
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 27 April 2022
Sec. Neonatology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.896331
This article is part of the Research Topic Respiratory Support Strategies in the Prevention and Treatment of Bronchopulmonary Dysplasia View all 14 articles
 Alejandro Avila-Alvarez1,2*
Alejandro Avila-Alvarez1,2* Fermín García-Muñoz Rodrigo3
Fermín García-Muñoz Rodrigo3 Gonzalo Solís-García4
Gonzalo Solís-García4 Sonia Pertega-Diaz2,5
Sonia Pertega-Diaz2,5 Manuel Sánchez Luna6
Manuel Sánchez Luna6 Martin Iriondo-Sanz7Dolores Elorza Fernandez8
Martin Iriondo-Sanz7Dolores Elorza Fernandez8 Carlos Zozaya8
Carlos Zozaya8
Introduction: While non-invasive positive-pressure ventilation (NIPPV) is increasingly used as a mode of respiratory support for preterm infants, it remains unclear whether this technique translates into improved respiratory outcomes. We assessed the association between NIPPV use and bronchopulmonary dysplasia (BPD)-free survival in never intubated very preterm infants.
Methods: This multicenter cohort study analyzed data from the Spanish Neonatal Network SEN1500 corresponding to preterm infants born at <32 weeks gestational age and <1,500 g and not intubated during first admission. The exposure of interest was use of NIPPV at any time and the main study outcome was survival without moderate-to-severe BPD. Analyses were performed both by patients and by units. Primary and secondary outcomes were compared using multilevel logistic-regression models. The standardized observed-to-expected (O/E) ratio was calculated to classify units by NIPPV utilization and outcome rates were compared among groups.
Results: Of the 6,735 infants included, 1,776 (26.4%) received NIPPV during admission and 6,441 (95.6%) survived without moderate-to-severe BPD. After adjusting for confounding variables, NIPPV was not associated with survival without moderate-to-severe BPD (OR 0.84; 95%CI 0.62–1.14). A higher incidence of moderate-to-severe BPD-free survival was observed in high- vs. very low-utilization units, but no consistent association was observed between O/E ratio and either primary or secondary outcomes.
Conclusion: NIPPV use did not appear to decisively influence the incidence of survival without moderate-to-severe BPD in patients managed exclusively with non-invasive ventilation.
Avoidance of invasive mechanical ventilation (IMV) is among the highest priorities of modern neonatal care and, globally, infants are managed less-invasively now than decades ago (1, 2). The mainstay of this non-invasive approach is prioritization of initial stabilization with continuous positive airway pressure (CPAP) rather than prophylactic intubation. However, this strategy still fails in a significant proportion of infants and emerging evidence suggests that its incorporation into clinical practice has not significantly improved rates of bronchopulmonary dysplasia (BPD) (2–6).
Efforts to reduce CPAP failure and potentially decrease the incidence of BPD prompted the incorporation of other modes of non-invasive ventilation (NIV). Nasal intermittent positive-pressure ventilation (NIPPV) is a type of NIV that combines intermittent ventilator inflations with CPAP throughout the respiratory cycle. NIPPV can be provided by conventional ventilators or bi-level CPAP devices, and the intermittent inflations may or may not be synchronized with the infant’s spontaneous breathing (7). This technique has become popular in some countries and is widely used with different indications (8–11).
Available evidence suggests that the incidence of respiratory failure and the need for intubation is reduced significantly by NIPPV vs. CPAP when used for primary respiratory support (12–15). Whether this translates into improved in-hospital respiratory outcomes is less clear, since the majority of individual studies and meta-analyses report little or no effect on BPD rates (13, 16). Most studies comparing CPAP and NIPPV include infants who were intubated at some point during neonatal admission (before, after, or in between periods of NIV). Those periods of IMV may have modified the risk of chronic respiratory morbidity. However, in current neonatal medicine many preterm babies are stabilized with NIV and are never intubated, or are only briefly intubated for surfactant administration (1).
The present study investigated the association between the use of NIPPV and BPD-free survival in very preterm infants managed non-invasively. We hypothesized that the use of NIPPV would increase the probability of BPD-free survival.
This multicenter cohort study is a retrospective analysis of data collected prospectively from infants who were born with a birth weight <1,500 g and/or at <32 weeks gestational age (GA), and were admitted to centers of the SEN1500 network. For this study, we selected patients born between 230/7 and 316/7 weeks GA who were managed exclusively with NIV. Outborn patients, infants who died in the delivery room (DR), and those with major congenital anomalies, as well as infants from units with intermittent data input, were excluded from the analysis, as were patients who did not receive any type of respiratory support. The study period was from January 2010 to December 2019.
The exposure of interest was NIPPV (synchronized and non-synchronized, bilevel and ventilator-delivered) at any time during the neonatal intensive care unit (NICU) stay. Infants were classified into two groups: the study group comprised patients who received NIPPV at any time during admission, while the control group consisted of patients managed only with CPAP and/or high flow nasal cannula (HFNC).
The primary outcome was survival without moderate-to-severe BPD until discharge from hospital. Secondary outcomes were survival without BPD, survival, BPD, gastrointestinal perforation, necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA), pneumothorax, intraventricular hemorrhage (IVH), and home oxygen. BPD was defined as the need for supplementary oxygen for at least 28 days and classified as moderate or severe depending on oxygen requirements and ventilator support at 36 weeks postmenstrual age (17, 18).
Data are presented as the mean ± standard deviation or n (%). Basal and demographic characteristics, as well as interventions and predefined outcomes, were compared between the study and control group. For univariate analyses the Student t-test and Mann-Whitney U test were used for continuous variables and the Chi-squared test or Fisher exact test for categorical variables, as appropriate.
The odds ratio (OR) for the primary and secondary outcomes were then compared between groups by two different multilevel logistic-regression models, one adjusted only for GA (model 1) and another adjusted for pre-defined confounding variables: GA, sex, small for GA (SGA), prenatal steroids, multiple gestation, and surfactant (model 2). A multilevel approach, including hospital identifier as a random effect, was considered to account for clustering of patients within hospitals. The adjusted OR with corresponding 95% confidence interval (CI) were calculated.
In addition to the analysis by individual patients, an analysis by units was performed. To this end, unadjusted rates of NIPPV use were calculated per unit (i.e., proportion of patients that received NIPPV at some point). Given that units assist children with different demographic and perinatal characteristics, and clinical management also differs between units, an expected rate of NIPPV utilization was calculated for each hospital by a logistic regression analysis adjusting for confounding variables. The results from this model were used to calculate the probability of receiving NIPPV for each newborn. The expected rate of NIPPV utilization for each hospital was then computed by averaging the predicted probability for each individual newborn within that hospital. Subsequently, for each unit, the standardized observed-to-expected ratio (O/E) was calculated. Ratios >1 indicate higher-than-average use, while ratios <1 indicate hospitals with lower NIPPV use.
NICUs were classified as very low-, low-, medium- or high-utilization units based on the quartiles of the O/E ratio of NIPPV use, and outcome rates were compared among these groups. To further analyze the relationship between the standardized O/E ratio of NIPPV use and the different outcomes, we applied a flexible simple regression approach. Each of the outcomes was considered as the dependent variable, including the O/E ratio as a continuous independent covariate. To avoid the linearity assumption, the ratio was modeled using cubic b-splines with three degrees of freedom. Finally, a multilevel logistic regression model was established, including the quartiles of the O/E ratio of NIPPV use as an independent factor, adjusting for the same pre-defined confounding variables.
P-values < 0.05 were considered statistically significant. Statistical analysis was performed with Stata 13.1 (StataCorp, College Station, TX, United States) and R 4.0 statistical software with the libraries splines and lme4 added.
A total of 26,307 VLBW infants were admitted to participating units during the study period. Of these, 6,735 infants were ultimately included in the analysis after applying exclusion criteria (shown in Figure 1). The mean GA and birthweight of the study sample were 29.6 ± 1.5 weeks and 1,175.8 ± 222.9 g, respectively.
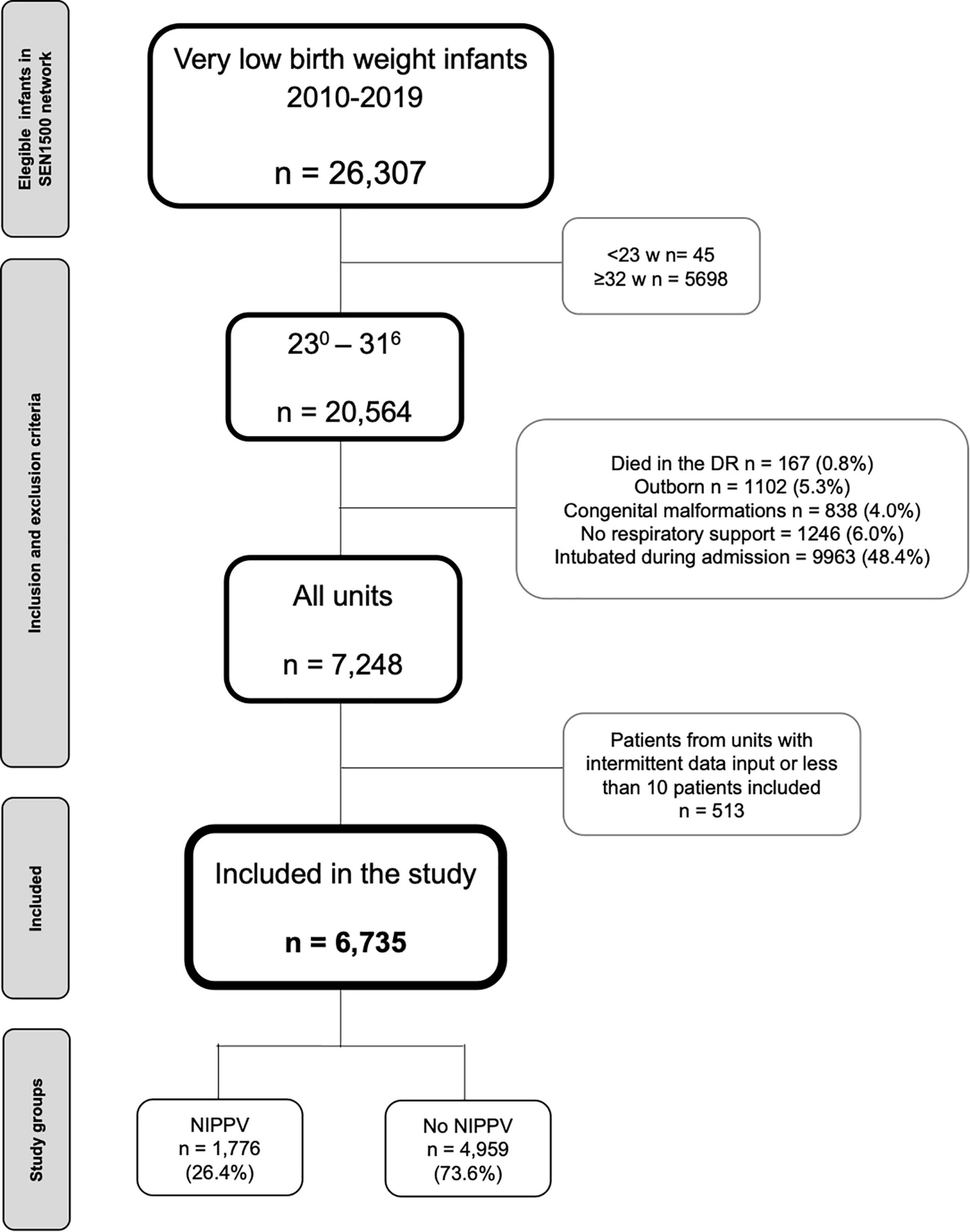
Figure 1. Flow chart depicting the recruitment of the cohort. DR, delivery room; NIPPV, non-invasive positive pressure ventilation.
In total, 1,776 patients (26.4%) received NIPPV during NICU admission and were designated as the NIPPV group. The remaining patients (n = 4,959, 73.6%) were assigned to the control group. Infants in the NIPPV group had a lower GA and birthweight, and more frequently received supplemental oxygen, CPAP, or NIPPV in DR, and surfactant, HFNC, and steroids during admission (Table 1). There were no other significant differences between groups.
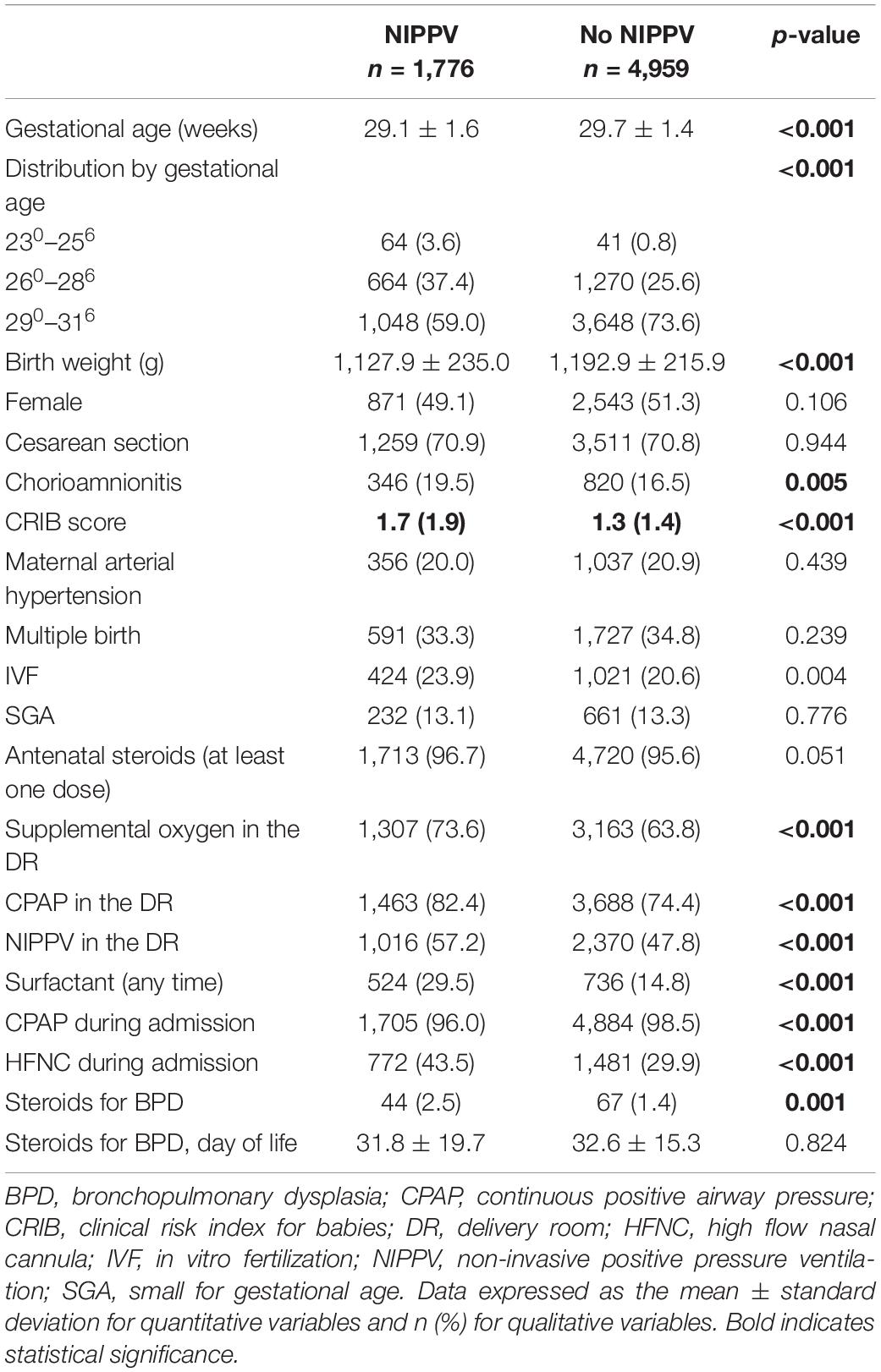
Table 1. Demographic and perinatal characteristics and interventions performed in the delivery room and during the NICU admission in the two study groups.
In the unadjusted analysis the NIPPV group showed a lower frequency of survival without moderate-to-severe BPD (94.5 vs. 96.0%; p < 0.001) and BPD-free survival (81.9 vs. 86.4%; p < 0.001) than the control group. Moreover, the incidence of BPD, moderate-to-severe BPD, severe IVH, medically treated PDA, and domiciliary oxygen were higher in the NIPPV than the control group. No significant differences in other secondary outcomes were observed (Table 2).
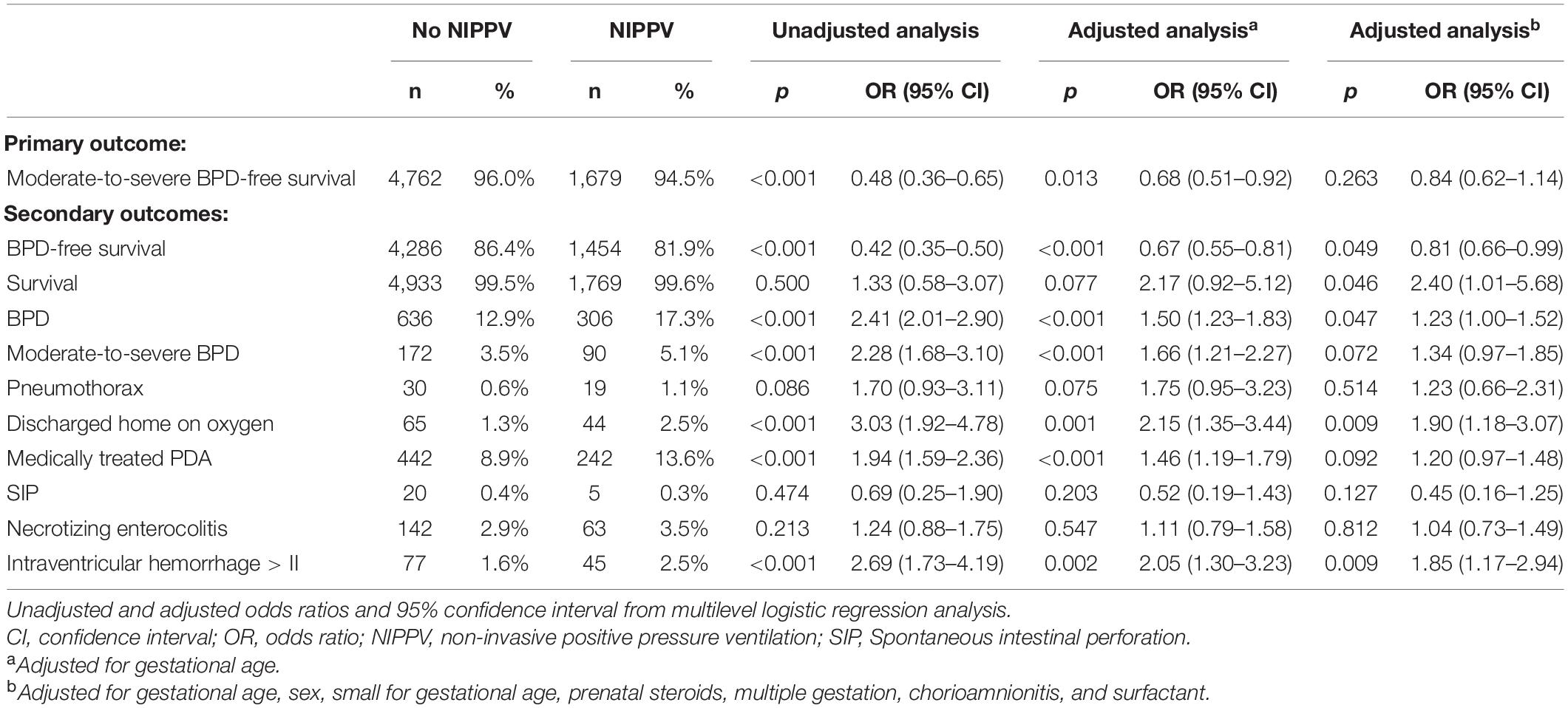
Table 2. Primary and secondary outcomes according to the use of non-invasive positive pressure ventilation (NIPPV).
After adjusting for GA (model 1) survival without moderate-to-severe BPD remained inversely associated with NIPPV use (OR 0.68; 95%CI 0.51–0.92). However, after adjusting for prespecified confounding variables (model 2) this association disappeared (OR 0.84; 95%CI 0.62–1.14). Significant associations persisted for other secondary outcomes, such as BPD-free survival, home oxygen, and severe IVH (Table 2). These results remained unchanged when focusing in the specific population of infants under 30 weeks GA (Supplementary Tables 1, 2).
In the analysis by units, mean observed NIPPV use was 27.7 ± 20.4% (range, 0–89.7%). After applying a logistic regression model and adjusting for potential confounding variables, expected NIPPV rates by unit ranged from 21.8 to 37.9%. Accordingly, the mean O/E ratio was 0.8 ± 0.8 (range, 0–3.5). We observed no significant and consistent association between O/E ratio by units and either primary or secondary outcomes, except for a higher incidence of survival without moderate-to-severe BPD in high-utilization vs. very-low-utilization units (shown in Table 3 and Figure 2).
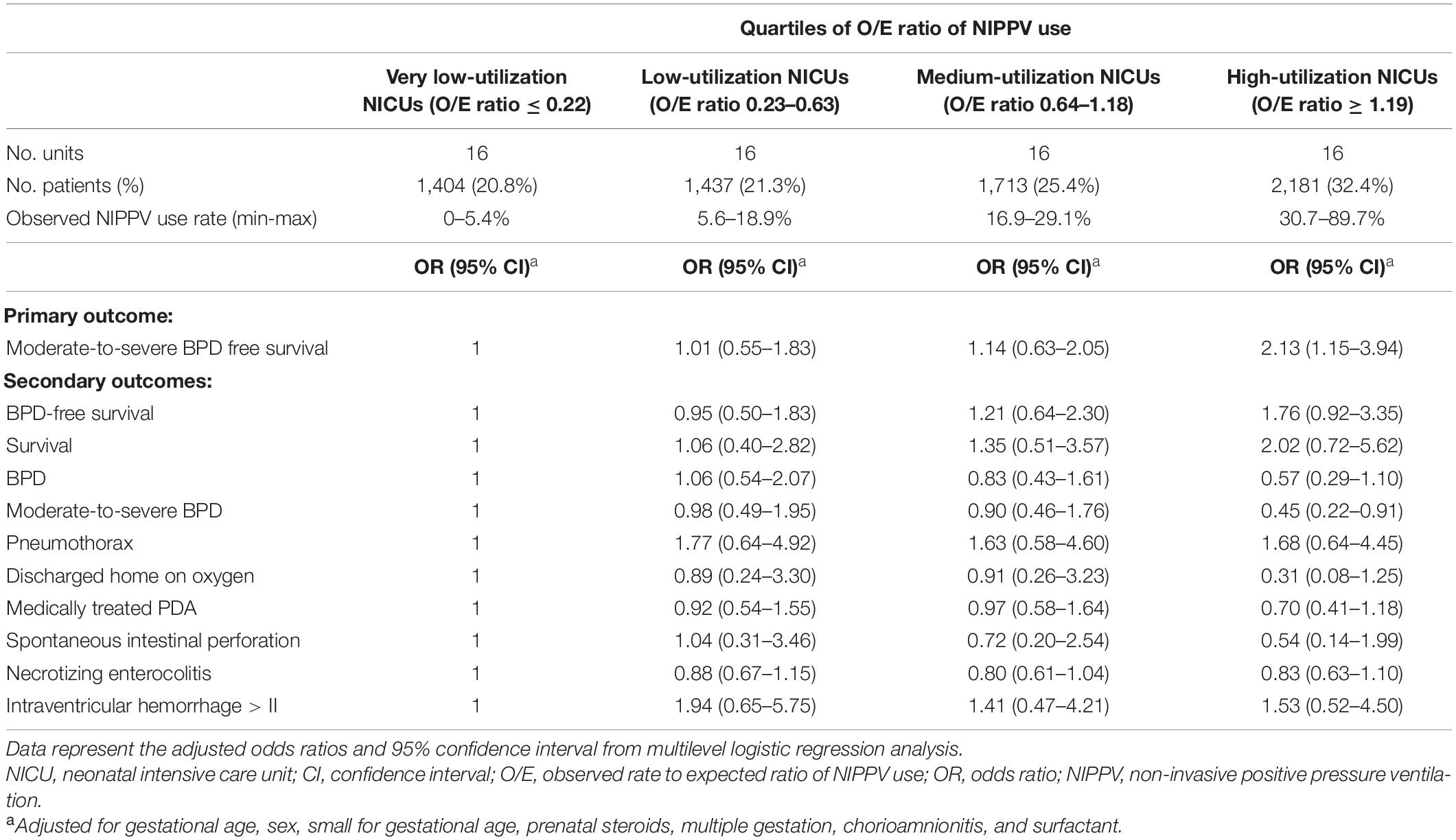
Table 3. Primary and secondary outcomes according to the hospital rate of non-invasive positive pressure ventilation (NIPPV).
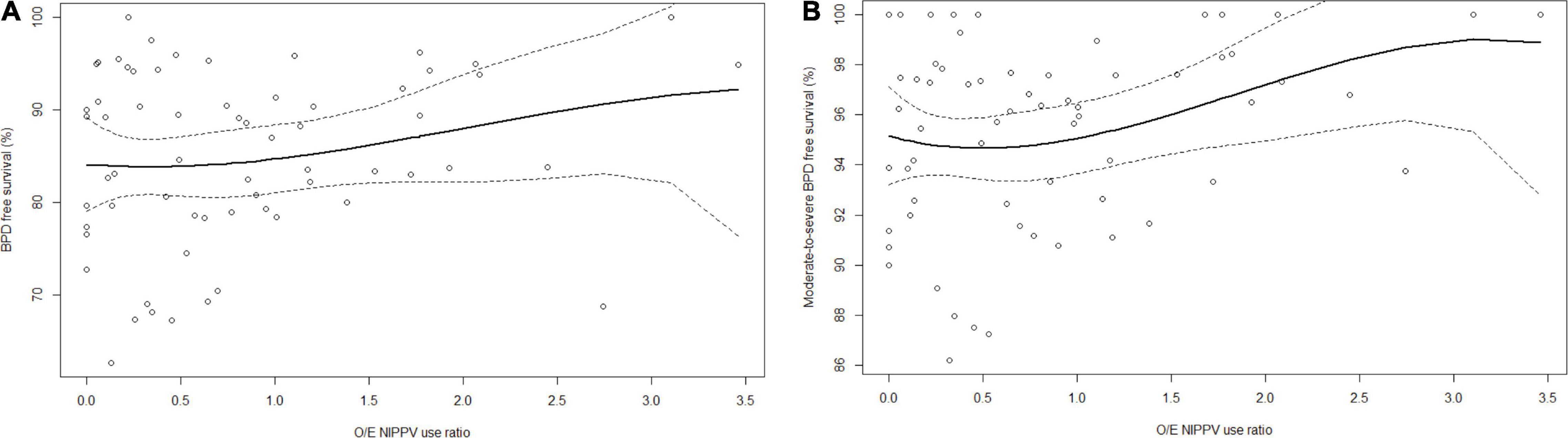
Figure 2. Relationships between O/E ratio of NIPPV use and (A) BPD and (B) survival without moderate-to-severe BPD. Solid line represents fitted flexible regression curve using a cubic b-splines basis with three degrees of freedom. Dashed lines represent 95% confidence intervals.
In this large, retrospective, multicenter, national cohort study we used patient and unit-based approaches to explore the relationship between NIPPV use and BPD among preterm infants that were successfully managed without IMV throughout admission. Our findings show that the use of NIPPV does not appear to decisively improve the probability of survival without BPD.
Non-invasive positive-pressure ventilation is widely used in adults and children with respiratory insufficiency (19, 20). It was first used in neonatology in the 1980s, but the last decade has seen renewed interest in NIPPV in an effort to reduce the frequency of CPAP failure. A survey of practice in 2008 found that NIPPV was used by 44 of 91 (48%) English neonatal units, with considerable variability (11) and we recently reported increasing use of NIPPV in very preterm infants in Spain (3).
Differences in mode and device terminology, as well as study designs, complicate the interpretation of published evidence on the relationship between NIPPV and BPD. The most relevant data come from trials comparing the efficacy of NIPPV vs. the standard of treatment (i.e., CPAP) in heterogeneous preterm infant populations. The largest randomized controlled trial (RCT) was published in 2013 by Kirpalani et al. (21). The authors randomized 1,009 infants <1,000 g and <30 weeks GA to either NIPPV or CPAP whenever NIV was going to be used for the first time. In line with our findings, NIPPV was not associated with a significant reduction in death or BPD.
Since the first trials comparing CPAP and NIPPV and showing promising results (22, 23), some 15 RCTs and several observational studies have specifically evaluated NIPPV as primary respiratory support. While some of these studies reported short-term benefits associated with NIPPV (mainly a reduction in the need for IMV), few differences were observed in the rates of BPD or other relevant outcomes (16, 22–27).
A Cochrane review that included many of the aforementioned RCTs found that, compared with CPAP as a primary mode, NIPPV was associated with a reduced need for intubation, with a relative risk (RR) of 0.78 (95%CI 0.64–0.94) (13), but observed no reduction in BPD risk (RR 0.78, 95%CI 0.58–1.06). As in the present study, that meta-analysis included NIPPV delivered by a ventilator or by bilevel devices, as well as synchronized and non-synchronized modes.
The aforementioned Cochrane review was followed by at least three other meta-analyses. Ekhaguere et al. pooled data from 16 trials and reported findings similar to those of the Cochrane review (14). More recently, a comprehensive network meta-analysis compared the efficacy of four different non-invasive respiratory support modes used as the primary method in preterm infants (12). The authors reported that NIPPV was more effective than CPAP in decreasing the requirement for IMV (RR 0.60; CI 95% 0.44–0.77) and resulted in a slightly lower incidence of BPD or mortality (RR 0.74; CI 95% 0.52–0.98).
The most recent meta-analysis is that of Rüegger et al. which analyzed 18 trials with a total of 1,900 infants, and included data from 8 newly published trials not included in the Cochrane study. Pooled data demonstrated a 37% relative reduction in the risk of respiratory failure and a 28% reduction in BPD at 36 weeks, with no differences in mortality. However, this difference in BPD risk was fully attributable to the studies using ventilator-generating synchronized systems (28).
All these trials included infants that received IMV at some point during their clinical course. Hence, we speculate that the conclusions of those studies may not be generalizable to intubation-naïve infants. To the best of our knowledge, no RCTs have focused specifically on the subset of infants managed only with NIV and never intubated, which constitutes an increasingly common profile in neonatal units (3).
Given the overall uncertainty surrounding published findings on the long-term efficacy of NIPPV, European consensus guidelines stated that there is insufficient evidence to recommend NIPPV as a primary mode of respiratory support for preterm infants (1). Notably, the mechanism of action of NIPPV itself is not yet completely understood and there is little information available to help clinicians optimize NIPPV settings. Some of the benefits seen in adult and children populations (19, 20) may not be replicated in neonatal patients due to anatomical differences, distinct pathophysiological pathways, or the use of different interfaces.
The most likely mechanism accounting for the greater reduction in BPD observed with NIPPV vs. CPAP is avoidance of IMV. However, the pathogenesis of BPD is complex and a single intervention is unlikely to significantly alter its incidence. Our study population did not include patients who failed CPAP and required intubation during admission, and even though we adjusted for the main confounding variables, this may have biased our sample selection by underestimating the BPD rate in the CPAP group. Moreover, infants in the NIPPV group were significantly smaller and probably sicker, which might translate into higher basal risk for BPD. Encouragingly, we observed no significant differences in the incidence of previously reported NIPPV-associated complications, such as gastrointestinal perforation (9). The observed association between NIPPV and both severe intraventricular hemorrhage and domiciliary oxygen in the multivariate analysis are worrisome findings that warrant further study.
The present study has some limitations. The database used did not record data on NIPPV indication, timing, duration, the devices used, synchronization, interfaces, or settings, nor were these parameters standardized in the participating centers. The combination of different devices and techniques in our series could have contributed to the apparent absence of a beneficial effect of NIPPV. However, a previous meta-analysis (13) and a large RCT (21) both used a similarly broad definition of NIPPV technique and indications, an approach that the respective authors considered pragmatic. Limitations inherent to population-based cohorts, such as inaccuracy in some data, cannot be excluded in this analysis. Strengths of our study include the large size of the sample of non-invasively managed infants, its multicenter nature, and the detailed evaluation of multiple clinical outcomes.
In conclusion, in this large, national-based cohort the use of NIPPV appeared not to decisively influence the incidence of survival without moderate-to-severe BPD in patients managed exclusively with NIV. Differences in the basal risk for BPD between groups and the better outcomes in high NIPPV-utilization units may show that NIPPV could in fact be protective. Uncertainty thus remains as to NIPPV efficacy in the context of longer-term outcomes. In our opinion, more data on the indications, settings, and physiological basis for NIPPV are needed before this approach can be considered as standard of treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by A Coruña-Ferrol Research Ethics Committee (Ref 2017/360, first author institution). Primary data collection was approved by the local ethics research committees of the participating centers when they joined the SEN1500 Network. This study protocol has no specific ethical approval as it only gathers anonymized data. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
AA-A developed the research idea. AA-A, FG-MR, and CZ designed the protocol and requested the data. AA-A and SP-D analyzed the data. AA-A wrote the initial draft of the manuscript, which was critically revised by FG-MR, CZ, MSL, SP-D, DE, GS-G, and MI-S. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the hospitals and investigators of the Neonatal Network SEN1500 (Supplementary Material).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.896331/full#supplementary-material
1. Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Te Pas A, et al. European consensus guidelines on the management of respiratory distress syndrome - 2019 update. Neonatology. (2019) 115:432–50. doi: 10.1159/000499361
2. Doyle LW, Carse E, Adams AM, Ranganathan S, Opie G, Cheong JLY. Ventilation in extremely preterm infants and respiratory function at 8 years. N Engl J Med. (2017) 377:329–37. doi: 10.1056/NEJMoa1700827
3. Avila-Alvarez A, Zozaya C, Pértega-Diaz S, Sanchez-Luna M, Iriondo-Sanz M, Elorza MD, et al. Spanish neonatal network SEN1500. temporal trends in respiratory care and bronchopulmonary dysplasia in very preterm infants over a 10-year period in Spain. Arch Dis Child Fetal Neonatal Ed. (2021) 107:143–9. doi: 10.1136/archdischild-2021-322402
4. Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. (2015) 314:1039–51. doi: 10.1001/jama.2015.10244
5. García-Muñoz Rodrigo F, Losada Martínez A, Elorza Fernández MD, Moreno Hernando J, Figueras Aloy J, Vento Torres M. The burden of respiratory disease in very-low-birth-weight infants: changes in perinatal care and outcomes in a decade in Spain. Neonatology. (2017) 112:30–9. doi: 10.1159/000455966
6. Lui K, Lee SK, Kusuda S, Adams M, Vento M, Reichman B, et al. Trends in outcomes for neonates born very preterm and very low birth weight in 11 high-income countries. J Pediatr. (2019) 215:32.e–40.e. doi: 10.1016/j.jpeds.2019.08.020
7. Owen LS, Manley BJ. Nasal intermittent positive pressure ventilation in preterm infants: equipment, evidence, and synchronization. Semin Fetal Neonatal Med. (2016) 21:146–53. doi: 10.1016/j.siny.2016.01.003
8. Ramaswamy VV, Bandyopadhyay T, Nanda D, Bandiya P, More K, Oommen VI, et al. Efficacy of noninvasive respiratory support modes as post extubation respiratory support in preterm neonates: a systematic review and network meta-analysis. Pediatr Pulmonol. (2020) 55:2924–39. doi: 10.1002/ppul.25007
9. Lemyre B, Davis PG, De Paoli AG, Kirpalani H. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane database Syst Rev. (2017) 2:CD003212. doi: 10.1002/14651858.CD003212.pub3
10. Kieran EA, Walsh H, O’Donnell CPF. Survey of nasal continuous positive airways pressure (NCPAP) and nasal intermittent positive pressure ventilation (NIPPV) use in Irish newborn nurseries. Arch Dis Child Fetal Neonatal Ed. (2011) 96:F156. doi: 10.1136/adc.2010.203190
11. Owen LS, Morley CJ, Davis PG. Neonatal nasal intermittent positive pressure ventilation: a survey of practice in England. Arch Dis Child Fetal Neonatal Ed. (2008) 93:F148–50. doi: 10.1136/adc.2007.118109
12. Ramaswamy VV, More K, Roehr CC, Bandiya P, Nangia S. Efficacy of noninvasive respiratory support modes for primary respiratory support in preterm neonates with respiratory distress syndrome: systematic review and network meta-analysis. Pediatr Pulmonol. (2020) 55:2940–63. doi: 10.1002/ppul.25011
13. Lemyre B, Laughon M, Bose C, Davis PG. Early nasal intermittent positive pressure ventilation (NIPPV) versus early nasal continuous positive airway pressure (NCPAP) for preterm infants. Cochrane database Syst Rev. (2016) 12:CD005384. doi: 10.1002/14651858.CD005384.pub2
14. Ekhaguere O, Patel S, Kirpalani H. Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure before and after invasive ventilatory support. Clin Perinatol. (2019) 46:517–36. doi: 10.1016/j.clp.2019.05.004
15. Buyuktiryaki M, Okur N, Sari FN, Ozer Bekmez B, Bezirganoglu H, Cakir U, et al. Comparison of three different noninvasive ventilation strategies as initial respiratory support in very low birth weight infants with respiratory distress syndrome: a retrospective study. Arch Pediatr. (2020) 27:322–7. doi: 10.1016/j.arcped.2020.06.002
16. Oncel MY, Arayici S, Uras N, Alyamac-Dizdar E, Sari FN, Karahan S, et al. Nasal continuous positive airway pressure versus nasal intermittent positive-pressure ventilation within the minimally invasive surfactant therapy approach in preterm infants: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. (2016) 101:F323–8. doi: 10.1136/archdischild-2015-308204
17. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. (2001) 163:1723–9. doi: 10.1164/ajrccm.163.7.2011060
18. Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. National institutes of child health and human development neonatal research network. validation of the national institutes of health consensus definition of bronchopulmonary dysplasia. Pediatrics. (2005) 116:1353–60. doi: 10.1542/peds.2005-0249
19. Bott J, Carroll MP, Conway JH, Keilty SE, Ward EM, Brown AM, et al. Randomised controlled trial of nasal ventilation in acute ventilatory failure due to chronic obstructive airways disease. Lancet (Lond Engl). (1993) 341:1555–7. doi: 10.1016/0140-6736(93)90696-e
20. Fortenberry JD, Del Toro J, Jefferson LS, Evey L, Haase D. Management of pediatric acute hypoxemic respiratory insufficiency with bilevel positive pressure (BiPAP) nasal mask ventilation. Chest. (1995) 108:1059–64. doi: 10.1378/chest.108.4.1059
21. Kirpalani H, Millar D, Lemyre B, Yoder BA, Chiu A, Roberts RS. NIPPV study group. a trial comparing noninvasive ventilation strategies in preterm infants. N Engl J Med. (2013) 369:611–20. doi: 10.1056/NEJMoa1214533
22. Kugelman A, Feferkorn I, Riskin A, Chistyakov I, Kaufman B, Bader D. Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for respiratory distress syndrome: a randomized, controlled, prospective study. J Pediatr. (2007) 150:521–6. doi: 10.1016/j.jpeds.2007.01.032
23. Bisceglia M, Belcastro A, Poerio V, Raimondi F, Mesuraca L, Crugliano C, et al. A comparison of nasal intermittent versus continuous positive pressure delivery for the treatment of moderate respiratory syndrome in preterm infants. Minerva Pediatr. (2007) 59:91–5.
24. Sai Sunil Kishore M, Dutta S, Kumar P. Early nasal intermittent positive pressure ventilation versus continuous positive airway pressure for respiratory distress syndrome. Acta Paediatr. (2009) 98:1412–5. doi: 10.1111/j.1651-2227.2009.01348.x
25. Meneses J, Bhandari V, Alves JG, Herrmann D. Noninvasive ventilation for respiratory distress syndrome: a randomized controlled trial. Pediatrics. (2011) 127:300–7. doi: 10.1542/peds.2010-0922
26. Bhandari V, Finer NN, Ehrenkranz RA, Saha S, Das A, Walsh MC, et al. Eunice kennedy shriver national institute of child health and human development neonatal research network. synchronized nasal intermittent positive-pressure ventilation and neonatal outcomes. Pediatrics. (2009) 124:517–26. doi: 10.1542/peds.2008-1302
27. Salvo V, Lista G, Lupo E, Ricotti A, Zimmermann LJI, Gavilanes AWD, et al. Comparison of three non-invasive ventilation strategies (NSIPPV/BiPAP/NCPAP) for RDS in VLBW infants. J Matern Fetal Neonatal Med. (2018) 31:2832–8. doi: 10.1080/14767058.2017.1357693
Keywords: very preterm infants, bronchopulmonary dysplasia, non-invasive ventilation, preterm outcomes, nasal intermittent positive pressure ventilation
Citation: Avila-Alvarez A, García-Muñoz Rodrigo F, Solís-García G, Pertega-Diaz S, Sánchez Luna M, Iriondo-Sanz M, Elorza Fernandez D and Zozaya C (2022) Nasal Intermittent Positive Pressure Ventilation and Bronchopulmonary Dysplasia Among Very Preterm Infants Never Intubated During the First Neonatal Admission: A Multicenter Cohort Study. Front. Pediatr. 10:896331. doi: 10.3389/fped.2022.896331
Received: 14 March 2022; Accepted: 08 April 2022;
Published: 27 April 2022.
Edited by:
Robin McKinney, Brown University, United StatesReviewed by:
Saadet Arsan, Ankara University, TurkeyCopyright © 2022 Avila-Alvarez, García-Muñoz Rodrigo, Solís-García, Pertega-Diaz, Sánchez Luna, Iriondo-Sanz, Elorza Fernandez and Zozaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandro Avila-Alvarez, YWxlamFuZHJvLmF2aWxhLm5lb25hdG9sb2dpYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.