 Francesca Santamaria
Francesca Santamaria Carla Ziello
Carla Ziello Paola Lorello
Paola Lorello Cristina Bouchè
Cristina Bouchè Melissa Borrelli
Melissa Borrelli
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 19 July 2022
Sec. Pediatric Pulmonology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.896865
This article is part of the Research TopicDifficult and Severe Asthma in Children, Volume IIView all 11 articles
Tiotropium bromide is the only long-acting muscarinic antagonist (LAMA) approved for treatment of patients aged ≥6 years old who have symptoms of uncontrolled asthma. Results from several clinical trials have found that once-daily inhaled tiotropium bromide is safe and efficacious in 6- to 17-year-olds with symptomatic asthma despite treatment with inhaled corticosteroids, with or without other medications. There are still few available studies investigating the impact of tiotropium bromide treatment in preschool children with suboptimal control. In this narrative review, we summarize the pharmacological effects of the LAMA tiotropium bromide, provide an overview about current asthma studies at different pediatric ages, and describe future research needs.
Asthma is a multifactorial inflammatory disorder of the airways that in 2019 affected approximately 262 million people and caused 461,000 deaths (1), with estimates that 400 million people will be affected by 2025 (2). Currently, asthma is also the most common chronic non-communicable pediatric disease worldwide (3). Exacerbations due to allergen or respiratory pathogens exposure, or exercise-induced are the main causes of hospitalization among children or adolescents with asthma, and this in turn results in schoolchildren and work-parents’ absenteeism and high direct and indirect health care costs (4).
In recent years, it has been emphasized that for improving health status the overall goal of asthma management is to achieve symptom control rather than assessing patients based on symptom severity (5). Lack of control in asthma includes persistence of clinical symptoms, high number of exacerbations requiring rescue medications, and progressive lung function deterioration. The importance of symptom control in children is underscored by the results of a national survey that found that asthma control fell short on nearly every goal, indicating a lack of effective asthma symptom control in affected children (6). Moreover, a great proportion of patients with even mild symptoms are inadequately controlled and may face severe exacerbations (7).
Reasons for suboptimal control in children and adolescents include incorrect diagnosis of asthma, especially when spirometry cannot be accurately obtained by uncooperating patients or young children; persistent exposure to environmental triggers such as tobacco smoke or allergens; low or non-adherence to treatment and/or poor inhaler techniques, which are frequently described when long-term anti-inflammatory medications are prescribed; personal concerns about potential adverse effects; evidence of comorbidities, for instance gastroesophageal reflux, obesity, rhinitis, and/or recurrent airway infections (8). Therefore, based on all the above observations, physicians dealing with asthma feel the strong need to have alternative therapeutic interventions available for patients with uncontrolled asthma.
Patients with asthma are now recommended to take inhaled corticosteroids (ICS) whenever given short-acting β2-agonists (SABA) as rescue therapy (9). This is supported by the evidence that ICS enhance the expression of β2-adrenergic receptors in the airways, prevent severe exacerbations and maintain symptoms control (10). Indeed, according to the Global Initiative for Asthma (GINA) and National Asthma Education and Prevention Program (NAEPP), low-dose ICS is recommended as the best initial treatment when asthma symptoms are under suboptimal control (9, 11). At GINA Steps 3–4 and at NAEPP Steps 4–5, the ICS/Long-Acting beta-agonists (LABA) combination is recommended and in case of further lack of response add-on alternative options are suggested (9, 11). Finally, patients at any age who have persistent symptoms or experience exacerbations despite good adherence to Step 4 treatment and in whom other controllers have been previously considered, should be referred to a center specialized in the management of severe asthma for treatment optimization, i.e., re-evaluation of diagnosis, modification of ongoing therapy or addition of other medications (9, 11, 12).
According to the most recent definitions from adult and pediatric literature, difficult-to-treat asthma is characterized by symptoms that persist despite ICS–LABA treatment even at high-dose ICS, while severe asthma is asthma that is uncontrolled despite good adherence with high-dose ICS– LABA and management of comorbidities, or that worsens when high-dose treatment is decreased (9, 11).
It is indeed important to identify any modifiable factors to differentiate children with difficult asthma from those with true severe therapy-resistant asthma. Acting early on modifiable factors in children with difficult asthma allows better control of symptoms without further investigations. In the absence of these factors, addressing a correct diagnosis of true therapy-resistant severe asthma avoids diagnostic and therapeutic delays, allowing patients to benefit from the use of new therapies (13).
In the last decades, the use of long-acting muscarinic antagonists (LAMA) including tiotropium bromide, glycopyrronium, and umeclidinium as bronchodilators in the long-term treatment of asthma has progressively increased (14). The LAMA tiotropium bromide has recently been incorporated into the GINA document at Steps 4 and 5 in patients with a history of exacerbations (9). However, GINA experts recommend that, in patients experiencing exacerbations despite low-dose ICS/LABA, the ICS dose should be increased to at least medium dose, or treatment converted to Maintenance and Reliever Therapy (MART) with ICS/formoterol before considering the addition of a LAMA (9). In individuals aged 12 years and older with persistent asthma that is not controlled by ICS therapy alone, the NAEPP Expert Panel recommends adding a LABA rather than a LAMA to an ICS (11). However, if the individual is not using or cannot use LABA therapy, adding a LAMA to an ICS is indicated as an acceptable alternative.
New treatment options for asthma are indeed strongly needed in children or adolescents with asthma, especially those with moderate or severe symptoms (15). In the last decade, several pediatric studies have evaluated the use of tiotropium bromide as an add-on to ICS maintenance therapy, with or without leukotriene receptor antagonist (LTRA) or LABA. This narrative review will summarize the pharmacological effects of the LAMA tiotropium bromide, provide an overview about current asthma studies at different pediatric ages, and describe future research needs.
Acetylcholine is a neurotransmitter which is released from the neurons of the parasympathetic nervous system in several tissues, including the lung. Acetylcholine stimulates smooth muscle contraction and mucus secretion through M1 to M5 muscarinic receptors (16).
Beyond bronchoconstriction, acetylcholine also regulates airway inflammation and remodeling (17).
Anticholinergic agents are antiasthma medications. Initially, most of the literature was focused on the use of the short-acting anticholinergic ipratropium bromide, a medication predominantly used in combination with SABA to treat bronchoconstriction during asthma exacerbations (18). In 1989, the tiotropium bromide (bromide salt) was patented and then approved for medical use in the form of inhalation powder in 2002 as LAMA bronchodilator drug (19).
Tiotropium bromide is a quaternary ammonium derivative, structurally related to ipratropium bromide (Figure 1), but with a significantly higher affinity for muscarinic receptors within the airways. Tiotropium bromide reversibly binds to the M1, M2, and M3 receptors of the airway smooth muscles, and blocks the effects of the acetylcholine released by parasympathetic nerve endings through a competitive and reversible inhibition, with faster dissociation rates from M2 than from M1 or M3 receptors (20). Tiotropium bromide has a maximum effect occurring at 30–60 min, and since the cholinergic transmission is blocked approximately for 35 h, its principal anti-asthmatic property is the long-acting bronchodilation, which allows a once-daily administration.
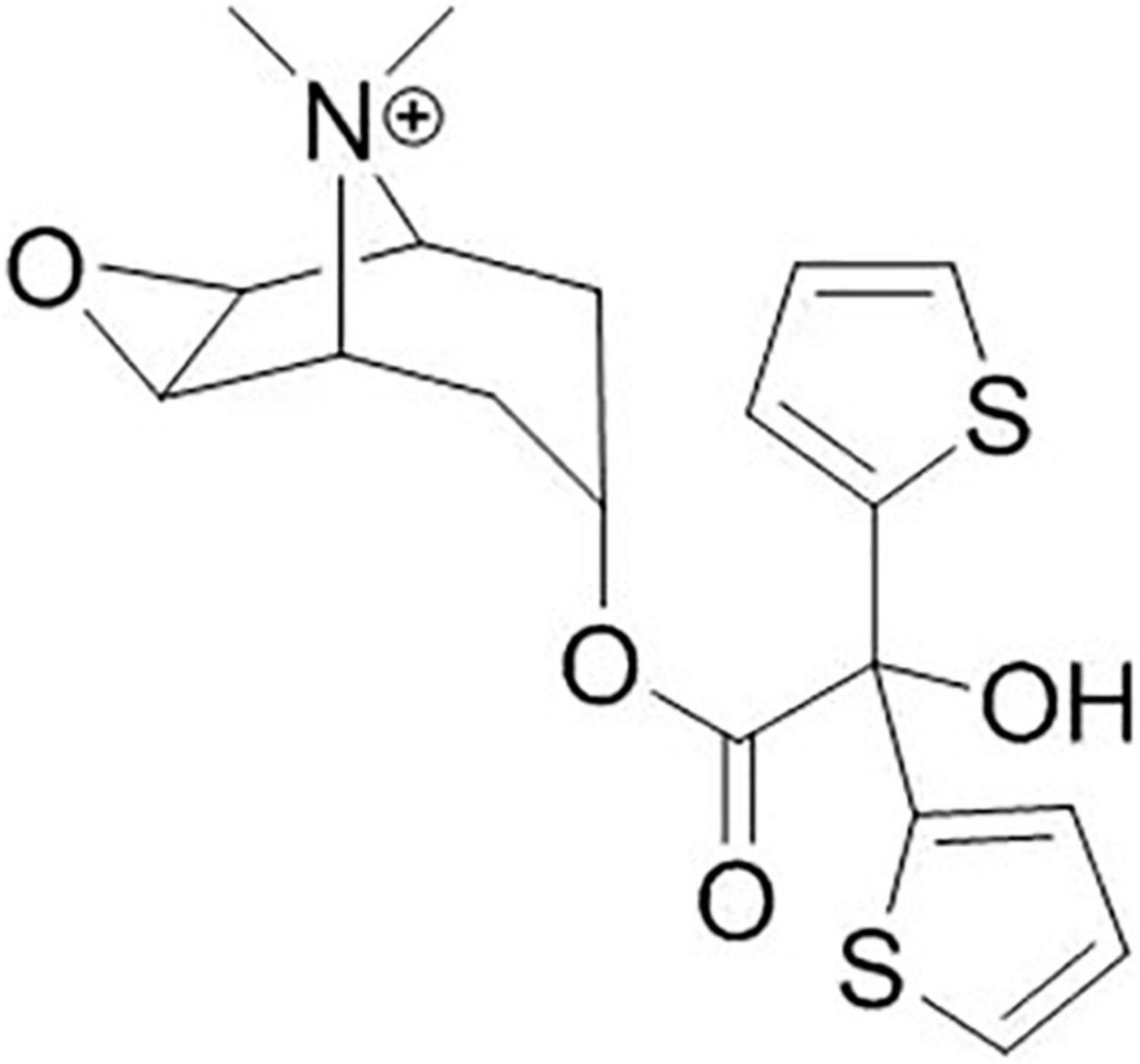
Figure 1. Moulecular structure of tiotropium.
A pharmacokinetic study in children aged 6–11 years old demonstrated that tiotropium bromide is rapidly absorbed following inhalation and then excreted into urine (21), confirming that systemic exposure of children to the medication is within the range observed in adults (22).
Tiotropium bromide is administered through the Respimat© inhaler (19) (Figures 2, 3). Most children aged ≥6 years can use a Respimat© inhaler without a valved spacer device (23) but younger children should use the Respimat in combination with a valved spacer (24, 25).
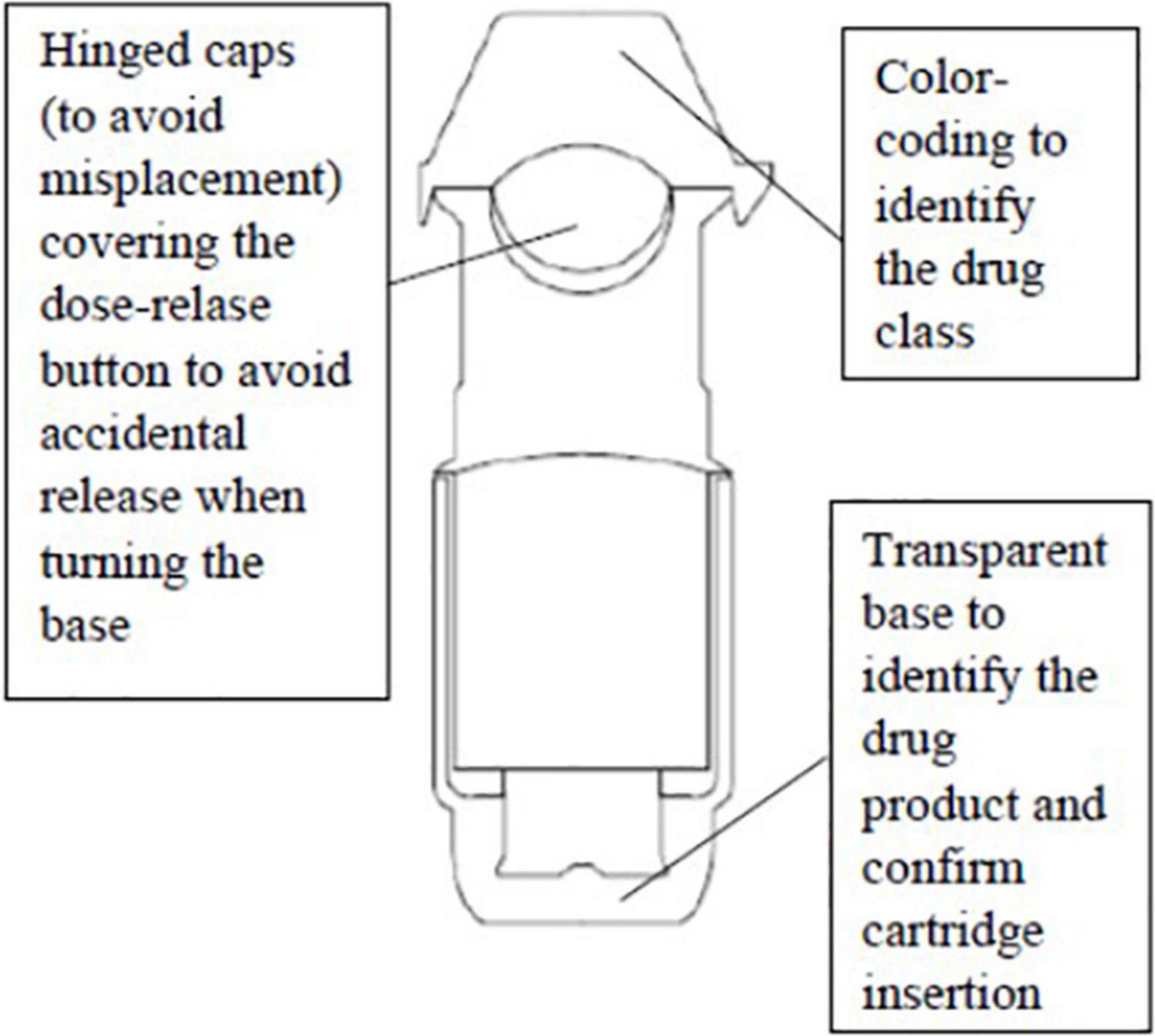
Figure 2. Externarl structure of Respimat© inhaler.

Figure 3. Internal structure of Respimat© inhaler.
Unlike inhaled short acting anticholinergic ipratropium bromide that has been extensively investigated in children or adolescents with acute asthma (26), LAMA has been less studied and pediatric studies regarding the use in chronic asthma only date back to the last 2 decades (Table 1).
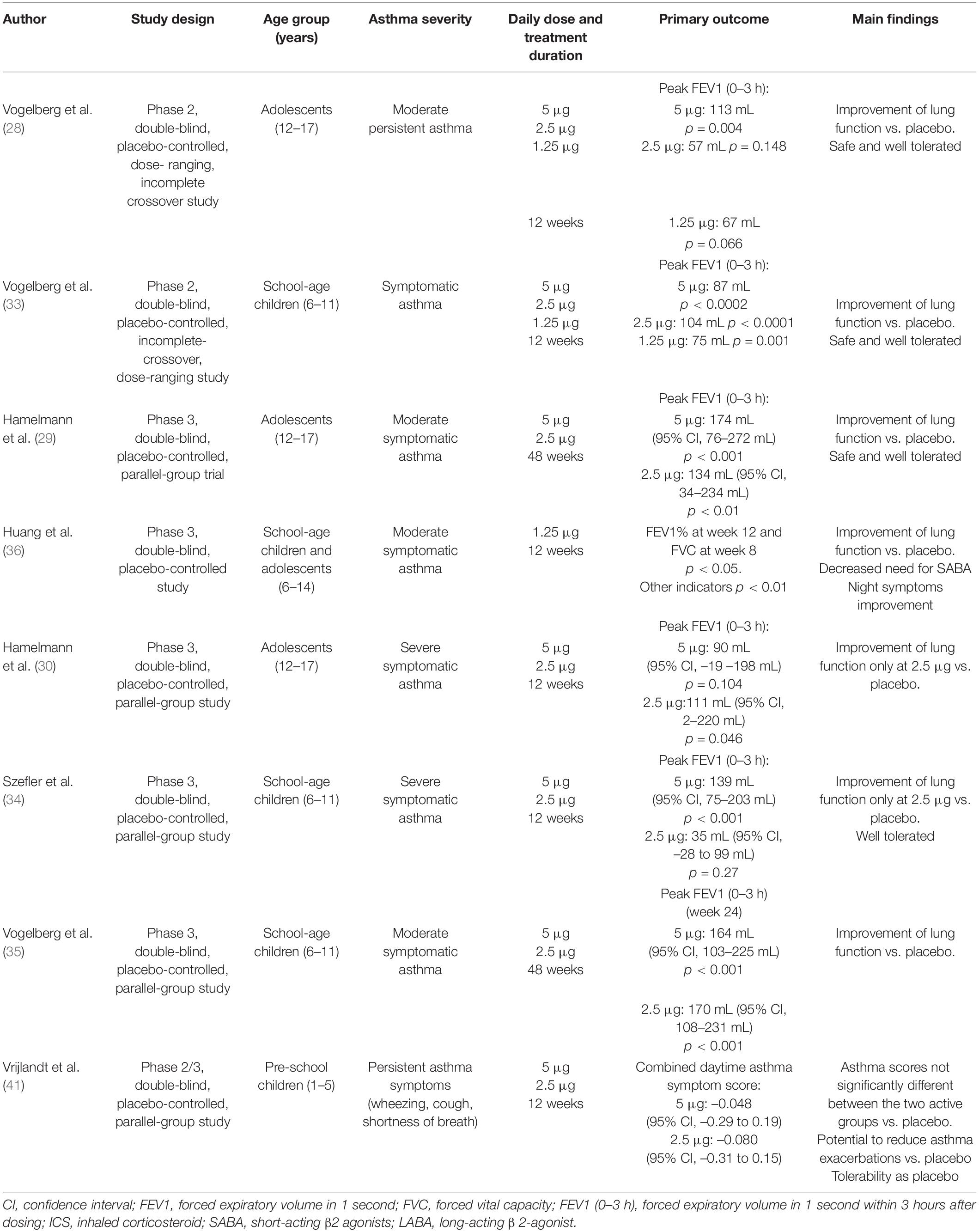
Table 1. Overview of published studies of tiotropium bromide in pediatric patients with asthma.
The effects of tiotropium bromide inhalation in the pediatric population with chronic uncontrolled asthma were first evaluated in adolescents, and results opened the road for assessing tiotropium in younger children. Most of the published studies are randomized controlled trials (RCT) and focus on type and severity of subjective clinical symptoms [evaluated by the asthma standardized questionnaires such as the Asthma Control Questionnaire (ACQ) or Asthma Control Test (ACT)], and lung function (namely, spirometry) as primary outcomes. The lung function end points included the peak expiratory flow (PEF) or the forced expiratory flow at 1 s (FEV1) either reported as peak FEV1 (within 3 h after administration of the study drug) or trough FEV1, i.e., the predose FEV1 measured at the end of the dosing interval, 10 minutes before the next dose of trial medication at week 24 or week 12 (27), or, less frequently, as forced expiratory flow at 25–75% of the lung volume (FEF25–75%). In 2014, Vogelberg conducted an incomplete crossover RCT of 105 adolescents with moderate symptomatic asthma, who were administered once-daily tiotropium (5, 2.5, and 1.25 μg) as an add-on therapy to medium-dose ICS with or without LTRA. Results showed that peak FEV1, trough FEV1 and FEV1 Area Under the Curve (AUC) (0–3 h) significantly improved (28). The term “incomplete” refers to the study design that requires that treatments are grouped into sets or “blocks,” not all of which include every treatment, and each block is administered to a different group of participants to avoid administering too many treatment conditions to the same group of participants.
Results from two additional phase III RCT of once- daily tiotropium administered for 12 or 48 weeks confirmed lung function beneficial effects in adolescents treated with long-term ICS with or without other controller therapies (29, 30). However, only the 5-μg dose significantly improved trough FEV1 at week 24, while in the 48-week RCT asthma control improved using both 5 and 2.5 μg doses of tiotropium, with the 2.5 μg dose also significantly reducing rescue medications use (29). The incidence of adverse effects including asthma worsening or exacerbations, decreased PEF rate, nasopharyngitis, and viral respiratory tract infection was comparable across the treatment groups and did not lead to discontinuation of treatment, as previously reported (31).
In conclusion, tiotropium appears to improve lung function and reduce the need for rescue treatments in adolescents with severe asthma and is well tolerated.
Once demonstrated that tiotropium was to be well tolerated and efficacious in adolescents with uncontrolled asthma, it became urgent to assessing its use for treatment of younger children. There are fewer therapeutic options for school-age children than adolescents and adults, however, this age group shows more unmet medical needs than others. A systematic review on the efficacy and safety of tiotropium as an add-on in children with moderate to severe asthma lasting from >3 to >6 months, uncontrolled despite use of an ICS with or without additional controller medications (32), has included the analysis of 3 RCT of 905 children aged 6–11 years (33–35). Duration of treatment ranged from 12- to 48-weeks. Once-daily tiotropium (5, 2.5, or 1.25 μg) improved lung function parameters, including peak and trough FEV1 or morning and evening PEF (only 5 μg dose) vs. placebo, however there were no statistically significant differences in asthma control and quality of life (33). Huang and coworkers conducted a 12 week-study of eighty children aged 6–14 years, with newly diagnosed moderate persistent asthma who were randomly administered fluticasone propionate aerosol or fluticasone propionate aerosol plus tiotropium via the dry powder HandiHaler® device (36). They showed that lung function significantly improved in both groups at 4, 8, and 12 weeks compared with baseline, in particular in the tiotropium group compared to the control group. Of all clinical variables, no significant difference in the incidence of severe asthma between the two groups (36.3 and 26.8%, respectively) was found, however the proportion of days and frequency of SABA use and awakenings during the night was significantly reduced in children given tiotropium, with no severe adverse effects (36).
In conclusion, in school-aged children, the use of tiotropium appears to improve lung function and, albeit on limited data, reduces the risk of exacerbations and the need for corticosteroid therapy even though a significant difference in the incidence of severe asthma was not documented.
In early life, asthma presentation and clinical course are very different from those described in school-aged children and adolescents due to variable phenotypic heterogeneity and different responses to asthma medications (37). Yet asthma treatment of preschool children is challenging since a high proportion of patients who require frequent health care use because of asthma exacerbations belong to that age group, and this makes prevention of such events a crucial goal for reducing future morbidity (38). However, in young children the response to ICS is sometimes unpredictable because of different airway inflammatory findings (39). Yet not all young children have evidence of eosinophilic airway inflammation, even those with recurrent severe multi-trigger wheeze, and this can justify the poor response to ICS at least in selected cases (40). All the above issues explain why alternative therapeutic options to ICS are warranted in the preschool age group.
In a small exploratory RCT of limited duration (only 12 weeks), tiotropium bromide was administered at 5 and 2.5 μg to 102 children aged 1–5 years with persistent asthma compared to a placebo group (41). The study showed no benefit in the primary outcome measures, i.e., safety, assessed by comparing adverse events between the active and placebo groups, and efficacy, measured as the change in weekly mean combined daytime asthma symptom score from baseline to week 12. Adverse events were less frequent with tiotropium treatment than with placebo, however, no formal statistical comparison between groups was performed by the authors, and more importantly, no significant differences in symptom scores vs. the placebo group were found (41).
A very recent study conducted by Zielen and coworkers in children aged <6 years with uncontrolled severe asthma has showed that adding tiotropium bromide to LABA/ICS significantly improved the systemic corticosteroid prescriptions, the physician’s visits and the antibiotics need recorded 6 months before and after treatment (42). However, the study design, that included the analysis of electronic records, has indeed many limitations, primarily its retrospective nature and the extremely low number of patients enrolled. An ongoing open-label trial of infants and toddlers with recurrent episodes of wheeze and/or shortness of breath is evaluating the effects on episode-free days of a novel strategy of LAMA administration, i.e., as needed intermittent inhaled tiotropium bromide (5 μg once a day, beginning at the onset of an upper respiratory tract infection and continuing for 7–14 days) and as needed SABA vs. intermittent fluticasone propionate and SABA as needed, or solely SABA as needed (NCT03199976). The rationale of the study is that in young children viral-induced wheezing episodes are associated with increased parasympathetic nerve activity, therefore acetylcholine production can be blocked by the inhaled anticholinergic agent tiotropium (43). In conclusion, based on the findings of the scant literature on tiotropium bromide at preschool age, at present there is insufficient evidence to support efficacy of tiotropium use in infants and toddlers with persistent asthmatic symptoms.
Based on the evidence from literature data on asthma (44), indications for administration of tiotropium bromide inhalation spray include the long-term, once-daily, maintenance treatment of moderate-to-severe asthma that is not adequately controlled on ICS. The drug was approved by the US Food and Drug Administration in 2015 in patients with asthma aged ≥12 years, and more recently in February 2017 in pediatric patients aged ≥6 years (18). The approved doses are 2.5 μg in the United States and 5 μg in the European Union (45).
The goal of asthma management is to achieve symptom control and prevent exacerbations by prescribing a therapeutic plan which ensures the greatest clinical benefits and the smallest risk of adverse effects to the patients. Current treatment options for children and adolescents with asthma are progressively growing, and overall, most bronchodilators and anti-inflammatory medications are effective on relevant clinical and lung function outcomes.
Ideally, as low adherence to multiple daily treatments is a big issue in school-aged children and adolescents, providing antiasthma medications once-daily via an easy-to-use inhaler has a beneficial added value.
A major issue that should not be underestimated when antiasthma treatment is prescribed to young children is lack of cooperation in inhaling medications (46). In young children the preferred delivery system of inhaled medications is the pressurized metered-dose inhaler with a valved spacer (with or without a face mask, according to the patient’s age) (9). Future research also including the development of devices designed for different pediatric patients ages and sizes will hopefully improve the standard of care to infants and children with severe wheezing disorders (46).
FEV1 is good indicator to assess the severity of asthma or the efficacy of asthma medications in adult population studies about tiotropium. However, FEV1 may not be the best measure of outcome of pediatric asthma because children spirometry does not always correlate well with symptom severity, especially during asthma exacerbations (47). Thus, since a post-hoc analysis found that improvements in FEF25–75% response with tiotropium vs. placebo were largely more pronounced than improvements in FEV1 (47), measurement of low to medium lung volume flows may be a more sensitive than FEV1 for evaluating peripheral airway response to tiotropium in children and adolescents.
Although studies of tiotropium in children and adolescents overall show improvement of spirometry, the small sample sizes, and short study duration of the trials indicate that the impact of tiotropium should be investigated in longer-term trial cohorts of sufficient size to estimate the maximum clinical effect and the long-term safety (48). Lung function should not be the single endpoint of future studies. Indeed, most of the RCTs demonstrate that spirometry significantly improved, but subjective clinical symptoms evaluated by the asthma questionnaires, or the proportion of exacerbations modestly or not significantly improved (29, 30, 33, 41). Finally, also quality of life should be included as a substantial outcomes measure. In conclusion, pediatric research on tiotropium needs to be indeed directed toward several primary objectives possibly including the identification of predictor response. Future studies should focus on the identification of subgroups of children or adolescents with severe asthma preferentially responsive to LAMA who do not show beneficial effects from treatment with ICS/LABA or high ICS dose. Interestingly, patients with fixed or baseline airflow obstruction might preferentially respond to LAMA, as indicated by two trials in children and adolescents that enrolled asthma patients with FEV1 60–90% predicted (30, 34). In addition to this, other clinical outcome measures, for instance a high proportion of exacerbations or worse asthma control test scores at baseline should be considered in the study design to identify which patients respond better than others to treatment. In the phase III RCT of a large group of children and adolescents, Szefler and coworkers concluded that the effects of tiotropium bromide as an add-on treatment were not influenced by Th 2 phenotype, indicating that the decision of adding tiotropium does not require the evaluation of Th 2 and that tiotropium is effective regardless of allergic status (49). Based on these findings, tiotropium bromide was proposed as alternate option to biologic agents which are recommended to patients aged ≥6 years with severe asthma allergic phenotype (50). Yet biologics are very expensive, therefore, pending further comparative studies of biologics vs. LAMA, tiotropium bromide may also be considered as an appropriate option to biologics in children or adolescents with uncontrolled severe asthma and a confirmed Th 2 phenotype.
Cost-utility of tiotropium bromide in children and adolescents has been rarely discussed. A unique study of children has shown that add-on tiotropium bromide achieves better outcomes at lower cost compared to ICS/LABA therapy (51).
Recently, the glycopyrronium and umeclidinium LAMA combined with LABA and ICS have been studied as add-on triple therapy in adults with asthma that is uncontrolled despite treatment with an ICS/LABA association (13). The single-inhaler ICS/LABA/LAMA regimen is now recommended by GINA before any biologic or systemic steroid treatment is initiated in individuals aged 18 years or older at GINA step 5 (9). There are no published pediatric studies of ICS/LABA/LAMA triple therapy and, given the beneficial effects on pulmonary function in adults (13), whether the regimen is efficacious also in children older than 6 years with uncontrolled asthma should be explored.
An additional point that deserves to be pointed out is the possible effects of tiotropium bromide on airways inflammation and remodeling. As several cells involved in the inflammatory cascade of the asthma process express muscarinic receptors, it has been hypothesized that tiotropium can modulate the function of these cells and attenuate airway inflammation and smooth muscle mass thickening (52). In an animal model of chronic asthma, Kistemaker et al. showed that eosinophilic inflammation in response to allergen exposure and remodeling were reduced by combined administration of tiotropium and ciclesonide (53), suggesting that inhibition of airway inflammation and remodeling may contribute to the long-term beneficial effects of tiotropium (54). An additional mechanism through which anticholinergic drugs may impact on airway diseases is by modulating the asthma-associated mucus overproduction. In a study of mice and mucin production in vitro, Arai et al. showed that tiotropium inhibits neutrophil elastase-induced goblet cell metaplasia, probably by suppressing inflammation and through a direct action on epithelial cells (55). These effects of tiotropium bromide have been poorly investigated in humans and might be the issue of future pediatric studies, also including the comparison vs. the cornerstone anti-inflammatory treatment of asthma with ICS.
Tiotropium bromide is the only LAMA licensed for asthma long-term treatment of patients aged ≥6 years who continue to have symptoms despite controller medication administration. Since the greatest effects of tiotropium bromide on lung function was evaluated in the short-term, whether treatment could affect also the long-term evolution of lung function is unknown. Most relevant changes are reported in spirometry when patients are administered 5 μg rather than other doses. Clinical effects are less significant, probably because most pediatric protocols include a short treatment period and therefore could not appraise the maximum clinical effect of an add-on therapy. An important limitation is also the difference in treatment duration (12 or 48 weeks), which hampers establishment of the long-term effectiveness of the medication.
Treatment with tiotropium bromide as an add-on medication appears to be well tolerated by children and adolescents with suboptimal control of moderate-to-severe asthma, is safe and no fatal events have been reported so far. However, long-term safety should be evaluated in future studies including longer periods of treatment. Since the goal of asthma treatment is to minimize symptom burden and risk of exacerbations, achieving adequate control of asthma symptoms is also imperative for reducing the risk of development of severe asthma. Although the results from the studies of children and adolescents with moderate-to-severe asthma are promising, additional well powered trials are needed to further assess the safety and efficacy of tiotropium bromide added-on to long-term treatment in larger pediatric populations also including preschool children, a population with special needs in whom the novel as needed intermittent administration might be an ideal treatment strategy.
FS and MB made substantial contributions to conception and design, involved in drafting the manuscript, and gave final approval of the version to be published. CZ conceived the idea, involved in drafting the manuscript, and gave final approval of the version to be published. PL made substantial contributions to conception and design, involved in drafting the manuscript and revised it critically for important intellectual content, and gave final approval of the version to be published. CB as graduate in Pharmacy supported all co-authors in the final revision of the manuscript, focusing on the critical aspects of tiotropium use in children and adolescents, and gave approval of the version to be published. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We gratefully thank Phoebe Ashley-Norman who provided medical writing assistance.
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Maciag MC, Phipatanakul W. Prevention of asthma: targets for intervention. Chest. (2020) 158:913–22. doi: 10.1016/j.chest.2020.04.011
3. Asher MI, Rutter CE, Bissell K, Chiang CY, El Sony A, Ellwood E, et al. Global asthma network phase i study group. worldwide trends in the burden of asthma symptoms in school-aged children: global asthma network phase I cross– sectional study. Lancet. (2021) 398:1569–80. doi: 10.1016/S0140-6736(21)01450-1
4. Hasegawa K, Tsugawa Y, Brown DF, Camargo CA Jr. Childhood asthma hospitalizations in the United States, 2000-2009. J Pediatr. (2013) 163:1127.e–33.e. doi: 10.1016/j.jpeds.2013.05.002
5. Chipps BE, Murphy KR, Oppenheimer J. 2020 NAEPP guidelines update and GINA 2021– asthma care differences, overlap, and challenges. J Allergy Clin Immunol Pract. (2022) 10:S19–30. doi: 10.1016/j.jaip.2021.10.032
6. Deschildre A, Pin I, El Abd K, Belmin-Larrar S, El Mourad S, Thumerelle C, et al. Asthma control assessment in a pediatric population: comparison between GINA/NAEPP guidelines, childhood asthma control test (C-ACT), and physician’s rating. Allergy. (2014) 69:784–90. doi: 10.1111/all.12402
7. Dusser D, Montani D, Chanez P, de Blic J, Delacourt C, Deschildre A, et al. Mild asthma: an expert review on epidemiology, clinical characteristics and treatment recommendations. Allergy. (2007) 62:591–604. doi: 10.1111/j.1398-9995.2007.01394.x
8. Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. Eur Respir J. (2008) 31:320–5. doi: 10.1183/09031936.00039707
9. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Fontana-on-Geneva Lake, WI: Global Initiative for Asthma (2022).
10. Sin DD, Man SF. Corticosteroids and adrenoceptor agonists: the compliments for combination therapy in chronic airways diseases. Eur J Pharmacol. (2006) 533:28–35. doi: 10.1016/j.ejphar.2005.12.049
11. Expert Panel Working Group of the National Heart, Lung, and Blood Institute (NHLBI) administered and coordinated National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC), Cloutier MM, Baptist AP, Blake KV, Brooks EG, Bryant-Stephens T, et al. Focused updates to the asthma management guidelines: a report from the national asthma education and prevention program coordinating committee expert panel working group. J Allergy Clin Immunol. (2020) 146:1217–70. doi: 10.1016/j.jaci.2020.10.003
12. Ullmann N, Mirra V, Di Marco A, Pavone M, Porcaro F, Negro V, et al. Asthma: differential diagnosis and comorbidities. Front Pediatr. (2018) 6:276. doi: 10.3389/fped.2018.00276
13. Papi A, Fabbri LM, Kerstjens HAM, Rogliani P, Watz H, Singh D. Inhaled long-acting muscarinic antagonists in asthma – a narrative review. Eur J Intern Med. (2021) 85:14–22. doi: 10.1016/j.ejim.2021.01.027
14. Santamaria F, Borrelli M, Baraldi E. GINA 2021: the missing pieces in the childhood asthma puzzle. Lancet Respir Med. (2021) 9:e98. doi: 10.1016/S2213-2600(21)00275-7
15. Porcaro F, Ullmann N, Allegorico A, Di Marco A, Cutrera R. Difficult and severe asthma in children. Children (Basel). (2020) 7:286. doi: 10.3390/children7120286
16. Cazzola M, Calzetta L, Matera MG. Long-acting muscarinic antagonists and small airways in asthma: which link? Allergy. (2021) 76:1990–2001. doi: 10.1111/all.14766
17. Kistemaker LE, Gosens R. Acetylcholine beyond bronchoconstriction: roles in inflammation and remodeling. Trends Pharmacol Sci. (2015) 36:164–71. doi: 10.1016/j.tips.2014.11.005
18. Rodrigo GJ, Castro-Rodriguez JA. Anticholinergics in the treatment of children and adults with acute asthma: a systematic review with meta-analysis. Thorax. (2005) 60:740–6. doi: 10.1136/thx.2005.040444
19. COL10534AK082021. SPIRIVA RESPIMAT (Tiotropium Bromide) Inhalation Spray, for Oral Inhalation. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc (2016).
20. Barnes PJ. Tiotropium bromide. Expert OpinInvestig Drugs. (2001) 10:733–40. doi: 10.1517/13543784.10.4.733
21. Sharma A, Aalbers R, Hamelmann E, Goldstein S, Engel M, Moroni-Zentgraf P, et al. Pharmacokinetics of tiotropium in asthmatic children aged 6-11 years support its safety profile. Pediatr Allergy Immunol. (2018) 29:773–6. doi: 10.1111/pai.12952
22. Sharma A, Kerstjens HA, Aalbers R, Moroni-Zentgraf P, Weber B, Dahl R. Pharmacokinetics of tiotropium administered by Respimat® in asthma patients. Analysis of pooled data from phase II and III clinical trials. Pulm Pharmacol Ther. (2017) 42:25–32. doi: 10.1016/j.pupt.2016.12.003
23. Von Berg A, Jeena PM, Soemantri PA, Vertruyen A, Schmidt P, Gerken F, et al. Efficacy and safety of ipratropium bromide plus fenoterol inhaled via respimat soft mist inhalervs. A conventional meter ed dose inhaler plus spacer in children with asthma. Pediatr Pulmonol. (2004) 37:264–72. doi: 10.1002/ppul.10428
24. Kamin W, Frank M, Kattenbeck S, Moroni-Zentgraf P, Wachtel H, Zielen S. A handling study to assess use of the Respimat(®)SoftMist™ inhaler in children under 5 years old. J Aerosol Med Pulm Drug Deliv. (2015) 28:372–81. doi: 10.1089/jamp.2014.1159
25. Vogelberg C. Emerging role of long-acting anticholinergics in children with asthma. Curr Opin Pulm Med. (2016) 22:74–9. doi: 10.1097/MCP.0000000000000229
26. Xu H, Tong L, Gao P, Hu Y, Wang H, Chen Z, et al. Combination of ipratropium bromide and salbutamol in children and adolescents with asthma : a meta-analysis. PLoS One. (2021) 16:e0237620. doi: 10.1371/journal.pone.0237620
27. Kerstjens HA, Engel M, Dahl R, Paggiaro P, Beck E, Vandewalker M, et al. Tiotropium in asthma poorly controlled withs tandard combination therapy. N Engl J Med. (2012) 367:1198–207. doi: 10.1056/NEJMoa1208606
28. Vogelberg C, Engel M, Moroni-Zentgraf P, Leonaviciute-Klimantaviciene M, Sigmund R, Downie J, et al. Tiotropium in asthmatic adolescents symptomatic despite inhaled corticosteroids : a randomised dose-ranging study. Respir Med. (2014) 108:1268–76. doi: 10.1016/j.rmed.2014.06.011
29. Hamelmann E, Bateman ED, Vogelberg C, Szefler SJ, Vandewalker M, Moroni Zentgraf P, et al. Tiotropiuma dd-ontherapy in adolescents with moderate asthma: a1-year randomized controlled trial. J Allergy Clin Immunol. (2016) 138:441.e–50.e. doi: 10.1016/j.jaci.2016.01.011
30. Hamelmann E, Bernstein JA, Vandewalker M, Moroni-Zentgraf P, Verri D, Unseld A, et al. A randomised controlled trial of tiotropium in adolescents with severe symptomatic asthma. Eur Respir J. (2017) 49:1601100. doi: 10.1183/13993003.01100-2016
31. Vogelberg C, Engel M, Moroni-Zentgraf P, Leonaviciute-klimantaviciene M, Sigmunf R, Downie J, et al. Tiotropium in asthmatic adolescents symptomatic despite inhaled corticosteroids: a randomised dose-ranging study. Respir Med. (2014) 108:1268.
32. Murphy KR, Chipps BE. Tiotropium in children and adolescents with asthma. Ann Allergy Asthma Immunol. (2020) 124:267.e–76.e. doi: 10.1016/j.anai.2019.11.030
33. Vogelberg C, Moroni-Zentgraf P, Leonaviciute-Klimantaviciene M, Sigmund R, Hamelmann E, Engel M, et al. A randomised dose-ranging study of tiotropium Respimat® in children with symptomatic asthma despite inhaled corticosteroids. Respir Res. (2015) 16:20. doi: 10.1186/s12931-015-0175-9
34. Szefler SJ, Murphy K, Harper T III, Boner A, Laki I, Engel M, et al. A phase III randomized controlled trial of tiotropium add-on therapy in children with severe symptomatic asthma. J Allergy Clin Immunol. (2017) 140:1277–87. doi: 10.1016/j.jaci.2017.01.014
35. Vogelberg C, Engel M, Laki I, Bernstein JA, Schmidt O, El Azzi G, et al. Tiotropium add-on therapy improves lung function in children with symptomatic moderate asthma. J Allergy Clin Immunol Pract. (2018) 6:2160.e–2.e. doi: 10.1016/j.jaip.2018.04.032
36. Huang J, Chen Y, Long Z, Zhou X, Shu J. Clinical efficacy of tiotropium in children with asthma. Pak J Med Sci. (2016) 32:462–5. doi: 10.12669/pjms.322.8836
37. Koefoed HJL, Zwitserloot AM, Vonk JM, Koppelman GH. Asthma, bronchial hyperresponsiveness, allergy and lung function development until early adulthood: a systematic literature review. Pediatr Allergy Immunol. (2021) 32:1238–54. doi: 10.1111/pai.13516
38. Bush A, Pavord ID. Challenging the paradigm: moving from umbrella labels to treatable traits in airway disease. Breathe (Sheff). (2021) 17:210053. doi: 10.1183/20734735.0053-2021
39. Castro-Rodriguez JA, Rodrigo GJ. Efficacy of inhaled corticosteroids in infants and preschoolers with recurrent wheezing and asthma: a systematic review with meta-analysis. Pediatrics. (2009) 123:e519–25. doi: 10.1542/peds.2008-2867
40. Robinson PFM, Fontanella S, Ananth S, Martin Alonso A, Cook J, Kaya-de Vries D, et al. Recurrent severe preschool wheeze: from prespecified diagnostic labels to underlying endotypes. Am J Respir Crit Care Med. (2021) 204:523–35. doi: 10.1164/rccm.202009-3696OC
41. Vrijlandt EJLE, El Azzi G, Vandewalker M, Rupp N, Harper T, Graham L, et al. Safety and efficacy of tiotropium in children aged 1-5 years with persistent asthmatic symptoms: a randomised, double-blind, placebo-controlled trial. Lancet Respir Med. (2018) 6:127–37. doi: 10.1016/S2213-2600(18)30012-2
42. Zielen S, Reichert G, Donath H, Trischler J, Schulze J, Eickmeier O, et al. Tiotropium as an add-on treatment option for severe uncontrolled asthma in preschool patients. J Asthma Allergy. (2021) 14:23–30. doi: 10.2147/JAA.S274544
43. Quizon A, Colin AA, Pelosi U, Rossi GA. Treatment of disorders characterized by reversible airway obstruction in childhood: are anti-cholinergic agents the answer? Curr Pharm Des. (2012) 18:3061–85. doi: 10.2174/1381612811209023061
44. Radovanovic D, Santus P, Blasi F, Mantero M. The evidence on tiotropium bromide in asthma: from the rationale to the bedside. Multidiscip Respir Med. (2017) 12:12. doi: 10.1186/s40248-017-0094-3
45. EMEA-000035-PIP02-09-M02. SPIRIVA RESPIMAT (Tiotropium Bromide) Inhalation Spray, for Oral Inhalation. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc (2022).
46. Rubin BK, Fink JB. The delivery of inhaled medication to the young child. Pediatr Clin North Am. (2003) 50:717–31. doi: 10.1016/s0031-3955(03)00049-x
47. Szefler SJ, Goldstein S, Vogelberg C, Bensch GW, Given J, Jugovic B, et al. Forced expiratory flow (FEF25-75%) as a clinical endpoint in children and adolescents with symptomatic asthma receiving tiotropium: a post hoc analysis. Pulm Ther. (2020) 6:151–8. doi: 10.1007/s41030-020-00117-6
48. Holguin F, Cardet JC, Chung KF, Diver S, Ferreira DS, Fitzpatrick A, et al. Management of evere asthma: a European respiratory Society/American thoracic society guideline. Eur Respir J. (2020) 55:1900588. doi: 10.1183/13993003.00588-2019
49. Szefler SJ, Hoch HE, Tuffli M, Gondalia R, Barrett MA, Van Sickle D, et al. Quantifying beta-agonist utilization: occasions or puffs? J Allergy Clin Immunol Pract. (2019) 7:1088–90. doi: 10.1016/j.jaip.2018.08.037
50. Hamelmann E, Szefler SJ. Efficacy and safety of tiotropium in children and adolescents. Drugs. (2018) 78:327–38. doi: 10.1007/s40265-018-0862-1
51. Buendía JA, Rodriguez-Martinez CE, Sossa-Briceño MP. Cost-utility of tiotropium for children with severe asthma in patients aged 1-5 years. Pediatr Allergy Immunol. (2021) 32:1866–8. doi: 10.1111/pai.13590
52. Matthiesen S, Bahulayan A, Holz O, Racké K. MAPK pathway mediates muscarinic receptor-induced human lung fibroblast proliferation. Life Sci. (2007) 80:2259–62. doi: 10.1016/j.lfs.2007.02.027)
53. Kistemaker LE, BosI S, Menzen MH, Maarsingh H, Meurs H, Gosens R. Combination therapy of tiotropium and ciclesonide attenuates airway inflammation and remodeling in a guinea pig model of chronic asthma. Respir Res. (2016) 17:13. doi: 10.1186/s12931-016-0327-6
54. Kang JY, Rhee CK, Kim JS, Park CK, Kim SJ, Lee SH, et al. Effect of tiotropium bromide on airway remodeling in a chronic asthma model. Ann Allergy Asthma Immunol. (2012) 109:29–35. doi: 10.1016/j.anai.2012.05.005
Keywords: asthma, children, adolescents, preschool children, long-acting anticholinergics, tiotropium bromide
Citation: Santamaria F, Ziello C, Lorello P, Bouchè C and Borrelli M (2022) Update on Long-Acting Anticholinergics in Children and Adolescents With Difficult and Severe Asthma. Front. Pediatr. 10:896865. doi: 10.3389/fped.2022.896865
Received: 15 March 2022; Accepted: 22 June 2022;
Published: 19 July 2022.
Edited by:
Andre Schultz, Perth Children’s Hospital, AustraliaReviewed by:
Louisa Owens, Sydney Children’s Hospital, AustraliaCopyright © 2022 Santamaria, Ziello, Lorello, Bouchè and Borrelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Melissa Borrelli, bWVsaXNzYS5ib3JyZWxsaUB1bmluYS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.