobón Uribe (Research and Research Ethics Committee of Pablo Tobón Uribe Hospital). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
LN-S conceptualized and designed the study, performed the data collection, the statistical analyses, drafted the initial manuscript, and reviewed the final manuscript. CT-M conceptualized and designed the study, performed the data collection, drafted the initial manuscript, and reviewed the final manuscript. IM and EL-B performed the data collection, drafted the initial manuscript, and reviewed the final manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Giraldo-Alzate C, Tamayo-Múnera C, López-Barón E, Caicedo-Baez MC, Piñeres-Olave BE. Síndrome inflamatorio multisistémico en niños asociado a COVID-19. Revisión narrativa de la literatura a propósito de un caso. Acta Colomb Cuid Intensivo. (2020). doi: 10.1016/j.acci.2020.11.002. [Epub ahead of print].
2. >WHO Coronavirus (COVID-19) Dashboard. WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. AVailable online at: https://covid19.who.int/ (accessed February 27, 2022).
3. Epidemic Diseases - Cumulative Suspected and Confirmed COVID-19 Cases Reported By Countries and Territories in the Americas. Available online at: https://ais.paho.org/phip/viz/COVID19Table.asp (accessed May 1, 2022).
4. Colombia: WHO Coronavirus Disease (COVID-19) Dashboard With Vaccination Data. Available online at: https://covid19.who.int/region/amro/country/co (accessed February 27, 2022).
5. Coronavirus Colombia. Available online at: https://www.ins.gov.co/Noticias/paginas/coronavirus.aspx (accessed February 27, 2022).
6. Kitano T, Kitano M, Krueger C, Jamal H, Al Rawahi H, Lee-Krueger R, et al. The differential impact of pediatric COVID-19 between high-income countries and low- and middle-income countries: a systematic review of fatality and ICU admission in children worldwide. PLoS ONE. (2021) 16:e0246326. doi: 10.1371/journal.pone.0246326
7. Hennis AJM, Coates A, Del PS, Ghidinelli M, Gomez Ponce De Leon R, Bolastig E, et al. COVID-19 and inequities in the Americas: lessons learned and implications for essential health services. Rev Panam Salud Publica. (2021) 45:e130. doi: 10.26633/RPSP.2021.130
8. Wasserman E, Toal M, Nellis ME, Traube C, Joyce C, Finkelstein R, et al. Rapid transition of a PICU space and staff to adult coronavirus disease 2019 ICU care. Pediatr Crit Care Med. (2021) 22:50–55. doi: 10.1097/PCC.0000000000002597
9. Schwalb A, Armyra E, Méndez-Aranda M, Ugarte-Gil C. COVID-19 in Latin America and the Caribbean: two years of the pandemic. J Intern Med. (2022). doi: 10.1111/joim.13499. [Epub ahead of print].
10. Antúnez-Montes OY, Escamilla MI, Figueroa-Uribe AF, Arteaga-Menchaca E, Lavariega-Saráchaga M, Salcedo-Lozada P, et al. COVID-19 and multisystem inflammatory syndrome in Latin American children: a multinational study. Pediatr Infect Dis J. (2021) 21:516–28. doi: 10.1101/2020.08.29.20184242
11. Acevedo L, Piñeres-Olave BE, Niño-Serna LF, Vega LM, Gomez IJA, Chacón S, et al. Mortality and clinical characteristics of multisystem inflammatory syndrome in children (MIS-C) associated with covid-19 in critically ill patients: an observational multicenter study (MISCO study). BMC Pediatr. (2021) 21:516. doi: 10.1186/s12887-021-02974-9
12. Lima-Setta F, Magalhães-Barbosa MC de, Rodrigues-Santos G, Figueiredo EA., das N, Jacques M, de L, Zeitel R, de S, et al. Multisystem inflammatory syndrome in children (MIS-C) during SARS-CoV-2 pandemic in Brazil: a multicenter, prospective cohort study. J Pediatr. (2021) 97:354–61. doi: 10.1016/j.jped.2020.10.008
13. Fernández-Sarmiento J, De Souza D, Jabornisky R, Gonzalez GA, Arias López M del P, Palacio G. Paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): a narrative review and the viewpoint of the Latin American society of pediatric intensive care (SLACIP) sepsis committee. BMJ Paediatr open. (2021) 5:e000894. doi: 10.1136/bmjpo-2020-000894
14. Diskin C, Orkin J, Agarwal T, Parmar A, Friedman JN. The secondary consequences of the COVID-19 pandemic in hospital pediatrics. Hosp Pediatr. (2021) 11:208–12. doi: 10.1542/hpeds.2020-002477
15. Vásquez-Hoyos P, Diaz-Rubio F, Monteverde-Fernandez N, Jaramillo-Bustamante JC, Carvajal C, Serra A, et al. Reduced PICU respiratory admissions during COVID-19. Arch Dis Child. (2020) 106:808–11. doi: 10.1136/archdischild-2020-320469
16. Morales GE, Técnico E, Liseth Rojas-Botero M, Ginna E, Saavedra P, Epidemióloga M, et al. FERNANDO RUÍZ GÓMEZ Ministro de Salud y Protección Social.
17. Li B, Zhang S, Zhang R, Chen X, Wang Y, Zhu C. Epidemiological and clinical characteristics of COVID-19 in children: a systematic review and meta-analysis. Front Pediatr. (2020) 8:591132. doi: 10.3389/fped.2020.591132
18. Rodríguez-Portilla R, Llaque-Quiroz P, Guerra-Ríos C, Cieza-Yamunaqué LP, Coila-Paricahua EJ, Baique-Sánchez PM, et al. Características clínicas y epidemiológicas de niños con infección por SARS-CoV-2 internados en un hospital peruano. Rev Peru Med Exp Salud Publica. (2021) 38:261–6. doi: 10.17843/rpmesp.2021.382.6719
19. Ferraro D, Arias AP, Pérez G, Gómez S, Deschutter V, Highton E, et al. Características epidemiológicas según el avance de la pandemia SARS-CoV-2 en un hospital pediátrico de alta complejidad en Argentina: estudio descriptivo. Rev Chil infectología. (2021) 38:506–11. doi: 10.4067/S0716-10182021000400506
20. Hendler JV, Miranda do Lago P, Müller GC, Santana JC, Piva JP, Daudt LE. Risk factors for severe COVID-19 infection in Brazilian children. Brazilian J Infect Dis. (2021) 25:101650. doi: 10.1016/j.bjid.2021.101650
21. Gentile Á, Juárez MDV, Romero Bollón L, Cancellara AD, Pasinovich M, Brizuela M, et al. A multicenter study of confirmed COVID-19 cases: preliminary data on 2690 pediatric patients in Argentina during the first year of the pandemic. Arch Argent Pediatr. (2022) 120:80–8. doi: 10.5546/aap.2022.eng.80
22. Chang TH, Wu JL, Chang LY. Clinical characteristics and diagnostic challenges of pediatric COVID-19: a systematic review and meta-analysis. J Formos Med Assoc. (2020) 119:982–9. doi: 10.1016/j.jfma.2020.04.007
23. Hoang A, Chorath K, Moreira A, Evans M, Burmeister-Morton F, Burmeister F, et al. COVID-19 in 7780 pediatric patients: a systematic review. EClinicalMedicine. (2020) 24:100433. doi: 10.1016/j.eclinm.2020.100433
24. Li J, Huang DQ, Zou B, Yang H, Hui WZ, Rui F, et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J Med Virol. (2021) 93:1449–58. doi: 10.1002/jmv.26424
25. Rahman MM, Bhattacharjee B, Farhana Z, Hamiduzzaman M, Chowdhury MAB, Hossain MS, et al. Age-related risk factors and severity of SARS-CoV-2 infection: a systematic review and meta-analysis. J Prev Med Hyg. (2021) 62:E329–71. doi: 10.15167/2421-4248/jpmh2021.62.2.1946
26. Zimmermann P, Curtis N. Why does the severity of COVID-19 differ with age?: understanding the mechanisms underlying the age gradient in outcome following SARS-CoV-2 infection. Pediatr Infect Dis J. (2022) 41:E36–45. doi: 10.1097/INF.0000000000003413
27. Bolaños-Almeida CE, Espitia Segura OM. Clinical and epidemiologic analysis of COVID-19 children cases in Colombia PEDIACOVID. Pediatr Infect Dis J. (2021) 40:7–11. doi: 10.1097/INF.0000000000002952
28. Descripción Epidemiológica De Niños, Niñas Y Adolescentes con COVID-19. Chile: Minist Salud Subsecr Salud Pública Div Planif Sanit Dep Epidemiol (2020).Available online at: https://www.minsal.cl/wp-content/uploads/2021/04/Informe-epidemiológico-COVID-19-en-niños-niñas-y-adolescentes_SE_9-11_2020-2021.pdf (accessed May 7, 2022).
29. Kevadiya BD, Machhi J, Herskovitz J, Oleynikov MD, Blomberg WR, Bajwa N, et al. Diagnostics for SARS-CoV-2 infections. Nat Mater. (2021) 20:593–605. doi: 10.1038/s41563-020-00906-z
30. Arevalo-Rodriguez I, Buitrago-Garcia D, Simancas-Racines D, Zambrano-Achig P, Del CR, Ciapponi A, et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE. (2020) 15:e20066787. doi: 10.1101/2020.04.16.20066787
31. Reich N, Lowe CF, Puddicombe D, Matic N, Greiner J, Simons J, et al. Repeat virological and serological profiles in hospitalized patients initially tested by nasopharyngeal RT-PCR for SARS-CoV-2. J Med Virol. (2021) 93:6808–12. doi: 10.1002/jmv.27227
32. Wurzel D, McMinn A, Hoq M, Blyth CC, Burgner D, Tosif S, et al. Prospective characterisation of SARS-CoV-2 infections among children presenting to tertiary paediatric hospitals across Australia in 2020: a national cohort study. BMJ Open. (2021) 11:e054510. doi: 10.1136/bmjopen-2021-054510
33. Bailey LC, Razzaghi H, Burrows EK, Bunnell HT, Camacho PEF, Christakis DA, et al. Assessment of 135 794 pediatric patients tested for severe acute respiratory syndrome coronavirus 2 across the United States. JAMA Pediatr. (2021) 175:176–84. doi: 10.1001/jamapediatrics.2020.5052
34. Gale C, Quigley MA, Placzek A, Knight M, Ladhani S, Draper ES, et al. Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: a prospective national cohort study using active surveillance. Lancet Child Adolesc Heal. (2021) 5:113–21. doi: 10.1016/S2352-4642(20)30342-4
35. Wu Q, Xing Y, Shi L, Li W, Gao Y, Pan S, et al. Coinfection and Other Clinical Characteristics of COVID-19 in Children. Pediatrics. (2020) 146:w20200961. doi: 10.1542/peds.2020-0961
36. Fernandes DM, Oliveira CR, Guerguis S, Eisenberg R, Choi J, Kim M, et al. Severe Acute respiratory syndrome coronavirus 2 clinical syndromes and predictors of disease severity in hospitalized children and youth. J Pediatr. (2021) 230:23–31.e10. doi: 10.1016/j.jpeds.2020.11.016
37. Duarte FOM, Gómez JEM, González DJG, Martínez MLM, Martínez HR, Bedoya MR. Enfermedad por coronavirus 2019 (COVID-19) en niños y adolescentes: un estudio multicéntrico. Pediatria. (2021) 54:95–104. doi: 10.14295/rp.v54i3.288
38. Martins MM, Prata-Barbosa A, da Cunha AJLA. Update on SARS-CoV-2 infection in children. Paediatr Int Child Health. (2021) 41:56–64. doi: 10.1080/20469047.2021.1888026
39. Ugas-Charcape CF, Ucar ME, Almanza-Aranda J, Rizo-Patrón E, Lazarte-Rantes C, Caro-Domínguez P, et al. Pulmonary imaging in coronavirus disease 2019 (COVID-19): a series of 140 Latin American children. Pediatr Radiol. (2021) 51:1597–607. doi: 10.1007/s00247-021-05055-2
Keywords: pediatrics, comorbidity, inpatients, pediatric intensive care unit, Latin America, COVID-19
Citation: Niño-Serna LF, López-Barón E, Maya Ángel IC and Tamayo-Múnera C (2022) Clinical Characteristics of Children With SARS-CoV-2 Infection in a Hospital in Latin America. Front. Pediatr. 10:921880. doi: 10.3389/fped.2022.921880
Received: 16 April 2022; Accepted: 16 May 2022;
Published: 09 June 2022.
Edited by:
Anna Camporesi, Ospedale dei Bambini Vittore Buzzi, ItalyReviewed by:
Miguel Rodríguez-Rubio, University Hospital La Paz, SpainFrancisco Abecasis, Centro Hospitalar Lisboa Norte (CHLN), Portugal
Copyright © 2022 Niño-Serna, López-Barón, Maya Ángel and Tamayo-Múnera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura F. Niño-Serna, ZmVybmFuZGEubmlub0B1ZGVhLmVkdS5jbw==