
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Pediatr., 26 April 2022
Sec. Child and Adolescent Psychiatry
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.806399
 Agnieszka Rynkiewicz1,2†
Agnieszka Rynkiewicz1,2† Łukasz Dembiński3,4†
Łukasz Dembiński3,4† Berthold Koletzko3,5
Berthold Koletzko3,5 Pierre-André Michaud3,6
Pierre-André Michaud3,6 Adamos Hadjipanayis3,7,8*
Adamos Hadjipanayis3,7,8* Zachi Grossman3,9,10
Zachi Grossman3,9,10 Kathryn Korslund11Bryan H. King12
Kathryn Korslund11Bryan H. King12 Janet Treasure13Jarosław Peregud-Pogorzelski14,15Stefano del Torso3,16
Janet Treasure13Jarosław Peregud-Pogorzelski14,15Stefano del Torso3,16 Arunas Valiulis3,17,18
Arunas Valiulis3,17,18 Artur Mazur3,19
Artur Mazur3,19
In the face of the growing number of adolescents suffering from eating disorders (EDs) and access to psychiatric care limited by the epidemiological and demographic situation, the primary care pediatrician’s role in diagnosing and treating EDs is growing. The European Academy of Paediatrics (EAP) decided to summarize knowledge about EDs and formulate recommendations to support European pediatricians and improve care for adolescents with EDs.
Pediatricians commonly encounter patients with suspected or confirmed eating disorders (EDs), who carry a considerable risk of morbidity and even mortality. Early detection, appropriate diagnostic workup, and effective treatment require transdisciplinary collaboration. They are all essential for improving the patients’ prognosis. Here we aim to review current knowledge relevant for practicing pediatricians and provide recommendations of the European Academy of Paediatrics (EAP) on the role of pediatricians in caring for adolescents with ED and for actions of authorities and pediatric societies aiming to improve healthcare for these patients.
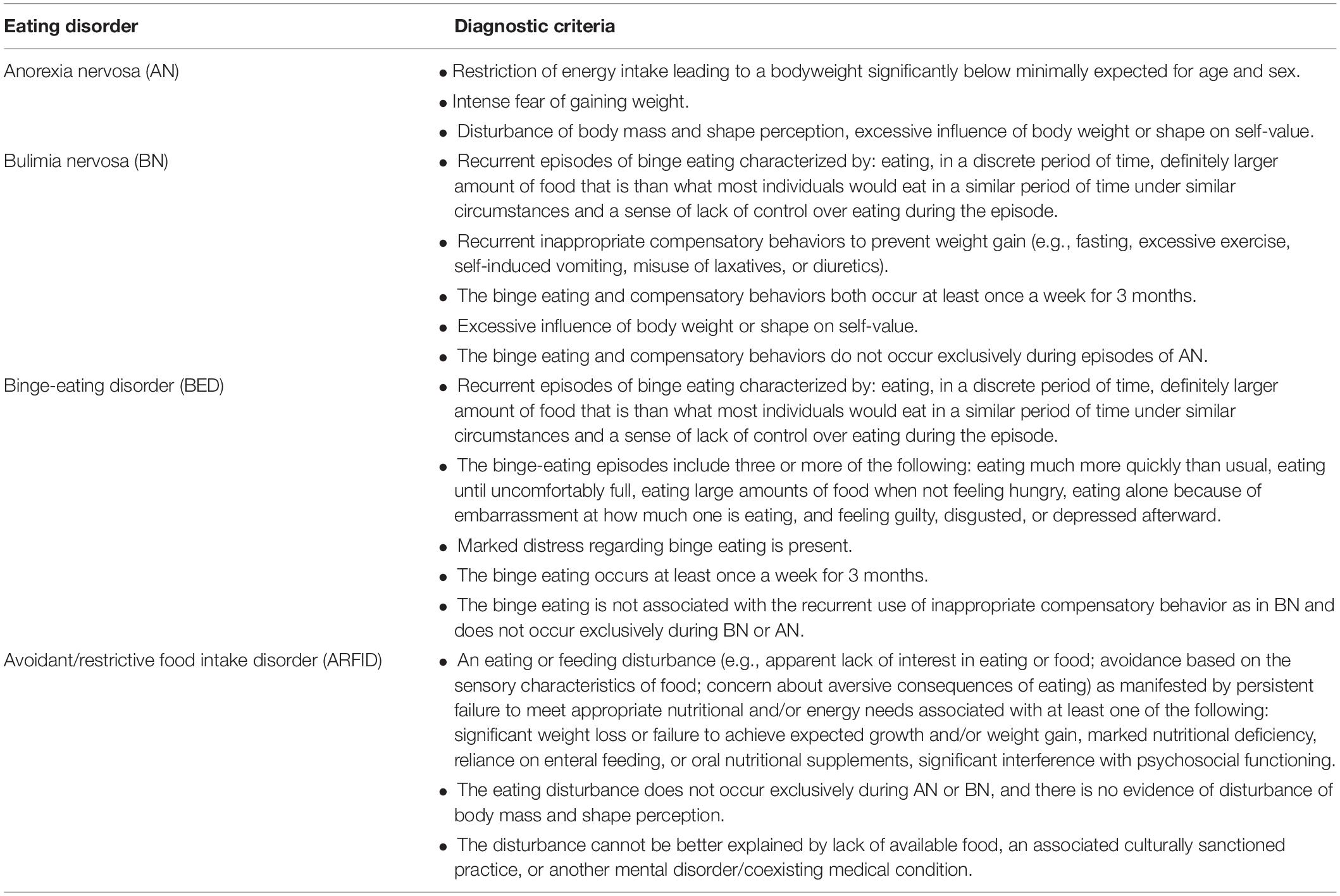
The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) and the 11th revision of the International Classification of Diseases (ICD-11) define ED as persistent abnormal eating behaviors that significantly impair physical health or psychosocial functioning (1, 2). The diagnostic criteria and characteristics of the most common ED in the adolescent population – anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder (BED), avoidant/restrictive food intake disorder (ARFID) – are presented in Table 1 (2).
Other less common EDs include:
• Atypical AN – AN with normal body weight;
• Rumination-regurgitation disorder – repeated regurgitation of food not associated with other medical conditions;
• Pica – persistent eating of non-nutritive/non-food substances;
• Purging disorder – recurrent purging behavior to influence weight or shape (e.g., vomiting, misuse of laxatives or diuretics, or other medications) in the absence of BED.
In practice, one type of ED may shift to another over time, and in some patients, it is difficult to diagnose a particular type of ED precisely.
As the onset of the disease is usually in the teenage years, pediatricians are the most likely to suspect a diagnosis of ED (4, 5). Data on the prevalence of ED are quite varied and depend on the population and diagnostic criteria used. Large-scale population surveys also have an underestimation bias due to patients’ tendency to minimize symptoms or deny the disease (6). However, the overall prevalence of ED is estimated from 2% to even 6%, with a nearly five times greater frequency of BED than other types of ED (7–10). The COVID-19 pandemic also contributed to a significant increase in stress, disturbances in school and family relations, and often limited access to psychological counseling, which increased the frequency of ED and deterioration of the prognosis (11).
Statistically, ED are more common in females, although in BED, the proportion of male patients is higher approximately a third (12).
Episodes of behavior typical of ED but not meeting all criteria may occur in up to one in five adolescents (13). However, some behaviors may mask or mimic ED at this age, which is mainly related to the adolescent gaining influence on their own nutrition and focusing attention on external appearance (14). Autism spectrum disorder shares some common features with ED, especially the restrictive ones, which should be considered in the differential diagnosis (15, 16). ED can also coexist with other mental or organic disorders, such as depression, celiac disease, or diabetes (17).
A specific cause of ED has not been established, but potential etiology includes genetic predisposition, cognitive and emotional vulnerability, social and environmental factors, such as pressure of the dominant cultural patterns and weight stigma (18). Moreover, in the group of children with ED, there are increased risks of emotional or behavioral disorders, attention-deficit/hyperactivity disorder and autism spectrum disorders (19, 20).
It should also be noted that an increased risk of ED occurs in children struggling with the lack of social acceptance (e.g., overweight, ethnic, racial, or sexual minorities) (21, 22).
Eating disorder should be seen not only as a mental illness but as a threat to health and even to life. Chronic malnutrition, nutritional deficiencies, frequent vomiting, and misuse of drugs can lead to irreversible effects that impair adolescents’ health and development. Chronic undernutrition can lead to long-term effects, such as diminished bone density or even cognitive impairment (23). Moreover, the consequences of ED can cause secondary peer acceptance problems, bullying, symptoms of post-traumatic stress disorder, and an increased risk of self-injury (24–26). ED has the second-highest mortality rate of all mental health disorders due to the increased frequency of suicide attempts but also due to the health consequences of cachexia (e.g., electrolyte problems, dehydration, heart failure) (27, 28).
The main health problems that adolescents with ED may report to a pediatrician are summarized in Table 2.
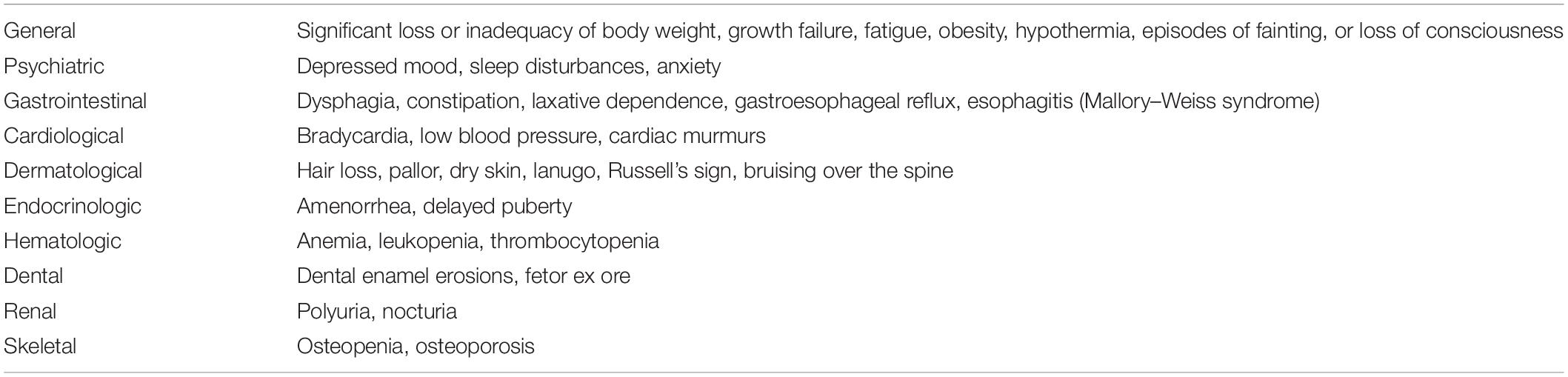
Table 2. Major health complaints, symptoms, and signs in adolescents with eating disorders.
Due to the fatal consequences of untreated ED, early diagnosis and therapeutic intervention improve outcomes. Awareness of the various ED symptoms and screening in risk groups is an essential role of the primary care pediatrician and nurse. Vaccination visits and annual health check-ups provide a unique opportunity to spot the first signs of ED. Therefore, assessing the nutritional status with reference to growth charts at each visit is essential (29).
Apart from the findings in the physical examination described in Table 2, blood pressure and heart rate should be assessed. Lowering these values in relation to age references may be a symptom of cachexia and (e.g., in the case of significant bradycardia) indicate the need for hospitalization.
In the ED risk assessment, several available tools can be used. To date, many different physician-filled or self-assessed screening questionnaires, which can help to detect abnormal behaviors and lead to earlier diagnosis, have been developed, e.g.:
• SCOFF questionnaire – containing five short questions about eating and its impact on life (30);
• Eating disorder Screen for Primary care (ESP) – containing questions about eating patterns and previous ED episodes (31);
• Eating Disorders Assessment for DSM-5 (EDA-5) – containing questions based on the DSM-5 diagnosis criteria (32);
• Child Eating Disorder Examination (ChEDE) – containing 28 questions to assess diagnostic criteria for BED and BN (33);
• Bright Futures Questionnaires – a relatively extensive questionnaire from the American Academy of Pediatrics containing questions about eating patterns and body image (34).
However, the results of questionnaires, especially those self-reported, should be interpreted with caution and in the context of the entire clinical picture. Due to the lack of an unequivocal advantage of one questionnaire, pediatricians should use the one with the interpretation of which they have the most experience and is available in the national language.
The primary care pediatrician can also directly ask questions about, e.g., inducing vomiting, using laxatives, or self-image, but it is essential to maintain an atmosphere of respect and trust. A comprehensive psychosocial assessment is also necessary, emphasizing the possibility of coexistence of addictions, bullying, and physical or sexual abuse (35, 36).
Laboratory tests should be considered in patients with suspected ED to exclude anemia, disturbances of electrolyte equilibrium, thyroid dysfunction, and celiac disease – Table 3. However, the diagnosis of ED is purely clinical, and diagnostic procedures mentioned above mainly aim to identify metabolic and physiological disturbances that are consequences of ED. Among patients with severe cachexia, cardiological evaluation (electrocardiogram and echocardiogram) is vital to exclude cardiac arrhythmias and pericardial effusion (37). Some patients may require additional radiological, gastroenterological, endocrinological, or neurological workup to rule out causes of symptoms other than ED.
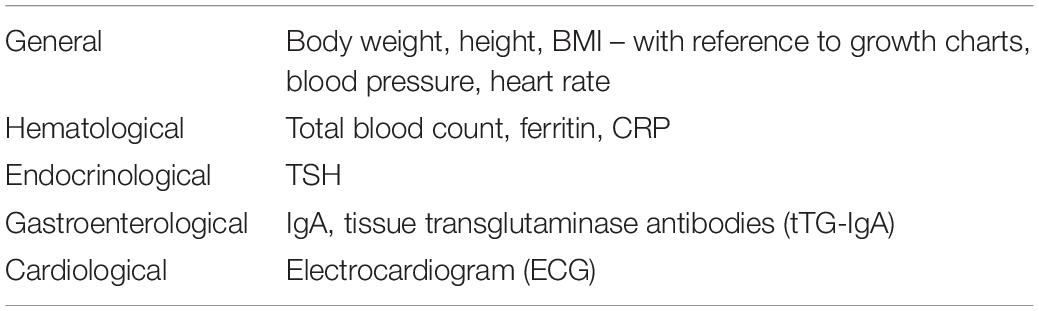
Table 3. Recommended diagnostics in patients with suspected ED in primary pediatric care.
Most adolescents with ED can be treated in an outpatient setting provided that a patient and family are motivated to cooperate, and there are no severe malnutrition, somatic complications, or other psychiatric problems requiring hospitalization (38). In such cases, cooperation between a psychiatrist and a psychologist with a primary care pediatrician is essential to optimize treatment strategies and ensure patient safety. In addition, since treatment of EDs requires an interdisciplinary approach, dietitians, family therapists, social workers, and teachers, whenever possible, should be involved in treating patients with ED.
Family based treatment is the recommended front-line treatment for ED in childhood and adolescents. However, Cognitive Behavior Therapy or its modification – Dialectical Behavior Therapy – can be a useful supplement (39). However, in addition, regular monitoring of the patient’s nutritional status by the primary care pediatrician is vital especially in cases of AN.
Hospitalization should be considered in adolescents who develop life-threatening complications of ED or have failed to restore weight with outpatient treatment. Effective hospital treatment needs a professional, multidisciplinary team with expertise and experience dealing with ED patients and a structured treatment plan that is regularly re-evaluated and revised when necessary. In addition, patients with coexisting mental and organic diseases, pericardial effusion, electrolyte disorders, and a high risk of developing the refeeding syndrome require special supervision (40, 41).
Pharmacotherapy (e.g., antidepressants or neuroleptics) is also used in the treatment of ED, but it should be carried out with the leading role of a psychiatrist.
Pediatricians should consider that, as with many chronic diseases, ED affects the patient’s entire family. For example, many parents can be depressed, grieve, or express guilt because of their child’s illness (42). Also, siblings may develop their own psychological and psychiatric problems (43).
Early diagnosis and adequate treatment can produce a partial remission in over 60% of patients (44, 45).
Primary care pediatricians play a crucial role in screening and early diagnosis of ED because they have the unique opportunity to monitor adolescents’ health regularly, and they have the chance, to some extent, assess adolescents’ family and social situations. Therefore, a mandatory part of the examination should be the assessment of nutritional status, as it may be the first sign of ED.
The role of pediatricians is also to educate and inform the community about ED and advocate for these patients. Moreover, in the face of the shortage of child psychiatrists in many European countries, the pediatrician often will have to act as the treatment coordinator (46).
For international and national state, health, and education authorities
• Adolescents with ED require multidisciplinary care. Therefore, this issue should be present in undergraduate and postgraduate medical education.
• National health authorities should provide adolescents with ED with multidisciplinary care and support for their families.
For European and national pediatric societies
• Pediatric societies should support their members through ongoing training in ED.
• Pediatric societies should advocate in increasing the availability of psychiatric and psychological care for adolescents with ED.
For pediatricians
• An integral part of each patient visit should be the assessment of their nutritional status.
• Measurement of blood pressure and heart rate should be a part of every physical examination of adolescents with ED.
• When assessing the risk of ED, pediatricians should use the questionnaires with which they have the most experience and are available in the local language.
• The role of a pediatrician is to cooperate with a psychiatrist and psychologist in the therapeutic process, with particular emphasis on regular assessment of the nutritional status and early identification of health risk signs.
• Adolescents with life-threatening complications of ED and those who have failed in weight normalization efforts should be referred to the hospital.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
AR, ŁD, BK, AH, and AM: study design. AR and ŁD: data collection. AR, ŁD, BK, and P-AM: data analysis and interpretation. AR, ŁD, BK, P-AM, AH, ZG, KK, BHK, JT, JP-P, ST, AV, and AM: manuscript preparation and critical revision. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. International Classification of Diseases 11th Revision. (2018). Available online at: https://icd.who.int/en (accessed October 14, 2021).
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Publishing (2013). doi: 10.1176/appi.books.9780890425596
3. Rosen DS. American academy of pediatrics committee on adolescence. Identification and management of eating disorders in children and adolescents. Pediatrics. (2010) 126:1240–53. doi: 10.1542/peds.2010-2821
4. Preti A, Girolamo Gd, Vilagut G, Alonso J, Graaf Rd, Bruffaerts R, et al. The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. J Psychiatr Res. (2009) 43:1125–32. doi: 10.1016/j.jpsychires.2009.04.003
5. Volpe U, Tortorella A, Manchia M, Monteleone AM, Albert U, Monteleone P. Eating disorders: what age at onset? Psychiatry Res. (2016) 238:225–7. doi: 10.1016/j.psychres.2016.02.048
6. Devaud C, Michaud PA, Narring F. Anorexia and bulimia: increasing disorders? A review of the literature on the epidemiology of eating disorders. Rev Epidemiol Sante Publique. (1995) 43:347–60.
7. Swanson SA, Crow SJ, Le Grange D, Swendsen J, Merikangas KR. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry. (2011) 68:714–23. doi: 10.1001/archgenpsychiatry.2011.22
8. Hay P, Girosi F, Mond J. Prevalence and sociodemographic correlates of DSM-5 eating disorders in the Australian population. J Eat Disord. (2015) 3:19. doi: 10.1186/s40337-015-0056-0
9. Smink FR, van Hoeken D, Hoek HW. Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep. (2012) 14:406–14. doi: 10.1007/s11920-012-0282-y
10. Stice E, Marti CN, Shaw H, Jaconis M. An 8-year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents. J Abnorm Psychol. (2009) 118:587–97. doi: 10.1037/a0016481
11. Castellini G, Cassioli E, Rossi E, Innocenti M, Gironi V, Sanfilippo G, et al. The impact of COVID-19 epidemic on eating disorders: a longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. Int J Eat Disord. (2020) 53:1855–62. doi: 10.1002/eat.23368
12. Mitchison D, Hay P, Slewa-Younan S, Mond J. The changing demographic profile of eating disorder behaviors in the community. BMC Public Health. (2014) 14:943. doi: 10.1186/1471-2458-14-943
13. Croll J, Neumark-Sztainer D, Story M, Ireland M. Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: relationship to gender and ethnicity. J Adolesc Health. (2002) 31:166–75. doi: 10.1016/s1054-139x(02)00368-3
14. Bardone-Cone AM, Fitzsimmons-Craft EE, Harney MB, Maldonado CR, Lawson MA, Smith R, et al. The inter-relationships between vegetarianism and eating disorders among females. J Acad Nutr Diet. (2012) 112:1247–52. doi: 10.1016/j.jand.2012.05.007
15. Karjalainen L, Råstam M, Paulson-Karlsson G, Wentz E. Do autism spectrum disorder and anorexia nervosa have some eating disturbances in common? Eur Child Adolesc Psychiatry. (2019) 28:69–78. doi: 10.1007/s00787-018-1188-y
16. Dell’Osso L, Carpita B, Gesi C, Cremone IM, Corsi M, Massimetti E, et al. Subthreshold autism spectrum disorder in patients with eating disorders. Compr Psychiatry. (2018) 81:66–72. doi: 10.1016/j.comppsych.2017.11.007
17. Nikniaz Z, Beheshti S, Abbasalizad Farhangi M, Nikniaz L. A systematic review and meta-analysis of the prevalence and odds of eating disorders in patients with celiac disease and vice-versa. Int J Eat Disord. (2021) 54:1563–74. doi: 10.1002/eat.23561
18. Rikani AA, Choudhry Z, Choudhry AM, Ikram H, Asghar MW, Kajal D, et al. A critique of the literature on etiology of eating disorders. Ann Neurosci. (2013) 20:157–61. doi: 10.5214/ans.0972.7531.200409
19. Shan H, Li F, Zhang J, Wang H, Li J. Feeding and eating disorder and risk of subsequent neurodevelopmental disorders: a population-based cohort study. Front Pediatr. (2021) 9:671631. doi: 10.3389/fped.2021.671631
20. Craig F, De Giacomo A, Operto FF, Margari M, Trabacca A, Margari L. Association between feeding/mealtime behavior problems and internalizing/externalizing problems in autism spectrum disorder (ASD), other neurodevelopmental disorders (n.d.) and typically developing children. Minerva Pediatr. (2019): doi: 10.23736/S0026-4946.19.05371-4 [Epub ahead of print].
21. Nagata JM, Garber AK, Tabler JL, Murray SB, Bibbins-Domingo K. Prevalence and correlates of disordered eating behaviors among young adults with overweight or obesity. J Gen Intern Med. (2018) 33:1337–43. doi: 10.1007/s11606-018-4465-z
22. Watson RJ, Adjei J, Saewyc E, Homma Y, Goodenow C. Trends and disparities in disordered eating among heterosexual and sexual minority adolescents. Int J Eat Disord. (2017) 50:22–31. doi: 10.1002/eat.22576
23. Tamiya H, Ouchi A, Chen R, Miyazawa S, Akimoto Y, Kaneda Y, et al. Neurocognitive impairments are more severe in the binge-eating/purging anorexia nervosa subtype than in the restricting subtype. Front Psychiatry. (2018) 9:138. doi: 10.3389/fpsyt.2018.00138
24. Day S, Bussey K, Trompeter N, Mitchison D. The impact of teasing and bullying victimization on disordered eating and body image disturbance among adolescents: a systematic review. Trauma Violence Abuse. (2021):1524838020985534. doi: 10.1177/1524838020985534 [Epub ahead of print].
25. Lie SØ, Rø Ø, Bang L. Is bullying and teasing associated with eating disorders? A systematic review and meta-analysis. Int J Eat Disord. (2019) 52:497–514. doi: 10.1002/eat.23035
26. Tagay S, Schlottbohm E, Reyes-Rodriguez ML, Repic N, Senf W. Eating disorders, trauma, PTSD, and psychosocial resources. Eat Disord. (2014) 22:33–49. doi: 10.1080/10640266.2014.857517
27. Cliffe C, Shetty H, Himmerich H, Schmidt U, Stewart R, Dutta R. Suicide attempts requiring hospitalization in patients with eating disorders: a retrospective cohort study. Int J Eat Disord. (2020) 53:458–65. doi: 10.1002/eat.23240
28. Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. (2014) 13:153–60. doi: 10.1002/wps.20128
29. World Health Organization. The WHO Child Growth Standards. (2009). Available online at: https://www.who.int/tools/child-growth-standards/standards (accessed September 30, 2021).
30. Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. (1999) 319:1467–8. doi: 10.1136/bmj.319.7223.1467
31. Cotton MA, Ball C, Robinson P. Four simple questions can help screen for eating disorders. J Gen Intern Med. (2003) 18:53–6. doi: 10.1046/j.1525-1497.2003.20374.x
32. Sysko R, Glasofer DR, Hildebrandt T, Klimek P, Mitchell JE, Berg KC, et al. The eating disorder assessment for DSM-5 (EDA-5): development and validation of a structured interview for feeding and eating disorders. Int J Eat Disord. (2015) 48:452–63. doi: 10.1002/eat.22388
33. Decaluwé V, Braet C. Assessment of eating disorder psychopathology in obese children and adolescents: interview versus self-report questionnaire. Behav Res Ther. (2004) 42:799–811. doi: 10.1016/j.brat.2003.07.008
34. Hagan JF, Shaw JS, Duncan PM. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. 4th ed. Elk Grove Village, IL: American Academy of Pediatrics (2017). Available on: https://brightfutures.aap.org/materials-and-tools/tool-and-resource-kit/Pages/adolescence-tools.aspx (Accessed September 30, 2021).
35. Ulfvebrand S, Birgegård A, Norring C, Högdahl L, von Hausswolff-Juhlin Y. Psychiatric comorbidity in women and men with eating disorders results from a large clinical database. Psychiatry Res. (2015) 230:294–9. doi: 10.1016/j.psychres.2015.09.008
36. Caslini M, Bartoli F, Crocamo C, Dakanalis A, Clerici M, Carrà G. Disentangling the association between child abuse and eating disorders: a systematic review and meta-analysis. Psychosom Med. (2016) 78:79–90. doi: 10.1097/PSY.0000000000000233
37. Docx MK, Gewillig M, Simons A, Vandenberghe P, Weyler J, Ramet J, et al. Pericardial effusions in adolescent girls with anorexia nervosa: clinical course and risk factors. Eat Disord. (2010) 18:218–25. doi: 10.1080/10640261003719484
38. Mehler PS, Winkelman AB, Andersen DM, Gaudiani JL. Nutritional rehabilitation: practical guidelines for refeeding the anorectic patient. J Nutr Metab. (2010) 2010:625782. doi: 10.1155/2010/625782
39. Lock J. An update on evidence-based psychosocial treatments for eating disorders in children and adolescents. J Clin Child Adolesc Psychol. (2015) 44:707–21. doi: 10.1080/15374416.2014.971458
40. Garber AK, Sawyer SM, Golden NH, Guarda AS, Katzman DK, Kohn MR, et al. A systematic review of approaches to refeeding in patients with anorexia nervosa. Int J Eat Disord. (2016) 49:293–310. doi: 10.1002/eat.22482
41. Wiley online library. The Management of Really Sick Patients with Anorexia Nervosa. (2020). Available online at: http://www.marsipan.org.uk (accessed September 30, 2021).
42. Anastasiadou D, Medina-Pradas C, Sepulveda AR, Treasure J. A systematic review of family caregiving in eating disorders. Eat Behav. (2014) 15:464–77. doi: 10.1016/j.eatbeh.2014.06.001
43. Dimitropoulos G, Klopfer K, Lazar L, Schacter R. Caring for a sibling with anorexia nervosa: a qualitative study. Eur Eat Disord Rev. (2009) 17:350–65. doi: 10.1002/erv.937
44. Mairhofer D, Zeiler M, Philipp J, Truttmann S, Wittek T, Skala K, et al. Short-term outcome of inpatient treatment for adolescents with anorexia nervosa using DSM-5 remission criteria. J Clin Med. (2021) 10:3190. doi: 10.3390/jcm10143190
45. Smink FR, van Hoeken D, Hoek HW. Epidemiology, course, and outcome of eating disorders. Curr Opin Psychiatry. (2013) 26:543–8. doi: 10.1097/YCO.0b013e328365a24f
46. European Network of Ombudspersons for Children. Child and Adolescent Mental Health in Europe. (2018). Available online at: http://enoc.eu/wp-content/uploads/2018/09/ENOC-2018-report-on-Child-Mental-Health-ENG-FV.pdf (accessed September 30, 2021).
Keywords: anorexia nervosa, binge-eating disorder, bulimia nervosa, early diagnosis, primary care
Citation: Rynkiewicz A, Dembiński Ł, Koletzko B, Michaud P-A, Hadjipanayis A, Grossman Z, Korslund K, King BH, Treasure J, Peregud-Pogorzelski J, del Torso S, Valiulis A and Mazur A (2022) Adolescents With Eating Disorders in Pediatric Practice – The European Academy of Paediatrics Recommendations. Front. Pediatr. 10:806399. doi: 10.3389/fped.2022.806399
Received: 31 October 2021; Accepted: 23 March 2022;
Published: 26 April 2022.
Edited by:
Sara Calderoni, Stella Maris Foundation (IRCCS), ItalyReviewed by:
Francesca Felicia Operto, University of Salerno, ItalyCopyright © 2022 Rynkiewicz, Dembiński, Koletzko, Michaud, Hadjipanayis, Grossman, Korslund, King, Treasure, Peregud-Pogorzelski, del Torso, Valiulis and Mazur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adamos Hadjipanayis, YWRhbW9zQHBhaWRpYXRyb3MuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.