 Mengyang He1†
Mengyang He1† Yuxiang Wan
Yuxiang Wan Jinchang Huang
Jinchang Huang Zhixin Zhang
Zhixin Zhang Wenquan Niu
Wenquan Niu- 1Graduate School, Beijing University of Chinese Medicine, Beijing, China
- 2Beijing University of Chinese Medicine Third Affiliated Hospital, Beijing, China
- 3Department of International Medical, China-Japan Friendship Hospital, Beijing, China
- 4Institute of Clinical Medical Sciences, China-Japan Friendship Hospital, Beijing, China
Objectives: The safety of recombinant human growth hormone (rhGH) treatment in childhood and the role of rhGH therapy in promoting tumorigenesis and progression have been the subject of debate for decades. We aimed to systematically assess the relationship between rhGH therapy in children and adolescents and clinical outcomes, including all-cause mortality, cancer mortality, cancer incidence, and risk of the second neoplasm.
Methods: Literature retrieval, study selection, and data extraction were completed independently and in duplicate. Effect-size estimates are expressed as standardized mortality ratios (SMRs), standardized incidence ratio (SIR), and relative risk (RR) with a 95% CI.
Results: Data from 24 articles, involving 254,776 persons, were meta-analyzed. Overall analyses revealed the association of rhGH therapy was not statistically significant with all-cause mortality (SMR = 1.28; 95% CI: 0.58–2.84; P = 0.547; I2 = 99.2%; Tau2 = 2.154) and cancer mortality (SMR = 2.59; 95% CI: 0.55–12.09; P = 0.228; I2 = 96.7%; Tau2 = 2.361) and also cancer incidence (SIR = 1.54; 95% CI: 0.68–3.47; P = 0.229; I2 = 97.5%; Tau2 = 2.287), yet statistical significance was observed for second neoplasm (RR = 1.77; 95% CI: 1.33–2.35; P = 0.001; I2 = 26.7%; Tau2 = 0.055). Differences in the geographic region, gender, treatment duration, mean rhGH dose, overall rhGH exposure dose, and initial disease accounted for heterogeneity in the subgroup analyses.
Conclusion: Our findings indicate that the rhGH therapy is not related to all-cause mortality and cancer mortality and cancer incidence, yet it seems to trigger a second tumor risk. Future prospective studies are needed to confirm our findings and answer the more challenging question regarding the optimal dose of rhGH therapy in children and adolescents.
Introduction
Since 1957, human growth hormone has been used to treat growth hormone deficiency and short stature, and it was supplanted by recombinant human growth hormone (rhGH) in 1985 (1). Initially, growth hormone was prescribed to patients with a severe growth hormone deficiency and its application is currently extended to children with short stature that is not primarily caused by an endogenous growth hormone deficiency, as well as to other scenarios, such as small for gestational age without catch-up growth or idiopathic short stature, Turner syndrome, short stature homeobox gene deficiency, Noonan syndrome, Prader–Willi syndrome, and growth failure associated with chronic renal insufficiency (2, 3). Generally, growth hormone therapy is considered to be safe, and serious adverse reactions rarely occur (4–6). However, in recent decades, the potential link between growth hormone therapy and tumor development or recurrence has gained increasing attention in clinical practice (7–11). In 2014, Deodati et al. (12) have undertaken a meta-analysis and reported that patients treated with growth hormone during childhood and adolescence had a significantly increased risk of all-cause mortality, cancer incidence, and second neoplasm after primary cancer. Contrastingly, in the to-date largest long-term follow-up study by Sävendahl et al., rhGH therapy was not associated with all-cause mortality in patients with isolated growth hormone deficiency or idiopathic short stature (13), and another large cohort study by Child et al. (2) also reported no significant association. In this context, the association between growth hormone therapy and all-cause mortality is still subject to an ongoing debate. With the accumulating publications afterward, there is a need to reexamine this association in a more comprehensive manner.
In an attempt to address this need and derive more reliable estimates, we performed an updated meta-analysis by pooling the results of both the prospective and retrospective cohorts in the medical literature to examine the association of rhGH therapy in children and adolescents with multiple clinical outcomes, including all-cause mortality, cancer mortality, cancer incidence, and risk of the second neoplasm. Another attempt was to identify the reasons for previous inconsistent reports, in other words, between-study heterogeneity.
Methods
The performance of the meta-analysis has adhered to the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (14). The PRISMA checklist is given in Supplementary Table 1.
This study is a meta-analysis of published studies; hence, ethical approval and informed consent are not needed.
Search Strategy
A literature search was conducted by reviewing the PubMed, MEDLINE, EMBASE, and Web of Science databases as of 6 November 2021. The following medical topic terms were used: (growth hormone or human growth hormone or somatotropin or somatropin or somatotrophin or GH or hGH or rhGH or rhGH or GH deficiency or growth hormone replacement therapy or GH replacement therapy) [Title] and (mortality or death or fatal or fatality or cancer or cancers or neoplasia or neoplasias or neoplasm or tumors or tumor or malignancy or malignancies or malignant neoplasm or CVD or cardiovascular disease) [Title/Abstract]. The reference lists of major retrieved articles were also manually searched to avoid potential missing hits.
The search process was independently conducted by two investigators (MH and XD) using the same medical topic terms. All the references retrieved were combined and duplicates were removed.
Inclusion/Exclusion Criteria
Our analysis was restricted to articles that met the following criteria: (1) study participants: women with BC; (2) endpoints: standardized mortality ratios (SMRs) or standardized incidence ratio (SIR) or relative risk (RR) with 95% CI; (3) study type: retrospective or prospective cohorts; (4) baseline exposure: growth hormone therapy; (5) follow-up rate: at least 70%; and (6) follow-up duration: ≥1 year. Articles were excluded if the involved study participants were adults or if they are case reports or case series, editorials, and narrative reviews.
Data Extraction
Two investigators (MH and XD) independently extracted data from each qualified article, including the first author, year of publication, the country where the study was conducted, sample size, study design, age at start rhGH therapy, rhGH dose, treatment duration, initial diagnosis, treatment duration, mean rhGH dose, overall exposure, effect estimation, and other confounding risk factors, if available. The divergence was resolved through a joint reevaluation of original articles, and if necessary, by a third author (WN).
Statistical Analyses
Data management was handled using the STATA software version 14.1 for Windows (Stata Corporation, College Station, Texas, USA). Effect-size estimates are expressed as SMR, SIR, or RR with 95% CI, where appropriate, and they are derived under the Mantel–Haenszel model. The difference between the two estimates was tested by the Z-test, as proposed by Altman and Bland (15). Pooled effect-size estimates were derived under a random-effects model, irrespective of the magnitude of between-study heterogeneity.
The inconsistency index (I2) statistic, which represents the percent of diversity that is due to heterogeneity rather than chance, is used to quantify the magnitude of heterogeneity that was derived from a random-effects Mantel–Haenszel model. The I2 >50% indicates the presence of significant heterogeneity and a higher percent corresponds to a higher degree of heterogeneity. Besides I2 statistic, another index, τ2 (Tau2), was used to explore the sensitivity of the results to different levels of between-study heterogeneity. To account for possible sources of between-study heterogeneity from clinical and methodological aspects, a panel of prespecified subgroup analyses were performed according to geographic region, published year, study design, age at start rhGH therapy, rhGH dose, treatment duration, initial diagnosis, mean rhGH dose, exposure, and follow-up interval, respectively.
The likelihood of publication bias was evaluated by both Begg's funnel plots and Egger's regression asymmetry tests at a significance level of 10%. The trim-and-fill method was also used to speculate the number of theoretically missing studies.
Results
Eligible Studies
A total of 3,199 articles were initially identified after searching predefined public datasets according to subject terms, of which 24 met our eligibility criteria, including 2,54,776 children and adolescents. The detailed selection process is shown in Figure 1. Among the eligible articles included, effect size estimates are expressed as SMR, SIR, and RR with 95% CIs.
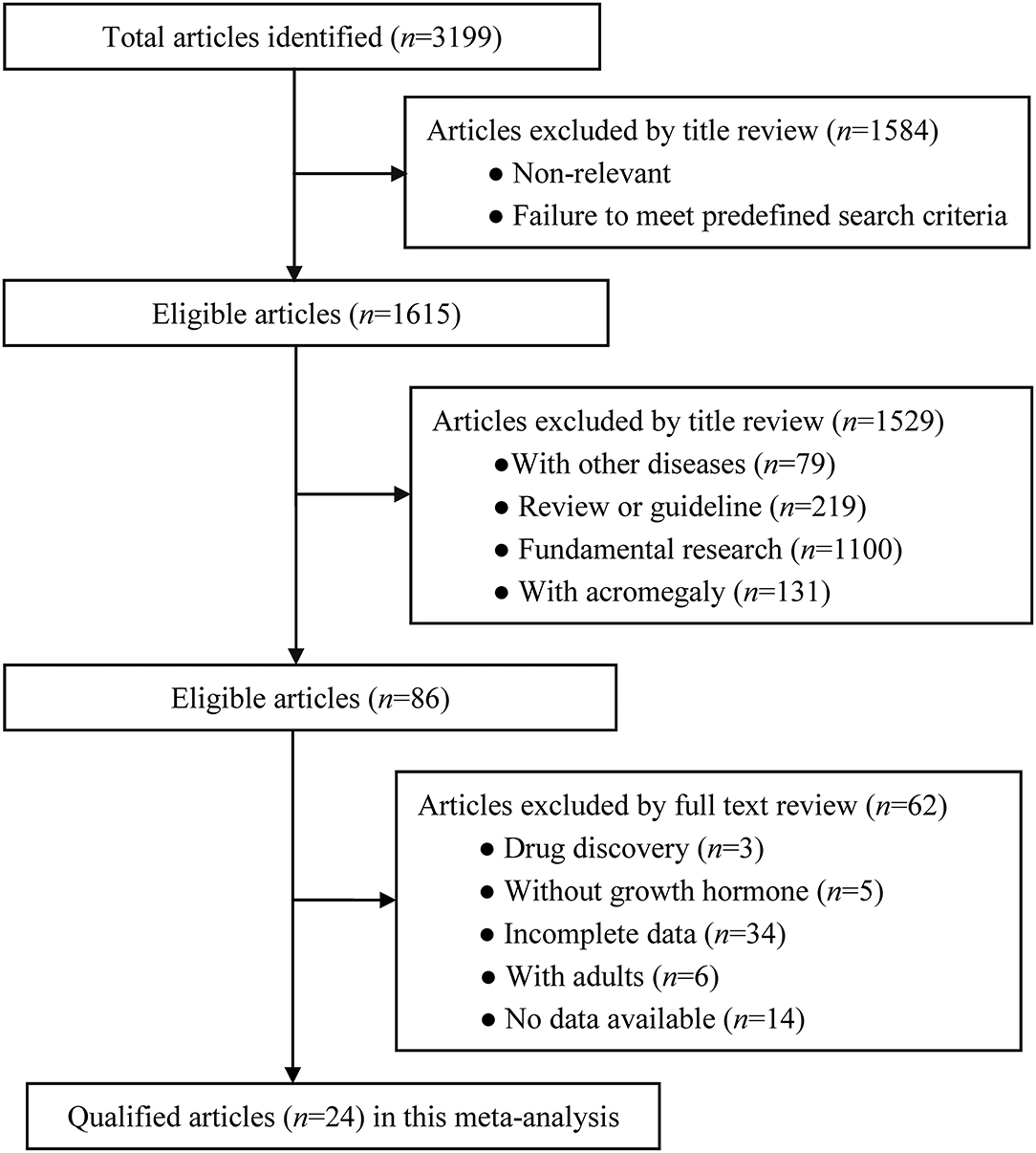
Figure 1. Flowchart of records retrieved, screened, and included in this meta-analysis.
Study Characteristics
Supplementary Table 2 shows the baseline characteristics of all the qualified articles in this meta-analysis. Of the 24 articles included, the outcome measure was all cause SMR in 7 articles (2, 13, 16–20), cancer SIR in 12 articles (1, 2, 5, 17, 19, 21–27), cancer SMR in 4 articles (16, 21, 25, 27), and second neoplasm in 8 articles (9, 10, 28–33). Only two articles (13, 16) presented data separately in boys and girls. Overall exposure of rhGH therapy was classified into four categories: <25, 25–50, 50–100, and ≥100 mg/kg.
Based on the previous medical history and physical health status, 3 articles (13, 16, 19) divided children into the low-risk, moderate-risk, and high-risk groups and 4 articles (5, 21, 22, 25) assorted children into the not-high-risk group.
Of the 24 qualified articles, two (13, 16) articles evaluated rhGH therapy duration <5 and ≥5 years. In total, eighteen articles were retrospective in design (5, 9, 10, 16, 18, 19, 21–24, 26–33) and 6 articles were prospective (1, 2, 13, 17, 20, 25). All the eligible articles were classified geographically into North America (5, 9, 10, 28), Asia (19), Europe (1, 13, 16–18, 21, 27, 29, 32, 33), and multinational (2, 20, 22–26, 30, 31).
Quality Assessment
Supplementary Table 3 shows the quality assessment of all the qualified articles by using the Newcastle–Ottawa Scale (NOS) tool for cohort studies. The average total score was 7.46 (range: 7–8), with an SD of 0.5.
Overall Analyses
After pooling the results of all the qualified articles, there was no statistical significance between rhGH therapy in childhood and all-cause mortality (SMR = 1.28; 95% CI: 0.58–2.84; P = 0.547; I2 = 99.2%; Tau2 = 2.154), cancer mortality (SMR = 2.59; 95% CI: 0.55–12.09; P = 0.228; I2 = 96.7%; Tau2 = 2.361), and standardized incidence ratio for cancer (SIR = 1.54; 95% CI: 0.68–3.47; P = 0.229; I2 = 97.5%; Tau2 = 2.287). In contrast, there was a statistically significant association with the development of second neoplasm (RR = 1.77; 95% CI: 1.33–2.35; P = 0.001; I2 = 26.7%; Tau2 = 0.055) (Figure 2).
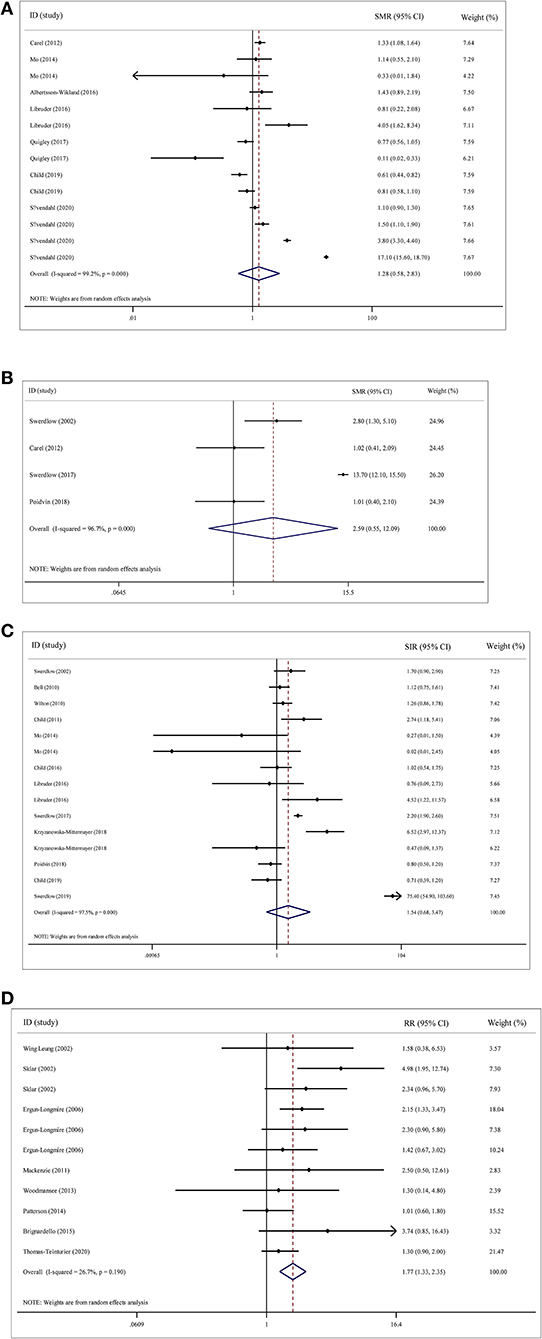
Figure 2. Overall analyses on the association of recombinant human growth hormone (rhGH) therapy with mortality and cancer risk. (A) rhGH therapy and all-cause mortality. (B) rhGH therapy and cancer mortality. (C) rhGH therapy and cancer incidence. (D) rhGH therapy and second neoplasm.
Cumulative and Influential Analyses
In the cumulative analyses, included studies got completely similar conclusions consistently and trends tended to stabilize. The influential analyses revealed no significant impact of any single study on overall effect-size estimates.
Publication Bias
Figure 3 shows Begg's funnel plot and Egger's test for assessing publication bias of rhGH therapy with all-cause mortality, cancer mortality, the standardized incidence of cancer, and the occurrence of the second neoplasm.
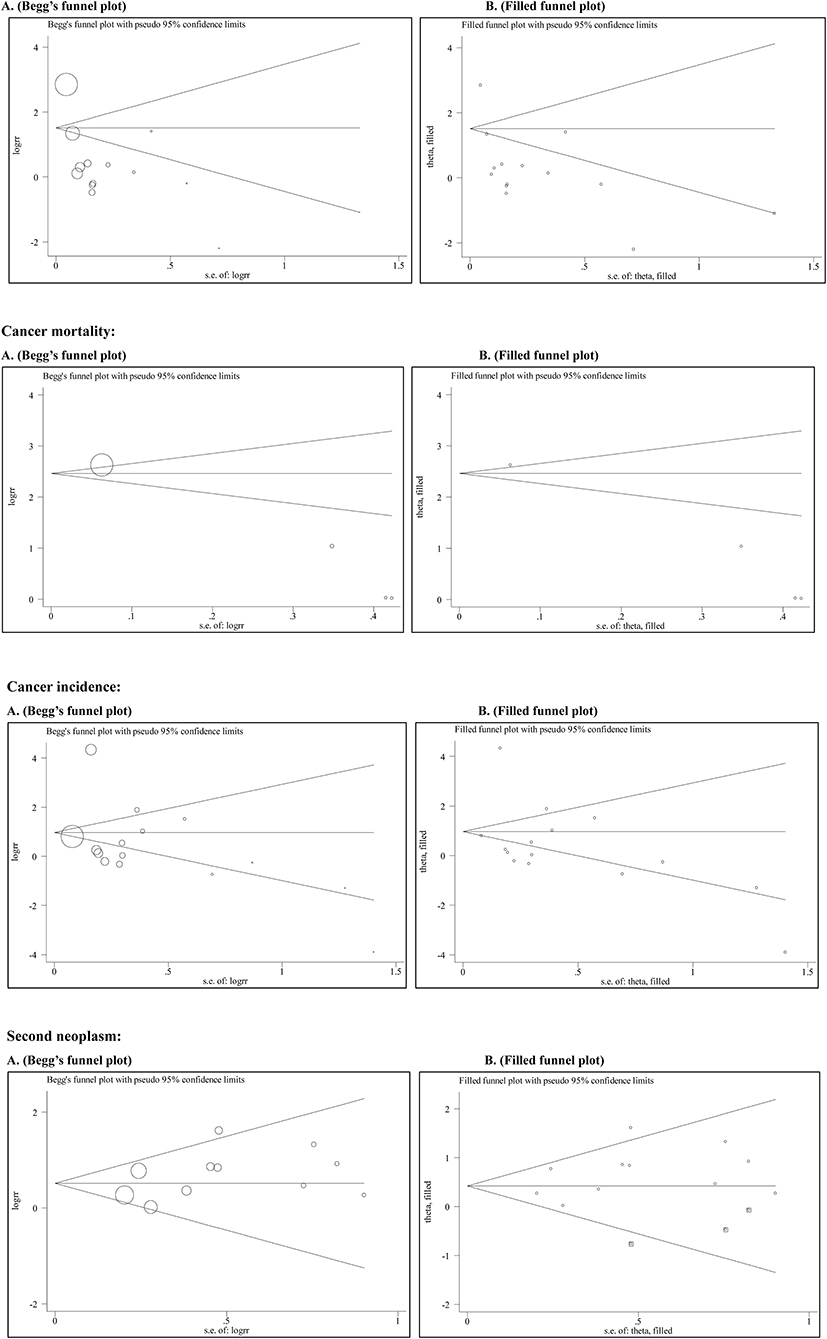
Figure 3. The Begg's and filled funnel plots for the association of rhGH therapy with mortality and cancer risk. All-cause mortality: (A) Begg's funnel plot, (B) Filled funnel plot. Cancer mortality: (A) Begg's funnel plot, (B) Filled funnel plot. Cancer incidence: (A) Begg's funnel plot, (B) Filled funnel plot. Second neoplasm: (A) Begg's funnel plot, (B) Filled funnel plot.
Begg's funnel plots seemed symmetrical. As reflected by Egger's test, there was a low likelihood of publication bias for standardized incidence of cancer (P = 0.525) and occurrence of second neoplasm (P = 0.167). Further investigations using the “trim and fill” method showed that 3 theoretically missing studies were required to make Begg's funnel plot symmetrical for the occurrence of the second neoplasm. However, no study was required in theory for standardized incidence of cancer.
There was statistical evidence of asymmetry by using Eggers's tests in all-cause mortality (P = 0.015) and cancer mortality (P = 0.008). The “trim and fill” method did not produce any derivations from the original estimates.
Subgroup Analyses
A series of prespecified subgroup analyses were conducted to account for possible sources of between-study heterogeneity for rhGH therapy with the all-cause mortality, cancer mortality, the standardized incidence of cancer, and the occurrence of second neoplasm (Table 1).
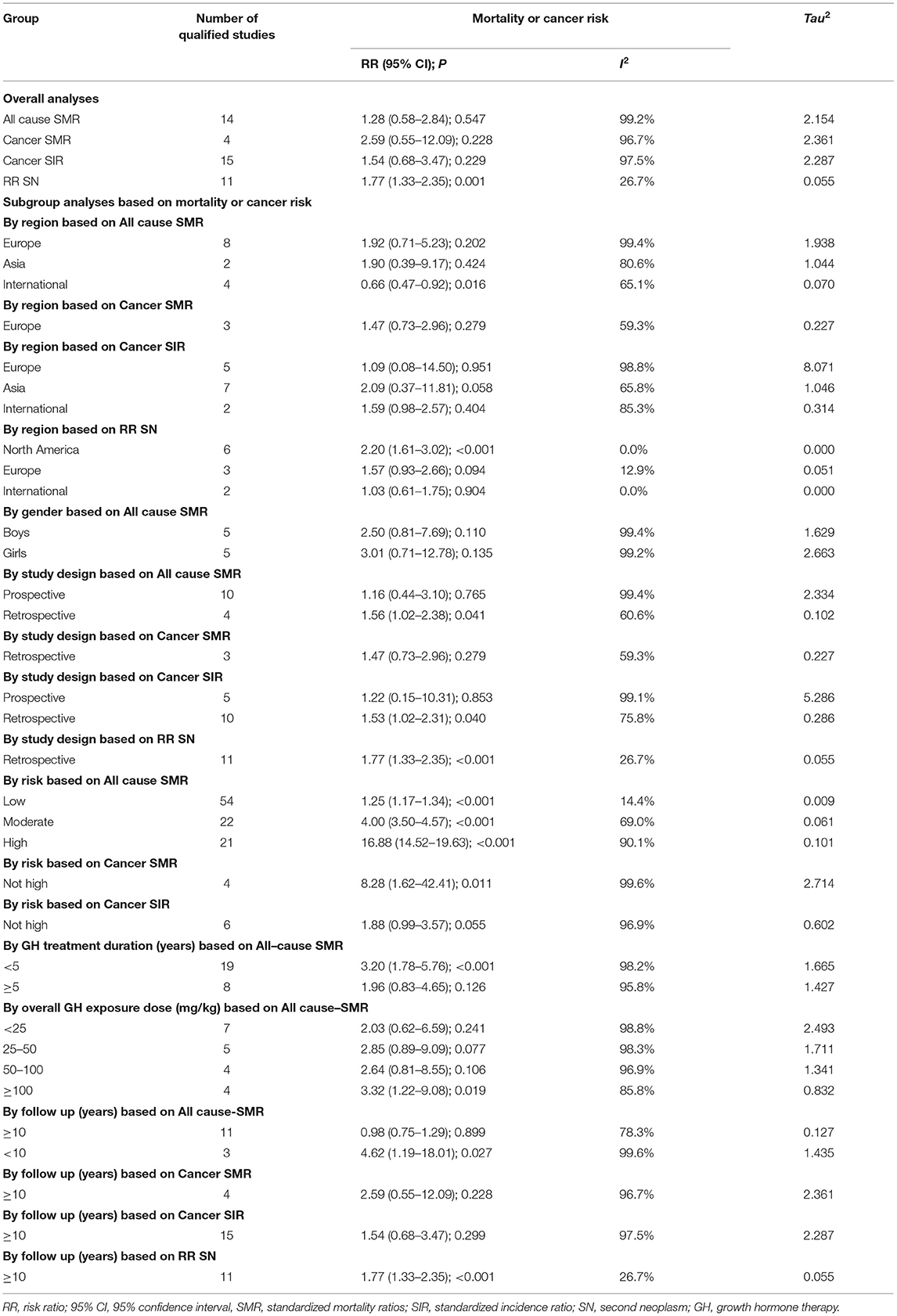
Table 1. Overall and subgroup analyses on the association of recombinant human growth hormone therapy with mortality and cancer risk.
By geographic regions based on the all-cause SMR, the association between pediatric somatropin treatment and the all-cause mortality was not statistically significant in Europe (SMR = 1.92, 95% CI: 0.71–5.23, P = 0.202; I2 = 99.4%; Tau2 = 1.938) and Asia (SMR = 1.90, 95% CI: 0.39–9.17, P = 0.424; I2 = 80.6%; Tau2 = 1.044) and also no significance was detected between rhGH therapy and cancer mortality in children in Europe (SMR = 1.47, 95% CI: 0.73–2.96, P = 0.279; I2 = 59.3%; Tau2 = 0.227) based on the geographical areas of cancer SMR. Based on cancer SIR by geographic regions, the association was nonsignificant between rhGH therapy and standard cancer incidence in both Europe (SIR = 1.09, 95% CI: 0.08–14.50, P = 0.951; I2 = 98.8%; Tau2 = 8.071) and Asia (SIR = 2.09, 95% CI: 0.37–11.81, P = 0.058; I2 = 65.8%; Tau2 = 1.046). The association between childhood rhGH therapy and second neoplasm was statistically significant in North America (RR = 2.20, 95% CI: 1.61–3.02, P < 0.001; I2 = 0.00%; Tau2 = 0.000). However, the statistical significance was not demonstrated in Europe (RR = 1.57, 95% CI: 0.93–2.66, P = 0.094; I2 = 12.9%; Tau2 = 0.051).
By gender based on the all-cause SMR, the association between rhGH therapy and all-cause mortality was not statistically significant in either boys (SMR = 2.50, 95% CI: 0.81–7.69, P = 0.110; I2 = 99.4%; Tau2 = 1.629) or girls (SMR = 3.01, 95% CI: 0.71–12.78, P = 0.135; I2 = 99.2%; Tau2 = 2.663).
By study design based on the all-cause SMR, the association between rhGH therapy and all-cause mortality in children was not statistically significant in prospective cohorts (SMR = 1.16, 95% CI: 0.44–3.10, P = 0.765; I2 = 99.4%; Tau2 = 1.629) and in retrospective cohorts, the SMR for rhGH therapy and all-cause mortality was 1.56 (95% CI: 1.02–2.38, P = 0.041; I2 = 60.6%; Tau2 = 0.102). Based on the study type of cancer SMR, there was no statistical significance between growth hormone therapy and tumor mortality in retrospective cohorts (SMR = 1.47, 95% CI: 0.73–2.96, P = 0.279; I2 = 59.3%; Tau2 = 0.227). Based on the study design of cancer SIR, in prospective cohorts, there was no statistical significance between rhGH therapy and the standard incidence of tumor (SIR =1.22, 95% CI: 0.15–10.31, P = 0.853; I2 = 99.1%; Tau2 = 5.286), yet significance was attained in retrospective cohorts (SIR = 1.53, 95% CI: 1.02–2.31, P = 0.040; I2 = 75.8%; Tau2 = 0.286). By the study design based on the second neoplasm, the association between rhGH therapy and second neoplasm reached statistical significance (RR = 1.77, 95% CI: 1.33–2.35, P < 0.001; I2 = 26.7%; Tau2 = 0.055).
By risk based on all-cause SMR, in children with low risk (SMR = 1.25, 95% CI: 1.17–1.34, P < 0.001; I2 = 14.4%; Tau2 = 0.009), moderate risk (SMR = 4.00, 95% CI: 3.50–4.57, P < 0.001; I2 = 69.0%; Tau2 = 0.061), or high risk (SMR = 16.88, 95% CI: 14.52–19.63, P < 0.001; I2 = 0.1%; Tau2 = 0.101), the relationship between rhGH therapy and all-cause mortality was statistically significant. Based on the risk of cancer SMR, there was statistical significance between rhGH therapy and cancer mortality in children with not-high risk (SMR = 8.28, 95% CI: 1.62–42.41, P = 0.011; I2 = 99.6%; Tau2 = 2.714). In addition, rhGH therapy did not significantly affect standard tumor incidence among children at not-high risk based on the risk of cancer SIR (SIR = 1.88, 95% CI: 0.99–3.57, P = 0.055; I2 = 96.9%; Tau2 = 0.602).
By duration of rhGH therapy based on the all-cause SMR, the association between rhGH therapy and all-cause mortality was not statistically significant when treatment duration was ≥5 years (SMR = 1.96, 95% CI: 0.83–4.65, P = 0.126; I2 = 95.8%; Tau2 = 1.427). However, when the treatment time was <5 years (SMR =3.20, 95% CI: 1.78–5.76, P < 0.001; I2 = 98.2%; Tau2 = 1.665), the association was significant.
By overall rhGH exposure dose based on all-cause SMR, the association between rhGH therapy and all-cause mortality was not statistically significant when rhGH exposure during childhood was <25 mg/kg (SMR = 2.03, 95% CI: 0.62–6.59, P = 0.241; I2 = 98.8%; Tau2 = 2.493), 25–50 mg/kg (SMR = 2.85, 95% CI: 0.89–9.09, P = 0.077; I2 = 98.3%; Tau2 = 1.711), and 50–100 mg/kg (SMR = 2.64, 95% CI: 0.81–8.55, P = 0.106; I2 = 96.9%; Tau2 = 1.341), whereas the association was statistically significant when total rhGH exposure was ≥100 mg/kg (SMR = 3.32, 95% CI: 1.22–9.08, P = 0.019; I2 = 85.8%; Tau2 = 0.832).
By follow-up period based on all-cause SMR, there was no statistically significant association between rhGH therapy and all-cause mortality when the follow-up period ≥10 years (SMR = 0.98, 95% CI: 0.75–1.29, P = 0.899; I2 = 78.3%; Tau2 = 0.127). The association between rhGH therapy and all-cause mortality was statistically significant in studies with follow-up duration <10 years (SMR = 4.62, 95% CI: 1.19–18.01, P = 0.027; I2 = 99.6%; Tau2 = 1.435). The association between rhGH therapy and cancer mortality was not statistically significant in studies with follow-up duration ≥10 years (SMR = 2.59, 95% CI: 0.55–12.09, P = 0.228; I2 = 96.7%; Tau2 = 2.361) based on cancer SMR. Based on cancer SIR of follow-up, there was no statistically significant association between rhGH therapy and standard cancer incidence at follow-up times ≥10 years (SIR =1.54, 95% CI: 0.68–3.47, P < 0.001; I2 = 97.5%; Tau2 = 2.287). Nevertheless, there was a statistically significant relationship between second neoplasm and rhGH therapy (RR = 1.77, 95% CI: 1.33–2.35, P < 0.001; I2 = 26.7%; Tau2 = 0.055).
Discussion
To the best of our knowledge, this is, thus far the most comprehensive meta-analysis that has examined the association between rhGH therapy during childhood and multiple clinical outcomes including the all-cause mortality, cancer mortality, standard cancer incidence, and second neoplasm. Our key findings suggested that rhGH therapy in childhood had no deleterious effects on all-cause mortality, cancer mortality, and standard cancer incidence. In contrast, rhGH therapy was a risk factor for the development of the second neoplasm. Furthermore, our analyses suggested that differences in the geographic region, gender, treatment duration, mean rhGH dose, overall rhGH exposure dose, and initial disease accounted for heterogeneity. Our findings highlight the relative safety of growth hormone use in childhood and provide high-quality evidence for pediatrics, particularly for these conditions requiring rhGH therapy.
Extending the findings of previous individual studies that assessed only one or two clinical outcomes after rhGH therapy, we, in this meta-analysis, comprehensively evaluated all the possible outcomes in both the overall analyses and subgroup analyses. It is worth noting that all-cause mortality and cancer incidence were significantly higher than expected in the low- and intermediate-risk groups. Although only 2 articles were involved in the analysis of total exposure to rhGH in children, the all-cause mortality rate was significantly higher than expected when the total exposure dose was over 100 mg/kg based on the results of the analysis of the overall exposure dose. However, this dose needs to be determined by future studies. Moreover, we also interestingly noticed that all-cause mortality was significantly lower than expected for both boys and girls. Although the exact mechanisms behind these positive findings are not fully understood, we agree that further well-designed, long-term studies are warranted to further enrich our understanding of the clinical implication of rhGH therapy in childhood in future mortality risk in adulthood.
The current meta-analysis is based on the previous meta-analysis conducted by Deodati et al. (12) by pooling the results of 12 studies, who found no significant increase in the malignant tumor SMRs, yet overall cancer SIRs (2.74; 95% CI: 1.18–4.41) and RRs of second tumors (1.99; 95% CI: 1.28–3.08) were significantly increased. In the present meta-analysis, by contrast, we found that all-cause mortality and malignancy incidence were significantly lower than expected, that is, rhGH therapy was not a risk factor for all-cause mortality and malignancy incidence. The reasons for the conflicting observations between the meta-analysis by Deodati et al. (12) and this meta-analysis are mainly because of the power to detect statistical significance, as we incorporated the results from 24 articles.
Our finding that no significant association was found between the dose of rhGH and mortality and cancer incidence makes causality less likely. However, some studies have reported an increased incidence of bone cancer and bladder cancer in patients treated with rhGH and in patients with Hodgkin lymphoma (2, 25). Nonetheless in this meta-analysis, we did not conduct relevant subgroup analysis due to a lack of data on the initial disease of patients with detailed types of cancers. In addition, we believe that rhGH therapy should be carried out with caution in high-risk patients and that the start of rhGH therapy should be carefully discussed (34).
Available evidence suggests an increased risk of secondary tumors in rhGH recipients. Growth hormone is potent mitosis and anti-apoptotic hormone, and increased activity of the growth hormone/IGF-I axis is associated with an increased risk of cancer (35). Therefore, with the use of growth hormone therapy, the researchers' vigilance against the potential cancer risk accompanied this treatment from the beginning. Animal experiments showed that in spontaneous pygmy rats lacking rhGH, the administration of the carcinogen N-methyl-N-nitrosourea did not induce breast tumors. However, the tumors were developed in GH-treated rats (36). Moreover, after stopping hormone replacement, almost all the tumors have completely degenerated in animal models of rhGH receptor knockout mice hybridizing with Tag mice prone to prostate tumors, and similar findings were described by other investigators (35, 37). High IGF-1 or high growth hormone levels may induce messenger RNA alterations or other molecular changes and angiogenesis and inhibit apoptosis. This may further stimulate the carcinogenic potential that already exists (33, 38, 39). Molecular signaling pathways that affect cell proliferation, differentiation, and survival are regulated by the GH-IGF-1 axis. The carcinogenic process interacts with GH-IGF-1 signaling pathways, employs these physiological signaling pathways, and converts them into abnormal signaling pathways (33, 38).
Generally, the findings of this meta-analysis are reassuring, but some biases, confounding factors, and weaknesses limit the value and interpretation of all data reported to date. Detailed information on dosage, duration of treatment, and primary disease in children need more literature support and although the relevant subgroup analysis was conducted in this study, the number of relevant articles was relatively small. Future prospective studies are also needed to confirm these results and answer more difficult questions about the appropriate period to start GH therapy after achieving complete remission, and how to deal with children with “chronic” low-grade tumor diseases and growth hormone deficiency (GHD). In addition, more research is required on the optimal dosage of rhGH therapy (34).
Conclusion
Our findings indicate that rhGH therapy is not related to all-cause mortality, cancer mortality, and cancer incidence, yet it seems to trigger a second tumor risk. The long-term safety of growth hormone therapy still deserves more attention as mortality from certain causes is increasing, and the need for long-term monitoring remains essential.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
JH, ZZ, and WN: conceived and designed the experiments. MH, XW, and ZZ: performed the experiments. MH, XD, and JH: analyzed the data and contributed materials/analysis tools. MH, XW, JH, and WN: wrote the article. All the authors read and approved the final manuscript before submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.866295/full#supplementary-material
References
1. Swerdlow AJ, Cooke R, Beckers D, Butler G, Carel JC, Cianfarani S, et al. Risk of meningioma in European patients treated with growth hormone in childhood: results from the SAGhE cohort. J Clin Endocrinol Metab. (2019) 104:658–64. doi: 10.1210/jc.2018-01133
2. Child CJ, Zimmermann AG, Chrousos GP, Cummings E, Deal CL, Hasegawa T, et al. Safety outcomes during pediatric GH therapy: final results from the prospective GeNeSIS observational program. J Clin Endocrinol Metab. (2019) 104:379–89. doi: 10.1210/jc.2018-01189
3. Tidblad A, Bottai M, Kieler H, Albertsson-Wikland K, Sävendahl L. Association of childhood growth hormone treatment with long-term cardiovascular morbidity. JAMA Pediatr. (2021) 175:e205199. doi: 10.1001/jamapediatrics.2020.5199
4. Clayton PE, Cowell CT. Safety issues in children and adolescents during growth hormone therapy–a review. Growth Horm IGF Res. (2000) 10:306–17. doi: 10.1054/ghir.2000.0175
5. Bell J, Parker KL, Swinford RD, Hoffman AR, Maneatis T, Lippe B. Long-term safety of recombinant human growth hormone in children. J Clin Endocrinol Metab. (2010) 95:167–77. doi: 10.1210/jc.2009-0178
6. Allen DB, Backeljauw P, Bidlingmaier M, Biller BM, Boguszewski M, Burman P, et al. GH safety workshop position paper: a critical appraisal of recombinant human GH therapy in children and adults. Eur J Endocrinol. (2016) 174:P1–9. doi: 10.1530/EJE-15-0873
7. (1988). Leukaemia in patients treated with growth hormone. Lancet. 1:1159–60. doi: 10.1016/S0140-6736(88)91968-X
8. Allen DB, Rundle AC, Graves DA, Blethen SL. Risk of leukemia in children treated with human growth hormone: review and reanalysis. J Pediatr. (1997) 131:S32–36. doi: 10.1016/S0022-3476(97)70008-8
9. Sklar CA, Mertens AC, Mitby P, Occhiogrosso G, Qin J, Heller G, et al. Risk of disease recurrence and second neoplasms in survivors of childhood cancer treated with growth hormone: a report from the Childhood Cancer Survivor Study. J Clin Endocrinol Metab. (2002) 87:3136–41. doi: 10.1210/jcem.87.7.8606
10. Ergun-Longmire B, Mertens AC, Mitby P, Qin J, Heller G, Shi W, et al. Growth hormone treatment and risk of second neoplasms in the childhood cancer survivor. J Clin Endocrinol Metab. (2006) 91:3494–8. doi: 10.1210/jc.2006-0656
11. Raman S, Grimberg A, Waguespack SG, Miller BS, Sklar CA, Meacham LR, et al. Risk of neoplasia in pediatric patients receiving growth hormone therapy—a report from the pediatric endocrine society drug and therapeutics committee. J Clin Endocrinol Metab. (2015) 100:2192–203. doi: 10.1210/jc.2015-1002
12. Deodati A, Ferroli BB, Cianfarani S. Association between growth hormone therapy and mortality, cancer and cardiovascular risk: systematic review and meta-analysis. Growth Horm IGF Res. (2014) 24:105–11. doi: 10.1016/j.ghir.2014.02.001
13. Sävendahl L, Cooke R, Tidblad A, Beckers D, Butler G, Cianfarani S, et al. Long-term mortality after childhood growth hormone treatment: the SAGhE cohort study. Lancet Diabetes Endocrinol. (2020) 8:683–92. doi: 10.1016/S2213-8587(20)30163-7
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
15. Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. (2003) 326:219. doi: 10.1136/bmj.326.7382.219
16. Carel JC, Ecosse E, Landier F, Meguellati-Hakkas D, Kaguelidou F, Rey G, et al. Long-term mortality after recombinant growth hormone treatment for isolated growth hormone deficiency or childhood short stature: preliminary report of the French SAGhE study. J Clin Endocrinol Metab. (2012) 97:416–25. doi: 10.1210/jc.2011-1995
17. Mo D, Hardin DS, Erfurth EM, Melmed S. Adult mortality or morbidity is not increased in childhood-onset growth hormone deficient patients who received pediatric GH treatment: an analysis of the Hypopituitary Control and Complications Study (HypoCCS). Pituitary. (2014) 17:477–85. doi: 10.1007/s11102-013-0529-6
18. Albertsson-Wikland K, Mårtensson A, Sävendahl L, Niklasson A, Bang P, Dahlgren J, et al. Mortality is not increased in recombinant human growth hormone-treated patients when adjusting for birth characteristics. J Clin Endocrinol Metab. (2016) 101:2149–59. doi: 10.1210/jc.2015-3951
19. Libruder C, Blumenfeld O, Dichtiar R, Laron Z, Zadik Z, Shohat T, et al. Mortality and cancer incidence among patients treated with recombinant growth hormone during childhood in Israel. Clin Endocrinol (Oxf). (2016) 85:813–8. doi: 10.1111/cen.13131
20. Quigley CA, Child CJ, Zimmermann AG, Rosenfeld RG, Robison LL, Blum WF. Mortality in children receiving growth hormone treatment of growth disorders: data from the genetics and neuroendocrinology of short stature international study. J Clin Endocrinol Metab. (2017) 102:3195–205. doi: 10.1210/jc.2017-00214
21. Swerdlow AJ, Higgins CD, Adlard P, Preece MA. Risk of cancer in patients treated with human pituitary growth hormone in the UK, 1959-85: a cohort study. Lancet. (2002) 360:273–7. doi: 10.1016/S0140-6736(02)09519-3
22. Wilton P, Mattsson AF, Darendeliler F. Growth hormone treatment in children is not associated with an increase in the incidence of cancer: experience from KIGS (Pfizer International Growth Database). J Pediatr. (2010) 157:265–70. doi: 10.1016/j.jpeds.2010.02.028
23. Child CJ, Zimmermann AG, Woodmansee WW, Green DM, Li JJ, Jung H, et al. Assessment of primary cancers in GH-treated adult hypopituitary patients: an analysis from the Hypopituitary Control and Complications Study. Eur J Endocrinol. (2011) 165:217–23. doi: 10.1530/EJE-11-0286
24. Child CJ, Zimmermann AG, Jia N, Robison LL, Brämswig JH, Blum WF. Assessment of primary cancer incidence in growth hormone-treated children: comparison of a multinational prospective observational study with population databases. Horm Res Paediatr. (2016) 85:198–206. doi: 10.1159/000444124
25. Swerdlow AJ, Cooke R, Beckers D, Borgstrom B, Butler G, Carel JC, et al. Cancer risks in patients treated with growth hormone in childhood: the SAGhE European Cohort Study. J Clin Endocrinol Metab. (2017) 102:1661–72. doi: 10.1210/jc.2016-2046
26. Krzyzanowska-Mittermayer K, Mattsson AF, Maiter D, Feldt-Rasmussen U, Camacho-Hübner C, Luger A, et al. New neoplasm during GH replacement in adults with pituitary deficiency following malignancy: a KIMS analysis. J Clin Endocrinol Metab. (2018) 103:523–31. doi: 10.1210/jc.2017-01899
27. Poidvin A, Carel JC, Ecosse E, Levy D, Michon J, Coste J. Increased risk of bone tumors after growth hormone treatment in childhood: a population-based cohort study in France. Cancer Med. (2018) 7:3465–73. doi: 10.1002/cam4.1602
28. Leung W, Rose SR, Zhou Y, Hancock ML, Burstein S, Schriock EA, et al. Outcomes of growth hormone replacement therapy in survivors of childhood acute lymphoblastic leukemia. J Clin Oncol. (2002) 20:2959–64. doi: 10.1200/JCO.2002.09.142
29. Mackenzie S, Craven T, Gattamaneni HR, Swindell R, Shalet SM, Brabant G. Long-term safety of growth hormone replacement after CNS irradiation. J Clin Endocrinol Metab. (2011) 96:2756–61. doi: 10.1210/jc.2011-0112
30. Woodmansee WW, Zimmermann AG, Child CJ, Rong Q, Erfurth EM, Beck-Peccoz P, et al. Incidence of second neoplasm in childhood cancer survivors treated with GH: an analysis of GeNeSIS and HypoCCS. Eur J Endocrinol. (2013) 168:565–73. doi: 10.1530/EJE-12-0967
31. Patterson BC, Chen Y, Sklar CA, Neglia J, Yasui Y, Mertens A, et al. Growth hormone exposure as a risk factor for the development of subsequent neoplasms of the central nervous system: a report from the childhood cancer survivor study. J Clin Endocrinol Metab. (2014) 99:2030–7. doi: 10.1210/jc.2013-4159
32. Brignardello E, Felicetti F, Castiglione A, Fortunati N, Matarazzo P, Biasin E, et al. GH replacement therapy and second neoplasms in adult survivors of childhood cancer: a retrospective study from a single institution. J Endocrinol Invest. (2015) 38:171–6. doi: 10.1007/s40618-014-0179-1
33. Thomas-Teinturier C, Oliver-Petit I, Pacquement H, Fresneau B, Allodji RS, Veres C, et al. Influence of growth hormone therapy on the occurrence of a second neoplasm in survivors of childhood cancer. Eur J Endocrinol. (2020) 183:471–80. doi: 10.1530/EJE-20-0369
34. van Santen HM. Safety of GH after treatment for childhood cancer. Eur J Endocrinol. (2020) 183:C15–c18. doi: 10.1530/EJE-20-0965
35. Tidblad A. The history, physiology and treatment safety of growth hormone. Acta Paediatr. (2021) 111:215–24 doi: 10.1111/apa.15948
36. Shen Q, Lantvit DD, Lin Q, Li Y, Christov K, Wang Z, et al. Advanced rat mammary cancers are growth hormone dependent. Endocrinology. (2007) 148:4536–44. doi: 10.1210/en.2007-0513
37. Wang Z, Prins GS, Coschigano KT, Kopchick JJ, Green JE, Ray VH, et al. Disruption of growth hormone signaling retards early stages of prostate carcinogenesis in the C3(1)/T antigen mouse. Endocrinology. (2005) 146:5188–96. doi: 10.1210/en.2005-0607
38. Brunet-Dunand SE, Vouyovitch C, Araneda S, Pandey V, Vidal LJ, Print C, et al. Autocrine human growth hormone promotes tumor angiogenesis in mammary carcinoma. Endocrinology. (2009) 150:1341–52. doi: 10.1210/en.2008-0608
Keywords: mortality, children, cancer, medication safety, rhGH
Citation: He M, Deng X, Wang X, Wan Y, Huang J, Zhang Z and Niu W (2022) Association Between Recombinant Growth Hormone Therapy and All-Cause Mortality and Cancer Risk in Childhood: Systematic Review and Meta-Analysis. Front. Pediatr. 10:866295. doi: 10.3389/fped.2022.866295
Received: 31 January 2022; Accepted: 07 March 2022;
Published: 22 April 2022.
Edited by:
M. Savage, Queen Mary University of London, United KingdomReviewed by:
Lorenzo Iughetti, University of Modena and Reggio Emilia, ItalyPasquale Dolce, University of Naples Federico II, Italy
Copyright © 2022 He, Deng, Wang, Wan, Huang, Zhang and Niu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenquan Niu, bml1d2VucXVhbl9zaGNuQDE2My5jb20=; Zhixin Zhang, emhhbmd6aGl4aW4wMzJAMTYzLmNvbQ==; Jinchang Huang, enJ5aGh1YW5nQDE2My5jb20=
†These authors share first authorship