 Ana Luísa Leite1*
Ana Luísa Leite1* Elisa Galo2Ana Antunes3Brígida Robalo4,5Daniela Amaral6Filipa Espada7Sofia Castro8Sara Simões Dias9,10Catarina Limbert11,12
Elisa Galo2Ana Antunes3Brígida Robalo4,5Daniela Amaral6Filipa Espada7Sofia Castro8Sara Simões Dias9,10Catarina Limbert11,12- 1Unidade de Endocrinologia e Diabetologia Pediátrica, Centro Hospitalar de Vila Nova de Gaia/Espinho, EPE, Espinho, Portugal
- 2Serviço de Pediatria, Departamento de Pediatria, Hospital da criança e do Adolescente, Hospital da Luz, Lisboa, Portugal
- 3Unidade de Endocrinologia Pediátrica, Hospital de Braga, Braga, Portugal
- 4Unidade de Endocrinologia, Serviço de Pediatria, Departamento de Pediatria, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte, Lisboa, Portugal
- 5Clínica Universitária de Pediatria, Faculdade de Medicina, Universidade de Lisboa, Lisboa, Portugal
- 6Serviço de Pediatria, Hospital Lusíadas Lisboa, Lisboa, Portugal
- 7Unidade de Endocrinologia Pediátrica, Hospital Pedro Hispano, Matosinhos, Portugal
- 8Serviço de Pediatria, Centro Hospitalar Barreiro Montijo, Barreiro, Portugal
- 9EpiDoc Nova Medical School, Faculdade Ciências Médicas, Universidade Nova de Lisboa, Lisboa, Portugal
- 10ciTechCare, Center for Innovative Care and Health Technology, Escola Superior de Saúde de Leiria, Politécnico de Leiria, Leiria, Portugal
- 11Unidade de Endocrinologia Pediátrica, Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal
- 12Nova Medical School, Universidade Nova de Lisboa, Lisboa, Portugal
Introduction: There are several concerns associated with gonadotropin-releasing hormone agonist (GnRHa) treatment for central precocious puberty (CPP), such as obesity and changes in body mass index (BMI). We aimed to investigate whether any anthropometric differences exist and if they persist over time.
Methods: We conducted an observational study of Portuguese children (both sexes) diagnosed with CPP between January 2000 and December 2017, using a digital platform, in order to analyze the influence of GnRHa treatment on BMI-SD score (BMI-SDS).
Results: Of the 241 patients diagnosed with CPP, we assessed 92 patients (8% boys) in this study. At baseline, 39% of the patients were overweight. BMI-SDS increased with treatment for girls but then diminished 1 year after stopping GnRHa therapy (p = 0.018). BMI-SDS variation at the end of treatment was negatively correlated with BMI-SDS at baseline (p < 0.001). Boys grew taller and faster during treatment than did girls (p < 0.001), and therefore, their BMI-SDS trajectory might be different.
Conclusions: This study showed an increase of body weight gain during GnRHa treatment only in girls, which reversed just 1 year after stopping treatment. The overall gain in BMI-SDS with treatment is associated with baseline BMI-SDS.
Introduction
Central precocious puberty (CPP) results from the premature activation of the hypothalamic–pituitary–gonadal axis. It mimics physiological pubertal development but occurs at an inappropriate chronological age (1). It is defined by the onset of pubertal development before the age of 8 and 9 years in girls and boys, respectively (2).
In recent decades, there have been global reports of a secular trend toward the earlier onset of puberty in the general population, but disconcertingly, it seems that CPP is also increasing (3).
Early recognition of CPP facilitates appropriate and prompt intervention such as treatment with gonadotropin-releasing hormone agonists (GnRHas) or surgical intervention in certain cases such as those involving central nervous system tumors (4, 5). GnRHas are synthetic peptide analogs of hypothalamic GnRH used to suppress puberty and have been the standard of care for more than two decades for children with CPP (6). GnRHa preparations help preserve adult height (AH) and prevent/ameliorate the presumed distress associated with early maturation and menarche in girls (7).
However, the possible effects of body weight gain, obesity, and untimely metabolic changes are the major concerns associated with GnRHa use (8–10). The available data are inconsistent owing to the heterogeneity of study protocols, the small number of patients, and the exclusion of boys from previous studies (11).
Some studies have reported an association between GnRHa treatment and body mass index (BMI) increase (9, 11–13), in previously normal-weight girls (14, 15) as well as in those with obesity (16). Other studies have found no influence of GnRHa treatment on weight status (8, 17, 18), and recently, it has been proposed that the increase of BMI occurs during treatment but reverts to baseline after GnRHa is discontinued (19, 20). In the literature, only one study was conducted in boys and reported no significant change in BMI-SDS over 2 years of therapy (21).
We aimed to evaluate sex-based differences and changes in BMI in a nationally representative group of Portuguese CPP patients treated with GnRHa and followed up for a year after treatment discontinuation.
Materials and Methods
Study Design
This was an observational multicentric study of children diagnosed with CPP in Portugal between January 2000 and December 2017. A digital platform was designed to record data, and eleven pediatric endocrinology centers throughout Portugal were enrolled.
The study was approved by the Portuguese Ethics Committee (CNPD no. 1704). The research was performed in adherence to the principles laid out in the Declaration of Helsinki.
The diagnosis of CPP was clinically defined as Tanner stage II breast development in girls younger than 8 years or testicular enlargement 4 ml or greater in boys younger than 9 years with baseline luteinizing hormone (LH) level ≥0.3 IU/L or GnRHa-stimulated LH peak >5 IU/L (22). Idiopathic and other cases of CPP were included.
The exclusion criteria were as follows: (1 not receiving treatment with GnRH agonists or not having yet completed treatment; (2 use of known weight-modifying medications (e.g., antipsychotics, stimulants, and steroids); and (3 having a weight-modifying illness (e.g., inflammatory bowel disease and type 1 diabetes) or unavailability of relevant data (including no baseline anthropometric data or no follow-up data).
From an initial cohort of 241 children diagnosed with CPP, a total of 92 patients were analyzed.
Anthropometric data were collected at baseline (Time I), at the end of GnRHa treatment (Time II), and 1 year after ending treatment with GnRHa formulations (Time III).
Baseline data included age at the onset of the first symptoms, clinical manifestation, age at the time of treatment initiation, sex, mid-parental height, Tanner stage, bone age (BA), GnRHa formulation and related medical information, previous relevant medical records, cause of CPP, and anthropometric measures. Body weight was measured in kilograms using a digital weighing scale with a sensitivity of 0.1 kg, and the height was measured in meters with a stadiometer, in the standing position, with a 0.1-cm sensitivity, both evaluated by trained medical staff. BMI was calculated as weight (in kilograms) divided by height (in meters) squared (absolute value). BMI-SD score [SDS] was calculated using Anthro software (WHO, Geneva, Switzerland; and CDC, USA) (23).
To allow a better understanding of anthropometric changes, we evaluated BMI categories according to the WHO classification: normal weight, between the 10th and 85th percentiles; overweight, between the 85th and 95th percentiles; and obesity, 95th percentile or greater. We had no children at <5th percentile BMI in our study.
We calculated the change in BMI-SDS from baseline to the end of treatment (ΔTime II–I) and from baseline to a year after ending treatment (ΔTime III–I).
To evaluate height changes over the course of treatment, we also calculated the change in height-SDS at Time II and at Time I compared with baseline.
Statistical Analysis
Statistical analysis was performed using the SPSS™ version 26.0 software (SPSS Inc., Chicago, IL, USA). All probabilities were two-tailed, and p-values < 0.05 were regarded as significant. Quantitative variables were described as mean ± SD and qualitative variables as absolute frequencies and percentages. The Kolmogorov–Smirnov test was performed to assess whether data were distributed normally. Student's t-test and ANOVA were used when variables were normally distributed; and when data were not normally distributed, we used the Mann–Whitney test. Qualitative variables were compared using the chi-square or Fisher's exact test. Linear regression models were used to study the association between BMI-SDS at the end of treatment (Time II) and BMI-SDS at baseline (Time I) after adjusting for age, sex, and duration of treatment.
Results
A total of 241 children were diagnosed with CPP during the time of the study, but only 92 were eligible for study participation. We report data after 1 year of completing GnRHa treatment (Time III) in 64 cases. Of the 92 patients enrolled, the majority were girls (n = 84; 91%). Of the eight boys included (8%), all had completed follow-up until 1 year after stopping treatment. Baseline characteristics of study participants are summarized in Table 1.
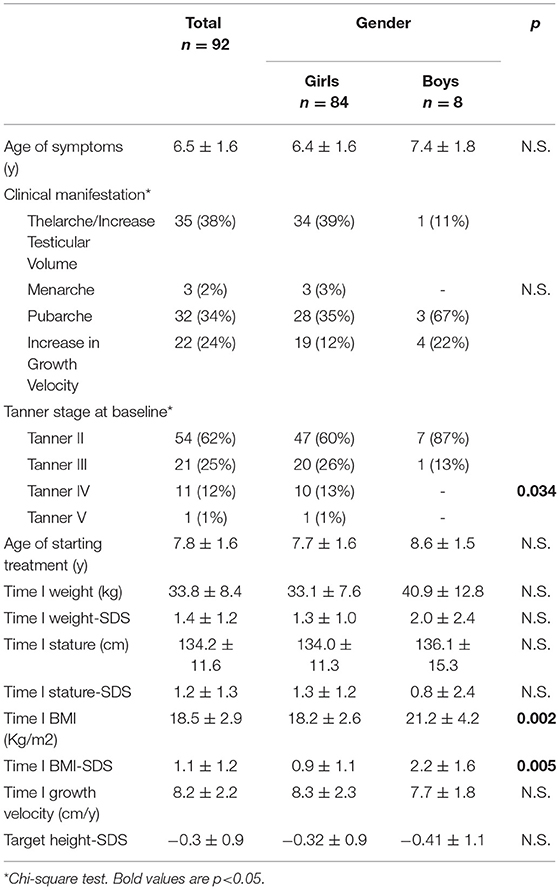
Table 1. Time I (T1 = baseline) clinical characteristics of the patients and gender comparison.
Their mean age at onset of symptoms was 6.5 ± 1.6 years, and the majority presented with thelarche/gonadarche. At baseline, girls showed a more advanced Tanner stage (p = 0.034) and initiated GnRHa treatment about 1.3 years after the onset of puberty signs. Boys were heavier than girls before treatment (girls BMI, 18.2 ± 2.6, and boys BMI, 21.2 ± 4.2, p = 0.002; and girls BMI-SDS, 0.9 ± 1.1, and boys BMI-SDS, 2.2 ± 1.6, p = 0.005). Our sample had a total of 81 white patients and 11 (12%) non-white patients. The 11% non-white participants were all girls. Idiopathic CPP was the main diagnosis (90%), with only 9 cases of secondary CPP (3 boys; 33% of secondary cases).
At baseline, less than half of the participants had normal BMI (42; 46%), 36 were overweight (39%), and 14 had obesity (15%), with differences noticed between sexes (4 boys, of whom 2 had obesity; p = 0.035).
BMI-SDS tended to increase with treatment but decreased a year after stopping GnRHa therapy (Figure 1: BMI-SDS 1.18 ± 1.0 at time I; 1.19 ± 1.0 at time II; and 1.06 ± 0.9 at time III; p = 0.06). To better understand this evolution, we analyzed changes in BMI-SDS over study duration (Table 2). BMI-SDS increased (0.013 ± 0.67) from baseline to time I and decreased (−0.12 ± 0.66; p = 0.032) from baseline to time III.
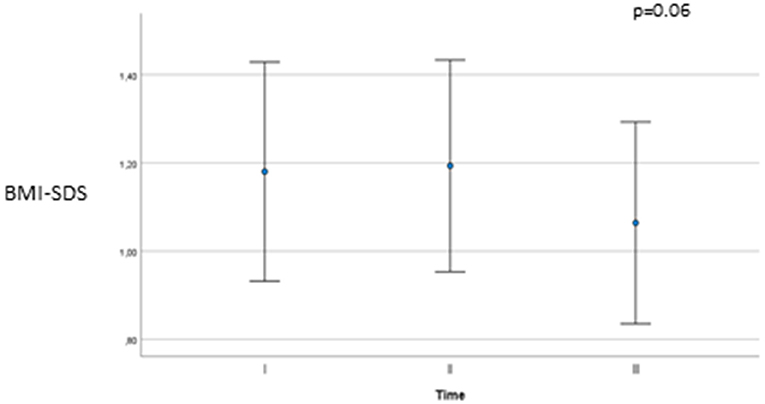
Figure 1. BMI-SDS at baseline (Time I), end of treatment (Time II) and one year after stopping GnRH agonists (Time III).
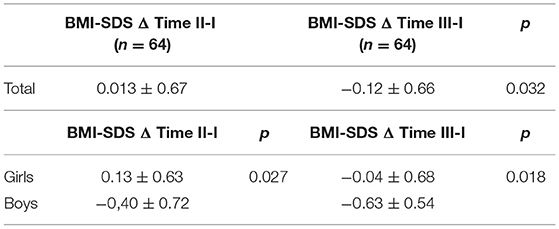
Table 2. Variations in BMI-SDS along study time according to sex.
Girls and boys differed such that the increase in BMI-SDS was noted in girls, but not boys (p = 0.027). Both sexes had a decrease in BMI-SDS from baseline to time III, but this decrease was greater in the boys (p = 0.012). Thus, BMI-SDS increased during treatment and decreased a year after the end of treatment in girls. In contrast, BMI-SDS decreased both during treatment and a year after the end of GnRHa treatment in boys.
A multivariable linear regression was computed to evaluate the independent predictors of change in BMI SDS from baseline to time II–I. After adjustment for age, sex, and duration of GnRHa use, BMI-SDS at baseline was associated negatively with the change from baseline to time II in those who were overweight or had obesity (β = −0.386, p = 0.005).
Considering BMI categories at baseline and progression over time, BMI-SDS significantly increased in the normal weight group compared with the group that was overweight or had obesity (ΔTime II–I, p = 0.033; and ΔTime III–I, p = 0.006) (Figures 2A,B).
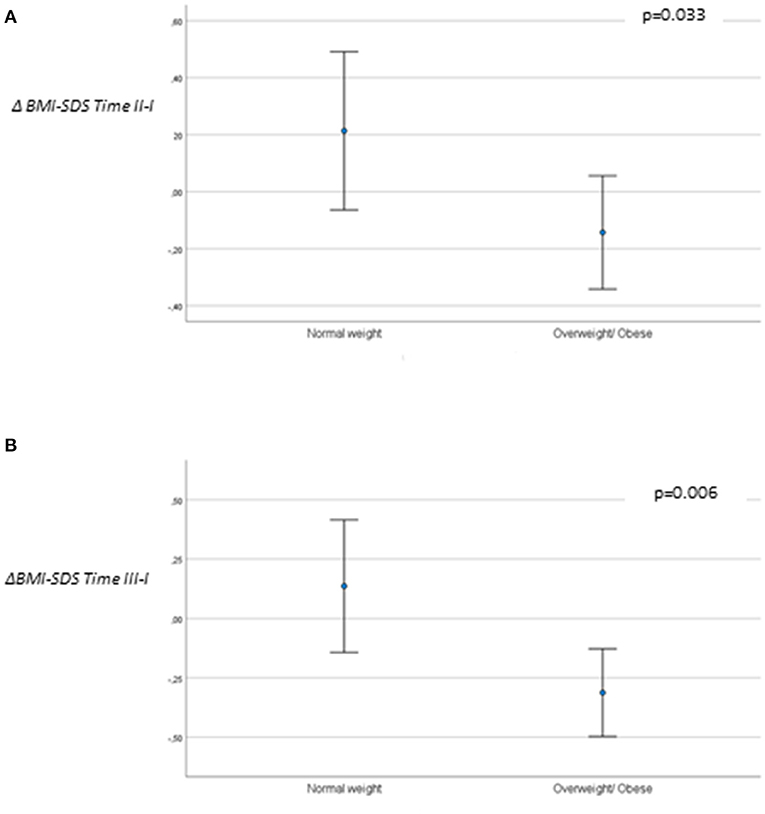
Figure 2. (A) BMI-SDS variation ΔTime II–I and (B) BMI-SDS variation ΔTime III–I, according to BMI group at baseline (n = 64).
Focusing on the effect of the agonists on growth, we observed a statistically significant difference in the variation of height-SDS during treatment between boys and girls (girls, −0.48 ± 0.67; boys, 0.69 ± 0.97; p < 0.001) (Figure 3).
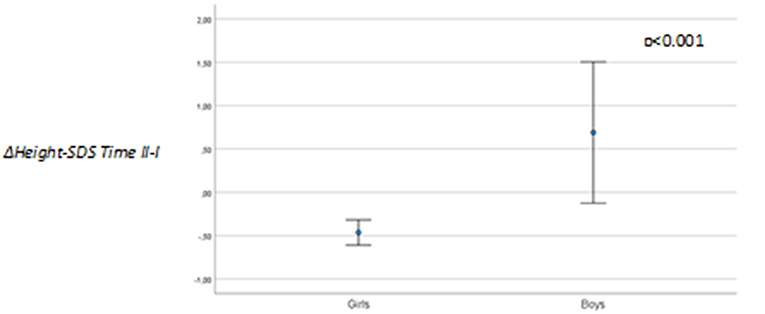
Figure 3. Height-SDS variation (ΔTime II–I) between genders (n = 92).
Discussion
In this study, we observed an increase in BMI-SDS during treatment with GnRH agonists in girls, but not in boys. However, this increase was temporary and reversed just 1 year after stopping treatment for the group as a whole. The overall treatment-related increase in BMI-SDS was inversely related to the pretreatment BMI. Therefore, the higher the BMI-SDS before the treatment, the less the weight gain is.
Few studies describe what happens when boys with CPP receive treatment. In our study, we found that the trend for gain in BMI-SDS is similar for boys and girls. The main difference is in height increment during treatment, which seems better controlled in girls. In the last 20 years, due to the increase in the prevalence of GnRHa use, several studies have started analyzing their impact not only on AH but also on BMI changes.
Yoon et al. described that in girls, overall, BMI-SDS for chronological age did not change significantly during or after GnRHa treatment discontinuation, regardless of their pretreatment BMI (22). These results contradict those reported by the Spanish PUBERE Group who noted that during treatment with GnRHa, girls experience a significant increase in BMI-SDS that persists after therapy is discontinued and AH has been reached (11). There are several conflicting findings, which are possibly attributable to the differences in race or ethnicity. In addition, differences in study protocols may also contribute to the conflicting data. In 2020, Vuralli et al. showed that BMI-SDS increased during GnRHa treatment only in girls in the “normal weight” category and not in those considered “overweight” and that this effect was reversible following treatment discontinuation (19).
In our study, we noted a similar increase in BMI, but we also observed its resolution and reversal after only 1 year of termination of the GnRHa therapy. As reported previously, our data demonstrated that the pattern of change in BMI-SDS varies according to the individual's BMI (14, 17). One explanation might be that fatty mass redistribution/deposition due to gonadal axis suppression is more significant in lean children than in overweight or obese children. The pharmacological interruption of the LH/follicle-stimulating hormone (LH/FSH) axis with suppression of estrogen production may be responsible for the enhanced deposition of adipose tissue in lean children compared with overweight or obese ones (23). The evidence of a transient effect on weight gain due to gonadal axis interruption leads us to propose that all patients with CPP on GnRHa therapy and their caregivers should be informed about weight management and that recommendations for lifestyle changes should be reinforced at every appointment, independent of BMI category (although effects are certainly most marked in those with lower BMI-SDS at treatment onset).
Our study is one of the very few studies that have enrolled boys treated with GnRHa for CPP and to our knowledge the only one that analyses what happens to these boys 1 year after stopping treatment. We demonstrate that the change in height-SDS significantly differs with sex, similar to the results found by Lee et al. (6). One explanation for this difference might be the pubertal growth spurt, which occurs at the beginning of puberty in girls and in the middle of puberty in boys (25). In addition, our results clearly show different BMI-SDS responses in girls and boys. This is probably due to a greater interruption of height increase in girls, which also contributes to the increase in BMI, given that BMI is calculated as weight (kg) divided by height (meters) squared. Leptin levels are positively related to adiposity and negatively related to testosterone levels. Additionally, blood leptin levels differ across the sexes through puberty to reach higher levels in girls than in boys (24–26). This would explain why BMI does not increase in boys as much as it does in girls during CPP treatment.
A limitation of this study is its retrospective nature, and consequently, we could not ensure that all patients were given similar dietary recommendations. Further, the number of boys in the study was small, and a larger number of boys would be necessary to further validate the different responses we noted between sexes to GnRHa treatment.
The multicentric CPP cohort with national representation and follow-up at 1 year after treatment in both boys and girls is the strength of our study.
Conclusions
The treatment of CPP with GnRHa causes a transient increase in BMI-SDS with a return to the basal BMI-SDS a year after stopping GnRHa. The increase in BMI-SDS is more evident in children with normal weight before treatment, but this effect is reversible and does not induce obesity.
Boys respond differently (with a lower BMI increase) to GnRH agonists.
National databases of CPP individuals are an important tool for conducting long-term follow-up studies and assessing anthropometric and metabolic variables that may be affected by the interruption of the hypothalamic–pituitary–gonadal axis.
Families and healthcare providers should be made aware of the importance of nutritional status and healthy lifestyles in CPP children.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Portuguese Ethics Committee (CNPD n° 1704/2015). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AL and EG wrote the first draft of the manuscript. SS, AL, and EG performed the analysis. SS draw the charts. CL undertook extensive critical review of the manuscript, but all authors together conceptualized the idea and approved the submission of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all the colleagues who collected data for the National Database: Joana Serra, Unidade de Endocrinologia Pediátrica, Hospital Pediátrico de Coimbra, Portugal; Marcelo Fonseca, Unidade de Endocrinologia Pediátrica, Hospital Pedro Hispano, Matosinhos, Portugal; Maria João Oliveira, Unidade de Endocrinologia Pediátrica, Centro Materno Infantil do Norte, Porto, Portugal; Maria Miguel Gomes, Unidade de Endocrinologia Pediátrica, Hospital de Braga, Portugal; Paula Vieira, Serviço de Pediatria, Hospital São Francisco Xavier, Lisbon, Portugal; Rita Silva, Unidade de Endocrinologia Pediátrica, Hospital de São João, Porto, Portugal; Sónia Gomes, Unidade de Endocrinologia Pediátrica, Centro Hospitalar Universitário de Lisboa Central, Lisbon, Portugal; Susana Figueiredo, Serviço de Pediatria, Hospital de Viana de Castelo, Portugal; and Susana Pacheco, Unidade de Endocrinologia Pediátrica, Hospital Fernando da Fonseca, Amadora, Portugal. We also thank all children, adolescents, and their parents for their cooperation and understanding. This investigator-initiated study was supported by an unconditional research grant from Ipsen.
References
1. Latronico AC, Brito VN, Carel JC. Causes, diagnosis, and treatment of central precocious puberty. Lancet Diabetes Endocrinol. (2016) 4:265–74. doi: 10.1016/S2213-8587(15)00380-0
2. Cantas-Orsdemir S, Eugster EA. Update on central precocious puberty: from etiologies to outcomes. Expert Rev Endocrinol Metab. (2019) 14:123–30. doi: 10.1080/17446651.2019.1575726
3. Bräuner EV, Busch AS, Eckert-Lind C, Koch T, Hickey M, Juul A. Trends in the incidence of central precocious puberty and normal variant puberty among children in Denmark, 1998 to 2017. JAMA Netw Open. (2020) 3:e2015665. doi: 10.1001/jamanetworkopen.2020.15665
4. Cheuiche AV, da Silveira LG, de Paula LCP, Lucena IRS, Silveiro SP. Diagnosis and management of precocious sexual maturation: an updated review. Eur J Pediatr. (2021) 180:3073–87. doi: 10.1007/s00431-021-04022-1
5. Soriano-Guillén L, Argente J. Central precocious puberty, functional and tumor-related. Best Pract Res Clin Endocrinol Metab. (2019) 33:101262. doi: 10.1016/j.beem.2019.01.003
6. Lee PA, Neely EK, Fuqua J, Yang D, Larsen LM, Mattia-Goldberg C, et al. Efficacy of leuprolide acetate 1-month depot for central precocious puberty (CPP): growth outcomes during a prospective, longitudinal study. Int J Pediatr Endocrinol. (2011) 2011:7. doi: 10.1186/1687-9856-2011-7
7. Kaplowitz PB, Backeljauw PF, Allen DB. Toward more targeted and cost-effective gonadotropin-releasing hormone analog treatment in girls with central precocious puberty. Horm Res Paediatr. (2018) 90:1–7. doi: 10.1159/000491103
8. Ko JH, Lee HS, Lim JS, Kim SM, Hwang JS. Changes in bone mineral density and body composition in children with central precocious puberty and early puberty before and after one year of treatment with GnRH agonist. Horm Res Paediatr. (2011) 75:174–9. doi: 10.1159/000320039
9. Park J, Kim JH. Change in body mass index and insulin resistance after 1-year treatment with gonadotropin-releasing hormone agonists in girls with central precocious puberty. Ann Pediatr Endocrinol Metab. (2017) 22:27–35. doi: 10.6065/apem.2017.22.1.27
10. Censani M, Feuer A, Orton S, Askin G, Vogiatzi M. Changes in body mass index in children on gonadotropin-releasing hormone agonist therapy with precocious puberty, early puberty or short stature. J Pediatr Endocrinol Metab. (2019) 32:1065–70. doi: 10.1515/jpem-2019-0105
11. Corripio R, Soriano-Guillén L, Herrero FJ, Cañete R, Castro-Feijoó L, Escribano A, et al. Changes in body mass index in girls with idiopathic central precocious puberty under gonadotropin-releasing hormone analogue therapy: the spanish registry. Horm Res Paediatr. (2016) 86:154–60. doi: 10.1159/000448552
12. Kim SW, Kim YB, Lee JE, Kim NR, Lee WK, Ku JK, et al. The influence of gonadotropin releasing hormone agonist treatment on the body weight and body mass index in girls with idiopathic precocious puberty and early puberty. Ann Pediatr Endocrinol Metab. (2017) 22:95–101. doi: 10.6065/apem.2017.22.2.95
13. Kim HR, Nam HK, Rhie YJ, Lee KH. Treatment outcomes of gonadotropin-releasing hormone agonist in obese girls with central precocious puberty. Ann Pediatr Endocrinol Metab. (2017) 22:259–65. doi: 10.6065/apem.2017.22.4.259
14. Arcari AJ, Gryngarten MG, Freire AV, Ballerini MG, Ropelato MG, Bergadá I, et al. Body mass index in girls with idiopathic central precocious puberty during and after treatment with GnRH analogues. Int J Pediatr Endocrinol. (2016) 2016:15. doi: 10.1186/s13633-016-0033-7
15. Lee SJ, Yang EM, Seo JY, Kim CJ. Effects of gonadotropin-releasing hormone agonist therapy on body mass index and height in girls with central precocious puberty. Chonnam Med J. (2012) 48:27–31. doi: 10.4068/cmj.2012.48.1.27
16. Anik A, Çatli G, Abaci A, Böber E. Effect of gonadotropin-releasing hormone agonist therapy on body mass index and growth in girls with idiopathic central precocious puberty. Indian J Endocrinol Metab. (2015) 19:267–71. doi: 10.4103/2230-8210.131770
17. Wolters B, Lass N, Reinehr T. Treatment with gonadotropin-releasing hormone analogues: different impact on body weight in normal-weight and overweight children. Horm Res Paediatr. (2012) 78:304–11. doi: 10.1159/000346145
18. Shiasi Arani K, Heidari F. Gonadotropin-releasing hormone agonist therapy and obesity in girls. Int J Endocrinol Metab. (2015) 13:e23085. doi: 10.5812/ijem.23085v2
19. Vuralli D, Ozon ZA, Gonc EN, Alikasifoglu A, Kandemir N. Long-term effects of GnRH agonist treatment on body mass index in girls with idiopathic central precocious puberty. J Pediatr Endocrinol Metab. (2020) 33:99–105. doi: 10.1515/jpem-2019-0214
20. Yoon JW, Park HA, Lee J, Kim JH. The influence of gonadotropin-releasing hormone agonists on anthropometric change in girls with central precocious puberty. Korean J Pediatr. (2017) 60:395–402. doi: 10.3345/kjp.2017.60.12.395
21. Lim KI, Lee HS, Hwang JS. Changes in body mass index in boys with central precocious puberty over 2 years of gonadotropin-releasing hormone agonist therapy. Ann Pediatr Endocrinol Metab. (2020) 25:169–73. doi: 10.6065/apem.1938176.088
22. Neely EK, Wilson DM, Lee PA, Stene M, Hintz RL. Spontaneous serum gonadotropin concentrations in the evaluation of precocious puberty. J Pediatr. (1995) 127:47–52. doi: 10.1016/S0022-3476(95)70255-5
23. WHO. Anthro for personal computers, version 3.2.2, 2011: Software for assessing growth and development of the world's children. Geneva: WHO, (2010). Available online at: http://www.who.int/childgrowth/software/en/.
24. Rosenfield R, Cooke D, Radovick S. Chapter 16: Puberty in the female and its disorders. In: Sperling M., Pediatric Endocrinology, , 5Th Edition. Philadelphia. Elsevier. (2021). p. 542–44. doi: 10.1016/B978-0-323-62520-3.00016-6
25. Loomba-Albrecht LA, Styne DM. Effect of puberty on body composition. Curr Opin Endocrinol Diabetes Obes. (2009) 16:10–5. doi: 10.1097/MED.0b013e328320d54c
Keywords: central precocious puberty (CPP), GnRH agonists, weight gain (WG), body mass index (BMI), obesity
Citation: Leite AL, Galo E, Antunes A, Robalo B, Amaral D, Espada F, Castro S, Simões Dias S and Limbert C (2022) Do GnRH Agonists Really Increase Body Weight Gain? Evaluation of a Multicentric Portuguese Cohort of Patients With Central Precocious Puberty. Front. Pediatr. 10:816635. doi: 10.3389/fped.2022.816635
Received: 16 November 2021; Accepted: 05 January 2022;
Published: 04 March 2022.
Edited by:
Madhusmita Misra, Massachusetts General Hospital and Harvard Medical School, United StatesReviewed by:
Carla Bizzarri, Bambino Gesù Children's Hospital (IRCCS), ItalyEce Bober, Dokuz Eylül University, Turkey
Copyright © 2022 Leite, Galo, Antunes, Robalo, Amaral, Espada, Castro, Simões Dias and Limbert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Luísa Leite, YW5hLmx1aXNhMjBAZ21haWwuY29t