 Ana M. Campos-Martinez
Ana M. Campos-Martinez J. Expósito-Herrera1
J. Expósito-Herrera1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 17 May 2022
Sec. Neonatology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.874976
This article is part of the Research Topic Risk and Preventive Factors in Necrotizing Enterocolitis and its Complications in Premature Infants View all 7 articles
Necrotizing enterocolitis (NEC) is a serious condition related to prematurity and the initiation of enteral feeding. In this article, we review the evidence published in recent years on necrotizing enterocolitis risk factors (prematurity, feeding with low-weight formula, existence of intestinal dysbiosis) and protective factors (human milk or donated milk supply, supplementation of human milk with oligosaccharides, probiotics administration, and the determination of disease predictive biomarkers). A systematic review was conducted of preventive, risk and predictive factors for necrotizing enterocolitis in neonates prior to 37 weeks' gestational age, based on a literature search for clinical trials, meta-analyses, randomized controlled trials and systematic reviews published between January 2018 and October 2021. For this purpose, the PubMed, MEDLINE, and Cochrane Library databases were consulted. The literature search obtained 113 articles, of which 19 were selected for further analysis after applying the inclusion and exclusion criteria. The conclusions drawn from this analysis were that adequate knowledge of risk factors that can be prevented or modified (such as alteration of the intestinal microbiota, oxidative stress, metabolic dysfunction at birth, or alteration of the immunity modulation) can reduce the incidence of NEC in premature infants. These factors include the supplementation of enteral nutrition with human milk oligosaccharides (with prebiotic and immunomodulatory effects), the combined administration of probiotics (especially the Lactobacillus spp and Bifidobacterium spp combination, which inhibits bacterial adhesion effects, improves the intestinal mucosa barrier function, strengthens the innate and adaptive immune system and increases the secretion of bioactive metabolites), the supplementation of human milk with lactoferrin and the use of donated milk fortified in accordance with the characteristics of the premature newborn. The determination of factors that can predict the existence of NEC, such as fecal calprotectin, increased TLR4 activity, and IL6 receptor, can lead to an early diagnosis of NEC. Although further studies should be conducted to determine the values of predictive biomarkers of NEC, and/or the recommended doses and strains of probiotics, lactoferrin or oligosaccharides, the knowledge acquired in recent years is encouraging.
In premature infants, necrotizing enterocolitis (NEC) is the leading cause of death due to gastrointestinal disease, affecting 5–12% of very low birth weight (VLBW) newborns (1, 2).
The pathophysiology of necrotizing enterocolitis is characterized by its multifactorial nature. Among the most common risk factors are those of prenatal origin, such as chorioamnionitis or genetic imprinting; perinatal factors such as low gestational age at birth, low birth weight, or abnormal gut microbiota (3); and risk factors derived from neonatal care and stage, such as mechanical ventilation, type of feeding, or pharmacological interventions (1).
Various strategies have been proposed for the prevention of NEC (4), including the routine use of different strains of probiotics, especially Lactobacillus and Bifidobacterium (5). However, the most suitable combination of strains and the optimum doses have yet to be determined.
In the newborn, microbiota are mainly formed by species of Bifidobacterium. The colonization of the newborn in the first stages of life is influenced by several factors, including the type of delivery, the type of infant feeding, gestational age at birth and the administration of antibiotics in the early stages of life. In cesarean deliveries, the intestinal colonization of the newborn may be delayed, coinciding with neonatal colonization with flora from the maternal skin. In vaginal deliveries, on the other hand, colonization occurs preferentially with flora from the birth canal. After cesarean delivery, newborns present a lower proportion of Bacteroides with fewer Bifidobacteria. Recent studies have reported a decrease in Bifidobacteria in the fecal flora of the newborn when the mother received intrapartum prophylaxis with ampicillin; however, other bacteria of the genus firmicutes, to which Lactobacillus and Clostridia belong, are not modified (6).
Human milk is another factor preventing NEC, both because of the microbiota it provides and because of the presence of immunoglobulin A and oligosaccharides (4). During lactation, the bacteria associated with the intestine are transported by the blood and lymphatics to the mammary gland. Human milk promotes a flora rich in Bifidobacterium, with lower counts of E. coli, Clostridium difficile, and Bacteroides fragilis. Formula milk is known to alter the profile of intestinal colonization, associating it with more Bifidobacterium and other facultative anaerobes.
After childbirth, breastfeeding contributes to increasing the initial inoculum with lactic acid-producing bacteria, Bifidobacterium, and bacteria from the mother's skin. Bifidobacterium and fecal Lactobacillus/Enterococci counts at 6 months are higher in breastfed infants than in formula-fed infants (7). Skin-to-skin contact, the administration of lactoferrin to human milk, the use of donated milk with fortification individualized to the characteristics of the premature newborn (8), as well as the determination of factors that can predict the existence of NEC, such as fecal calprotectin, increased TLR4 activity and IL6 receptor (9), can all modify the NEC outcome.
The aim of this study is to review the existing evidence on preventive and risk factors for necrotizing enterocolitis in premature infants.
This study is a systematic review. The review was conducted of preventive, risk and predictive factors for necrotizing enterocolitis in neonates prior to 37 weeks' gestational age, based on a literature search for clinical trials, meta-analyses, randomized controlled trials, and systematic reviews published between January 2018 and October 2021. This review was performed via a search of the following websites presenting data on relevant clinical practice: the Cochrane Library, PubMed and Medline databases. In PubMed, the MeSH terms used were “Necrotizing enterocolitis”[Mesh] AND “Infant, Very Low Birth Weight”[Mesh] OR “Necrotizing enterocolitis”[Mesh] AND “Probiotics”[Mesh] OR “Necrotizing enterocolitis”[Mesh] AND “Nutrition”[Mesh] OR “Necrotizing enterocolitis”[Mesh] AND “Preventive factor”[Mesh] OR “Necrotizing enterocolitis”[Mesh] AND “Risk factor”[Mesh] AND 2018[PDAT]: 2021[PDAT] AND (English[lang] OR Spanish[lang]) AND (Clinical Trial[ptyp] OR Meta-Analysis [ptyp] OR Practice Guideline [ptyp] OR Randomized Controlled Trial [ptyp] OR Review [ptyp]).
We use the PRISMA 2020 chek list for this systematic review (10).
The following selection criteria were applied: (a) Premature infants with <37 weeks' gestational age or <2,500 g birth weight; (b) Studies published during the period 2018 to 2021; (c) Studies focused on risk or preventive factors from NEC (primary or secondary outcomes); (d) Comparison between intervention groups, with placebo or negative control.
The exclusion criteria were: (a) Articles in languages other than Spanish or English; (b) Studies dealing exclusively with animals; (c) Articles that presented insufficient data or confusing data; (d) Articles that did not differentiate between premature infants and other age groups.
We assessed the risk of bias and extracted the following data: general study information (author's name, publication year), study population details, details of the intervention and comparison and outcomes.
Of the articles used, 13 had the existence or not of necrotizing enterocolitis as the primary outcome of their study, but in any case, even if the outcome was secondary, the presented significant statistical data regarding the NEC development or not.
For each study, we look at and assess the odds ratio (OR) or relative risk (RR), and 95% confidence intervals (IC) on the results.
The PRISMA 2020 flow diagram for the source selection process is shown in Figure 1.
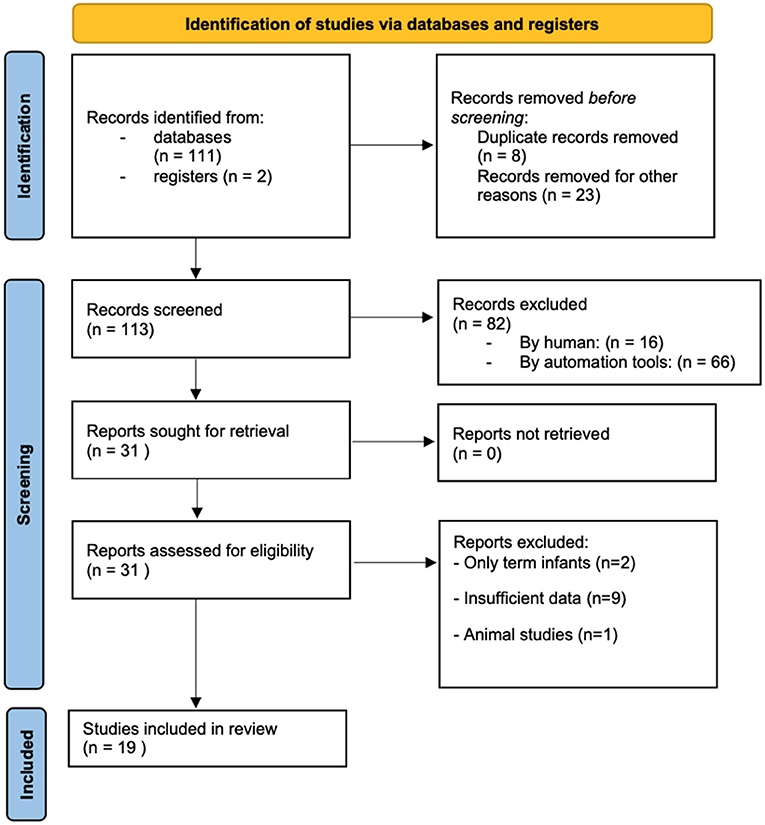
Figure 1. PRISMA 2020 flow diagram of the studies selected for analysis.
The literature search initially yielded 113 articles. After discarding duplicates and excluding unrelated articles (according to the document title and abstract), 31 papers remained, for which the full texts were obtained. Following application of the inclusion/exclusion criteria described, eleven of these papers were excluded, leaving nineteen for the final analysis (Figure 1).
The following studies were included in the final analysis: seven systematic reviews (SR), eight meta-analyses (NMA), two narrative reviews (NR), one cohort study (OS), and one case-control study (CC).
Table 1 summarizes the main results obtained, showing the type of study, sample size (it it can be specified) and the factors studied: preventive factors (probiotics, oligosaccharides, human and donated milk, lactoferrin, inmunomoulators, and other factors), risk factors and predictive factors for NEC.
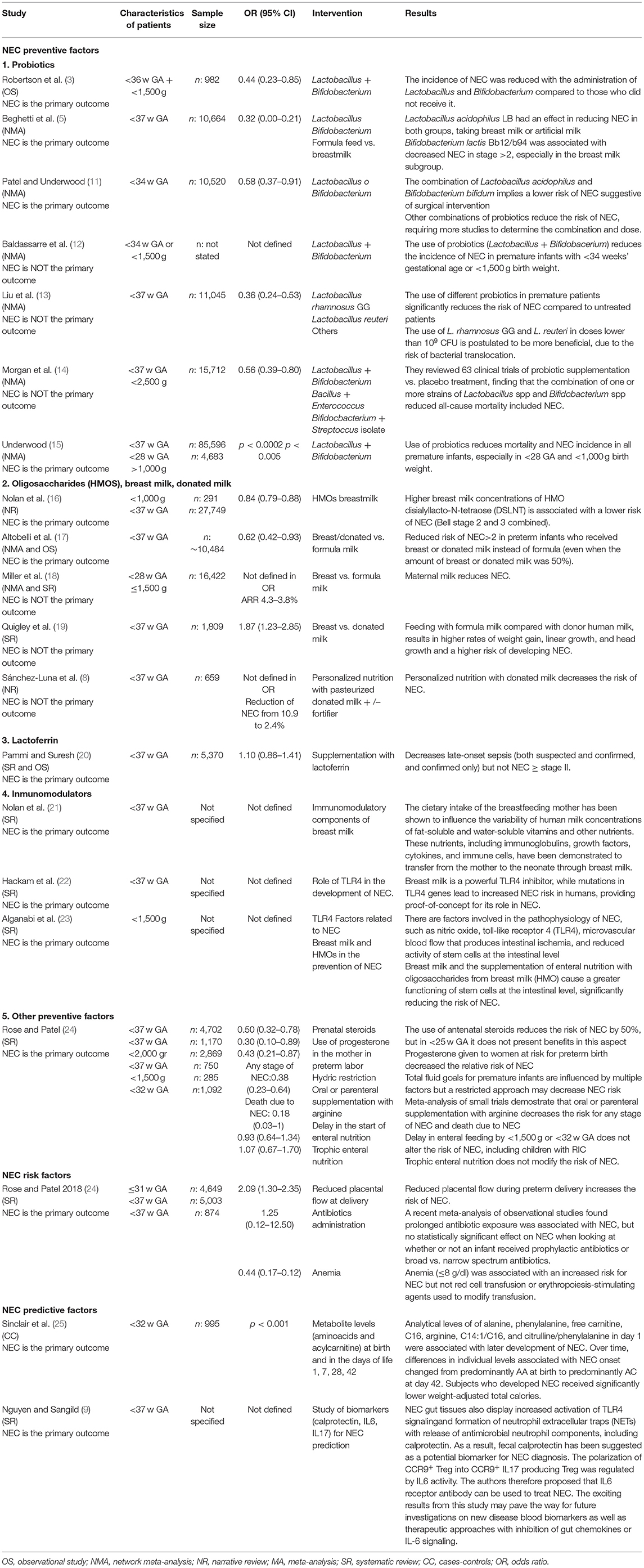
Table 1. Characteristics of the studies included in the systematic review.
About the relationship of probiotics with the reduction in the risk of NEC, we selected 7 studies (1 OS, 6 NMA), with ~134.000 patients, of <37 weeks (the sample size can be consulted in Table 1), showing that the administration of different strains of Lactobacillus and Bifidobacterium (3, 5, 11–15), compared with the use of the other probiotics or placebo, reduces the incidence of NEC Bell stage ≥2, especially in <28 AG and <1,000 g birth weight (15). In one of the studies included, belonging to Patel and Underwood (11), it is assessed that the combination of Lactobacillus acidophuilus and Bifidobacterium bifidum in <34 weeks, implies a decrease both in NEC and in presenting NEC that requires surgical intervention. Other authors such as Liu et al. (13), propose Lactobacillus rhamnosus GG and Lactobacillus reuteri at doses <109 CFU as the best combination of probiotics in <37 weeks, due to the risk of bacterial translocations.
In four of the seven articles included in this section, the appearance or not of NEC was part of their primary outcomes. Other outcomes studied were the reduction in mortality and the appearance or not of late sepsis. In both cases, the incidence was lower in the probiotics administration group (Lactobacillus and Bifidobacterium).
Five studies (8, 16–19) were collected in this section to assess whether the use of oligosaccharides from breast milk, and the administration of donated and human milk vs. formula, reduced the incidence of NEC. Of the 5 studies (2 NR, 1 SR, 2 NMA), 2 of them presented the development or not of NEC as the primary outcome. Nolan et al. (16) reviewed a series of studies with a sample size of 27.749 preterms <37 weeks (291 patients <1,000 g), to determine whether human milk oligosaccharides (HMOs) contributed to the prevention of NEC. The results obtained suggest that a higher human milk concentration of HMO disialyllacto-N-tetraose (DSLNT) is associated with a lower risk of the infant developing NEC (Bell stages 2 and 3 combined).
Three studies (17–19) with a sample size of 28.715 patients, show the benefit of using breast milk and donated milk instead of formula milk in reducing the risk of developing NEC Bell stage ≥2, even showing benefit in this reduction when mixed feeding is taken instead of only formula milk (19).
Pammi and Suresh (20) conducted a systematic review of the preventive role of lactoferrin in NEC and reported low-certainty evidence from studies of good methodological quality that lactoferrin supplementation of enteral feeds decreases late-onset sepsis (both suspected and confirmed, and confirmed only) but not NEC ≥ stage II.
This section contains 3 systematic reviews in which the results on the role that immunomodulators in breast milk have on the development of NEC have been evaluated.
In the first study in this section, led by Nolan et al. (21), observed that major immunologic components in human milk, such as secretory immunoglobulin A (IgA), and growh factors, protecting against NEC.
The other 2 sistematic reviews (22, 23), showed that NEC develops in response to exaggerated bacterial signaling in the premature intestine, as a consequence of elevated expression and activity of the bacterial receptor toll-like receptor 4 (TLR4), which is important for normal gut development. Human milk is a powerful TLR4 inhibitor, while mutations in TLR4 genes lead to increased NEC risk in humans, providing proof-of-concept for its role in NEC.
Rose and Patel (24) performed an systematic review with an extensive critical analysis of the preventive factors. With respect to maternal and neonatal factors, these authors observed that antenatal steroid (ANS) administration decreased the relative risk of NEC by 50%, in preterm infants, but they reported no benefit with respect to NEC from the use of ANS at very low gestational ages, perhaps due to effects on the competing cause of death (more survivors increase the number of infants at risk for NEC). Progesterone given to women at risk for preterm birth decreases the relative risk of NEC by 70%. Total fluid goals for premature infants are influenced by multiple factors, but a restricted approach may decrease the risk of NEC in infants <2,000 g (n = 526 infants).
On the other hand, oral or parenteral supplementation with arginine (26) decreases the risk for any stage of NEC and death due to NEC. Delayed feeding in infants <1,500 g or <32 weeks does not alter the NEC risk even for IUGR infants with abnormal umbilical Doppler flow velocities. Therefore, the best feeding strategy for the most immature infants remains unclear. A systematic review (27) included in the Rose and Patel work, showed that the question of trophic feeding vs. enteral fasting in extremely low birth weight infants has yet to be clarified. In patients <1500 g suggests there is no increased risk of NEC with trophic feeding.
Within this section, we value various studies collected in the systematic review prepared by Rose and Patel (24), observing the negative impact that some factors have on the appearance of NEC. Among factors related to intrauterine growth, compromised fetal blood flow before or at the time of delivery may result in fetal ischemia, contributing to NEC (20).
Two studies were included in this section (1 SR and 1 CC). In both studies, the primary outcome was the NEC development or not. Sinclair et al. (25) published a multicenter case-control study with 995 patients <32 weeks, and hypothesized that in addition to nutritional variability, metabolic dysfunction is associated with the onset of NEC, specially the measure of amino acid (AA) and acylcarnitine (AC) in blood. A review by Nguyen and Sangild (9) reported a significant reduction in lamina propria Treg density in the ileum of NEC infants, suggesting impaired intestinal Treg function and excessive inflammatory responses during NEC progression. As a result, fecal calprotectin has been suggested as a potential biomarker for NEC diagnosis.
Necrotizing enterocolitis is a serious health problem for premature newborns. Knowledge of the protective, risk, and predictive factors of this disease will help us reduce its incidence.
Preventive factors against the development of NEC are becoming clearer. These include breastfeeding or donated human milk, the combined use of probiotics from different strains of Lactobacillus and Bifidobacterium, the exogenous administration of oligosaccharides from human milk (which are a protective factor for the immature intestine), and other immunomodulators, especially from human milk. On the other hand, controversy remains about the benefit of the systematic administration of lactoferrin.
Different studies have shown the preventive effect of the administration of different strains of Lactobacillus + Bifidobacterium on the development of NEC in premature infants <37 weeks (3, 5, 11, 12, 14, 15). In the works by Patel and Underwood (11), and Baldasarre et al. (12), the patients included in the study are <34 weeks, but one of the limitations in the study by Baldasarre et al. (12) is that it does not specify the sample size analyzed. Underwood (15) analyzed patients <28 weeks and <1,000 g, with similar results to patients of higher gestational age. In the work of Beguetti et al. (5), they studied the effect of different probiotics on NEC, differentiating infants given formula milk from those who were breastfed. These authors reported that the administration of Lactobacillus acidophilus reduced the risk of NEC (OR 0.03; 95% CI 0.00–0.21) in both groups, while the use of Bifidobacterium lactis Bb12/b94 was associated with fewer cases of NEC in stage >2. Liu et al. (13) found that the relative risk (RR) ratio of developing NEC in premature infants given probiotics was 0.33 (95% C.I 0.24–0.46), indicating a powerful preventive effect. A limitation of this study was that different probiotics were used and in different doses. Lactobacillus rhamnosus GG and Lactobacillus reuteri are among the best candidates. However, caution should be taken not to exceed doses of 109 CFU in premature neonates because of the risk of bacterial translocation.
Nolan (16) reviewed evidence on the association between the presence of oligosaccharides in human milk and the incidence of NEC, observing that this incidence decreased with HMO supplementation. Similarly, Alganabi et al. (23) highlighted the role played by HMOs in enhancing the functioning of stem cells at the intestinal level, thereby reducing the risk of NEC.
In the last study of this section, Sanchez Luna et al. (8) conducted a narrative review. They established a personalized nutrition unit (PNU), providing donated milk and fortification appropriate to individual need. After the introduction of this PNU, mother's-own-milk (MOM) feeding increased from 90% of the premature infants to 98.8%, and exclusive MOM feeding increased from 39 to 55%. The authors also reported a clear difference in total protein content by gestational age and lactation, by the existence of the PNU was also associated with decreased NEC, although it is true that the existence or not of necrotizing enterocolitis was not the primary outcome of this study.
About the inmunomodulators of human milk, Nolan et al. (21) reviewed the immutable components of human milk and their protective influence on necrotizing enterocolitis. Major immunologic components in human milk, such as secretory immunoglobulin A (IgA) and growth factors, are known to play a role in regulating gut barrier integrity and microbial colonization, there by protecting against NEC. Human milk supplements infants with human milk oligosaccharides, leukocytes, cytokines, nitric oxide, and growth factors, all of which attenuate inflammatory responses and provide immunological defenses to reduce the incidence of NEC, and both Hackham et al. (22) and Alganabi et al. (23) examined the role of human milk as an inhibitor of TLR4. Given that certain mutations in the TLR4 genes increase the risk of NEC, this effect of human milk would protect against enterocolitis in such cases.
One of the limitations of the Rose and Patel (24) study, was that they performed a systematic review with an extensive critical analysis of the preventive factors, and some studies are old, so they have been discarded. Some of the preventive factors analyzed in this study, and that they present validity for their study, are the use of prenatal steroids (especially in infants older than 25 w), the use of EPO or red blood cell transfusions, fluid restriction, and probiotic supplementation. Delay in enteral feeding in newborns weighing <1,500 g or with a gestational age of <32 w does not alter the risk of NEC, even for infants with intrauterine growth restriction. Neither is this risk modified by trophic enteral nutrition.
Known risk factors for NEC include prenatal factors (genetics, chorioamnionitis, intestinal immaturity), perinatal factors (low gestational age, low birth weight, abnormal colonization of the intestinal microbiota) and those derived from the neonatal stage and the care provided during this phase (environmental stress, mechanical ventilation, central catheters, pharmacological interventions, or antibiotic therapy) (1). In a cohort of infants aged <34 weeks (28), those with a persistent ductus arteriosus (PDA) with or without indomethacin treatment had an increased risk of NEC compared to infants with no PDA.
Among other factors that may favor the appearance of NEC find reduced placental flow, fluid overload, anemia (Hb ≤ 8 g/dl, but not red cell transfusion) or the prolonged use of antibiotics (24).
Sinclair et al. (25) considered the levels of metabolites (amino acids and acylcarnitine) at birth and on days 1, 7, 28, and 42 of life. This analysis revealed higher levels of acylcarnitine and lower levels of amino acids in infants with NEC, and so these factors should be taken into account as possible predictors of NEC. Finally, Nguyen and Sangild (9) studied various predictive biomarkers of NEC, including fecal calprotectin and IL 6 and 17: this review reported a significant reduction in lamina propria Treg density in the ileum of NEC infants, suggesting impaired intestinal Treg function and excessive inflammatory responses during NEC progression. Furthermore, NEC gut tissues also display increased activation of TLR4 signaling and the formation of neutrophil extracellular traps (NETs) with the release of antimicrobial neutrophil components, including calprotectin. As a result, fecal calprotectin has been suggested as a potential biomarker for NEC diagnosis.
Although some of these studies were only performed in the laboratory or used small samples, they provide a valuable basis for further research that may achieve more reliable and consistent results.
The number of studies conducted to determine the risk and preventive factors for NEC is constantly increasing. In this respect, the use of probiotics, especially Lactobacillus and Bifidobacterium in combination, is becoming widespread as a preventive measure, although the best strains and optimum doses have yet to be established. However, supplementation with oligosaccharides from human milk is known to be beneficial, and there is no doubt that both human milk and donated milk have a protective effect against NEC, due to the presence of specific microbiota, HMOs, metabolites, and immunomodulatory factors. The likelihood of NEC can be reduced by avoiding formula milk and the prolonged use of antibiotics and by preventing neonatal anemia. A better understanding of new biomarkers, such as IL 6 or IL 17, would facilitate the early identification of NEC and thus reduce its incidence.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Meister AL, Doheny KK, Travagli RA. Necrotizing enterocolitis: it's not all in the gut. Exp Biol Med. (2020) 245:85–95. doi: 10.1177/1535370219891971
2. Xiong T, Maheshwari A, Neu J, Ei-Saie A, Pammi M. An overview of systematic reviews of randomized-controlled trials for preventing necrotizing enterocolitis in preterm infants. Neonatology. (2020) 117:46–56. doi: 10.1159/000504371
3. Robertson C, Robertson C, Savva GM, Clapuci R, Jones J, Maimouni H, et al. Incidence of necrotising enterocolitis before and after introducing routine prophylactic Lactobacillus and Bifidobacterium probiotics. Arch Dis Childh Fetal Neonatal Ed. (2020) 105:380–6. doi: 10.1136/archdischild-2019-317346
4. Jin Y-T, Duan Y, Deng X-K, Lin J. Prevention of necrotizing enterocolitis in premature infants – an updated review. World J Clin Pediatr. (2019) 8:23–32. doi: 10.5409/wjcp.v8.i2.23
5. Beghetti I, Panizza D, Lenzi J, Gori D, Martini S, Corvaglia L, et al. Probiotics for preventing necrotizing enterocolitis in preterm infants: a network meta-analysis. Nutrients. (2021) 13:192. doi: 10.3390/nu13010192
6. Aloisio I, Quagliariello A, de Fanti S, Luiselli D, de Filippo C, Albanese D, et al. Evaluation of the effects of intrapartum antibiotic prophylaxis on newborn intestinal microbiota using a sequencing approach targeted to multi hypervariable 16S rDNA regions. Appl Microbiol Biotechnol. (2016) 100:5537–46. doi: 10.1007/s00253-016-7410-2
7. Rigon G, Vallone C, Lucantoni V, Signore F. Maternal factors pre- and during delivery contribute to gut microbiota shaping in newborns. Front Cell Infect Microbiol. (2012) 2:93. doi: 10.3389/fcimb.2012.00093
8. Sánchez Luna M, Martin SC, Gómez-de-Orgaz CS. Human milk bank and personalized nutrition in the NICU: a narrative review. Euro J Pediatr. (2021) 180:1327–33. doi: 10.1007/s00431-020-03887-y
9. Nguyen DN, Sangild PT. Pathogenesis and biomarkers for necrotizing enterocolitis: getting any closer? EBioMedicine. (2019) 45:13–4. doi: 10.1016/j.ebiom.2019.06.029
10. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. (2021) 372:n160. doi: 10.1136/bmj.n160
11. Patel RM, Underwood MA. Probiotics and necrotizing enterocolitis. Semin Pediatr Surg. (2018) 27:39–46. doi: 10.1053/j.sempedsurg.2017.11.008
12. Baldassarre ME, Mauro A di, Capozza M, Rizzo V, Schettini F, Panza R, et al. Dysbiosis and prematurity: is there a role for probiotics? Nutrients. (2019) 11:1273. doi: 10.3390/nu11061273
13. Liu Y, Tran DQ, Rhoads JM. Probiotics in disease prevention and treatment. J Clin Pharmacol. (2018) 58:S164–79. doi: 10.1002/jcph.1121
14. Morgan RL, Preidis GA, Kashyap PC, Weizman AV, Sadeghirad B, Chang Y, et al. Probiotics reduce mortality and morbidity in preterm, low-birth-weight infants: a systematic review and network meta-analysis of randomized trials. Gastroenterology. (2020) 159:467–80. doi: 10.1053/j.gastro.2020.05.096
15. Underwood MA. Probiotics and the prevention of necrotizing enterocolitis. J Pediatr Surg. (2019) 54:405–12. doi: 10.1016/j.jpedsurg.2018.08.055
16. Nolan LS, Rimer JM, Good M. The role of human milk oligosaccharides and probiotics on the neonatal microbiome and risk of necrotizing enterocolitis: a narrative review. Nutrients. (2020) 12:3052. doi: 10.3390/nu12103052
17. Altobelli E, Angeletti PM, Verrotti A, Petrocelli R. The impact of human milk on necrotizing enterocolitis: a systematic review and meta-analysis. Nutrients. (2020) 12:1322. doi: 10.3390/nu12051322
18. Miller J, Tonkin E, Damarell RA, McPhee AJ, Suganuma M, Suganuma H, et al. A systematic review and meta-analysis of human milk feeding and morbidity in very low birth weight infants. Nutrients. (2018) 10:35. doi: 10.3390/nu10060707
19. Quigley M, Embleton ND, Mcguire W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev. (2018) 6:CD002971. doi: 10.1002/14651858.CD002971.pub4
20. Pammi M, Suresh G. Enteral lactoferrin supplementation for prevention of sepsis and necrotizing enterocolitis in preterm infants. Cochrane Database Syst Rev. (2020) 3:CD007137. doi: 10.1002/14651858.CD007137.pub6
21. Nolan LS, Parks OB, Good M. A review of the immunomodulating components of maternal breast milk and protection against necrotizing enterocolitis. Nutrients. (2020) 12:14. doi: 10.3390/nu12010014
22. Hackam DJ, Sodhi CP, Good M. New insights into necrotizing enterocolitis: from laboratory observation to personalized prevention and treatment. J Pediatr Surg. (2019) 54:398–404. doi: 10.1016/j.jpedsurg.2018.06.012
23. Alganabi M, Lee C, Bindi E, Li B, Pierro A. Recent advances in understanding necrotizing enterocolitis [version 1; referees: 2 approved]. F1000Research. (2019) 8:F1000. doi: 10.12688/f1000research.17228.1
24. Rose AT, Patel RM. A critical analysis of risk factors for necrotizing enterocolitis. Semin Fetal Neonatal Med. (2018) 23:374–9. doi: 10.1016/j.siny.2018.07.005
25. Sinclair TJ, Ye C, Chen Y, Zhang D, Li T, Ling XB, et al. Progressive metabolic dysfunction and nutritional variability precedes necrotizing enterocolitis. Nutrients. (2020) 12:1275. doi: 10.3390/nu12051275
26. Shah PS, Shah VS, Kelly LE. Arginine supplementation for prevention of necrotising enterocolitis in preterm infants. Cochrane Database Syst Rev. (2017) 2017:CD004339. doi: 10.1002/14651858.CD004339.pub4
27. Morgan J, Bombell S, Mcguire W. Early trophic feeding versus enteral fasting for very preterm or very low birth weight infants. Cochrane Database Syst Rev. (2013) 2013:14651858. doi: 10.1002/14651858.CD000504.pub4
Keywords: necrotizing enterocolitis, enteral nutrition, human milk, dysbiosis, probiotics
Citation: Campos-Martinez AM, Expósito-Herrera J, Gonzalez-Bolívar M, Fernández-Marin E and Uberos J (2022) Evaluation of Risk and Preventive Factors for Necrotizing Enterocolitis in Premature Newborns. A Systematic Review of the Literature. Front. Pediatr. 10:874976. doi: 10.3389/fped.2022.874976
Received: 13 February 2022; Accepted: 25 April 2022;
Published: 17 May 2022.
Edited by:
María L. Couce, Complejo Hospitalario Universitario de Santiago, SpainReviewed by:
María Gormaz, Agencia Valenciana de Salud, SpainCopyright © 2022 Campos-Martinez, Expósito-Herrera, Gonzalez-Bolívar, Fernández-Marin and Uberos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana M. Campos-Martinez, YW5hY2FtcG9zbWFyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.