
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 15 April 2022
Sec. General Pediatrics and Pediatric Emergency Care
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.784911
 Sandra Herrera1*
Sandra Herrera1* Véronique Pierrat1,2
Véronique Pierrat1,2 Monique Kaminski1Valérie Benhammou1
Monique Kaminski1Valérie Benhammou1 Laetitia Marchand-Martin1
Laetitia Marchand-Martin1 Andrei S. Morgan1,3,4Elvire Le Norcy5Pierre-Yves Ancel1,6
Andrei S. Morgan1,3,4Elvire Le Norcy5Pierre-Yves Ancel1,6 Alice Germa1,7
Alice Germa1,7Introduction: Children born very preterm have an immature sucking reflex at birth and are exposed to neonatal care that can impede proper palate growth.
Objectives: We aimed to describe the frequency of high-arched palate and posterior crossbite at the age of 5 in children born very preterm and to identify their respective risk factors.
Methods: Our study was based on the data from EPIPAGE-2, a French national prospective cohort study, and included 2,594 children born between 24- and 31-week gestation. Outcomes were high-arched palate and posterior crossbite. Multivariable models estimated by generalized estimation equations with multiple imputation were used to study the association between the potential risk factors studied and each outcome.
Results: Overall, 8% of children born very preterm had a high-arched palate and 15% posterior crossbite. The odds of high-arched palate were increased for children with low gestational age (24–29 vs. 30–31 weeks of gestation) [adjusted odds ratio (aOR) 1.76, 95% confidence interval (CI) 1.17, 2.66], thumb-sucking habits at the age of 2 (aOR 1.53, 95% CI 1.03, 2.28), and cerebral palsy (aOR 2.18, 95% CI 1.28, 3.69). The odds of posterior crossbite were increased for children with pacifier-sucking habits at the age of 2 (aOR 1.75, 95% CI 1.30, 2.36).
Conclusions: Among very preterm children, low gestational age and cerebral palsy are the specific risk factors for a high-arched palate. High-arched palate and posterior crossbite share non-nutritive sucking habits as a common risk factor. The oro-facial growth of these children should be monitored.
Each year, 2.4 million babies are born very preterm worldwide (before 32-week gestation) (1). Children born very preterm are exposed to a wide range of major and minor health problems and impairments, which includes maxillofacial growth anomalies such as high-arched palate and posterior crossbite (2).
Both are maxillofacial growth anomalies occurring in the transverse plane and seem very related to each other. A high-arched palate (or high-vaulted palate) is characterized as an unusually high and narrow palate and thus may result in higher risk for malocclusion. Posterior crossbite is a transverse malocclusion most often associated with a narrow upper dental arch (the palatal cusps of the upper teeth do not fit in the central fossae of the lower teeth as expected) (3). Posterior crossbite may have functional consequences (difficulties in chewing and phonation), may, in some cases, lead to pain (in chewing muscles and in the temporomandibular joint), and may affect esthetics or generate psychological issues that may negatively affect emotional and social well-being (3–6). In addition, high-arched palate is often associated with decreased nasal airway volume, which predisposes the child to sleep disordered breathing (such as obstructive sleep apnea) (7, 8).
The frequency of high-arched palate has not been established owing to the lack of a standard definition (9, 10). Posterior crossbite has been estimated to occur in at least 17% of children born preterm (11) (13% of children born full-term) (12).
The transverse growth of the palate is enhanced by the pressure of the tongue against the palate. Insufficient transverse growth may occur if the tongue is not sufficiently competent (e.g., with neuromotor dysfunctions) (13) or if it remains in a low position (e.g., with a pacifier habit). Prolonged non-nutritive sucking habits (NNSHs, i.e., sucking a pacifier or thumb) are the main risk factors for both high-arched palate and posterior crossbite in children in the general population (14–17). Pacifier sucking is common and even recommended in infants born very preterm during neonatal hospitalization to support maturation of oro-facial motor function and to minimize pain (18–20). The frequency of NNSHs during infancy seems higher in infants born preterm than those born full-term (21).
Moreover, infants born very preterm may be exposed to intubation and tube feeding enhancing low tongue positioning. Consequently, identifying among factors linked to preterm birth those associated with maxillofacial growth anomalies may contribute to early diagnosis, thus facilitating timely interceptive orthodontic treatment (22).
Our work is based on EPIPAGE-2 data. EPIPAGE-2 is a French nationwide population-based cohort study designed to follow very preterm children born in 2011 during their first 12 years of life (23). The objectives of this current work, which is a part of the comprehensive 5-year medical and neurodevelopmental follow-up in the EPIPAGE-2 cohort study, were to describe the frequency of high-arched palate and posterior crossbite at the age of 5 and to identify the respective risk factors including neonatal characteristics and care, NNSHs at age 2, and cerebral palsy (CP) at the age of 5.
Children included in this study were the part of the EPIPAGE-2 national population-based cohort study (described elsewhere) (23). Briefly, children were recruited in 2011, during 8 months for those born between 24 and 26 completed weeks of gestation and during 6 months for those born between 27 and 31 weeks of gestation. Survivors were enrolled for longitudinal follow-up and were included in the study at the age of 2 corrected age and age 5 (hereafter age 5) if their parents consented. In this study, we included children with complete data on their NNSHs (pacifier or thumb/fingers) at the age of 2.
EPIPAGE-2 data were collected by the use of standardized questionnaires during the neonatal period and at the ages of 2 and 5. Neonatal questionnaires included demographic, social and delivery data, infant's condition at birth, neonatal complications, and care received in the neonatal intensive care unit (NICU). Pacifier and thumb-sucking habits were collected by the use of a self-administered questionnaire completed by the parents at the age of 2. At the age of 5, children were examined by pediatricians specifically trained for the study. This examination included a neurodevelopmental evaluation with the diagnosis of CP and a clinical oral assessment for high-arched palate and posterior crossbite.
The primary outcomes were high-arched palate and posterior crossbite (No/Yes) at the age of 5. High-arched palate was defined as deep and narrow. Posterior crossbite was defined as at least one mandibular molar cusp positioned buccal to the maxillary cups. Pediatricians were assisted in their assessment of high-arched palate and posterior crossbite by a guidance chart with illustrative drawings and photos (refer to Supplementary Figure S1).
The factors studied were selected based on their association with high-arched palate and posterior crossbite shown in the general population (24, 25) or in children born preterm (13, 26–29) and were defined as (1) neonatal characteristics: sex, gestational age (defined as the best obstetric estimate, combining the last menstrual period and the first-trimester ultrasonography assessment), small-for-gestational-age (defined as birth weight less than the 10th percentile according to the gestational age and sex based on French EPOPé intrauterine growth curves) (30), and severe neonatal morbidities (31) (including severe bronchopulmonary dysplasia, severe necrotizing enterocolitis, severe retinopathy, or severe cerebral abnormalities defined as intraventricular hemorrhage grade III/IV or cystic periventricular leukomalacia; definitions are provided in the note to Appendix 1); (2) neonatal care practices: duration of intubation (none or <24 h, 24 h−28 days, >28 days), feeding by nasogastric tube at 36 weeks, oral stimulation, and breastfeeding at discharge; (3) pacifier and thumb-sucking habits at the age of 2; and (4) CP at the age of 5 defined according to the criteria of the Surveillance of Cerebral Palsy in Europe (32) network.
Because the population was selected based on the children who survived to the age of 5 with complete data for NNSHs at the age of 2, we described perinatal and sociodemographic characteristics of children with complete data for NNSHs at the age 2 but with missing data for the outcomes at the age of 5 and those with missing data for NNSHs at the age of 2.
Frequencies of high-arched palate and posterior crossbite are described according to all the studied factors. All percentages and odds ratios (ORs) were weighted to account for differences in the sampling process between gestational age groups.
The adjusted analyses involved multivariable logistic regression models to identify the factors associated with high-arched palate and posterior crossbite, which includes neonatal factors (i.e., sex, gestational age, and small-for-gestational-age), neonatal morbidities and care practices (i.e., duration of intubation, oral stimulation, and breastfeeding at discharge), pacifier and thumb-sucking habits at the age of 2, and CP at the age of 5.
Intubation may be considered a marker of poor health, but endotracheal tubes also potentially exert pressure on the palate. Because of its relation with the palate area, duration of intubation was used in the final model rather than severe neonatal morbidities or feeding by nasogastric tube at 36 weeks, both being closely linked to duration of intubation.
Because twins and triplets share pregnancy and family characteristics, we used generalized estimation equations to take into account intra-family correlations (33). Results are reported as adjusted ORs (aORs) with 95% confidence intervals (95% Cls).
The analyses involved using imputed datasets to limit the possible impact of both lost to follow-up and missing data on the outcomes and covariates (34–36). The imputed datasets using chained equations were created using variables that potentially predicted non-response on the outcomes. Missing data were 36% of the outcome measures, and among covariates, 0% of neonatal factors, fewer than 6% of neonatal morbidities and care practices, and 20% of CP. In total, 50 independent imputed datasets were generated. Estimates were pooled according to the Rubin's rule (37). Further imputation details are provided in Supplementary Table S1. Statistical analyses were performed with R v3.6.3.
A total of two sensitivity analyses were performed, one of complete cases and the other of all children surviving at the age of 2 including those with missing data for NNSHs at the age of 2.
Among the 2,594 children alive at the age of 2 with the complete data on NNSHs, 2,488 were eligible for follow-up at the age of 5, and 1,654 had a medical examination with complete data regarding high-arched palate and posterior crossbite (Figure 1).
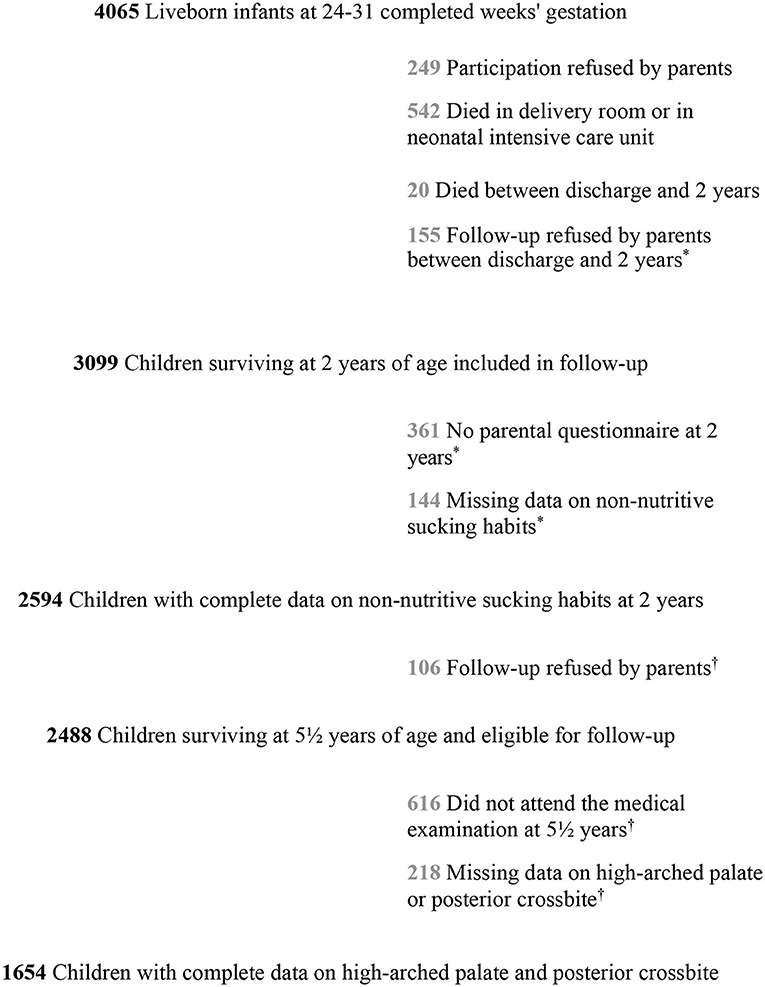
Figure 1. Flow chart of the study population: EPIPAGE-2 cohort at 5 years. *Considered “missing data on non-nutritive sucking habits at 2 years' corrected age” = 660 children. Considered “missing data at 5 years” = 940 children.
As compared to children included in the analysis, those with missing data at the age of 5 and those with missing data on NNSHs were more often born to mothers born outside France or to parents with low socioeconomic status and with 2 or more older siblings and were less frequently breastfed at discharge (Table 1).
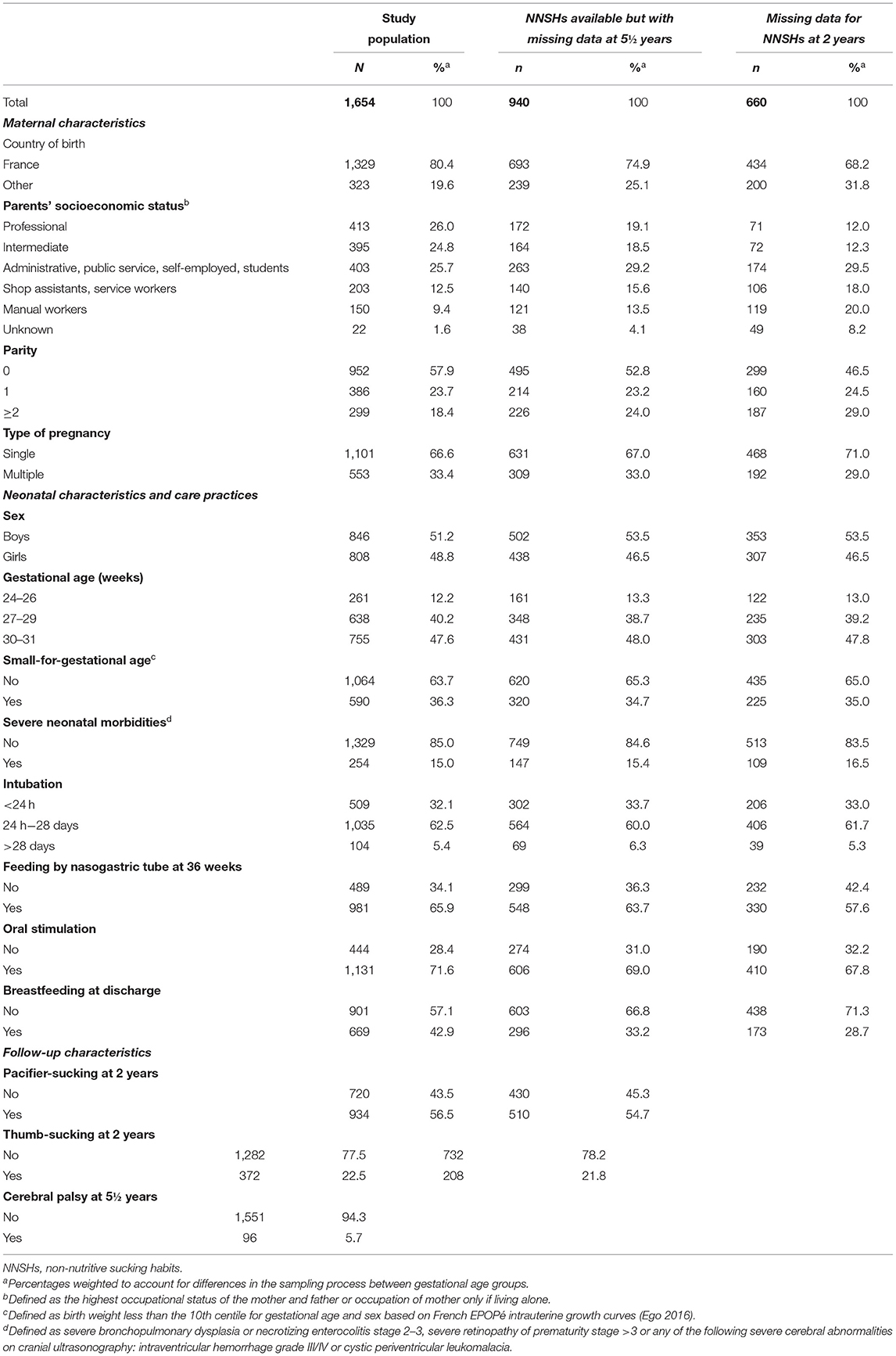
Table 1. Maternal, neonatal, and follow-up characteristics of the study population and those with missing data.
Among the 1,654 children with available information, 7.5% (95% CI 6.0–9.0) had a high-arched palate and 15.0% (95% CI 13.3–16.8) had a posterior crossbite (Table 2). After multiple imputation, the frequency of high-arched palate was 8.0% (95% CI 7.0–10.0), that of posterior crossbite was 15.0% (95% CI 13.7–16.5), that of anterior crossbite was 12% (95% CI 11.1–13.7), that of bilateral was crossbite 3% (95% CI 2.0–4.0), and that of complete crossbite (anterior crossbite and bilateral crossbite) was 1% (data not shown).

Table 2. Frequency of high-arched palate and posterior crossbite at 5 years by neonatal characteristics, non-nutritive sucking habits (NNSHs) at 2 years, and cerebral palsy at 5 years: complete cases (n = 1,654).
Table 3 shows the association between the two anomalies. In 70% of cases of high-arched palate, there was no posterior crossbite.
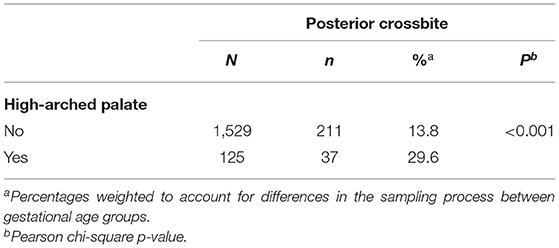
Table 3. Association between high-arched palate and posterior crossbite at 5 years.
Table 2 shows the distribution of high-arched palate and posterior crossbite according to the factors studied. After adjustment (Table 4), the odds of high-arched palate were increased for children with thumb-sucking habits at the age of 2 and children with CP. The odds of high-arched palate were increased with low gestational age (p = 0.05) and the lack of breastfeeding at discharge (p = 0.08), although not significantly. High-arched palate was not associated with sex, duration of intubation, oral stimulation in a NICU, or pacifier-sucking habits.
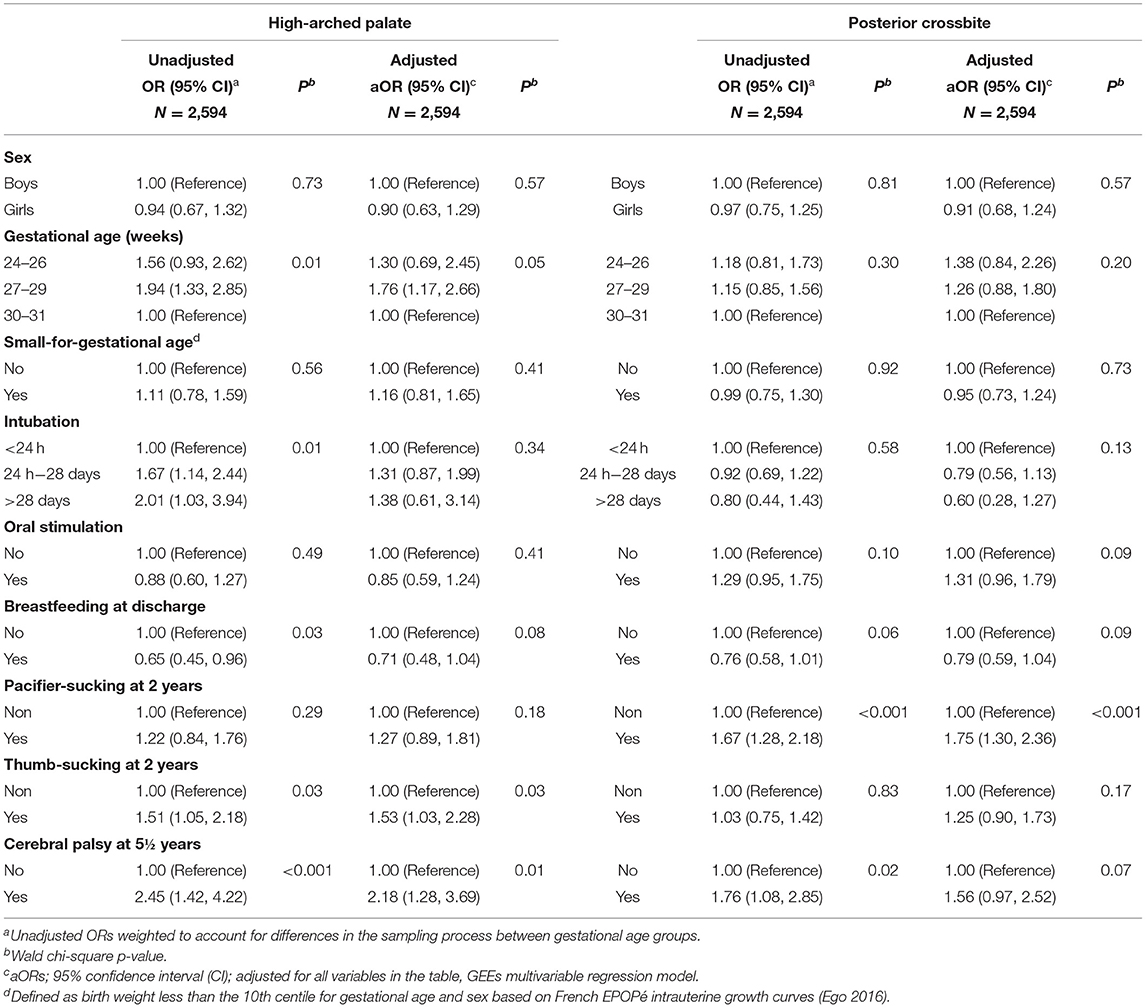
Table 4. High-arched palate and posterior crossbite at 5 years by neonatal characteristics, non-nutritive sucking habits (NNSHs) at 2 years and cerebral palsy at 5 years: unadjusted and adjusted odds ratios (ORs), multivariable regression models with generalized estimating equations (GEEs) and multiple imputation (n = 2,594).
The odds of posterior crossbite were increased for children with pacifier-sucking habits and children with CP (p = 0.07), although not significantly. Posterior crossbite was not associated with sex, duration of intubation, oral stimulation in a NICU, or thumb-sucking habits.
The results of the analyses of complete cases and children with missing data for NNSHs provided aORs very similar to those of children with complete data for NNSHs (Supplementary Tables S2, S3).
In this study, 8% of children had a high arched-palate and 15% a posterior crossbite at the age of 5. In 30% of cases of high-arched palate, these anomalies were associated with each other. High-arched palate was frequent in children with thumb-sucking habits and those with CP. Posterior crossbite was frequent in children with pacifier-sucking.
All data were collected prospectively, which includes pacifier and thumb-sucking habits at the age of 2, thus avoiding recall bias. The study population-based design and the large sample size provided reasonable precision in estimating frequencies and associations.
The main limitation of the study was missing data, mostly due to lost to follow-up at the ages of 2 and 5; multiple imputation was used to reduce the potential selection bias arising from this situation. Children with missing data for NNSHs were often born to mothers born outside of France and with a low socioeconomic background and were infrequently breastfed at discharge; thus, the association between breastfeeding and both outcomes might be underestimated.
In our study, both outcomes were assessed by the pediatricians. High-arched palate is present in many syndromic diseases (38, 39), and pediatricians are familiar with this clinical feature. Moreover, pediatricians were assisted by drawings and a photo chart for better consistency. However, pediatricians are not specialist in this area, even when specifically trained, we assumed that the more severe situations were more likely to be detected, situations that would most probably need orthodontic treatment; therefore, the frequency of high-arched palate is likely underestimated. The definition of posterior crossbite was more precise than that of high-arched palate, but its assessment was probably more unusual for examiners. Thus, even with the guidance chart, the pediatricians may have more difficulties with assessment, possibly leading to non-differential misclassification, which would imply an underestimation of posterior crossbite frequency.
Comparing the frequency of high-arched palate, we observed with that in the literature is difficult because of no standard definition (40). The previous studies among preterm or low-birth-weight infants have been conducted in the United States (26, 27), Brazil (28), and Japan (29), but included only small samples (37 to 74 children). However, the results of our study were consistent with those from the previous EPIPAGE study (13).
The frequency of posterior crossbite we observed was slightly lower than that observed in Finland (17% of children born preterm under the age of 6) (11) and the United States (17% of low-birth-weight children aged 2–5 and 22% of children aged 3–5) (26, 27). However, such frequencies do not vary much from the frequencies observed in the general population (up to 25%) (16, 24, 41).
We studied high-arched palate and posterior crossbite and associated risk factors in the same cohort of children born very preterm because both are related to possible problems in chewing, phonation, mouth breathing, and facial asymmetry. Both are the disorders of the transverse plane and are therefore linked, but they are neither superimposable nor embedded. High-arched palate is a more severe anomaly because growth in height occurs at the expense of width. However, posterior crossbite reflects a discrepancy in the relation between the upper maxillary arch and the lower mandibular arch. If both upper and lower arches are narrow, there is no posterior crossbite, but the situation may need treatment. If only one upper tooth is oriented lingually, there may be a posterior crossbite, but with less need for treatment.
Prolonged NNSHs have been associated with maxillofacial growth anomalies in children, including high-arched palate and posterior crossbite (14–16, 42–45). The habit of a thumb or a pacifier in the mouth accustoms the tongue to be in a low position where it cannot exert pressure on the palate, which potentially results in a high-arched palate. In contrast, low tongue position puts more constant pressure on the lower arch, thus enhancing its growth in the transverse direction and creating a growth discrepancy between the two arches and potential posterior crossbite (46). The evidence suggests that at least 2 years of pacifier use are necessary for substantial alteration in palate morphology (47). Preterm children seem more likely to have NNSHs than full-term children (69 vs. 51% at the age of 2) (16, 21).
This study demonstrated that thumb-sucking at the age of 2 was associated with high-arched palate at the age of 5 and pacifier-sucking with posterior crossbite. The vertical pressure of the thumb on the palate may be stronger than the pressure of the pacifier, thus leading to a deep palate. The studies of the general population in the United States and Europe found similar associations (16, 45, 48).
In our study, frequency of high-arched palate was high for children born at low gestational age. In addition to an immature sucking pattern, infants born very preterm are exposed to invasive neonatal care such as mechanical ventilation by a naso- or orotracheal tube. Orotracheal intubation seems to be associated with increased risk of high-arched palate or palatal groove (26, 28, 29). In our study, prolonged intubation was not associated with high-arched palate, perhaps because intubation is mainly nasal in France.
Neonatal units promote developmental practices (including oral stimulation and breastfeeding), which encourage sucking and feeding skills necessary for survival and better development of infants born very preterm. We expected such practices to play a protective role preventing the development of maxillofacial growth anomalies; however, oral stimulation was not associated with the anomalies in our study. Oral stimulation may include heterogeneous intraoral practices (sometimes with the use of pacifiers) and less “intrusive” practices (e.g., chin-only stimulation), which might not have the same impact on palatal growth.
Breastfeeding was associated with less NNSHs in children born very preterm (21). The recent studies of preterm children and the general population in Brazil concluded shorter duration of breastfeeding associated with increased risk of malocclusions (including posterior crossbite) at the age of 5 (25, 49). However, in one such study (25), the association between breastfeeding and posterior crossbite was observed only when it was not adjusted for NNSHs. Once adjusted for NNSHs, the association disappeared, as in our study. Because breastfeeding and NNSHs are closely related, in our case, we could not clearly distinguish the role that breastfeeding plays in the development of high-arched palate and posterior crossbite.
Cerebral palsy was assessed at the age of 5, but it reflects neurological disturbances that occur in the infant brain much earlier in life. Our study confirmed that children with CP are particularly at risk of high-arched palate. CP involves a limitation of oro-facial motor skills (50, 51), so the lingual pressure on the palate may be insufficient, possibly altering its growth. This result endorses close monitoring of maxillofacial growth in infants with CP born preterm. It also generates new research questions about specific care and future treatments that could be used for this spectrum of disorders.
Early interceptive orthodontic treatment aims to reduce the severity of maxillofacial growth anomalies or prevent a situation from becoming more severe. Interceptive treatment should be used at an early age (between 4–9 years old), its goal being to reduce the potential functional and aesthetic consequences of these anomalies over time. For example, in the case of a growth deficit in the upper maxillary arch, palatal expansion appliances are often used to help to stimulate the growth of the maxilla transversely (52). In the case of a posterior crossbite, removable expansion plates are often used to help to guide the growth of the upper maxillary alveolar processes outside the mandibular arch and thus reduce the risk of persistent malocclusion in the adult dentition (3). Another option is the use of a fixed appliance (Quand-helix) (53) that can help rotation of molars or create expansion at the premolar and canine levels (54).
Upper airway dimensions and craniofacial morphology are closely related (55). High-arched palate is often associated with mouth breathing and may even be a risk factor for sleep disorders breathing. (8, 56, 57). The recent research has assessed different orthodontic appliances (such as rapid maxillary expansion) as treatment modalities in pediatric obstructive sleep apnea (58). Even if evidence is still low to conclude, interdisciplinary collaboration between pediatricians and dentists such as sharing of early diagnoses could make it possible to prevent and treat these various disorders at the early stages. Moreover, high-arched palate could be a call sign for sleep-disordered breathing in child examination.
In this study among children born very preterm, we found high-arched palate associated with thumb-sucking habits and CP and posterior crossbite mainly associated with pacifier-sucking habits. The high frequency of both disorders justifies particular attention owing to potential longer-term consequences, as shown in other studies. The oral health of infants born very preterm should be regularly monitored throughout early childhood to identify and address these problems at the young age, especially when children have neuromotor dysfunctions or prolonged NNSHs.
Standardized definition of high-arched palate and other types of palatal alteration, which includes grooving, should be developed. Such definitions would help to improve the design of future clinical and observational studies and understanding the mechanisms associated with the occurrence of maxillofacial growth anomalies in general population and in children born preterm.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by French Data Protection Authority (Commission Nationale de l'informatique et des Libertés, No. 911009) and the two relevant Ethics Committees [the Consultative Committee on the Treatment of Information on Personal Health Data for Research Purposes (CCTIRS), No. 10.626, and the Committee for the Protection of People Participating in Biomedical Research (CPP), No. SC-2873]. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
SH conceptualized the study, carried out the analysis, and drafted the initial manuscript. VP, P-YA, and MK conceptualized and designed the study. VB coordinated and supervised the data collection. EL designed the data collection instrument. LM-M and AM supervised the statistical analysis. AG designed the study and supervised the statistical analysis. All authors revised and approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
The EPIPAGE-2 Study was supported by the French Institute of Public Health Research/Institute of Public Health and its partners: the French Health Ministry; the National Institute of Health and Medical Research (INSERM); the National Institute of Cancer, and the National Solidarity Fund for Autonomy (CNSA); The National Research Agency through the French EQUIPEX program of investments in the future (Reference ANR-11-EQPX-0038); the PREMUP Foundation; and the Foundation de France (Reference 00050329).
Alsace: D. Astruc, P. Kuhn, B. Langer, J. Matis (Strasbourg), C. Ramousset; Aquitaine: X. Hernandorena (Bayonne), P. Chabanier, L. Joly-Pedespan (Bordeaux), M.J. Costedoat, A. Leguen; Auvergne: B. Lecomte, D. Lemery, F. Vendittelli (Clermont-Ferrand); Basse-Normandie: G. Beucher, M. Dreyfus, B. Guillois (Caen), Y. Toure; Bourgogne: A. Burguet, S Couvreur, J.B. Gouyon, P. Sagot (Dijon), N. Colas; Bretagne: J. Sizun (Brest), A. Beuchée, P. Pladys, F. Rouget (Rennes), R.P. Dupuy (St-Brieuc), D. Soupre (Vannes), F. Charlot, S. Roudaut; Centre: A. Favreau, E. Saliba (Tours), L. Reboul; Champagne-Ardenne: N. Bednarek, P. Morville (Reims), V. Verrière; Franche-Comté: G. Thiriez (Besançon), C. Balamou; Haute-Normandie: L. Marpeau, S. Marret (Rouen), C. Barbier; Ile-de-France: G. Kayem (Colombes), X. Durrmeyer (Créteil), M. Granier (Evry), M. Ayoubi, A. Baud, B. Carbonne, L. Foix L'Hélias, F. Goffinet, P.H. Jarreau, D. Mitanchez (Paris), P. Boileau (Poissy), L. Cornu, R. Moras; Languedoc-Roussillon: P. Boulot, G. Cambonie, H. Daudé (Montpellier), A. Badessi, N. Tsaoussis; Limousin: A. Bédu, F. Mons (Limoges), C. Bahans; Lorraine: M.H. Binet, J. Fresson, J.M. Hascoët, A. Milton, O. Morel, R. Vieux (Nancy), L. Hilpert; Midi-Pyrénées: C. Alberge, C. Arnaud, C. Vayssière (Toulouse), M. Baron; Nord-Pas-de-Calais: M.L. Charkaluk, V. Pierrat, D. Subtil, P. Truffert (Lille), S. Akowanou, D. Roche; PACA et Corse: C. D'Ercole, C. Gire, U. Simeoni (Marseille), A. Bongain (Nice), M. Deschamps; Pays de Loire: B. Branger (FFRSP), J.C. Rozé, N. Winer (Nantes), V. Rouger, C. Dupont; Picardie: J. Gondry, G. Krim (Amiens), B. Baby; Rhône-Alpes: M. Debeir (Chambéry), O. Claris, J.C. Picaud, S. Rubio-Gurung (Lyon), C. Cans, A. Ego, T. Debillon (Grenoble), H. Patural (Saint-Etienne), A. Rannaud; Guadeloupe: E. Janky, A. Poulichet, J.M. Rosenthal (Point à Pitre), E. Coliné; Guyane: A. Favre (Cayenne), N. Joly; Martinique: S. Châlons (Fort de France), V. Lochelongue; La Réunion: P.Y. Robillard (Saint-Pierre), S. Samperiz, D. Ramful (Saint-Denis).
Inserm UMR 1153: P.Y. Ancel, V. Benhammou, B. Blondel, M. Bonet, A. Brinis, M.L. Charkaluk, A. Coquelin, M. Durox, L. Foix-L'Hélias, F. Goffinet, M. Kaminski, G. Kayem, B. Khoshnood, C. Lebeaux, L. Marchand-Martin, A.S. Morgan, V. Pierrat, J. Rousseau, M.J. Saurel-Cubizolles, D. Sylla, D. Tran, L. Vasante-Annamale, J. Zeitlin.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are grateful to the families of preterm infants for their participation in the EPIPAGE-2 cohort study and for the cooperation of all maternity and neonatal units in France. We thank the EPIPAGE-2 Study Group for its substantial contribution to the conception, design, and acquisition of data.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.784911/full#supplementary-material
1. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. (2012) 379:2162–72. doi: 10.1016/S0140-6736(12)60820-4
2. Paulsson L, Bondemark L, Söderfeldt B A. systematic review of the consequences of premature birth on palatal morphology, dental occlusion, tooth-crown dimensions, and tooth maturity and eruption. Angle Orthod. (2004) 74:269–79.
3. Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int J Paediatr Dent. (2004) 14:155–66. doi: 10.1111/j.1365-263X.2004.00546.x
4. Olsen JA, Inglehart MR. Malocclusions and perceptions of attractiveness, intelligence, and personality, and behavioral intentions. Am J Orthod Dentofacial Orthop. (2011) 140:669–79. doi: 10.1016/j.ajodo.2011.02.025
5. Magalhães IB, Pereira LJ, Marques LS, Gameiro GH. The influence of malocclusion on masticatory performance. A systematic review. Angle Orthod. (2010) 80:981–7. doi: 10.2319/011910-33.1
6. Dimberg L, Arnrup K, Bondemark L. The impact of malocclusion on the quality of life among children and adolescents: a systematic review of quantitative studies. Eur J Orthod. (2015) 37:238–247. doi: 10.1093/ejo/cju046
7. Löfstrand-Tideström B, Thilander B, Ahlqvist-Rastad J, Jakobsson O, Hultcrantz E. Breathing obstruction in relation to craniofacial and dental arch morphology in 4-year-old children. Eur J Orthod. (1999) 21:323–32. doi: 10.1093/ejo/21.4.323
8. Hansen C, Markström A, Sonnesen L. Specific dento-craniofacial characteristics in non-syndromic children can predispose to sleep-disordered breathing. Acta Paediatr. (2022) 111:473–7. doi: 10.1111/apa.16202
9. Hohoff A, Rabe H, Ehmer U, Harms E. Palatal development of preterm and low birthweight infants compared to term infants – What do we know? Part 1: the palate of the term newborn. Head Face Med. (2005) 1:8. doi: 10.1186/1746-160X-1-8
10. Hohoff A, Rabe H, Ehmer U, Harms E. Palatal development of preterm and low birthweight infants compared to term infants – What do we know? Part 2: the palate of the preterm/low birthweight infant. Head Face Medicine. (2005) 1:9. doi: 10.1186/1746-160X-1-9
11. Maaniitty E, Vahlberg T, Lüthje P, Rautava P, Svedström-Oristo A-L. Malocclusions in primary and early mixed dentition in very preterm children. Acta Odontol Scand. (2020) 78:52–6. doi: 10.1080/00016357.2019.1650954
12. Dimberg L, Bondemark L, Söderfeldt B, Lennartsson B. Prevalence of malocclusion traits and sucking habits among 3-year-old children. Swed Dent J. (2010) 34:35–42.
13. Germa A, Marret S, Thiriez G, Rousseau S, Hascoët J-M, Paulsson-Björnsson L, et al. Neonatal factors associated with alteration of palatal morphology in very preterm children: the EPIPAGE cohort study. Early Hum Dev. (2012) 88:413–20. doi: 10.1016/j.earlhumdev.2011.10.006
14. Zardetto CG., del C, Rodrigues CRMD, Stefani FM. Effects of different pacifiers on the primary dentition and oral myofunctional structures of preschool children. Pediatr Dent. (2002) 24:552–60.
15. Warren JJ, Bishara SE. Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition. Am J Orthod Dentofacial Orthop. (2002) 121:347–56. doi: 10.1067/mod.2002.121445
16. Duncan K, Mcnamara C, Ireland AJ, Sandy JR. Sucking habits in childhood and the effects on the primary dentition: findings of the Avon Longitudinal Study of Pregnancy and Childhood. Int J Paediatr Dent. (2008) 18:178–88. doi: 10.1111/j.1365-263X.2007.00905.x
17. Bueno SB, Bittar TO, Vazquez F de L, Meneghim MC, Pereira AC. Association of breastfeeding, pacifier use, breathing pattern and malocclusions in preschoolers. Dent Press J Orthod. (2013) 18:30e1–e6. doi: 10.1590/S2176-94512013000100006
18. Fucile S, Gisel E, Lau C. Oral stimulation accelerates the transition from tube to oral feeding in preterm infants. J Pediatr. (2002) 141:230–6. doi: 10.1067/mpd.2002.125731
19. Kristoffersen L, Skogvoll E, Hafström M. Pain reduction on insertion of a feeding tube in preterm infants: a randomized controlled trial. Pediatrics. (2011) 127:e1449–54. doi: 10.1542/peds.2010-3438
20. Arvedson Joan, Clark Heather, Lazarus Cathy, Schooling Tracy, Frymark Tobi. Evidence-based systematic review: effects of oral motor interventions on feeding and swallowing in preterm infants. Am J Speech-Lang Pathol. (2010) 19:321–40. doi: 10.1044/1058-0360(2010/09-0067)
21. Herrera S, Pierrat V, Kaminski M, Benhammou V, Bonnet A-L, Ancel P-Y, et al. Factors associated with non-nutritive sucking habits at 2 years of age among very preterm children: EPIPAGE-2 cohort study. Paediatr Perinat Epidemiol. (2021) 35:217–26. doi: 10.1111/ppe.12725
22. Caplin J, Han MD, Miloro M, Allareddy V, Markiewicz MR. Interceptive Dentofacial Orthopedics (Growth Modification). Oral Maxillofac Surg Clin North Am. (2020) 32:39–51. doi: 10.1016/j.coms.2019.08.006
23. Lorthe E, Benhammou V, Marchand-Martin L, Pierrat V, Lebeaux C, Durox M, et al. Cohort Profile: The Etude Epidémiologique sur les Petits Ages Gestationnels-2 (EPIPAGE-2) preterm birth cohort. Int J Epidemiol. (2021) 50:1428–29m. doi: 10.1093/ije/dyaa282
24. Germa A, Clément C, Weissenbach M, Heude B, Forhan A, Martin-Marchand L, et al. Early risk factors for posterior crossbite and anterior open bite in the primary dentition. Angle Orthod. (2016) 86:832–8. doi: 10.2319/102715-723.1
25. Peres KG, Cascaes AM, Peres MA, Demarco FF, Santos IS, Matijasevich A, et al. Exclusive breastfeeding and risk of dental malocclusion. Pediatrics. (2015) 136:e60–67. doi: 10.1542/peds.2014-3276
26. Fadavi S, Adeni S, Dziedzic K, Punwani I, Vidyasagar D. The oral effects of orotracheal intubation in prematurely born preschoolers. ASDC J Dent Child. (1992) 59:420–4.
27. Kopra DE, Davis EL. Prevalence of oral defects among neonatally intubated 3- to 5- and 7- to 10-year old children. Pediatr Dent. (1991) 13:349–55.
28. Cortines AAO, Costa LR. Associated factors and persistence of palatal groove in preterm infants: a cohort study. BMC Pediatr. (2016) 16:1–6. doi: 10.1186/s12887-016-0671-1
29. Enomoto M, Sezaki H, Muranishi R, Sato Y, Kikuchi S, Katayama Y, et al. Acquired palatal groove and delayed oral feeding in preterm infants. Pediatrics International. (2017) 59:171–5. doi: 10.1111/ped.13113
30. Ego A, Prunet C, Blondel B, Kaminski M, Goffinet F, Zeitlin J. [Customized and non-customized French intrauterine growth curves. II - Comparison with existing curves and benefits of customization]. J Gynecol Obstet Biol Reprod. (2016) 45:165–76. doi: 10.1016/j.jgyn.2015.08.008
31. Ancel P, Goffinet F, EPIPAGE-2 Writing Group. Survival and morbidity of preterm children born at 22 through 34 weeks' gestation in france in 2011: Results of the epipage-2 cohort study. JAMA Pediatr. (2015) 169:230–8. doi: 10.1001/jamapediatrics.2014.3351
32. Surveillance of Cerebral Palsy in Europe. Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. surveillance of cerebral palsy in Europe (SCPE). Dev Med Child Neurol. (2000) 42:816–824. doi: 10.1017/S0012162200001511
33. Halekoh U, Højsgaard S, Yan J. The R package geepack for generalized estimating equations. J Stat Softw. (2006) 15:1–11. doi: 10.18637/jss.v015.i02
34. White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. (2011) 30:377–99. doi: 10.1002/sim.4067
35. Buuren S van, Groothuis-Oudshoorn K. mice : Multivariate Imputation by Chained Equations in R. J Stat Softw. (2011) 45. doi: 10.18637/jss.v045.i03
36. Grund S, Robitzsch A, Luedtke O, Grund MS. Package ‘mitml'. 2019. (2019). Available online at: https://www.R-project.org/ (accessed March 19, 2021)
37. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York: John Wiley & 568 Sons (2004). p. 326
38. Nargozian C. The airway in patients with craniofacial abnormalities. Pediatr Anesth. (2004) 14:53–9. doi: 10.1046/j.1460-9592.2003.01200.x
39. Tsukamoto M, Hitosugi T, Yamanaka H, Yokoyama T. Bifid epiglottis, high-arched palate, and mental disorder in a patient with Pallister–Hall syndrome. Indian J Anaesth. (2018) 62:825–7. doi: 10.4103/ija.IJA_317_18
40. Hohoff A, Rabe H, Ehmer U, Harms E. Palatal development of preterm and low birthweight infants compared to term infants - what do we know? Part 3: discussion and conclusion. Head Face Med. (2005) 1:10. doi: 10.1186/1746-160X-1-10
41. Scavone-Junior H, Ferreira RI, Mendes TE, Ferreira FV. Prevalence of posterior crossbite among pacifier users: a study in the deciduous dentition. Braz Oral Res. (2007) 21:153–8. doi: 10.1590/S1806-83242007000200010
43. Adair SM, Milano M, Lorenzo I, Russell C. Effects of current and former pacifier use on the dentition of 24- to 59-month-old children. Pediatr Dent. (1995) 17:437–44.
44. Modéer T, Odenrick L, Lindner A. Sucking habits and their relation to posterior cross-bite in 4-year-old children. Scand J Dent Res. (1982) 90:323–8. doi: 10.1111/j.1600-0722.1982.tb00744.x
45. Larsson E. Sucking, chewing, and feeding habits and the development of crossbite: a longitudinal study of girls from birth to 3 years of age. Angle Orthod. (2001) 71:116–9. doi: 10.1043/0003-3219(2001)071<0116:SCAFHA>2.0.CO;2
46. Larsson E. The effect of dummy-sucking on the occlusion: a review. Eur J Orthod. (1986) 8:127–30. doi: 10.1093/ejo/8.2.127
47. Øgaard B, Larsson E, Lindsten R. The effect of sucking habits, cohort, sex, intercanine arch widths, and breast or bottle feeding on posterior crossbite in Norwegian and Swedish 3-year-old children. Am J Orthod Dentofacial Orthop. (1994) 106:161–6. doi: 10.1016/S0889-5406(94)70034-6
48. Warren JJ, Levy SM, Nowak AJ, Tang S. Non-nutritive sucking behaviors in preschool children: a longitudinal study. Pediatr Dent. (2000) 22:187–91.
49. da Rosa DP, Bonow MLM, Goettems ML, Demarco FF, Santos IS, Matijasevich A, et al. The influence of breastfeeding and pacifier use on the association between preterm birth and primary-dentition malocclusion: A population-based birth cohort study. Am J Orthod Dentofacial Orthop. (2020) 157:754–63. doi: 10.1016/j.ajodo.2019.06.014
50. Shandley S, Capilouto G, Tamilia E, Riley DM, Johnson YR, Papadelis C. Abnormal nutritive sucking as an indicator of neonatal brain injury. Front Pediatr. (2021) 8:875. doi: 10.3389/fped.2020.599633
51. Parkes J, Hill N, Platt MJ, Donnelly C. Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Dev Med Child Neurol. (2010) 52:1113–9. doi: 10.1111/j.1469-8749.2010.03765.x
52. Lippold C, Stamm T, Meyer U, Végh A, Moiseenko T, Danesh G. Early treatment of posterior crossbite - a randomised clinical trial. Trials. (2013) 14:20. doi: 10.1186/1745-6215-14-20
53. Brizuela M, Palla A, N DK. Posterior Crossbite. (2021). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK499873/ (accessed January 24, 2021)
54. Fleming PS. Timing orthodontic treatment: early or late? Aust Dent J. (2017) 62:11–9. doi: 10.1111/adj.12474
55. Anandarajah S, Dudhia R, Sandham A, Sonnesen L. Risk factors for small pharyngeal airway dimensions in preorthodontic children: a three-dimensional study. Angle Orthod. (2017) 87:138–46. doi: 10.2319/012616-71.1
56. Vázquez-Casas I, Sans-Capdevila O, Moncunill-Mira J, Rivera-Baró A. Prevalence of sleep-related breathing disorders in children with malocclusion. J Clin Exp Dent. (2020) 12:e555–60. doi: 10.4317/jced.56855
57. Fagundes NCF, Flores-Mir C. Pediatric obstructive sleep apnea-dental professionals can play a crucial role. Pediatr Pulmonol. (2021). doi: 10.1002/ppul.25291
Keywords: cohort study, very preterm, high-arched palate, posterior crossbite, non-nutritive sucking habits, cerebral palsy
Citation: Herrera S, Pierrat V, Kaminski M, Benhammou V, Marchand-Martin L, Morgan AS, Le Norcy E, Ancel P-Y and Germa A (2022) Risk Factors for High-Arched Palate and Posterior Crossbite at the Age of 5 in Children Born Very Preterm: EPIPAGE-2 Cohort Study. Front. Pediatr. 10:784911. doi: 10.3389/fped.2022.784911
Received: 28 September 2021; Accepted: 16 March 2022;
Published: 15 April 2022.
Edited by:
Zachi Grossman, Adelson School of Medicine, Ariel University, IsraelReviewed by:
Roman Khonsari, Assistance Publique Hopitaux De Paris, FranceCopyright © 2022 Herrera, Pierrat, Kaminski, Benhammou, Marchand-Martin, Morgan, Le Norcy, Ancel and Germa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Herrera, c2FuZHJhLmhlcnJlcmFAaW5zZXJtLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.