
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 24 February 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.836708
 Anne-Margaux Collignon1,2,3,4*
Anne-Margaux Collignon1,2,3,4* Jean-Noël Vergnes4,5
Jean-Noël Vergnes4,5 Alice Germa2,3,6Sylvie Azogui2,3,7
Alice Germa2,3,6Sylvie Azogui2,3,7 Sophie Breinig5,8Clémence Hollande9
Sophie Breinig5,8Clémence Hollande9 Anne-Laure Bonnet1,2,3Cathy Nabet4,5
Anne-Laure Bonnet1,2,3Cathy Nabet4,5Background: Developmental Defects of Enamel (DDE) is a pathology of the teeth that can greatly alter the quality of life of patients (hypersensitivity, esthetic issues, loss of function, etc.). The acquired DDE may occur as a result of a wide range of acquired etiological factors and his prevalence of this pathology may reach up to 89.9%. The main objective of this research was to identify and analyze, in current literature, the factors related to acquired DDE, in order to propose a general theory about the mechanisms involved.
Methods: The search of the primary literature was conducted until [December 31, 2021]. Our search strategy uses the Pubmed/MEDLINE database and was structured around 3 terms [“Development,” “Defect,” and “Enamel”]. To be included, references had to be primary studies, written in English. Exclusion criteria were reviews, in vitro, animal, genetic or archeology studies, and studies focused on clinical management of DDE. One hundred and twenty three articles were included in this scoping review: 4 Randomized clinical trials, 1 letter, 5 cases reports, 2 fundamentals studies, and 111 observational studies (33 Cross-sectional studies, 68 Cohort study and 10 Case-control study). The quality of evidence was assessed using the PEDro scale for clinical trials, the Newcastle-Ottawa scale for observational studies, and a published tool to assess the quality of case reports and case series.
Results: A scoping review of the literature identified 114 factors potentially involved in acquired DDE. The most frequently encountered pathologies are those causing a disorder of calcium homeostasis or a perturbation of the ARNT pathway in mother or child. The link between the ARNT pathway and metabolism deficiency in uncertain and needs to be defined. Also, the implication of this mechanism in tissue impairment is still unclear and needs to be explored.
Conclusions: By identifying and grouping the risk factors cited in the literature, this taxonomy and the hypotheses related to the mechanism allow health practitioners to adopt behaviors that limit the risk of developing aDDE and to set up a prevention of dental pathology. In addition, by reviewing the current literature, this work provides guidance for basic research, clinical studies, and literature searches.
Developmental Defects of Enamel (DDE) are defined as disturbances in hard tissue matrices and their mineralization that arise during odontogenesis (1) (from 16 weeks of gestation to the age of 5). This set of non-carious lesions can affect both primary and permanent teeth and negatively impacts the health of children. Short to long-term potential adverse effects may occur, such as tooth sensitivity, carious lesions, low self-esteem or stigma experiences, and social costs including children's absence from school (2).
Prevalence of acquired DDE may reach up to 89.9% (3). A large body of literature exists about risk factors for DDE; however, DDE have been studied in silos rather than comprehensively, which has led to a rather poor understanding of pathogenic mechanisms involved in their occurrence.
Factors that may interfere with the metabolic process of enamel formation and lead to DDE are traditionally dichotomized as hereditary or acquired. A complete meta-analysis on the hereditary factors has been recently published (4). Acquired DDE (aDDE) occur when the disturbance is sufficient to alter the regular growth pattern of the enamel tissue. Currently, the etiology is still unclear, perhaps because the literature is extensive and sometimes inconsistent.
The main objective of this research was to identify and analyze the factors related to acquired DDE, in order to propose a general theory about the mechanisms involved. To achieve this objective, we designed a research framework based on the scoping review methodology, synthesizing current scientific knowledge on the subject. This work aims to help improve prevention, treatment, and multidisciplinary management strategies.
To combine the exploratory and systematic nature of our research, we followed the Arksey and O'Malley methodological framework for scoping reviews (5), and completed the PRISMA for Scoping review guidelines (see Supplementary Material 1). The search of the primary literature was conducted until [December 31, 2021]. We focused our search strategy on the Pubmed/MEDLINE database, considering it would include all the major factors identified by biomedical research. We structured our search strategy around 3 terms [“Development,” “Defect,” and “Enamel”], allowing for explosion search, and using the Boolean operator AND (see details in Supplementary Material 2). We did not use terms involving any risk factor for DDE, so as to scan the database broadly without preconceived notions about the factors we were looking for. The screening process was performed by one author (AMC).
To be included, references had to be primary studies, written in English. Exclusion criteria were determined iteratively by a team approach (AMC, JNV, CN), i.e., as the data were filtered, according to the nature of the studies discovered during the initial screening, in accordance with the methodology of scoping reviews (5). Thus, excluded articles were reviews, in vitro, animal, genetic or archeology studies, and studies focused on clinical management of DDE. Two raters (AMC, CN) independently assessed the quality of evidence, using the PEDro Scale for clinical trials, the Newcastle-Ottawa scale for observational studies, and a published tool for evaluating the quality of case reports and case series. Agreement on quality ratings of full- text articles was assessed for each, including references, and disagreements were resolved by a consensus-based discussion with a third rater (JNV). Finally, one author (AMC) completed the search strategy using a snowball approach to scour the references sections of all included articles (see details in Supplementary Material 3).
The initial electronic database search represented a total of 1,096 articles. Considering exclusion criteria, 128 full-text articles were eligible for inclusion. We excluded 5 articles with a quality assessment score of 0 and without published references, or with references that could not be consulted. Finally, 123 articles were included in this scoping review (Supplementary Material 3). Figure 1 describes the flowchart for the entire process.
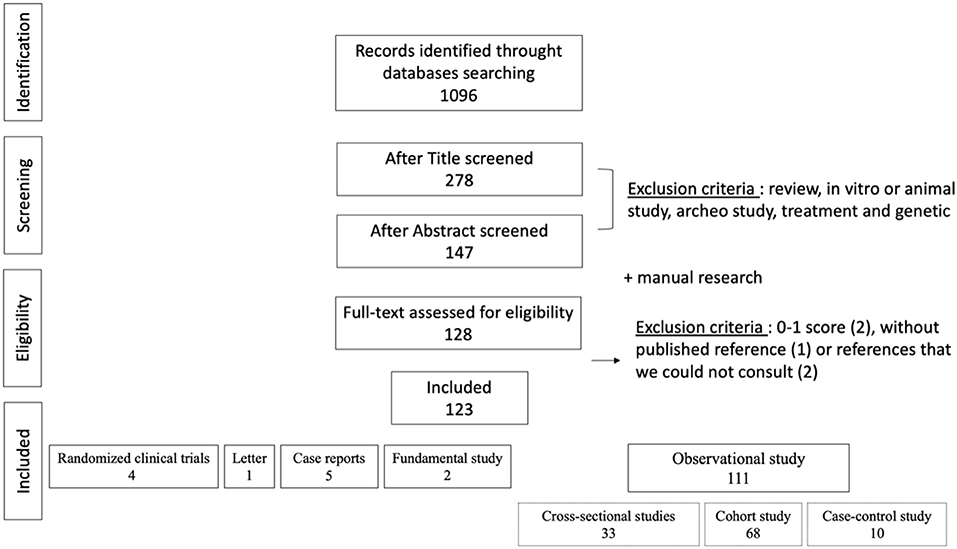
Figure 1. Flow chart of the research strategy.
Our explicative model about the mechanisms involved in acquired DDE (aDDE) is presented according to (1) a chronological timeframe of tooth development (Figure 2) and (2) putative biological mechanisms (Figure 3). All the factors are sorted alphabetically, without any prioritization.
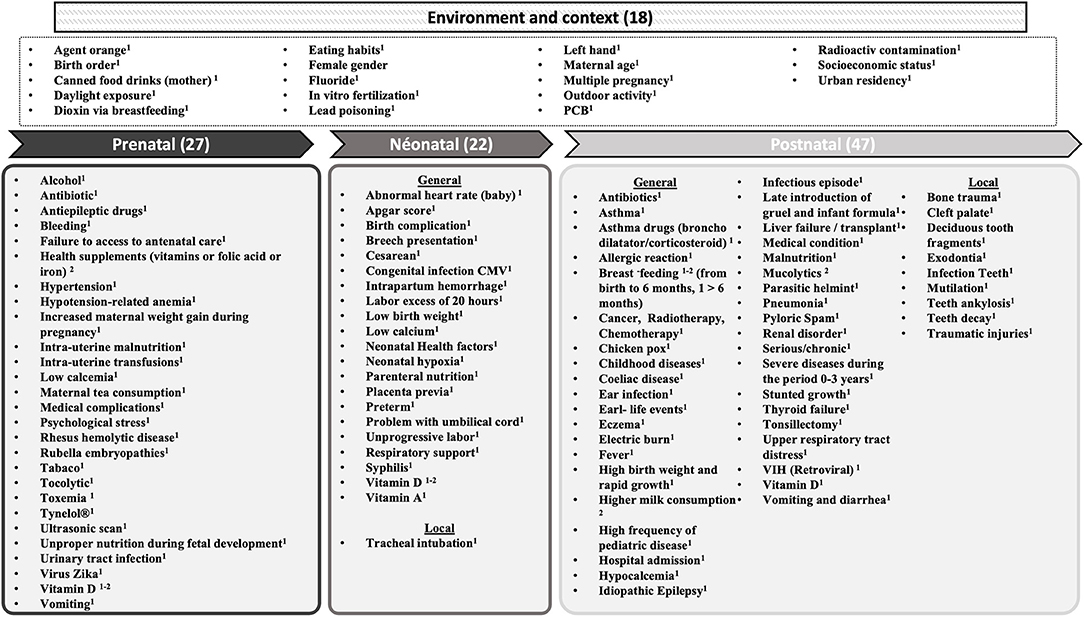
Figure 2. Factors cited in the literature related to aDDE, according to periods of damage. (–) number of factor, Risk factor1, Protective factor2.
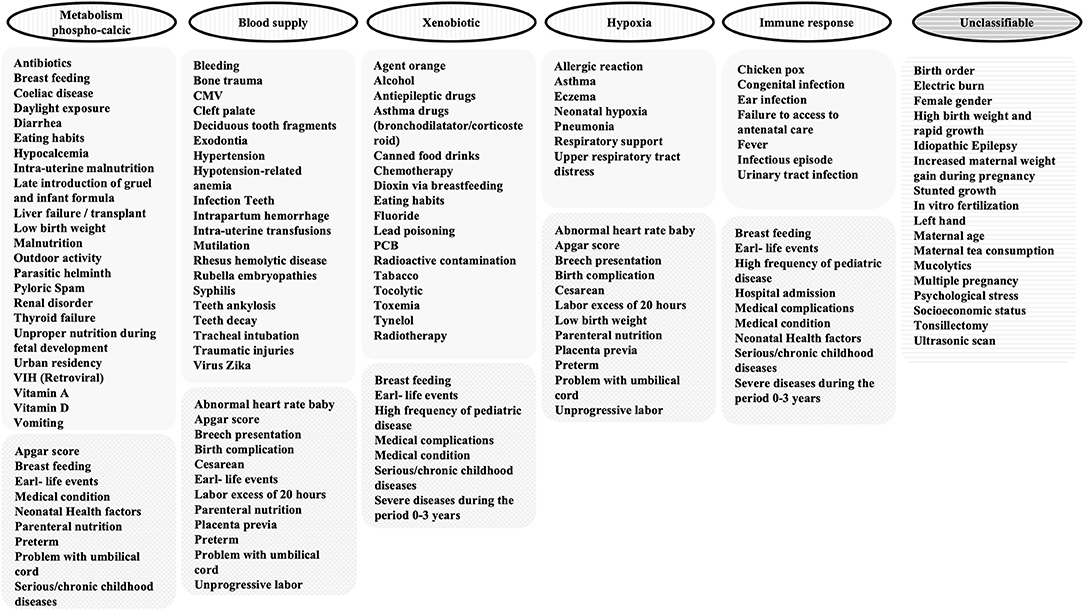
Figure 3. Clustering of aDDE risk and protector factors in 5 categories according/corresponding to the possible mechanisms.
1) Chronological timeframe of tooth development
As aDDE pathology occurs during a more or less extensive time-lapse of morphogenesis and biomineralization of the teeth and in agreement with Elzein et al. (6), we first classified the risk- or protective-related factors into three sections, corresponding to prenatal, neonatal, and postnatal periods. Some factors have been identified in each of these periods. Moreover, environmental (social context and geographic) factors were added (Figure 2).
Studies showed a higher frequency of aDDE among children: who suffered from intrauterine malnutrition (7, 8), improper nutrition during fetal development (9), and survivors after prenatal intra-uterine transfusions (for rhesus incompatibility for example) (10).
Medicals complications (11) or toxemia during pregnancy (12) are related to DDE. More specifically: ZIKV (13, 14), rubella embryopathy (15), deficiencies of vitamin D (16–18), low calcemia (16, 19), increased maternal weight gain and failure to access to antenatal care (20), urinary tract infection (21), gestational diabetes (16, 22, 23), bleeding (24), frequent vomiting (25), maternal psychological stress (26), hypotension-related anemia (26), hypertension (27), and frequent exposure to ultrasonic scans during the last gestational trimester (26). Maternal consumption of Tynelol during pregnancy (20), antibiotic (28) prenatal anti-epileptic drugs (29), tocolytic agent (30), alcohol (31, 32), tea (20), tobacco use (25, 33) were associated to DDE. A relationship between the number of cigarettes smoked per day and the prevalence of hypoplasia was described (27, 34). Conversely, several studies suggested that vitamin D supplementation (35–37) or health supplements (vitamins or folic acid or iron) (25) during pregnancy would be beneficial to prevent aDDE.
Neonatal health factors appeared to be associated with enamel defects (38). Delivery complications (39), non-progressive labor, umbilical cord issues and/or an abnormal heart rate of the baby (6), labor more than 20 hours, breech presentation, intrapartum hemorrhage, and placenta previa (12), cesarean delivery (12, 34) were associated with DDE.
Preterm birth could be considered as risk factor for aDDE (8, 12, 40–43) and low birth weight has been associated with DDE (7, 8, 34, 44–47) or the association preterm low birth weight children (48). A lower Apgar score was associated with a higher prevalence of enamel defects (34, 49–51).
Associations between vitamin D deficiencies (33), low calcemia (19, 52), low vitamin A levels (53), infections [syphilis (54) or CMV (55)] and DDE were also described.
Tracheal intubation (34, 43, 56) may cause local trauma and dental lesions associated with endotracheal intubation are asymmetrical. And even that the longer the duration of mechanical ventilation, the greater the chance of developing dental enamel defect (57). aDDE were more common in children who received parenteral nutrition during the neonatal period (34).
Early-life events (49), medical condition (26), severe diseases during the period 0–3 years (58), and high frequency of pediatric disease (21) appear to be associated with aDDE. This may involve serious/chronic childhood diseases (11, 14, 59), such as the following factors cited in the literature: vitamin D deficiencies (17), hypocalcemia (60), chicken pox (61), infectious episodes (38, 53), high fever (6, 62), hospital admission (40), ear infection (27, 63), renal disorders (64), liver failure/ liver transplant (65), thyroid dysfunction (both hypothyroidism and hyperthyroidism) (66), infantile eczema (33), tonsillectomy (67), intestinal disturbance [parasitic helminth infection (68) and pyloric spasm (63), celiac disease (69, 70), vomiting and diarrhea (61)], electric burns (71), idiopathic epilepsy (72), and the use of some drugs: antiretroviral therapy (24), antibiotic use (6, 14, 33, 73), specifically penicillins (74, 75) and cephalosporins (76).
Age of children (when perturbation happens) matters: first month (50), first year of life (40, 62), the first 2 years of the child's life (77) or the 3-year barrier are cited (39, 73).
aDDE are described in children surviving cancer (78–82) because of the disease itself, or anticancer therapy (83): antineoplastic agents (84–86), and/or radiotherapy (87). Dental abnormalities occur more frequently in patients who have undergone treatment during odontogenesis [different studies have proposed some ages: children younger than 1 (78), 3 (88), 5 (84, 89), or 6 (87) years].
The association of severe respiratory distress syndromes leading to oxygen deprivation (asthma, upper respiratory tract distress, pneumonia) and aDDE is reported by several studies (38, 39, 61, 77, 90, 91). More specifically, the severity (61) of asthma, asthma drugs (92) (bronchodilator/corticosteroid) or severe allergic reactions (91) are linked to a higher prevalence of aDDE.
Malnutrition is related to the prevalence of aDDE (28, 59, 68). Stunted growth (68, 93) seems to lead to enamel defects. Children with a high birth weight and rapid growth during their first year of life were more vulnerable to the occurrence of aDDE in their permanent dentition (3).
Higher milk consumption postnatally (94) and treatment with mucolytics (21) seemed to exert a protective effect against aDDE.
Breastfeeding was described as a protective factor for enamel defect development (95, 96) and children who were not breast-fed could be considered at risk for developing enamel defects (41, 94, 97). On the contrary, an association between aDDE and breastfeeding for more than 6 months, with late introduction of gruel and infant formula was found (98). The conclusion was that nutritional conditions during the first 6 months of life may influence the risk of developing severe demarcated opacities in the first permanent molars.
Cleft palate (CLP) is associated with aDDE (99, 100). The prevalence of dental abnormalities in CLP patients will depend on treatment protocol (101, 102) and that surgical repair will contribute to this defect (103).
Also, a correlation between aDDE on permanent teeth and pathology of the predecessors is suggested: retained deciduous tooth fragments (104), ankylosis (105), exodontia (106), traumatic injuries (107–111), periapical infection (16, 112), decays (113, 114), mutilation (115, 116), self-inflicted minor oral trauma among infants learning to handle and mouth objects (94).
The prevalence of aDDE seems to be higher with younger maternal age (34, 97), in case of multiple pregnancy (12, 34), in vitro fertilization (14) and with Sibling birth order (26, 50).
Higher socioeconomic status was found to be a risk factor for aDDE (33). The rate rose when moving from the most deprived categories to the least deprived categories (117). Female gender (21) and Left -handers may be associated with hypoplastic defect (20).
Reduced exposure to daylight because of winter months (17, 96, 118), little outdoor activity (25, 118), Urban residency during a child's first 2 years (119) and eating habits (118) seem associated with enamel disturbances, possibly reflecting vitamin D status.
Chemical elements may cause an adverse effect on dental formation. An association appears to exist between aDDE and some toxins: radioactive contamination (120), dioxin exposure (121) (“Agent Orange”), chronic lead poisoning (122), and long- term exposure to PCBs (123) and excess fluoride (124).
Prolonged breast feeding (more than 8 months) may increase the risk of mineralization defects in healthy children (125–127), possibly because of environmental contaminants that interfere with tooth development (128). Maternal consumption of canned food and drinks during breastfeeding was associated with aDDE (6).
2) Putative biological mechanisms
The mechanisms involved in aDDE identified in the scoping review were regrouped into 5 categories according/corresponding to the possible mechanisms (Figure 3).
Metabolic stresses/disorder (18, 129) or hypocalcemia during enamel formation (130) may be associated with aDDE. More specifically, some pathologies identified in the scoping review may cause calcemia disorders and have a link with aDDE: chronic illness or malnutrition problems (131), vitamin D deficiency (16, 132), phosphate deficiency (130, 131, 133), thyroid dysfunction (130, 131), celiac disease (issue in calcium absorption) (134), diabetic disease (23), gestational diabetes (135), cancer (136) calcium metabolism (16, 130, 133), pediatric conditions (18), and antiretroviral therapy (HIV treatment) for children and adolescents because it leads to a reduced level of calcium (137).
Local trauma due to CLP surgery (102), decay (because there is spread of inflammation to the underlying permanent teeth germs) (113) and virus (due to vascular changes leading to the lack of cellular nutrition) (138) perturbs blood supplies. Even if a possible direct cause due to the virus is not ruled out (139).
Teeth are most vulnerable and sensitive to the toxic effects of environmental chemicals and drugs during their development and before eruption into the mouth (140).
Exposure to dioxins is therefore not without danger for the dental organ and its consequences are closely linked to the stage of development of the tooth and the toxic dose received (141).
Conditions such as neonatal hypoxia (16), severe allergies (91), asthma, and other respiratory diseases (129) can cause respiratory acidosis and abnormal oxygen levels (142) and may be associated with aDDE. Moreover, because ameloblasts (cells which secrete the enamel proteins) are highly sensitive to oxygen supply (77), oxygen deficiency was proposed as perturbing the mineralization of the enamel matrix (143).
Infections affect the immune system and cause systemic repercussions that can affect dental development (129, 144), especially by altering normal ameloblast function (30).
This scoping review which meets the objectives described in the Munn et al. (145) report made it possible to:
The research on factors related to aDDE is mainly supported by observational studies (Figure 1). Quality scores of the included studies were heterogeneous, ranging from 1/8 to 8/9, with a mean score of 4.8/8 and a median at 5/8 (Supplementary Material 3). One hundred and fourteen factors were cited in the literature. This allows a mapping chronological timeframe (Figure 2) and a classification by putative biological mechanisms (Figure 3).
Some factors are well-reported and have been the subject of review papers (not analyzed in this SC): severe respiratory distress syndromes (146), preterm birth (147), vitamin D deficiencies during childhood (148), cleft palate (149), syphilis (150), excess fluoride (151), renal disorders (133), diabetes type 1 (152), cancer therapy (153), organic pollutants (154), dioxin exposure (155), dietary components (156), drugs during pregnancy and the first year of life (157), and drugs during infancy (158); these do not always relay clear evidence between DDE and risk factors supporting our hypothesis of accumulation and synergy effects. Generalist reviews were found, but either did not identify as many factors in a systematic way (159), or focused on one type of DDE (160), dentition (161) or treatment (162). Even if our results are close/comparable to the recent published study (163) on a particular form of DDE affecting the 1st molar and permanent incisors (MIH), this taxonomy raise some lacks in the current literature. This SC opens research perspectives by pointing out that some factors could be the object of review and that conduct large-scale epidemiological studies could be beneficial to study potential associations of protective or risk factors.
For the construction of common pathophysiological mechanisms, we looked at whether the 5 categories previously identified (Figure 3) were related to a general disruption (maternal health, infant health, birth complication, or impact or not by the environment) or to a local disruption. Figure 4 summarizes the 2 main pathways that will be modified upon exposure to these factors: the metabolism of calcium balance pathway and the aryl hydrocarbon receptor nuclear translocator (ARNT) pathway that is split into 3 mechanisms (response to hypoxia, response to xenobiotics, and immune response).
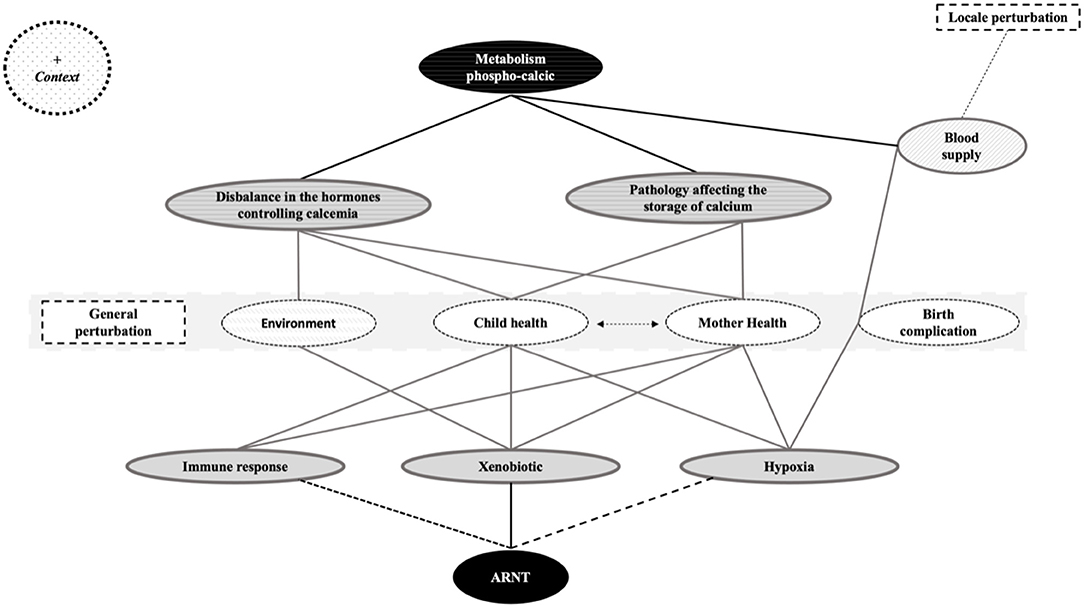
Figure 4. Identification of the different mechanisms showed by the clustering of aDDE risk and protector factors. ARNT, aryl hydrocarbon receptor nuclear translocator.
Tooth developments occur in three stages: a) ameloblast secretion (directly influenced by adequate levels of vitamin A, C, and D); b) mineralization; and c) maturing (directly affected by levels of calcium and phosphorus). An inadequate supply of calcium phosphate leads to a perturbation calcium phosphate deposit in the matrix (164) and deficiency of calcium can affect epithelial cell function and the mineralization process (165). During mineralization and maturation of enamel, many exchanges with the blood medium take place and involve the massive arrival of calcium and phosphate ions from the interstitial fluid.
Following this observation, the mechanisms disrupting calcium homeostasis could also disrupt enamel formation and the ameloblasts will not obtain the nutrients they need to secrete enamel (49). This observation will link perturbation of the blood supply of the developing tooth to its consequences for cellular nutrition, thus leading to aDDE. This explanation can also be applicable to exodontia and trauma. Globally (166), calcium and phosphate homeostasis is related to the levels of calcitriol (hormonally active form of vitamin D), of parathormone (PTH) and calcitonin. Organs involved in this process are the thyroid, bones, kidneys, and digestive tract. In this way, different groups of pathologies have an impact on enamel development:
1) Pathologies affecting the organs (digestive tract, bone, and kidney) responsible for storage of calcium.
2) An imbalance in the hormones controlling calcemia and phosphatemia, or a pathology of organs responsible for hormonal regulation (parathyroid and thyroid).
The protein aryl hydrocarbon Receptor (AhR) is involved in the response to environmental pollutants (154). Its function is to regulate the expression of xenobiotic metabolizing enzymes involved in detoxication using the ARNT (167).
The conditions of hypoxia lead to reprogramming the cell via the Hypoxia-Inducible Factor (HIF) protein (168), who also required ARNT. These etiologies are different, but the molecular mechanisms involved seem to converge on a single path, as they use ARNT as a partner. At the cellular level, this could result in a disturbance of the normal ameloblastic activity (142, 164) and lead to disorders of dental enamel matrix protein. Vorrink and Domann (167) explained that the normal xenobiotic responses may be perturbed under physiological hypoxia, so the xenobiotic response and hypoxia response pathways intersect. The important role of ARNT in both the AhR and HIF signaling pathways establishes a meaningful foundation for a possible crosstalk between these two vitally important signaling pathways.
Because the AhR receptor is expressed on a majority of immune cell types, this reflects the importance of AhR in immunological processes (169). In addition, AhR signaling pathways have been reported to influence a few genes responsible for mediating inflammation and other immune responses, so an involvement of the immune response in the ARNT pathway is to be explored.
Skinner and Hung (94), postulated that a systemic event combined with a local traumatic event was a possible etiology of aDDE and Goho (170), reports that chemotherapy damage is directly related to dose (the ameloblast does not appear to be affected by a low dose of radiation, but that a high dose of radiation causes its death) and/or to the repetition of the various agents. This make us suggest that these mechanisms are cumulative and that when the equilibrium is destabilized, the other pathways adapt. However, there would be a threshold beyond which the organism cannot adapt and the very extensive clinical picture of aDDE raises the hypothesis of a host response (sex/age…) even an epigenetic control (171) although authors (172) report that it is likely that environmental factors exert a greater influence (Figure 5). We can suppose that the defects result from the nature and/or the accumulation of the aggressions (intensity, duration, and moment) but also from their interactions between them. Thus, we believe that the risk of developing enamel defects arises from a metabolic disorder or disruption involving the ARNT pathway that needs further study. But because many diseases can produce hypocalcemia, hypoxia and pyrexia (173) and that micronutrient deficiencies have been linked to compromised conception, gestation length, fetal development, and growth, potentially leading to pregnancy loss, preterm delivery, small birth size, birth defects, and long-term metabolic disruption (174), both pathways may be involved at the same time. Finally, because 2,3,7,8-Tetrachlorodibenzo-p-dioxin (TCDD) rapidly increases intracellular calcium concentrations via AhR pathways (175), it is possible that ARNT and metabolic balance are linked (Figure 5).
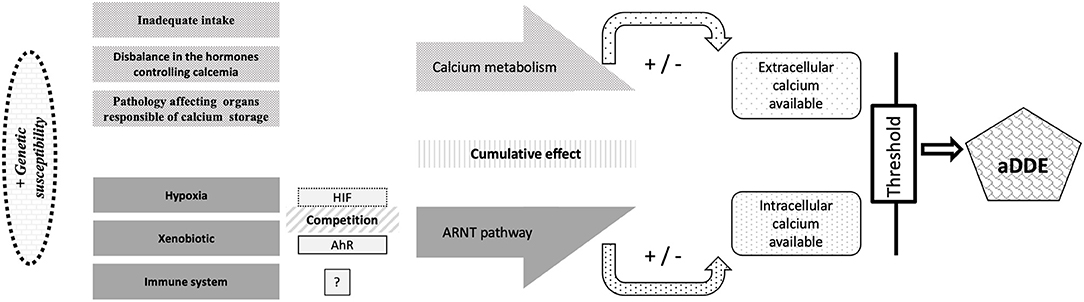
Figure 5. Proposed link between the mechanisms involved in aDDE formation and the cumulative and synergistic effect of the factors involved. HIF, Hypoxia-Inducible Factor; ARNT, aryl hydrocarbon receptor nuclear translocator; AhR, Aryl hydrocarbon Receptor; aDDE, aquired Developmental Defects of Enamel.
This proposal of pathophysiological mechanism is supported by the fact that some factors coexist: Dos Reis et al. (176) reports a higher prevalence of preterm baby and low birth weight observed in infants born to mothers with Acquired Immunodeficiency Syndrome (AIDS). de Oliveira et al. (13) reports that Children with congenital Zika syndrome had a higher frequency of problems related to breastfeeding and low weight compared with healthy children. Suckling et al. (61) reports that asthma may in part be associated with an increased frequency of, or susceptibility to viral infections. Otitis media is an infectious condition that could coexist with the presence of fever and use of medicines (27). Preterm and low birth weight children are at increased risk of lower respiratory tract infections (177). Maternal risk factors are numerous and some are also cited as risk factors for DDE: smoking, drug and alcohol use, medication consumption, maternal malnutrition, multiple births, congenital malformations, genital infections, unspecified bleeding, maternal age (under 17 and older than 34), and may result in intrauterine growth restriction and the infant being small for its gestational age (177). Grahnén et al.'s (129) study indicates that the common complications of pre-term birth such as asphyxia and/or hyperbilirubinemia seem to explain the higher incidence of aDDE in this children.
This taxonomy and the hypotheses related to the mechanism allow us to make, with caution (due to confounding factors in the interpretation of the different results), some recommendations:
Because differences in nutritional status, or obstetric and pediatric care may be important etiological factors for DDE, medical teams (dentists, midwives, obstetricians, pediatricians and others) should be aware that maternal health during pregnancy and infancy care is related to children's oral health. Optimal nutritional intakes during the pre- peri- and postnatal periods, careful handling of high fever, greater public awareness regarding misuse of drugs, education about xenobiotics and how to prevent DDE, are recommended to decrease its occurrence.
In view of our results, children with a complex health history (perinatal events or healthiness during childhood), with hypomineralized secondary primary molars (25, 48), and with a history of oral trauma should be considered at risk for DDE. Globally, the presence of DDE increases the risk of cavities and tooth wear because defective enamel is thinner, holds more plaque and is less resistant to dissolving in acid. Early detection of DDE is beneficial in establishing a prevention program to manage tooth sensitivity, cavities, and tooth wear (178). Children with DDE should be seen by a dentist as soon as the temporary teeth erupt and monitored on a regular basis as long as the permanent teeth erupt. Early management of these teeth allows a better long-term prognosis and quality of life.
If we extrapolate Murray and Johnsen's (179) results, the position and kind of defect on the enamel is useful to determine its origin and can help with a diagnosis. Therefore, since dental enamel tissue cannot remodel, anomaly of the teeth can represent a “past pathology map,” and DDE may indicate the time of insult to the developing fetus or infant. This allows for vigilance and motivation for early detection of disorders. Specifically, this can help with the diagnosis of deafness and neurological lesions (180), or may even allow early detection of children with learning problems (181). They can also, based on the observation that enamel defects may present among the first symptoms of celiac disease (70), the diagnosis of these oral manifestations might be helpful for an early diagnosis (69).
DDE may result from a wide range of acquired etiological factors, 114 were listed and classified in this scoping review. The most frequently encountered pathologies are those causing a disorder of calcium homeostasis or a perturbation of the ARNT pathway in mother or child. The link between the ARNT pathway and metabolism deficiency in uncertain and needs to be defined. Furthermore, the role of this mechanism in tissue impairment is still unclear and needs to be explored.
This work confirmed that the child's general health, medical history, and oral health are intimately linked. Communication between medical teams is essential because some risk factors should alert health practitioners to set up a prevention of dental pathology, DDE can be a warning sign of general pathologies and modifying some behaviors could limit the risk of developing DDE. Finally, this scoping review may help the practitioner explaining to the patient the possible causes of his condition.
All the authors participated in drafting the manuscript, revising it critically, and approved the final version of the submitted manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We sincerely thank Dr. Catherine Arnaud for welcoming A-MC in her team and for her expertise in the construction of this work.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.836708/full#supplementary-material
AhR, protein aryl hydrocarbon Receptor; aDDE, acquired Developmental Defects of Enamel; ARNT, aryl hydrocarbon receptor nuclear translocator; DDE, Developmental Defects of Enamel; HIF, Hypoxia-Inducible Factor.
1. A review of the developmental defects of enamel index (DDE Index) Commission on Oral Health, Research & Epidemiology. Report of an FDI Working Group. Int Dent J. (1992) 42:411–26.
3. Wong HM, Peng S-M, King NM, McGrath C. Infant growth and the occurrence of developmental defects of enamel in 12-year-olds. Caries Res. (2015) 49:575–82. doi: 10.1159/000381425
4. de La Dure-Molla M, Fournier BP, Manzanares MC, Acevedo AC, Hennekam RC, Friedlander L, et al. Elements of morphology: standard terminology for the teeth and classifying genetic dental disorders. Am J Med Genet A. (2019) 179:1913–81. doi: 10.1002/ajmg.a.61316
5. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
6. Elzein R, Chouery E, Abdel-Sater F, Bacho R, Ayoub F. Molar-incisor hypomineralisation in Lebanon: association with prenatal, natal and postnatal factors. Eur Arch Paediatr Dent. (2020) 22:283–90. doi: 10.1007/s40368-020-00555-5
7. Pinho JRO, Filho FL, Thomaz EB a. F, Lamy ZC, Libério SA, Ferreira EB. Are low birth weight, intrauterine growth restriction, and preterm birth associated with enamel developmental defects? Pediatr Dent. (2012) 34:244–8.
8. Thomaz ÉBAF, Alves CMC, Ribeiro CCC, Batista RFL, Simões VMF, Cavalli R, et al. Perinatal outcomes and changes in the oral cavity: Brazilian cohorts of Ribeirão Preto and São Luís. Rev Bras Epidemiol Braz J Epidemiol. (2015) 18:966–70. doi: 10.1590/1980-5497201500040023
9. Li Y, Navia JM, Bian JY. Prevalence and distribution of developmental enamel defects in primary dentition of Chinese children 3-5 years old. Community Dent Oral Epidemiol. (1995) 23:72–9. doi: 10.1111/j.1600-0528.1995.tb00204.x
10. Bock JE, Winkel S. A follow-up study of infants who received intra-uterine transfusions because of severe rhesus haemolytic disease. Acta Obstet Gynecol Scand Suppl. (1976) 53:37–40. doi: 10.3109/00016347609156443
11. Rai A, Singh A, Menon I, Singh J, Rai V, Aswal GS. Molar incisor hypomineralization: prevalence and risk factors among 7-9 years old school children in Muradnagar, Ghaziabad. Open Dent J. (2018) 12:714–22. doi: 10.2174/1745017901814010714
12. Via WF, Churchill JA. Relationship of enamel hypoplasia to abnormal events of gestation and birth. J Am Dent Assoc. (1959) 59:702–7. doi: 10.14219/jada.archive.1959.0209
13. de Oliveira AMM, de Melo EGM, Mendes MLT, Dos Santos Oliveira SJG, Tavares CSS, Vaez AC, et al. Oral and maxillofacial conditions, dietary aspects, and nutritional status of children with congenital Zika syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol. (2020) 130:71–7. doi: 10.1016/j.oooo.2020.02.019
14. da Silva MCPM, de Arnaud MA, Lyra MCA, de Alencar Filho AV, Rocha MÂW, Ramos RCF, et al. Dental development in children born to Zikv-infected mothers: a case-based study. Arch Oral Biol. (2020) 110:104598. doi: 10.1016/j.archoralbio.2019.104598
15. Hall RK. Prevalence of developmental defects of tooth enamel (DDE) in a pediatric hospital department of dentistry population (1). Adv Dent Res. (1989) 3:114–9. doi: 10.1177/08959374890030020801
16. Neto MBC, da Silva-Souza KP, Maranhão VF, Botelho KVG, Heimer MV, Dos Santos-Junior VE. Enamel defects in deciduous dentition and their association with the occurrence of adverse effects from pregnancy to early childhood. Oral Health Prev Dent. (2020) 18:741–6. doi: 10.3290/j.ohpd.a45077
17. Purvis RJ, Barrie WJ, MacKay GS, Wilkinson EM, Cockburn F, Belton NR. Enamel hypoplasia of the teeth associated with neonatal tetany: a manifestation of maternal vitamin-D deficiency. Lancet Lond Engl. (1973) 2:811–4. doi: 10.1016/S0140-6736(73)90857-X
18. Pimlott JF, Howley TP, Nikiforuk G, Fitzhardinge PM. Enamel defects in prematurely born, low birth-weight infants. Pediatr Dent. (1985) 7:218–23.
19. Reed SG, Miller CS, Wagner CL, Hollis BW, Lawson AB. Toward preventing enamel hypoplasia: modeling maternal and neonatal biomarkers of human calcium homeostasis. Caries Res. (2020) 54:55–67. doi: 10.1159/000502793
20. Needleman HL, Allred E, Bellinger D, Leviton A, Rabinowitz M, Iverson K. Antecedents and correlates of hypoplastic enamel defects of primary incisors. Pediatr Dent. (1992) 14:158–66.
21. Tapias-Ledesma MA, Jiménez R, Lamas F, González A, Carrasco P, Gíl de Miguel A. Factors associated with first molar dental enamel defects: a multivariate epidemiological approach. J Dent Child Chic Ill. (2003) 70:215–20.
22. Ghapanchi J, Kamali F, Siavash Z, Homan Ebrahimi, Pourshahidi S, Ranjbar Z. The Relationship between gestational diabetes, enamel hypoplasia and DMFT in children: a clinical study in southern Iran. Br J Med Med Res. (2015) 10:1–6. doi: 10.9734/BJMMR/2015/19574
23. Pascon T, Barbosa AMP, Cordeiro RCL, Bussaneli DG, Prudencio CB, Nunes SK, et al. Prenatal exposure to gestational diabetes mellitus increases developmental defects in the enamel of offspring. PloS ONE. (2019) 14:e0211771. doi: 10.1371/journal.pone.0211771
24. Pontes AS, Lima M de DM, Andrade NS, de Moura MS, Moura L de FA de D. Dental enamel development defects in children and adolescents with HIV infection: case-control study. Spec Care Dent. (2017) 37:19–27. doi: 10.1111/scd.12188
25. Lee D-W, Kim Y-J, Oh Kim S, Choi SC, Kim J, Lee JH, et al. Factors associated with molar-incisor hypomineralization: a population-based case-control study. Pediatr Dent. (2020) 42:134–40.
26. Ghanim A, Manton D, Bailey D, Mariño R, Morgan M. Risk factors in the occurrence of molar-incisor hypomineralization amongst a group of Iraqi children. Int J Paediatr Dent. (2013) 23:197–206. doi: 10.1111/j.1365-263X.2012.01244.x
27. Lopes-Fatturi A, Menezes JVNB, Fraiz FC, Assunção LR da S, de Souza JF. Systemic exposures associated with hypomineralized primary second molars. Pediatr Dent. (2019) 41:364–70.
28. França TKXS, de Lima M de DM, Lima CCB, de Moura MS, Lopes TSP, de Moura JSS, et al. Quilombola children and adolescents show high prevalence of developmental defects of enamel. Cienc Saude Coletiva. juill. (2021) 26:2889–98. doi: 10.1590/1413-81232021267.12762019
29. Jacobsen PE, Henriksen TB, Haubek D, Ostergaard JR. Developmental enamel defects in children prenatally exposed to anti-epileptic drugs. PloS ONE. (2013) 8:e58213. doi: 10.1371/journal.pone.0058213
30. Lamm CI, Norton KI, Murphy RJ, Wilkins IA, Rabinowitz JG. Congenital rickets associated with magnesium sulfate infusion for tocolysis. J Pediatr. (1988) 113:1078–82. doi: 10.1016/S0022-3476(88)80586-9
31. Blanck-Lubarsch M, Dirksen D, Feldmann R, Sauerland C, Hohoff A. Tooth malformations, DMFT index, speech impairment and oral habits in patients with fetal alcohol syndrome. Int J Environ Res Public Health. (2019) 16:4401. doi: 10.3390/ijerph16224401
32. Elfrink MEC, Moll HA, Kiefte-de Jong JC, Jaddoe VWV, Hofman A, ten Cate JM, et al. Pre- and postnatal determinants of deciduous molar hypomineralisation in 6-year-old children. The generation R study. PloS ONE. (2014) 9:e91057. doi: 10.1371/journal.pone.0091057
33. Silva MJ, Kilpatrick NM, Craig JM, Manton DJ, Leong P, Burgner D, et al. Etiology of hypomineralized second primary molars: a prospective twin study. J Dent Res. (2019) 98:77–83. doi: 10.1177/0022034518792870
34. Velló MA, Martínez-Costa C, Catalá M, Fons J, Brines J, Guijarro-Martínez R. Prenatal and neonatal risk factors for the development of enamel defects in low birth weight children. Oral Dis. (2010) 16:257–62. doi: 10.1111/j.1601-0825.2009.01629.x
35. Reed SG, Voronca D, Wingate JS, Murali M, Lawson AB, Hulsey TC, et al. Prenatal vitamin D and enamel hypoplasia in human primary maxillary central incisors: a pilot study. Pediatr Dent J Int J Jpn Soc Pediatr Dent. (2017) 27:21–8. doi: 10.1016/j.pdj.2016.08.001
36. Cockburn F, Belton NR, Purvis RJ, Giles MM, Brown JK, Turner TL, et al. Maternal vitamin D intake and mineral metabolism in mothers and their newborn infants. Br Med J. (1980) 281:11–4. doi: 10.1136/bmj.281.6232.11
37. Nørrisgaard PE, Haubek D, Kühnisch J, Chawes BL, Stokholm J, Bønnelykke K, et al. Association of high-dose vitamin D supplementation during pregnancy with the risk of enamel defects in offspring: a 6-year follow-up of a randomized clinical trial. JAMA Pediatr. (2019) 173:924–30. doi: 10.1001/jamapediatrics.2019.2545
38. Arrow P. Risk factors in the occurrence of enamel defects of the first permanent molars among schoolchildren in Western Australia. Community Dent Oral Epidemiol. (2009) 37:405–15. doi: 10.1111/j.1600-0528.2009.00480.x
39. Pitiphat W, Luangchaichaweng S, Pungchanchaikul P, Angwaravong O, Chansamak N. Factors associated with molar incisor hypomineralization in Thai children. Eur J Oral Sci. (2014) 122:265–70. doi: 10.1111/eos.12136
40. Wagner Y. Developmental defects of enamel in primary teeth - findings of a regional German birth cohort study. BMC Oral Health. (2016) 17:10. doi: 10.1186/s12903-016-0235-7
41. Lunardelli SE, Peres MA. Breast-feeding and other mother-child factors associated with developmental enamel defects in the primary teeth of Brazilian children. J Dent Child Chic Ill. (2006) 73:70–8.
42. Schüler IM, Haberstroh S, Dawczynski K, Lehmann T, Heinrich-Weltzien R. Dental caries and developmental defects of enamel in the primary dentition of preterm infants: case-control observational study. Caries Res. (2018) 52:22–31. doi: 10.1159/000480124
43. Cortines AA de O, Corrêa-Faria P, Paulsson L, Costa PS, Costa LR. Developmental defects of enamel in the deciduous incisors of infants born preterm: prospective cohort. Oral Dis. (2019) 25:543–9. doi: 10.1111/odi.13011
44. Ferrini FRD, Marba STM, Gavião MBD. Oral conditions in very low and extremely low birth weight children. J Dent Child Chic Ill. (2008) 75:235–42.
45. Corrêa-Faria P, Martins-Júnior PA, Vieira-Andrade RG, Oliveira-Ferreira F, Marques LS, Ramos-Jorge ML. Developmental defects of enamel in primary teeth: prevalence and associated factors. Int J Paediatr Dent. (2013) 23:173–9. doi: 10.1111/j.1365-263X.2012.01241.x
46. Nelson S, Albert JM, Lombardi G, Wishnek S, Asaad G, Kirchner HL, et al. Dental caries and enamel defects in very low birth weight adolescents. Caries Res. (2010) 44:509–18. doi: 10.1159/000320160
47. Reis CLB, Barbosa MCF, de Lima DC, Brancher JA, Lopes CMCF, Baratto-Filho F, et al. Risk factors for developmental defects of enamel in children from southeastern Brazil. Community Dent Health. (2021) 38:178–81. doi: 10.1922/CDH_00242Reis04
48. Noor Mohamed R, Basha S, Virupaxi SG, Idawara Eregowda N, Parameshwarappa P. Hypomineralized primary teeth in preterm low birth weight children and its association with molar incisor hypomineralization-a 3-year-prospective study. Child Basel Switz. (2021) 8:1111. doi: 10.3390/children8121111
49. Pinto GDS, Costa FDS, Machado TV, Hartwig A, Pinheiro RT, Goettems ML, et al. Early-life events and developmental defects of enamel in the primary dentition. Community Dent Oral Epidemiol. (2018) 46:511–7. doi: 10.1111/cdoe.12408
50. Memarpour M, Golkari A, Ahmadian R. Association of characteristics of delivery and medical conditions during the first month of life with developmental defects of enamel. BMC Oral Health. (2014) 14:122. doi: 10.1186/1472-6831-14-122
51. Nirmala SVSG, Quadar MA, Veluru S, Tharay N, Kolli NK, Minor Babu MS. Apgar index as a probable risk indicator for enamel defects in primary dentition: a cross sectional study. J Indian Soc Pedod Prev Dent. (2015) 33:229–33. doi: 10.4103/0970-4388.160396
52. Stimmler L, Snodgrass GJ, Jaffe E. Dental defects associated with neonatal symptomatic hypocalcaemia. Arch Dis Child. (1973) 48:217–20. doi: 10.1136/adc.48.3.217
53. Sweeney EA, Cabrera J, Urrutia J, Mata L. Factors associated with linear hypoplasia of human deciduous incisors. J Dent Res. (1969) 48:1275–9. doi: 10.1177/00220345690480063201
54. Franco J, Maia SÉ, Vieira A, Santos C, Fonseca Silva T. Dental manifestations of congenital syphilis. Int J Inf Res Rev. (2016) 3:2620–2.
55. Stagno S, Pass RF, Thomas JP, Navia JM, Dworsky ME. Defects of tooth structure in congenital cytomegalovirus infection. Pediatrics. (1982) 69:646–8. doi: 10.1542/peds.69.5.646
56. Norén JG, Ranggård L, Klingberg G, Persson C, Nilsson K. Intubation and mineralization disturbances in the enamel of primary teeth. Acta Odontol Scand. (1993) 51:271–5. doi: 10.3109/00016359309040577
57. Suely Falcao de Oliveira Melo N, Guimaraes Vieira Cavalcante da Silva RP, Adilson Soares de Lima A. The neonatal intubation causes defects in primary teeth of premature infants. Biomed Pap Med Fac Univ Palacky Olomouc Czechoslov. (2014) 158:605–12. doi: 10.5507/bp.2013.004
58. Wong HM, Peng S-M, Wen YF, King NM, McGrath CPJ. Risk factors of developmental defects of enamel–a prospective cohort study. PloS ONE. (2014) 9:e109351. doi: 10.1371/journal.pone.0109351
59. Rugg-Gunn AJ, Al-Mohammadi SM, Butler TJ. Malnutrition and developmental defects of enamel in 2- to 6-year-old Saudi boys. Caries Res. (1998) 32:181–92. doi: 10.1159/000016451
60. Elger W, Illge C, Kiess W, Körner A, Kratzsch J, Schrock A, et al. Relationship between deciduous molar hypomineralisation and parameters of bone metabolism in preschool children. Int Dent J. (2020) 70:303–7. doi: 10.1111/idj.12550
61. Suckling GW, Herbison GP, Brown RH. Etiological factors influencing the prevalence of developmental defects of dental enamel in nine-year-old New Zealand children participating in a health and development study. J Dent Res. (1987) 66:1466–9. doi: 10.1177/00220345870660091101
62. Jackson D. A clinical study of non-endemic mottling of enamel. Arch Oral Biol. (1961) 5:212–23. doi: 10.1016/0003-9969(61)90059-0
63. Stein G. Enamel damage of systemic origin in premature birth and diseases of early infancy. Am J Orthod. (1947) 33:831–41. doi: 10.1016/0096-6347(47)90200-7
64. Subramaniam P, Gupta M, Mehta A. Oral health status in children with renal disorders. J Clin Pediatr Dent. (2012) 37:89–93. doi: 10.17796/jcpd.37.1.7l913347q0232v01
65. Olczak-Kowalczyk D, Kowalczyk W, Krasuska-Sławińska E, Dadalski M, Kostewicz K, Pawłowska J. Oral health and liver function in children and adolescents with cirrhosis of the liver. Przeglad Gastroenterol. (2014) 9:24–31. doi: 10.5114/pg.2014.40846
66. Venkatesh Babu NS, Patel PB. Oral health status of children suffering from thyroid disorders. J Indian Soc Pedod Prev Dent. (2016) 34:139–44. doi: 10.4103/0970-4388.180443
67. Muratbegovic A, Markovic N, Ganibegovic Selimovic M. Molar incisor hypomineralisation in Bosnia and Herzegovina: aetiology and clinical consequences in medium caries activity population. Eur Arch Paediatr Dent. (2007) 8:189–94. doi: 10.1007/BF03262595
68. Masterson EE, Fitzpatrick AL, Enquobahrie DA, Mancl LA, Conde E, Hujoel PP. Malnutrition-related early childhood exposures and enamel defects in the permanent dentition: a longitudinal study from the Bolivian Amazon. Am J Phys Anthropol. (2017) 164:416–23. doi: 10.1002/ajpa.23283
69. Acar S, Yetkiner AA, Ersin N, Oncag O, Aydogdu S, Arikan C. Oral findings and salivary parameters in children with celiac disease: a preliminary study. Med Princ Pract Int J Kuwait Univ Health Sci Cent. (2012) 21:129–33. doi: 10.1159/000331794
70. Shteyer E, Berson T, Lachmanovitz O, Hidas A, Wilschanski M, Menachem M, et al. Oral health status and salivary properties in relation to gluten-free diet in children with celiac disease. J Pediatr Gastroenterol Nutr. (2013) 57:49–52. doi: 10.1097/MPG.0b013e31828b3705
71. Alexander WN. Composite dysplasia of a single tooth as a result of electric burn damage: report of case. J Am Dent Assoc. (1964) 69:589–91. doi: 10.14219/jada.archive.1964.0330
72. Spitzer R. Enamel hypoplasia in idiopathic epilepsy. Br Med J. (1942) 1:110. doi: 10.1136/bmj.1.4229.110
73. Chawla N, Messer LB, Silva M. Clinical studies on molar-incisor-hypomineralisation part 1: distribution and putative associations. Eur Arch Paediatr Dent. (2008) 9:180–90. doi: 10.1007/BF03262634
74. Hong L, Levy SM, Warren JJ, Bergus GR, Dawson DV, Wefel JS, et al. Primary tooth fluorosis and amoxicillin use during infancy. J Public Health Dent. (2004) 64:38–44. doi: 10.1111/j.1752-7325.2004.tb02724.x
75. Hong L, Levy SM, Warren JJ, Broffitt B. Amoxicillin use during early childhood and fluorosis of later developing tooth zones. J Public Health Dent. (2011) 71:229–35. doi: 10.1111/j.1752-7325.2011.00254.x
76. Tariq A, Alam Ansari M, Owais Ismail M, Memon Z. Association of the use of bacterial cell wall synthesis Inhibitor drugs in early childhood with the Developmental Defects of Enamel. Pak J Med Sci. (2014) 30:393–7. doi: 10.12669/pjms.302.4508
77. Jälevik B, Norén JG, Klingberg G, Barregård L. Etiologic factors influencing the prevalence of demarcated opacities in permanent first molars in a group of Swedish children. Eur J Oral Sci. (2001) 109:230–4. doi: 10.1034/j.1600-0722.2001.00047.x
78. Kaste SC, Hopkins KP, Bowman LC, Santana VM. Dental abnormalities in children treated for neuroblastoma. Med Pediatr Oncol. (1998) 30:22–7.
79. Owosho AA, Brady P, Wolden SL, Wexler LH, Antonescu CR, Huryn JM, et al. Long-term effect of chemotherapy-intensity-modulated radiation therapy (chemo-IMRT) on dentofacial development in head and neck rhabdomyosarcoma patients. Pediatr Hematol Oncol. (2016) 33:383–92. doi: 10.1080/08880018.2016.1219797
80. Avşar A, Elli M, Darka O, Pinarli G. Long-term effects of chemotherapy on caries formation, dental development, and salivary factors in childhood cancer survivors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2007) 104:781–9. doi: 10.1016/j.tripleo.2007.02.029
81. Çetiner D, Çetiner S, Uraz A, Alpaslan GH, Alpaslan C, Toygar Memikoglu TU, et al. Oral and dental alterations and growth disruption following chemotherapy in long-term survivors of childhood malignancies. Support Care Cancer. (2019) 27:1891–9. doi: 10.1007/s00520-018-4454-0
82. Pajari U, Lanning M, Larmas M. Prevalence and location of enamel opacities in children after anti-neoplastic therapy. Community Dent Oral Epidemiol. (1988) 16:222–6. doi: 10.1111/j.1600-0528.1988.tb01759.x
83. Atif M, Mathur VP, Tewari N, Bansal K, Rahul M, Bakhshi S. Long-term effect of anticancer therapy on dentition in childhood cancer survivors: an observational, cross-sectional study. Indian J Pediatr. (2021). doi: 10.1007/s12098-021-03818-1. [Epub ahead of print].
84. Pajari U, Lanning M. Developmental defects of teeth in survivors of childhood ALL are related to the therapy and age at diagnosis. Med Pediatr Oncol. (1995) 24:310–4. doi: 10.1002/mpo.2950240508
85. Alpaslan G, Alpaslan C, Gögen H, Oguz A, Cetiner S, Karadeniz C. Disturbances in oral and dental structures in patients with pediatric lymphoma after chemotherapy: a preliminary report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (1999) 87:317–21. doi: 10.1016/S1079-2104(99)70215-5
86. Lauritano D, Petruzzi M. Decayed, missing and filled teeth index and dental anomalies in long-term survivors leukaemic children: a prospective controlled study. Med Oral Patol Oral Cirugia Bucal. (2012) 17:e977–80. doi: 10.4317/medoral.17955
87. Dahllöf G, Barr M, Bolme P, Modéer T, Lönnqvist B, Ringdén O, et al. Disturbances in dental development after total body irradiation in bone marrow transplant recipients. Oral Surg Oral Med Oral Pathol. (1988) 65:41–4. doi: 10.1016/0030-4220(88)90189-2
88. Bagattoni S, D'Alessandro G, Prete A, Piana G, Pession A. Oral health and dental late adverse effects in children in remission from malignant disease. A pilot case-control study in Italian children. Eur J Paediatr Dent. (2014) 15:45–50.
89. Sonis AL, Tarbell N, Valachovic RW, Gelber R, Schwenn M, Sallan S. Dentofacial development in long-term survivors of acute lymphoblastic leukemia. A comparison of three treatment modalities. Cancer. (1990) 66:2645–52.
90. Johnsen D, Krejci C, Hack M, Fanaroff A. Distribution of enamel defects and the association with respiratory distress in very low birthweight infants. J Dent Res. (1984) 63:59–64. doi: 10.1177/00220345840630011401
91. Rattner LJ, Myers HM. Occurrence of enamel hypoplasia in children with congenital allergies. J Dent Res. (1962) 41:646–9. doi: 10.1177/00220345620410031701
92. Mastora A, Vadiakas G, Agouropoulos A, Gartagani-Panagiotopoulou P, Gemou Engesaeth V. Developmental defects of enamel in first permanent molars associated with use of asthma drugs in preschool aged children: a retrospective case-control study. Eur Arch Paediatr Dent. (2017) 18:105–11. doi: 10.1007/s40368-017-0280-1
93. Takaoka LAMV, Goulart AL, Kopelman BI, Weiler RME. Enamel defects in the complete primary dentition of children born at term and preterm. Pediatr Dent. (2011) 33:171–6.
94. Skinner MF, Hung JT. Social and biological correlates of localized enamel hypoplasia of the human deciduous canine tooth. Am J Phys Anthropol. (1989) 79:159–75. doi: 10.1002/ajpa.1330790204
95. Pinho JRO, Thomaz EBAF, Ribeiro CCC, Alves CMC, da Silva AAM. Factors associated with the development of dental defects acquired in the extrauterine environment. Braz Oral Res. (2019) 33:e094. doi: 10.1590/1807-3107bor-2019.vol33.0094
96. Mellander M, Norén JG, Fredén H, Kjellmer I. Mineralization defects in deciduous teeth of low birthweight infants. Acta Paediatr Scand. (1982) 71:727–33. doi: 10.1111/j.1651-2227.1982.tb09511.x
97. Corrêa-Faria P, Martins-Júnior PA, Vieira-Andrade RG, Marques LS, Ramos-Jorge ML. Perinatal factors associated with developmental defects of enamel in primary teeth: a case-control study. Braz Oral Res. (2013) 27:363–8. doi: 10.1590/S1806-83242013005000017
98. Fagrell TG, Ludvigsson J, Ullbro C, Lundin S-A, Koch G. Aetiology of severe demarcated enamel opacities–an evaluation based on prospective medical and social data from 17,000 children. Swed Dent J. (2011) 35:57–67.
99. Pegelow M, Alqadi N, Karsten AL-A. The prevalence of various dental characteristics in the primary and mixed dentition in patients born with non-syndromic unilateral cleft lip with or without cleft palate. Eur J Orthod. (2012) 34:561–70. doi: 10.1093/ejo/cjr074
100. Malanczuk T, Opitz C, Retzlaff R. Structural changes of dental enamel in both dentitions of cleft lip and palate patients. J Orofac Orthop Fortschritte Kieferorthopadie Organ. (1999) 60:259–68. doi: 10.1007/BF01299784
101. Carpentier S, Ghijselings E, Schoenaers J, Carels C, Verdonck A. Enamel defects on the maxillary premolars in patients with cleft lip and/or palate: a retrospective case-control study. Eur Arch Paediatr Dent. (2014) 15:159–65. doi: 10.1007/s40368-013-0078-8
102. Korolenkova MV, Starikova NV, Udalova NV. The role of external aetiological factors in dental anomalies in non-syndromic cleft lip and palate patients. Eur Arch Paediatr Dent. (2019) 20:105–11. doi: 10.1007/s40368-018-0397-x
103. Dixon DA. Defects of structure and formation of the teeth in persons with cleft palate and the effect of reparative surgery on the dental tissues. Oral Surg Oral Med Oral Pathol. (1968) 25:435–46. doi: 10.1016/0030-4220(68)90019-4
104. Niswander JD, Sujaku C. Relationship of enamel defects of permanent teeth to retention of deciduous tooth fragments. J Dent Res. (1962) 41:808–14. doi: 10.1177/00220345620410041201
105. Rule JT, Zacherl WA, Pfefferle AM. The relationship between ankylosed primary molars and multiple enamel defects. ASDC J Dent Child. (1972) 39:29–35.
106. Williamson JJ. Trauma during exodontia. An aetiologic factor in hypoplastic premolars. Br Dent J. (1966) 121:284–9.
107. Andreasen JO, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. II. A clinical and radiographic follow-up study of 213 teeth. Scand J Dent Res. (1971) 79:284–94. doi: 10.1111/j.1600-0722.1971.tb02014.x
108. Skaare AB, Aas A-LM, Wang NJ. Enamel defects on permanent successors following luxation injuries to primary teeth and carers' experiences. Int J Paediatr Dent. (2015) 25:221–8. doi: 10.1111/ipd.12136
109. Ravn JJ. Developmental disturbances in permanent teeth after exarticulation of their primary predecessors. Scand J Dent Res. (1975) 83:131–4. doi: 10.1111/j.1600-0722.1975.tb01190.x
110. de Amorim CS, Americano GCA, Moliterno LFM, de Marsillac MWS, Andrade MRTC, Campos V. Frequency of crown and root dilaceration of permanent incisors after dental trauma to their predecessor teeth. Dent Traumatol. (2018) 34:401–5. doi: 10.1111/edt.12433
111. Holan G, Topf J, Fuks AB. Effect of root canal infection and treatment of traumatized primary incisors on their permanent successors. Endod Dent Traumatol. (1992) 8:12–5. doi: 10.1111/j.1600-9657.1992.tb00219.x
112. McCormick J, Filostrat DJ. Injury to the teeth of succession by abscess of the temporary teeth. J Dent Child. (1967) 34:501–4.
113. Lo ECM, Zheng CG, King NM. Relationship between the presence of demarcated opacities and hypoplasia in permanent teeth and caries in their primary predecessors. Caries Res. (2003) 37:456–61. doi: 10.1159/000073400
114. Broadbent JM, Thomson WM, Williams SM. Does caries in primary teeth predict enamel defects in permanent teeth? A longitudinal study. J Dent Res. (2005) 84:260–4. doi: 10.1177/154405910508400310
115. Pindborg JJ. Dental mutilation and associated abnormalities in Uganda. Am J Phys Anthropol. (1969) 31:383–9. doi: 10.1002/ajpa.1330310313
116. Dinur N, Becker T, Levin A, Zadik Y, Itzhak JB, Azizi H, et al. Long-term dental implications of infant oral mutilation: a case series. Br Dent J. (2021) 231:335–40. doi: 10.1038/s41415-021-3456-3
117. Balmer R, Toumba J, Godson J, Duggal M. The prevalence of molar incisor hypomineralisation in Northern England and its relationship to socioeconomic status and water fluoridation. Int J Paediatr Dent. (2012) 22:250–7. doi: 10.1111/j.1365-263X.2011.01189.x
118. Saitoh M, Nakamura Y, Hanasaki M, Saitoh I, Murai Y, Kurashige Y, et al. Prevalence of molar incisor hypomineralization and regional differences throughout Japan. Environ Health Prev Med. (2018) 23:55. doi: 10.1186/s12199-018-0748-6
119. Wuollet E, Laisi S, Salmela E, Ess A, Alaluusua S. Background factors of molar-incisor hypomineralization in a group of Finnish children. Acta Odontol Scand. (2014) 72:963–9. doi: 10.3109/00016357.2014.931459
120. Sevbitov A, Kuznetsova M, Dorofeev A, Borisov V, Mironov S, Iusupova I. Dental anomalies in people living in radionuclide-contaminated regions. J Environ Radioact. (2020) 216:106190. doi: 10.1016/j.jenvrad.2020.106190
121. Ngoc VTN, Huong LT, Van Nhon B, Tan NTM, Van Thuc P, Hien VTT, et al. The higher prevalence of developmental defects of enamel in the dioxin-affected region than non-dioxin-affected region: result from a cross-sectional study in Vietnam. Odontology. (2019) 107:17–22. doi: 10.1007/s10266-018-0358-1
122. Lawson BF, Stout FW, Ahern DE, Sneed WD. The incidence of enamel hypoplasia associated with chronic pediatric lead poisoning. S C Dent J. (1971) 29:5–10.
123. Jan J, Vrbic V. Polychlorinated biphenyls cause developmental enamel defects in children. Caries Res. (2000) 34:469–73. doi: 10.1159/000016625
124. Jackson RD, Kelly SA, Katz B, Brizendine E, Stookey GK. Dental fluorosis in children residing in communities with different water fluoride levels: 33-month follow-up. Pediatr Dent. (1999) 21:248–54.
125. Alaluusua S, Lukinmaa PL, Koskimies M, Pirinen S, Hölttä P, Kallio M, et al. Developmental dental defects associated with long breast feeding. Eur J Oral Sci. (1996) 104:493–7. doi: 10.1111/j.1600-0722.1996.tb00131.x
126. Alaluusua S, Calderara P, Gerthoux PM, Lukinmaa P-L, Kovero O, Needham L, et al. Developmental dental aberrations after the dioxin accident in Seveso. Environ Health Perspect. (2004) 112:1313–8. doi: 10.1289/ehp.6920
127. Alaluusua S, Lukinmaa PL, Vartiainen T, Partanen M, Torppa J, Tuomisto J. Polychlorinated dibenzo-p-dioxins and dibenzofurans via mother's milk may cause developmental defects in the child's teeth. Environ Toxicol Pharmacol. (1996) 1:193–7. doi: 10.1016/1382-6689(96)00007-5
128. Hölttä P, Kiviranta H, Leppäniemi A, Vartiainen T, Lukinmaa PL, Alaluusua S. Developmental dental defetcts in childre who reside by a river polluted by dioxins and furans. Arch Environ Health. (2001) 56:522–8. doi: 10.1080/00039890109602901
129. Grahnén H, Sjölin S, Stenström A. Mineralization defects of primary teeth in children born pre-term. Scand J Dent Res. (1974) 82:396–400. doi: 10.1111/j.1600-0722.1974.tb00392.x
130. Nikiforuk G, Fraser D. The etiology of enamel hypoplasia: a unifying concept. J Pediatr. (1981) 98:888–93. doi: 10.1016/S0022-3476(81)80580-X
131. Norén JG. Enamel structure in deciduous teeth from low-birth-weight infants. Acta Odontol Scand. (1983) 41:355–62. doi: 10.3109/00016358309162347
132. Pindborg JJ. Aetiology of developmental enamel defects not related to fluorosis. Int Dent J. (1982) 32:123–34.
133. Davidovich E, Davidovits M, Eidelman E, Schwarz Z, Bimstein E. Pathophysiology, therapy, and oral implications of renal failure in children and adolescents: an update. Pediatr Dent. (2005) 27:98–106.
134. Aine L, Mäki M, Collin P, Keyriläinen O. Dental enamel defects in celiac disease. J Oral Pathol Med. (1990) 19:241–5. doi: 10.1111/j.1600-0714.1990.tb00834.x
135. Norén JG. Microscopic study of enamel defects in deciduous teeth of infants of diabetic mothers. Acta Odontol Scand. (1984) 42:153–6. doi: 10.3109/00016358408993866
136. Krasuska-Sławińska E, Dembowska-Bagińska B, Brozyna A, Olczak-Kowalczyk D, Czarnowska E, Sowińska A. Changes in the chemical composition of mineralised teeth in children after antineoplastic treatment. Contemp Oncol Poznan Pol. (2018) 22:37–41. doi: 10.5114/wo.2018.74392
137. Hileman CO, Eckard AR, McComsey GA. Bone loss in HIV: a contemporary review. Curr Opin Endocrinol Diabetes Obes. (2015) 22:446–51. doi: 10.1097/MED.0000000000000200
138. Bhatia SK, Goyal A, Dubey M, Kapur A, Ritwik P. Congenital Rubella Syndrome: dental manifestations and management in a 5 year old child. J Clin Pediatr Dent. (2012) 37:71–5. doi: 10.17796/jcpd.37.1.m8281502231550u2
139. Kraus BS, Ames MD, Clark GR. Special review: effects of maternal Rubella on dental crown development. Clin Pediatr. (1969) 8:204–15. doi: 10.1177/000992286900800408
140. Billings RJ, Berkowitz RJ, Watson G. Teeth. Pediatrics. (2004) 113(Suppl. 3):1120–7. doi: 10.1542/peds.113.S3.1120
141. Maurin JC, Bleicher F, Magloire H. [Clinical consequences of dioxins exposure during tooth development]. Arch Pediatr Organe. (2005) 12:1636–40. doi: 10.1016/j.arcped.2005.06.012
142. Rodd HD, Graham A, Tajmehr N, Timms L, Hasmun N. Molar incisor hypomineralisation: current knowledge and practice. Int Dent J. (2020) 71:285–91. doi: 10.1111/idj.12624
143. Jälevik B, Norén J. Enamel hypomineralization of permanent first molars: a morphological study and survey of possible aetiological factors. Int J Paediatr Dent Br Paedodontic Soc Int Assoc Dent Child. (2001) 10:278–89. doi: 10.1046/j.1365-263x.2000.00210.x
144. Atar M, Körperich EJ. Systemic disorders and their influence on the development of dental hard tissues: a literature review. J Dent. (2010) 38:296–306. doi: 10.1016/j.jdent.2009.12.001
145. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
146. Willmott NS, Bryan R a. E, Duggal MS. Molar-incisor-hypomineralisation: a literature review. Eur Arch Paediatr Dent. (2008) 9:172–9. doi: 10.1007/BF03262633
147. Bensi C, Costacurta M, Belli S, Paradiso D, Docimo R. Relationship between preterm birth and developmental defects of enamel: a systematic review and meta-analysis. Int J Paediatr Dent. (2020) 30:676–86. doi: 10.1111/ipd.12646
148. Fulton A, Amlani M, Parekh S. Oral manifestations of vitamin D deficiency in children. Br Dent J. (2020) 228:515–8. doi: 10.1038/s41415-020-1424-y
149. Ranta R. A review of tooth formation in children with cleft lip/palate. Am J Orthod Dentofac Orthop. (1986) 90:11–8. doi: 10.1016/0889-5406(86)90022-3
150. Ioannou S, Sassani S, Henneberg M, Henneberg RJ. Diagnosing congenital syphilis using Hutchinson's method: differentiating between syphilitic, mercurial, and syphilitic-mercurial dental defects. Am J Phys Anthropol. (2016) 159:617–29. doi: 10.1002/ajpa.22924
151. Abanto Alvarez J, Rezende KMPC, Marocho SMS, Alves FBT, Celiberti P, Ciamponi AL. Dental fluorosis: exposure, prevention and management. Med Oral Patol Oral Cirugia Bucal. (2009) 14:E103–7.
152. Chałas R, Rudzka O, Wójcik-Checińska I, Vodanović M. The impact of type 1 diabetes on the development of the craniofacial mineralised tissues (bones and teeth): literature review. Folia Morphol. (2016) 75:275–80. doi: 10.5603/FM.a2016.0001
153. Carrillo CM, Corrêa FNP, Lopes NNF, Fava M, Odone Filho V. Dental anomalies in children submitted to antineoplastic therapy. Clin São Paulo Braz. (2014) 69:433–7. doi: 10.6061/clinics/2014(06)11
154. Bianchi S, Bernardi S, Belli M, Varvara G, Macchiarelli G. Exposure to persistent organic pollutants during tooth formation: molecular mechanisms and clinical findings. Rev Environ Health. (2020) 35:303–10. doi: 10.1515/reveh-2019-0093
155. Alaluusua S, Lukinmaa P-L. Developmental dental toxicity of dioxin and related compounds–a review. Int Dent J. (2006) 56:323–31. doi: 10.1111/j.1875-595X.2006.tb00336.x
156. Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. (2004) 7:201–26. doi: 10.1079/PHN2003589
157. Serna Muñoz C, Ortiz Ruiz AJ, Pérez Silva A, Bravo-González LA, Vicente A. Second primary molar hypomineralisation and drugs used during pregnancy and infancy. A systematic review. Clin Oral Investig. (2020) 24:1287–97. doi: 10.1007/s00784-019-03007-7
158. Serna C, Vicente A, Finke C, Ortiz AJ. Drugs related to the etiology of molar incisor hypomineralization: a systematic review. J Am Dent Assoc. (2016) 147:120–30. doi: 10.1016/j.adaj.2015.08.011
159. Giro CM. Enamel hypoplasia in human teeth; an examination of its causes. J Am Dent Assoc. (1947) 34:310–7. doi: 10.14219/jada.archive.1947.0073
160. Dulla JA, Meyer-Lueckel H. Molar-incisor hypomineralisation: narrative review on etiology, epidemiology, diagnostics and treatment decision. Swiss Dent J. (2021) 131.
161. Salanitri S, Seow WK. Developmental enamel defects in the primary dentition: aetiology and clinical management. Aust Dent J. (2013) 58: 133–40; quiz 266. doi: 10.1111/adj.12039
162. da Cunha Coelho ASE, Mata PCM, Lino CA, Macho VMP, Areias CMFGP, Norton APMAP, et al. Dental hypomineralization treatment: a systematic review. J Esthet Restor Dent. (2019) 31:26–39. doi: 10.1111/jerd.12420
163. Garot E, Rouas P, Somani C, Taylor GD, Wong F, Lygidakis NA. An update of the aetiological factors involved in molar incisor hypomineralisation (MIH): a systematic review and meta-analysis. Eur Arch Paediatr Dent. (2021). doi: 10.1007/s40368-021-00646-x. [Epub ahead of print].
164. van Amerongen WE, Kreulen CM. Cheese molars: a pilot study of the etiology of hypocalcifications in first permanent molars. ASDC J Dent Child. (1995) 62:266–9.
165. Seow WK, Masel JP, Weir C, Tudehope DI. Mineral deficiency in the pathogenesis of enamel hypoplasia in prematurely born, very low birthweight children. Pediatr Dent. (1989) 11:297–302.
166. Peacock M. Phosphate metabolism in health and disease. Calcif Tissue Int. (2021) 108:3–15. doi: 10.1007/s00223-020-00686-3
167. Vorrink SU, Domann FE. Regulatory crosstalk and interference between the xenobiotic and hypoxia sensing pathways at the AhR-ARNT-HIF1α signaling node. Chem Biol Interact. (2014) 218:82–8. doi: 10.1016/j.cbi.2014.05.001
168. Parks SK, Cormerais Y, Pouysségur J. Hypoxia and cellular metabolism in tumour pathophysiology. J Physiol. (2017) 595:2439–50. doi: 10.1113/JP273309
169. Busbee PB, Rouse M, Nagarkatti M, Nagarkatti PS. Use of natural AhR ligands as potential therapeutic modalities against inflammatory disorders. Nutr Rev. (2013) 71:353–69. doi: 10.1111/nure.12024
171. Jeremias F, Pierri RAG, Souza JF, Fragelli CMB, Restrepo M, Finoti LS, et al. Family-based genetic association for molar-incisor hypomineralization. Caries Res. (2016) 50:310–8. doi: 10.1159/000445726
172. Taji SS, Seow WK, Townsend GC, Holcombe T. Enamel hypoplasia in the primary dentition of monozygotic and dizygotic twins compared with singleton controls. Int J Paediatr Dent. (2011) 21:175–84. doi: 10.1111/j.1365-263X.2010.01106.x
173. Lygidakis NA, Dimou G, Marinou D. Molar-incisor-hypomineralisation (MIH) A retrospective clinical study in Greek children. II. Possible medical aetiological factors. Eur Arch Paediatr Dent. (2008) 9:207–17. doi: 10.1007/BF03262637
174. Gernand AD, Schulze KJ, Stewart CP, West KP, Christian P. Micronutrient deficiencies in pregnancy worldwide: health effects and prevention. Nat Rev Endocrinol. (2016) 12:274–89. doi: 10.1038/nrendo.2016.37
175. Larigot L, Juricek L, Dairou J, Coumoul X. AhR signaling pathways and regulatory functions. Biochim Open. (2018) 7:1–9. doi: 10.1016/j.biopen.2018.05.001
176. Dos Reis HLB, Araujo K da S, Ribeiro LP, Da Rocha DR, Rosato DP, Passos MRL, et al. Preterm birth and fetal growth restriction in HIV-infected Brazilian pregnant women. Rev Inst Med Trop São Paulo. (2015) 57:111–20. doi: 10.1590/S0036-46652015000200003
177. Žemgulyte S, Vasiliauskiene I, Slabšinskiene E, Sandunaite K, Narbutaite J. Influence of preterm birth for child's oral health status. Stomatologija. (2019) 21:107–12.
178. Garg N, Jain AK, Saha S, Singh J. Essentiality of early diagnosis of molar incisor hypomineralization in children and review of its clinical presentation, etiology and management. Int J Clin Pediatr Dent. (2012) 5:190–6. doi: 10.5005/jp-journals-10005-1164
179. Murray GS, Johnsen DC. Hearing deficits correlated with the timing of systemic disturbance as indicated by primary incisor defects. Ear Hear. (1985) 6:255–9. doi: 10.1097/00003446-198509000-00006
180. Bhat M, Nelson KB. Developmental enamel defects in primary teeth in children with cerebral palsy, mental retardation, or hearing defects: a review. Adv Dent Res. (1989) 3:132–42. doi: 10.1177/08959374890030021101
Keywords: enamel, defect, scoping review, acquired—etiology, protective factor, risk factor
Citation: Collignon A-M, Vergnes J-N, Germa A, Azogui S, Breinig S, Hollande C, Bonnet A-L and Nabet C (2022) Factors and Mechanisms Involved in Acquired Developmental Defects of Enamel: A Scoping Review. Front. Pediatr. 10:836708. doi: 10.3389/fped.2022.836708
Received: 15 December 2021; Accepted: 20 January 2022;
Published: 24 February 2022.
Edited by:
Sreekanth Kumar Mallineni, Majmaah University, Saudi ArabiaReviewed by:
Jayakumar Jayaraman, Virginia Commonwealth University, United StatesCopyright © 2022 Collignon, Vergnes, Germa, Azogui, Breinig, Hollande, Bonnet and Nabet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne-Margaux Collignon, YW5uZS1tYXJnYXV4LmNvbGxpZ25vbkB1LXBhcmlzLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.