
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 24 November 2022
Sec. Pediatric Infectious Diseases
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1022669
This article is part of the Research Topic Impact of SARS-CoV-2 and COVID-19 Pandemic in Pediatrics View all 25 articles
 Maire Brasseler1,2,3*
Maire Brasseler1,2,3* Anne Schönecker4
Anne Schönecker4 Mathis Steindor4
Mathis Steindor4 Adela Della Marina1,2
Adela Della Marina1,2 Nora Bruns1,2
Nora Bruns1,2 Burcin Dogan1,3
Burcin Dogan1,3 Ursula Felderhoff-Müser1,2
Ursula Felderhoff-Müser1,2 Johannes Hebebrand2,5
Johannes Hebebrand2,5 Christian Dohna-Schwake1,2,3
Christian Dohna-Schwake1,2,3 Sarah C. Goretzki1,2,3*
Sarah C. Goretzki1,2,3*
Background: Absent or abnormal senses of smell and taste have been frequently reported during both acute and long COVID in adult patients. In contrast, pediatric patients who test positive for SARS-CoV-2 are often asymptomatic and the loss of smell and/or taste has been infrequently reported. After observing several young patients with COVID-associated anosmia and ageusia at our clinic, we decided to investigate the incidence of subsequent eating disorders in these patients and in SARS-CoV-2 positive patients who did not experience anosmia and ageusia during the same period.
Material and methods: A single-site retrospective cohort study of 84 pediatric patients with suspected long COVID who were treated in the Pediatric Infectious Diseases Outpatient Clinic at the University Hospital Essen were evaluated for persistent symptoms of COVID-19. Smell and taste dysfunction as well as eating behaviors were among the signs and symptoms analyzed in this study.
Results: 24 out of 84 children and adolescents described smell and taste dysfunction after confirmed or suspected SARS-CoV-2 infections. A large number of these patients (6 out of 24) demonstrated increased fixation on their eating behavior post-COVID and over time these patients developed anorexia nervosa.
Discussion/Conclusion: In this study we saw a possible association of long-lasting post-COVID smell and taste dysfunction with subsequent development of eating disorders. This observation is worrisome and merits further investigation by healthcare providers at multiple clinical sites.
Since the first patient with SARS-CoV-2 pneumonia was identified in Wuhan China in December 2019, significant morbidity and mortality associated with both the acute and long-term effects of COVID in adults has been reported worldwide. However, in children and adolescents, the majority of SARS-CoV-2-PCR-positive patients remain asymptomatic. Only a few pediatric patients present with severe acute COVID-19 (1). Apart from the acute disease, different courses of illnesses associated with previous SARS-CoV-2 infection have been reported such as Pediatric-Inflammatory-Multisystem-Syndrome temporally associated with SARS-CoV-2 (PIMS) (2–5) or long COVID and “Post-COVID-Syndrome” (6, 7).
While the two latter diagnoses are clearly defined for adults (6, 7), no clear case definition for pediatric patients exists, although children and adolescents display similar symptoms such as fatigue, muscle pain, headaches, concentration difficulty, and/or olfactory and gustatory dysfunction (8, 9). In adults, symptoms of long COVID, especially persistent olfactory dysfunction, are associated with a lower quality of life and a negative impact on mental health (10, 11). The prevalence of childhood long COVID remains unclear, as very few studies exist and among them even fewer that include a control group (10).
Moreover, the COVID pandemic has caused an increase in mental stress in children, adolescents, and their families worldwide. A rise in depression and anxiety disorders has been reported, as reflected by increased admissions due to severe eating disorders and suicide attempts (5,12–15).
During the treatment course of children and adolescents with suspected long COVID, we observed a possible association between changes in smell and taste and restrictive eating behavior. Recently, other studies have also described significantly disturbed eating habits in children with changes in smell and taste due to Long COVID (16). Several reports have revealed an increased incidence of anorexia nervosa after the onset of COVID-19 and associated measures to control the epidemic (17, 18). Hence, we retrospectively investigated smell and taste dysfunction (SAT) in our cohort to determine whether such a dysfunction represented a symptom of long COVID and whether SAT led to the development of anorexia nervosa or another eating disorder-associated disease.
Our investigation consisted of a single-site, retrospective cohort study of patients treated in the Pediatric Infectious Diseases Outpatient Clinic at the Department of Pediatrics I, University Hospital Essen. Data were collected from existing patient records.
This study was approved by the Ethics Committee of the Medical Faculty of the University Duisburg-Essen (22-10581-BO) and conducted in accordance with the latest version of the Declaration of Helsinki. As the study presents a retrospective analysis with anonymous data, the ethics committee waived the need for informed consent.
Included were all patients (age 0–18 years, n = 84) treated in the Pediatric Infectious Diseases Outpatient Clinic at the Department of Pediatrics I, University Hospital Essen from April 2021 to April 2022 with a diagnosis of suspected long COVID. Twenty-four patients, who met the criteria of long COVID according to the German Association of the Scientific Medical Societies (AWMF) and NICE guidelines (6, 7) and reported changes in their olfactory and/or gustatory senses, were further evaluated. These patients were divided into two groups according to the presence (“LC+SAT+ED”-group) or absence (“LC+SAT”-group) of restrictive eating behavior and anorexia nervosa as defined by the International Classification of Disease ICD-11 (19). Patients without changes in their eating behavior and no diagnosed eating disorder comprised the “LC+SAT”-group (see Diagram 1).
In cases where the diagnosis of long COVID could not be confirmed (n = 25), SAT was not reported (n = 30), or the long COVID diagnosis was rejected due to insufficient data (n = 5), patients were excluded.
A detailed medical history, blood tests (see Supplementary material), physical examination, oxygen saturation, blood pressure, and a consultation with an Ear Nose and Throat (ENT) specialist were obtained from all patients. Body mass indices (BMI; kg/m²) were assessed using BMI-centiles adapted to age, sex, and race (20). All further consultations with other medical specialists were conducted based on clinical presentation. Electroencephalogram (EEG), electrocardiogram (ECG), electrocardiography (ECHO), ultrasound of the abdomen and thyroid, chest-x-rays, lung function with lung clearance index (LCI) measurement, cranial or spinal magnetic resonance imaging (MRI), and Nerve Conduction Velocity (NCV) were performed if necessary. We recommended a consultation with a child and adolescent psychiatrist for all patients with newly developed restrictive eating behavior to rule out or confirm the diagnosis of a possible eating disorder and initiate treatment. Demographic variables, preexisting diagnoses, and newly detected underlying diseases as well as other known long COVID-associated symptoms (fatigue, headaches, etc.) were documented. Patients were systematically queried as to symptoms associated with long COVID and restrictive eating behavior and psychological or other somatic symptoms were included in the evaluation. Amenorrhea was defined by three or more missing menstrual cycles; menstruation was defined as irregular if a time shift of more than 30% had occurred for three months after at least three months of regular menstrual cycles. The subjective change in recalled symptoms over time was monitored. An improvement was defined by less reported intensity, quantity of symptoms, and/or alleviation of restrictions in daily routines, and numbers of symptoms or less restrictions in daily routines caused by long COVID symptoms.
Statistical analysis was performed with SPSS 27 Statistic Software (IBM; Armonk, NY). Continuous variables were presented as median. The confidence interval (CI) was set at 95%. Mann-Whitney-U-test for continuous variables or Chi-Square test for categorical variables were used to test for differences between cases and control groups. The level of significance was set at p = 0.05. Percentiles for height, weight, and BMI were used according to ICD-11, 6B80 Anorexia Nervosa.
Twenty-four (28.6%) of the 84 patients evaluated in this study met both the criteria of long COVID according to the AWMF Guidelines (see Table 1) and had SAT. These symptoms were evaluated by systematic anamnesis and excluded anatomic reasons (Table 2 and Diagram 1 in Supplementary material). Six patients (3 male and 3 female) showed restrictive eating behavior and 5 of them met the ICD-11 guidelines for anorexia nervosa (25% of the children with SAT and 8.6% of the entire group with suspected long COVID) (see Diagram 1). None of the long COVID patients without SAT showed differences in their eating behavior or developed anorexia nervosa.
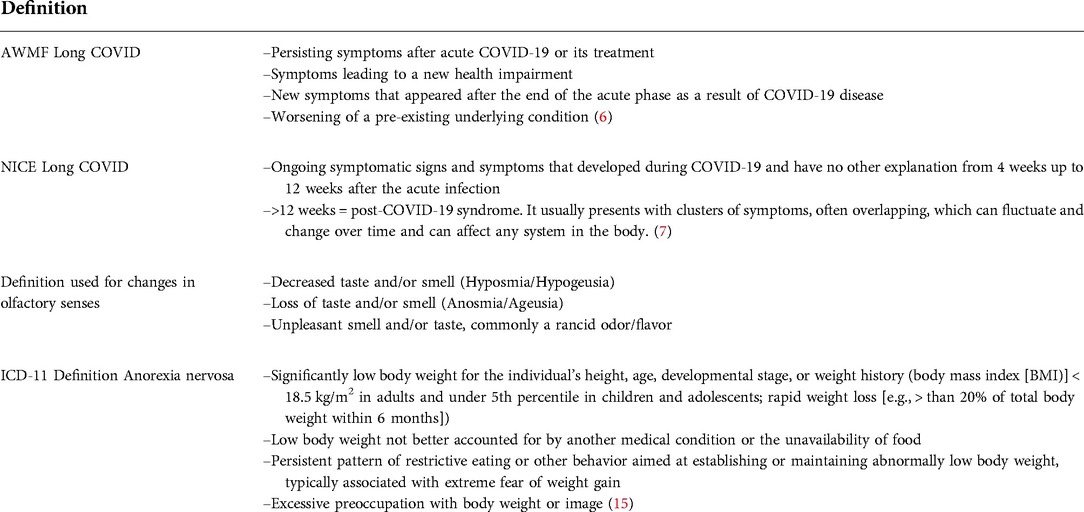
Table 1. Definitions.
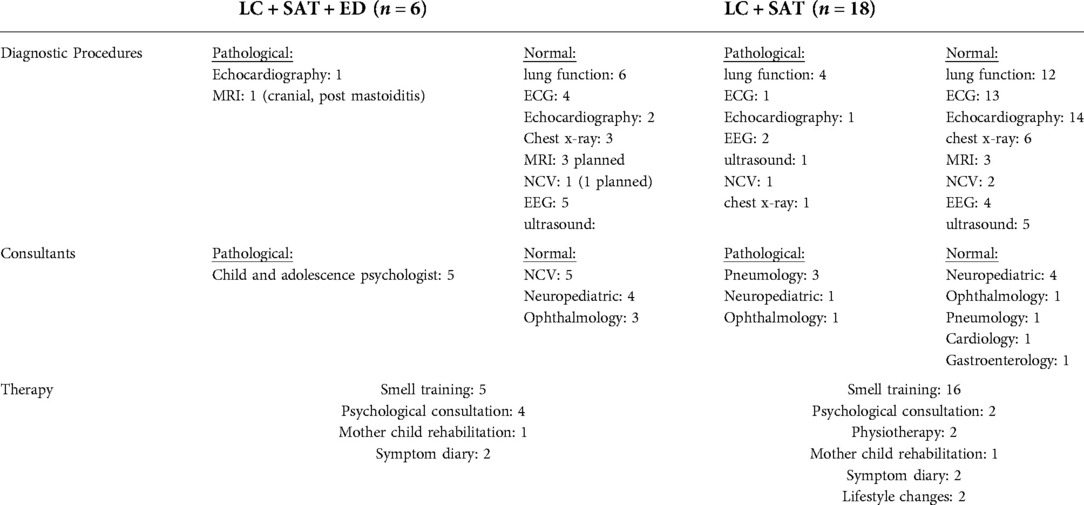
Table 2. Diagnostics and therapy.
The 24 patients were ages 6–17 years. SARS-CoV-2 infection had been confirmed by PCR tests in all patients. None of the 24 patients with SAT had been hospitalized due to COVID-19. None of them suffered from gastrointestinal symptoms during acute or long COVID. Long COVID symptoms without an association to eating disorders included: decreased general condition (87.5%), “brain fog”/concentration difficulty (37.5%), hyperesthesia (50.0%), and headaches (75.0%). There were no significant differences between concentrations of SARS-CoV-2 antibodies in the “LC + SAT + ED”-group and “LC + SAT”-group (median: 125.6 BAU/ml [binding antibody units/mL] vs. 450 BAU/ml; standard deviation 870.8). Additionally, there were no significant differences in SARS-CoV-2 viral variants between the two groups (see Table 3).
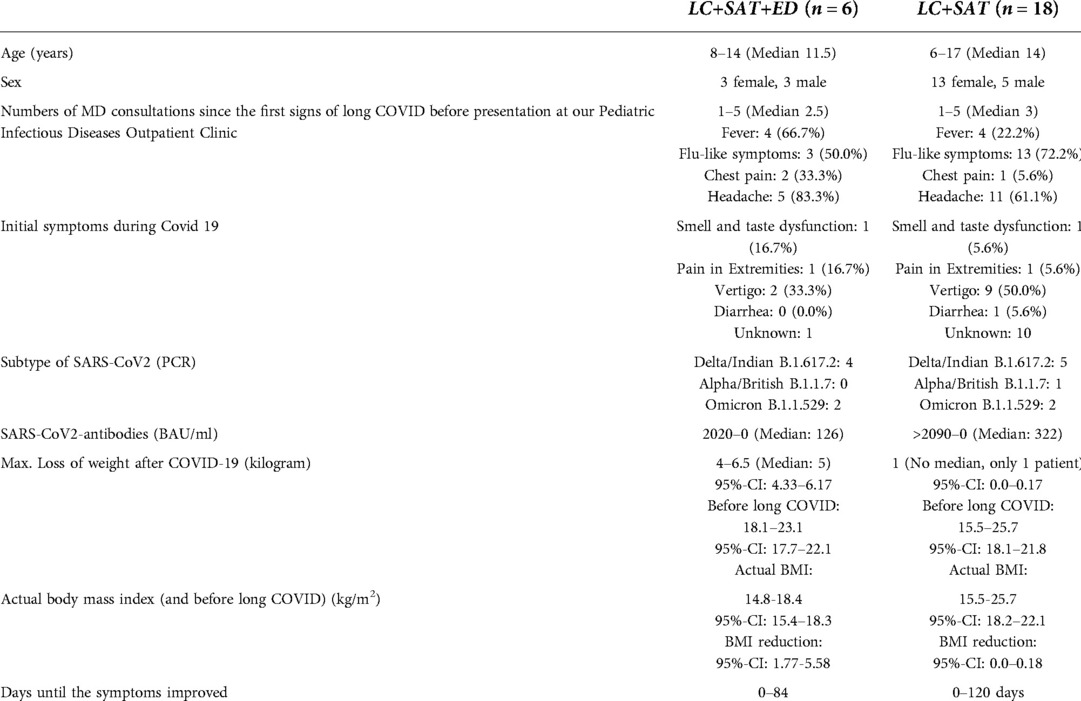
Table 3. Patient characteristics and COVID-19 associated symptoms.
Five of the 6 patients with restrictive eating behavior reported a reduced appetite. This symptom, as well as hair loss or changes in menstrual cycle were significantly more common in the “LC+SAT+ED”-group than in the “LC+SAT”-group (hair loss p = 0.001, menstrual cycle p = 0.042, Chi-quadrant). In addition, 5 patients reported symptoms of depression, stress, and no longer enjoying food. Noticeably all patients felt misunderstood by family, friends, and professionals. Depressive symptoms and anxiety were significantly more common in the “LC+SAT+ED”-group than in the “LC+SAT”-group (p = 0,005, Mann-Whitney-U-test, z = −2,835) (see Table 4); one of the “LC+SAT”-group patients had been diagnosed with depression and an eating disorder before COVID infection, which did not worsen during the course of disease.
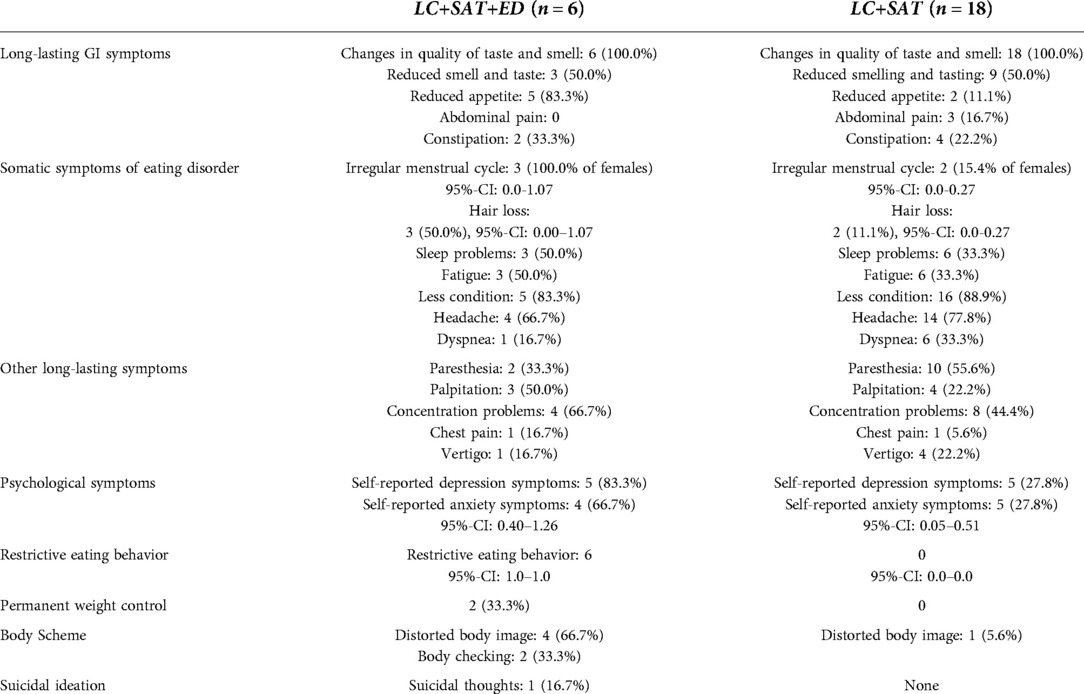
Table 4. Long COVID symptoms and eating behavior.
None of the “LC+SAT+ED”-group or “LC+SAT”-group patients followed a special diet (e.g., vegetarian, vegan, or gluten-free). The 6 patients of the “LC+SAT+ED”-group reported restrictive eating behavior and lost between 4 and 6.5 kilograms of body weight (see Tables 3, 5). The period from the beginning of long COVID symptoms to the maximum loss of weight was between 3 and 5 months. Four of the patients reported a distorted body image and two of them had to weigh themselves frequently. No compensatory mechanisms were reported. Associated symptoms like decreased general condition, amenorrhea, constipation, and malnutrition also existed (see Table 4). None of the “LC+SAT”-group patients lost weight (see Table 3). Weight loss and BMI reduction during long COVID were significantly higher in the the 6 patients of the “LC+SAT+ED”-group (p < 0.001, p = 0.009, chi-quadrant, Table 4) than in patients of the “LC+SAT”-group.
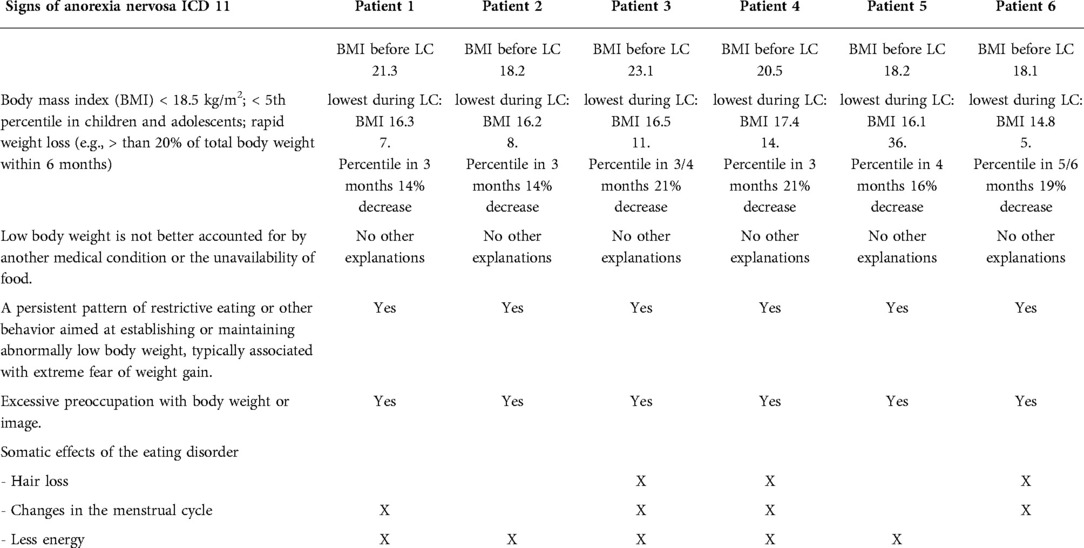
Table 5. Signs of eating disorder within the six described LC+SAT+ED
Treatment recommendations included training of the olfactory nerve (twice a day smelling of 4 different essential oils, each for a period of 10 s), keeping a diary of symptoms, weight check-ups by a pediatrician, consultations with a child and adolescent psychiatrist, and provision of emergency contacts to both patients and their families (Table 2). These recommendations were made with the intention of symptom management. In 5 of the 6 patients of the “LC+SAT+ED”-group, the diagnosis of anorexia nervosa was confirmed during further examinations by a child and adolescent psychiatrist or a psychologist. Three of the “LC+SAT+ED”-group patients reported fewer symptoms after 32 to 84 days. One of them reported decreased symptoms following SARS-CoV-2-vaccination (Pfizer/BioNTech). Three patients attributed their improvementto psychotherapy.
Here, we describe a group of 24 pediatric patients ages 6–17 years with long COVID or Post-COVID Syndrome and concurrent SAT. A clinically important proportion of patients developed a restrictive eating behavior and secondary eating disorder as defined by ICD-11. SAT is a widely recognized symptom of acute SARS-CoV-2 infection. In cases of COVID-19 persistence for more than 4 weeks, the diagnosis of long COVID was confirmed; when persistence continued beyond 12 weeks, Post-COVID Syndrome was confirmed. A relevant impact of long COVID on the mental health in affected adults has already been documented (10). However, to our knowledge, the association of SAT dysfunction and eating disorders in childhood has not been reported to date.
Even if the prevalence of long COVID in children remains unclear (10), some studies report its ubiquity in children with symptoms like persistent fatigue (25.2%), cognitive sequelae such as irritability (24.3%) and mood changes (23.3%), headaches (16.9%), rhinorrhea (16.1%), coughing (14.4%), and anosmia/dysgeusia (12.3%) (8, 9). Patients included in this study presented with these symptoms.
Within the study population all patients with a secondary eating disorder showed somatic symptoms (reduced fitness, constipation, malnutrition and amenorrhea) and were ages 8–14 years. Normally, the incidence of eating disorders is highest for girls ages 15–19 years and for boys ages 10–14 years (21). In all 6 patients in this study, the focus on food and restrictive eating occurred after quality changes in smell and taste. Increased attention to eating behavior like obsession with the daily meal plan is a risk factor for the development of eating disorders and may have promoted their development (22). In adults, persistent olfactory dysfunction has been associated with a lower quality of life and impaired mental health (10).
Female patients are usually more prone to develop an eating disorder than males. Only 5%–10% of patients who were reported with anorexia and bulimia nervosa during the COVID pandemic were male (23–26). Our results showed an equal distribution of both sexes who developed an eating disorder due to restrictive eating behavior. This implies that long COVID may affect male and female adolescents alike and override the usual gender differences in eating disorders, suggesting that SAT represents a clinically important individual risk factor for a new eating disorder.
Well documented research has proven that patients with eating disorders, especially with anorexia nervosa, are at risk of many somatic and psychiatric comorbidities and higher mortality (15, 27–30). Our study results show a positive correlation between restrictive eating behavior and symptoms of depression. These facts and the significant loss of weight in our patients emphasizes the importance of assessing both female and male pediatric patients for possible eating disorders after COVID-19. Physicians, caregivers, and patients should be able to recognize symptoms of an eating disorder, especially in all cases of SAT. Follow-up departments with multidisciplinary teams are needed for children and adolescents who experience signs of long COVID. In the case of SAT, screening methods like the SCOFF Questionnaire to detect eating disorders in children and adolescents at an early stage could be helpful (31).
There are several limitations to our study. As there is no acknowledged definition for long COVID in pediatric patients, we used the definition for adults which might not be suitable for pediatric patients in every sense. In addition, smell and taste dysfunctions are subjective symptoms. Only 5 patients were diagnosed by a mental health specialist prior to our study because of very limited resources due to higher demand for psychological and psychiatric services for children during the pandemic. Therefore, not all of our patients had the opportunity to get standard psychological evaluations during their visit in our outpatient clinic. Due to the different home addresses of patients included in this study and different geographic locations of their respective healthcare providers, the corresponding psychiatrist or psychologist was not always the same person. Furthermore, as long COVID is a relatively rare and new diagnosis, in this single-site retrospective cohort study we only report on a small patient group, which may result in statistical biases.
Pediatric patients with the diagnosis of long COVID and changes in smell and taste seem to be at risk of developing an eating disorder. Pediatricians should be aware of red flags while obtaining a medical history and performing a physical examination of these patients. As stated on many occasions, the mental health of children and young adults has suffered during the pandemic of SARS-CoV-2 (13). The possibility of consultation with a Child and Adolescent Psychiatrist or a Child Psychologist and access to necessary psychotherapies are urgently needed (32). Screening methods to detect secondary eating disorders in patients suffering from long COVID could be a helpful to pediatricians and child psychiatrists. Collaboration with child and adolescent psychiatrists as well as teachers, sports coaches, social workers, and families is even more necessary during the COVID-19 pandemic than in non-COVID-19 times. More research with larger patient groups is needed to support the hypothesis that changes in taste and smell due to long COVID are a risk for developing anorexia nervosa in pediatric patients. We hope to test this in a multicenter prospective study in the near future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical Faculty of the University Duisburg-Essen (22-10581-BO). Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Study conception and design: SG, CDS, MB, JH; Acquisition of data: SG, MB; Analysis and interpretation of data: SG, CDS, MB, JH, NB; Drafting and revising the manuscript: SG, CDS, MB, BD, JH, NB, UF. All authors read and approved the final manuscript. All authors contributed to the article and approved the submitted version.
We thank our patients and their families for the trust they have placed in us. We would also like to thank our colleagues in pediatric cardiology, pediatric pneumology and neuropediatric, who have always supported us with great personal commitment in the care. Furthermore, we would like to thank our colleagues of the psychosomatic department, as well as the colleagues of the child and adolescents for all the acute appointments that were made possible. The authors thank M. Schuendeln, Department of Pediatrics III, Pediatric Oncology and Hematology, University Hospital Essen, Germany for his expert statistical advice, and Catherine Bolger, Palo Alto, CA for her critical review of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.1022669/full#supplementary-material.
AWMF, German national guidelines; BAU, Binding antibody units; BMI, Body mass index; CI, Confidence interval; ECG, Electrocardiogram; ECHO, Electrocardiography; ED, Eating disorder; EEG, Electroencephalogram; ENT, Ear Nose and Throat Specialist; ICD-11, International Classification of Disease 11; kg, Kilogram; LC, Long COVID; LCI, Lung Clearance Index; m², Square meter; MRI, Magnetic Resonance Imaging; N, Number; NCV, Nerve Conduction Velocity; Perc, Percentile; PIMS, Pediatric-Inflammatory-Multisystem-Syndrome; SAT, Smell and taste dysfunction; SCOFF, Anorexia questionnaire (“Sick, Control, One, Fat, Food”).
1. Swann OV, Holden KA, Turtle L, Pollock L, Fairfield CJ, Drake TM, et al.; ISARIC4C investigators. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: prospective multicenter observational cohort study. Br Med J. (2020) 370:m3249. doi: 10.1136/bmj.m3249
2. Rimensberger PC, Kneyber MCJ, Deep A, Bansal M, Hoskote A, Javouhey E, et al.; European society of paediatric and neonatal intensive care (ESPNIC) scientific Sections’ collaborative group. Caring for critically ill children with suspected or proven coronavirus disease 2019 infection: recommendations by the scientific Sections’ collaborative of the European society of paediatric and neonatal intensive care. Pediatr Crit Care Med. (2021) 22(1):56–67. doi: 10.1097/PCC.0000000000002599
3. Freedman S, Godfred-Cato S, Gorman R, Lodha R, Mofenson L, Murthy S, et al. Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19. https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19: World Health Organization; (2020)
4. Martin B, DeWitt PE, Russell S, Anand A, Bradwell KR, Bremer C, et al. Characteristics, outcomes, and severity risk factors associated with SARS- CoV-2 infection among children in the US national COVID cohort collaborative. JAMA Netw Open. (2022) 5(2):e2143151. doi: 10.1001/jamanetworkopen.2021.43151
5. Jackson WM, Price JC, Eisler L, Sun LS, Lee JJ. COVID-19 in pediatric patients: a systematic review. J Neurosurg Anesthesiol. (2022) 34(1):141–7. doi: 10.1097/ANA.0000000000000803
6. Koczulla AR, Ankermann T, Behrends U, Berlit P, Böing S, Brinkmann F, et al. S1-Leitlinie Post-COVID/Long- COVID. https://www.awmf.org/uploads/tx_szleitlinien/020027l_S1_Post_COVID_Long_COVID_2021-07.pdf (Stand 12.07.2021)
7. Venkatesan P. NICE Guideline on long COVID. Lancet Respir Med. (2021) 9(2):129. doi: 10.1016/SS2213-2600(21)00031-X
8. Buonsenso D, Di Gennaro L, Rose C, Morello R, D'llario F, Zampino G, et al. Long-term outcomes of pediatric infections: from traditional infectious diseases to long COVID [published online ahead of print, 2022 mar 10]. Future Microbiol. (2022) 8(17):554–7. doi: 10.2217/fmb-2022-0031
9. Roge I, Smane L, Kivite-Urtane A, Pucuka Z, Racko I, Klavina L, et al. Comparison of persistent symptoms after COVID-19 and other non-SARS-CoV-2 infections in children. Front Pediatr. (2021) 9:752385. doi: 10.3389/fped.2021.752385
10. Radtke T, Ulyte A, Puhan MA, Kriemler S. Long-term symptoms after SARS-CoV-2 infection in children and adolescents. JAMA. (2021) 326(9):869–71. doi: 10.1001/jama.2021.11880
11. Hintschich CA, Fischer R, Hummel T, Wenzel JJ, Bohr C, Vielsmeier V. Persisting olfactory dysfunction in post-COVID-19 is associated with gustatory impairment: results from chemosensitive testing eight months after the acute infection. PLoS One. (2022) 17(3):e0265686. doi: 10.1371/journal.pone.0265686
12. Bruns N, Willemsen L, Stang A, Kowall B, Holtkamp K, Kamp O, et al. Pediatric intensive care unit admissions after adolescent suicide attempts during the pandemic. Pediatrics. (2022) 150(2):4–7. doi: 10.1542/peds.2021-055973
13. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. (2021) 175(11):1142–50. doi: 10.1001/jamapaediatrics.2021.2482
14. Ougrin D, Wong BH, Vaezinejad M, Plener PL, Mehdi T, Romaniuk L, et al. Pandemic-related emergency psychiatric presentations for self-harm of children and adolescents in 10 countries (PREP-kids): a retrospective international cohort study. Eur Child Adolesc Psychiatry. (2021):1–13. doi: 10.1007/s00787-021-01741-6
15. Spina G, Roversi M, Marchili MR, Raucci U, Fini F, Mirra G, et al. Psychiatric comorbidities and dehydration are more common in children admitted to the emergency department for eating disorders in the COVID-19 era. Eat Weight Disord. (2022):1–8. doi: 10.1007/s40519-022-01386-7
16. Buonsenso D, Martino L, Morello R, De Rose C, Valentini P. Chronic olfactory dysfunction in children with long COVID: a retrospective study. Children (Basel). (2022) 9(8):1251. doi: 10.3390/children9081251
17. Haripersad YV, Kannegiesser-Bailey M, Morton K, Skeldon S, Shipton N, Edwards K, et al. Outbreak of anorexia nervosa admissions during the COVID-19 pandemic. Arch Dis Child. (2021) 106(3):e15. doi: 10.1136/archdischild-2020-319868
18. Agostino H, Burstein B, Moubayed D, Taddeo D, Grady R, Vyver E, et al. Trends in the incidence of new-onset anorexia Nervosa and atypical anorexia Nervosa among youth during the COVID-19 pandemic in Canada. JAMA network Open vol. 4. (2021) 12:e2137395. doi: 10.1001/jamanetworkopen.2021.37395
20. Kromeyer-Hauschild M, Wabitsch D, Kunze F, Geller HC, Geiß V, Hesse A, et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben; Monatsschrift Kinderheilkunde. (2001) Ausgabe 8/2001; 01.08.2001
21. Micali N, Hagberg KW, Petersen I, Treasure J. The incidence of eating disorders in the UK in 2000–2009: findings from the general practice research database. BMJ Open. (2013) 3(5):e002646. https://doi.org/10.1136/bmjopen-2013-00264623793681
22. Brockmeyer T, Cuntz U, Ehrlich S, Fichter MM, Friedrich H-C, Greetfeld M, et al. S3-Leitlinie Diagnostik und Behandlung der Essstörung. (Stand 31.05.2018) https://www.awmf.org/uploads/tx_szleitlinien/051-026l_S3_Essstoerung-Diagnostik-Therapie_2020-03.pdf
23. Vyver E, Katzman DK. Anorexia nervosa: a paediatric health crisis during the COVID-19 pandemic. Paediatrics Child Health. (2021) 2021:1–2. doi: 10.1093/pch/pxab031
24. Fan Y, Li Y, Liu A, Hu X, Ma G, Xu G. Associations between body mass index, weight control concerns and behaviours, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health. (2010) 10:314. doi: 10.1186/1471-2458-10-314
25. Micali N, Hilton K, Nakatani E, Heyman I, Turner C, Mataix-Cols D. Is childhood OCD a risk factor for eating disorders later in life? A longitudinal study. Psychol Med. (2011) 41(12):2507–13. doi: 10.1017/S003329171100078X. Epub 2011 Jun 7. Erratum in: Psychol Med. 2011 Dec;41(12):2514. Natatani, E [corrected to Nakatani, E].21733209
26. Fichter MM. Epidemiologie der essstörungen. In: Herpertz S, de Zwaan M, Zipfel S, editors. Handbuch essstörungen und adipositas. Heidelberg: Springer-Verlag (2008). p. 38–41.
27. Gravina G, Milano W, Nebbiai G, Piccione C, Capasso A. Medical complications in anorexia and bulimia Nervosa. Endocr Metab Immune Disord Drug Targets. (2018) 18(5):477–88. doi: 10.2174/1871530318666180531094508
28. Herpertz-Dahlmann B. Adolescent eating disorders: update on definitions, symptomatology, epidemiology, and comorbidity. Child Adolesc Psychiatr Clin N Am. (2015) 24(1):177–96. doi: 10.1016/j.chc.2014.08.003
29. Iwajomo T, Bondy SJ, de Oliveira C, Colton P, Trottier K, Kurdyak P. Excess mortality associated with eating disorders: population-based cohort study. Br J Psychiatry. (2021) 219(3):487–93. doi: 10.1192/bjp.2020.197
30. van Hoeken D, Hoek HW. Review of the burden of eating disorders: mortality, disability, costs, quality of life, and family burden. Curr Opin Psychiatry. (2020) 33(6):521–7. doi: 10.1097/YCO.0000000000000641
31. Morgan JF, Reid F, Lacey JH. SCOFF Questionnaire: a new screening tool for eating disorders. West J Med. (2000) 172(3):164–4. doi: 10.1136/ewjm.172.3.164
32. Statistical press notice, Children and Young People with an Eating Disorder Waiting Times Q1 2021-22,. The Government Statistical Service (GSS) statistician with overall responsibility for the data in this report is: Performance Analysis Team, Primary Care, Public Health, Mental Health and Quality (PPMQ), NHS England and NHS Improvement, Premier House, 60 Caversham Road, Reading RG1 7EB https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2021/08/CYP-ED-Waiting-Times-Statistical-Press-Notice-Q1-2021-22.pdf.
Keywords: pediatric long COVID, anosmia, ageusia, eating disorder, anorexia
Citation: Brasseler M, Schönecker A, Steindor M, Della Marina A, Bruns N, Dogan B, Felderhoff-Müser U, Hebebrand J, Dohna-Schwake C and Goretzki SC (2022) Development of restrictive eating disorders in children and adolescents with long-COVID-associated smell and taste dysfunction. Front. Pediatr. 10:1022669. doi: 10.3389/fped.2022.1022669
Received: 18 August 2022; Accepted: 10 October 2022;
Published: 24 November 2022.
Edited by:
Hulya Bukulmez, Case Western Reserve University, United StatesReviewed by:
Martin Brizuela, Hospital Velez Sarsfield, Argentina© 2022 Brasseler, Schönecker, Steindor, Della Marina, Bruns, Dogan, Felderhoff-Müser, Hebebrand Dohna-Schwake and Goretzki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maire Brasseler TWFpcmUuQnJhc3NlbGVyQHVrLWVzc2VuLmRl Sarah C. Goretzki U2FyYWguR29yZXR6a2lAdWstZXNzZW4uZGU=
Specialty Section: This article was submitted to Pediatric Infectious Diseases, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.