 Libny Martínez-Valdez
Libny Martínez-Valdez Vesta Richardson*
Vesta Richardson*- Dirección de Prestaciones Económicas y Sociales, El Instituto Mexicano del Seguro Social, Mexico City, Mexico
Background: Sudden Infant Death Syndrome (SIDS) constitutes one of the main causes of mortality in children under one year of age in developed countries; it's frequency to varies geographically. In Mexico the real incidence of SIDS is not known.
Methods: National databases of deaths in children under one year of age, from 2005 to 2020, were analyzed, due to Sudden Unexpected Infant Death (SUID) [SIDS (R95), accidental suffocation in a sleeping environment (W75), and other ill-defined and unspecified causes of mortality (R99), according to the International Classification of Diseases, tenth revision (ICD 10)]. Mortality rates per year of occurrence due to SUID and their subcategories were calculated. Simple frequencies of SIDS were obtained per year and month of occurrence, state of residence, age, place of death, and access to social security services.
Results: In the study period 473,545 infant deaths occurred; 7,714 (1.62%) deaths were due to SUID; of these, 6,489 (84%) were due to SIDS, which is among the 10 leading causes of infant death in Mexico. The average mortality rate for SUID was 22.4/100,000 live births, for SIDS was 18.8/100,000 live births. Mortality rates within the states were variable, ranging from 2.4/100,000 to 105.1/100,000 live births. In 81% of SIDS records there was no autopsy; 38% of deaths due to SIDS occurred in infants under one month of age, up to 87% of deaths occurred in families without social security services or it was unknown, and 76.2% of deaths occurred at home. Deaths were more frequent during the last months of autumn and during winter.
Conclusion: In Mexico there is an underregistry of SIDS as cause of death, along with other SUID categories. Health workers need to be trained to improve diagnosis and data registration, including the practice of autopsies; additionally, it is necessary to implement a public health campaign.
Introduction
SIDS is defined as “the sudden unexpected death of an infant younger than one year of age, with onset of the fatal episode apparently occurring during sleep, that remains unexplained after a thorough investigation, including performance of a complete autopsy and review of the circumstances of death and the clinical history” (1–10).
SIDS must be considered a specific subcategory of Sudden Unexpected Infant Death (SUID) (11). In the last several years, the Centers for Disease Control in the US (CDC) suggested that SUID should be used as a broad term that encompasses all sudden infant deaths (12) whether explained or unexplained, which occur during the first year of life (2, 3, 13), including Sudden Infant Death Syndrome (SIDS), accidental suffocation in a sleeping environment (ASSB), and other deaths from unknown causes (14–16).
Therefore, for any SUID, when the cause of death after case investigation is not attributed to any explained cause such as suffocation, asphyxia, infection or metabolic diseases, the case must be classified as SIDS, which is an ultimate diagnosis reached by exclusion (15).
In developed countries, SIDS is the most common cause of death between 30 days and 12 months of life (4, 17) and represents 40%–50% of deaths in this age group (17).
Multiple studies have described the risk factors for SIDS, which are shown in Table 1.
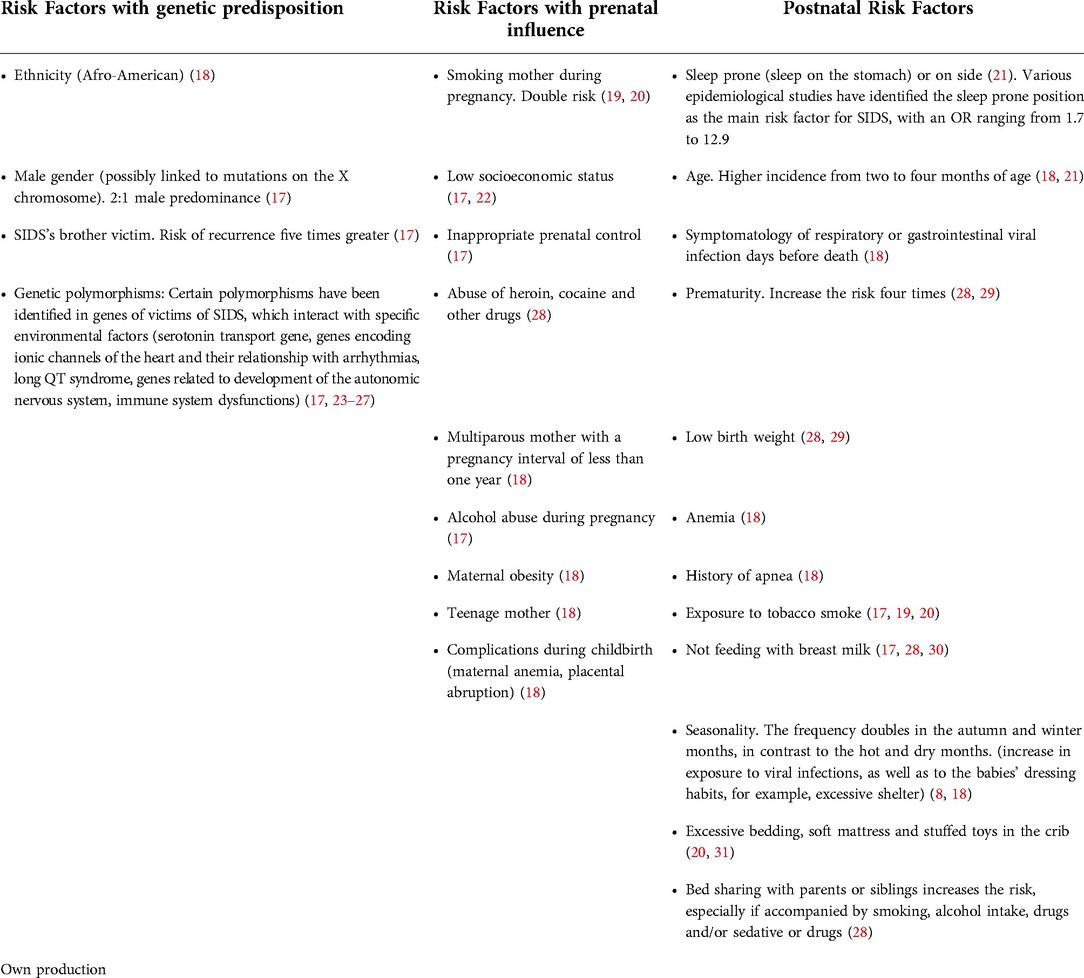
Table 1. Risk factors for SIDS.
Public health campaigns with simple and low-cost recommendations, such as supine position for sleeping, have been established since the 1980s worldwide and have shown to significantly reduce mortality. SIDS incidence has been significantly reduced after these campaigns (4–6, 13, 17, 20, 30, 32–34) in several developed and developing countries, as shown in Table 2.
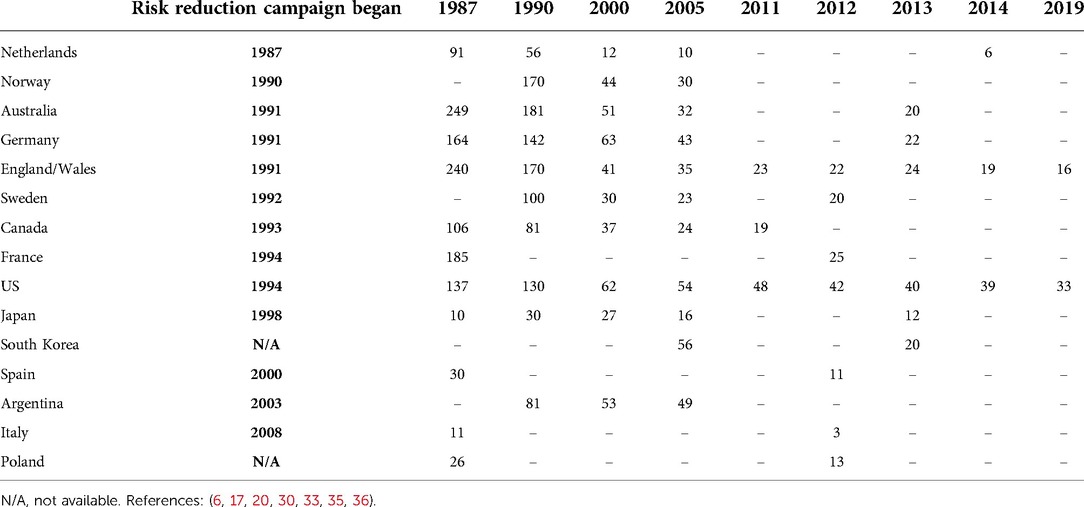
Table 2. Mortality rates due SIDS (deaths/100,000 births) by year.
A study analyzed mortality rates trends from 2005 to 2015 due to SUID, SIDS, unknown/unattended/unspecified cause and accidental threats to breathing in 14 western European countries; the total rate of SUID was estimated at 34.9 per 100,000 live births, ranging from 12 to 76.4 among countries; Austria, Finland, France, Germany, Italy, the Netherlands, Norway, Spain and the United Kingdom reduced their mortality rates from this cause and mortality rates due to SIDS also decreased, however mortality rates due to unknown/unattended/unspecified causes increased (34). This also has been documented in the US, SUID rates declined from 154.6 per 100,000 live births in 1990 to 90.1 in 2019; SIDS rates also declined from 130.2 in 1990 to 33.3 in 2019 (16), although SIDS mortality rates declined, ASSB mortality rates increased; researchers have hypothesized that the continued decline may be due to changes in reporting or better diagnostic practices (37–39).
In Mexico, the real incidence of SIDS is not known; it is not considered a public health problem, there are very few specific preventive programs and no public health campaigns to reduce this cause of death, which may be related to the fact that there is under-registration of the number of cases or misdiagnosis (21). SIDS implies ruling out other possible causes of death, so there must be a precise diagnostic protocol (4) which in most cases is not practiced. In Mexico when a death occurs outside the hospital, the forensic service determines the causes of death and issues the certificate, the statistics area encodes and reports to the “civil registry”, which concentrates the information and notifies to the health jurisdiction, where experts review the certificates to request rectification or ratification as applicable, to the ones who emitted the certificate. The forensic, civil registry and health jurisdiction areas notify their State parties to validate or rectify the death certificate, later the process is repeated in the central offices at the national level with the same purpose, to finally publish the data.
Current guidelines recommend molecular autopsy in cases without a conclusive cause of death, especially in infants. In these situations, cardiac arrhythmia of genetic origin is suspected as the most plausible cause of death (23, 24, 27, 40). It is important to carefully study the clinical history of the victim and the circumstances of his death, because in case of negative autopsy, the pathologist can promptly collect fresh blood and samples of tissues for genetic testing (41).
Mexico's health system is composed of two sectors: public (90% of the population) and private (10% of the population). Health services can be offered as part of social security services by Institutions such as the Mexican Social Security Institute (IMSS for its name in Spanish), Institute of Social Security and Services for State Workers (ISSSTE for its name in Spanish), Petróleos Mexicanos (PEMEX), Ministry of National Defense (SEDENA for its name in Spanish), Ministry of Marine (SEMAR for its name in Spanish), which provide services to workers in the formal sector of the economy; and the Ministry of Health (including the extinct Seguro Popular), institution that provides medical services to the poorest population without access to social security services. In 2020, 73.4% of the population had access to public health services (42).
The aim of this study is to estimate the mortality rate due to SIDS in Mexico and its epidemiological characteristics, in order to understand the magnitude of SIDS as a public health problem and prioritize preventive interventions.
Materials and methods
This is a retrospective population-based study which includes data related to infant deaths and births occurred in Mexico between 2005 and 2020. Births from 2008 to 2020 and all deaths were obtained from databases of the National General Office for Health Information (DGIS for its name in Spanish), of the Ministry of Health (43, 44). Births from 2005 to 2007 were obtained from databases of the National Institute of Statistics and Geography (INEGI for its name in Spanish) (45).
Outcome measures were the total number of deaths that occurred in infants younger than one year of age and the number of deaths due to SUID, including R95, Sudden infant death syndrome (before 2014); R950, Sudden infant death syndrome with mention of autopsy; R959, Sudden infant death syndrome without mention of autopsy; R99, Other ill-defined and unspecified causes of mortality; W75, Accidental suffocation and strangulation in bed (ASSB), including suffocation and strangulation due to bed linen, mother's body and pillow (occurred at house, residential institution, school, another place, place not specified); according to the International Classification of Diseases, tenth revision (ICD 10) version 2019.
Main causes of death in children under one year of age between 2005 and 2020 were identified, to understand the characteristics and factors associated with SIDS over time.
Simple frequencies of deaths and mortality rates due to SUID [SIDS, accidental suffocation in a sleeping environment (ASSB), and other ill-defined and unspecified causes of mortality] were calculated according to year of occurrence. Mortality rates were calculated using the number of deaths due to SUID as numerator and the number of live births as denominator.
Simple frequencies of deaths due to SIDS were obtained per year of occurrence, by age in months, sex, necropsy record, place where death occurred, state of residence and type of health system that provided care. Also, mortality rates per 100,000 live births were calculated by year at national level, and the average mortality rates through 2005–2020 were calculated for each of the thirty-two states of Mexico, using the number of deaths due to SIDS as numerator and the number of live births as denominator.
The number of deaths due to SIDS per month from 2005 to 2020 were plotted to identify if there was any temporal pattern in the occurrence of these deaths.
Results
From 2005 to 2020, 473,545 infant deaths were recorded in Mexico; 7,714 (1.62%) deaths were due to SUID; of these, 6,489 (84%) were due to SIDS (an average of 405 deaths per year), 1,134 (14.7%) were due to other ill-defined and unspecified causes of mortality (R99), and 91 (1.17%) were due to ASSB (W75). The average mortality rates for the study period were: for SUID 22.4/100,000 live births, for SIDS 18.8/100,000 live births, for other ill-defined and unspecified causes of mortality 3.3/100,000 live births, and for accidental suffocation and strangulation in bed 0.3/100,000 live births (Figure 1).
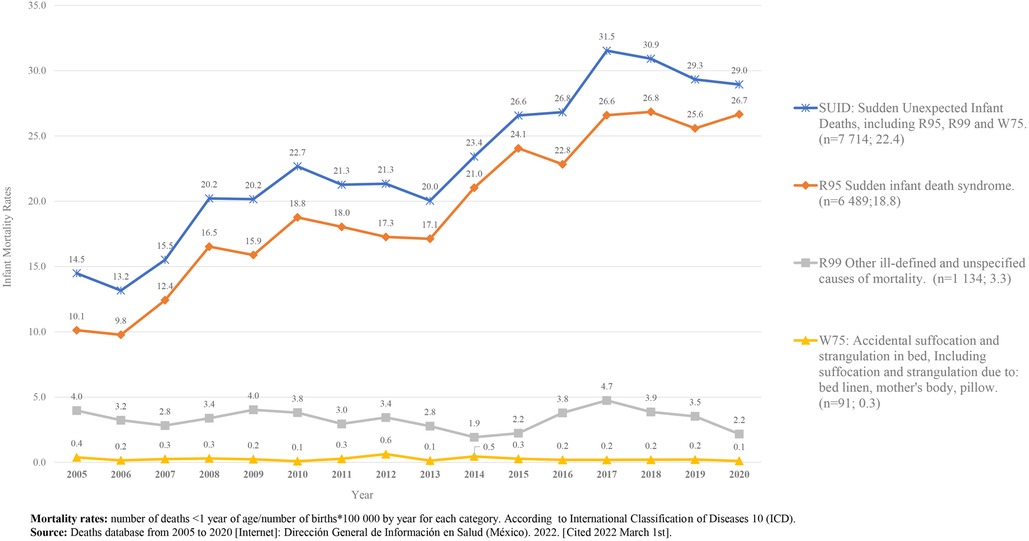
Figure 1. Infant mortality rates due to SUID. 2005–2020. México [Graph].
In Mexico, in 2005, SIDS was in the twenty fifth cause of death in children under one year of age and in 2020, it was the seventh cause of death (Figure 2).
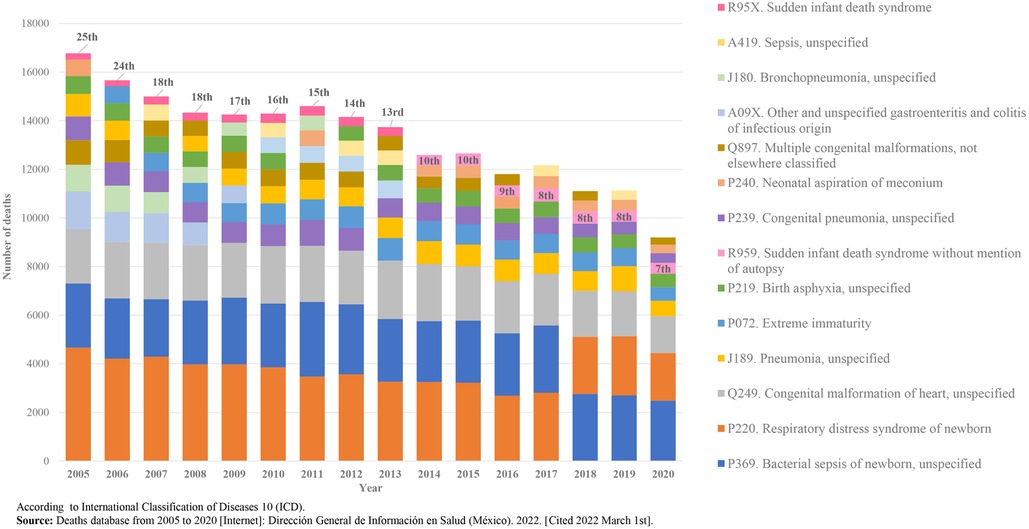
Figure 2. SIDS’ position as leading cause of death in children under one year of age, 2005–2020. Mexico. [Graph].
We found that 5,255 (81%) SIDS cases did not have an autopsy recorded, in 883 (14%) this information was not specified and in 351 (5%) an autopsy was performed; of these cases, 212 (60%) were males, and 117 (33%) occurred in infants less than one month of age.
In relation to gender, 58% of deaths due to SIDS during the study period occurred in males.
The national average mortality rates due SIDS during the period shows that the trend goes up, with the highest national mortality rate, registered in 2018 (26.8 deaths/100,000 live births) Figure 3.
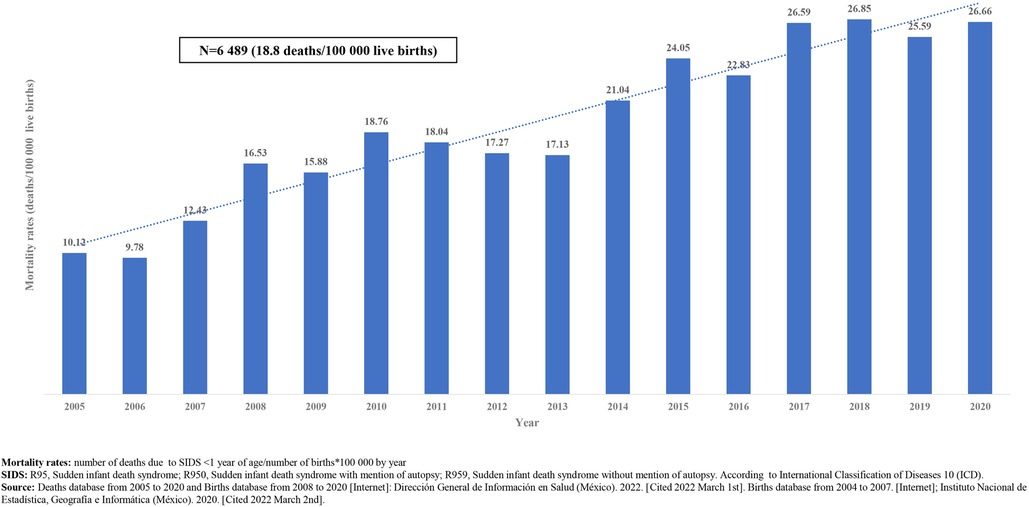
Figure 3. Mortality rates (deaths/100,000 live births) due to SIDS, 2005–2020. Mexico. [Graph].
When analyzing data by state of residence, we found that there is high variability in the average mortality rate for the analyzed period, ranging from 2.4 deaths/100,000 live births in Colima (in the occidental coast of Mexico) to 105.1 deaths/100,000 live births in Chihuahua (in the north of Mexico). Additionally, we found that nine states have mortality rates higher than the national average mortality rate for the period, as shown in Figure 4. The trend of mortality rates due to SIDS in 29 states (91%) goes up and in three states (9%) the trend goes down (Chihuahua, México City and Querétaro).
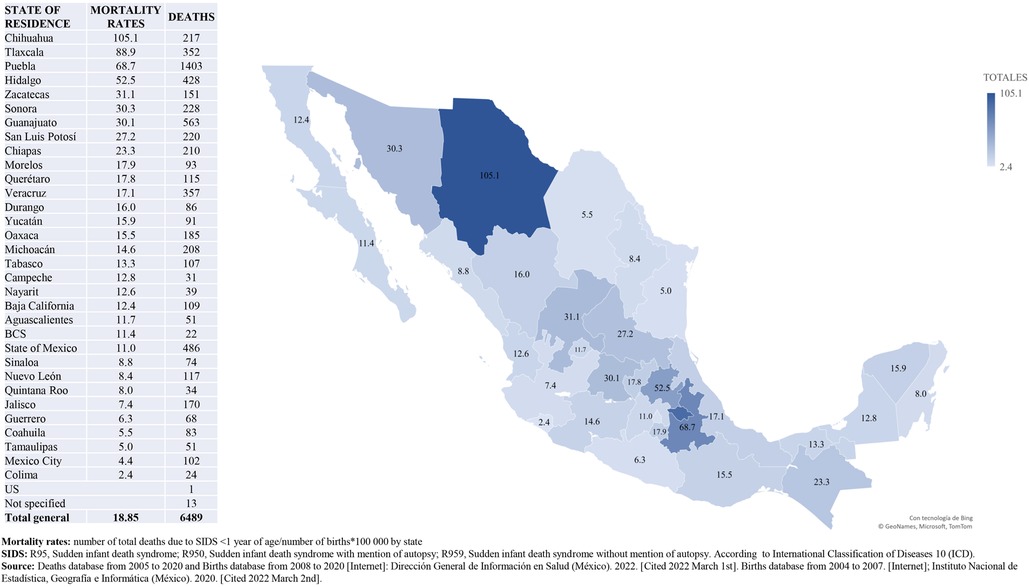
Figure 4. Mortality rates (deaths/100,000 live births) due to SIDS. State of residence, Mexico. 2005–2020 [Graph].
Of all deaths due to SIDS (6,489) during the study period, 2,452 (38%) occurred in infants under one month of age, 4,805 (74%) in infants less three months of age and 6,190 (95%) occurred during the first 6 months of life. Figure 5 shows distribution of deaths by age of occurrence pear year.
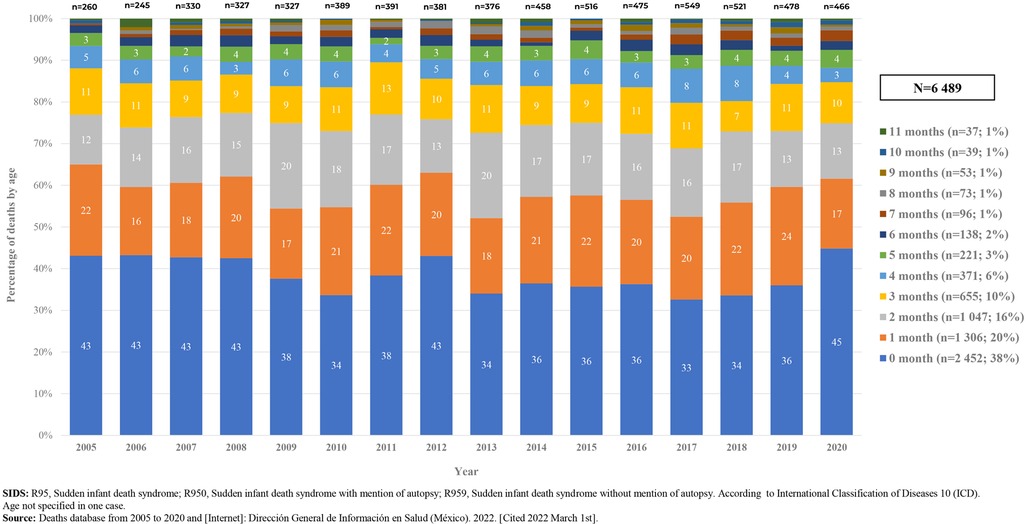
Figure 5. Deaths due to SIDS, by age, 2005–2020. Mexico. [Graph].
As can be observed in Figure 6, deaths due to SIDS in Mexico, occurred throughout the year; however, most deaths happened from september/october to february/march; with a peak in december or january, with an average of 59–55 deaths in these months, respectively. The highest frequency was recorded in december 2017, with 95 deaths.
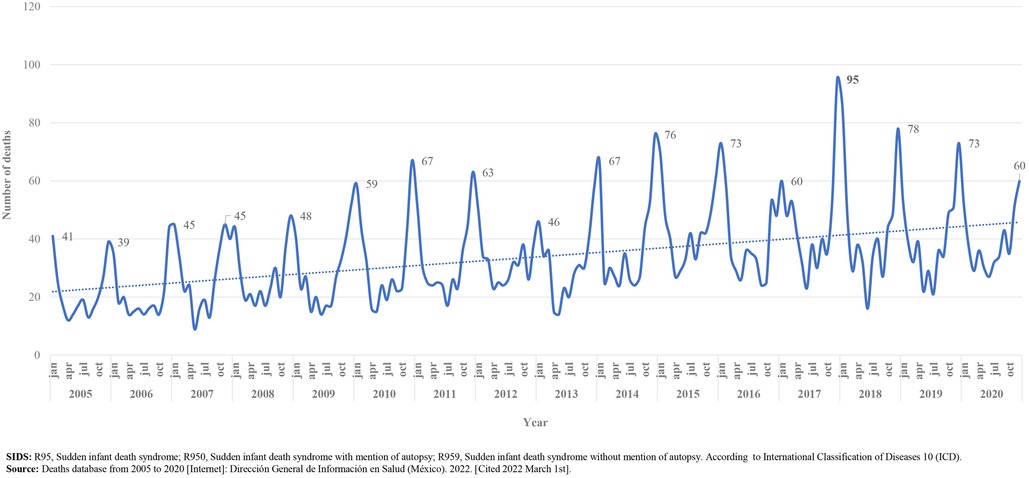
Figure 6. Deaths due to SIDS, monthly variation, 2005–2020. Mexico. [Graph].
We also found that in the analyzed period (2005–2020), 4,948 (76.2%) of deaths due to SIDS occurred at home; 1,031(15.8%) occurred in a medical unit (public or private); 434 (6.6%) occurred in an unspecified place, and 76 (1.1%) occurred on public roads. 4,415 (68%) of deaths due to SIDS occurred in infants without social security services; 1,233 (19%) of deaths occurred in infants whose social security status was not specified or unknown; and 841 (13%) deaths occurred in social security Institutions (IMSS, ISSSTE, PEMEX, SEDENA, SEMAR) Figure 7.
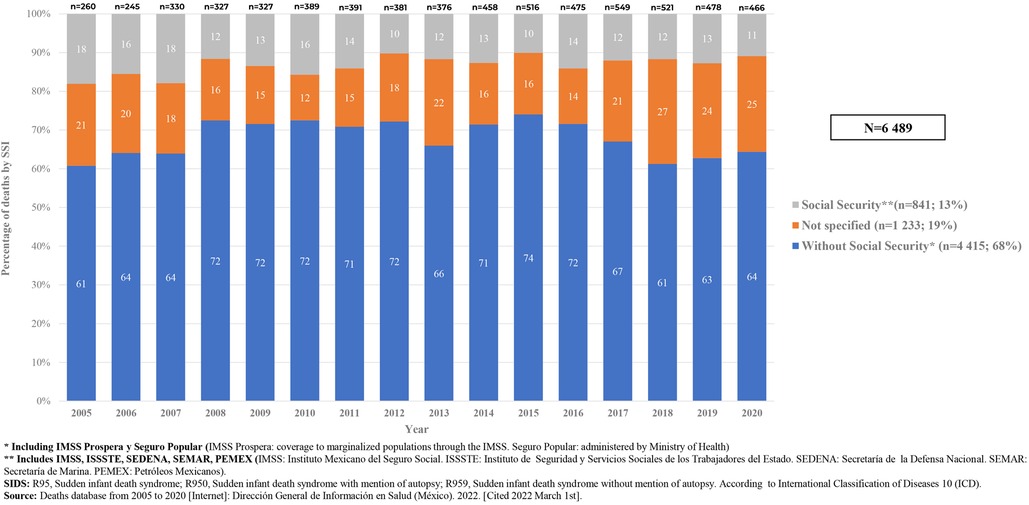
Figure 7. Deaths due to SIDS, by access to social security services, 2005–2020, Mexico. [Graph].
Discussion
In contrast to what has been seen in various countries where SIDS preventive campaigns have been implemented, in Mexico SIDS mortality rates have increased over time, and other diagnoses considered as part of SUID remain low and stable (Figure 1).
In Mexico, from 1998 to 2002, an average of 245 cases of SIDS/year (9 deaths/100,000 live births) were registered (21). From 2000 to 2011, the estimated average mortality rate was 13/100,000 live births (46). In our analysis, the estimated average mortality rate for the 2005 to 2020 period was 18/100,000 live births (Figure 3).
This increase in mortality rates may be due to excessive diagnosis without an exhaustive investigation of the underlying cause of death, including the analysis of the circumstances in which the death occurred, and the lack of an autopsy in the majority of cases. In addition, this may be due to inadequate training of forensic and medical staff and scarcity of human and economic resources (9, 10).
The fact that mortality rates due to SIDS in Mexico are much lower than those in the US and other developed countries (Table 2), suggests that there is still significant underregistry, underdiagnosis or misdiagnosis. Further research is needed to determine if race/ethnicity/genetic factors have a strong influence in the lower mortality rates, or if these are mainly related to prenatal and postnatal risk factors (Table 1).
In a European study, SUID was one of the five main infant causes of death, after those classified as “certain conditions originating in the perinatal period” and “congenital malformations or chromosomal abnormalities” (34). SIDS was the third leading cause of infant mortality in the US in 2020, after those classified as Congenital Anomalies and Short Gestation (47).
Another study compared the rates of SUID in several countries from 2002 to 2010 and found wide variability in how each country codes SUID, for example, the proportion of SUIDs coded as Sudden Infant Death Syndrome (R95) ranged from 32.6% in Japan to 72.5% in Germany (48). More recently, in European countries from 2005 to 2015, it ranges from 13.2% in Denmark to 67.7% in Belgium (34), while in our country SIDS represents 84.9% of the total SUID during the study period.
Since 2014, SIDS codification in Mexico includes the variable “with or without mention of autopsy”, and as shown in Figure 2, since 2014 SIDS has appeared within the ten main causes of death; this may be due to the substantial reduction in the number of deaths caused by gastrointestinal and respiratory disorders, infectious diseases, necrotizing enterocolitis and certain congenital malformations. More frequent than SIDS as causes of infant death in Mexico are congenital heart malformations, non-infectious respiratory disorders (respiratory distress syndrome of the newborn), birth asphyxia, newborn bacterial sepsis, unspecified pneumonia and disorders related to extreme immaturity.
We found high mortality rates due to SIDS in states of Mexico located at the north and centre of the country (Figure 4), states where during the winter season, the temperature is very cold. Additionally, as has been described in previous reports (3), we found that deaths have a specific temporal pattern: deaths accumulate during the last months of autumn and during the winter, with higher peaks in December and January (Figure 6). These two findings (geographic and seasonal distribution) are directly related to cold weather, season in which excessive clothing and/or bedding are used, and respiratory infections are more common, factors related with deaths due to ASSB or infection (38).
In our analysis, deaths due SIDS are more frequent in males, as described in other series (35).
It has been described that the most vulnerable period to die due to SIDS is within the first six months of age or before infants can roll over on their own (7). In our study, 95% of deaths classified as SIDS occurred in this period, as reported previously in countries such as Denmark, UK, Canada, US and Sweden (80%–90%) (3, 6, 21); nevertheless, we found that 38% of deaths due to SIDS occurred in infants under one month of age. In several reports' incidence of SIDS peaks between 2 and 4 months of age (5, 8, 21, 35). In our series, 58% of cases occurred during the first two months of age and as age progresses, the incidence decreased (Figure 5).
This analysis also shows that in Mexico, for the studied period, 76.2% of deaths due SIDS occurred at home and up to 87% occurred in families without social security services or where their social security status was not known (Figure 7). This fact is directly related to the socioeconomic status of families and formal jobs, and probably most of these deaths occurred among poor families (22, 49).
The loss of an apparently healthy baby is a catastrophic event for any family, disconcerting for a doctor and a challenge for the forensic expert or pathologist in charge of proving the cause of death (50), as well as for the person responsible for the categorization.
Conclusion
SIDS in Mexico must be recognized as a public health problem that could be prevented with simple and non-expensive measures (19, 28–31, 51–54), as it has shifted to occupy one of the most common causes of infant death and mortality rates have doubled since 2005.
Our analysis suggests that in Mexico is an inaccurate classification of SIDS as cause of death, along with underregistry of other SUID categories, which makes it very difficult to estimate the real magnitude of these problems. Health workers need to be trained in SUID and SIDS definitions to improve diagnosis, coding and registry. Also the practice of autopsies according to specific protocols and consistency in application of an international classification system, is necessary.
Analysis of factors associated with deaths and the relationship with infant care practices in the general population are also needed for the development of more effective and appropriate public health campaigns, aimed to reach parents and caregivers within homes and childcare centers especially in children with known risk factors (55).
Data availability statement
Publicly accessible dataset were analyzed in this study. These can be found in Cubos dinámicos, Dirección General de Información en Salud. Available from: http://dgis.salud.gob.mx/contenidos/basesdedatos/BD_Cubos_gobmx.html
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
LMV contributed with data collection, analysis and with manuscript writing. ABM contributed with manuscript writing and review. VR contributed with manuscript writing, review and supervision of the research. MHA contributed with supervision of the research. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mitchell EA, Krous HF. Sudden unexpected death in infancy: a historical perspective. J Paediatr Child Health. (2015) 51:108–12. doi: 10.1111/jpc.12818
2. Chapur VF, Alfaro EL, Bronberg R, Dipierri JE. Epidemiology of sudden unexpected death in infancy in Argentina: secular trend and spatial variation. Arch Argent Pediatr. (2019) 117(3):164–70. doi: 10.5546/aap.2019.eng.164
3. Möllborg P. Sudden infant death syndrome—epidemiology and environmental factors Prevention is still a challenge. [Dissertation]. Gothenburg, Sweden: Department of Pediatrics Institute of Clinical Sciences at Sahlgrenska Academy University of Gothenburg. (2016). 120 p [Cited Nov 2019]. Available from: http://hdl.handle.net/2077/41249
4. Brockmann PE, Oyarzún MA, Villarroel L, Bertrand P. Síndrome de muerte súbita del lactante: prevalencia y cambios en los últimos años en Chile. Rev méd Chile. (2013) [Cited 2022 Apr 07] 141(5):589–94. doi: 10.4067/S0034-98872013000500006
5. Goldberg N, Rodriguez-Prado Y, Tillery R, Chua C. Sudden infant death syndrome: a review. Pediatr Ann. (2018) 47(3):e118–23. doi: 10.3928/19382359-20180221-03
6. de Luca F, Hinde A. Effectiveness of the “back-to-sleep” campaigns among healthcare professionals in the past 20 years: a systematic review. BMJ Open. (2016) 6:e011435. doi: 10.1136/bmjopen-2016-011435
7. Buchanan GF. Impaired CO2-induced arousal in SIDS and SUDEP. Trends Neurosci. (2019) 42(4):242–50. doi: 10.1016/j.tins.2019.02.002
8. Goldwater PN. The science (or nonscience) of research into sudden infant death syndrome (SIDS). Front Pediatr. (2022) 10:865051. doi: 10.3389/fped.2022.865051
9. Sawaguchi T, Fujita T, Sawaguchi A, Nishida H. The epidemiological study on registered cases of sudden infant death syndrome (SIDS) in Tokyo: examination of the effect of autopsy on diagnosis of SIDS and the mortality statistics in Japan. Forensic Sci Int. (2000) 109(1):65–74. doi: 10.1016/S0379-0738(99)00218-2
10. Rizzo S, De Gaspari M, Carturan E, Paradiso B, Favretto D, Thiene G, et al. A standardized postmortem protocol to assess the real burden of sudden infant death syndrome. Virchows Arch. (2020) 477:177–83. doi: 10.1007/s00428-020-02747-2
11. Shapiro-Mendoza CK, Palusci VJ, Hoffman B, Batra E, Yester M, Corey TS, et al. Task force on sudden infant death syndrome, council on child abuse and neglect, council on injury, violence, and poison prevention, section on child death review and prevention, national association of medical examiners. Half century since SIDS: a reappraisal of terminology. Pediatrics. (2021) 148(4):e2021053746. doi: 10.1542/peds.2021-053746
12. Centers for Disease Control and Prevention. Sudden unexpected infant death and sudden infant death syndrome. About SUID and SIDS. Atlanta Georgia, United States: CDC (2021) [cited 2022 Apr 8]. Available from: https://www.cdc.gov/sids/about/index.htm.
13. Erck Lambert AB, Parks SE, Shapiro-Mendoza CK. National and state trends in sudden unexpected infant death: 1990-2015. Pediatrics. (2018) 141(3):e20173519. doi: 10.1542/peds.2017-3519
14. Wilson AL, Randall B. Trends in rates of sudden unexpected infant death (SUID): hopes for prevention. S D Med. (2021) 74(5):220–6.34437780
15. Jullien S. Sudden infant death syndrome prevention. BMC Pediatr. (2021) 21(Suppl 1):320. doi: 10.1186/s12887-021-02536-z
16. Centers for Disease Control and Prevention: Sudden Unexpected Infant Death and Sudden Infant Death Syndrome. Data and statistics. Atlanta Georgia, United States: CDC (2021). [cited 2022 Apr 8]. Available from: https://www.cdc.gov/sids/data.htm#graph
17. Sánchez Ruiz-Cabello FJ, Ortiz González LC, Grupo PrevInfad/PAPPS Infancia y adolescencia. Síndrome de muerte súbita de lactante (parte 1). Factores de Riesgo. Rev Pediatr Aten Primaria. (2013) 15(60):361–70. doi: 10.4321/S1139-76322013000500017
18. Arnau MA, Giner J, Izquierdo MI, Molina P, Zorio E. Abordaje multidisciplinar de la muerte súbita infantil. En: Grupo de Trabajo de Muerte Súbita Infantil. Asociación Española de Pediatría. Libro Blanco de la muerte súbita infantil. 3ª ed.. Madrid: Ergon Creación (2013). 19 p. Available from: https://www.aeped.es/sites/default/files/documentos/libro_blanco_muerte_subita_3ed_.pdf
19. Anderson T, Lavista J, You Ren S, Moon R, Goldstein R, Ramirez JM, et al. Maternal smoking before and during pregnancy and the risk of sudden unexpected infant death. Pediatrics. (2019) 143(4):e20183325. doi: 10.1542/peds.2018-3325
20. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome: stabilization of rates requires further action. Pediatrics. (2008) 122(3):660–6. doi: 10.1542/peds.2007-0135
21. Martínez Alcázar MA, Matías Martínez DR, Rodríguez Suárez R. Muerte súbita del lactante. Qué hacemos y qué debemos hacer para prevenirla. Acta Pediatr Mex. (2006) 27(5):253–8.
22. Shipstone RA, Young J, Kearney L, Thompson JMD. Applying a social exclusion framework to explore the relationship between sudden unexpected deaths in infancy (SUDI) and social vulnerability. Front Public Health. (2020) 8:563573. doi: 10.3389/fpubh.2020.563573
23. Neubauer J, Lecca MR, Russo G, Bartsch C, Medeiros-Domingo A, Berger W, et al. Post-mortem whole-exome analysis in a large sudden infant death syndrome cohort with a focus on cardiovascular and metabolic genetic diseases. Eur J Hum Genet. (2017) 25(4):404–9. doi: 10.1038/ejhg.2016.199
24. Mates J, Mademont-Soler I, Fernandez-Falgueras A, Sarquella-Brugada G, Cesar S, Arbelo E, et al. Sudden cardiac death and copy number variants: what do we know after 10 years of genetic analysis? Forensic Sci Int Genet. (2020) 47:102281. doi: 10.1016/j.fsigen.2020.102281
25. Ivanov D, Mironova E, Polyakova V, Evsyukova I, Osetrov M, Kvetnoy I, et al. Sudden infant death syndrome: melatonin, serotonin, and CD34 factor as possible diagnostic markers and prophylactic targets. PLoS One. (2021) 16(9):e0256197. doi: 10.1371/journal.pone.0256197
26. Mehboob R, Kurdi M, Ahmad M, Gilani SA, Khalid S, Nasief H, et al. Comprehensive analysis of genes associated with sudden infant death syndrome. Front Pediatr. (2021) 9:742225. doi: 10.3389/fped.2021.742225
27. Baruteau AE, Tester DJ, Kapplinger JD, Ackerman MJ, Behr ER. Sudden infant death syndrome and inherited cardiac conditions. Nat Rev Cardiol. (2017) 14(12):715–26. doi: 10.1038/nrcardio.2017.129
28. Subcomisión de Lactancia Materna y Grupo de Trabajo de Muerte Súbita e Inesperada del Lactante. Colecho en el hogar, lactancia materna y muerte súbita del lactante. Recomendaciones para los profesionales de la salud. Arch Argent Pediatr. (2017) 115(Supl 5):S105–10. doi: 10.5546/aap.2017.S105
29. Ball HL, Volpe LE. Sudden infant death syndrome (SIDS) risk reduction and infant sleep location e moving the discussion forward. Soc Sci Med. (2013) 79:84–91. doi: 10.1016/j.socscimed.2012.03.025
30. Alm B, Wennergren G, Möllborg P, Lagercrantz H. Breastfeeding and dummy use have a protective effect on sudden infant death syndrome. Acta Pædiatr. (2016) 105:31–8. doi: 10.1111/apa.13124
31. Erck Lambert AB, Parks SE, Cottengim C, Faulkner M, Hauck FR, Shapiro-Mendoza CK. Sleep-related infant suffocation deaths attributable to soft bedding, overlay, and wedging. Pediatrics. (2019) 143(5):e20183408. doi: 10.1542/peds.2018-3408
32. Hauck FR, Tanabe KO. Beyond “back to sleep”: ways to further reduce the risk of sudden infant death syndrome. Pediatr Ann. (2017) 46(8):e284–90. doi: 10.3928/19382359-20170721-01
33. Kochanek KD, Murphy SL, Xu J, Arias E. Deaths: Final Data for 2017.National Vital Statistics Reports: Centers for Disease Control and Prevention; June 24, 2019 [Consulted july 23, 2019]. Available from: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf
34. de Visme S, Chalumeau M, Levieux K, Patural H, Harrewijn I, Briand-Huchet E, et al. National variations in recent trends of sudden unexpected infant death rate in Western Europe. J Pediatr. (2020) 226:179–85.e4. doi: 10.1016/j.jpeds.2020.06.052
35. Perrone S, Lembo C, Moretti S, Prezioso G, Buonocore G, Toscani G, et al. Sudden infant death syndrome: beyond risk factors. Life (Basel). (2021) 11(3):184. doi: 10.3390/life11030184
36. Bradford S. Unexplained deaths in infancy, England and Wales: 2019. London, United Kingdom: Office for National Statistics (2021). [cited 2022 May 25]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/unexplaineddeathsininfancyenglandandwales/2019
37. Shapiro-Mendoza CK, Tomashek KM, Anderson RN, Wingo J. Recent national trends in sudden, unexpected infant deaths: more evidence supporting a change in classification or reporting. Am J Epidemiol. (2006) 163(8):762–9. doi: 10.1093/aje/kwj117
38. Olecká I, Dobiáš M, Lemrová A, Ivanová K, Fürst T, Krajsa J, et al. Indeterminacy of the diagnosis of sudden infant death syndrome leading to problems with the validity of data. Diagnostics (Basel). (2022) 12(7):1512. doi: 10.3390/diagnostics12071512
39. Byard RW. SIDS Or suffocation-the problem continues. Acta Paediatr. (2021) 110(1):364. doi: 10.1111/apa.15436
40. Campuzano O, Beltramo P, Fernandez A, Iglesias A, García L, Allegue C, et al. Molecular autopsy in a cohort of infants died suddenly at rest. Forensic Sci Int Genet. (2018) 37:54–63. doi: 10.1016/j.fsigen.2018.07.023
41. Grassi S, Campuzano O, Coll M, Cazzato F, Sarquella-Brugada G, Rossi R, et al. Update on the diagnostic pitfalls of autopsy and post-mortem genetic testing in cardiomyopathies. Int J Mol Sci. (2021) 22(8):4124. doi: 10.3390/ijms22084124
42. Instituto Nacional de Estadística y Geografía. Población según condición de afiliación a servicios de salud y sexo por entidad federativa, 2020. Mexico: INEGI (2020). [cited 2022 May 19]. Available from: https://inegi.org.mx/app/tabulados/interactivos/?pxq=Derechohabiencia_Derechohabiencia_01_3e83e8a1-690d-4cfb-8af0-a1e675979b3e
43. Births database from 2008 to 2020: Dirección General de Información en Salud (México). 2022. [Cited 2022 March 1st]. Available from: http://www.dgis.salud.gob.mx/contenidos/basesdedatos/bdc_nacimientos_gobmx.html
44. Deaths database from 2005 to 2020: Dirección General de Información en Salud (México). 2022. [Cited 2022 March 1st]. Available from: http://dgis.salud.gob.mx/contenidos/basesdedatos/bdc_defunciones_gobmx.html
45. Births database from 2004 to 2007.; Instituto Nacional de Estadística, Geografía e Informática (México). 2020. [Cited 2022 March 2nd]. Available from: https://www.inegi.org.mx/sistemas/olap/proyectos/bd/continuas/natalidad/nacimientos.asp?s=est&c=23699&proy=nat_nac
46. Bernal A. Safe Sleep Update. 2012 National Meeting of children's program heads. National Center for Child and Adolescent Health (CeNSIA) Ministry of Health. México. Consulted (2019).
47. Centers for Disease Control and Prevention: Leading Causes of Death Visualization Tool. US: CDC (2020). [cited 2022 Apr 8]. Available from: https://wisqars.cdc.gov/data/lcd/home
48. Taylor BJ, Garstang J, Engelberts A, Obonai T, Cote A, Freemantle J, et al. International comparison of sudden unexpected death in infancy rates using a newly proposed set of cause-of-death codes. Arch Dis Child. (2015) 100(11):1018–23. doi: 10.1136/archdischild-2015-308239
49. Harpur A, Minton J, Ramsay J, McCartney G, Fenton L, Campbell H, et al. Trends in infant mortality and stillbirth rates in Scotland by socio-economic position, 2000-2018: a longitudinal ecological study. BMC Public Health. (2021) 21(1):995. doi: 10.1186/s12889-021-10928-0
50. Fitzgerald DA, Jeffery H, Arbuckle S, du Toit-Prinsloo L, O’Sullivan T, Waters K. Sudden Unexpected Death in Infancy [SUDI]: what the clinician, pathologist, coroner and researchers want to know. Paediatr Respir Rev. (2022) 41:14–20. doi: 10.1016/j.prrv.2021.08.002
51. Task Force on Sudden Infant Death Syndrome, Moon RY, Darnall RA, Feldman-Winter L, Goodstein MH, Hauck FR. SIDS And other sleep-related infant deaths: updated 2016 recommendations for a safe infant sleeping environment. Pediatrics. (2016) 138(5):e20162938. doi: 10.1542/peds.2016-2938
52. Subramonian A, Featherstone R. Interventions for the prevention of sudden infant death syndrome and sudden unexplained death in infancy: a review of guidelines. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health (2020).
53. Cole R, Young J, Kearney L, Thompson JMD. Awareness of infant safe sleep messages and associated care practices: findings from an Australian cohort of families with young infants. BMJ Paediatr Open. (2021) 5(1):e000972. doi: 10.1136/bmjpo-2020-000972
54. Carlin RF, Moon RY. Risk factors, protective factors, and current recommendations to reduce sudden infant death syndrome: a review. JAMA Pediatr. (2017) 171(2):175–80. doi: 10.1001/jamapediatrics.2016.3345
55. Pease A, Garstang JJ, Ellis C, Watson D, Ingram J, Cabral C, et al. Decision-making for the infant sleep environment among families with children considered to be at risk of sudden unexpected death in infancy: a systematic review and qualitative metasynthesis. BMJ Paediatr Open. (2021) 5(1):e000983. doi: 10.1136/bmjpo-2020-000983
Keywords: epidemiology, sudden unexpected infant death (SUID), sudden infant death syndrome—SIDS, Mexico, children death
Citation: Martínez-Valdez L, Richardson V, Bautista-Márquez A and Hernández-Ávila M (2022) Epidemiology of sudden infant death syndrome in Mexico, 2005–2020. Front. Pediatr. 10:1001089. doi: 10.3389/fped.2022.1001089
Received: 22 July 2022; Accepted: 11 November 2022;
Published: 8 December 2022.
Edited by:
Antonio Oliva, Università Cattolica del Sacro Cuore, ItalyReviewed by:
Francesca Cazzato, Università Cattolica del Sacro Cuore, ItalyJeanine Young, University of the Sunshine Coast, Australia
© 2022 Martínez-Valdez, Richardson, Bautista-Márquez and Hernández-Ávila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vesta Richardson dmVzdGEucmljaGFyZHNvbkBpbXNzLmdvYi5teA==
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics