
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 14 April 2022
Sec. General Pediatrics and Pediatric Emergency Care
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.803323
This article is part of the Research TopicHot Topics in PediatricsView all 50 articles
 Alfonso Galderisi1
Alfonso Galderisi1 Giorgio Perilongo1
Giorgio Perilongo1 Sonia Caprio2
Sonia Caprio2 Liviana Da Dalt1
Liviana Da Dalt1 Giovanni Di Salvo1
Giovanni Di Salvo1 Michela Gatta1
Michela Gatta1 Carlo Giaquinto1
Carlo Giaquinto1 Rosario Rizzuto3Adelaide Robb4
Rosario Rizzuto3Adelaide Robb4 Peter David Sly5
Peter David Sly5 Alessandra Simonelli6
Alessandra Simonelli6 Annamaria Staiano7
Annamaria Staiano7 Roberto Vettor8
Roberto Vettor8 Eugenio Baraldi1*
Eugenio Baraldi1*Importance: The Padova Chart for Health in Children (PCHC) aims to gather the evidence of healthcare promotion and protection for chidren and adolescents (i.e., aged <18 y) into a single document in order to guide families, healthcare providers and social actors on healthy choices. No more than 2% of Europeans and North Americans aged <30 y have a healthy lifestyle. This, together with metabolic and brain plasticity during childhood, creates the ideal opportunity to implement preventive strategies. Guided interventions promoting healthy lifestyle in children and families therefore have a key role in abating the unprecedented pandemic of non-communicable diseases (NCDs) in adulthood.
Observations: The PCHC is divided into four sections: nutrition, cardiovascular health, respiratory health, and mental and social health. Each section is structured in an ALICE approach (assessment, lobbying, intervention, call-for-action, evaluation): assessment of necessity, describing relevance to healthcare; lobbying to identify those who can effect the proposed interventions; interventions involving family, school and peers; a call-for-action to define priorities among the proposed interventions; and objective evaluation measures that can be applied on a population basis.
Conclusions and Relevance: Interventions promoting health in childhood require joint action from multiple institutional, local and family representatives, with the shared goal of promoting health across the entire age group. These lifestyle interventions have the potential to change the lifetime risk trajectory for NCDs.
Optimizing pediatric health is key to reducing social inequality and ensuring sustainable growth. Although 30% of the European and North-American population is younger than 30 years (1), only 2% of this group has a healthy lifestyle, defined as being physically active for at least 60 min/d, consuming fruit and vegetables daily, spending <2 h/d on screen-based activities, and abstaining from alcohol and tobacco (2). This creates the conditions for an unprecedented pandemic of non-communicable diseases (NCDs), many of which start early in life, although not always with an overt onset in childhood or early adulthood (3). NCDs directly or indirectly account for ~90% of deaths in middle-to-high income countries (4). More recently, the combination of NCDs (specifically diabetes, obesity, hypertension, chronic lung and cardiovascular diseases, and mental illnesses) and socio-economic disparities have worsened outcomes in those affected by COVID-19, compelling national healthcare systems to target health as the only truly sustainable strategy to “prevent a “syndemic” disease” approach (5, 6). Targeting health promotion in children is ideal, as they have a metabolic (7, 8) and brain plasticity (9, 10) that offers the opportunity to instill life-long healthy habits (11). Interventions promoting healthy lifestyle in childhood are the sole sustainable and effective action to prevent NCDs in adulthood (1, 11).
We therefore decided to gather current evidence and guidance into a single document to inform and promote child health. We identified four areas, based on their potential impact on morbidity and mortality (4). 1. nutrition; 2. cardiovascular health; 3. respiratory health, 4. mental and social health.
Each area was investigated by a team of two experts. Research was performed using PubMed, UpToDate, and WebOfScience. Guidelines and position statements published by European and North American scientific societies were also considered, as were position statements from the World Health Organization and Centers for Disease Control, systematic reviews, and Cochrane Reviews. The Chart targets “children” according to the broad UNICEF definition as those aged <18 years.
Each section is formatted using a call-for-action (ALICE) approach: Assessment of necessity, based on current evidence; Lobbying: identifying targets (families, primary healthcare providers and/or schools) to effect the proposed interventions; Interventions and guidance involving family, school and peers; Call for action to define priorities among the proposed interventions; Evaluate: proposed measurable population-level indicators to give a long-term assessment of the effectiveness of the interventions.
Over the past 30 years, the prevalence of overweight and obesity have increased 10-fold in youth (12, 13), with 20% of those aged 2–19 years now obese (14), and one out of four having impaired glucose metabolism. Childhood obesity increases the risk of NCDs in adulthood, including type 2 diabetes, cardiovascular disease, asthma and other respiratory problems, sleep disorders, and liver disease (15). Further, longitudinal data from the SEARCH for Diabetes in Youth and the Restoring Insulin Secretion studies (16–18) have highlighted the morbidity in children with early type 2 (i.e., obesity-related) diabetes. This is important as more than 50% of those with childhood-onset type 2 diabetes have kidney disease or retinopathy by the age of 30 y (19). Treatment of childhood-onset type 2 diabetes focuses on dietary and behavioral interventions, with limited effective pharmacologic interventions available. Indeed, nutrition and lifestyle interventions remain the key tools to prevent childhood obesity and its comorbidities (20, 21). Ultra-processed food (22) and high-fructose beverages (23) are major sources of energy for children, both of which are associated with higher cardiometabolic risk (24–26). Despite this, children are exposed to the marketing of such products through techniques that exploit their developmental vulnerabilities.
It has been estimated that dietary changes may prevent ~11 millions deaths per year, that represent from the 19% to the 24% of deaths in adulthood. The benefit deriving from a healthy diet may be accounted as direct benefits—when directly impacting the disease determinants (e.g., reducing fat-saturated food directly impact cardiovascular risk) and indirect. These latter include the global impact of choosing sustainable foods, that include preferring plant-based dietary patterns (fruits, vegetables, nuts, seeds and whole grains—while limiting animal source foods), reducing food waste, and improving food production practices. Such an approach would imply a new definition of agricultural priorities and would imply an action at different levels of the food chain.
Sustainability of food results from the action of different “influencers”—determinants (27), that involves the food chain of production, the individual and collective choices and, ultimately, the food consumption. This latter is by itself a major determinant of food sustainability, thereby healthy food choices may drive food production chain in a bidirectional way.
Nutrition interventions should target not only children themselves, but their families and schools, along with food industries. Sustainable food promotion targets consumers but also regional and national authorities deputed to the agriculture to shift the current food-production paradigms.
We identified two main intervention areas (20, 21): healthy food choices, education in food preparation. The access to age-appropriate high-quality nutrition is an important step toward combating malnutrition, one of the WHO millennium goals (28, 29). Malnutrition in Europe and North America is largely due to poor-quality nutrition (23). Food marketing, and children's own food preferences (including their requests for purchase and consumption) are major determinants of the obesity epidemic. Governments in France, Israel, and the United Kingdom have endorsed labeling policies that provide qualitative information on nutrient content, including highlighting excess salt and fat, and, in certain cases, age-appropriateness. Considering the needs of children when labeling food is a mandatory step if governments are to support healthy choices. Our recommendations combine guidelines from the American Heart Association (AHA) (30), WHO (31), and UNICEF (27), and target the two environments where food is consumed during childhood: schools and homes. As summarized in Table 1, interventions are meant to guide food choices, instead of defining age-adjusted dietary regimens. This strategy has been proven to be effective in large clinical studies (20, 21) and regional programs.

Table 1. Nutrition.
Educational programs aimed to implement healthy food choice have a successful track record: family-based lifestyle intervention targeting for children and their families—and accounting for minorities and divesified groups—have been proven to successfully impact glucose tolerance and body weight in a safe and sustainable way (20, 21).
The Call for action includes proposals aimed at communities and industry.
The longitudinal Evaluation of the interventions will rely on regional studies tracking the prevalence of obesity and glucose metabolism impairment. Local authorities are expected to verify quality assessment of school nutrition.
The AHA defines good cardiovascular health through seven health behaviors: abstinence from smoking; body-mass index <85th percentile; ≥60 min of moderate or vigorous physical activity daily; a diet emphasizing fruits, vegetables, fish, and whole grains, low in sodium and with few sugar-laden foods and drinks (40, 41); total cholesterol <170 mg/dL; blood pressure <90th percentile; and a fasting plasma glucose level <100 mg/dL (42). Less than 50% of adolescents aged 12–19 y achieve at least five out of these seven behaviors. As ~80% of cardiovascular events (CVD) could be prevented through these health behaviors (43), educational interventions starting in childhood are expected to have the highest impact on the incidence of CVD in adulthood (41). Beside nutrition (see Section Introduction), physical activity and screen time are the two main behavioral interventions able to affect the lifetime trajectory of cardiovascular risk.
Physical activity (structured or unstructured) for preschool (44, 45) and school children (46) is a major determinant of pediatric health. Physical activity in preschool age is important to develop large motor skills and foster coordination (important aspects of school readiness), yet infants and preschool children in many middle- and high-income countries spend more than 30% of their time in sedentary activities such as screen time (45, 46).
Screen time is defined as the time spent engaging with visual screen-based technologies such as televisions, computers, videogames, smart phones, and tablets, including accessing the Internet and social media. In the last decade, there has been a widespread cultural adoption of media devices in young children; in one French study in 2018, 90% of those aged 2 y used touch-screen devices (47, 48). In this rapidly evolving digital age, much more time is spent in front of screens than previous generations; children's screen use is a key concern for parents and healthcare providers (49).
Evidence suggests that moderate screen time can be beneficial to children's wellbeing, widening social connections and improving learning skills, especially from activities including education and early learning. However, excessive use can be detrimental (50, 51), with potential negative impacts on physical, cognitive, emotional, and social wellbeing (48, 52), including a range of adverse physical, psychosocial, and cognitive outcomes (53). Further, the “time displacement hypothesis” suggests that excessive screen time displaces important protective health behaviors such as physical activity, green time, and adequate sleep (54). In addition, excessive screen time and social media use by children is associated with the development of obesity, sleep disturbances/problems (55), language delay, inattention (or attention disorders) (56), and depression (53, 57, 58). Yet, <20% of pediatricians ask families about their children's use of electronic devices (59, 60).
Proposed interventions target families, schools and primary healthcare providers.
Interventions to promote physical activity and reducing screen time are summarized in Table 2. Age-specific recommendations are provided and should be explained with oral and written informative factsheets to families. Healthcare providers are the primary information source to effectively promote physical activity in preschool children, and one of the main sources of information in school-aged children along with schools. Universal screening for dyslipidemia at 9–11 years is still controversial (37), though scientific societies convened for the necessity for screening at risk children (overweight/obese children with/without a family history of early CVD) (Table 2) (61).
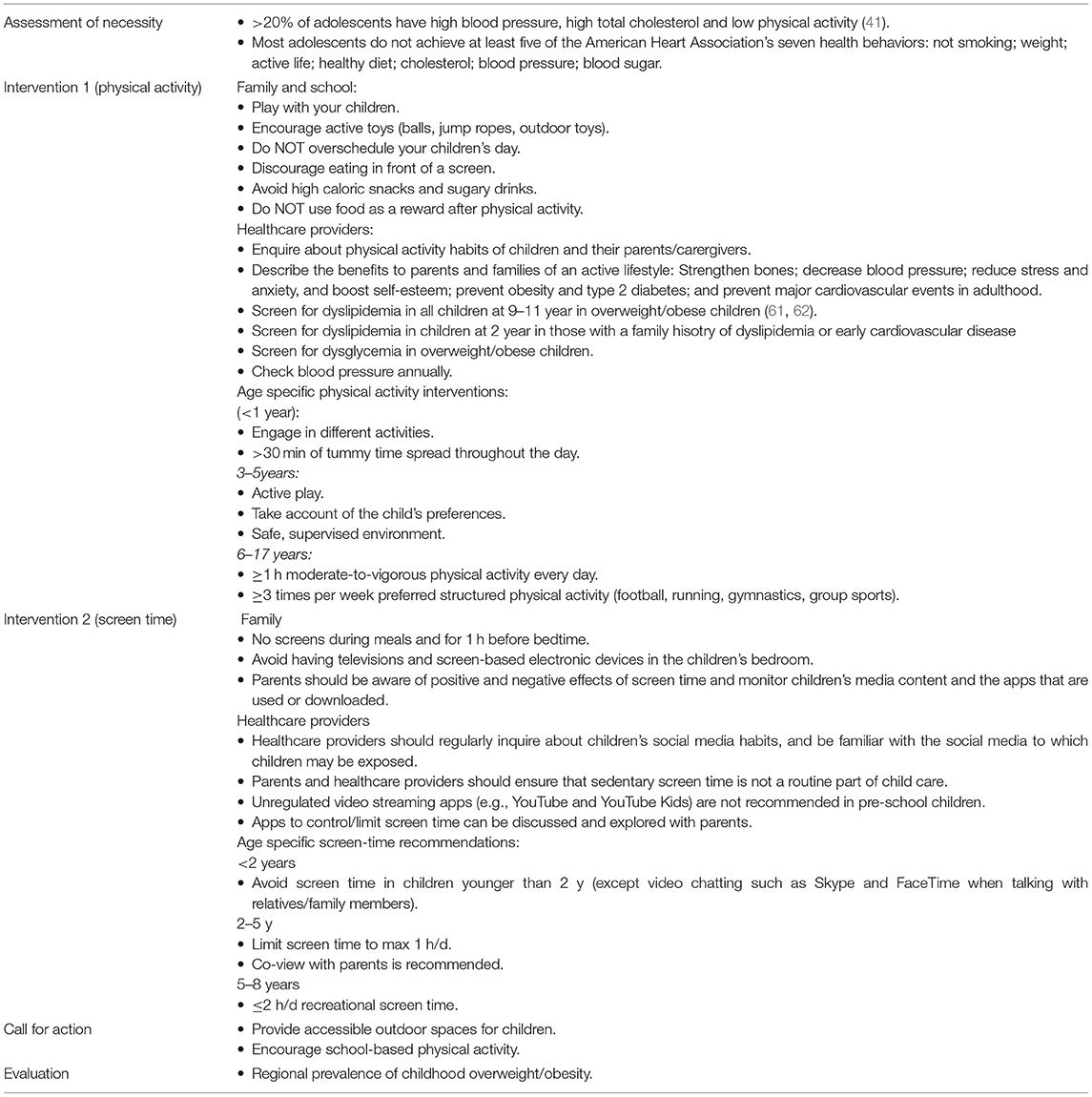
Table 2. Cardiovascular health.
The Call for action involves institutional local and regional groups to facilitate access to spaces for physical activity.
The Evaluation of the proposed interventions is through the prevalence in children of the seven cardiovascular health behaviors.
Chronic respiratory diseases (CRD)—and in particular chronic obstructive pulmonary disease (COPD) and asthma—contribute significantly to the global burden of NCDs, and are major causes of morbidity and mortality. Tobacco smoking, e-cigarettes (vaping), and air pollution increase the burden of CRD. Further, although e-cigarettes have been proposed as an aid to smoking cessation in adults, there is mixed evidence for their effectiveness (63), and they can be a gateway to tobacco and nicotine use in adolescents naïve to tobacco (64, 65), E-cigarette users outnumber traditional smokers among adolescents (66); in one study 27.5% of high school and 10.5% of middle school students were current e-cigarette users (67), and in another, half of e-cigarette users aged 15–17 y had never used combustible cigarettes (68). This high use of e-cigarettes is of concern, as adolescents using e-cigarettes have an increased incidence of chronic bronchitis and asthma exacerbations compared with non-users (69, 70). E-cigarette use is also becoming more common in pregnant women, thus exposing the developing fetus to nicotine, which crosses the placenta and thus reaches the fetal bloodstream. Nicotine is not only a known teratogen (71, 72), but has been associated with major congenital anomalies such as cleft palette, prematurity and stillbirth (73, 74).
Pollution is a major contributor to global morbidity and mortality (75). Children are especially vulnerable to the effects of pollution as they receive a relatively higher dose of toxins in any given environment, and are also more susceptible due to the physiology of their developing airways (76). Further, maternal exposure to pollutants during pregnancy may affect lung development in offspring (75). There is also convincing evidence that air pollution has negative impacts on respiratory health during childhood, and is associated with reduced maximal lung growth function (77, 78), potentially leading to the development of asthma (79) and COPD (80, 81).
Asthma is more common in children exposed to particulate air pollution, and there is evidence of a correlation between traffic-related air pollution and asthma occurrence (82, 83). Ambient air pollution is therefore recognized as a preventable risk factor for a spectrum of pediatric health problems (84).
Interventions should target families, healthcare practitioners and community/social organizations.
Interventions include educational sessions to be delivered through healthcare providers and schools, and local-community programs and regional politics aimed to reduce pollution exposure. Interventions are summarized in Table 3.
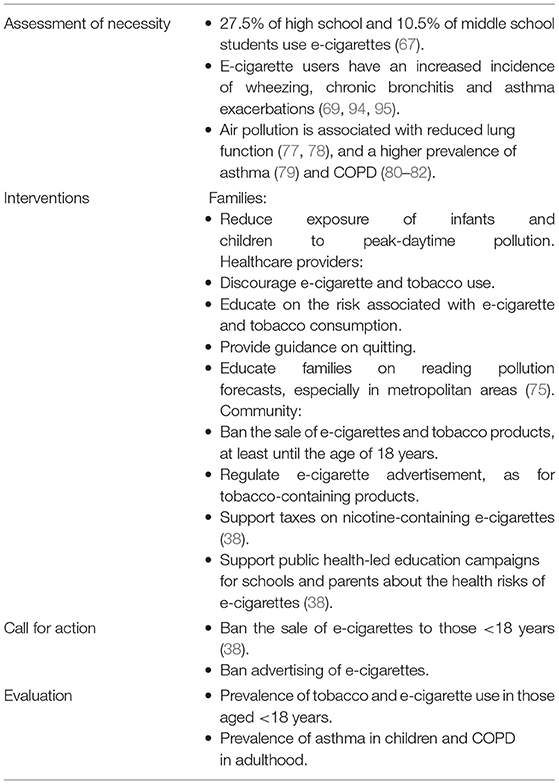
Table 3. Respiratory health.
The Call for action targets e-cigarette regulatory policies, which are currently highly heterogeneous (85).
The efficacy of the proposed interventions can be evaluated through the prevalence of asthma in childhood and of COPD in adulthood from population studies.
Neuropsychiatric conditions are the leading cause of disability in young people, with half of all chronic mental illnesses beginning by the age of 14 years. Suicide is the second cause of death in adolescents and young adults, with 10 out of 100,000 adolescents completing suicide each year (86), while attention-deficit/hyperactivity disorder (ADHD), behavior problems, anxiety, and depression are the most common mental disorders in children (87). Further, gender discrimination and economic inequity are key determinants of mental health in children (62, 88, 89).
The COVID-19 pandemic, with the resulting quarantine, social isolation, mortality, and lack of proper education, has dramatically accelerated the course of a variety of childhood mental illnesses. Community includes family, schools, and peers; thus, to achieve optimal mental wellbeing a child needs support across these domains. Gender identity, self-image and family/school environment are the three key areas for childhood mental wellbeing.
Gender interacts with, but is different from, the binary categories of biological sex. Girls (but not boys) are more likely to view girls as victims of discrimination than boys, and children with egalitarian gender attitudes are more likely to perceive discrimination than are their peers (39, 90). Youths with lesbian, gay, bisexual, transgender, or queer (LGBTQ) orientations have higher rates of anxiety and mood disorders, as well as suicide and suicide attempts. Promoting acceptance of gender diversity allows children to develop without the burden of social isolation and discrimination that people may experience surrounding their gender identity.
The health impact of social media on children is greatest on mental health, and specifically self-esteem and wellbeing, with related issues around cyberbullying, with an association between the use of social media and self-esteem or body image. One of the more recent impacts of social media during the COVID-19 pandemic has been a sharp increase in eating disorders among children, in particular female teenagers. These vulnerable children restrict food and exercise excessively, presenting to pediatric wards with signs and symptoms of extreme starvation.
Income remains a major determinant of family and individual mental health (88). A population study in Great Britain found that the more debt people had, the more likely they were to have some form of mental disorder, even after adjustment for income and other sociodemographic variables. A review of European population surveys found that depression and anxiety are associated with low educational attainment, material disadvantage and unemployment, and for older people, social isolation. The pattern of social distribution of common mental disorders is observed as a social class gradient and is more marked in women than in men.
The impact of economical inequity goes beyond the paradigm of mental health: families' income impact the access to healthy food and food insecurity is, in turn, a major determinant of pediatric obesity. Thereby, the sociodemographic interactions– as resulting from housing policies, social interactions, neighborhood features—determine the individual risk of pediatric and adulthood obesity (62, 91).
The concept of ACEs—adverse childhood experiences—such as poverty, discrimination, loss of a parent, insecure housing put children at higher risk of poor physical and mental health outcomes in adulthood. Interventions to reduce and mitigate ACEs will have tremendous payoffs as these children grow into working happy and healthy adults.
Exposure to violence and poverty during childhood and adolescence is an independent risk factor for risky behaviors as substance abuse and alcohol use among adolescence. In spite of a transient decrease for substance abuse during the first year of COVID-19 pandemic, almost 5% of youth between 8 and 12th grade use illicit drugs other than marijuana and ~17% of eight graders consume alcohol (92).
Mental health cannot be improved by policies focused only on the most disadvantaged, but should consider the community as a whole, supporting children's capability to do and to be. Policies should be universal yet proportionate to need. Focusing solely on the most disadvantaged will fail to achieve the required reduction in health inequalities necessary to reduce the steepness of the social gradient in health. Families, schools, communities are the target bodies for interventions aimed to preserve and promote mental and social health of youth.
The interventions are based on the scientific consensus that giving every child the best possible start will generate the greatest societal and mental health benefits (93). Certain subgroups are at a higher risk of mental disorders because of greater exposure and vulnerability to unfavorable social, economic, and environmental circumstances, interrelated with gender.
Facilitating the access to diagnosis and support for children and families living with mental health disorders is of pivotal importance. Recommended interventions are deployed at schools (presence of advisors and supports), at home to support families within the domestic environment or to ensure a shelter environment as necessary, and in local communities (Table 4). Screening for substance abuse in primary care should be advised starting 8th grade (92).
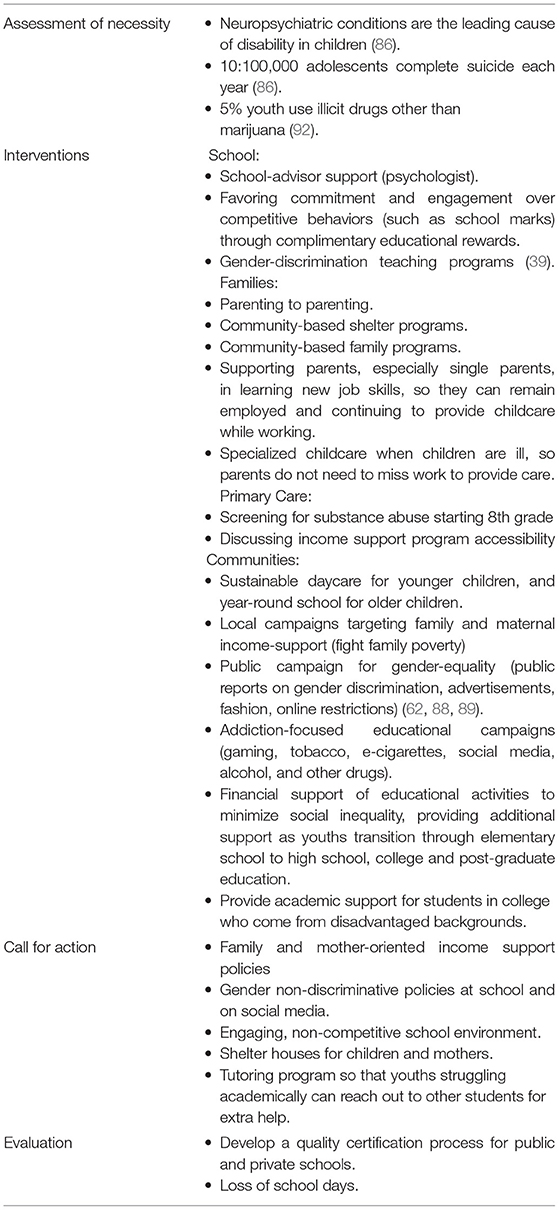
Table 4. Mental and social health.
The call for action to maximize the impact of the proposed interventions involves supporting shelter houses for children and mothers, creating engaging, non-competitive school environments, and gender non-discriminative policies at school and in the media. These interventions are expected to reduce the risk determinants of mental health disorders in children, though their implementation relies on regional and state policies.
Community-based interventions targeting poverty remain a major leverage to promote mental health throughout all the age groups.
The evaluation of the efficacy of regional and state interventions could be quantified through certification processes for schools and educational environments. Additionally, regional school performance could be an indirect measure of effective mental health programs on a regional basis.
Less than 2% of young adults (<30 years) have a healthy lifestyle, and no more than 50% of adolescents aged 12–19 years meet at least five of the seven ideal cardiovascular health behaviors. Childhood presents a unique window of opportunity to effect strategic interventions to promote healthy lifestyles, due to the metabolic and brain plasticity of children. Interventions targeting childhood therefore hold the potential to dramatically abate the rising incidence of NCDs and should involve families, schools and community-social groups. The ALICE approach we propose aims to define priority areas, targets and interventions, actions and measurable indicators to be used by primary healthcare providers and pediatricians to address health promotion strategies in childhood.
EB and AG designed the project and drafted the manuscript. GP, MG, ASi, and AR contributed to the Mental and Social Health section. AG and SC contributed to the Nutrition section. GD and RV contributed to the Cardiovascular Health section. EB and PS contributed to the Respiratory Health section. LD, CG, ASt, RR, and EB critically revised the manuscript. All authors approved the final version of the document.
This document was supported by an unrestricted grant from the University of Padova on the occasion of the 800 years anniversary (800 years Committee 1222-2022).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are grateful to the Italian Society of Pediatrics for non-conditional endorsement and to the Salus Pueri Foundation of the Department of Woman and Child's Health at the University Hospital of Padova (Padova, Italy) for logistic support.
1. Lloyd J, Creanor S, Logan S, Green C, Dean S, Hillsdon M, et al. Effectiveness of the healthy lifestyles programme (HeLP) to prevent obesity in UK primary-school children: a cluster randomised controlled trial. Lancet Child Adolesc Health. (2018) 2:35–45. doi: 10.1016/S2352-4642(17)30151-7
2. Marques A, Bordado J, Tesler R, Demetriou Y, Sturm D, de Matos M. A composite measure of healthy lifestyle: a study from 38 countries and regions from Europe and North America, from the health behavior in school-aged children survey. Am J Hum Biol. (2020) 32:e23419. doi: 10.1002/ajhb.23419
3. Dabelea D, Stafford JM, Mayer-Davis EJ, D'Agostino R, Dolan L, Imperatore G, et al. Association of type 1 diabetes vs type 2 diabetes diagnosed during childhood and adolescence with complications during teenage years and young adulthood. JAMA. (2017) 317:825–35. doi: 10.1001/jama.2017.0686
4. NCD Countdown 2030 collaborators. Worldwide trends in non-communicable disease mortality and progress towards sustainable development goal target 3.4. Lancet. (2018) 392:1072–88. doi: 10.1016/S0140-6736(18)31992-5
5. Horton R. Offline: science and politics in the era of COVID-19. Lancet. (2020) 396:1319. doi: 10.1016/S0140-6736(20)32221-2
6. Coates MM, Kintu A, Gupta N, Wroe EB, Adler AJ, Kwan GF, et al. Burden of non-communicable diseases from infectious causes in 2017: a modelling study. Lancet Glob Health. (2020) 8:e1489–8. doi: 10.1016/S2214-109X(20)30358-2
7. Harper ME, Patti ME. Metabolic terminology: what's in a name? Nat Metab. (2020) 2:476–7. doi: 10.1038/s42255-020-0216-7
8. Galderisi A, Giannini C, Weiss R, Kim G, Shabanova V, Santoro N, et al. Trajectories of changes in glucose tolerance in a multiethnic cohort of obese youths: an observational prospective analysis. Lancet Child Adolesc Health. (2018) 2:726–35. doi: 10.1016/S2352-4642(18)30235-9
9. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/s0749-3797(98)00017-8
10. Fandakova Y, Hartley CA. Mechanisms of learning and plasticity in childhood and adolescence. Dev Cogn Neurosci. (2020) 42:100764. doi: 10.1016/j.dcn.2020.100764
11. Fernandez-Jimenez R, Al-Kazaz M, Jaslow R, Carvajal I, Fuster V. Children present a window of opportunity for promoting health: JACC review topic of the week. J Am Coll Cardiol. (2018) 72:3310–9. doi: 10.1016/j.jacc.2018.10.031
12. SEARCH for Diabetes in Youth Study Group, Liese AD, D'Agostino RB Jr, Hamman RF, Kilgo PD, Lawrence JM, et al. The burden of diabetes mellitus among US youth: prevalence estimates from the SEARCH for diabetes in youth study. Pediatrics. (2006) 118:1510–8. doi: 10.1542/peds.2006-0690
13. Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. SEARCH for diabetes in youth study. Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. (2017) 376:1419–29. doi: 10.1056/NEJMoa1610187
14. Centers for Disease Control Prevention. Childhood Obesity Facts | Overweight & Obesity. (2021). Available online at: https://www.cdc.gov/obesity/data/childhood.html (accessed April 05, 2021).
15. Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B, Allen K, et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med. (2002) 346:802–10. doi: 10.1056/NEJMoa012578
16. RISE Consortium. Metabolic contrasts between youth adults with impaired glucose tolerance or recently diagnosed type 2 diabetes: I. Observations using the hyperglycemic clamp. Diabetes Care. (2018) 41:1696–706. doi: 10.2337/dc18-0244
17. Imperatore G, Boyle JP, Thompson TJ, Case D, Dabelea D, Hamman RF, et al. Projections of type 1 and type 2 diabetes burden in the U.S. population aged <20 years through 2050: dynamic modeling of incidence, mortality, and population growth. Diabetes Care. (2012) 35:2515–20. doi: 10.2337/dc12-0669
18. Hamman RF, Bell RA, Dabelea D, D'Agostino RB Jr, Dolan L, Imperatore G, et al. The SEARCH for diabetes in youth study: rationale, findings, and future directions. Diabetes Care. (2014) 37:3336–44. doi: 10.2337/dc14-0574
19. TODAY Study Group, Bjornstad P, Drews KL, Caprio S, Gubitosi-Klug R, Nathan DM, et al. Long-term complications in youth-onset type 2 diabetes. N Engl J Med. (2021) 385:416–26. doi: 10.1056/NEJMoa2100165
20. Savoye M, Caprio S, Dziura J, Camp A, Germain G, Summers C, et al. Reversal of early abnormalities in glucose metabolism in obese youth: results of an intensive lifestyle randomized controlled trial. Diabetes Care. (2014) 37:317–24. doi: 10.2337/dc13-1571
21. Savoye M, Shaw M, Dziura J, Tamborlane WV, Rose P, Guandalini C, et al. Effects of a weight management program on body composition and metabolic parameters in overweight children: a randomized controlled trial. JAMA. (2007) 297:2697–704. doi: 10.1001/jama.297.24.2697
22. Wang L, Martínez Steele E, Du M, Pomeranz JL, O'Connor LE, Herrick KA, et al. Trends in consumption of ultraprocessed foods among US youths aged 2-19 years, 1999-2018. JAMA. (2021) 326:519–30. doi: 10.1001/jama.2021.10238
23. Fidler Mis N, Braegger C, Bronsky J, Campoy C, Domellöf M, Embleton ND, et al. ESPGHAN committee on nutrition:. Sugar in infants, children and adolescents: a position paper of the European society for paediatric gastroenterology, hepatology and nutrition committee on nutrition. J Pediatr Gastroenterol Nutr. (2017) 65:681–96. doi: 10.1097/MPG.0000000000001733
24. Van Name M, Giannini C, Santoro N, Jastreboff AM, Kubat J, Li F, et al. Blunted suppression of acyl-ghrelin in response to fructose ingestion in obese adolescents: the role of insulin resistance. Obesity. (2015) 23:653–61. doi: 10.1002/oby.21019
25. Galderisi A, Giannini C, Van Name M, Caprio S. Fructose consumption contributes to hyperinsulinemia in adolescents with obesity through a GLP-1-mediated mechanism. J Clin Endocrinol Metab. (2019) 104:3481–90. doi: 10.1210/jc.2019-00161
26. Morgan RE. Does consumption of high-fructose corn syrup beverages cause obesity in children? Pediatr Obes. (2013) 8:249–54. doi: 10.1111/j.2047-6310.2013.00173.x
27. United Nations Children's Emergency Fund (UNICEF). Nutrition, for Every Child. Available online at: https://www.unicef.org/media/92031/file/UNICEF%20Nutrition%20Strategy%202020-2030.pdf
28. Oruamabo RS. Child malnutrition and the millennium development goals: much haste but less speed? Arch Dis Child. (2015) 100(Suppl. 1):S19–22. doi: 10.1136/archdischild-2013-305384
29. World Health Organization. Millennium Development Goals (MDGs). Available online at: https://www.who.int/news-room/fact-sheets/detail/millennium-development-goals-(mdgs) (accessed February 1, 2022).
30. Gidding SS, Dennison BA, Birch LL, Daniels SR, Gillman MW, Lichtenstein AH, et al. Dietary recommendations for children and adolescents: a guide for practitioners. Pediatrics. (2006) 117:544–59. doi: 10.1542/peds.2005-2374
31. World Health Organization. Comprehensive Implementation Plan on Maternal, Infant and Young Child Nutrition: World Health Organization. (2018). Available online at: https://www.who.int/nutrition/publications/CIP_document/en/ (accessed April 24, 2018).
32. Weinstock RS, Drews KL, Caprio S, Leibel NI, McKay SV, Zeitler PS, et al. Metabolic syndrome is common and persistent in youth-onset type 2 diabetes: results from the TODAY clinical trial. Obesity. (2015) 23:1357–61. doi: 10.1002/oby.21120
33. Food and Agriculture Organization of the United Nations. Food Labelling. (2021). Available online at: https://www.fao.org/food-labelling/en/ (accessed February 1, 2022).
34. Lobstein T, Jackson-Leach R, Moodie ML, Hall KD, Gortmaker SL, Swinburn BA, et al. Child and adolescent obesity: part of a bigger picture. Lancet. (2015) 385:2510–20. doi: 10.1016/S0140-6736(14)61746-3
35. Dereń K, Dembiński Ł, Wyszyńska J, Mazur A, Weghuber D, Łuszczki E et al. Front-of-pack nutrition labelling: a position statement of the European academy of paediatrics and the European childhood obesity group. Ann Nutr Metab. (2021) 77:23–8. doi: 10.1159/000514336
36. Sassi F, Belloni A, Mirelman A, Suhrcke M, Thomas A, Salti N, et al. Equity impacts of price policies to promote healthy behaviours. Lancet. (2018) 391:2059–2070. doi: 10.1016/S0140-6736(18)30531-2 [Epub ahead of print].
37. Margolis KL, Greenspan LC, Trower NK, Daley MF, Daniels SR, Lo JC, et al. Lipid screening in children and adolescents in community practice: 2007 to 2010. Circ Cardiovasc Qual Outcomes. (2014) 7:718–26. doi: 10.1161/CIRCOUTCOMES.114.000842
38. Chadi N, Schroeder R, Jensen JW, Levy S. Association between electronic cigarette use and marijuana use among adolescents and young adults: a systematic review and meta-analysis. JAMA Pediatr. (2019) 173:e192574. doi: 10.1001/jamapediatrics.2019.2574
39. Brown CS, Stone EA. Gender stereotypes and discrimination: how sexism impacts development. Adv Child Dev Behav. (2016) 50:105–33. doi: 10.1016/bs.acdb.2015.11.001
40. Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American heart association's strategic impact goal through 2020 and beyond. Circulation. (2010) 121:586–613. doi: 10.1161/CIRCULATIONAHA.109.192703
41. Shay CM, Ning H, Daniels SR, Rooks CR, Gidding SS, Lloyd-Jones DM. Status of cardiovascular health in US adolescents: prevalence estimates from the national health and nutrition examination surveys (NHANES) 2005-2010. Circulation. (2013) 127:1369–76. doi: 10.1161/CIRCULATIONAHA.113.001559
42. Steinberger J, Daniels SR, Hagberg N, Isasi CR, Kelly AS, Lloyd-Jones D, et al. Cardiovascular health promotion in children: challenges and opportunities for 2020 and beyond: a scientific statement from the American heart association. Circulation. (2016) 134:e236–55. doi: 10.1161/CIR.0000000000000441
43. Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. (2000) 343:16–22. doi: 10.1056/NEJM200007063430103
44. American Academy of Pediatrics. Preschooler - Physical Activity: @AmerAcadPeds. (2020). Available online at: http://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/HALF-Implementation-Guide/Age-Specific-Content/Pages/Preschooler-Physical-Activity.aspx (accessed February 1, 2022).
45. World Health Organization (WHO). Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children Under 5 Years of Age. (2019). Available online at: https://www.who.int/publications/i/item/9789241550536 (accessed February 1, 2022).
46. Centers for Disease Control Prevention. How Much Physical Activity do Children Need? (2021). Available online at: https://www.cdc.gov/physicalactivity/basics/children/index.htm (accessed May 08, 2021).
47. Cristia A, Seidl A. Parental reports on touch screen use in early childhood. PLoS ONE. (2015) 10:e0128338. doi: 10.1371/journal.pone.0128338
48. Straker L, Zabatiero J, Danby S, Thorpe K, Edwards S. Conflicting guidelines on young children's screen time and use of digital technology create policy and practice dilemmas. J Pediatr. (2018) 202:300–3. doi: 10.1016/j.jpeds.2018.07.019
49. Dumuid D. Screen time in early childhood. Lancet Child Adolesc Health. (2020) 4:169–70. doi: 10.1016/S2352-4642(20)30005-5
50. O'Keeffe GS, Clarke-Pearson K. Council on communications and media. The impact of social media on children, adolescents, and families. Pediatrics. (2011) 127:800–4. doi: 10.1542/peds.2011-0054
51. Richards D, Caldwell PH, Go H. Impact of social media on the health of children and young people. J Paediatr Child Health. (2015) 51:1152–7. doi: 10.1111/jpc.13023
52. American Academy of Child & Adolescent Psychiatry. Screen Time and Children 2021. Available online at: https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/Children-And-Watching-TV-054.aspx (accessed February 1, 2022).
53. Domingues-Montanari S. Clinical and psychological effects of excessive screen time on children. J Paediatr Child Health. (2017) 53:333–8. doi: 10.1111/jpc.13462
54. Roberts DF, Henriksen L, Voelker DH, van Vuuren DP. Television and schooling: displacement and distraction hypotheses. Austr J Educ. (1993) 37:198–211. doi: 10.1177/000494419303700207
55. Chindamo S, Buja A, DeBattisti E, Terraneo A, Marini E, Gomez Perez LJ, et al. Sleep and new media usage in toddlers. Eur J Pediatr. (2019) 178:483–90. doi: 10.1007/s00431-019-03318-7
56. Tamana SK, Ezeugwu V, Chikuma J, Lefebvre DL, Azad MB, Moraes TJ, et al. Screen-time is associated with inattention problems in preschoolers: results from the CHILD birth cohort study. PLoS ONE. (2019) 14:e0213995. doi: 10.1371/journal.pone.0213995
57. Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. (2019) 9:e023191. doi: 10.1136/bmjopen-2018-023191
58. Chen B, Bernard JY, Padmapriya N, Ning Y, Cai S, Lança C, et al. Associations between early-life screen viewing and 24 hour movement behaviours: findings from a longitudinal birth cohort study. Lancet Child Adolesc Health. (2020) 4:201–9. doi: 10.1016/S2352-4642(19)30424-9
59. Reid Chassiakos YL, Radesky J, Christakis D, Moreno MA, Cross C. Council on communications and media. Children and adolescents and digital media. Pediatrics. (2016) 138:e20162593. doi: 10.1542/peds.2016-2593
60. Hadjipanayis A, Efstathiou E, Altorjai P, Stiris T, Valiulis A, Koletzko B, et al. Social media and children: what is the paediatrician's role? Eur J Pediatr. (2019) 178:1605–12. doi: 10.1007/s00431-019-03458-w
61. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, Curry SJ, Davidson KW, Epling JW Jr, et al. Screening for lipid disorders in children and adolescents: US preventive services task force recommendation statement. JAMA. (2016) 316:625–33. doi: 10.1001/jama.2016.9852
62. Hodgkinson S, Godoy L, Beers LS, Lewin A. Improving mental health access for low-income children and families in the primary care setting. Pediatrics. (2017) 139:e20151175. doi: 10.1542/peds.2015-1175
63. Hajek P, Phillips-Waller A, Przulj D, Pesola F, Myers Smith K, Bisal N, et al. A randomized trial of E-cigarettes versus nicotine-replacement therapy. N Engl J Med. (2019) 380:629–37. doi: 10.1056/NEJMoa1808779
64. Cassidy RN, Meisel MK, DiGuiseppi G, Balestrieri S, Barnett NP. Initiation of vaporizing cannabis: individual and social network predictors in a longitudinal study of young adults. Drug Alcohol Depend. (2018) 188:334–40. doi: 10.1016/j.drugalcdep.2018.04.014
65. Soneji S, Barrington-Trimis JL, Wills TA, Leventhal AM, Unger JB, Gibson LA, et al. Association between initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: a systematic review and meta-analysis. JAMA Pediatr. (2017) 171:788–97. doi: 10.1001/jamapediatrics.2017.1488
66. Hammond D, Reid JL, Rynard VL, Fong GT, Cummings KM, McNeill A, et al. Prevalence of vaping and smoking among adolescents in Canada, England, and the United States: repeat national cross sectional surveys. BMJ. (2019) 365:l2219. doi: 10.1136/bmj.l2219
67. Cullen KA, Liu ST, Bernat JK, Slavit WI, Tynan MA, King BA, et al. Flavored tobacco product use among middle and high school students - United States, 2014-2018. MMWR Morb Mortal Wkly Rep. (2019) 68:839–44. doi: 10.15585/mmwr.mm6839a2
68. Vallone DM, Cuccia AF, Briggs J, Xiao H, Schillo BA, Hair EC. Electronic cigarette and JUUL use among adolescents and young adults. JAMA Pediatr. (2020) 174:277–86. doi: 10.1001/jamapediatrics.2019.5436
69. McConnell R, Barrington-Trimis JL, Wang K, Urman R, Hong H, Unger J, et al. Electronic cigarette use and respiratory symptoms in adolescents. Am J Respir Crit Care Med. (2017) 195:1043–9. doi: 10.1164/rccm.201604-0804OC
70. Xie W, Tackett AP, Berlowitz JB, Harlow AF, Kathuria H, Galiatsatos P, et al. Association of electronic cigarette use with respiratory symptom development among US young adults. Am J Respir Crit Care Med. (2022). doi: 10.1164/rccm.202107-1718OC [Epub ahead of print].
71. Czoli CD, Goniewicz ML, Palumbo M, White CM, Hammond D. E-cigarette nicotine content and labelling practices in a restricted market: findings from Ontario, Canada. Int J Drug Policy. (2018) 58:9–12. doi: 10.1016/j.drugpo.2018.04.001
72. Bozier J, Chivers EK, Chapman DG, Larcombe AN, Bastian NA, Masso-Silva JA, et al. The evolving landscape of e-cigarettes: a systematic review of recent evidence. Chest. (2020) 157:1362–90. doi: 10.1016/j.chest.2019.12.042
73. McGrath-Morrow SA, Gorzkowski J, Groner JA, Rule AM, Wilson K, Tanski SE, et al. The effects of nicotine on development. Pediatrics. (2020) 145:e20191346. doi: 10.1542/peds.2019-1346
74. Larcombe AN. Early-life exposure to electronic cigarettes: cause for concern. Lancet Respir Med. (2019) 7:985–92. doi: 10.1016/S2213-2600(19)30189-4
75. Landrigan PJ, Fuller R, Acosta NJR, Adeyi O, Arnold R, Basu NN, et al. The lancet commission on pollution and health. Lancet. (2018) 391:462–512. doi: 10.1016/S0140-6736(17)32345-0
76. Martinez FD. Early-life origins of chronic obstructive pulmonary disease. N Engl J Med. (2016) 375:871–8. doi: 10.1056/NEJMra1603287
77. Gauderman WJ, Avol E, Gilliland F, Vora H, Thomas D, Berhane K, et al. The effect of air pollution on lung development from 10 to 18 years of age. N Engl J Med. (2004) 351:1057–67. doi: 10.1056/NEJMoa040610
78. Soto-Martinez M, Sly PD. Relationship between environmental exposures in children and adult lung disease: the case for outdoor exposures. Chron Respir Dis. (2010) 7:173–86. doi: 10.1177/1479972309345929
79. Gehring U, Wijga AH, Hoek G, Bellander T, Berdel D, Brüske I, et al. Exposure to air pollution and development of asthma and rhinoconjunctivitis throughout childhood and adolescence: a population-based birth cohort study. Lancet Respir Med. (2015) 3:933–42. doi: 10.1016/S2213-2600(15)00426-9
80. Gauderman WJ, Urman R, Avol E, Berhane K, McConnell R, Rappaport E, et al. Association of improved air quality with lung development in children. N Engl J Med. (2015) 372:905–13. doi: 10.1056/NEJMoa1414123
81. Goldizen FC, Sly PD, Knibbs LD. Respiratory effects of air pollution on children. Pediatr Pulmonol. (2016) 51:94–108. doi: 10.1002/ppul.23262
82. Friedman MS, Powell KE, Hutwagner L, Graham LM, Teague WG. Impact of changes in transportation and commuting behaviors during the 1996 summer olympic games in Atlanta on air quality and childhood asthma. JAMA. (2001) 285:897–905. doi: 10.1001/jama.285.7.897
83. McConnell R, Berhane K, Gilliland F, London SJ, Islam T, Gauderman WJ, et al. Asthma in exercising children exposed to ozone: a cohort study. Lancet. (2002) 359:386–91. doi: 10.1016/S0140-6736(02)07597-9
84. Ramadour M, Burel C, Lanteaume A, Vervloet D, Charpin D, Brisse F, et al. Prevalence of asthma and rhinitis in relation to long-term exposure to gaseous air pollutants. Allergy. (2000) 55:1163–9. doi: 10.1034/j.1398-9995.2000.00637.x
85. Brumberg HL, Karr CJ. Council on environmental health. Ambient air pollution: health hazards to children. Pediatrics. (2021) 147:e2021051484. doi: 10.1542/peds.2021-051484
86. Centers for Disease Control Prevention. FastStats - Adolescent Health. (2021). Available online at: https://www.cdc.gov/nchs/fastats/adolescent-health.htm (accessed June, 11, 2021).
87. Centers for Disease Control Prevention. Data Statistics on Children's Mental Health | CDC: @CDCgov. (2021). Available online at: https://www.cdc.gov/childrensmentalhealth/data.html#ref (accessed March 22, 2021).
88. Sareen J, Afifi TO, McMillan KA, Asmundson GJ. Relationship between household income and mental disorders: findings from a population-based longitudinal study. Arch Gen Psychiatry. (2011) 68:419–27. doi: 10.1001/archgenpsychiatry.2011.15
89. Dohrenwend BP, Levav I, Shrout PE, Schwartz S, Naveh G, Link BG, et al. Socioeconomic status and psychiatric disorders: the causation-selection issue. Science. (1992) 255:946–52. doi: 10.1126/science.1546291
90. Spears Brown C, Bigler RS. Children's perceptions of gender discrimination. Dev Psychol. (2004) 40:714–26. doi: 10.1037/0012-1649.40.5.714
91. Andes LJ, Cheng YJ, Rolka DB, Gregg EW, Imperatore G. Prevalence of prediabetes among adolescents and young adults in the United States, 2005-2016. JAMA Pediatr. (2020) 174:e194498. doi: 10.1001/jamapediatrics.2019.4498
92. O'Rahilly S, Barroso I, Wareham NJ. Genetic factors in type 2 diabetes: the end of the beginning? Science. (2005) 307:370–3. doi: 10.1126/science.1104346
93. Weiss R, Santoro N, Giannini C, Galderisi A, Umano GR, Caprio S. Prediabetes in youth - mechanisms and biomarkers. Lancet Child Adolesc Health. (2017) 1:240–8. doi: 10.1016/S2352-4642(17)30044-5
94. Sly PD. Adverse environmental exposure and respiratory health in children. Pediatr Clin North Am. (2021) 68:277–91. doi: 10.1016/j.pcl.2020.09.018
Keywords: pediatric health care, non-communicable chronic diseases, pediatric preventative care, lifestyle related disease, lifestyle and behavior
Citation: Galderisi A, Perilongo G, Caprio S, Da Dalt L, Di Salvo G, Gatta M, Giaquinto C, Rizzuto R, Robb A, Sly PD, Simonelli A, Staiano A, Vettor R and Baraldi E (2022) Pediatric Preventive Care in Middle-High Resource Countries—The Padova Chart for Health in Children. Front. Pediatr. 10:803323. doi: 10.3389/fped.2022.803323
Received: 27 October 2021; Accepted: 14 February 2022;
Published: 14 April 2022.
Edited by:
Adamos A. Hadjipanayis, European University Cyprus, CyprusReviewed by:
Péter Altorjai, European Academy of Paediatrics (EAP), BelgiumCopyright © 2022 Galderisi, Perilongo, Caprio, Da Dalt, Di Salvo, Gatta, Giaquinto, Rizzuto, Robb, Sly, Simonelli, Staiano, Vettor and Baraldi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eugenio Baraldi, ZXVnZW5pby5iYXJhbGRpQHVuaXBkLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.