 Jinghua Wu
Jinghua Wu Yi Yu
Yi Yu Xinmeng Yao
Xinmeng Yao Qinzhun Zhang
Qinzhun Zhang Qin Zhou3
Qin Zhou3 Chengyin Ye
Chengyin Ye
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 30 September 2022
Sec. Pediatric Immunology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.1019371
Background: Asthma is one of the most common chronic diseases in children globally. In recent decades, advances have been made in understanding the mechanism, diagnosis, treatment and management for childhood asthma, but few studies have explored its knowledge structure and future interests comprehensively.
Objective: This scientometric study aims to understand the research status and emerging trends of childhood asthma.
Methods: CiteSpace (version 5.8.R3) was used to demonstrate national and institutional collaborations in childhood asthma, analyze research subjects and journal distribution, review research keywords and their clusters, as well as detect research bursts.
Results: A total of 14,340 publications related to childhood asthma were extracted from Web of Science (core database) during January 2011 to December 2021. The results showed that academic activities of childhood asthma had increased steadily in the last decade. Most of the research was conducted by developed countries while China, as a developing country, was also actively engaged in this field. In addition to subjects of allergy and immunology, both public health aspects and ecological environmental impacts on the disease were emphasized recently in this research field. Keywords clustering analysis indicated that research on asthma management and atopy was constantly updated and became the two major research focuses recently, as a significant shift in research hotspots from etiology and diagnosis to atopic march and asthma management was identified. Subgroup analysis for childhood asthma management and atopy suggested that caregiver- or physician-based education and interventions were emerging directions for asthma management, and that asthma should be carefully studied in the context of atopy, together with other allergic diseases.
Conclusions: This study presented a comprehensive and systematic overview of the research status of childhood asthma, provided clues to future research directions, and highlighted two significant research trends of asthma management and atopy in this field.
As a non-communicable disease that often onsets in childhood, asthma affects approximately 300 million people of all ages worldwide (1). Among children aged 0 to 18, asthma is the most common chronic disease and has been called the epidemic of the 21st century, ranking among the top 20 conditions worldwide for disability-adjusted life years (2). The ISAAC study estimated that the global prevalence of parent-reported and doctor-diagnosed asthma among 6-7-year-old children to be 10.8%, with lower rates in Northern and Eastern Europe (4.5%), and the highest rates in North America (20.0%) and Oceania (29.2%) (3). At the same time, asthma not only causes substantial disability, impaired quality of life, or deaths in children, but also brings significant health and economic burden to their families and the whole society. It was reported by the U.S. Center for Disease Control and Prevention that asthma was the third leading cause of hospitalization among children under the age of 15 years, and asthma attacks caused approximately 13.8 million days of absence in school-aged children in 2013 (4). Globally speaking, developed economies spent 1% to 2% of their healthcare budget on asthma (1). In England, 69% of parents or guardians of asthmatic children reported having to take time off work due to their children's asthma, and 13% had lost their jobs (5). In addition, it is worth noting that childhood asthma prevalence in developing countries is increasing rapidly with advancing industrialization and urbanization, with increased mortality related to asthma and higher burden observed in these underserved regions (6, 7). Therefore, new insights are demanded in order to develop localized asthma prevention and treatment strategies in developing countries, to reduce its morbidity and disease burden and to benefit the treatment of other related respiratory or allergic diseases.
Currently, emerging epidemiological studies of asthma have been reported and plenty of risk and protective factors have been identified and recognized. Evidence has shown that exposure to smoking, air pollution, obesity and viral infection etc. is associated with an increased risk for asthma, while vitamin D or fish oil supplementation and exposure to diverse environmental microbiome can decrease the risk of asthma or its symptoms (8–13). Meanwhile, progress has also been made in understanding pathophysiological mechanisms of asthma development and exacerbation in children, especially in cytokines, innate lymphoid cells, macrophages/monocytes, T cells, as well as epithelium (14–18). In terms of diagnosis, several scoring systems and novel measures of airway physiology (e.g., electronic nose breath prints) have been developed, in addition to traditional approaches based on symptoms and evidence of variable expiratory airflow limitation obtained from bronchodilator reversibility testing or other tests (19–21). In terms of treatment and management, although treatments for type 2 (T2) inflammations, including drugs targeting interleukin (IL)-4, IL-5, and IL-13, have been well developed over the past decade, population heterogeneity and medication adherence are still challenges and broad psychosocial, behavioral or public health approaches should be further explored (22). The Global Initiative for Asthma (GINA) Strategy Report points out that asthma management is not a “one-size-fits-all” solution but a personalized assess–treat–review cycle, where either regular personalized assessment, treatment of modifiable risk factors, self-management education, skills training, or appropriate medication adjustment and review are essential to optimize treatment outcomes (19). On the other hand, the concept of atopic march has recently been put forward, referring to the natural progress of allergic diseases. This atopic march usually develops throughout the course of infancy and childhood, begins with atopic dermatitis (AD), and progresses to IgE-mediated food allergy (FA), asthma, and allergic rhinitis (AR). This well-recognized concept has also provided a new perspective for mechanistic research, prevention, treatment and management of asthma (23).
Although studies on asthma have increased substantially, researchers have not systematically analyzed the evolution of academic achievements in this field over the last decades. Therefore, a literature review is needed to understand the research status and future interests of childhood asthma. Scientometric measures and analyzes the quantitative features and characteristics of science, science communication, and scientific research (24). As a component of scientometric analysis, bibliometric mapping/analysis combines mathematical and statistical methods of quantitative analysis and has been widely used in various fields to describe academic landscapes, explore evolutionary processes and predict emerging trends in a particular study field (25, 26). CiteSpace, an informational visualization software which was developed by Chaomei Chen using Java programming language, can combine information visualization methods, bibliometrics, and data mining algorithms in an interactive visualization tool to extract patterns in citation data (27). This software has been widely used to conduct scientometric analyses in various scientific areas, such as harnessing telemedicine, Alzheimer's disease, HIV and so on (25, 28, 29).
However, limited study has been conducted to analyze bibliometric and scientometric features of scientific studies related to childhood asthma, and to explore the research trends and hotspots of this field. In this study, we aimed to employ CiteSpace to analyze the retrieved literatures in this research field in a visualization way, constructing co-occurrence networks and detecting the research hotspots and frontiers by time. It is anticipated that this work could provide a comprehensive and systematic understanding of recent research status and give clues to the development trends of childhood asthma.
First, Web of Science (WOS) core database, which includes Social Science Citation Index (SCI-EXPANDED), Social Science Citation Index (SSCI), Arts / Humanities Citation Index (AHCI), Emerging Sources Citations Index (ESCI), Current Chemical Reactions (CCR-EXPANDED) and Index Chemicus (CI), were used as the data source to conduct an academic search. During the retrieval process, the inclusion criteria for publications were as follows: (1) published between January 2011 and December 2021, (2) the topic search was “childhood asthma” or “pediatric asthma”, (3) published in English, (4) the document type was “article” or “review”. Initially, a total of 14,678 publications were collected. Then, by using CiteSpace, 338 publications were excluded due to duplication or irrelevance. Finally, a total of 14,340 literatures, containing 12,051 articles and 2,289 reviews, were collected and used for the following analysis. More details about the workflow of data collection could be found in Figure 1. Bibliographic records of all these studies were downloaded, including title, abstract, author details, affiliation, keywords, and citations.
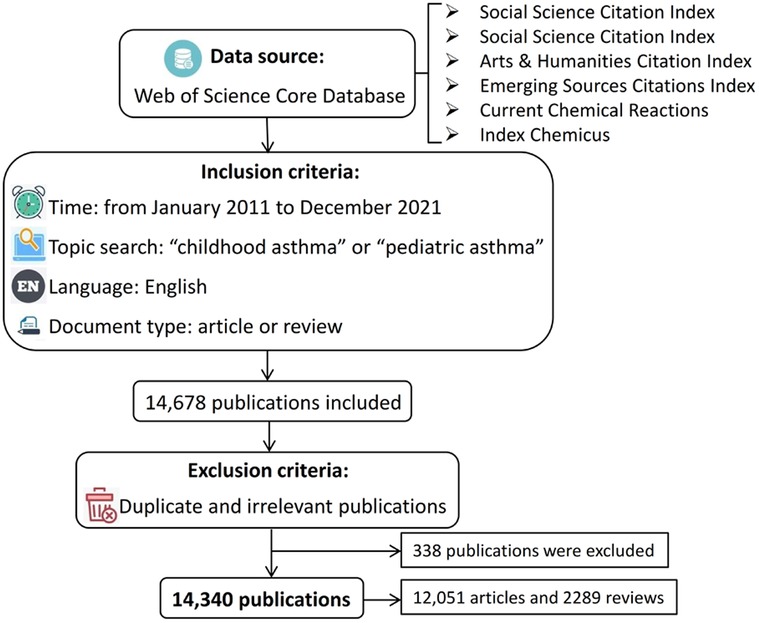
Figure 1. Workflow of data selection.
In subgroup keywords analysis, those met all of the following criteria were included in data of “childhood asthma management”: (1) published between January 2011 and December 2021, (2) the topic search was “childhood asthma management” or “pediatric asthma management”, (3) published in English, (4) the document type was “article” or “review”. After excluding duplicate publications, 2,765 literatures with their bibliographic records were downloaded for analysis. For the subgroup analysis of atopy, the term “atopy” was used, and articles or reviews published between January 2011 and December 2021 in English were included. After excluding duplicate publications, a total of 4,770 literatures were collected.
CiteSpace is a Java-based software developed by Chaomei Chen to map the structure and dynamics of knowledge domains in a certain scientific field via computer algorithms and interactive visualizations (30). Specifically, CiteSpace can be used to identify the leading collaborations among countries, authors, and institutions, visualize the distribution of research fields, analyze co-occurring keywords and burst terms, and generate clusters of keywords or co-citing reference publications (27). Compared with other methods such as co-citation, CiteSpace's keywords analysis also provided research focus and structure of a certain discipline, and is more suitable for analyzing the development trends and frontiers of either mature disciplines or emerging disciplines. In addition, CiteSpace's cluster analysis can categorize scientific papers and their features according to the degree of similarity, providing prominent groups, and discerning what methods and tools have been developed (27, 30).
SPSS 24 was used to create the fitting curve for the number of publications. Journals' impact factors were all obtained from the 2020 version of Journal Citation Reports, which provides transparent, publisher-neutral data and statistics. CiteSpace (version 5.8.R3) was used for analyzing and visualizing co-occurrence and co-citation networks. Based on the collected data, we reviewed the main countries and institutional collaborations that contributed to childhood asthma research, analyzed the research categories and journals' distribution, summarized keywords and their clusters, and detected research bursts over the last decade. Besides, subgroup keywords analysis for childhood asthma management and atopy were also conducted respectively. First, to map and visualize networks, term source was set as title, abstract, author keywords and keywords plus, while node type was set as country, institution, category, cited journal or keyword, successively. In addition, we ran network analyses by using the cosine link reduction method and selected pathfinder to prune the merged network, as this technique can simplify the network and highlight the important structural features. Then, following the keyword co-occurrence analysis, we used the burst detection function to catch the decline or rise of a keyword and explored the emerging trend during a certain period of time. After that, to further study salient topics and research trends in childhood asthma, we conducted the cluster analysis, where similar objects were combined to determine related areas of study. Specifically, we employed the latent semantic indexing (LSI) algorithm to analyze adjacent terms and keywords of childhood asthma, and ultimately formed clusters. This algorithm can not only reflect the frequency of term occurrence but also overcome the situation of polysemy and synonym. The size of the cluster depends on the involved number of objects, as ID 0 (#0) is the largest cluster that contains the largest number of keywords. When measuring how similar an object was to its own cluster compared to other clusters, the silhouette value (S) was adopted, where S > 0.7 indicated a high level of term consistency within the certain cluster.
In terms of visualization, each item is presented as a node, and a link between two nodes describes co-occurrence or co-citation. A thicker link indicates that the two nodes cooperate or co-occur more often. Rings of different colors in the node represent the node's frequency of occurrence in different years (i.e., the larger the ring, the higher the frequency), and details about the year represented by each color can be found in the legend for each figure. It is worth noting that the betweenness centrality is an indicator that can be used to evaluate the importance of each item in the visualization network, generally items with centrality ≥0.1 will be displayed in purple in their outer circle, indicating that this node as a hub that has important interactive significance.
A total of 14,340 publications related to childhood asthma were extracted from Web of Science (core database) during the last decade, from January 2011 to December 2021. In 2011, the publication number was 911, then, over the next decade, there was a steadily increasing trend in the number of publications in this research field. Besides, according to the cubic fitting curve (R2 = 0.9468, p < 0.05), the number of publications was expected to continue growing rapidly over the next five years (Figure 2).

Figure 2. Yearly number of publications related to childhood asthma from 2011 to 2021.
In order to explore the discipline distribution of the above 14,340 publications, we performed the co-occurrence analysis for their involved subjects. As a result, a total of 182 nodes and 1,098 links were generated on the map, as shown in Figure 3. It was found that most publications centered on subjects of allergy, immunology, and pediatrics. Specifically, subjects (centrality > 0.1) with the most prominent collaborative influence on pediatric asthma were public, environmental and occupational health, environmental sciences / ecology and pediatrics (Multimedia Supplementary Appendix 1), showing a trend of multi-polarization of research subjects. When analyzing the engaged journals in the research field, the top three co-cited journals were sorted as follows: J ALLERGY CLIN IMMUN (9,375, IF2020 = 10.793), AM J RESP CRIT CARE (6,958, IF2020 = 20.405) and EUR RESPIR J (6,342, IF2020 = 16.671). These journals were also the hubs in the network having relatively more interactions with other journals, indicating their significant impacts on childhood asthma research (see Multimedia Supplementary Appendix 2). It was worth noting that, two comprehensive top-level medical journals, “NEW ENGL J MED” and “LANCET”, were also found to provide research frontiers and hotspots in childhood asthma, facilitating the construction of the disease's knowledge base from perspectives of medicine, biology, management and psychology.
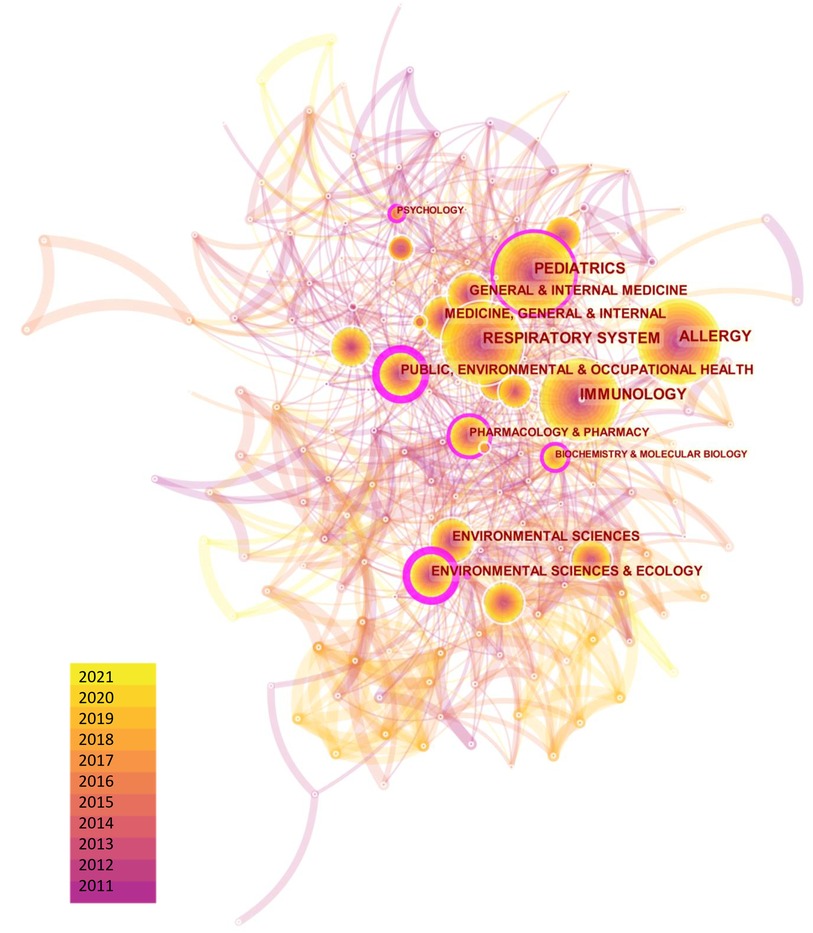
Figure 3. Distribution of subjects involved in childhood asthma research.
We also generated regional and institutional distribution maps using CiteSpace to explore the contribution of different countries and the collaboration among major institutions to childhood asthma research. Figure 4A showed the collaborative network between different countries, where 144 nodes and 1,679 links were generated in total. It was found that, most of the top 10 countries actively in this field were concentrated in developed countries, including the USA (n = 5,716), the UK (n = 1,336), or European Union countries (n = 3,342), etc. On the other hand, as a developing country, People's Republic of China ranked third in the number of publications and it surpassed the UK since 2019, indicating that, along with the rapid development of the economy and technology, research interests in childhood asthma in China have a booming trend (Figure 4C), which may be attributed to the continued increase in asthma prevalence in this country. However, no country's centrality was ≥0.1, indicating that cooperation among countries has yet to be promoted. The distribution of institutions engaged in childhood asthma has been displayed in Figure 4B. Geographical location had a great impact on scientific collaboration between institutions, as the network revealed that the institutions with active collaborations were mainly divided into two parts, one was gathered by universities and hospitals in the USA, and the other is assembled by European countries in a relatively scattered way (see Multimedia Supplementary Appendix 3).
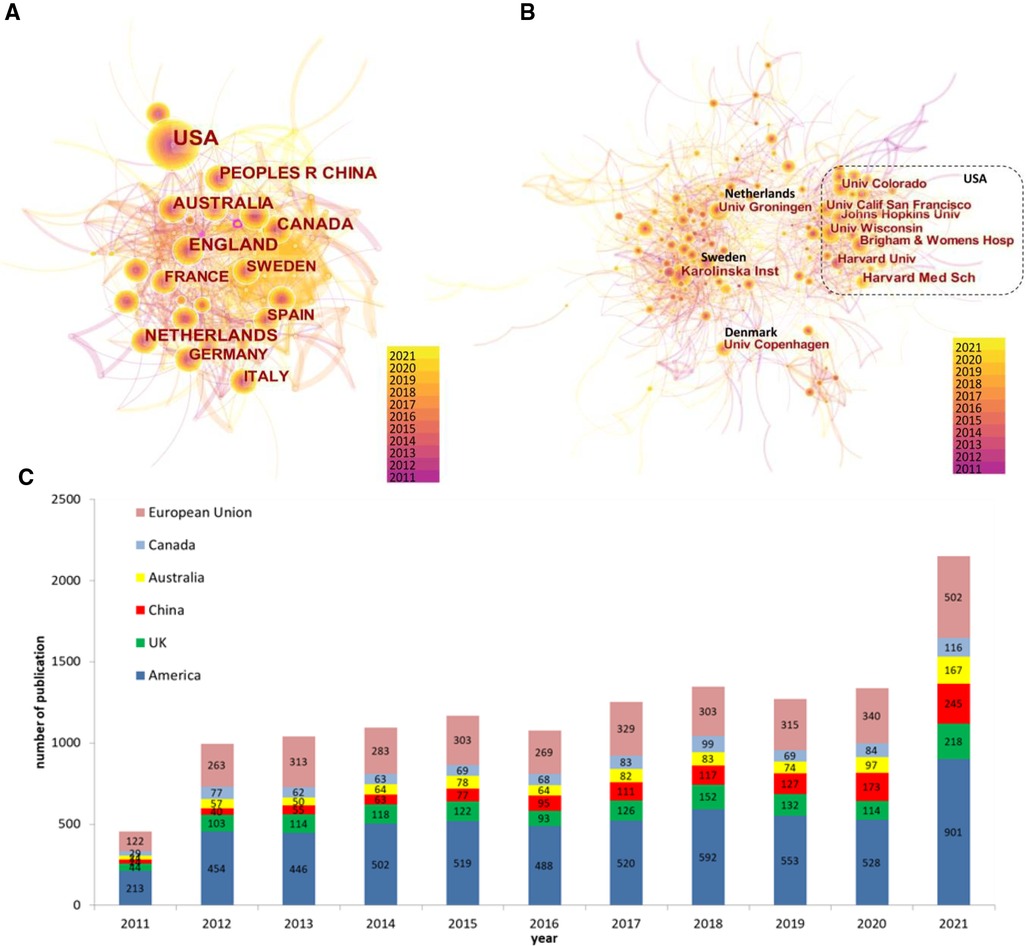
Figure 4. Distribution of (A) regions, (B) institutions, and (C) the top-10 countries' annual number of publications in childhood asthma research. *European Union includes Netherlands, German, Italy, Sweden and Spain.
Keywords reflect the core and focus of a paper. A total of 76 keywords were identified in the field of childhood asthma during the keyword co-occurrence analysis, revealing the research topics of greatest interests (Figure 5). Then, we classified the top keywords into 6 different themes to identify research priorities (Table 1), including atopy, management, risk factor, population, pathogenesis and diagnosis. Among them, the top 10 keywords ranked by frequency and centrality were also listed in the Multimedia Supplementary Appendix 4. Besides, we further conducted the cluster analysis by LSI algorithm to aggregate closely related and often concurrent keywords together, detailed information was summarized in Table 2 and Multimedia Supplementary Appendix 5. A total of 9 clusters were obtained and their silhouette values were all greater than 0.8, indicating that the keywords under each cluster attained a high level of consistency.
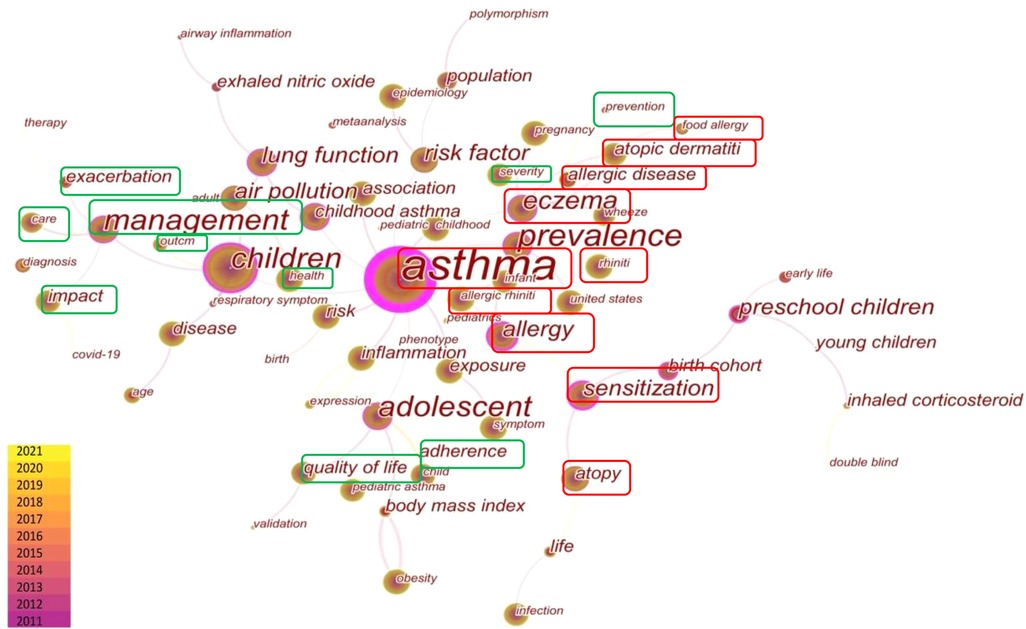
Figure 5. Distribution of co-occurring keywords.
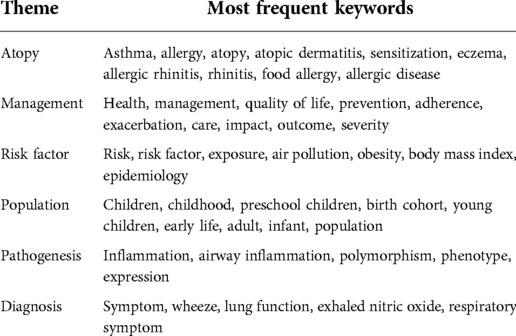
Table 1. Research keywords in childhood asthma listed by theme.

Table 2. Detailed information for keywords clusters.
Specifically, the most predominant theme was atopy. Atopic march usually begins in early life, and the most common feature of these diseases is allergy (cluster#7) or sensitization. Poor control of one allergic disease often triggers or aggravates others, and thus having atopic dermatitis (cluster#4) or food allergy in early life greatly increases the risk of allergic rhinitis (cluster#6) and asthma (cluster#0) later. Therefore, asthma, as an end point event of atopic march, is often placed in the context of atopy and co-studied with other allergic diseases. Another extensive theme is childhood asthma management, the keywords indicated that, according to the severity of asthma, a series of care services were investigated and explored to improve patients' adherence, prevent exacerbation of asthma, and ultimately achieve the outcome of improving the quality of life and health status for children.
In the theme of risk factors, exposure to air pollution (cluster#2) and obesity (cluster#3) were the most commonly studied factors. Researchers also focused on the impact of cigarette smoking and PM2.5 on asthma and the risk of developing COPD in the future. Physical education via smartphones was considered as an important way to manage obesity in asthmatic children. As for population, preschool children (cluster#5) received more attention, with particular research focus on the disease “severity” and “association” with atopy, such as allergic rhinitis and milk sensitization. Lastly, inflammation and polymorphism has been widely investigated in the pathogenesis theme, and combining respiratory symptoms and exhaled nitric oxide to access lung function was the continuous focus in the asthma diagnosis theme.
To further investigate changes of research hotspots over the last decade, we used the CiteSpace built-in burst detection algorithm and detected 17 keywords that had citation bursts (Figure 6). The burst strength was calculated as the growth rate of keywords being cited over time. Notably, the result showed that research hotspots have shifted significantly over the last decade.
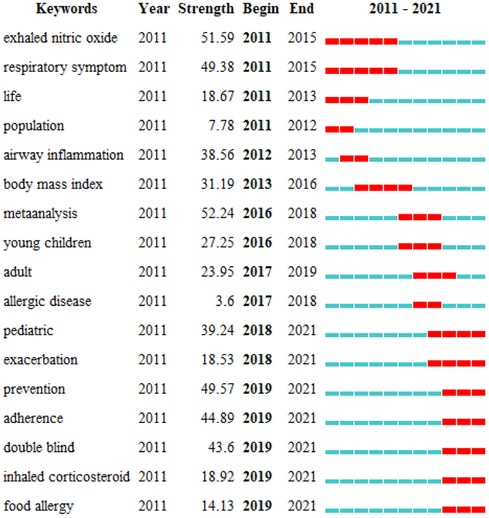
Figure 6. Top 17 keywords with the strongest citation bursts.
From 2011 to 2016, the research hotspots were mainly related to the categories of asthma etiology (e.g., mechanisms of airway inflammation), diagnosis (e.g., exhaled nitric oxide detection and respiratory symptoms), and risk factors (e.g., obesity related body mass index), where most of the publications were related to development of diagnostic/prognostic tools or investigation of risk factor (Table 3). To facilitate asthma prognostic, Leif Bjermer et al. demonstrated that exhaled nitric oxide was a valuable tool for improving the personalized management (31). With regard to airway inflammation, H L Petsky et al. provided evidence that monitoring airway inflammation by eosinophils in induced sputum was useful in reducing asthma exacerbations (35). Shu Mei Teo et al. proposed that early asymptomatic colonization with streptococcus was a strong asthma predictor (33). In terms of risk factors, Guarnieri et al. showed that exposure to poor air quality may increase the risk of exacerbations of asthma symptoms (32). Notably, regarding to BMI, Pulgarón ER pointed out that the interaction between healthy weight and asthma control was still unclear (36).
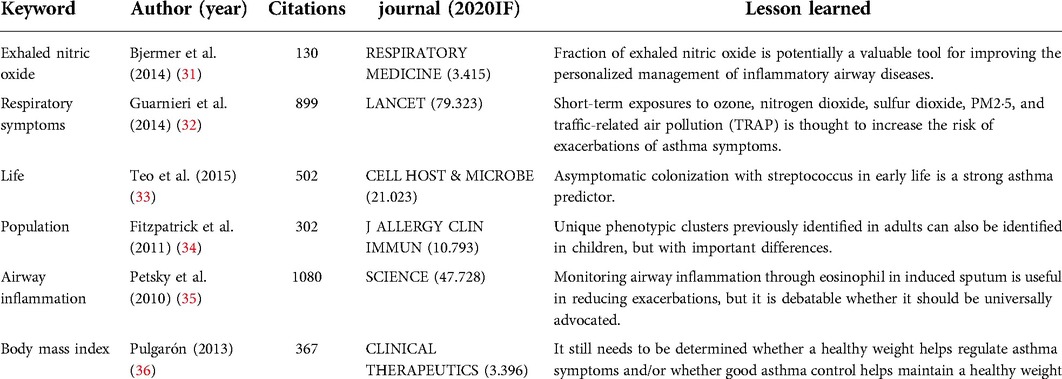
Table 3. Lessons learned from landmark publications from 2011 to 2016.
From 2016 to 2021, the scholarly activity in childhood asthma was shifted to themes of asthma management and atopy, which were different from the earlier landmarks (Table 4). With regard to asthma management, how to improve adherence and prevent exacerbation gradually attracted more attention recently. Specifically, Petsky et al. presented a method of reducing asthma exacerbation by adjusting treatment to sputum eosinophil (35). Greer et al. reported that breastfeeding ≥3 to 4 months can prevent wheezing in the first 2 years of life and a longer duration of breastfeeding can prevent asthma even after 5 years of age (42). Trivedi et al. reported poor adherence with inhaled glucocorticoids (41). In order to overcome this problem, Gupta et al. introduced a sensor-based inhaler monitoring with clinical feedback intervention to potentially improve the adherence of inhalable corticosteroids (43). From the perspective of atopy, allergic diseases, especially food allergy, had showed the citation burst. Lodge et al. described that breastfeeding had varying degrees of protection against various allergic diseases (40), and Peters et al. reported that the prevalence of allergic diseases, including asthma, has risen sharply (45).
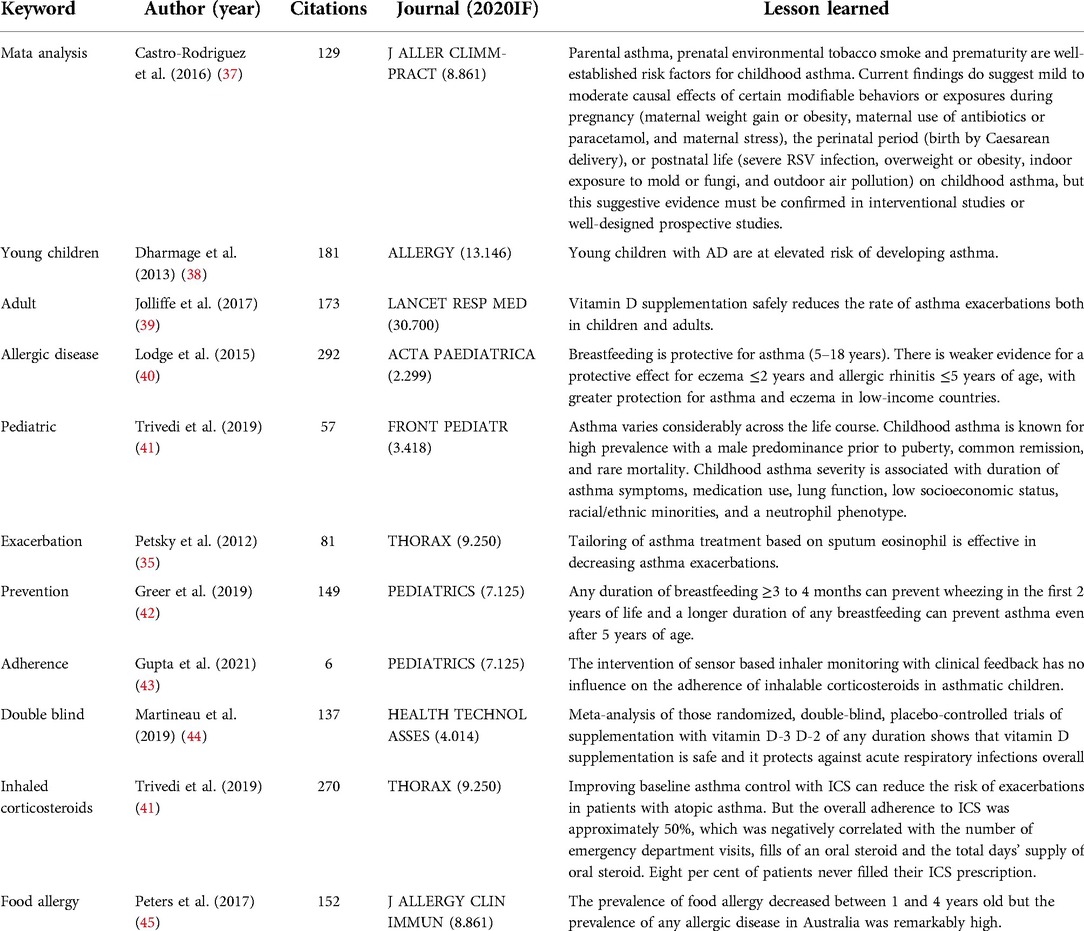
Table 4. Lessons learned from landmark publications from 2016 to 2021.
Since “management” and “atopy” have become the research hotspots in childhood asthma in recent years, keyword subgroup analysis was further conducted on these two themes individually.
In the keyword cluster investigation for “childhood asthma management”, a total of 7 clusters were generated (Figure 7A). The most significant cluster was ADRB2 (cluster#0). The ADRB2 gene polymorphism was found to not only be associated with the susceptibility and severity of asthma, but also affected the therapeutic effect of bronchodilators, and thus specific genetic testing was recommended before certain medication treatments, so as to select the most suitable drug for pediatric asthma management (46, 47).

Figure 7. (A) Distribution of keywords cluster in childhood asthma management; (B) Keywords with the strongest citation burst nearly five years in childhood asthma management.
Cluster#1, #2 and #7 investigated the adverse effects of poor asthma management. Poor asthma control not only caused the hyperresponsiveness, but also increased direct and indirect cost, including hospitalizations, emergency department presentations, medical practitioner visits and medication. Meanwhile, clusters#3, #4, #5 and #6 attempted to provide solutions to minimize these adverse effects. First, plenty of studies suggested that asthma needs to be managed as part of the atopic march in association with other allergic diseases (cluster#3), which was consistent with our findings that atopy-related keywords (e.g., atopic dermatitis, food allergy and allergy) have recently shown the strongest citation bursts together with childhood asthma (Figure 7B). Second, due to the caregivers' cognitive errors, lack of knowledge, or difficulties in adhering to medication, researchers emphasized the family-based interventions, such as cognitive, behavioral and psychological education for caregivers (cluster#4) (48–50). With regard to medications, poor adherence to inhaled corticosteroids was still a key problem in asthma management, and global guidelines were constantly updated to adjust the dose and timing of medicines used in stepwise asthma management (cluster#5) (51–53). The “national asthma education and prevention program” was formed as cluster#6. The program, initiated by the National Heart, Lung, and Blood Institute in the United States, developed the first national consensus clinical practice guidelines for asthma treatment in 1991 and has been continuously updated since then. The program not only pointed out for the first time the significance of physician education, but also called for clinical education outreach, improved physician decision support tools, as well as redesign of health system, to facilitate childhood asthma management (54).
Similarly, cluster map and keywords analysis for the theme of atopy were performed and shown in Figure 8. A total of 10 clusters were captured, 7 of which were directly associated with atopy. During the course of the atopic march, atopic dermatitis (cluster#0), allergic condition (cluster#1), and food allergies (cluster#2) usually appear in infancy and then progress to asthma (cluster#3) or allergic rhinitis (cluster#6). All these allergic diseases formed independently as distinct clusters in our cluster map of the “atopy” theme. Besides, other gastrointestinal or skin symptoms or complications, such as chronic urticaria (cluster#8) and eosinophilic esophagitis (cluster#9), also appeared in the cluster map of atopy.

Figure 8. (A) Distribution of keywords cluster in atopy; (B) Keywords with the strongest citation burst nearly five years in atopy.
Notably, “asthma phenotypes” (cluster#3) not only formed a unique cluster, but also attained the strongest citation burst, indicating the significance of asthma phenotype research in the “atopy” theme. After retrieving the relevant literatures, it was found that heterogeneity of asthma was widely discussed recently. According to the atopic response, duration of asthma, and airflow restriction, childhood asthma could be divided into four phenotypes, namely late-onset symptomatic asthma, early-onset atopic asthma with normal lung function, early-onset atopic asthma with mild airflow limitation and co-morbidities, and early-onset atopic asthma with advanced airflow limitation (34). Another study of two large birth cohorts divided the typical symptom of asthma—wheeze into five phenotypes, which were never/infrequent wheeze, transient early wheeze, intermediate-onset wheeze, late-onset wheeze and persistent wheeze (55). Among them, intermediate-onset wheeze was found to be closely related to atopy, reduced lung function and increased airway hyperresponsiveness. It was worth noting that, in the keywords analysis of the “atopy” theme, “management” has also become an emerging hotspot since 2018, further suggesting that asthma control and prevention should be carried out in the context of atopic march.
In this study, we searched the core data of WOS based on the search formula and obtained 14,340 literature data of childhood asthma from 2011 to 2021. Bibliometric and scientometric analysis was applied to explore the intellectual landscape and the evolution of trends. A sustained growth in the volume of publications was detected. The regional and institutional distribution network revealed that the USA and European countries were leaders in childhood asthma research, while China, as a developing country, was also emerging in this field. Keywords and cluster analysis showed that research on asthma management and atopy was constantly updated and became the research trends recently. The burst detection algorithm also found a significant shift of hotspots from etiology and diagnosis to atopic march and asthma management. In keywords subgroup analysis for childhood asthma management and atopy, it was found that asthma should be co-studied with other allergic disease while caregiver- or physician-based education should become important directions for improving medication adherence and asthma management.
Our analysis revealed a steady increase in publications in the field of childhood asthma, which was consistent with the rising trend of literatures reviewed by GINA report and other previous studies (56–58). In terms of regional output, the top 10 most prolific countries were almost all dominated by developed countries, which may be related to their advancement in industrialization. However, China, as a developing country, ranked third in terms of the number of publications and showed an increasing trend year by year. Moreover, in China, the prevalence of childhood asthma has raised significantly from 0.91% in 1990 to 2.12% in 2010, at an increasing rate of nearly 50% every 10 years (59). As one of the most populous countries with the fastest socio-economic development in the world, China's urbanization process has undergone unprecedented changes, resulting in dense populations moving into megacities and subsequent environmental challenges, such as air pollution (60). These rapid changes of lifestyle and environment may indirectly accelerate the increase of asthma prevalence and incidence, as explained by the immune system development theory of the hygiene hypothesis (61).
As an outcome of complex gene–environment interactions, asthma is usually triggered by environmental factors such as exposure to allergens. Research has also provided evidence of interactions among and between environmental and other intrinsic factors, such as genetics and atopy (62). As the prevalence of childhood asthma continues to rise, it is becoming a public health problem in both developed and developing countries. Therefore, with regard to subject categories, our study found that childhood asthma was not limited to the research of allergy, immunology and pediatrics, but is also widely studied from perspectives of public, environmental and occupational health, environmental sciences / ecology. Nowadays, activities conducted at the public health scale were incorporated into national guidelines to improve asthma outcomes, including asthma education and self-management training to increase patient adherence, coordination of care across various settings to reduce asthma triggers indoors and outdoors, and institutional reforms to improve quality of care (63–65).
We revealed two emerging trends in academic research on childhood asthma based on the keywords analysis. The first is that keywords such as atopic dermatitis (AD), allergic rhinitis (AR) and allergy appeared more frequently in the analysis results, indicating that the atopic march and asthma's relationship with other allergic diseases have been studied extensively. Epidemiological studies have provided strong evidence for the link between childhood asthma and other allergic diseases. A longitudinal study has found that early-onset AD (onset within first 2 years of life) increase the odds of developing childhood asthma (OR 1.74, 95% CI 1.30–2.34), and the presence of food allergy is also an independent risk factor of asthma (66, 67). This may be explained by the fact that allergic diseases in childhood shared common genetic, epigenetic and environmental risk factors, and their symptoms or underpinning pathogenesis is marked by disrupted skin, lung and gut barriers, altered microbiome and local and systemic Th-2-driven immunological pathways (68). Specifically, studies have shown that the occurrence of asthma, bronchial, rhinitis, history of atopy, pollen allergy, and sensitization to food allergens is significantly higher in AD patients with IgE above 200 IU/ml compared with those who had IgE under 200 IU/ml (69, 70). At the molecular level, various asthma/atopy-related biomarkers from genomes, epigenetics, transcriptomes, and metabolomics have been gradually explored and evaluated for their role in more precise diagnosis and individualized therapy of allergic diseases (56, 71–74). A GWAS study has identified immune-related gene variants (e.g., FLG and GSDMB) shared by asthma, hay fever and AD, suggesting that these allergic diseases may share the same mechanism that leads to dysregulation of immune-related genes (75). Meanwhile, Qi et al. identified replicable DNA methylation sites (e.g., cg20372759 and cg08844313) as prediction biomarkers of asthma and rhinitis (76). For transcriptomes, Kord et al. revealed that miR-1 was the hallmark of allergic airway inflammation, which had the potential therapeutic value by directly inhibiting the eosinophilic response in patients with asthma or rhinitis (77). In addition, after metabolomic analysis of fecal and blood samples, as well as intestinal microbiome measures, Lee-Sarwar et al. found an inverse association of polyunsaturated fatty acids and other lipids with asthma at age of 3 years (78). Although several features of asthma and atopic march have been well recognized, its underlying mechanism remains widely debated. Therefore, more comprehensive and systematic studies of the interplay between genomic, epigenetic, transcriptomic, and metabolomic signatures, as well as their interaction with microbes, are still needed to better understand how AD may progress to asthma (56, 68, 79).
Secondly, asthma management was also considered as an emerging trend in this study, as keywords such as management, prevention, adherence and exacerbation have frequently occurred or showed bursts in more recent studies. Asthma is a chronic disease that is difficult to cure completely; therefore, management plays a pivotal role throughout the disease course, in order to achieve the goal of symptom control, and to minimize future asthma-related deaths, exacerbations, persistent airflow limitation and side-effects of treatments (80). On the other hand, asthma management may be affected by disparities in socioeconomic status and quality of health service, and thus a single universal management might not be suitable for all people (81). Additionally, the 2018 Global Asthma Report noted that many governments have overlooked asthma in their plans when addressing non-communicable diseases and have made little progress in improving access to asthma management (82). Therefore, numerous studies are emerging to explore efficient strategies for asthma management, such as monitoring and assessing the effectiveness and outcomes of asthma management activities at the global and national levels, or exploring personalized disease management interventions at the individual level (81, 82). Eakin et al. improved asthma control and reduced the course of oral corticosteroids therapy and length of hospital stay in children through an intervention that combined family asthma education and a federally funded Head Start program (83). In addition, research has recently been emerging on Internet-based solutions, social media, and mobile technologies to improve asthma self-management in children and to facilitate the delivery of patient care (84–86). Wiecha et al. suggested that a multidimensional web-based educational, monitoring, and communication platform may have a positive impact on improving parental asthma-related knowledge and the use of asthma preventive medications in children (87).
Despite a continuous rise in scholarly activity in childhood asthma, we noticed several gaps in this study and put forward the following recommendations for future research accordingly. First, based on the fact that most of the institutional cooperation is carried out within a country, and the interactions between countries were still lacking, we advocate that academic institutes should strengthen collaborations and links among different countries, especially exchanges between developed and developing countries. Second, keyword analysis suggested that, in addition to these well-established asthma diagnostic techniques based on symptoms, exhaled nitric oxide, lung function, and detection of IgE immunoreactivity against specific allergens, potential biomarkers from multi-omics remain to be discovered to either assist the precise diagnosis/prediction of asthma or facilitate personalized treatment of the disease at the molecular level (74). Third, with the increasing understanding of the atopic march, identifying risk factors for allergic diseases should be considered crucial for early warning of childhood asthma. Moreover, studies are needed to explore the role of age, severity, phenotype heterogeneity, and genetic characteristics to help better understand how AD develops into asthma, and to benefit disease prevention and management ultimately. Forth, pediatric allergy and asthma still face challenges in seeking appropriate care and management currently, so more efforts should be made to improve asthma control, prevent asthma attacks, and reduce asthma burden (7). As reported by CDC of USA, a total of 50.3% of children with current asthma had uncontrolled asthma during 2012–2014, thus, by integrating various medical, behavioral, and psychological theories and research findings, large intervention trials are still required to explore better disease management strategies to improve patients' adherence and prevent asthma exacerbations (88). Lastly, with the current outbreak of coronavirus disease-2019 (COVID-19), questions about the link between childhood asthma and COVID-19 remains unclear. (i.e., does asthma contribute as a risk factor of COVID-19 infection? Are asthma medications protective or detrimental for COVID-19 infection?). Given the limited number of pediatric cases of COVID-19 worldwide, international collaborations are badly needed to illuminate this field.
There are some limitations in this study. First, we only collected data from the Web of Science Core Collection Database when retrieving literatures, while future research could be extended to other databases. Second, our study only extracted data on childhood asthma from 2011 to 2021, and thus we have only reviewed the research trend of childhood asthma over the last decade. Third, due to the software's features and limitations, the information analysis by CiteSpace was not based on the full text, and also the visualization of figures may lack some crucial details.
In conclusion, based on the WOS core database, we adopted the analysis tool CiteSpace and obtained a systematic and comprehensive overview of childhood asthma research from 2011 to 2021, which provided important insights into research priorities, trending themes, and future directions. The number of childhood asthma studies has shown an ascending trend over the past decade. Developed countries and their institutions played a leading role in this research field, while developing countries such as China also actively engaged in this field. Furthermore, the management and prevention of childhood asthma, as well as the pathogenesis of atopic march, were considered two emerging trends recently. We hope this systematic bibliometric analysis will help discuss future research directions, provide effective strategies for interdisciplinary research, as well as promote cross-regional collaborations in childhood asthma studies.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
JW contributed to the data analysis, manuscript writing, review and revising. YY participated in data analysis, manuscript reviewing and revising. XY contributed to reviewing and revising the manuscript. QZ undertook data capture and analysis. QZ, WT and XH provided comments, reviewed and revised the manuscript. CY contributed to the study design, manuscript reviewing and revising. All authors contributed to the article and approved the submitted version.
This study has been funded by the Basic Public Welfare Research Program of Zhejiang Province (LGF22H260004).
The authors thank and express their gratitude to the experts in the fields of pediatrics and statistics, for them providing guidance and advice on childhood asthma and CiteSpace.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fped.2022.1019371/full#supplementary-material.
GINA, Global Initiative for Asthma; AD, atopic dermatitis; FA, food allergy; AR, allergic rhinitis; WOS, Web of Science; SCI-EXPANDED, Social Science Citation Index; SSCI, Social Science Citation Index; AHCI, Arts / Humanities Citation Index; ESCI, Emerging Sources Citations Index; CCR-EXPANDED, Current Chemical Reactions; CI, Index Chemicus; LSI, latent semantic indexing; S, silhouette value; TRAP, traffic-related air pollution; COVID-19, coronavirus disease-2019.
1. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA dissemination committee report. Allergy. (2004) 59(5):469–78. doi: 10.1111/j.1398-9995.2004.00526.x
2. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. (2012) 380(9859):2163–96. doi: 10.1016/S0140-6736(12)61729-2
3. Pearce N, Aït-Khaled N, Beasley R, Mallol J, Keil U, Mitchell E, et al. Worldwide trends in the prevalence of asthma symptoms: phase III of the international study of asthma and allergies in childhood (ISAAC). Thorax. (2007) 62(9):758–66. doi: 10.1136/thx.2006.070169
4. US Department of Health and Human Services C for DC and P. National Hospital Discharge Survey, 1995–2010. https://www.cdc.gov/nchs/nhds/nhds_questionnaires.htm. 2013.
6. Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet. (2018) 391(10122):783–800. doi: 10.1016/S0140-6736(17)33311-1
7. Trikamjee T, Comberiati P, Peter J. Pediatric asthma in developing countries: challenges and future directions. Curr Opin Allergy Clin Immunol. (2022) 22(2):80–5. doi: 10.1097/ACI.0000000000000806
8. Vardavas CI, Hohmann C, Patelarou E, Martinez D, Henderson AJ, Granell R, et al. The independent role of prenatal and postnatal exposure to active and passive smoking on the development of early wheeze in children. Eur Respir J. (2016) 48(1):115–24. doi: 10.1183/13993003.01016-2015
9. Egan KB, Ettinger AS, Bracken MB. Childhood body mass index and subsequent physician-diagnosed asthma: a systematic review and meta-analysis of prospective cohort studies. BMC Pediatr. (2013) 13:121. doi: 10.1186/1471-2431-13-121
10. Ding G, Ji R, Bao Y. Risk and protective factors for the development of childhood asthma. Paediatr Respir Rev. (2015) 16(2):133–9. doi: 10.1016/j.prrv.2014.07.004
11. von Mutius E. The microbial environment and its influence on asthma prevention in early life. J Allergy Clin Immunol. (2016) 137(3):680–9. doi: 10.1016/j.jaci.2015.12.1301
12. Beckhaus AA, Garcia-Marcos L, Forno E, Pacheco-Gonzalez RM, Celedón JC, Castro-Rodriguez JA. Maternal nutrition during pregnancy and risk of asthma, wheeze, and atopic diseases during childhood: a systematic review and meta-analysis. Allergy. (2015) 70(12):1588–604. doi: 10.1111/all.12729
13. Yang H, Xun P, He K. Fish and fish oil intake in relation to risk of asthma: a systematic review and meta-analysis. PLoS One. (2013) 8(11):e80048. doi: 10.1371/journal.pone.0080048
14. Manson ML, Säfholm J, James A, Johnsson A-K, Bergman P, Al-Ameri M, et al. IL-13 and IL-4, but not IL-5 nor IL-17A, induce hyperresponsiveness in isolated human small airways. J Allergy Clin Immunol. (2020) 145(3):808–17. e2. doi: 10.1016/j.jaci.2019.10.037
15. Winkler C, Hochdörfer T, Israelsson E, Hasselberg A, Cavallin A, Thörn K, et al. Activation of group 2 innate lymphoid cells after allergen challenge in asthmatic patients. J Allergy Clin Immunol. (2019) 144(1):61–9.e7. doi: 10.1016/j.jaci.2019.01.027
16. Kim J, Chang Y, Bae B, Sohn K-H, Cho S-H, Chung DH, et al. Innate immune crosstalk in asthmatic airways: innate lymphoid cells coordinate polarization of lung macrophages. J Allergy Clin Immunol. (2019) 143(5):1769–82.e11. doi: 10.1016/j.jaci.2018.10.040
17. Ning F, Takeda K, Schedel M, Domenico J, Joetham A, Gelfand EW. Hypoxia enhances CD8(+) T(C)2 cell-dependent airway hyperresponsiveness and inflammation through hypoxia-inducible factor 1α. J Allergy Clin Immunol. (2019) 143(6):2026–37.e7. doi: 10.1016/j.jaci.2018.11.049
18. Saku A, Hirose K, Ito T, Iwata A, Sato T, Kaji H, et al. Fucosyltransferase 2 induces lung epithelial fucosylation and exacerbates house dust mite-induced airway inflammation. J Allergy Clin Immunol. (2019) 144(3):698–709.e9. doi: 10.1016/j.jaci.2019.05.010
19. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2020. https://ginasthma.org/2020.
20. Biagini Myers JM, Schauberger E, He H, Martin LJ, Kroner J, Hill GM, et al. A pediatric asthma risk score to better predict asthma development in young children. J Allergy Clin Immunol. (2019) 143(5):1803–10.e2. doi: 10.1016/j.jaci.2018.09.037
21. Abdel-Aziz MI, Brinkman P, Vijverberg SJH, Neerincx AH, de Vries R, Dagelet YWF, et al. Enose breath prints as a surrogate biomarker for classifying patients with asthma by atopy. J Allergy Clin Immunol. (2020) 146(5):1045–55. doi: 10.1016/j.jaci.2020.05.038
22. Parulekar AD, Diamant Z, Hanania NA. Role of biologics targeting type 2 airway inflammation in asthma: what have we learned so far? Curr Opin Pulm Med. (2017) 23(1):3–11. doi: 10.1097/MCP.0000000000000343
23. Moreno MA. Atopic diseases in children. JAMA Pediatr. (2016) 170(1):96. doi: 10.1001/jamapediatrics.2015.3886
25. Liu S, Sun YP, Gao XL, Sui Y. Knowledge domain and emerging trends in Alzheimer’s disease: a scientometric review based on CiteSpace analysis. Neural Regen Res. (2019) 14(9):1643–50. doi: 10.4103/1673-5374.255995
26. Wang L, Xue X, Zhang Y, Luo X. Exploring the emerging evolution trends of urban resilience research by scientometric analysis. Int J Environ Res Public Health. (2018) 15(10):2181. doi: 10.3390/ijerph15102181
27. Liu X. Full-text citation analysis : a new method to enhance. J Am Soc Inf Sci Technol. (2013) 64(July):1852–63. Available from: http://onlinelibrary.wiley.com/doi/10.1002/asi.22883/abstract. doi: 10.1002/asi.22883
28. Waqas A, Teoh SH, Lapão LV, Messina LA, Correia JC. Harnessing telemedicine for the provision of health care: bibliometric and scientometric analysis. J Med Internet Res. (2020) 22(10). doi: 10.2196/18835
29. Liang C, Qiao S, Olatosi B, Lyu T, Li X. Emergence and evolution of big data science in HIV research: bibliometric analysis of federally sponsored studies 2000–2019. Int J Med Inform. (2021) 154(July):104558. doi: 10.1016/j.ijmedinf.2021.104558
30. Synnestvedt MB, Chen C, Holmes JH. Citespace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8. PMID: 16779135
31. Bjermer L, Alving K, Diamant Z, Magnussen H, Pavord I, Piacentini G, et al. Current evidence and future research needs for FeNO measurement in respiratory diseases. Respir Med. (2014) 108(6):830–41. doi: 10.1016/j.rmed.2014.02.005
32. Guarnieri M, Balmes JR. Outdoor air pollution and asthma. Lancet. (2014) 383(9928):1581–92. Available from: https://www.sciencedirect.com/science/article/pii/S0140673614606176. doi: 10.1016/S0140-6736(14)60617-6
33. Teo SM, Mok D, Pham K, Kusel M, Serralha M, Troy N, et al. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell Host Microbe. (2015) 17(5):704–15. doi: 10.1016/j.chom.2015.03.008
34. Fitzpatrick AM, Teague WG, Meyers DA, Peters SP, Li X, Li H, et al. Heterogeneity of severe asthma in childhood: confirmation by cluster analysis of children in the national institutes of health/national heart, lung, and blood institute severe asthma research program. J Allergy Clin Immunol. (2011) 127(2):0–20. doi: 10.1016/j.jaci.2010.11.015
35. Petsky HL, Cates CJ, Lasserson TJ, Li AM, Turner C, Kynaston JA, et al. A systematic review and meta-analysis: tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils). Thorax. (2012) 67(3):199–208. doi: 10.1136/thx.2010.135574
36. Pulgarón ER. Childhood obesity: a review of increased risk for physical and psychological comorbidities. Clin Ther. (2013) 35(1):A18–32. doi: 10.1016/j.clinthera.2012.12.014
37. Castro-Rodriguez JA, Forno E, Rodriguez-Martinez CE, Celedón JC. Risk and protective factors for childhood asthma: what is the evidence? J Allergy Clin Immunol Pract. (2016) 4(6):1111–22. doi: 10.1016/j.jaip.2016.05.003
38. Dharmage SC, Lowe AJ, Matheson MC, Burgess JA, Allen KJ, Abramson MJ. Atopic dermatitis and the atopic march revisited. Allergy. (2014) 69(1):17–27. doi: 10.1111/all.12268
39. Jolliffe DA, Greenberg L, Hooper RL, Griffiths CJ, Camargo CAJ, Kerley CP, et al. Vitamin D supplementation to prevent asthma exacerbations: a systematic review and meta-analysis of individual participant data. Lancet Respir Med. (2017) 5(11):881–90. doi: 10.1016/S2213-2600(17)30306-5
40. Lodge CJ, Tan DJ, Lau MXZ, Dai X, Tham R, Lowe AJ, et al. Breastfeeding and asthma and allergies: a systematic review and meta-analysis. Acta Paediatr. (2015) 104(467):38–53. doi: 10.1111/apa.13132
41. Trivedi M, Denton E. Asthma in children and adults-what are the differences and what can they tell US about asthma? Front Pediatr. (2019) 7:256. doi: 10.3389/fped.2019.00256
42. Greer FR, Sicherer SH, Burks AW. The effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, hydrolyzed formulas, and timing of introduction of allergenic complementary foods. Pediatrics. (2019) 143(4):e20190281. doi: 10.1542/peds.2019-0281
43. Gupta RS, Fierstein JL, Boon KL, Kanaley MK, Bozen A, Kan K, et al. Sensor-based electronic monitoring for asthma: a randomized controlled trial. Pediatrics. (2021) 147(1):e20201330. doi: 10.1542/peds.2020-1330
44. Martineau AR, Jolliffe DA, Greenberg L, Aloia JF, Bergman P, Dubnov-Raz G, et al. Vitamin D supplementation to prevent acute respiratory infections: individual participant data meta-analysis. Health Technol Assess. (2019) 23:1–44. doi: 10.3310/hta23020
45. Peters RL, Koplin JJ, Gurrin LC, Dharmage SC, Wake M, Ponsonby A-L, et al. The prevalence of food allergy and other allergic diseases in early childhood in a population-based study: HealthNuts age 4-year follow-up. J Allergy Clin Immunol. (2017) 140(1):145–53.e8. doi: 10.1016/j.jaci.2017.02.019
46. Karimi L, Vijverberg SJ, Engelkes M, Hernandez-Pacheco N, Farzan N, Soares P, et al. ADRB2 Haplotypes and asthma exacerbations in children and young adults: an individual participant data meta-analysis. Clin Exp Allergy. (2021) 51:1157–71. doi: 10.1111/cea.13965
47. Senn S. Childhood asthma exacerbations and ADRB2 polymorphism: caution is needed. J Allergy Clin Immunol . (2018) 141(5):1954–5. doi: 10.1016/j.jaci.2018.01.023
48. Cousino MK, Hazen RA. Parenting stress among caregivers of children with chronic illness: a systematic review. J Pediatr Psychol. (2013) 38(8):809–28. doi: 10.1093/jpepsy/jst049
49. Oland AA, Booster GD, Bender BG. Psychological and lifestyle risk factors for asthma exacerbations and morbidity in children. World Allergy Organ J. (2017) 10(1):1–7. doi: 10.1186/s40413-017-0169-9
50. Bellin MH, Land C, Newsome A, Kub J, Mudd SS, Bollinger ME, et al. Caregiver perception of asthma management of children in the context of poverty. J Asthma. (2017) 54(2):162–72. doi: 10.1080/02770903.2016.1198375
51. Riekert KA, Borrelli B, Bilderback A, Cynthia S. American Adolescents with asthma. Patient Educ Couns. (2011) 82(1):117–22. doi: 10.1016/j.pec.2010.03.005
52. Sleath B, Gratie D, Carpenter D, Davis SA, Lee C, Loughlin CE, et al. Reported problems and adherence in using asthma medications among adolescents and their caregivers. Ann Pharmacother. (2018) 52(9):855–61. doi: 10.1177/1060028018766603
53. Triasih R, Duke T RC. Outcomes following admission to intensive care for asthma. Arch Dis Child. (2011) 96(8):729–38. doi: 10.1136/adc.2010.205062
54. Gupta RS, Weiss KB. The 2007 national asthma education and prevention program asthma guidelines: accelerating their implementation and facilitating their impact on children with asthma. Pediatrics. (2009) 123(SUPPL. 3):S193–8. doi: 10.1542/peds.2008-2233J
55. Savenije OE, Granell R, Caudri D, Koppelman GH, Smit HA, Wijga A, et al. Comparison of childhood wheezing phenotypes in 2 birth cohorts: ALSPAC and PIAMA. J Allergy Clin Immunol. (2011) 127(6):1505–12.e14. doi: 10.1016/j.jaci.2011.02.002
56. Miller RL, Grayson MH, Strothman K. Advances in asthma: new understandings of asthma’s natural history, risk factors, underlying mechanisms, and clinical management. J Allergy Clin Immunol. (2021) 148(6):1430–41. doi: 10.1016/j.jaci.2021.10.001
57. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2011. https://ginasthma.org/2011.
58. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2021. https://ginasthma.org/2021.
59. Li X, Song P, Zhu Y, Lei H, Chan KY, Campbell H, et al. The disease burden of childhood asthma in China: a systematic review and meta-analysis. J Glob Health. (2020) 10(1):10801. doi: 10.7189/jogh.10.010801
60. Brusselle GG, Ko FW-S. Prevalence and burden of asthma in China: time to act. Lancet. (2019) 394(10196):364–6. doi: 10.1016/S0140-6736(19)31349-2
61. Okada H, Kuhn C, Feillet H, Bach J-F. The “hygiene hypothesis” for autoimmune and allergic diseases: an update. Clin Exp Immunol. (2010) 160(1):1–9. doi: 10.1111/j.1365-2249.2010.04139.x
62. Dharmage SC, Perret JL, Custovic A. Epidemiology of asthma in children and adults. Front Pediatr. (2019) 7:246. doi: 10.3389/fped.2019.00246
63. Bousquet J, Bousquet PJ, Godard P, Daures J-P. The public health implications of asthma. Bull World Health Organ. (2005) 83(7):548–54. https://www.scielosp.org/article/bwho/2005.v83n7/548-554/en/16175830
64. Michel FB, Neukirch F, Bousquet J. Asthma: a world problem of public health. Bull Acad Natl Med. (1995) 179(2):277–9. PMID: 7614059
65. Labre MP, Herman EJ, Dumitru GG, Valenzuela KA, Cechman CL. Public health interventions for asthma: an umbrella review, 1990-2010. Am J Prev Med. (2012) 42(4):403–10. doi: 10.1016/j.amepre.2011.11.016
66. Burgess JA, Dharmage SC, Byrnes GB, Matheson MC, Gurrin LC, Wharton CL, et al. Childhood eczema and asthma incidence and persistence: a cohort study from childhood to middle age. J Allergy Clin Immunol. (2008) 122(2):280–5. doi: 10.1016/j.jaci.2008.05.018
67. Alduraywish SA, Lodge CJ, Campbell B, Allen KJ, Erbas B, Lowe AJ, et al. The march from early life food sensitization to allergic disease: a systematic review and meta-analyses of birth cohort studies. Allergy. (2016) 71(1):77–89. doi: 10.1111/all.12784
69. Čelakovská J, Ettlerová K, Ettler K, Bukač J. Food allergy, asthma bronchiale, and rhinitis in atopic dermatitis patients with total immunoglobulin E under and above 200 IU/ml. Food Agric Immunol. (2015) 26(5):671–81. doi: 10.1080/09540105.2015.1007447
70. Čelakovská J, Bukač J. Food allergy in patients suffering from atopic dermatitis – association with concomitant allergic diseases. Food Agric Immunol. (2015) 26(3):325–39. doi: 10.1080/09540105.2014.914470
71. Hallmark B, Wegienka G, Havstad S, Billheimer D, Ownby D, Mendonca EA, et al. Chromosome 17q12-21 variants are associated with multiple wheezing phenotypes in childhood. Am J Respir Crit Care Med. (2021) 203(7):864–70. doi: 10.1164/rccm.202003-0820OC
72. Ober C, McKennan CG, Magnaye KM, Altman MC, Washington C, Stanhope C, et al. Expression quantitative trait locus fine mapping of the 17q12–21 asthma locus in African American children: a genetic association and gene expression study. Lancet Respir Med. (2020) 8(5):482–92. doi: 10.1016/S2213-2600(20)30011-4
73. Papamichael MM, Katsardis C, Sarandi E, Georgaki S, Frima ES, Varvarigou A, et al. Application of metabolomics in pediatric asthma: prediction, diagnosis and personalized treatment. Metabolites. (2021) 11(4):251. doi: 10.3390/metabo11040251
74. Breiteneder H, Peng YQ, Agache I, Diamant Z, Eiwegger T, Fokkens WJ, et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy Eur J Allergy Clin Immunol. (2020) 75(12):3039–68. doi: 10.1111/all.14582
75. Ferreira MA, Vonk JM, Baurecht H, Marenholz I, Tian C, Hoffman JD, et al. Shared genetic origin of asthma, hay fever and eczema elucidates allergic disease biology. Nat Genet. (2017) 49(12):1752–7. doi: 10.1038/ng.3985
76. Qi C, Jiang Y, Yang I V, Forno E, Wang T, Vonk JM, et al. Nasal DNA methylation profiling of asthma and rhinitis. J Allergy Clin Immunol. (2020) 145(6):1655–63. doi: 10.1016/j.jaci.2019.12.911
77. Korde A, Ahangari F, Haslip M, Zhang X, Liu Q, Cohn L, et al. An endothelial microRNA-1–regulated network controls eosinophil trafficking in asthma and chronic rhinosinusitis. J Allergy Clin Immunol. (2020) 145(2):550–62. doi: 10.1016/j.jaci.2019.10.031
78. Lee-Sarwar KA, Kelly RS, Lasky-Su J, Zeiger RS, O’Connor GT, Sandel MT, et al. Integrative analysis of the intestinal metabolome of childhood asthma. J Allergy Clin Immunol. (2019) 144(2):442–54. doi: 10.1016/j.jaci.2019.02.032
79. Aw M, Penn J, Gauvreau GM, Lima H, Sehmi R. Atopic march: collegium internationale allergologicum update 2020. Int Arch Allergy Immunol. (2020) 181(1):1–10. doi: 10.1159/000502958
80. Stoodley I, Williams L, Thompson C, Scott H, Wood L. Evidence for lifestyle interventions in asthma. Breathe. (2019) 15(2):e50–61. doi: 10.1183/20734735.0019-2019
81. Lancet T. Asthma - hope for the future? Lancet. (2015) 386(9998):1014. doi: 10.1016/S0140-6736(15)00192-0
83. Eakin MN, Zaeh S, Eckmann T, Ruvalcaba E, Rand CS, Hilliard ME, et al. Effectiveness of a home- and school-based asthma educational program for head start children with asthma: a randomized clinical trial. JAMA Pediatr. (2020) 174(12):1191–8. doi: 10.1001/jamapediatrics.2020.3375
84. Roberts CA, Geryk LL, Sage AJ, Sleath BL, Tate DF, Carpenter DM. Adolescent, caregiver, and friend preferences for integrating social support and communication features into an asthma self-management app. J Asthma. (2016) 53(9):948–54. doi: 10.3109/02770903.2016.1171339
85. Al-Durra M, Torio M-B, Cafazzo JA. The use of behavior change theory in Internet-based asthma self-management interventions: a systematic review. J Med Internet Res. (2015) 17(4):e89. doi: 10.2196/jmir.4110
86. Kosse RC, Bouvy ML, de Vries TW, Kaptein AA, Geers HC, van Dijk L, et al. Mhealth intervention to support asthma self-management in adolescents: the ADAPT study. Patient Prefer Adherence. (2017) 11:571–7. doi: 10.2147/PPA.S124615
Keywords: childhood asthma, citespace, bibliometrics analysis, scientometric analysis, atopic march, asthma management
Citation: Wu J, Yu Y, Yao X, Zhang Q, Zhou Q, Tang W, Huang X and Ye C (2022) Visualizing the knowledge domains and research trends of childhood asthma: A scientometric analysis with CiteSpace. Front. Pediatr. 10:1019371. doi: 10.3389/fped.2022.1019371
Received: 15 August 2022; Accepted: 15 September 2022;
Published: 30 September 2022.
Edited by:
Kostas N. Priftis, National and Kapodistrian University of Athens, GreeceReviewed by:
Jarmila Celakovska, Charles University, Czechia© 2022 Wu, Yu, Yao, Zhang, Zhou, Tang, Huang and Ye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chengyin Ye eWVjaGVuZ3lpbkBoem51LmVkdS5jbg==
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Pediatric Immunology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.