 Rosanna Fulchiero
Rosanna Fulchiero Sandra Amaral
Sandra Amaral
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr., 07 December 2022
Sec. Pediatric Nephrology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1087864
This article is part of the Research TopicInfections and Post-Transplant Lymphoproliferative Disease after Pediatric Kidney TransplantationView all 8 articles
Post-transplant lymphoproliferative disease (PTLD) is the most common malignancy complicating solid organ transplantation (SOT) in adults and children. PTLD encompasses a spectrum of histopathologic features and organ involvement, ranging from benign lymphoproliferation and infectious-mononucleosis like presentation to invasive neoplastic processes such as classical Hodgkin lymphoma. The predominant risk factors for PTLD are Epstein-Barr virus (EBV) serostatus at the time of transplant and the intensity of immunosuppression following transplantation; with EBV-negative recipients of EBV-positive donor organs at the highest risk. In children, PTLD commonly presents in the first two years after transplant, with 80% of cases in the first year, and over 90% of cases associated with EBV-positive B-cell proliferation. Though pediatric kidney transplant recipients are at lower risk (1–3%) for PTLD compared to their other SOT counterparts, there is still a significant risk of morbidity, allograft failure, and an estimated 5-year mortality rate of up to 50%. In spite of this, there is no consensus for monitoring of at-risk patients or optimal management strategies for pediatric patients with PTLD. Here we review pathogenesis and risk factors for the development of PTLD, with current practices for prevention, diagnosis, and management of PTLD in pediatric kidney transplant recipients. We also highlight emerging concepts, current research gaps and potential future developments to improve clinical outcomes and longevity in these patients.
Post-transplant lymphoproliferative disease (PTLD) is the most common malignancy complicating solid organ transplantation (SOT) in adults and children (1). Incidence is variable across allograft type, with a relatively low incidence of 1%–3% in pediatric kidney transplant recipients compared with other SOT patients: intestinal and multi-organ (5%–20%), heart and lung (2%–10%) and liver (1%–5%) (2–5). Generally, PTLD in SOT patients has a bimodal presentation, with “early” PTLD developing within the first two years of transplant, and “late” PTLD developing 5–10 years after transplant (6, 7). The majority of PTLD is “early” and related to Epstein-Barr virus (EBV) infection; with over 80% of pediatric cases presenting in the first year after transplant (8, 9) during the most intensive period of T-cell immunosuppression.
While reduction of immunosuppression is a cornerstone of therapy, patients often require additional treatments, including rituximab, chemotherapy, and adoptive immunotherapy, with radiation and surgical therapy reserved for select cases. Current literature in pediatric PTLD is limited to case series and small studies and many practice patterns for treatment are adopted from the adult literature, as outlined in this review. Importantly, PTLD is associated with significant morbidity and mortality, and at present, there is no consensus for monitoring of at-risk patients or optimal management strategies for pediatric patients with PTLD. Early recognition of risk factors with close attention to prevention efforts and prompt intervention is paramount for improving survival.
Here we review pathogenesis and risk factors for the development of PTLD, with current practices for prevention, diagnosis, and management of PTLD in pediatric kidney transplant recipients. We also highlight emerging concepts, current research gaps and potential future developments to improve clinical outcomes and longevity in these patients.
Though there are several reported risk factors for the development of PTLD, the two major risk factors in pediatric kidney transplant recipients are: EBV-serostatus at the time of transplant and the intensity of T-cell immunosuppression following transplantation (10).
Over 90% of pediatric PTLD is due to EBV positive B-cell proliferation in the setting of immunosuppression and decreased T-cell immune surveillance. Typically, acute EBV infection results in a polyclonal expansion of B-cells containing the virus. In healthy, immunocompetent hosts, EBV infected B-cells are rapidly eliminated by EBV-specific cytotoxic T-cells. However, in the setting of high-dose T-cell immunosuppression (such as thymoglobulin), cytotoxic T-cell function is diminished, resulting in uncontrolled proliferation of EBV-infected B-cells and the development of PTLD (11, 12).
Patients who are at highest risk for PTLD are EBV-negative recipients of EBV-positive donor organs (13, 14). EBV infection is more common in adults than children, with approximately 90%–95% of adults showing serologic evidence of infection and acquired immunity at the time of transplantation. Conversely, children are more likely to be EBV-negative, and may acquire EBV from the donor organ and/or primary EBV infection post-transplant, putting them at increased risk for PTLD. This was highlighted in one study of 276 pediatric kidney transplant recipients in which EBV-negative recipients of EBV-positive donor organs demonstrated a 6-fold higher risk of PTLD (15). The highest incidence of PTLD occurs at primary EBV seroconversion due to de novo infection or when it is acquired from passenger lymphocytes in the graft (16). Both primary EBV infections in EBV-negative patients and reactivation in EBV-positive individuals with latent infection can lead to uninhibited growth of EBV-infected B-cells and the development of PTLD (17).
While there is a strong association between EBV and PTLD, not all patients with high EBV viral load will go on to develop PTLD. Furthermore, an estimated 20%–30% of PTLD cases are not associated with EBV (17, 18). The pathogenesis of EBV-negative PTLD is not well understood, but these cases typically present later, 7–10 years after transplantation, compared with the earlier presentation of EBV-positive PTLD (7, 19, 20). These inconsistencies complicate post-transplant monitoring protocols and pose challenges in managing patients with EBV-viremia. Regardless, prior studies in pediatric kidney transplant recipients have demonstrated up to 35% mortality from PTLD (21–23), highlighting the importance of monitoring, prompt diagnosis and intervention, as well as prevention.
As previously discussed, the predominant risk factors for development of PTLD are the degree of T-cell immunosuppression and development of EBV infection. Thus, prevention of PTLD is centered around minimizing risk by limiting immunosuppressive exposure and optimizing opportunities for early intervention with screening for EBV viremia.
The role of immunosuppression after transplant is to prevent acute rejection and loss of the allograft while balancing the risk of treatment-related toxicities and complications such as infection and malignancy. High-level induction immunosuppression is required in the immediate post-transplant period to dampen the immune response to the allograft and prevent early rejection. Over time, as the risk of acute rejection decreases, chronic immunosuppression is lessened accordingly in an effort to promote long-term graft survival and reduce long-term toxicities. Conventional maintenance regimens generally consist of a combination of three immunosuppressive agents with different mechanisms of action based on widely adopted clinical practice guidelines (24). Though these regimens differ by patient, transplant center and geographic region, most pediatric patients will receive a calcineurin inhibitor (tacrolimus or cyclosporine), an antimetabolite (mycophenolate mofetil, azathioprine) and varying degrees of prednisone based on immunological risk of rejection and center-specific protocols.
It is not clear whether any particular immunosuppressive regimen is more protective for PTLD than another. Some studies have suggested protective effects of mTOR inhibitors due to their anti-proliferative effects, but other studies suggest potential increased risk of PTLD with mTOR introduction (25–28). Historically, increased risk of PTLD has been observed in patients with higher target tacrolimus trough concentrations (10, 14, 29, 30). In general, current practice patterns have focused on minimization of overall immunosuppression which is favorable for reducing the risk of PTLD.
Steroid reduction or withdrawal is another key area of interest (31). Though several small randomized controlled trials have evaluated steroid avoidance or withdrawal protocols in pediatric kidney transplant patients, most have had insufficient sample sizes with conflicting results. A recent meta-analysis shows justification for steroid avoidance/withdrawal in select pediatric kidney transplant recipients because of benefits in post-transplant growth with minimal effects on risk of acute rejection, and graft function (32). Though it was not a primary focus of the analysis, there was no difference in PTLD cases between groups. This suggests a potential future benefit to reduction of corticosteroids in select patient populations at increased risk for PTLD, though more research in larger patient populations is needed.
Monitoring of the EBV viral load is essential for early detection of current or impending PTLD in pediatric kidney transplant patients, and higher viral loads are associated with increased predilection for disease (33–38). In line with current society guidelines, many centers monitor high risk kidney transplant recipients (donor positive/recipient negative) for EBV viremia at varying intervals following transplant, starting once in the first week after transplant, then monthly for the first 3–6 months, and every 3 months until the end of the first year; with additional testing as necessary, particularly after anti-rejection therapy (24). Studies have shown that frequent monitoring of EBV per the aforementioned protocol, with more frequent testing (every 2 weeks) once EBV is >1,000 genome equivalents/mL, may lower the incidence of PTLD, especially in EBV seronegative patients (39, 40). Frequent monitoring allows for an earlier opportunity for intervention and preemptive treatment with increased likelihood for favorable outcomes.
Data regarding the use of antiviral prophylaxis for the prevention of PTLD is limited with conflicting results. In 2005, a retrospective multicenter case-control study of pediatric and adult kidney transplant recipients demonstrated a decreased risk of PTLD by 38% for every 30 days of treatment with ganciclovir in the first 12 months after transplant (41). This effect was not sustained in a larger, more recent systematic review which showed no significant difference in the rate of EBV-associated PTLD in high-risk, EBV naïve SOT recipients who received prophylaxis compared with those who didn't, regardless of age or type of organ transplant (42). Irrespective of these results, most kidney transplant recipients are exposed to antiviral prophylaxis against cytomegalovirus for at least the first three months after transplant, and it is possible this antiviral exposure is playing an unrecognized role in the prevention of early-onset PTLD.
Research on EBV vaccine development has been longstanding, however progress has been hampered by the complex nature of the EBV replication cycle and vast range of host cells. In May 2022, the National Institutes of Health in the United States announced a phase I clinical trial to evaluate the safety and immunogenicity of an investigational EBV gp350-Ferritin nanoparticle vaccine with a saponin-based Matrix-M adjuvant in healthy adults (43, 44). Results will be eagerly anticipated and have potential to significantly reduce the incidence of PTLD for transplant recipients.
The diagnosis of PTLD involves a multifaceted approach with histologic confirmation in the context of high clinical suspicion.
Clinically, signs and symptoms of PTLD are highly variable, ranging from asymptomatic to life threatening disease, and depend in part on the specific category of PTLD and the organ(s) involved. Patients will typically have non-specific constitutional symptoms such as fever, fatigue and weight loss (7, 45). Frequently, PTLD presents with extra-nodal masses in various organ systems: abdominal involvement in 60%–70%; thorax involvement in 45%–65%, head and neck in 20%–30% and central nervous system disease in up to 20%–25% (46, 47). Additionally, 20%–25% may have infiltrative lesions in the allograft and present with allograft dysfunction. Thus, additional symptoms may reflect primary or secondary organ dysfunction from mass compression of surrounding structures.
Patients may also present with laboratory abnormalities similar to non-transplant patients with lymphoproliferative disorders, such as: anemia, thrombocytopenia, leukopenia, elevated serum lactate dehydrogenase, hypercalcemia or hyperuricemia (48). There may also be radiologic evidence of a mass or positive positron emission tomography (PET) scanning indicating possible metabolically active areas, which also favors the diagnosis.
Although an elevated EBV viral load should raise suspicion for EBV-positive PTLD, this is not sufficient for diagnosis. In patients with a high clinical suspicion for PTLD (based on symptoms, EBV viremia, or both), diagnosis and classification require tissue biopsy, with excisional biopsy of a suspicious lesion when possible (49). And, while the absence of EBV in the peripheral blood makes PTLD less likely, it does not completely exclude the diagnosis (50).
The most recent World Health Organization guidelines divide PTLD into four main categories based on morphologic, immunophenotypic, genetic and clinical features (51). Identifying the category in which a patient belongs is paramount for guiding management as outlined in Table 1. Here we review a brief description of the four histopathologic categories.
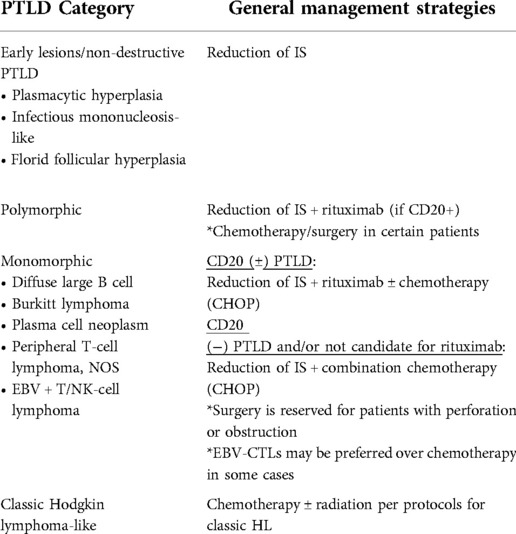
Table 1. Overview of management strategies based on classification of PTLD.
The first category of PTLD is non-destructive and encompasses three patterns: plasmacytic hyperplasia, infectious mononucleosis-like and florid follicular hyperplasia. These are considered early lesions with benign proliferations.
The remaining three categories are considered neoplastic processes and the presence of a lymphoid tumor in combination with two of the three following features confirm a diagnosis of PTLD: disruption of underlying tissue architecture by a lymphoid proliferation, presence of mono- or oligoclonal lymphoid cell populations, and EBV infection of many cells.
Monomorphic PTLD meets the criteria for a non-Hodgkin B cell or T/NK cell lymphoma with monoclonal malignant cells. The majority are B cell lymphomas (most commonly diffuse large B cell lymphoma) but can include Burkitt lymphoma, plasma cell neoplasm, peripheral T-cell lymphoma not otherwise specified or EBV + T/NK cell lymphoma.
Polymorphic PTLD has a pleomorphic lymphoid infiltrate that does not fill criteria for one of the aforementioned B cell or T/NK cell lymphomas above.
Classical Hodgkin lymphoma-like PTLD fulfills the criteria required for the diagnosis of classic HL and is the least common form of PTLD.
The overarching goals for PTLD management are eradication of the PTLD and preservation of allograft function. These priorities often involve conflicting treatment approaches, and typically one goal will take precedence over the other based on the specific needs of the patient. For example, a mainstay of PTLD eradication involves reduction of immunosuppression, but this increases the risk of graft rejection and failure.
The main approaches to PTLD management largely depend on the PTLD subtype but nuances may vary from institution to institution. Here we review the most common PTLD treatment strategies, their respective indications, and the risks and benefits to each approach.
Reduction of immunosuppression (RIS) is the cornerstone of management for all types of PTLD, with the goal of restoring EBV-specific cellular immunity without increasing the risk of acute rejection. This remains the most common practice at diagnosis of PTLD in pediatric SOT recipients (16, 24). Generally, immunosuppression is reduced to the lowest tolerable level, and at times can reach as low as 25%–50% of baseline therapy. Although there are no specific protocols for a graded decrease in IS, many centers reduce calcineurin inhibitors by 50% given prior published literature regarding the interplay between high serum tacrolimus troughs, EBV-viremia and development of PTLD (14, 29, 30). Antimetabolite therapy is often decreased in parallel or after initial reduction in CNI, with variable reduction or withdrawal of corticosteroids per center preference (7). As mentioned earlier, there is no specific immunosuppressive agent that is shown to be more or less PTLD-inducing, rather the overall degree of immunosuppression is the major risk factor.
Retrospective studies regarding the efficacy of RIS in adults and children are challenging to interpret due to study design and small sample sizes with conflicting results. Some studies suggest resolution of early PTLD lesions with RIS alone, but other studies suggest that many patients treated initially with RIS go on to require additional therapy, and up to 50% may have evidence of organ rejection during their reduced immunosuppression phase (52). Prospective study data in children is scarce, but adult solid organ transplant studies demonstrate a complete response rate of 37% from RIS alone; though this was balanced against a 32% rate of acute rejection in the same study population (53). RIS alone may be insufficient for treatment of PTLD, but early RIS in the setting of increasing EBV-viral load may prevent progression to PTLD and thus it remains first-line management in patients at risk for- and with confirmed PTLD (23, 40, 45).
Rituximab is an anti-CD20 monoclonal antibody and a reasonable therapeutic option for patients with CD20+ PTLD with residual disease despite RIS or for those who are not candidates for RIS.
Rituximab can be used alone or in conjunction with chemotherapy depending on the clinical circumstance. There are no current consensus guidelines for whom would benefit from both therapies and whether to administer them concurrently or sequentially. Patients with minimal symptoms and/or those who are not candidates for initial chemotherapy can begin with rituximab alone at a typical dosing regimen of 375 mg/m2 weekly for 3–4 doses. Adult SOT studies demonstrate response rates of 44%–79% with rituximab monotherapy and complete remission rates in 20%–55%, obviating the need for chemotherapy in many patients (7). There is a paucity of data for outcomes of rituximab monotherapy in pediatric patients with PTLD. One small study suggested complete remission rates of 70%–75% in pediatric SOT patients (54), and one study limited to pediatric kidney recipients demonstrated stable graft function and favorable graft survival with rituximab alone or in combination with chemotherapy (55); but more research with larger, prospective studies is necessary. Of note, rituximab imposes a risk of infusion reactions (fevers, rigors, hypotension), hepatitis B reactivation in patients with positive hepatitis B surface antigen or hepatitis B core antigen antibodies, and isolated neutropenia.
Patients with CD20 + PTLD may receive chemotherapy in conjunction with rituximab in a regimen known as R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone). The ideal time course of these therapies remains unknown; however, many authors suggest the addition of chemotherapy in patients who don't achieve an adequate response or complete remission after initial treatment with rituximab (56–58). These studies demonstrate improved response and remission rates when CHOP therapy was added to rituximab, with increased complete remission rates to 50%–65%. One phase II trial in pediatric patients with EBV + CD20+ PTLD showed a complete remission rate of 69% when receiving rituximab in combination with low-dose cyclophosphamide and prednisone, with 2-year event free survival (alive with functioning allograft and no PTLD) of 83% (59).
Patients with CD20- PTLD or those who are not candidates for rituximab may receive CHOP chemotherapy alone; and patients with classic Hodgkin lymphoma (HL) like PTLD will receive chemotherapy in accordance with HL protocols. There are no randomized trials comparing chemotherapy regimens in PTLD and some patients may require other regimens at the discretion of their physician or based on their personal risk of side effects. Indication for and selection of additional agents is beyond the scope of this review.
Local therapy by surgery or radiation is limited to rare situations, such as treatment of local disease, symptomatic control, or palliative care. For disseminated or central nervous system disease, radiation therapy may be indicated in conjunction with chemotherapy (60, 61).
Adoptive cell therapy with EBV-cytotoxic T-lymphocytes (EBV-CTLs) involves transferring naturally occurring EBV-specific CTLs that can kill EBV-transformed B cells into recipients with EBV + PTLD (62). Up to this point, the majority of published research regarding use of EBV-CTLs has been in hematopoietic stem cell transplant patients (HSCT). Use of EBV-CTLs in solid organ transplant recipients is gaining popularity in the last decade, particularly in patients with treatment-refractory PTLD.
One systematic review of 36 adult patients demonstrated a 66% response rate, with rare adverse effects limited to mild, nonspecific symptoms (nausea, vomiting, fever, tachycardia) (63). Use of EBV-CTLs in pediatric SOT patients is limited, but published results mimic those of adult studies, with 80% remission rate and survival rates of 89% and 86% at 2 and 5 years respectively (64).
Previous limitations surrounding the time required to generate autologous EBV-CTLs (2–3 months) in critically ill patients at risk for rapid progression of disease have now been addressed with availability of third party, HLA compatible EBV-CTLs with favorable safety profile and outcomes (62, 65). While a clear benefit to adoptive cell therapy is the potential to establish viral specific T-cell memory while avoiding immune-ablation and organ toxicity seen in chemotherapy (66), patients who receive EBV-CTLs may continue to require long-term immunosuppression to prevent allograft rejection, which poses an increased risk for invasive infections and additional malignancies. More research in larger populations is necessary to understand risks, benefits and long-term effects of EBV-CTLs in pediatric SOT patients (62).
Published data in all pediatric transplant recipients suggest a multitude of parameters associated with poor prognosis, including: advanced disease, multifocal and extra-nodal disease, CNS involvement, allograft involvement and high EBV load at the time of diagnosis. Morphologically, CD20-negative, EBV-negative, monomorphic subtype and late-onset PTLD are all associated with less favorable outcomes (67); as well as poor response to initial therapy (68). Pediatric kidney transplant recipients may have a more favorable outcome than their lung, liver, or HSCT counterparts; and overall, children diagnosed with PTLD have a better prognosis than adults (10, 68–70). Survival data in childhood PTLD is limited to small case series and studies across all allograft types and varied clinical and histological presentations; but in general, 5-year survival rates are estimated at 53%–80% (6, 59, 67, 68, 71–73). More long-term follow-up studies are necessary to determine late-onset morbidity and mortality associated with PTLD, including identifying parameters for safe re-transplantation (74, 75).
There are currently two major gaps in research of PTLD. First, not all EBV is the same. Many patients are chronic EBV carriers and never develop PTLD. A better understanding of the viral and host factors and immune responses that determine whether EBV-positive PLTD develops is critically needed (76). In addition, PTLD genotypes and phenotypes are vast, and once PTLD develops, there are no tailored protocols. Further research to improve characterization of the tumor microenvironment would help advance tailored therapeutic strategies to optimize outcomes and reduce adverse effects, ideally minimizing risk to the allograft (77).
Overall, PTLD is a rare but serious complication after kidney transplantation, and many questions remain unanswered given the wide spectrum of disease presentation with variable phenotypes, organ involvement and the complex interplay among factors that determine treatment and prognosis. Until vaccines are proven safe and effective and become readily available, attention must continue to be focused on prevention and management.
All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Penn I. Cancers complicating organ transplantation. N Engl J Med. (1990) 323(25):1767–9. doi: 10.1056/NEJM199012203232510
2. Petrara MR, Giunco S, Serraino D, Dolcetti R, De Rossi A. Post-transplant lymphoproliferative disorders: from epidemiology to pathogenesis-driven treatment. Cancer Lett. (2015) 369(1):37–44. doi: 10.1016/j.canlet.2015.08.007
3. Dharnidharka VR, Tejani AH, Ho P-L, Harmon WE. Post-transplant lymphoproliferative disorder in the United States: young Caucasian males are at highest risk. Am J Transplant. (2002) 2(10):993–8. doi: 10.1034/j.1600-6143.2002.21019.x
4. Opelz G, Döhler B. Lymphomas after solid organ transplantation: a collaborative transplant study report. Am J Transplant. (2004) 4(2):222–30. doi: 10.1046/j.1600-6143.2003.00325.x
5. Debray D, Baudouin V, Lacaille F, Charbit M, Rivet C, Harambat J, et al. De novo malignancy after solid organ transplantation in children. Transplant Proc. (2009) 41(2):674–5. doi: 10.1016/j.transproceed.2008.12.020
6. Schober T, Framke T, Kreipe H, Schulz TF, Großhennig A, Hussein K, et al. Characteristics of early and late PTLD development in pediatric solid organ transplant recipients. Transplantation. (2013) 95(1):240–6. doi: 10.1097/TP.0b013e318277e344
7. Abbas F, El Kossi M, Shaheen IS, Sharma A, Halawa A. Post-transplantation lymphoproliferative disorders: current concepts and future therapeutic approaches. World J Transplant. (2020) 10(2):29–46. doi: 10.5500/wjt.v10.i2.29
8. Dharnidharka VR, Sullivan EK, Stablein DM, Tejani AH, Harmon WE. Risk factors for posttransplant lymphoproliferative disorder (ptld) in pediatric kidney transplantation: a report of the north American pediatric renal transplant cooperative study (NAPRTCS)1. Transplantation. (2001) 71(8):1065–8. doi: 10.1097/00007890-200104270-00010
9. Kitchlu A, Dixon S, Dirk JS, Chanchlani R, Vasilevska-Ristovska J, Borges K, et al. Elevated risk of cancer after solid organ transplant in childhood: a population-based cohort study. Transplantation. (2019) 103(3):588–96. doi: 10.1097/TP.0000000000002378
10. Mynarek M, Schober T, Behrends U, Maecker-Kolhoff B. Posttransplant lymphoproliferative disease after pediatric solid organ transplantation. Clin Dev Immunol. (2013) 2013:1–14. doi: 10.1155/2013/814973
11. Lucas KG, Small TN, Heller G, Dupont B, O'Reilly RJ. The development of cellular immunity to epstein-barr virus after allogeneic bone marrow transplantation. Blood. (1996) 87(6):2594–603. doi: 10.1182/blood.V87.6.2594.bloodjournal8762594
12. Al-Mansour Z, Nelson BP, Evens AM. Post-transplant lymphoproliferative disease (PTLD): risk factors, diagnosis, and current treatment strategies. Curr Hematol Malig Rep. (2013) 8(3):173–83. doi: 10.1007/s11899-013-0162-5
13. Sampaio MS, Cho YW, Shah T, Bunnapradist S, Hutchinson IV. Impact of epstein-barr virus donor and recipient serostatus on the incidence of post-transplant lymphoproliferative disorder in kidney transplant recipients. Nephrol Dial Transplant. (2012) 27(7):2971–9. doi: 10.1093/ndt/gfr769
14. Ellis D, Jaffe R, Green M, Janosky JJ, Lombardozzi-Lane S, Shapiro R, et al. Epstein-Barr virus-related disorders in children undergoing renal transplantation with tacrolimus-based immunosuppression. Transplantation. (1999) 68(7):997–1003. doi: 10.1097/00007890-199910150-00017
15. McDonald RA, Smith JM, Ho M, Lindblad R, Ikle D, Grimm P, et al. Incidence of PTLD in pediatric renal transplant recipients receiving basiliximab, calcineurin inhibitor, sirolimus and steroids. Am J Transplant. (2008) 8(5):984–9. doi: 10.1111/j.1600-6143.2008.02167.x
16. Baker A, Frauca Remacha E, Torres Canizales J, Bravo-Gallego LY, Fitzpatrick E, Alonso Melgar A, et al. Current practices on diagnosis, prevention and treatment of post-transplant lymphoproliferative disorder in pediatric patients after solid organ transplantation: results of ERN transplantChild healthcare working group survey. Children. (2021) 8(8):661. doi: 10.3390/children8080661
17. Nijland ML, Kersten MJ, Pals ST, Bemelman FJ, Ten Berge IJ. Epstein-Barr virus-positive posttransplant lymphoproliferative disease after solid organ transplantation: pathogenesis, clinical manifestations, diagnosis, and management. Transplant Direct. (2016) 2(1):e48. doi: 10.1097/TXD.0000000000000557
18. Leblond V, Davi F, Charlotte F, Dorent R, Bitker MO, Sutton L, et al. Posttransplant lymphoproliferative disorders not associated with epstein-barr virus: a distinct entity? J Clin Oncol. (1998) 16(6):2052–9. doi: 10.1200/JCO.1998.16.6.2052
19. Destefano CB, Desai SH, Shenoy AG, Catlett JP. Management of post-transplant lymphoproliferative disorders. Br J Haematol. (2018) 182(3):330–43. doi: 10.1111/bjh.15263
20. Quinlan SC, Pfeiffer RM, Morton LM, Engels EA. Risk factors for early-onset and late-onset post-transplant lymphoproliferative disorder in kidney recipients in the United States. Am J Hematol. (2011) 86(2):206–9. doi: 10.1002/ajh.21911
21. Cleper R, Ben Shalom E, Landau D, Weissman I, Krause I, Konen O, et al. Post-transplantation lymphoproliferative disorder in pediatric kidney-transplant recipients - A national study. Pediatr Transplant. (2012) 16(6):619–26. doi: 10.1111/j.1399-3046.2012.01731.x
22. Longmore DK, Conwell LS, Burke JR, McDonald SP, McTaggart SJ. Post-transplant lymphoproliferative disorder: no relationship to recombinant human growth hormone use in Australian and New Zealand pediatric kidney transplant recipients. Pediatr Transplant. (2013) 17(8):731–6. doi: 10.1111/petr.12167
23. Haider MZ, Zamani Z, Taqi M, Mirza HM, Irfan A, Sami KN, et al. Post-Transplant lymphoproliferative disorder after renal transplant in the pediatric population: a systematic review. Blood. (2020) 136:35–6. doi: 10.1182/blood-2020-143333
24. KDIGO Clinical practice guideline for the care of kidney transplant recipients. Am J Transplant. (2009) 9(Suppl 3):S1–155. doi: 10.1111/j.1600-6143.2009.02834.x
25. Krams SM, Martinez OM. Epstein-Barr virus, rapamycin, and host immune responses. Curr Opin Organ Transplant. (2008) 13(6):563–8. doi: 10.1097/MOT.0b013e3283186ba9
26. Adamson AL, Le BT, Siedenburg BD. Inhibition of mTORC1 inhibits lytic replication of epstein-barr virus in a cell-type specific manner. Virol J. (2014) 11:110. doi: 10.1186/1743-422X-11-110
27. Kirk AD, Cherikh WS, Ring M, Burke G, Kaufman D, Knechtle SJ, et al. Dissociation of depletional induction and posttransplant lymphoproliferative disease in kidney recipients treated with alemtuzumab. Am J Transplant. (2007) 7(11):2619–25. doi: 10.1111/j.1600-6143.2007.01972.x
28. Hymes LC, Warshaw BL. Sirolimus in pediatric patients: results in the first 6 months post-renal transplant. Pediatr Transplant. (2005) 9(4):520–2. doi: 10.1111/j.1399-3046.2005.00324.x
29. Shapiro R, Scantlebury VP, Jordan ML, Vivas C, Tzakis AG, Ellis D, et al. FK506 In pediatric kidney transplantation—primary and rescue experience. Pediatr Nephrol. (1995) 9(S1):S43–S8. doi: 10.1007/BF00867683
30. Shapiro R, Scantlebury VP, Jordan ML, Vivas C, Ellis D, Lombardozzi-Lane S, et al. Pediatric renal transplantation under tacrolimus-based immunosuppression1. Transplantation. (1999) 67(2):299–303. doi: 10.1097/00007890-199901270-00020
31. Pape L. State-of-the-art immunosuppression protocols for pediatric renal transplant recipients. Pediatr Nephrol. (2019) 34(2):187–94. doi: 10.1007/s00467-017-3826-x
32. Zhang H, Zheng Y, Liu L, Fu Q, Li J, Huang Q, et al. Steroid avoidance or withdrawal regimens in paediatric kidney transplantation: a meta-analysis of randomised controlled trials. PloS One. (2016) 11(3):e0146523. doi: 10.1371/journal.pone.0146523
33. Gulley ML, Tang W. Using epstein-barr viral load assays to diagnose, monitor, and prevent posttransplant lymphoproliferative disorder. Clin Microbiol Rev. (2010) 23(2):350–66. doi: 10.1128/CMR.00006-09
34. Stevens SJC, Verschuuren EAM, Pronk I, Van Der Bij W, Harmsen MC, The TH, et al. Frequent monitoring of epstein-barr virus DNA load in unfractionated whole blood is essential for early detection of posttransplant lymphoproliferative disease in high-risk patients. Blood. (2001) 97(5):1165–71. doi: 10.1182/blood.V97.5.1165
35. Green M, Bueno J, Rowe D, Mazariegos G, Qu L, Abu-Almagd K, et al. Predictive negative value of persistent low epstein-barr virus viral load after intestinal transplantation in children. Transplantation. (2000) 70(4):593–6. doi: 10.1097/00007890-200008270-00010
36. Le J, Durand CM, Agha I, Brennan DC. Epstein-Barr virus and renal transplantation. Transplant Rev (Orlando). (2017) 31(1):55–60. doi: 10.1016/j.trre.2016.12.001
37. Colombini E, Guzzo I, Morolli F, Longo G, Russo C, Lombardi A, et al. Viral load of EBV DNAemia is a predictor of EBV-related post-transplant lymphoproliferative disorders in pediatric renal transplant recipients. Pediatr Nephrol. (2017) 32(8):1433–42. doi: 10.1007/s00467-017-3627-2
38. Riddler SA, Breinig MC, McKnight JL. Increased levels of circulating epstein-barr virus (EBV)-infected lymphocytes and decreased EBV nuclear antigen antibody responses are associated with the development of posttransplant lymphoproliferative disease in solid-organ transplant recipients. Blood. (1994) 84(3):972–84. doi: 10.1182/blood.V84.3.972.972
39. McDiarmid SV, Jordan S, Kim GS, Toyoda M, Goss JA, Vargas JH, et al. Prevention and preemptive therapy of postransplant lymphoproliferative disease in pediatric liver recipients. Transplantation. (1998) 66(12):1604–11. doi: 10.1097/00007890-199812270-00006
40. Hyun H, Park E, Cho M, Min S-I, Ha J, Kang HJ, et al. Post-Transplant lymphoproliferative diseases in pediatric kidney allograft recipients with epstein-barr virus viremia. J Korean Med Sci. (2019) 34(30):203–15. doi: 10.3346/jkms.2019.34.e203
41. Funch DP, Walker AM, Schneider G, Ziyadeh NJ, Pescovitz MD. Ganciclovir and Acyclovir reduce the risk of post-transplant lymphoproliferative disorder in renal transplant recipients. Am J Transplant. (2005) 5(12):2894–900. doi: 10.1111/j.1600-6143.2005.01115.x
42. Aldabbagh MA, Gitman MR, Kumar D, Humar A, Rotstein C, Husain S. The role of antiviral prophylaxis for the prevention of epstein-barr virus-associated posttransplant lymphoproliferative disease in solid organ transplant recipients: a systematic review. Am J Transplant. (2017) 17(3):770–81. doi: 10.1111/ajt.14020
43. Rozman M, Korać P, Jambrosic K, Židovec Lepej S. Progress in prophylactic and therapeutic EBV vaccine development based on molecular characteristics of EBV target antigens. Pathogens. (2022) 11(8):864–75. doi: 10.3390/pathogens11080864
44. Safety and Immunogenicity of an Epstein-Barr Virus (EBV) gp350-Ferritin Nanoparticle Vaccine in Healthy Adults With or Without EBV Infection. https://ClinicalTrials.gov/show/NCT04645147
45. Green M, Michaels MG. Epstein-Barr virus infection and posttransplant lymphoproliferative disorder. Am J Transplant. (2013) 13(Suppl 3):41–54. quiz. doi: 10.1111/ajt.12004
46. Pickhardt PJ, Siegel MJ, Hayashi RJ, Kelly M. Posttransplantation lymphoproliferative disorder in children: clinical, histopathologic, and imaging features. Radiology. (2000) 217(1):16–25. doi: 10.1148/radiology.217.1.r00oc3816
47. Penn I, Porat G. Central nervous system lymphomas in organ allograft recipients. Transplantation. (1995) 59(2):240–4. doi: 10.1097/00007890-199501000-00016
48. Preiksaitis JK, Keay S. Diagnosis and management of posttransplant lymphoproliferative disorder in solid-organ transplant recipients. Clin Infect Dis. (2001) 33(s1):S38–46. doi: 10.1086/320903
49. Paya CV, Fung JJ, Nalesnik MA, Kieff E, Green M, Gores G, et al. Epstein-Barr virus-induced posttransplant lymphoproliferative disorders. ASTS/ASTP EBV-PTLD task force and the mayo clinic organized international consensus development meeting. Transplantation. (1999) 68(10):1517–25. doi: 10.1097/00007890-199911270-00015
50. Singavi AK, Harrington AM, Fenske TS. Post-transplant lymphoproliferative disorders. Cancer Treat Res. (2015) 165:305–27. doi: 10.1007/978-3-319-13150-4_13
51. Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the world health organization classification of lymphoid neoplasms. Blood. (2016) 127(20):2375–90. doi: 10.1182/blood-2016-01-643569
52. Ramos-Gonzalez G, Crum R, Allain A, Agur T, O’Melia L, Staffa S, et al. Presentation and outcomes of post-transplant lymphoproliferative disorder at a single institution pediatric transplant center. Pediatr Transplant. (2022) 26(5):e14268. doi: 10.1111/petr.14268
53. Reshef R, Vardhanabhuti S, Luskin MR, Heitjan DF, Hadjiliadis D, Goral S, et al. Reduction of immunosuppression as initial therapy for posttransplantation lymphoproliferative disorder★. Am J Transplant. (2011) 11(2):336–47. doi: 10.1111/j.1600-6143.2010.03387.x
54. Webber S, Harmon W, Faro A, Green M, Sarwal M, Hayashi R, et al. Anti-CD20 monoclonal antibody (rituximab) for refractory PTLD after pediatric solid organ transplantation: multicenter experience from a registry and from a prospective clinical trial. Blood. (2004) 104(11):746. doi: 10.1182/blood.V104.11.746.746
55. Zierhut H, Kanzelmeyer N, Buescher A, Höcker B, Mauz-Körholz C, Tönshoff B, et al. Course of renal allograft function after diagnosis and treatment of post-transplant lymphoproliferative disorders in pediatric kidney transplant recipients. Pediatr Transplant. (2021) 25(6):e14042. doi: 10.1111/petr.14042
56. Trappe RU, Dierickx D, Zimmermann H, Morschhauser F, Mollee P, Zaucha JM, et al. Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful stratification into rituximab or R-CHOP consolidation in an international, prospective, multicenter phase II trial. J Clin Oncol. (2017) 35(5):536–43. doi: 10.1200/JCO.2016.69.3564
57. Trappe R, Riess H, Babel N, Hummel M, Lehmkuhl H, Jonas S, et al. Salvage chemotherapy for refractory and relapsed posttransplant lymphoproliferative disorders (PTLD) after treatment with single-agent rituximab. Transplantation. (2007) 83(7):912–8. doi: 10.1097/01.tp.0000258647.50947.78
58. Elstrom RL, Andreadis C, Aqui NA, Ahya VN, Bloom RD, Brozena SC, et al. Treatment of PTLD with rituximab or chemotherapy. Am J Transplant. (2006) 6(3):569–76. doi: 10.1111/j.1600-6143.2005.01211.x
59. Gross TG, Orjuela MA, Perkins SL, Park JR, Lynch JC, Cairo MS, et al. Low-Dose chemotherapy and rituximab for posttransplant lymphoproliferative disease (PTLD): a Children's Oncology group report. Am J Transplant. (2012) 12(11):3069–75. doi: 10.1111/j.1600-6143.2012.04206.x
60. Dierickx D, Habermann TM. Post-Transplantation lymphoproliferative disorders in adults. N Engl J Med. (2018) 378(6):549–62. doi: 10.1056/NEJMra1702693
61. Dierickx D, Vergote V. Management of post-transplant lymphoproliferative disorders. HemaSphere. (2019) 3:74–7. doi: 10.1097/HS9.0000000000000226
62. Shahid S, Prockop SE. Epstein-Barr virus-associated post-transplant lymphoproliferative disorders: beyond chemotherapy treatment. Cancer Drug Resistance. (2021) 4(3):646–64. doi: 10.20517/cdr.2021.34
63. Liu JY, Zhang JM, Zhan HS, Sun LY, Wei L. EBV-Specific cytotoxic T lymphocytes for refractory EBV-associated post-transplant lymphoproliferative disorder in solid organ transplant recipients: a systematic review. Transpl Int. (2021) 34(12):2483–93. doi: 10.1111/tri.14107
64. Chiou FK, Beath SV, Wilkie GM, Vickers MA, Morland B, Gupte GL. Cytotoxic T-lymphocyte therapy for post-transplant lymphoproliferative disorder after solid organ transplantation in children. Pediatr Transplant. (2018) 22(2):e13133. doi: 10.1111/petr.13133
65. Prockop S, Doubrovina E, Suser S, Heller G, Barker J, Dahi P, et al. Off-the-shelf EBV-specific T cell immunotherapy for rituximab-refractory EBV-associated lymphoma following transplantation. J Clin Invest. (2020) 130(2):733–47. doi: 10.1172/JCI121127
66. Sutrave G, Gottlieb DJ. Adoptive cell therapies for posttransplant infections. Curr Opin Oncol. (2019) 31(6):574–90. doi: 10.1097/CCO.0000000000000580
67. Füreder A, Kropshofer G, Benesch M, Dworzak M, Greil S, Huber WD, et al. Characteristics, management, and outcome of pediatric patients with post-transplant lymphoproliferative disease—a 20 years’ experience from Austria. Cancer Rep. (2021) 4(5):e1375. doi: 10.1002/cnr2.1375
68. Bosse RC, Franke AJ, Paul Skelton W, Woody LE, Bishnoi R, Wang Y, et al. Post transplant lymphoproliferative disorder risk factors in children: analysis of a 23-year single-institutional experience. Pediatr Transplant. (2020) 24(5):e13747. doi: 10.1111/petr.13747
69. Hussein K, Tiede C, Maecker-Kolhoff B, Kreipe H. Posttransplant lymphoproliferative disorder in pediatric patients. Pathobiology. (2013) 80(6):289–96. doi: 10.1159/000350331
70. Jain A, Nalesnik M, Reyes J, Pokharna R, Mazariegos G, Green M, et al. Posttransplant lymphoproliferative disorders in liver transplantation: a 20-year experience. Ann Surg. (2002) 236(4):429–36. doi: 10.1097/00000658-200210000-00005
71. Trappe R, Oertel S, Leblond V, Mollee P, Sender M, Reinke P, et al. Sequential treatment with rituximab followed by CHOP chemotherapy in adult B-cell post-transplant lymphoproliferative disorder (PTLD): the prospective international multicentre phase 2 PTLD-1 trial. Lancet Oncol. (2012) 13(2):196–206. doi: 10.1016/S1470-2045(11)70300-X
72. Caillard S, Porcher R, Provot F, Dantal J, Choquet S, Durrbach A, et al. Post-transplantation lymphoproliferative disorder after kidney transplantation: report of a nationwide French registry and the development of a new prognostic score. J Clin Oncol. (2013) 31(10):1302–9. doi: 10.1200/JCO.2012.43.2344
73. Maecker B, Jack T, Zimmermann M, Abdul-Khaliq H, Burdelski M, Fuchs A, et al. CNS Or bone marrow involvement as risk factors for poor survival in post-transplantation lymphoproliferative disorders in children after solid organ transplantation. J Clin Oncol. (2007) 25(31):4902–8. doi: 10.1200/JCO.2006.10.2392
74. Karras A, Thervet E, Meur YL, Baudet-Bonneville V, Kessler M, Legendre C. Successful renal retransplantation after post-transplant lymphoproliferative disease. Am J Transplant. (2004) 4(11):1904–9. doi: 10.1111/j.1600-6143.2004.00562.x
75. Rouphael B, Lankireddy S, Lazaryan A, Kukla A, Ibrahim HN, Matas AJ, et al. Outcomes of kidney retransplantation in recipients with prior post-transplant lymphoproliferative disorder. Clin Transplant. (2016) 30(1):60–5. doi: 10.1111/ctr.12659
76. Martinez OM. Biomarkers for PTLD diagnosis and therapies. Pediatr Nephrol. (2020) 35(7):1173–81. doi: 10.1007/s00467-019-04284-w
Keywords: pediatrics, kidney transplant, Epstein-Barr virus infection, post-transplant lymphoproliferative disease, malignancy
Citation: Fulchiero R and Amaral S (2022) Post-transplant lymphoproliferative disease after pediatric kidney transplant. Front. Pediatr. 10:1087864. doi: 10.3389/fped.2022.1087864
Received: 2 November 2022; Accepted: 22 November 2022;
Published: 7 December 2022.
Edited by:
Sarah Kizilbash, University of Minnesota Twin Cities, United StatesReviewed by:
Priya Sara Verghese, Ann & Robert H. Lurie Children's Hospital of Chicago, United States© 2022 Fulchiero and Amaral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosanna Fulchiero ZnVsY2hpZXJyMkBjaG9wLmVkdQ==
Specialty Section: This article was submitted to Pediatric Nephrology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.