
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 11 May 2022
Sec. Pediatric Cardiology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.877431
This article is part of the Research TopicPediatric Cardiology and Cardiac Surgery in Developing Countries: Current Needs and Future PerspectivesView all 15 articles
 Patricia Arnaiz1*
Patricia Arnaiz1* Ivan Müller1
Ivan Müller1 Harald Seelig1
Harald Seelig1 Markus Gerber1Jacob Bosma2Danielle Dolley2Larissa Adams2Jan Degen1Stefanie Gall1
Markus Gerber1Jacob Bosma2Danielle Dolley2Larissa Adams2Jan Degen1Stefanie Gall1 Nandi Joubert1,3,4Madeleine Nienaber2Siphesihle Nqweniso2Ann Aerts5Peter Steinmann3,4Rosa du Randt2Cheryl Walter2Jürg Utzinger3,4
Nandi Joubert1,3,4Madeleine Nienaber2Siphesihle Nqweniso2Ann Aerts5Peter Steinmann3,4Rosa du Randt2Cheryl Walter2Jürg Utzinger3,4 Uwe Pühse1
Uwe Pühse1Introduction: Hypertension in children has increased globally over the past 20 years; yet, little is known about this issue among disadvantaged communities from low- and middle-income countries. Age-, sex-, and height-adjusted normative tables are the “gold” standard for the diagnosis and estimation of pediatric hypertension worldwide, but it is unclear whether the use of international standards is appropriate for all contexts. The purpose of this study was to evaluate and compare different international references to identify hypertension among South African school-aged children from disadvantaged communities.
Methods: Blood pressure, weight, and height were measured in a cohort of 897 children aged 8–16 years from eight peri-urban schools in the Eastern Cape of South Africa. Cross-sectional prevalence of hypertension was calculated according to American, German, and global normative tables, as well as pseudo-normative data from the own study population. Isolated systolic hypertension and body mass index (BMI) were considered markers for cardiovascular disease. Multinomial logistic regression was used to compare the likelihood of blood pressure categorization with increasing BMI levels.
Results: Hypertension prevalence ranged from 11.4% with the pseudo-normative study tables to 28.8% based on the German reference. Global guidelines showed the highest agreement both among international standards (92.5% with American guidelines) and with the study reference (72.5%). While the global and the American references presented higher systolic over diastolic hypertension rates (23.6 vs. 10.6% and 24.2 vs. 14.7%, respectively), the American guidelines predicted the highest increased risk for hypertension stage 2 [odds ratio, 1.72 (95% confidence interval: 1.43–2.07)] with raising levels of BMI.
Conclusion: Our results support the heterogeneity of blood pressure estimates found in the South African literature, and highlight the underrepresentation of African children in international guidelines. We call for caution in the use of international standards in different contexts and advocate for the development of normative tables that are representative of the South African pediatric population necessary to ensure an accurate identification of hypertension both from the clinical and epidemiological perspective.
Cardiovascular disease (CVD) is the leading cause of mortality worldwide, accounting for over 17 million deaths yearly (1). Among the most prominent risk factors for CVD is early vascular aging, characterized by arterial stiffness (arteriosclerosis) (2). There is extensive evidence that risk factors for CVD occur early in life, causing premature organ damage that tracks into adulthood (3). In fact, arterial stiffness has been observed and related to hypertension in children (4). Hence, early detection of asymptomatic vascular changes such as elevated blood pressure (BP) is essential for effective intervention and prevention of health consequences in older ages.
However, pediatric hypertension has received little attention, especially in low- and middle-income countries (LMICs). As new research emerges, we are gaining awareness of the extent of a long underappreciated problem and the consequences of its (mis)management, such as impaired development, economic burden, years of life lost, etc. (5). A recent meta-analysis revealed that global hypertension rates among children have increased about 75% over the past 20 years (6), which has been partially attributed to the steep escalation in childhood obesity, an early-life risk factor for CVD. A similar trend for childhood hypertension is expected in African countries, where “the number of overweight children under 5 has increased by nearly 24 percent since 2000” (7). The strong association between body mass index (BMI) and BP in children has been established both globally (8) and in South Africa (9), where their relation with arterial stiffness (10) and the tracking of BP from childhood into late adolescence have been described (11). This emphasizes the need to rely on accurate estimates to monitor childhood hypertension progress and react to long-term health impacts, especially in marginalized settings, to inform policy making and ensure meaningful allocation of scarce resources (12). Despite this new knowledge, global attention and prevention efforts are still focused on high-income countries (HICs), while vulnerable populations in LMICs are often neglected.
Several guidelines have established the definition of pediatric hypertension based on normative BP tables that account for age, sex, and height, and settled abnormally elevated BP levels in children at the 90th percentile and hypertension at the 95th percentile (13, 14). Currently, the most widely used guidelines were developed by the American Academy of Pediatrics (AAP) and include normative charts based on normal-weight American children and revised cut-off points (15). However, other efforts to establish BP reference tables have been made. In Germany, reference charts were derived from a population of non-overweight children participating in the KiGGS study, and are broadly used in the literature, as well (16). Xi et al. pooled data from 7 different countries in an attempt to develop universal BP references for children (17). Notwithstanding, no normative tables exist for African children, and these populations have been underrepresented in attempts to develop global references.
Furthermore, it is unclear whether country-specific BP reference tables and uniform international standards are appropriate for the estimation of pediatric hypertension prevalence in different contexts (18). Whereas the percentile values differ between the reference populations used to calculate them, context-specific socioeconomic and environmental factors might make the broad use of such standards unsuitable. Accordingly, studies have shown low consistency between international and local normative tables (19). Indeed, the prevalence of pediatric elevated BP in the African literature varies substantially, and South African studies present conflicting results (8). Different normative data and cut-offs to define high BP are used in these studies, and it remains unclear whether some authors have developed age-, sex-, and height-specific BP reference values based on their own study population, similar to the example from the Gambian study of Modou et al. (20).
Against this background, the current study aims to examine the hypertension prevalence in 897 children from lower-income families in the Eastern Cape province of South Africa considering four different BP references. Subsequently, these BP standards are compared based on their association with increasing BMI-for-age levels, an indicator of poorer cardiovascular health. We hypothesize that international normative tables and charts developed from the same study population will yield different estimates of hypertension prevalence and a different risk profile associated with BMI-for-age among children from marginalized communities in South Africa.
Results are based on cross-sectional analyzes of the KaziBantu project cohort baseline assessment, which took place between January and March 2019 (21). Children aged 8–16 years were recruited from eight schools from the economically disadvantaged peri-urban townships and northern areas of Gqeberha, South Africa. All study sites consisted of non-fee paying, quintile 3 schools (South African schools are ranked from quintile one, the poorest, to quintile five, the least poor). In total, 975 children were enrolled in the KaziBantu study. Of those, 897 children (449 boys, 448 girls) presented with complete data records, after excluding those participants with missing data for sex (n = 8), age (n = 9), height (n = 47), weight (n = 57), and BP (n = 31).
BP was measured three times on the upper left arm after a seated period of 5 min and with a 1-min rest between readings. A validated, automated oscillometric device (Omron®M6AC; Hoofddorp, Netherlands) and a child appropriate cuff, sized 17–22 cm, were used. Systolic and diastolic BP values were calculated as the mean of the last two readings to avoid overestimation usually observed on the first run.
Sex-, age-, and height-adjusted normative tables for pediatric BP were used to calculate systolic BP (SBP) and diastolic BP (DBP) percentiles. The following three widely recognized normative data charts were applied by running the programs indicated by each author: (i) AAP 2017 based on an American reference population (15, 22), (ii) Robert Koch-Institute based on a German reference population (16), and (iii) an international reference based on data pooled from 7 countries (China, India, Iran, Korea, Poland, Tunisia, and USA) (17). Furthermore, a fourth reference derived from normal-weight children from the KaziBantu study population was used (21). Because the study sample is classified through its own constructed normative tables, the study reference will henceforth be considered pseudo-normative. Details of the reference populations are presented in Supplementary Table S1.
Thereafter, the obtained percentiles were classified as normotension, elevated BP or hypertension stages 1 and 2, for both SBP and DBP, based on the cut-offs suggested in each reference, with the exception of the 99th + 5 mm Hg percentile recommended by Neuhauser et al. for stage 2 hypertension, where we applied a comparable cut-off at the 99.75th percentile to facilitate analysis. The highest value of either SBP or DBP was allocated to determine combined BP.
Body weight was measured on a digital weighing scale; children were barefoot and wore school uniform. Body height was measured against a stadiometer; children were asked to stand still with their back erect and shoulders relaxed. BMI was calculated from both weight and height according to weight (kg)/height (m)2. BMI-for-age Z-scores (BAZ) stratified by sex, a measure for obesity, overweight and thinness, were determined according to World Health Organization's (WHO) growth charts (23).
Descriptive statistics for all variables comprised means (M) and standard deviation (SD). Differences between the means for boys and girls were analyzed via independent t-tests for significance and Cohen's d for effect size. Polynomial regressions were used to construct pseudo-normative tables from the KaziBantu study population after removing outlying participants and those children whose BMI was higher than 1 SD above the group average. SBP and DBP pseudo-normative charts for boys and girls are available in the Supplementary Table S2. Prevalence of BP categorization is expressed as frequencies (N) and percentages (%) for all four classification standards. Pearson chi-square (χ2) tests were carried out to assess the distribution of sex (girls and boys) and age (≤ 10, 10, 11, ≥11 years) in all BP categories for SBP, DBP, and BP combined. Multinomial logistic regression analyzes were used to explore the association of increasing BAZ values with the prediction of BP classification into higher categories.
Statistical tests were performed using IBM SPSS version 26 (IBM; Armonk, New York, USA). Normative BP tables were applied in STATA version 15.1 (StataCorp; College Station, Texas, USA) for the German reference population and in SAS version 9.4 (SAS Institute; Cary, North Carolina, USA) for the American and global references. BP percentile tables of the KaziBantu study population were constructed in Statistica version 13 (TIBCO Software Inc., Palo Alto, USA).
Table 1 presents descriptive statistics and characteristics of the study participants, stratified by sex. Girls showed a statistically significant lower mean age (10.2 vs. 10.6 years; p < 0.001), while presenting higher mean values for the other variables. Differences in weight (36.7 vs. 34.5 kg), BMI (18.4 vs. 17.5 kg/m2), and BAZ (0.2 vs. 0.0) were of statistical significance at the p < 0.001 level. However, the Cohen's effect size was small for all sex differences in age (d = 0.30), weight (d = 0.22), BMI (d = 0.25), and BAZ (d = 0.21).
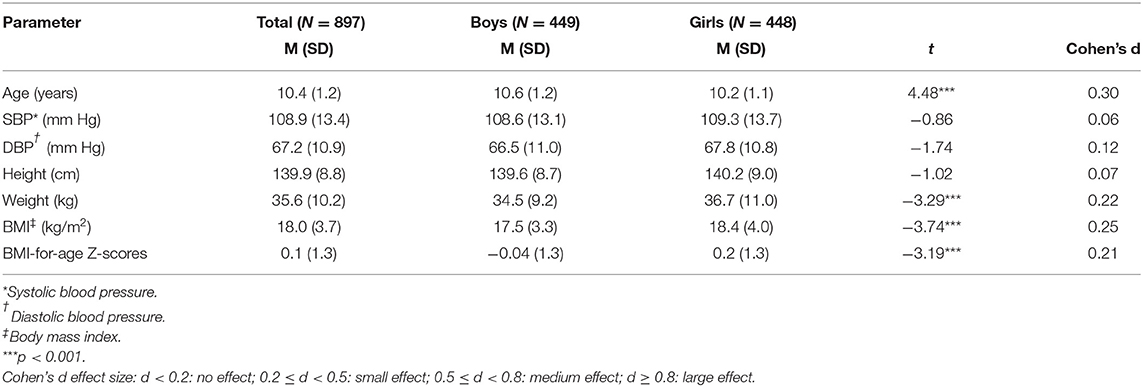
Table 1. Participant characteristics and comparison between South African girls and boys from the KaziBantu study population in Gqeberha, South Africa.
We classified BP levels according to the four normative charts and their corresponding cut-offs (Table 2). Similar combined hypertension prevalence was observed for the three international references, namely 28.6% based on the American, 28.8% on the German, and 25.6% on the global. In contrast, only 11.4% of children were identified as hypertensive according to the pseudo-normative study reference. The highest level of agreement was found between the American and the global references with 92.5%, whereby 830 children were equally stratified throughout all four categories. The KaziBantu classification revealed the highest agreement percentage with the global reference (71.5%) (data not shown).
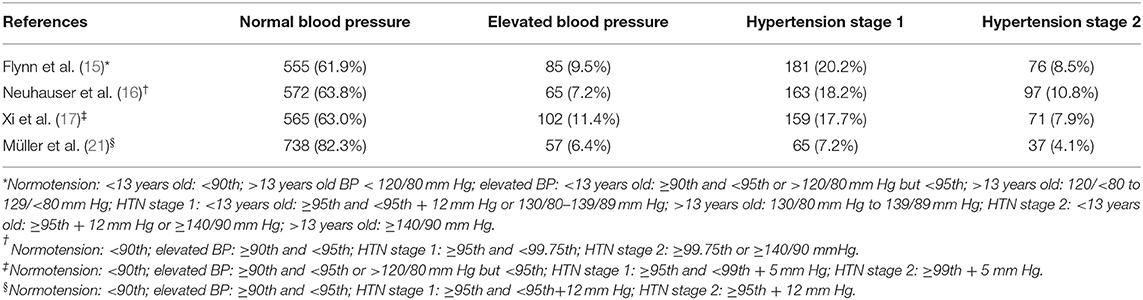
Table 2. Comparison of high blood pressure prevalence among school-aged children in Gqeberha, South Africa, in July 2019 according to the (i) American Academic of Pediatrics, (ii) German guidelines, (iii) a global reference population, and (iv) the KaziBantu study population (N = 897).
Sub-analyzes showed that the biggest disagreement between the study reference and international guidelines lied in the classification of SBP. While hypertension was more than three times higher for SBP with the American classification compared to KaziBantu's (24.2 vs. 7.2%), it was almost double for DBP (14.7 vs. 7.7%). Thus, the main driver for hypertension when applying the American guidelines was SBP rather than DBP. The higher systolic over diastolic hypertension prevalence was also observed with the global reference (23.6% for SBP vs. 10.6% for DBP).
All four standards showed similar distributions between girls and boys regardless of systolic, diastolic, or combined BP. Only in the American reference, a significant association between sex and DBP classification was observed [ = 10.46, p = 0.015], whereby girls were disproportionately associated with hypertension stage 1 (64.6%) at the p = 0.05 significance level. Age showed no association with SBP, DBP, or combined BP categorization for any of the references. Sub-analyzes can be found in the Supplementary Tables S3–S5.
The association between being classified as hypertensive with higher BMI levels for all studied references is illustrated in Figure 1. All four standards showed a significant increased risk for being categorized as having elevated BP, hypertension stage 1, and hypertension stage 2 per standard deviation increase in BMI-for-age relative to the normotensive group. The highest odds for hypertension stage 2 with increasing BAZ was seen with the American guidelines with a 72% increased risk (95% CI: 1.43–2.07; p < 0.001), followed by a 65% increased risk with both the global (95% CI: 1.37–1.99; p < 0.001) and German references (95% CI: 1.40–1.95; p < 0.001). The lowest odds were found with the pseudo-normative KaziBantu reference at 51% (95% CI: 1.18–1.92; p < 0.001). The increased risk for hypertension stage 1 with increasing BAZ was similar across the American, global, and KaziBantu study references at ~45%, being lowest with the German classification (OR = 1.37; 95% CI: 1.20–1.57; p < 0.001). Further sub-analyzes are shown in Supplementary Table S6. A significant increased risk of 43% (p = 0.003) per unit increase in BAZ was found between elevated BP and hypertension stage 2 for the American reference. With the German guidelines, increased categorization risk was significant between elevated BP and hypertension stage 2 (OR = 1.31, p = 0.027), and between hypertension stage 1 and hypertension stage 2 (OR = 1.20, p = 0.05). No significant differences were observed for the global and KaziBantu references.
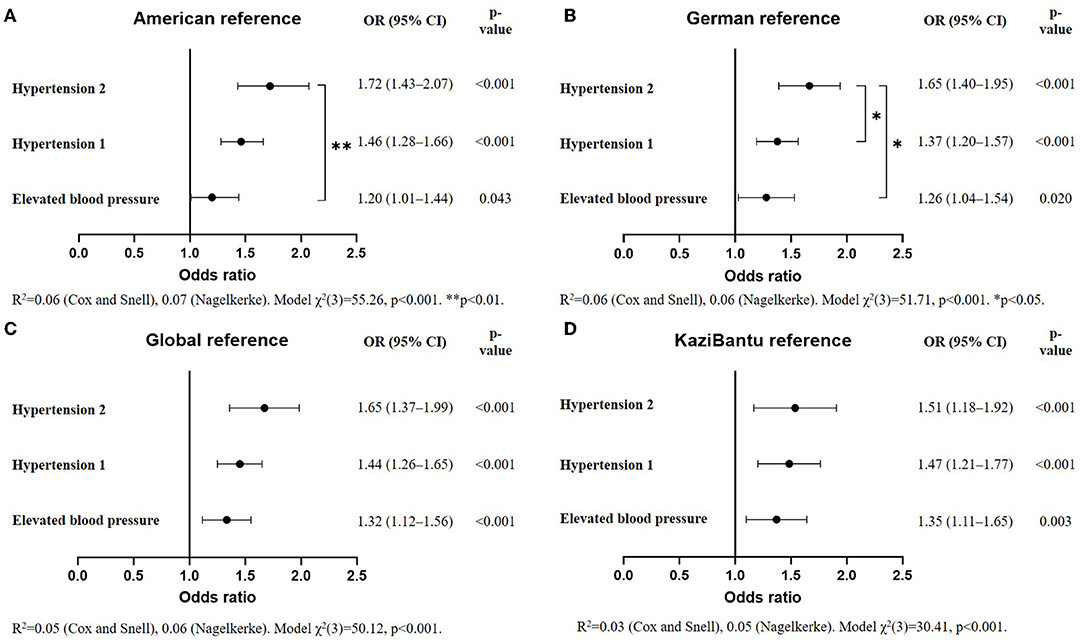
Figure 1. Odds ratio (OR) of the classification of blood pressure (BP) as elevated, hypertension stage 1 or stage 2, relative to normotension, with increasing BMI-for-age Z-scores according to (A) American, (B) German, (C) global, and (D) the KaziBantu reference populations (N = 897).
This study demonstrates differences in the implementation of international standards for the classification of BP in diverse contexts. Among school-aged children from disadvantaged communities in the Eastern Cape Province of South Africa, the obtained prevalence of hypertension ranged from 11.4%, when pseudo-normative tables from the own study population were used, to 28.8% based on international standards. Further analyzes show that the risk of being categorized as hypertensive with increasing levels of BAZ, a marker for adiposity, also varied among these standards, with the highest risk observed when international references were applied.
The first aim of the study was to establish and compare the prevalence of elevated BP and hypertension based on HIC standards, a pooled global reference, and pseudo-normative tables derived from the KaziBantu study population. We encountered a pronounced variability when different normative data were employed. International guidelines yielded the highest prevalence of hypertension in our study population at almost 30%. Although South Africa presents a higher hypertension prevalence than other sub-Saharan African countries, attributed partly to differences in countries' socioeconomic development (24), the estimates in the present study lie far above those reported by other authors. In fact, only one study has shown a higher combined hypertension prevalence of 32.6% (25). Interestingly, the authors used the German reference population from Neuhauser et al. (26). In contrast, when the KaziBantu pseudo-normative reference was used, hypertension prevalence was almost three times lower (11.4%) and thus, closer to the estimations found in the literature. However, they still remain higher than the 7.9% prevalence rates reported for Southern Africa (27) and the 8.1% for South Africa (8) in similar age groups. Nevertheless, it is noteworthy that a considerable heterogeneity exists within the South African literature, where pediatric hypertension ranges from 2.6 to 20.7% (28, 29).
This variability might be partly explained by methodological factors, such as the use of different instruments (electronic devices, sphygmomanometer, and finger-arterial pressure apparatus), or the number and occasions of BP readings (lowest of three readings, average of last two of three readings, average of three out of five measurements with the smallest variation). Arguably, we believe that this disparity is particularly governed by the use of different categorization standards and cut-offs. Many South African authors have based their estimations on outdated guidelines (29, 30), potentially leading to an underestimation of prevalence rates (31). Others have made use of the updated AAP 2017 guideline by applying simplified cut-offs. For example, Matjuda et al. considered exclusively percentiles disregarding whole values (in mm Hg) and age differences (<13 vs. >13 years) (10). In some studies, it is unclear whether researchers have developed pseudo-normative percentiles based on their own study population and subsequently classified them according to international standards (11, 32). Other studies do not describe the analysis altogether (33). Our results are in line with the disparities in hypertension estimates found in the literature and highlight an unstandardized use of methods and classification guidelines.
The discussion around the accuracy of hypertension estimates should however focus on their clinical significance, that is, on establishing BP levels that relate to a real risk for early organ damage and CVD. Hence, other environmental and socioeconomic factors that influence BP should also be taken into account when applying standards that aim at stratifying risk across different contexts. Contrary to common belief, two recent meta-analyzes have shown that hypertension was more prevalent among LMICs than HICs (34, 35). The most affected are middle-transitioning economies like South Africa, which through unplanned and rapid urbanization are adopting westernized lifestyles, while communicable diseases continue to thrive (36). In fact, infections are a cause of undernutrition, anemia, and growth retardation, which, in turn, have been associated with hypertension (37). Similarly, lower socioeconomic status has been associated with higher prevalence of CVD risk factors (38) and hypertension (39). Kagura et al. corroborated these findings in adolescents from the township of Soweto in South Africa, showing a protective role for SBP with transition from low to high socioeconomic status (40). The previously exposed suggests that particular sociological, economic, and demographic characteristics account for the variability in the pattern of CVD risk factors and justify questioning the accuracy and significance of hypertension estimates, as well as their generalizability.
The second study aim was to evaluate whether the association of BMI with BP categorization differed between international references and pseudo-normative percentiles derived from the studied population, for the relation between obesity and elevated BP in African children has been extensively described in the literature (41–43). In the “Birth to Twenty” cohort from Soweto, adiposity in early life associated with the later development of elevated BP in black adolescents (44). Kruger et al. have reported a 60% increased risk of having hypertension per unit increase in BAZ in children from the Western Cape, South Africa (9). In our sample, American guidelines showed the highest increased risk for hypertension stage 2 at 72% compared to 51% with the KaziBantu pseudo-normative reference. In our view, the association of increasing BAZ levels with a higher risk for being ranked into upper BP categories obtained with the American guidelines speaks for a potentially better classification.
Furthermore, ~50% of hypertension participants in the American and global references were hypertensive due to isolated systolic hypertension (ISH) compared to isolated diastolic and combined hypertension. This difference was not observed with the KaziBantu pseudo-normative reference. In the last years, SBP has gained relevance as a standalone risk factor for cardiovascular morbidity and mortality in adults (45). The primary prognostic significance of ISH has been observed in children too (46). Concluding, in our sample CVD risk understood as increased BMI-for-age levels and ISH was better predicted by the American and global guidelines.
The results of the present study must be considered in light of the following limitations. First, international guidelines suggest that clinical hypertension needs to be confirmed as a high BP on three separate occasions since the prevalence of elevated BP tends to decrease over subsequent visits. In line with other epidemiological studies, we have measured BP on one visit and discarded the first reading to avoid an overestimation of results. Still, Kruger et al. stated that “by using three BP measurements during a single visit and averaging either all or the last two measurements, provides larger statistical variance and yields higher BP averages” (p. 8) (9).
Second, the study population has a specific profile of children living in low-income, urban areas of the Eastern Cape of South Africa, and is thus, not representative of the broad demographic spectrum characteristic of the population of South Africa. Furthermore, we had a relatively small population size, while simplified normative BP tables were calculated due to an unequal distribution of age. It is worth mentioning that while American and global guidelines both consist of a sample size of around 50,000 children, the relative small sample size of the KaziBantu study reference may have led to an underestimation of the hypertension prevalence and a weaker risk prediction potential.
Third, this study evaluated solely the association between BP and BMI to assess risk prediction of the standards, but did not collect data on other determinants of health that influence BP. Moreover, the design of the study does not allow to link BP levels to future adverse health events. Thus, it is not possible to draw definitive conclusions about suitability, or superiority, of any of the standards.
Our findings underscore the need for further research into the medical significance of current BP management guidelines in Southern Africa. Prospective longitudinal studies will be required to associate BP levels in childhood with the incidence of CVD and mortality later in life, and to establish clinically relevant cut-off values.
We found differences in hypertension prevalence depending on the normative BP tables applied to a population of 8- to 16-year-old children from disadvantaged communities in South Africa. Furthermore, we portray a marked underrepresentation of African children in international guidelines and a need for the standardization of BP data collection and analysis in this region. Hence, we advocate for the development of normative tables that are representative of the (South) African pediatric population (and other distinct populations currently not represented in panels informing international guidelines) and the definition of cutoffs that are based on clinical evidence to ensure accurate identification of hypertension both from the clinical and epidemiological perspective in marginalized populations. We conclude that until national or regional guidelines exist, large-enough international reference populations may be used in contexts different from the ones they were developed, albeit findings must be interpreted with caution.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Nelson Mandela University Ethics Committee (H18-HEA-HMS-001), Eastern Cape Department of Education, Eastern Cape Department of Health, Ethics Committee (EC_201804_00), and Northwest and Central Switzerland (R-2018-00047). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin, while oral assent was sought from children.
PA research idea, statistical analysis and interpretation of data, and draft preparation. JB and HS conceptualization and statistical analysis. IM, MG, and HS preparation of manuscript. LA, JD, DD, SG, NJ, IM, MN, and SN data collection and curation. All authors critical revision of the manuscript, provided approval for publication of the content, and agree to be accountable for the content of the work.
The work presented here was financially supported by the Novartis Foundation (Basel, Switzerland) and the Swiss National Science Foundation (Bern, Switzerland; grant no. 192651), and took place under the auspices of the UNESCO Chair on Physical Activity and Health in Educational Settings. The funders had no role in study design, data collection, data analysis or data interpretation, nor the decision to submit the manuscript for publication.
AA was employed by the company Novartis Foundation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are grateful to the learners and parents/guardians for their participation in the study. We would especially like to thank Ms. Zaahira Ismail for her assistance with data collection and data management.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.877431/full#supplementary-material
1. World Health Organization. Cardiovascular Diseases (Cvds). (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed January 12, 2022).
2. Kruger R, Gafane-Matemane LF, Kagura J. Racial differences of early vascular aging in children and adolescents. Pediatr Nephrol. (2021) 36:1087–108. doi: 10.1007/s00467-020-04593-5
3. Climie RE, Park C, Avolio A, Mynard JP, Kruger R, Bruno RM. Vascular ageing in youth: a call to action. Heart Lung Circ. (2021) 30:1613–26. doi: 10.1016/j.hlc.2021.06.516
4. Nilsson PM, Lurbe E, Laurent S. The early life origins of vascular ageing and cardiovascular risk: the Eva syndrome. J Hypertens. (2008) 26:1049–57. doi: 10.1097/HJH.0b013e3282f82c3e
5. Kagura J, Ong KK, Adair LS, Pettifor JM, Norris SA. Paediatric hypertension in South Africa: an underestimated problem calling for action. S Afr Med J. (2018) 108:708–9. doi: 10.7196/SAMJ.2018.v108i9.13317
6. Song P, Zhang Y, Yu J, Zha M, Zhu Y, Rahimi K, et al. Global prevalence of hypertension in children: a systematic review and meta-analysis. JAMA Pediatr. (2019) 173:1154–63. doi: 10.1001/jamapediatrics.2019.3310
7. World Health Organization. Obesity and Overweight. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed January 14, 2022).
8. Noubiap JJ, Essouma M, Bigna JJ, Jingi AM, Aminde LN, Nansseu JR. Prevalence of elevated blood pressure in children and adolescents in Africa: a systematic review and meta-analysis. Lancet Public Health. (2017) 2:e375–86. doi: 10.1016/S2468-2667(17)30123-8
9. Kruger R, Kruger HS, Monyeki MA, Pienaar AE, Roux SB-L, Gafane-Matemane LF, et al. A demographic approach to assess elevated blood pressure and obesity in prepubescent children. J Hypertens. (2021) 39:2190–99. doi: 10.1097/HJH.0000000000002917
10. Matjuda EN, Engwa GA, Anye SNC, Nkeh-Chungag BN, Goswami N. Cardiovascular risk factors and their relationship with vascular dysfunction in south african children of African ancestry. J Clin Med. (2021) 10:354. doi: 10.3390/jcm10020354
11. Kagura J, Adair LS, Musa MG, Pettifor JM, Norris SA. Blood pressure tracking in urban black South African children: birth to twenty cohort. BMC Pediatr. (2015) 15:78. doi: 10.1186/s12887-015-0402-z
12. Shung-King M, Lake L, Sanders D, Hendricks M. Child and adolescent health – leave no one behind. South Afr Child Gauge. (2019) 264. Available online at: http://www.ci.uct.ac.za/cg-2019-child-and-adolescent-health
13. Expert Panel on Integrated Guidelines for Cardiovascular H, Risk Reduction in C, Adolescents National Heart L, Blood I. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. (2011) 128 (Suppl. 5):S213–56. doi: 10.1542/peds.2009-2107C
14. Lurbe E, Cifkova R, Cruickshank JK, Dillon MJ, Ferreira I, Invitti C, et al. Management of high blood pressure in children and adolescents: recommendations of the european society of hypertension. J Hypertens. (2009) 27:1719–42. doi: 10.1097/HJH.0b013e32832f4f6b
15. Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. (2017) 140:e20171904. doi: 10.1542/peds.2017-1904
16. Neuhauser H, Schienkiewitz A, Schaffrath AR, Dortschy R, Kurth B-M. Referenzperzentile Für Anthropometrische Maßzahlen Und Blutdruck Aus Der Studie Zur Gesundheit Von Kindern Und Jugendlichen in Deutschalnd (Kiggs). In: Bundes Gd, editor: Robert Koch-Institut. (2013). p. 101.
17. Xi B, Zong X, Kelishadi R, Hong YM, Khadilkar A, Steffen LM, et al. Establishing international blood pressure references among nonoverweight children and adolescents aged 6 to 17 years. Circulation. (2016) 133:398–408. doi: 10.1161/CIRCULATIONAHA.115.017936
18. Daniels SR. How to define hypertension in children and adolescents. Circulation. (2016) 133:350–1. doi: 10.1161/CIRCULATIONAHA.115.020531
19. Agirbasli M, Dilek HF, Tatlisu MA, Ankarali H. Reliability of normative tables in assessing elevated blood pressure in children. J Hum Hypertens. (2020) 34:241–7. doi: 10.1038/s41371-019-0290-z
20. Jobe M, Agbla SC, Prentice AM, Hennig BJ. High blood pressure and associated risk factors as indicator of preclinical hypertension in rural West Africa: a focus on children and adolescents in the Gambia. Medicine. (2017) 96:e6170. doi: 10.1097/MD.0000000000006170
21. Müller I, Smith D, Adams L, Aerts A, Damons BP, Degen J, et al. Effects of a school-based health intervention program in marginalized communities of port Elizabeth, South Africa (the Kazibantu Study): protocol for a randomized controlled trial. JMIR Res Protoc. (2019) 8:e14097. doi: 10.2196/14097
22. Rosner B. Pediatric Blood Pressure. (2021). Available online at: https://sites.google.com/a/channing.harvard.edu/bernardrosner/pediatric-blood-press (accessed June 25, 2021).
23. World Health Organization. Growth Reference Data for 5-19 Years: Bmi-for-Age. World Health Organization (2007). Available online at: https://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed September 13, 2020).
24. Gomez-Olive FX, Ali SA, Made F, Kyobutungi C, Nonterah E, Micklesfield L, et al. Regional and sex differences in the prevalence and awareness of hypertension: an H3africa Awi-Gen study across 6 sites in sub-Saharan Africa. Glob Heart. (2017) 12:81–90. doi: 10.1016/j.gheart.2017.01.007
25. Gerber M, Müller I, Walter C, du Randt R, Adams L, Gall S, et al. Physical activity and dual disease burden among south african primary schoolchildren from disadvantaged neighbourhoods. Prev Med. (2018) 112:104–10. doi: 10.1016/j.ypmed.2018.04.001
26. Neuhauser HK, Thamm M, Ellert U, Hense HW, Rosario AS. Blood pressure percentiles by age and height from nonoverweight children and adolescents in Germany. Pediatrics. (2011) 127:e978–88. doi: 10.1542/peds.2010-1290
27. Crouch SH, Soepnel LM, Kolkenbeck-Ruh A, Maposa I, Naidoo S, Davies J, et al. Paediatric hypertension in africa: a systematic review and meta-analysis. EClinicalMedicine. (2022) 43:101229. doi: 10.1016/j.eclinm.2021.101229
28. Negash S, Agyemang C, Matsha TE, Peer N, Erasmus RT, Kengne AP. Differential prevalence and associations of overweight and obesity by gender and population group among school learners in South Africa: a cross-sectional study. BMC Obes. (2017) 4:29. doi: 10.1186/s40608-017-0165-1
29. Chungag A, Tata CM, Sewani-Rusike CR, Nel W, Nkeh-Chungag BN. Ellisras longitudinal study 2017: association of hypertension with increasing levels of adiposity in 10- to 14-year-old boys and girls in the Eastern Cape (Els 31). Cardiovasc J Afr. (2019) 30:258–61. doi: 10.5830/CVJA-2019-017
30. Gomwe H, Seekoe E, Lyoka P, Marange CS. The relationship between body composition and blood pressure among primary school children in Eastern Cape Province, South Africa. Afr J Prim Health Care Fam Med. (2019) 11:e1–6. doi: 10.4102/phcfm.v11i1.2000
31. Yang L, Kelishadi R, Hong YM, Khadilkar A, Nawarycz T, Krzywinska-Wiewiorowska M, et al. Impact of the 2017 American academy of pediatrics guideline on hypertension prevalence compared with the fourth report in an international cohort. Hypertension. (2019) 74:1343–8. doi: 10.1161/HYPERTENSIONAHA.119.13807
32. Nkeh-Chungag BN, Sekokotla AM, Sewani-Rusike C, Namugowa A, Iputo JE. Prevalence of hypertension and pre-hypertension in 13-17 year old adolescents living in Mthatha - South Africa: a cross-sectional study. Cent Eur J Public Health. (2015) 23:59–64. doi: 10.21101/cejph.a3922
33. Mokwatsi GG, Schutte AE, Kruger R. Ethnic differences regarding arterial stiffness of 6-8-year-old black and white boys. J Hypertens. (2017) 35:960–7. doi: 10.1097/HJH.0000000000001267
34. Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. (2016) 134:441–50. doi: 10.1161/CIRCULATIONAHA.115.018912
35. Zhou B, Perel P, Mensah GA, Ezzati M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol. (2021) 18:785–802. doi: 10.1038/s41569-021-00559-8
36. Mbogori T, Kimmel K, Zhang M, Kandiah J, Wang Y. Nutrition transition and double burden of malnutrition in Africa: a case study of four selected countries with different social economic development. AIMS Public Health. (2020) 7:425–39. doi: 10.3934/publichealth.2020035
37. Sawaya AL, Sesso R, Florêncio TMdMT, Fernandes MTB, Martins PA. Association between chronic undernutrition and hypertension. Maternal Child Nutr. (2005) 1:155–63. doi: 10.1111/j.1740-8709.2005.00033.x
38. Pisa PT, Behanan R, Vorster HH, Kruger A. Social drift of cardiovascular disease risk factors in Africans from the North West province of South Africa: the pure study. Cardiovasc J Afr. (2012) 23:371–8, e9–88. doi: 10.5830/CVJA-2012-018
39. Stringhini S, Forrester TE, Plange-Rhule J, Lambert EV, Viswanathan B, Riesen W, et al. The social patterning of risk factors for noncommunicable diseases in five countries: evidence from the modeling the epidemiologic transition study (Mets). BMC Public Health. (2016) 16:956. doi: 10.1186/s12889-016-3589-5
40. Kagura J, Adair LS, Pisa PT, Griffiths PL, Pettifor JM, Norris SA. Association of socioeconomic status change between infancy and adolescence, and blood pressure, in South African Young adults: birth to twenty cohort. BMJ Open. (2016) 6:e008805. doi: 10.1136/bmjopen-2015-008805
41. Kemp C. The prevalence of hypertension and the relationship with body composition in grade 1 learners in the North West Province of South Africa. South Afr J Sports Med. (2011) 23. doi: 10.17159/2078-516X/2011/v23i4a324
42. Chedjou-Nono E, Sap S, Choukem SP, Ngosso Tetanye I, Nebongo D, Koki Ndombo O. Cardiometabolic profile of obese children in a sub-saharan african setting: a cross-sectional study. BMC Pediatr. (2017) 17:129. doi: 10.1186/s12887-017-0880-2
43. Nyangasa MA, Buck C, Kelm S, Sheikh MA, Brackmann KL, Hebestreit A. Association between cardiometabolic risk factors and body mass index, waist circumferences and body fat in a Zanzibari cross-sectional study. BMJ Open. (2019) 9:e025397. doi: 10.1136/bmjopen-2018-025397
44. Munthali RJ, Kagura J, Lombard Z, Norris SA. Childhood adiposity trajectories are associated with late adolescent blood pressure: birth to twenty cohort. BMC Public Health. (2016) 16:665. doi: 10.1186/s12889-016-3337-x
45. Tin L, Beevers D, Lip G. Systolic vs diastolic blood pressure and the burden of hypertension. J Hum Hypertens. (2002) 16:147–50. doi: 10.1038/sj.jhh.1001373
Keywords: pediatric hypertension, prevalence, identification, normative blood pressure tables, international guidelines, marginalized settings, Africa
Citation: Arnaiz P, Müller I, Seelig H, Gerber M, Bosma J, Dolley D, Adams L, Degen J, Gall S, Joubert N, Nienaber M, Nqweniso S, Aerts A, Steinmann P, Randt Rd, Walter C, Utzinger J and Pühse U (2022) Practice Change Needed for the Identification of Pediatric Hypertension in Marginalized Populations: An Example From South Africa. Front. Pediatr. 10:877431. doi: 10.3389/fped.2022.877431
Received: 16 February 2022; Accepted: 18 April 2022;
Published: 11 May 2022.
Edited by:
Alessandro Giamberti, IRCCS San Donato Polyclinic, ItalyReviewed by:
Paolo Ferrero, IRCCS San Donato Polyclinic, ItalyCopyright © 2022 Arnaiz, Müller, Seelig, Gerber, Bosma, Dolley, Adams, Degen, Gall, Joubert, Nienaber, Nqweniso, Aerts, Steinmann, Randt, Walter, Utzinger and Pühse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patricia Arnaiz, cGF0cmljaWEuYXJuYWl6QHVuaWJhcy5jaA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.