
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr., 07 April 2022
Sec. General Pediatrics and Pediatric Emergency Care
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.826262
This article is part of the Research TopicBuilding Capacity for Sickle Cell Disease Research and HealthcareView all 16 articles
 Maddalena Martella1
Maddalena Martella1 Mimma Campeggio1
Mimma Campeggio1 Gift Pulè2
Gift Pulè2 Ambroise Wonkam2Federica Menzato1Vania Munaretto1
Ambroise Wonkam2Federica Menzato1Vania Munaretto1 Giampietro Viola1Sabado P. Da Costa3Giulia Reggiani1Antonia Araujo3Dionisio Cumbà4Giuseppe Liotta5Laura Sainati1Fabio Riccardi5,6
Giampietro Viola1Sabado P. Da Costa3Giulia Reggiani1Antonia Araujo3Dionisio Cumbà4Giuseppe Liotta5Laura Sainati1Fabio Riccardi5,6 Raffaella Colombatti1,6*
Raffaella Colombatti1,6*Background: Sickle Cell Disease (SCD) is an inherited condition that is widespread globally and especially in malaria-endemic West African countries. Limited epidemiological data on SCD are available for Guinea Bissau, where newborn screening is not yet implemented, routine diagnosis is not available, and care is case directed.
Methods: Dried blood spots were collected from children accessing two hospitals managed by Italian Non-Governmental Organizations in the capital city of Bissau and sent to Padova for Hemoglobin (Hb) quantification through HPLC and molecular analysis. Beta globin gene analysis was performed in all; and Hb haplotype of the HbSS and HbSA patients was performed in South Africa. One hundred samples belonging to the most frequent ethnic groups were randomly selected for detection of G6PD mutations.
Results: Samples from 848 consecutive children (498 males and 350 females, mean age 6.8 years) accessing the two hospitals were analyzed: 6.95% AS (4.42% allelic frequency), 0.94% SS, and 0.23% AC. 376G G6PD allelic frequency was 24%; 14.8% in AS individuals. The Senegal haplotype was the most prevalent (31%), and the proposition of chromosomes with the atypical haplotype was surprisingly high (56%).
Conclusion: Our study demonstrates a significant frequency of the HbS allele in the population of Guinea Bissau supporting the implementation of screening strategies. The differences among ethnic groups can help guide targeted interventions for SCD awareness campaigns and determine priority areas for public health interventions. The pilot analysis on haplotypes reveals a large proportion of the atypical haplotype, which may be indicative of a genetically heterogeneous population.
Sickle Cell Disease (SCD) is an inherited condition frequently found in people of African descent. SCD is the most common monogenic disease worldwide (1) and is recognized by the World Health Organization (WHO) and the United Nations (UN) as a global public health problem. A call to action was launched by the two organizations in 2006 and 2008 due to the burden of SCD on childhood mortality in sub-Saharan Africa, as it contributes to 9-16% of deaths in children under 5 years of age on that continent (2–4). Neonatal screening, penicillin prophylaxis, immunization, and stroke prevention have dramatically increased survival for patients with SCD in developed countries but they are seldom available in Africa (5, 6), where the majority of patients live. Recent population movements have increased the number of people carrying the HbS allele coming to Europe, thereby challenging health systems to adapt to this particular group of patients with SCD (7–10).
Guinea Bissau (Supplementary Figure 1), a former Portuguese colony located in the West African Atlantic Coast, embedded between Senegal and Guinea Conakry, lies in the malaria belt. Malaria is endemic in the country with a peak transmission during the rainy season (July–October). Guinea Bissau has a population of 1,726,170 inhabitants and children aged 0–14 years constitute 39.53% (male 340,575/female 341,747). The capital of Bissau has 492,000 inhabitants (2015). The population is multi-ethnic, because more than 20 ethnic groups are present in the country, the most frequent being Balanta and Fula (11). The official national language is Portuguese-creole, although many people speak only the local languages.
In spite of the high prevalence of SCD in the surrounding West African countries, like Senegal, Mali, Guinea Conakry, and Liberia (12–14), there are limited data on the frequency of HbS (15) in Guinea Bissau. The actual health burden of SCD in the country is not known and there are no national SCD screening programs yet.
Accurate epidemiologic information is necessary for the development of sustainable health interventions and targeted health education and prevention programs in the field of SCD. The two main objectives of our pilot study were, therefore, to determine the feasibility of a SCD screening program in two hospitals in the capital city of Bissau (in terms of capacity of correct sample collection, data recording and affected patient tracking and counseling), and to determine the prevalence of SCD among the various ethnic groups of Bissau. These data, collected through a public-private partnership with non-Governmental organizations (NGOs), could help develop further research in the field of SCD in Guinea-Bissau.
This cross-sectional study took place in two hospitals in the capital city, Bissau: the Raoul Follereau Hospital (HRF, public hospital) and the Bor Children's Hospital (BCH, private hospital), both managed within the National Health System of Guinea Bissau by Italian NGOs that had already conducted projects regarding children's health in the country (16–20).
Doctors and laboratory technicians received training on SCD and sample collection in December 2012. Sample collection began during the same month, using leftover blood from samples of children who consecutively accessed both hospitals in the following 8 months. During a routine clinical visit for any health reason in which a blood sample collection was planned for other purposes, parents were offered the possibility to perform the HbS analysis utilizing the leftover blood of their child. In case of acceptance, dried blood spots were prepared from the already drawn blood samples. Basic demographics (age, gender, ethnic group, residence) were collected for each patient in a dedicated paper form and transferred to excel for data analysis.
The study was approved by the local hospital ethics board and oral informed consent was collected from the parents.
After oral informed consent from parents, peripheral blood samples were collected on filter paper (Whatman™ 3MM Chr Chromatography Paper). The blood spots were air dried at room temperature, individually wrapped in aluminum film, placed in a single envelope, kept in the dark, and in a location without humidity to ensure the integrity of the sample during the processes of collection, storage, and transport. Every “collection card” had 4–5 blood spots with demographic and ethno-linguistic records. The samples were shipped via courier to the Laboratory of Pediatric Onco-Haematology of University of Padova, Italy for processing. At arrival in Padua, all samples underwent Bglobin gene molecular analysis and High-performance Liquid Chromatography (HPLC) analysis. After genetic analysis, the DNA from HbAS and HbSS subjects was shipped to South Africa to determine the Hb haplotype.
Analyses were performed on all samples with the Alliance e2695 liquid chromatography (Waters) connected with a UV-Vis detector (Waters 2489), and settled at 415 nm. The system was equipped with a 35 length × 4.6 I.D. mm, chromatography column packed with a strong cation-exchanger, 6.5 μm microparticulate (IEC SP-420N, Shodex).
The gradient was made up of mobile phase A [MES, 2-(N-morpholino) ethanesulfonic acid 20 mM, pH = 5.6] and mobile phase B (MES+ Na2SO4 0.5 M, pH = 5.6) with a flow rate of 1 ml/min. After injection of the sample, the proportion of B was increased linearly to B:A (90:10) at 5 min and to 100:0 at 9 min; finally, the mobile phase was returned to A:B 95:5 at 11 min, for equilibration.
Genomic DNA of high molecular weight, extracted according to the QIAGEN protocol by dried blood spot, was subjected to amplification (Applied Biosiystems Thermal Cycler 2720) of the exons of the β-globin and direct sequencing. DNA samples that were heterozygous HbS/HbA were also analyzed at exon 2 and 3.
The entire coding sequence of the βglobin gene, 11p15.5 (NM_000518; OMIM#603903), was PCR-amplified with 30 cycles reactions at 94°C for 1 min, at 56°C for 1 min and at 72°C for 1 min. The reaction was done in a final volume of 50 μl comprising 50 ng DNA, Buffer II 10X, MgCl2 Solution 25 mM, dNTP's 10 mM, Primers 100 μM, AmpliTaq Gold DNA Polymerase 5 u/μl. The purified PCR products were subjected to direct sequencing (3500Dx Genetic Analyzer, Applied Biosystems).
The concentration and purity of each DNA sample was determined by Nanodrop spectrophotometry and dilutions of 100 ng/μL concentration were used for all reactions. A previously optimized 5 restriction-site PCR protocol was used for the SCD haplotype analysis. The reaction comprised 5 μL GoTaq 5X colorless buffer (Promega, USA), 1 μL dNTPs (Fermentas, USA), 0.5 μL of each primer (iDT, RSA), 0.1 μL GoTaq (Promega, USA), 1 μL DNA and made up to 25 μL with distilled water. Briefly, the reaction was cycled on the BIO-RAD Thermal cycler (BIO-RAD T100, USA) at 95°C for 5 min, 35 cycles of 94°C for 30 s, 53 or 55°C for 40 s, 72°C for 2 min and lastly kept at 72°C for 7 min. To confirm correct amplification, a 2% agarose gel (Seakem Lonza, RSA) was prepared in 1 X TBE buffer to visualize the amplicons using SYBR Safe DNA gel stain (Invitrogen, Life Technologies SA). The electrophoresis was carried out for approximately 60 min at 160 V and gel images were acquired using a protected imaging capture system (UVIPro Gold transilluminator, UK). To genotype the samples, restriction digests were done using 0.5 or 1 μL of the specific restriction enzyme (Promega, USA), 2 μL of the associated buffer (Promega, USA), 10 μL PCR product and made up to 15 μL using sterile deionized water. The digests were incubated overnight at 37°C on a thermal cycler (BIO-RAD T100, USA) and electrophoresed on a 2% agarose gel for 60 min at 160 V. Visualization was done using the UVIPro Gold transilluminator (UVItec, UK).
G6PD genetic variants that confer resistance to severe malaria including 202, 376, 542, 680, and 968 A-deficiency polymorphisms referred as G6PD202, G6PD376, G6PD542, were evaluated after performing HPLC and HbS molecular Analysis in 100 randomly selected DNA samples belonging to the five more frequent ethnic groups (Balanta, Fula, Papel, Manjaco, Mandingo), and in HbS gene carriers who had DNA remaining for the analysis.
The coding sequence of exons analyzed of the G6PD gene, Xq28 (NM_X03674; OMIM#305900), for G202A, A376G, A542T, T968C polymorphisms, was PCR-amplified with 30-cycle reactions at 94°C for 1 min, at 58°C for 1 min and at 72°C for 1 min. The reaction was done in a final volume of 50 μl comprising 50 ng DNA, Buffer II 10X, MgCl2 Solution 25 mM, dNTP's 10 mM, Primers 100 μM, AmpliTaq Gold DNA Polymerase 5 u/μl.
The amplification products for G6PD202, G6PD376, G6PD542, G6PD968 polymorphisms were subjected to direct sequencing (3500Dx Genetic Analyzer, Applied Biosystems), instead the product PCR for G6PD680 was digested with BstNI restriction enzyme (New England, BioLabs): 4 μl PCR product with 2 μl of enzyme at 60°C for 15 min.
Eight doctors and three technicians from the two hospitals were trained on SCD and sampling techniques through several on site meetings. Accessing the two hospitals consecutively, 848 children (503 from BCH 345 from HRF) were tested comprising of 498 males and 350 females, with a mean age of 6.8 years (range: 1–16). The children belonged to the most frequent ethnic groups of Guinea Bissau (Table 1). The families all resided in the capital city and came from different parts of town.
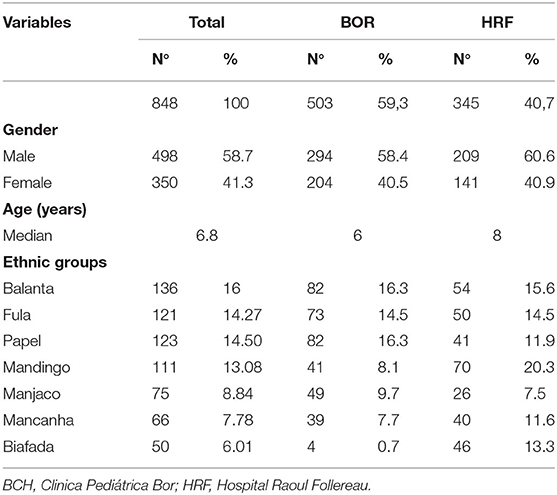
Table 1. Basic demographics of the pediatric population in the two hospitals.
The blood samples collected on absorbent paper were of excellent quality.
HBB molecular analysis identified 8 individuals with Hb SS SCD (0.94%) (mean age 7.27 years), 59 individuals with HbSA (6.95 %) (mean age 6.05 years), 2 individuals with HbAC (0.23%) (mean age 2 years), 1 individual bearer of a sequence variant samesense (0.19 %) (8 years). None had HbSC or HbSβthalassemia, frequent in other West African countries.
HbS allelic frequency was 4.42%. Details are given in Table 2.
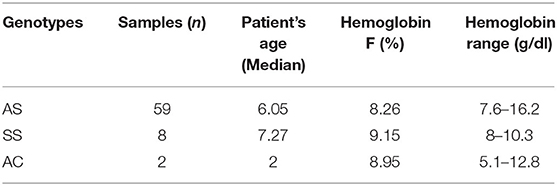
Table 2. Genotype and hemoglobin F %.
A significant difference in the frequency of HbS was found between ethnic groups: Fulas 25.42%, Mandingas 18.64%, Pepel 11.86%, Mandjau 6.77%, Biafada 13.55%, 10.16% Balanta, and 11.86% the others (Table 3).
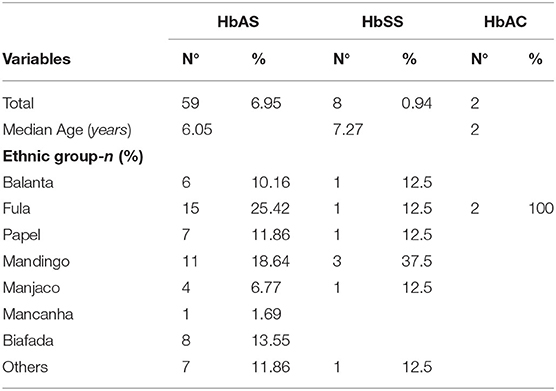
Table 3. Distribution of abnormal hemoglobin in the different ethnic groups.
Thirty-two patients with the HbS gene had enough genetic material to be analyzed for the SCD haplotype background: 5 HbSS and 27 HbAS. Sixty-four chromosomes were therefore analyzed.
The Senegal haplotype was the most prevalent of all 5 SCD haplotypes with 31% (n = 20) followed by Cameroon haplotype with 11% (n = 7), with 1 chromosome from the Benin haplotype (2%). There was neither the Indian-Arab nor Central African haplotypes in this study (Supplementary Table 1; Supplementary Figure 2). The proposition of chromosomes with the atypical haplotype was surprisingly high (56%; n = 30) with 83.3% (n = 30) positive for the HinfI(5'β) restriction site.
One hundred forty-one samples were analyzed for G6PD: 100 randomly selected samples of the five more frequent ethnic groups (20 each from Balanta, Fula Pepel, Mandjaco, Mandingo) with HbAA genotype, 37 samples from individuals with HbAS, and 4 samples from HbSS individuals (details in Supplementary Table 2) according to the availability of DNA.
Mutational analysis with PCR and direct sequencing of the G6PD gene showed the presence of 376G and 968G alleles, not 202A, 542T, and 680T.
376G allele is 35% of 100 samples belonging to five ethnic groups more frequent in the population, and 21.6% of HbAS carriers with allelic frequency, respectively, of 24 and 14.8%.
G6PD molecular analysis in HbSS samples gave no significant results.
Interestingly, differences are noted between different ethnic groups: 11/35 (31.4%) 376G individuals are Fulas (1 homozygous female, and 5 heterozygotes, 5 hemizigous males); 8/37 (21.6%) HbAS samples have 376G and 3/8 (37.5%) are Fulas.
Allele 968G is 8% of 100 samples evenly distributed between five ethnic groups (1 homozygous female, and 3 heterozygotes, 4 hemizigous males), 2.7% of SCD HbAS and 25% of HbSS patients, 37.5% of AS and 25% of SS are Fulas. The percentage of 376G/968G is the same between different ethnic groups.
Figure 1 displays the distribution of G6PD mutation and HbS allele in the three main ethnic groups.
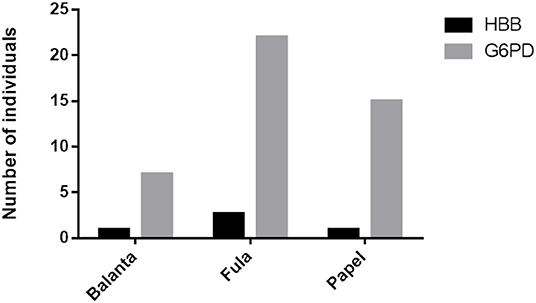
Figure 1. Distribution of the HbS allele (HBB mutation) and the G6PD mutation in the three main ethnic groups: Balanta, Fula, and Papel.
In this first study after the publication of the 2008 UN recommendation to strengthen SCD programs throughout the world (21), we found higher prevalence of HbS allele in a pediatric population in Bissau, Guinea-Bissau, compared to previous studies (15), confirming the need to develop nationwide SCD screening and comprehensive care programs in the country. Moreover, our results demonstrate the feasibility of good sample collection by staff that has been adequately trained within the framework of North-South and South-South international collaborative projects.
The overall HbS allelic frequency was 4.42%, lower than neighboring countries. The prevalence of HbSA carriers also seems lower, which was 6.95% (12–14). Interestingly, the prevalence of the carrier state was different in the various ethnic groups, being higher in the Fula and the Mandingo. Minor differences were also observed among ethnic groups in the neighboring Republic of Guinea (22), although not as high. Specific characteristics of Guinea Bissau might justify this data. It is a very secluded country, with less connections to the other West African countries and to Europe, with a widely spread rural population and significant numbers of interfamily marriages between some of the ethnic groups. The country is therefore not new to unique epidemiological characteristics. It was, for example, the only country in which HIV 2 was more widespread than HIV 1 in the past decades (23); and multidrug resistant uberculosis (TB) has lower incidence than in other West-African countries (24). Furthermore, the very high maternal and infant mortality rates of Guinea Bissau (child mortality rates are the highest worldwide at 152.5 per 1,000 livebirths) (25), as well as the increased risk of stillbirth in SA carriers (26), could justify a higher number of children with SS dying earlier and not being diagnosed. Also, there is a lower rate of HbSA children being born from S carrier mothers. Moreover, the relatively high mean age of our pediatric cohort (mean age 6.8 years) and of the children with SCD (mean age 7.27 years) could have excluded children with SCD who might have died before 5 years of age (4). Taken together, these data reinforce the need for screening early in life, such as in newborn screening programs, in Guinea Bissau.
It is also often difficult to know exactly how the coupling of individuals in a population happens, in particular, it is difficult to know if a population presents the rule of panmixy. If there is genetic isolation between subpopulations, it is possible that there is also a certain differentiation of allele frequencies, so the population shows a deviation from the Hardy-Weinberg equilibrium, even if the balance is respected within each population (27).
While the different ethnic distribution of the HbS allele warrants a deeper understanding of the genetic background of the population and further research (28–30), it can also aid to prioritize actions for SCD, such as starting awareness campaigns and screening in areas of the country or sectors of the city where the highest rate of carriers is living. Unfortunately, Guinea Bissau has very limited resources allocated to health care and other urgent health priorities like infectious diseases -HIV, TB, and cholera which catalyzed health care energy and resources in the past years. No resources were available for non-communicable diseases. Implementing screening in a stepwise manner with a priority list could be beneficial in this limited resource setting.
The co-existence of the HbS allele and the G6PD mutation in the setting of Guinea Bissau is important for phenotypic variability of hematological diseases. In fact, G6PD has been shown to influence severity of hemolysis and cerebrovascular manifestations (31–33). Moreover, the G6PD 376G allele is present in 35% of the HbAA samples and in 21.6% of the HbAS carriers, with an allelic frequency of 24 and 14.8%, respectively. The prevalence of G6PD genotypes in HbSS and HbSA did not differ (p > 0.05) from those found in the controls. The prevalence of G6PD deficiency did not change when patients were stratified by age, suggesting that there is no advantage of the association of G6PD deficiency with HbSS.
The Senegal haplotype is the most prevalent in our cohort, followed by the Cameroon haplotype. This could justify the relatively high percentage of HbF found in our cohort as it is well known that the Senegalese haplotype presents higher HbF (34). However, there is also a large proportion of atypical haplotypes in this cohort, which may be indicative of a genetically heterogeneous population that may have high levels of admixture or be a site of early migration. In fact, atypical haplotypes not belonging to the 5 most common ones (Senegalese, Benin, Bantu, Cameroon, Arab), have been described in other populations (Brazil, Nigeria, India) and could be responsible for the extreme phenotypic diversity of SCD (34–36). Future genetic studies are needed in this field.
Our study has several limitations. First of all, the sample collection involved only children living in the capital city of Bissau and occurred in a timeframe of only 8 months due to limited funding and staff capacity. Therefore, a wider sample, including also children from rural areas might be useful to estimate the real nationwide prevalence. Secondly, the organization of the blood sample analysis was complex and cannot be reproduced on large scale. Today, several rapid tests have become available and allow point-of care testing through a less complex diagnostic pathway than the one evaluated in this study. Nevertheless, the prevalence of HbS carriers and HbSS was high and warrants the development of a newborn screening program in Guinea Bissau. The possibility to screen with the different types of rapid tests that are now on the market (37) will hopefully enhance the screening capacity, both in the urban and rural areas of Guinea Bissau, as a pilot project has demonstrated (38).
This was the first study where data on sickle cell trait and G6PD deficiency frequencies were obtained for Guinea-Bissau pediatric populations. These data contribute to the evidence of the need to develop a SCD screening program in the country. Moreover, our results support the need to further explore the genetic background of various SCD populations across Africa in order to contextualize the heterogeneous clinical phenotypes seen across the continent. Such diverse populations are ideal for more precise haplotyping techniques to investigate the genomic background of SCD in West Africa, where there is an apparent lack of literature on SCD and the understanding of genotype-phenotype correlations.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Hospital RAoul Follereau in Guinea Bissau; Ethics Committee of the Province of Padova, Padova, Italy. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
RC, FR, and MM designed the study. DC, AA, and SD collected the samples. MC, MM, FM, AW, GP, and GV performed the analysis. RC wrote the manuscript. All authors reviewed the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the Fondazione Zanetti, the Regione Friuli Venezia Giulia (Cooperazione Decentrata Grant), the Regione Veneto (Cooperazione Decentrata Grant) and Aid, Health and Development Onlus for the support for Health Structures in Guinea Bìssau and the Fondazione Città della Speranza for the support in the Sickle Cell Disease Program.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.826262/full#supplementary-material
1. Weatherall D, Hofman K, Rodgers G, Ruffin J, Hrynkow S. A case for developing North-South partnerships for research in sickle cell disease. Blood. (2005) 105:921–3. doi: 10.1182/blood-2004-06-2404
2. Aygun B, Odame I. A global perspective on sickle cell disease. Pediatr Blood Cancer. (2012) 59:386–90. doi: 10.1002/pbc.24175
3. Grosse SD, Odame I, Atrash HK, Amendah DD, Piel FB, Williams TN. Sickle cell disease in Africa: a neglected cause of early childhood mortality. Am J Prev Med. (2011) 41 (6 Suppl. 4):S398–405. doi: 10.1016/j.amepre.2011.09.013
4. Piel FB, Hay SI, Gupta S, Weatherall DJ, Williams TN. Global burden of sickle cell anaemia in children under five, 2010–2050: modelling based on demographics, excess mortality, and interventions. PLoS Med. (2013) 10:e1001484. doi: 10.1371/journal.pmed.1001484
5. Lobitz S, Telfer P, Cela E, Allaf B, Angastiniotis M, Backman Johansson C, et al. Newborn screening for sickle cell disease in Europe: recommendations from a Pan-European Consensus Conference. Br J Haematol. (2018) 183:648–60. doi: 10.1111/bjh.15600
6. Lubeck D, Agodoa I, Bhakta N, Danese M, Pappu K, Howard R, et al. Estimated life expectancy and income of patients with sickle cell disease compared with those without sickle cell disease. JAMA Netw Open. (2019) 2:e1915374. doi: 10.1001/jamanetworkopen.2019.15374
7. Piel FB, Tatem AJ, Huang Z, Gupta S, Williams TN, Weatherall DJ. Global migration and the changing distribution of sickle haemoglobin: a quantitative study of temporal trends between 1960 and 2000. Lancet Glob Health. (2014) 2:e80–9. doi: 10.1016/S2214-109X(13)70150-5
8. Inusa BPD, Colombatti R. European migration crises: the role of national hemoglobinopathy registries in improving patient access to care. Pediatr Blood Cancer. (2017) 64. doi: 10.1002/pbc.26515
9. Colombatti R, Dalla Pozza LV, Mazzucato M, Sainati L, Pierobon M, Facchin P. Hospitalization of children with sickle cell disease in a region with increasing immigration rates. Haematologica. (2008) 93:463–4. doi: 10.3324/haematol.11766
10. Colombatti R, Montanaro M, Guasti F, Rampazzo P, Meneghetti G, Giordan M, et al. Comprehensive care for sickle cell disease immigrant patients: a reproducible model achieving high adherence to minimum standards of care. Pediatr Blood Cancer. (2012) 59:1275–9. doi: 10.1002/pbc.24110
11. The World Factbook Guinea Bissau. Available online at: https://www.cia.gov/the-world-factbook/countries/guinea-bissau/ (accessed January 10, 2021).
12. Tubman VN, Marshall R, Jallah W, Guo D, Ma C, Ohene-Frempong K, et al. Newborn screening for sickle cell disease in liberia: a pilot study. Pediatr Blood Cancer. (2016) 63:671–6. doi: 10.1002/pbc.25875
13. Esoh K, Wonkam A. Evolutionary history of sickle-cell mutation: implications for global genetic medicine. Hum Mol Genet. (2021) 30:R119–28. doi: 10.1093/hmg/ddab004
14. Millimono TS, Loua KM, Rath SL, Relvas L, Bento C, Diakite M, et al. High prevalence of hemoglobin disorders and glucose-6-phosphate dehydrogenase (G6PD) deficiency in the Republic of Guinea (West Africa). Hemoglobin. (2012) 36:25–37. doi: 10.3109/03630269.2011.600491
15. Masmas TN, Garly ML, Lisse IM, Rodriques A, Petersen PT, Birgens H. Inherited hemoglobin disorders in Guinea-Bissau, West Africa: a population study. Hemoglobin. (2006) 30:355–64. doi: 10.1080/03630260600755385
16. Vieira F, Sanha MS, Riccardi F, Colombatti R. Short term advantages of a public-private partnership for tuberculosis in Guinea Bissau: reduction of mortality and increased diagnostic capacity. Mediterr J Hematol Infect Dis. (2014) 6:e2014049. doi: 10.4084/mjhid.2014.049
17. Colombatti R, Penazzato M, Bassani F, Vieira CS, Lourenço AA, Vieira F, et al. Malaria prevention reduces in-hospital mortality among severely ill tuberculosis patients: a three-step intervention in Bissau, Guinea-Bissau. BMC Infect Dis. (2011) 11:57. doi: 10.1186/1471-2334-11-57
18. Colombatti R, Vieira CS, Bassani F, Cristofoli R, Coin A, Bertinato L, et al. Contamination of drinking water sources during the rainy season in an urban post-conflict community in Guinea Bissau: implications for sanitation priority. Afr J Med Med Sci. (2009) 38:155–61.
19. Colombatti R, Coin A, Bestagini P, Vieira CS, Schiavon L, Ambrosini V, et al. A short-term intervention for the treatment of severe malnutrition in a post-conflict country: results of a survey in Guinea Bissau. Public Health Nutr. (2008) 11:1357–64. doi: 10.1017/S1368980008003297
20. Rabna P, Ramos J, Ponce G, Sanca L, Mané M, Armada A, et al. Direct detection by the Xpert MTB/RIF assay and characterization of multi and poly drug-resistant tuberculosis in Guinea-Bissau, West Africa. PLoS ONE. (2015) 10:e0127536. doi: 10.1371/journal.pone.0127536
21. UN Resolution A/63/L,.63 “Recognition of Sickle-Cell Anaemia as a Public Health Problem”. (2008). Available online at: http://www.un.org/News/Press/docs/2008/ga10803.doc.htm
22. Spivak VA, Sou A, Lutsenko IN. Distribution of abnormal hemoglobins S and C in the Republic of Guinea. Genetika. (1992) 28:159–65.
23. Esbjörnsson J, Månsson F, Kvist A, da Silva ZJ, Andersson S, Fenyö EM, et al. Long-term follow-up of HIV-2-related AIDS and mortality in Guinea-Bissau: a prospective open cohort study. Lancet HIV. (2018) 6:E25–31. doi: 10.1016/S2352-3018(18)30254-6
24. Gehre F, Otu J, Kendall L, Forson A, Kwara A, Kudzawu S, et al. The emerging threat of pre-extensively drug-resistant tuberculosis in West Africa: preparing for large-scale tuberculosis research and drug resistance surveillance. BMC Med. (2016) 14:160. doi: 10.1186/s12916-016-0704-5
25. Wang H, Liddell CA, Coates MM, Mooney MD, Levitz CE, Schumacher AE, et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2014) 384:957–79 doi: 10.1016/S0140-6736(14)60497-9
26. Canelón SP, Butts S, Boland MR. Evaluation of stillbirth among pregnant people with sickle cell trait. JAMA Netw Open. (2021) 4:e2134274. doi: 10.1001/jamanetworkopen.2021.34274
27. Piel FB, Adamkiewicz TV, Amendah D, Williams TN, Gupta S, Grosse SD. Observed and expected frequencies of structural hemoglobin variants in newborn screening surveys in Africa and the Middle East: deviations from Hardy-Weinberg equilibrium. Genet Med. (2015) 18:265–74. doi: 10.1038/gim.2015.143
28. Wonkam A, Chimusa ER, Mnika K, Pule GD, Ngo Bitoungui VJ, Mulder N, et al. Genetic modifiers of long-term survival in sickle cell anemia. Clin Transl Med. (2020) 10:e152. doi: 10.1002/ctm2.152
29. Campbell AD, Colombatti R, Andemariam B, Strunk C, Tartaglione I, Piccone CM, et al. An analysis of racial and ethnic backgrounds within the CASiRe international cohort of sickle cell disease patients: implications for disease phenotype and clinical research. J Racial Ethn Health Disparities. (2021) 8:99–106. doi: 10.1007/s40615-020-00762-2
30. Gueye Tall F, Martin C, Malick Ndour EH, Déme Ly I, Renoux C, Chillotti L, et al. Genetic background of the sickle cell disease pediatric population of Dakar, Senegal, and characterization of a novel frameshift β-thalassemia mutation [HBB: c.265_266del; p.Leu89Glufs*2]. Hemoglobin. (2017) 41:89–95. doi: 10.1080/03630269.2017.1339610
31. Gordeuk VR, Shah BN, Zhang X, Thuma PE, Zulu S, Moono R, et al. The CYB5R3(c) (.350C>G) and G6PD A alleles modify severity of anemia in malaria and sickle cell disease. Am J Hematol. (2020) 95:1269–79. doi: 10.1002/ajh.25941
32. Joly P, Garnier N, Kebaili K, Renoux C, Dony A, Cheikh N, et al. G6PD deficiency and absence of α-thalassemia increase the risk for cerebral vasculopathy in children with sickle cell anemia. Eur J Haematol. (2015) 96:404–8. doi: 10.1111/ejh.12607
33. Benkerrou M, Alberti C, Couque N, Haouari Z, Ba A, Missud F, et al. Impact of glucose-6-phosphate dehydrogenase deficiency on sickle cell anaemia expression in infancy and early childhood: a prospective study. Br J Haematol. (2013) 163:646–54. doi: 10.1111/bjh.12590
34. Adabale A, Makanjuola SBL, Akinbami A, Dosunmu A, Akanmu A, Javid FA, et al. Frequency of beta S globin gene haplotypes among sickle cell patients in Nigeria. J Int Med Res. (2021) 49:3000605211019918. doi: 10.1177/03000605211019918
35. Alves AC, da Silva VAL, Dos Santos A, Serra MB, Marques FA, Cruz SMP, et al. Sickle cell anemia in the state of Maranhao: a haplotype study. Ann Hematol. (2020) 99:1225–30. doi: 10.1007/s00277-020-04048-9
36. Okumura JV, Silva DGH, Torres LS, Belini-Junior E, Venancio LPR, Carrocini GCS, et al. Atypical beta-S haplotypes: classification and genetic modulation in patients with sickle cell anemia. J Hum Genet. (2019) 64:239–48. doi: 10.1038/s10038-018-0554-4
37. Dexter D, McGann PT. Saving lives through early diagnosis: the promise and role of point of care testing for sickle cell disease. Br J Haematol. (2022) 196:63–9. doi: 10.1111/bjh.17678
38. Menzato F, Bosa L, Sifna A, Da Silva L, Gasperoni E, Martella M, et al. Successful simultaneous screening of sickle cell disease, HIV and tuberculosis in rural Guinea Bissau, West Africa through rapid tests and a standardized clinical questionnaire: an outreach program due to a public-private partnership. Blood. (2018) 132:4715. doi: 10.1182/blood-2018-99-119006
Keywords: HbS, sickle cell, screening, Guinea Bissau, multi-ethnic, haplotypes
Citation: Martella M, Campeggio M, Pulè G, Wonkam A, Menzato F, Munaretto V, Viola G, Da Costa SP, Reggiani G, Araujo A, Cumbà D, Liotta G, Sainati L, Riccardi F and Colombatti R (2022) Distribution of HbS Allele and Haplotypes in a Multi-Ethnic Population of Guinea Bissau, West Africa: Implications for Public Health Screening. Front. Pediatr. 10:826262. doi: 10.3389/fped.2022.826262
Received: 30 November 2021; Accepted: 23 February 2022;
Published: 07 April 2022.
Edited by:
Melissa Taylor, Assistance Publique Hopitaux De Paris, FranceReviewed by:
Joséphine Brice, Université Paris Descartes, FranceCopyright © 2022 Martella, Campeggio, Pulè, Wonkam, Menzato, Munaretto, Viola, Da Costa, Reggiani, Araujo, Cumbà, Liotta, Sainati, Riccardi and Colombatti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raffaella Colombatti, cmFmZmFlbGxhLmNvbG9tYmF0dGlAdW5pcGQuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.