
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 03 December 2021
Sec. Neonatology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.777614
 Tessa Martherus1*
Tessa Martherus1* Kristel L. A. M. Kuypers1
Kristel L. A. M. Kuypers1 Stefan Böhringer2
Stefan Böhringer2 Janneke Dekker1
Janneke Dekker1 Ruben S. G. M. Witlox1
Ruben S. G. M. Witlox1 Stuart B. Hooper3,4
Stuart B. Hooper3,4 Arjan B. te Pas1
Arjan B. te Pas1Background: Preterm infants are commonly supported with 5–8 cmH2O CPAP. However, animal studies demonstrate that high initial CPAP levels (12–15 cmH2O) which are then reduced (termed physiological based (PB)-CPAP), improve lung aeration without adversely affecting cardiovascular function. We investigated the feasibility of PB-CPAP and the effect in preterm infants at birth.
Methods: Preterm infants (24–30 weeks gestation) were randomized to PB-CPAP or 5–8 cmH2O CPAP for the first 10 min after birth. PB-CPAP consisted of 15 cmH2O CPAP that was decreased when infants were stabilized (heart rate ≥100 bpm, SpO2 ≥85%, FiO2 ≤ 0.4, spontaneous breathing) to 8 cmH2O with steps of ~2/3 cmH2O/min. Primary outcomes were feasibility and SpO2 in the first 5 min after birth. Secondary outcomes included physiological and breathing parameters and short-term neonatal outcomes. Planned enrollment was 42 infants.
Results: The trial was stopped after enrolling 31 infants due to a low inclusion rate and recent changes in the local resuscitation guideline that conflict with the study protocol. Measurements were available for analysis in 28 infants (PB-CPAP n = 8, 5–8 cmH2O n = 20). Protocol deviations in the PB-CPAP group included one infant receiving 3 inflations with 15 cmH2O PEEP and two infants in which CPAP levels were decreased faster than described in the study protocol. In the 5–8 cmH2O CPAP group, three infants received 4, 10, and 12 cmH2O CPAP. During evaluations, caregivers indicated that the current PB-CPAP protocol was difficult to execute. The SpO2 in the first 5 min after birth was not different [61 (49–70) vs. 64 (47–74), p = 0.973]. However, infants receiving PB-CPAP achieved higher heart rates [121 (111–130) vs. 97 (82–119) bpm, p = 0.016] and duration of mask ventilation was shorter [0:42 (0:34–2:22) vs. 2:58 (1:36–6:03) min, p = 0.020]. Infants in the PB-CPAP group required 6:36 (5:49-11:03) min to stabilize, compared to 9:57 (6:58–15:06) min in the 5–8 cmH2O CPAP group (p = 0.256). There were no differences in short-term outcomes.
Conclusion: Stabilization of preterm infants with PB-CPAP is feasible but tailoring CPAP appeared challenging. PB-CPAP did not lead to higher SpO2 but increased heart rate and shortened the duration of mask ventilation, which may reflect faster lung aeration.
Historically, elective intubation and mechanical ventilation were standard care in the delivery room (DR), but now respiratory support is primarily given non-invasively to minimize risk of injury (1–3). The effectiveness of non-invasive support is dependent on infants having a patent airway since the larynx of newborn infants closes during apnea (4–8). As the larynx only opens during a breath, support at birth now focuses on stimulating and supporting spontaneous breathing (9). Recent studies showed that breathing effort can be stimulated by adequate oxygenation, repetitive tactile stimulation and caffeine (10–12). However, ongoing breathing activity is totally reliant on lung aeration and these interventions do not necessarily enhance lung aeration (13). Respiratory support in the DR can further be optimized by improving lung aeration.
Lung aeration is driven by the transpulmonary pressure, which is a pressure gradient generated during inspiration (14–16) and can be increased by applying continuous positive airway pressure (CPAP) to the mouth opening. Preterm infants are routinely supported with 5–8 cmH2O CPAP in the DR, yet this strategy has been extrapolated from care used in the neonatal intensive care unit (NICU). However, in the NICU, CPAP is used to support infants hours to days after birth when the lungs are well-aerated (17, 18). There is little evidence that a CPAP of 5–8 cmH2O is the optimal pressure range to promote lung aeration when infants have a liquid-filled highly incompliant lung at birth.
Physiological based (PB)-CPAP takes the changes that are required to transition from fetus to newborn infant into consideration (Figure 1). When infants are born, their airways are filled with liquid that needs to be replaced with air. Initially, the role of CPAP is to assist liquid movement from the airways into the interstitial tissue during inspiration, by increasing the pressure gradient across the airway wall (19, 20). High pressures are needed to overcome the high airway resistance generated by the viscosity of liquid and its movement across the epithelium (14–16). Once lung aeration is established, the role of CPAP changes to maintaining lung aeration. Lower CPAP levels are then likely sufficient to prevent liquid re-entry and alveolar collapse at end-expiration (14–16, 19–24). As real time parameters guide how caregivers decrease CPAP levels, PB-CPAP is tailored to each individual and CPAP levels will suit the different phases of the neonatal transition.
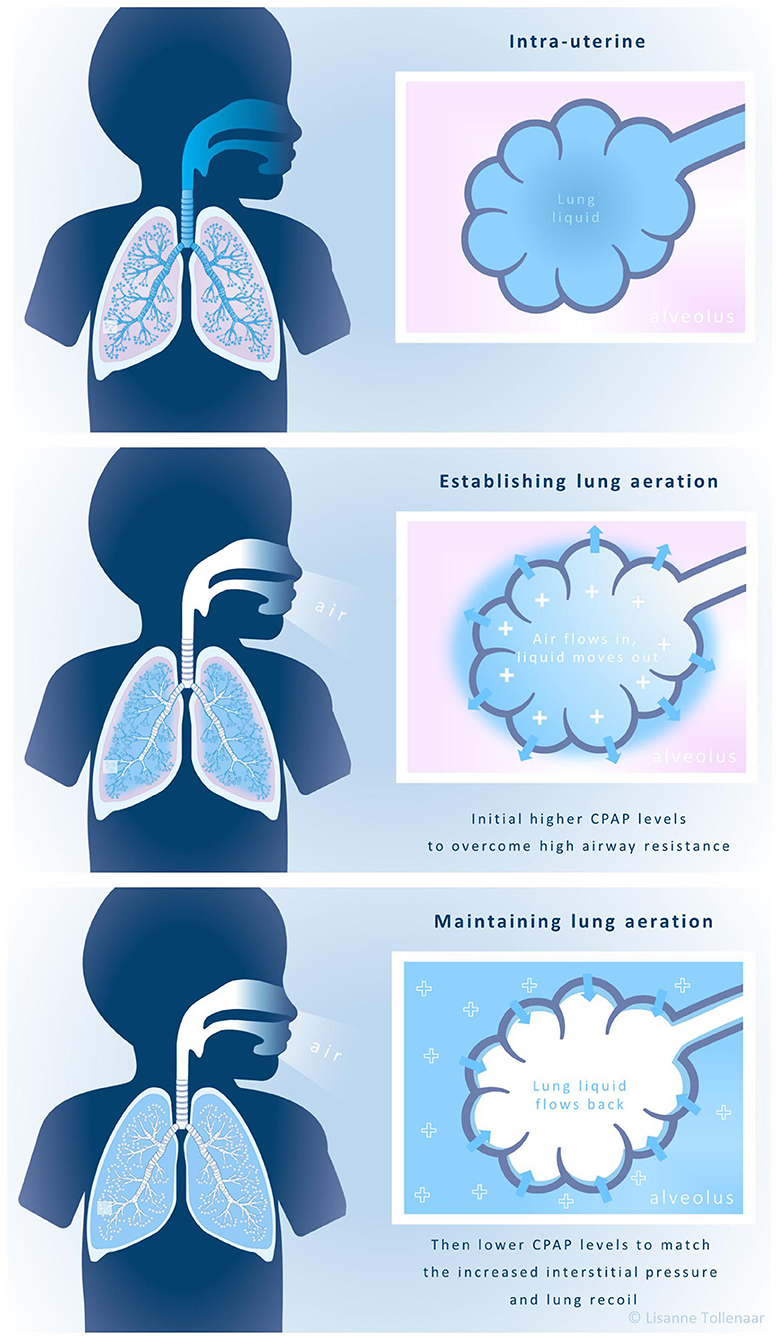
Figure 1. Physiological-based CPAP.
PB-CPAP has so far only been investigated in a preclinical setting. Preterm rabbit (25) and sheep (26) studies demonstrated that initially, 15 cmH2O CPAP improves lung aeration, facilitates cardiovascular stability and better supports spontaneous breathing compared to the currently used CPAP levels. Lung aeration and breathing rates could be maintained if CPAP was gradually decreased to at least 8 cmH2O but did increase oxygen requirements. Overall, there were no indications that PB-CPAP impedes the cardiovascular system or increases the risk on pneumothorax, CPAP belly or intraventricular hemorrhages.
This is the first clinical study that investigates PB-CPAP in preterm infants and we aimed to test the feasibility of using this strategy in the DR and evaluate the effect on physiological parameters.
This single-blinded randomized controlled trial was conducted at the Leiden University Medical Center (LUMC). Preterm infants born between 24+0 and 29+6 weeks gestation were eligible for inclusion. Exclusion criteria were congenital malformations or abnormalities (observed during pregnancy) that affect the transition at birth. Parents were not approached for study participation if there was a language barrier, if there was no time to acquire informed consent or if it was considered inappropriate.
Infants were randomized to PB-CPAP or 5–8 cmH2O CPAP prior to the delivery using an electronic data capture system (Castor EDC, Amsterdam, the Netherlands). Twin pregnancies were randomized as pairs. While allocation was initially solely stratified by gestational age [24+0-26+6 and 27+0-29+6 weeks, variable block sizes (4–6)], the stratification number of infants per pregnancy (single and twin pregnancies) was added after randomizing twenty-three infants in November 2020 and documented in a protocol amendment.
Infants randomized to PB-CPAP received 15 cmH2O CPAP until they reached all predefined stabilization criteria (heart rate ≥100 bpm, SpO2 ≥85%, FiO2 ≤ 0.4, spontaneous breathing), then CPAP was decreased to 8 cmH2O in three steps (2–2-3 cmH2O/min). The decrease in CPAP only continued if the infant still met the stabilization criteria. If infants became apneic, intermittent positive pressure ventilation (iPPV) was initiated with a PEEP of 8 cmH2O. Once infants continued on CPAP after a period of iPPV, the pressure was increased back to the CPAP level that had been used prior to the ventilation period. After completing the 10 min study duration, all infants continued with CPAP levels conforming to local protocols. Infants randomized to PB-CPAP could also receive an escape strategy if deemed appropriate by the caregiver. We assumed that infants who were breathing sufficiently prior to the start of respiratory support, would have already established lung aeration. Therefore, continuous 8 cmH2O CPAP would be sufficient to maintain aeration. Infants supported with this escape strategy were still included in the PB-CPAP group during the analysis. Infants randomized to the control group, received 5–8 cmH2O CPAP. Remaining procedures were executed in line with the local protocol, with exception of infants who participated in the ABC3 study (NCT0380851) and were randomized to physiological based cord clamping. In our local resuscitation guideline, iPPV is initially given non-invasive via mask. However, caregivers can change the interface and apply iPPV via endotracheal intubation if required. Furthermore, the decision to administer caffeine remains at the discretion of the caregiver.
To record SpO2 and heart rate, a Radical-7 Masimo SET pulse oximeter probe (Masimo Corporation, CA, USA) was placed around the infant's right wrist. The Teledyne Oxygen Analyser AX300-I (Teledyne Analytical Instruments, CA, USA) inserted into the inspiratory limb of the Neopuff™ circuit measured fraction of inspired oxygen (FiO2), while the disposable Avea Varflex Flow transducer (Carefusion, CA, USA) connected between the Neopuff™ and the facemask measured flows and pressures. Signals were collected by the New Life BOX Neo-RDS (Applied Biosignals, Weener, Germany) and saved by Polybench software (Applied Biosignals, Weener, Germany). Pulmochart software (Applied Biosignals, Weener, Germany) allowed a breath-by-breath analysis to calculate breathing parameters, corrected for birth weight.
The primary outcomes were feasibility and SpO2 in the first 5 min after birth. Feasibility was explored by evaluating the data from the New Life Box Neo-RDS and videos of resuscitations focusing on protocol adherence and via post-trial evaluations with neonatologists. The neonatologists evaluated this trial individually, as they were asked about their general understanding and experience with this study and obstacles and possible improvements with regard to the PB-CPAP protocol specifically. Physiological outcomes included SpO2, FiO2, SpO2/FiO2 ratio, heart rate, duration of hypoxia [SpO2 <25th percentile of Dawson's target ranges (27)] and bradycardia (heart rate <100 bpm) during the first 5 and 10 min after birth. Respiratory effort parameters included breathing rate, inter-breath interval variability, minute volume, inspired tidal volume, peak inspiratory flow rate (PIFR) and the use of iPPV and caffeine. The infant's overall stability was reflected by Apgar scores and time until stabilization (defined as above). Short-term outcomes included intubation in the DR, intubation <24 h, pneumothorax <5 days, pulmonary hemorrhage, surfactant administration, intraventricular hemorrhages (IVH), spontaneous intestinal perforations and death before NICU discharge. Collected demographical characteristics were gestational age, birth weight, gender, type of pregnancy, mode of delivery, time of cord clamping, 1 min Apgar score, antenatal corticosteroids (full course defined as two doses administered at least 24 h, but at a maximum of 2 weeks prior to delivery), complications during pregnancy and maternal medication use.
The sample size calculation is based on infants who were born in the LUMC, participated in DR studies (11, 28) and received 5–8 cmH2O CPAP. Infants (n = 78) achieved a mean SpO2 of 59% ± 13 in the first 5 min after birth. An increase to 72% was considered to be clinically relevant and for this a sample size of 32 infants would be required [α = 0.05, power (1–β) = 0.8, 2-sided]. Because we randomized per pregnancy and our study population is enriched with twin pregnancies (with the LUMC being the national referral center for complicated twin pregnancies), an additional number of infants needed to be included to prevent loss of power. In February 2019, 28.5% infants included in the MONitoR trial (29) were twins and showed an intra-class correlation of 0.586 for SpO2. Therefore, our sample size required an additional 16.7% (0.285*0.586*100). Anticipating 10% drop-outs due to technical errors or study withdraw, a sample size of 21 infants per group was anticipated.
Statistical analysis was performed using SPSS software version 25.0 (IBM, Chicago, Illinois, 2021). Outcomes were analyzed per group considering the number of included infants, despite stratification criteria. Data were presented as median (IQR) or number (%). When continuous data covered a time period, a mean was calculated for that specific time period per individual. The individual means were then used to calculate and present the group median (IQR). P-values < 0.05 were considered statistically significant.
The primary outcome SpO2 was compared over time using a linear mixed-effect regression model, accounting for the relation between multiple measurements of the same infants. Physiological effects of the CPAP strategies were examined in a per-protocol analysis that excluded infants who were randomized to PB-CPAP but rather received 5–8 cmH2O CPAP. Additional intention-to-treat and a sensitivity analysis were performed to test the robustness of the study outcomes. Fixed effects in the regression models were group, time and the interaction group*time. P-values of the group variable were used to determine the results of the primary outcome while graphical representations have been used to illustrate the effects of randomization groups over time.
Demographic and secondary outcomes were analyzed as per-protocol. Area under the curve (AUC) was calculated for outcomes over time wherein missing values were replaced by the mean, previous or following measurement. Numerical outcomes were analyzed using a Mann-Whitney U test, whereas categorical outcomes were analyzed using a Fisher's exact test or a Logrank test.
One hundred and twenty-seven eligible infants were born in the LUMC during the study enrolment period from October 2019 until March 2021, with the study being halted from March 2020 until May 2020 due to COVID-19 restrictions. Ninety-six infants were not included as they met exclusion criteria (n = 23), parents declined to participate (n = 37), there was insufficient time to ask for study participation (n = 34) or there was insufficient time to complete the randomization procedure (n = 2) in an emergency setting. Thirty-one infants were randomized. One infant was excluded from the analysis due to withdrawal of parental consent, leaving thirty infants for inclusion in the intention-to-treat analysis (PB-CPAP n = 10, 5–8 cmH2O n = 20). There was only one twin pair randomized to PB-CPAP (by chance). As this twin pair received 5–8 cmH2O in an emergency setting, these infants were excluded from the per-protocol analysis due to protocol violation. Therefore, twenty-eight infants were included in the per-protocol analysis (PB-CPAP n = 8, 5–8 cmH2O n = 20, Figure 2). In the PB-CPAP group, seven infants were supported with the initial 15 cmH2O CPAP that was gradually decreased to 8 cmH2O, while one infant received the escape strategy of continuous 8 cmH2O CPAP.
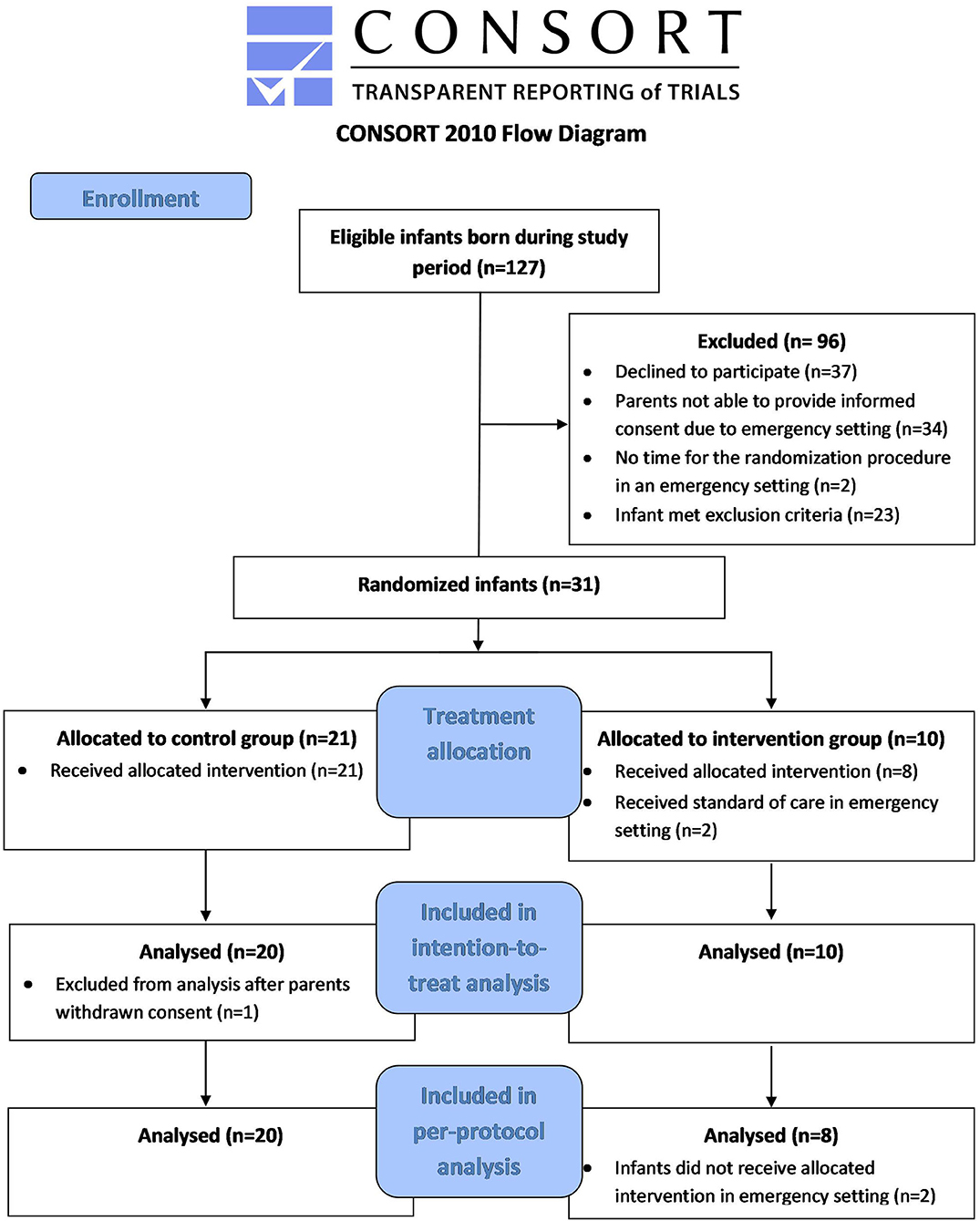
Figure 2. Consort 2010 flowchart.
Table 1 shows baseline characteristics for both groups. Infants in the PB-CPAP group had a median (IQR) gestational age of 26+5 (25+4-27+4) weeks, whereas infants in the 5–8 cmH2O group were 28+5 (25+4-29+4) gestational age (p = 0.601). There were no statistical differences with regard to birth weight, gender, mode of delivery and the use of antenatal steroids. The number of twin pregnancies was significantly higher in the 5–8 cmH2O CPAP group (50%) as compared to the PB-CPAP group (0%, p = 0.025). There were no significant differences regarding maternal medication use, complications that occurred during the pregnancy or physiological based cord clamping that could have affected the respiratory effort at birth. Apgar scores at 1 min were similar between groups.
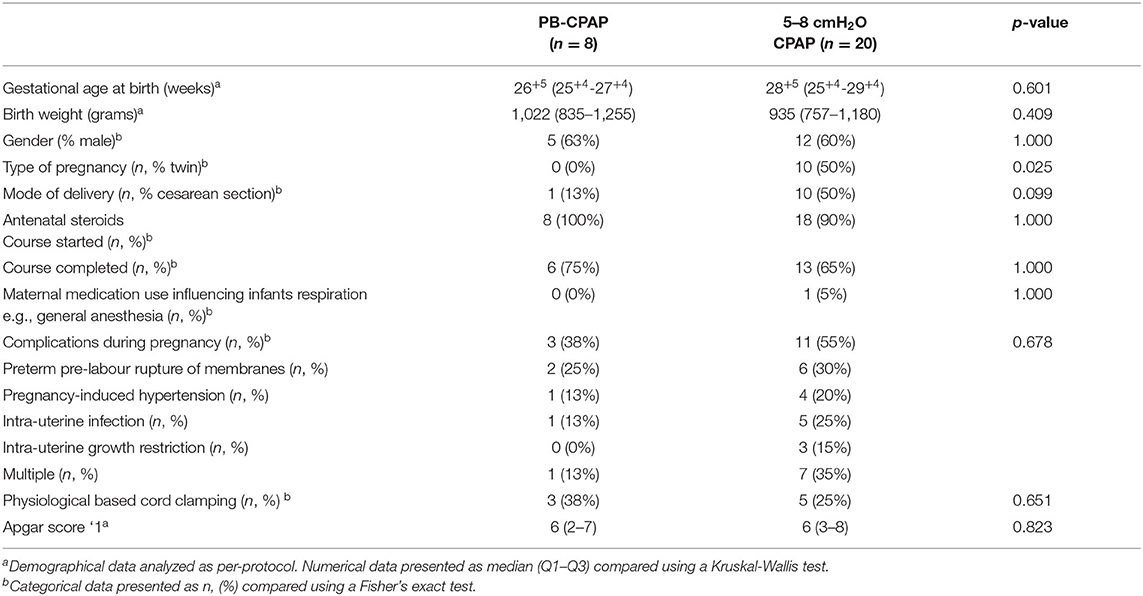
Table 1. Demographical data (per-protocol).
Protocol adherence could not be evaluated in all infants due to technical errors. Protocol adherence was evaluated in 7/8 infants of the PB-CPAP group and three minor protocol deviations were found. One infant received three inflations with a PEEP of 15 cmH2O and in two infants CPAP was decreased faster than described in the study protocol. When protocol adherence was evaluated in 18/20 infants of the 5–8 cmH2O group, it was found that three infants received a CPAP/PEEP level of 4, 10, and 12 cmH2O unintentionally for several minutes.
Evaluations showed that although all caregivers supported the concept of PB-CPAP, only a few (3/11) felt comfortable in performing the protocol. While caregivers often use CPAP, monitor parameters and adjust settings (e.g., FiO2), the PB-CPAP protocol was considered too complex using existing equipment due to the many predefined actions and evaluation moments. If infants became apneic, CPAP was decreased from 15 to 8 cmH2O during iPPV, increased back to 15 cmH2O once CPAP was continued and was decreased step-wise to 8 cmH2O once infants were stabilized. Caregivers indicated that it was challenging to perform these CPAP changes while providing stabilization and a dedicated person (who focused on CPAP) was required to ensure protocol adherence.
The SpO2 in the first 5 min after birth was not significantly different between groups in the per-protocol [PB-CPAP vs. 5–8 cmH2O CPAP, 61 (49–70) vs. 64 (47–74)%, variance of random intercept 128.7, variance of residual 307.3, p = 0.973, Figure 3A] and the intention-to-treat analysis [62 (52–70) vs. 64 (47–74)%, variance of random intercept 123.3, variance of residual 305.9, p = 0.992, Supplementary Table]. There were no significant differences between groups in SpO2 (Figure 3A), FiO2 (Figure 3B) and the SpO2/FiO2 ratio. However, infants supported with PB-CPAP achieved significantly higher heart rates in the first 5 min [121 (111–130) vs. 97 (82–119) bpm, p = 0.016] and tended to have higher heart rates in the first 10 min after birth [135 (127–141) vs. 123 (107–136) bpm, p = 0.075] (Figure 3C). Infants stabilized with PB-CPAP required significantly less time to achieve a stable heart rate >100 bpm [03:01 (01:40–03:19) vs. 04:13 (02:25–05:07) min, p = 0.009, Figure 3D] (Table 2).
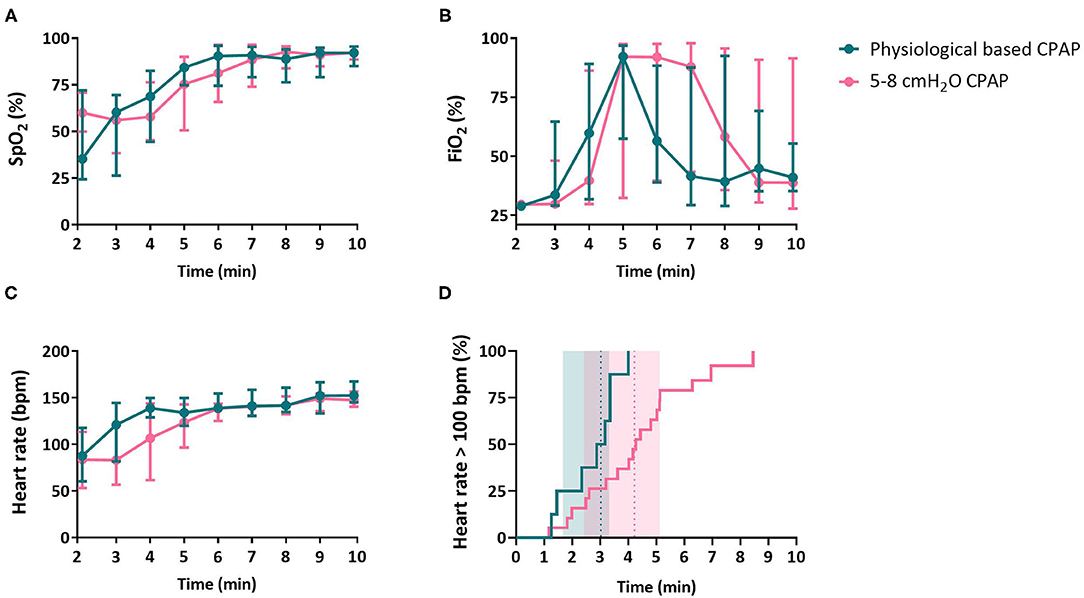
Figure 3. Physiological outcomes. Physiological outcomes oxygen saturation [SpO2, (A)], fraction of inspired oxygen [FiO2, (B)], heart rate (C) and time that heart rate exceeds 100 bpm (D) of infants receiving PB-CPAP and 5–8 cmH2O CPAP following the per-protocol analysis. In (D), heart rate >100 bpm is illustrated as the incidence over time (continuous line) with the median group time (dotted vertical line) and (shaded) inter quartile range.
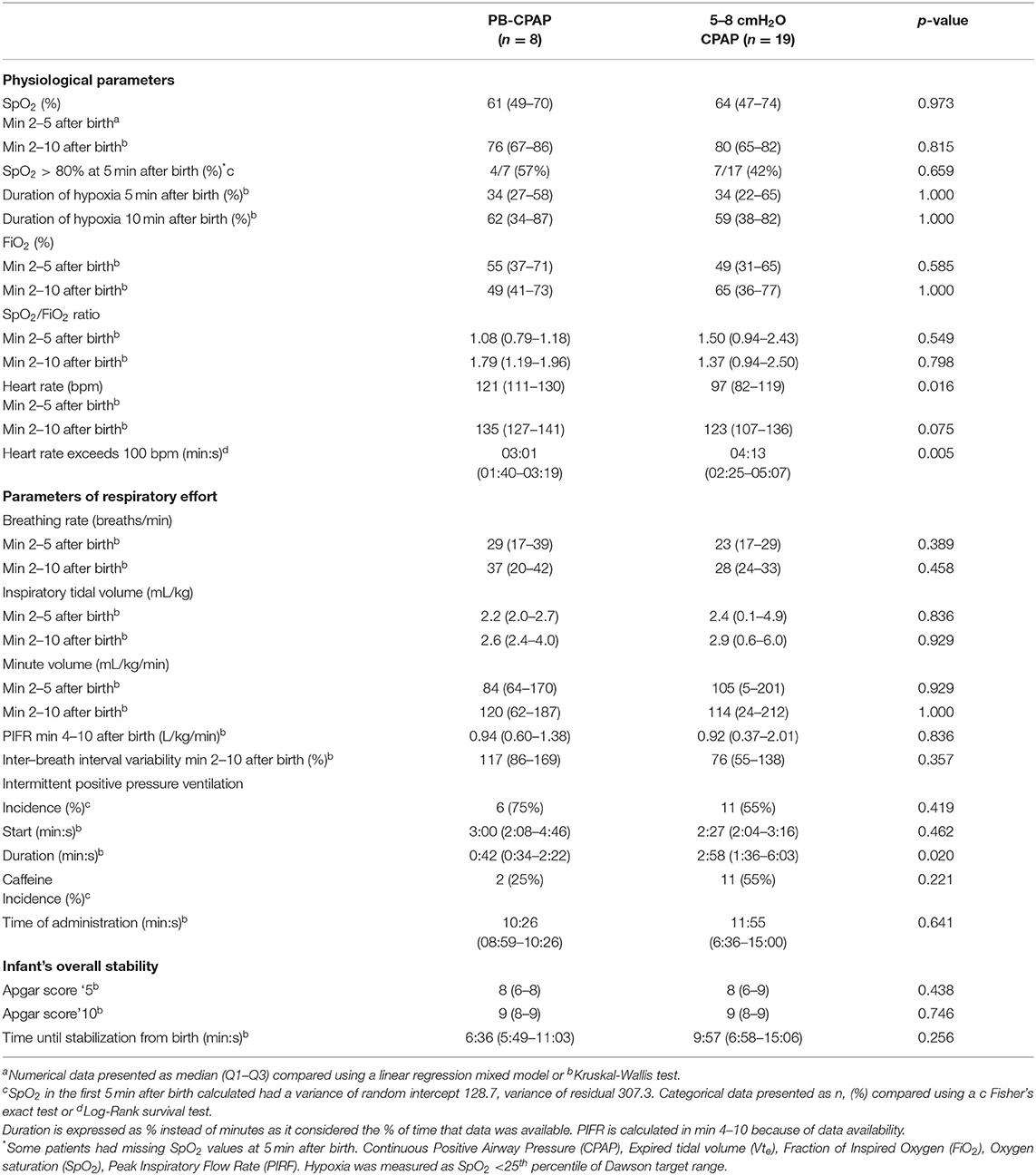
Table 2. Parameters of physiology and respiratory effort in the delivery room.
The groups showed no significant differences regarding breathing rate [37 (20–42) vs. 28 (24–33) breaths/min, p = 0.458, Figure 4A], tidal volume [2.6 (2.4–4.0) vs. 2.9 (0.6–6.0) mL/kg, p = 0.929, Figure 4B] and minute volume [120 (62–187) vs. 114 (24–212) mL/kg/min, p = 1.000, Figure 4C]. There were no differences in inter-breath interval variability or peak inspiratory flow rate (Table 2).
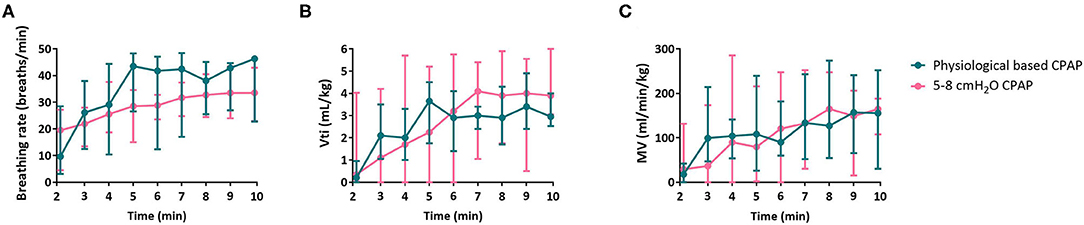
Figure 4. Outcomes of respiratory effort. Outcomes of respiratory effort breathing rate (A), inspiratory tidal volume [Vti, (B)] and minute volume [MV, (C)] of infants receiving PB-CPAP and 5-8 cmH2O CPAP following the per-protocol analysis.
There were no significant differences in the number of infants receiving caffeine (25 vs. 55%, p = 0.221) or iPPV (75 vs. 55%, p = 0.419), yet the duration of mask ventilation was significantly shorter in those supported with PB-CPAP [0:42 (0:34–2:22) min] as compared to 5–8 cmH2O CPAP [2:58 (1:36–6:03) min, p = 0.020]. In the PB-CPAP group, two infants started to breathe spontaneously during mask ventilation and continued afterwards until CPAP was increased back to 15 cmH2O. These infants then stopped breathing and required interventions to re-start spontaneous breathing (Table 2).
The groups showed similar Apgar scores at 5 and 10 min after birth. Infants were considered stable after 6:36 (5:49–11:03) min in the PB-CPAP group and 9:57 (6:58–15:06) min in the 5–8 cmH2O CPAP group (p = 0.256) (Table 2).
Comparing the modes of respiratory support, mean airway pressures (MAP) were significantly higher during iPPV [16.2 (15.4–17.8) cmH2O] than during 5–8 cmH2O CPAP [7.8 (7.3–8.4) cmH2O] but did not differ with 15 cmH2O CPAP [13.8 (13.7–14.6) cmH2O, p = 0.006]. During iPPV, there was significantly more mask leak than when 5-8 cmH2O CPAP was given with the difference being 10 (2–20)% (p = 0.010). There was no significant difference in the amount of leak created during 15 cmH2O and 5–8 cmH2O CPAP [leak difference, 4 (−1 to 17) %, p = 0.345] (Figure 5).
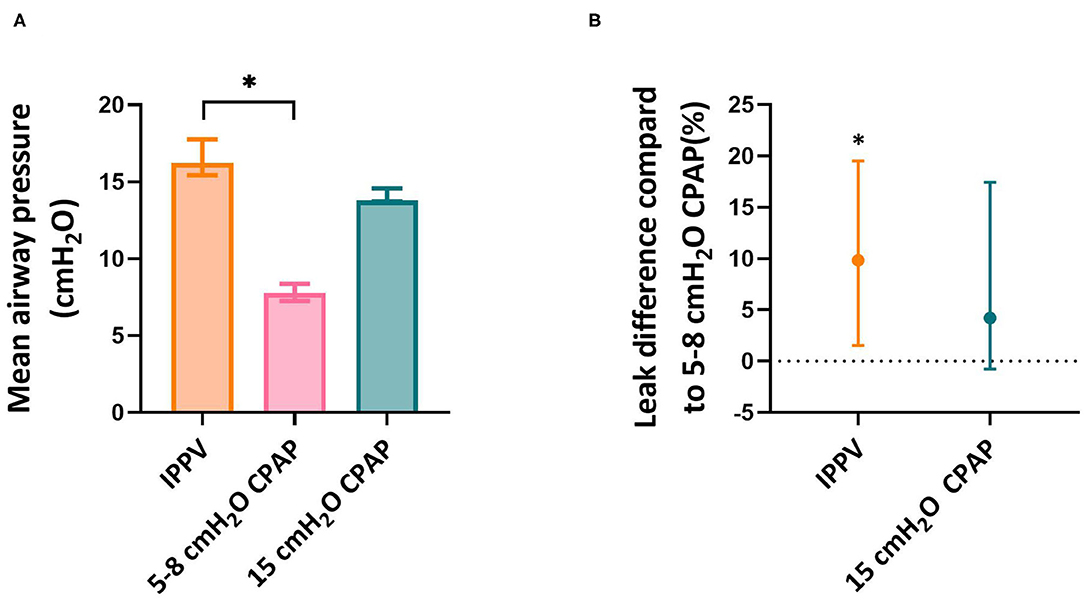
Figure 5. Mean airway pressure and leak. Mean airway pressure (A) and leak (B) per respiratory support mode. Leak per respiratory support mode is calculated as difference in leak compared to 5–8 cmH2O CPAP as it is calculated within infants. Asterisk indicates significant difference.
There were no differences in short-term neonatal respiratory outcomes including incidences of pneumothorax <5 days, intubation in the DR, intubation <24 h, surfactant administration or pulmonary hemorrhages. Groups showed no statistical significance regarding the incidences of spontaneous intestinal perforations, IVH and/or neonatal mortality (Table 3).
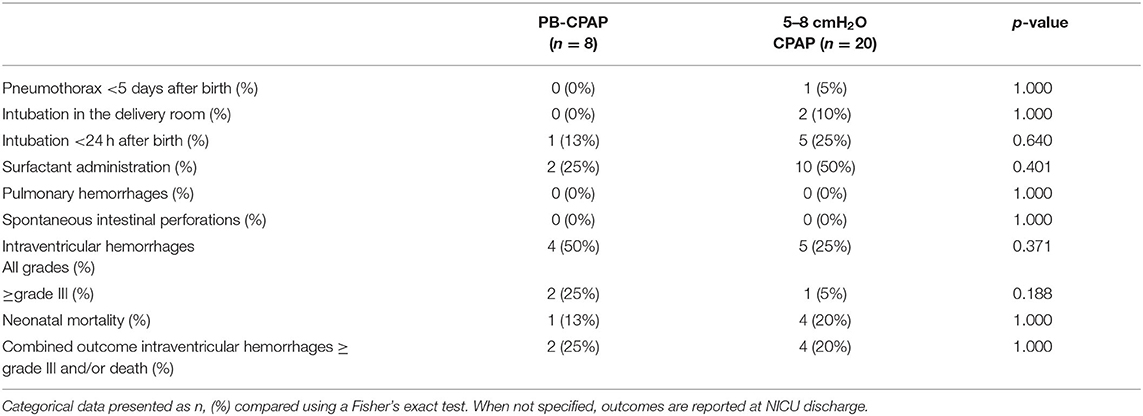
Table 3. Short-term clinical outcomes.
This study was the first to evaluate the feasibility and the direct effect of PB-CPAP for preterm infants in the DR. The study was halted prematurely due to low inclusion rates and recent changes in our local guideline with regard to initial FiO2 levels that conflicted with the study protocol. Although the protocol adherence was high, evaluations by caregivers after the trial indicated that the current PB-CPAP approach is feasible in a research setting but requires simplification before it can be used routinely. Although PB-CPAP did not improve oxygenation, it seemed beneficial for preterm infants as they showed increased heart rate and shortened duration of mask ventilation which reflects a faster and/or improved lung aeration.
The feasibility of our current PB-CPAP approach was evaluated by protocol adherence and post-trial evaluations. There were three minor protocol deviations in the PB-CPAP group, despite the presence of a dedicated person present in the DR who focused on CPAP support. Post-trial evaluations showed that the current approach is too complex. Although routine use of PB-CPAP will likely improve dexterity and the sense of competence among caregivers, the approach requires simplification which can be achieved in various manners. First, the escape strategy (consistent 8 cmH2O CPAP) seems redundant and could be removed. The condition for using the escape strategy was good breathing effort, however we now know that this is not reflective of lung aeration (30) and infants with good breathing efforts may still benefit from PB-CPAP. Second, the number of predefined evaluation moments could be reduced by leaving the decision to adjust CPAP levels to the discretion of the caregiver. Third, a consistent CPAP level could be used until the infant stabilizes and interfaces are switched and/or the infant is transferred to the NICU. This would be the most pragmatic option and is already common practice in some centers. While details of how PB-CPAP can be used may differ between centers depending on how it best fits into the overall DR care, early involvement of the medical team and scenario trainings may increase the usability of PB-CPAP.
We hypothesized that PB-CPAP would improve lung aeration and subsequently improve physiological parameters but found no effects on SpO2 or FiO2. Recent rabbit studies have demonstrated that the increase in lung aeration and oxygenation are not necessarily co-dependent (25, 30), yet they are likely to be additive and at least some lung aeration is essential. Aeration must positively affect SpO2 but the relative contribution of aeration vs. the gradient for oxygen diffusion is complex and influenced by other factors such as pulmonary blood flow and cardiac output. Previous studies in preterm sheep showed that 8 and 15 cmH2O CPAP improved oxygenation and lowered FiO2 requirements as compared to 5 cmH2O CPAP (26, 31). We found no effect on oxygenation in this study, however the effect of PB-CPAP on SpO2 could have been diminished by the large difference in gestational age, high FiO2 levels in both groups and the fact that the power requirements with respect to sample size could not be met. The actual effect of CPAP on oxygenation in preterm infants remains inconclusive.
PB-CPAP led to a larger increase in heart rate, which may reflect a better lung aeration. When infants are born and aerate their lungs, this stimulates a very large increase in pulmonary blood flow. Recent evidence suggests that as lung liquid moves into the interstitial tissue it triggers J-receptors located in the alveolar wall (15, 23). Stimulation of these receptors is thought to initiate a vagal reflex facilitating global pulmonary vasodilation and a subsequent increase in pulmonary blood flow and heart rate (32, 33). The outcomes of this study resemble preclinical studies demonstrating that 15 cmH2O CPAP improves lung aeration (25), PBF and heart rate (26) compared to the currently used CPAP levels. Improved lung aeration would explain why infants required a shortened duration of mask ventilation. Although the time until stabilization was not significantly different between groups, it was striking that infants were stabilized 3 min earlier in the PB-CPAP group.
Two infants restarted breathing during iPPV but stopped when CPAP was increased to 15 cmH2O. We speculate that these infants had already established lung aeration and apnea had been caused by a Hering-Breuer reflex or trigeminal reflex (34). Similar findings have been described in preterm rabbits that had established lung aeration, but became apneic as CPAP was suddenly increased from below to above 7 cmH2O (4). While this is speculative, some infants may establish aeration during iPPV (25) and future studies have to investigate if increasing CPAP levels after iPPV may induce apnea in some infants. Preferably, CPAP is guided by lung aeration, this cannot be measured during the stabilization of preterm infants yet.
The small number of infants included in this study prevents us from making appropriate conclusions regarding safety. We can only note that there were no direct signs of harm, as there were no pneumothoraxes in the PB-CPAP group. In preclinical studies (25, 26) there were no indications that PB-CPAP causes adverse events at birth. We hypothesize that PB-CPAP does not cause lung over-expansion because the lungs are liquid-filled during the initial stage of the transition (creating a relatively high airway resistance) and due to the involvement of the larynx during non-invasive support. A recent sheep study (26) demonstrated that the larynx is involved in pressure transmission to the lungs during spontaneous breathing and can protect the lungs from overexpansion. Also, the pressure given during PB-CPAP are comparable to the pressures generated by the current DR respiratory support approaches, as MAPs of ~15 cmH2O are a common occurrence when mask ventilation includes intermittent positive pressure ventilation (35). Larger clinical trials are needed to examine if PB-CPAP is indeed harmless for preterm infants at birth.
The main limitation of this study is the number of included infants, which prevents us from making appropriate conclusions. While this was caused by various problems that occurred during the trial, a particular problem was low consent rate as 37 parents declined and 33 parents consented (31 randomized, 2 parents gave consent but there was insufficient time to perform the randomization procedure). We found that it was difficult for parents to comprehend the complexity of the procedure as CPAP was an abstract concept for them. Potentially, this selection might lead to bias but we have no indication of difference between the patient cohorts (consent vs. no consent). Since we did not observe adverse effects in this study, deferred consent could be considered for the next study to increase recruitment and decrease the risk of bias.
This study demonstrated that PB-CPAP may be beneficial but that our current approach is too complex. We were unable to demonstrate if PB-CPAP improves oxygen saturation. Nevertheless, PB-CPAP did increase heart rate and shortened the duration of iPPV, which is presumably the result of improved lung aeration. Short-term neonatal outcomes were similar between groups, however due to the low number of included infants it is not possible to make appropriate conclusions from our study. Future studies may continue investigating PB-CPAP using a simplified version of the current approach.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical Research Ethics Committee (METC) Leiden-Den Haag-Delft. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
This study was registered in the Netherlands Trial Register (www.trialregister.nl), titled CPAP titration at birth (NL8089).
TM, SB, AtP, and SH made substantial contributions to conception and design of the study. TM and KK set-up the study and provided the data collection. TM and SB were responsible for data analysis. TM, KK, JD, SB, and AtP were involved in the data interpretation. TM, AtP, and SH drafted the first version of the manuscript. All authors provided feedback and approved the final version of the manuscript.
AtP is a recipient of a NWO innervational research incentives scheme (VIDI 91716428).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.777614/full#supplementary-material
CPAP, Continuous Positive Airway Pressure; FiO2, Fraction of inspired Oxygen; iPPV, intermittent Positive Pressure Ventilation; IQR, Inter quartile Range; IVH, Intra Ventricular Hemorrhage; LUMC, Leiden University Medical Center; MAP, Mean Airway Pressure; NICU, Neonatal Intensive Care Unit; PEEP, Positive End-Expiratory Pressure; RFM, Respiratory Function Monitor; SD, Standard Deviation; SpO2, Oxygen Saturation.
1. Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB, et al. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med. (2008) 358:700–8. doi: 10.1056/NEJMoa072788
2. SUPPORT SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network, Finer NN, Carlo WA, Walsh MC, Rich W, Gantz MG, et al. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med. (2010) 362:1970–9. doi: 10.1056/NEJMoa0911783
3. Trevisanuto D, Satariano I, Doglioni N, Criscoli G, Cavallin F, Gizzi C, et al. Changes over time in delivery room management of extremely low birth weight infants in Italy. Resuscitation. (2014) 85:1072–6. doi: 10.1016/j.resuscitation.2014.04.024
4. Crawshaw JR, Kitchen MJ, Binder-Heschl C, Thio M, Wallace MJ, Kerr LT, et al. Laryngeal closure impedes non-invasive ventilation at birth. Arch Dis Child Fetal Neonatal Ed. (2018) 103:F112–9. doi: 10.1136/archdischild-2017-312681
5. Harding R, Bocking AD, Sigger JN. Upper airway resistances in fetal sheep: the influence of breathing activity. J Appl Physiol. (1986) 60:160–5. doi: 10.1152/jappl.1986.60.1.160
6. Renolleau S, Letourneau P, Niyonsenga T, Praud JP, Gagne B. Thyroarytenoid muscle electrical activity during spontaneous apneas in preterm lambs. Am J Respir Crit Care Med. (1999) 159(5 Pt 1):1396–404. doi: 10.1164/ajrccm.159.5.9807088
7. Moreau-Bussiere F, Samson N, St-Hilaire M, Reix P, Lafond JR, Nsegbe E, et al. Laryngeal response to nasal ventilation in nonsedated newborn lambs. J Appl Physiol. (2007) 102:2149–57. doi: 10.1152/japplphysiol.00891.2006
8. van Vonderen JJ, Hooper SB, Hummler HD, Lopriore E, te Pas AB. Effects of a sustained inflation in preterm infants at birth. J Pediatr. (2014) 165:903–8.e1. doi: 10.1016/j.jpeds.2014.06.007
9. Dekker J, van Kaam AH, Roehr CC, Flemmer AW, Foglia EE, Hooper SB, et al. Stimulating and maintaining spontaneous breathing during transition of preterm infants. Pediatr Res. (2019) 90:722–30. doi: 10.1038/s41390-019-0468-7
10. Dekker J, Hooper SB, Martherus T, Cramer SJE, van Geloven N, Te Pas AB. Repetitive versus standard tactile stimulation of preterm infants at birth - a randomized controlled trial. Resuscitation. (2018) 127:37–43. doi: 10.1016/j.resuscitation.2018.03.030
11. Dekker J, Hooper SB, van Vonderen JJ, Witlox R, Lopriore E, Te Pas AB. Caffeine to improve breathing effort of preterm infants at birth: a randomized controlled trial. Pediatr Res. (2017) 82:290–6. doi: 10.1038/pr.2017.45
12. Dekker J, Martherus T, Lopriore E, Giera M, McGillick EV, Hutten J, et al. The effect of initial high vs. low FiO2 on breathing effort in preterm infants at birth: a randomized controlled trial. Front Pediatr. (2019) 7:504. doi: 10.3389/fped.2019.00504
13. Dekker J, Hooper SB, Croughan MK, Crossley KJ, Wallace MJ, McGillick EV, et al. Increasing Respiratory effort with 100% oxygen during resuscitation of preterm rabbits at birth. Front Pediatr. (2019) 7:427. doi: 10.3389/fped.2019.00427
14. Hooper SB, Kitchen MJ, Wallace MJ, Yagi N, Uesugi K, Morgan MJ, et al. Imaging lung aeration and lung liquid clearance at birth. FASEB J. (2007) 21:3329–37. doi: 10.1096/fj.07-8208com
15. Siew ML, Wallace MJ, Kitchen MJ, Lewis RA, Fouras A, Te Pas AB, et al. Inspiration regulates the rate and temporal pattern of lung liquid clearance and lung aeration at birth. J Appl Physiol. (2009) 106:1888–95. doi: 10.1152/japplphysiol.91526.2008
16. Siew ML, Wallace MJ, Allison BJ, Kitchen MJ, te Pas AB, Islam MS, et al. The role of lung inflation and sodium transport in airway liquid clearance during lung aeration in newborn rabbits. Pediatr Res. (2013) 73(4 Pt 1):443–9. doi: 10.1038/pr.2012.197
17. Wyllie J, Bruinenberg J, Roehr CC, Rudiger M, Trevisanuto D, Urlesberger B. European resuscitation council guidelines for resuscitation 2015: section 7. Resuscitation and support of transition of babies at birth. Resuscitation. (2015) 95:249–63. doi: 10.1016/j.resuscitation.2015.07.029
18. Wyckoff MH, Aziz K, Escobedo MB, Kapadia VS, Kattwinkel J, Perlman JM, et al. Part 13: neonatal resuscitation: 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. (2015) 132(18 Suppl. 2):S543–60. doi: 10.1161/CIR.0000000000000267
19. te Pas AB, Siew M, Wallace MJ, Kitchen MJ, Fouras A, Lewis RA, et al. Effect of sustained inflation length on establishing functional residual capacity at birth in ventilated premature rabbits. Pediatr Res. (2009) 66:295–300. doi: 10.1203/PDR.0b013e3181b1bca4
20. te Pas AB, Siew M, Wallace MJ, Kitchen MJ, Fouras A, Lewis RA, et al. Establishing functional residual capacity at birth: the effect of sustained inflation and positive end-expiratory pressure in a preterm rabbit model. Pediatr Res. (2009) 65:537–41. doi: 10.1203/PDR.0b013e31819da21b
21. Siew ML, Te Pas AB, Wallace MJ, Kitchen MJ, Islam MS, Lewis RA, et al. Surfactant increases the uniformity of lung aeration at birth in ventilated preterm rabbits. Pediatr Res. (2011) 70:50–5. doi: 10.1203/PDR.0b013e31821be094
22. Miserocchi G, Poskurica BH, Del Fabbro M. Pulmonary interstitial pressure in anesthetized paralyzed newborn rabbits. J Appl Physiol. (1994) 77:2260–8. doi: 10.1152/jappl.1994.77.5.2260
23. Bland RD, McMillan DD, Bressack MA, Dong L. Clearance of liquid from lungs of newborn rabbits. J Appl Physiol Respir Environ Exerc Physiol. (1980) 49:171–7. doi: 10.1152/jappl.1980.49.2.171
24. Hooper SB, Te Pas AB, Kitchen MJ. Respiratory transition in the newborn: a three-phase process. Arch Dis Child Fetal Neonatal Ed. (2016) 101:F266–71. doi: 10.1136/archdischild-2013-305704
25. Martherus T, Croughan MK, Crossley KJ, Wallace MJ, McGillick EV, Thio M, et al. Higher CPAP levels improve functional residual capacity at birth in preterm rabbits. Pediatr Res. (2021). doi: 10.1038/s41390-021-01647-8. [Epub ahead of print].
26. Martherus T, Crossley KJ, Rodgers KA, Dekker J, Demel A, Moxham AM, et al. High-CPAP does not impede cardiovascular changes at birth in preterm sheep. Front Pediatr. (2020) 8:584138. doi: 10.3389/fped.2020.584138
27. Dawson JA, Kamlin CO, Vento M, Wong C, Cole TJ, Donath SM, et al. Defining the reference range for oxygen saturation for infants after birth. Pediatrics. (2010) 125:e1340–7. doi: 10.1542/peds.2009-1510
28. van Zanten HA, K LAMK, van Zwet EW, van Vonderen JJ, Omar FKC, Springer L, et al. A multi-centre randomised controlled trial of respiratory function monitoring during stabilisation of very preterm infants at birth. Resuscitation. (2021) 167:317–25. doi: 10.1016/j.resuscitation.2021.07.012
29. Dekker J, Lopriore E, van Zanten HA, Tan R, Hooper SB, Te Pas AB. Sedation during minimal invasive surfactant therapy: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. (2019) 104:F378–83. doi: 10.1136/archdischild-2018-315015
30. van Henten TMA, Dekker J, Te Pas AB, Zivanovic S, Hooper SB, Roehr CC. Tactile stimulation in the delivery room: do we practice what we preach? Arch Dis Child Fetal Neonatal Ed. (2019) 104:F661–2. doi: 10.1136/archdischild-2018-316344
31. Mulrooney N, Champion Z, Moss TJ, Nitsos I, Ikegami M, Jobe AH. Surfactant and physiologic responses of preterm lambs to continuous positive airway pressure. Am J Respir Crit Care Med. (2005) 171:488–93. doi: 10.1164/rccm.200406-774OC
32. Lang JA, Pearson JT, Binder-Heschl C, Wallace MJ, Siew ML, Kitchen MJ, et al. Increase in pulmonary blood flow at birth: role of oxygen and lung aeration. J Physiol. (2016) 594:1389–98. doi: 10.1113/JP270926
33. Lang JA, Pearson JT, Binder-Heschl C, Wallace MJ, Siew ML, Kitchen MJ, et al. Vagal denervation inhibits the increase in pulmonary blood flow during partial lung aeration at birth. J Physiol. (2017) 595:1593–606. doi: 10.1113/JP273682
34. Sankaran K, Leahy FN, Cates D, MacCallum M, Rigatto H. Effect of lung inflation on ventilation and various phases of the respiratory cycle in preterm infants. Biol Neonate. (1981) 40:160–6. doi: 10.1159/000241485
Keywords: CPAP, respiratory support, physiology, birth, preterm
Citation: Martherus T, Kuypers KLAM, Böhringer S, Dekker J, Witlox RSGM, Hooper SB and Pas ABt (2021) Feasibility and Effect of Physiological-Based CPAP in Preterm Infants at Birth. Front. Pediatr. 9:777614. doi: 10.3389/fped.2021.777614
Received: 15 September 2021; Accepted: 09 November 2021;
Published: 03 December 2021.
Edited by:
Quen Mok, Great Ormond Street Hospital for Children NHS Foundation Trust, United KingdomReviewed by:
Bernhard Schwaberger, Medical University of Graz, AustriaCopyright © 2021 Martherus, Kuypers, Böhringer, Dekker, Witlox, Hooper and Pas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tessa Martherus, dC5tYXJ0aGVydXNAbHVtYy5ubA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.