
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 29 November 2021
Sec. Pediatric Cardiology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.767394
This article is part of the Research Topic Determinants and Impact of Early Vascular Aging in Children and Adolescents View all 10 articles
 Piotr Skrzypczyk1*
Piotr Skrzypczyk1* Anna Maria Wabik1
Anna Maria Wabik1 Michał Szyszka2
Michał Szyszka2 Sergiusz Józwiak3
Sergiusz Józwiak3 Przemysław Bombiński4
Przemysław Bombiński4 Aleksandra Jakimów-Kostrzewa4Michał Brzewski4Małgorzata Pańczyk-Tomaszewska1
Aleksandra Jakimów-Kostrzewa4Michał Brzewski4Małgorzata Pańczyk-Tomaszewska1Objectives: Experimental data indicate that activating mutations in the mTOR (mammalian target of rapamycin) pathway may lead to abnormal arterial wall structure. Vascular anomalies like arterial stenoses are reported in pediatric patients with tuberous sclerosis complex (TSC). In addition, large renal lesions (angiomyolipoma—AML and cysts) are risk factors for arterial hypertension in adult patients with TSC. This study aimed to assess blood pressure, including central blood pressure and arterial damage (early vascular aging—EVA) in children with TSC.
Materials and Methods: In a group of 33 pediatric patients with TSC (11.13 ± 4.03 years, 15 boys, 18 girls), we evaluated peripheral and central office blood pressure, 24-h ambulatory blood pressure, and arterial damage: aortic pulse wave velocity (aPWV) [m/s], [Z-score], augmentation index (AIx75HR [%]), common carotid artery intima-media thickness (cIMT) [mm], [Z-score], stiffness of common carotid artery (E-tracking), renal lesions in magnetic resonance and ultrasonography, and selected biochemical parameters. The control group consisted of 33 healthy children (11.23 ± 3.28 years, 15 boys, 18 girls).
Results: In TSC group 7 (21.2%) children had arterial hypertension, 27 (81.8%) children had renal angiomyolipomas, 26 (78.8%)—renal cysts, and 4 (12.1%) patients were treated with mTOR inhibitors (2 patients with everolimus and 2 patients with sirolimus) at the moment of evaluation. Children with TSC had higher central systolic blood pressure (AoSBP) (98.63 ± 9.65 vs. 90.45 ± 6.87 [mm Hg], p < 0.001), cIMT (0.42 ± 0.05 vs. 0.39 ± 0.03 [mm], p = 0.011), cIMT Z-score (0.81 ± 1.21 vs. 0.16 ± 0.57, p = 0.007), aPWV (4.78 ± 0.81 vs. 4.25 ± 0.56 [m/s], p = 0.003) and aPWV Z-score (−0.14 ± 1.15 vs. −0.96 ± 0.87, p = 0.002) compared to healthy children, without differences in AIx75HR (8.71 ± 15.90 vs. 5.24 ± 11.12 [%], p = 0.319) and stiffness of common carotid artery. In children with TSC AoSBP correlated positively with serum cystatin C concentration (r = 0.377, p = 0.030) and with maximum diameter of renal cyst (R = 0.419, p = 0.033); mean arterial pressure (MAP) 24 h Z-score correlated with serum cystatin C concentration (R = 0.433, p = 0.013); and aPWV Z-score with daily urinary albumin loss [mg/24 h] (R = 0.412, p = 0.029).
Conclusions: Children with tuberous sclerosis complex are at risk of elevated central blood pressure and early vascular aging. In children with TSC, blood pressure and arterial stiffness are related to renal involvement.
Tuberous sclerosis complex (TSC, Bournevile-Pringle disease) is an autosomal dominant disorder found in 1:5,800–1:12,500 births. At present, TSC is diagnosed on the basis of recently updated 2021 International Tuberous Sclerosis Complex Consensus Group (ITSCCG) genetic and clinical criteria (1). The mutation in tumor suppressor genes: TSC1 (chromosome 9q34) or TSC2 (chromosome 16p13) are found in 85–90% of the TSC patients; remaining individuals were found to have mutations in non-coding regions of the genes or to show genetic mosaicism (2). In most patients, family history is negative (de novo mutation); approximately 30% of cases are inherited from one of the affected parents (3). TSC1 and TSC2 genes encode natural inhibitors of the mTOR (mammalian target of rapamycin) signaling pathway, i.e., hamartin and tuberin, respectively. Constant activation of the mTOR pathway leads to uncontrolled cell proliferation and formation of hamartomas, benign neoplasms, and rarely, malignant neoplasms in virtually all parts of the body. Thus, the spectrum of TSC-associated disorders includes skin lesions (e.g., depigmented spots, facial angiofibromas, shagreen patches, seen in ~90% of patients), retinal lesions (87% of patients), central nervous system abnormalities (70–90% of patients), heart (self-limiting rhabdomyoma found in approximately half of the patients), lungs (angiomyolipoma and lymphangioleiomyomatosis present mainly in women) and, finally, diversified renal lesions (1).
Renal abnormalities are present in as many as 50–80% of TSC individuals and are the second cause of mortality (just after brain tumors) in these patients. The spectrum of renal abnormalities involves angiomyolipomas (AML)—present in 55–90% of patients with kidney lesions, renal cysts, glomerulocystic disease, oncocytoma, and renal cell carcinoma (RCC) (4, 5). Angiomyolipomas belong to a family of neoplasms called perivascular epithelioid cell tumors. They can be classified histologically as typical (triphasic or lipid-rich) or atypical or fat-poor (monophasic or epithelioid). Typical, lipid-rich AMLs are benign tumors histologically characterized by (in varying proportions) proliferation of spindle cells, epithelioid cells, and adipocytic cells in concert with many abnormal, thick-walled blood vessels (6). AMLs pose a risk of life-threatening spontaneous bleeding (Wünderlich syndrome) once the tumor's diameter exceeds 30 mm (1, 6).
Experimental data indicate that activating mutations in the mTOR pathway may lead to degenerative phenotype and uncontrolled proliferation of vascular smooth muscle cells (SMC) and abnormal structure of arterial wall (7, 8). Arterial stenoses (e.g., renal artery stenosis, mid-aortic syndrome) or aneurysms have been reported in children and adults with TSC (9–12). In addition, large renal lesions are risk factors for arterial hypertension in adult patients with TSC (3, 13). These factors might theoretically put children with TSC at risk of arterial damage and early vascular aging (EVA), a state of accelerated adverse changes in the biochemical and cellular components of the vascular tree (14, 15). However, to the best of our knowledge, there are no reports on arterial damage in both children and adults with TSC. Thus, this study aimed to assess whether children with TSC are at risk of EVA and evaluate potential arterial damage determinants in this group of patients.
This single-center cross-sectional study included patients with TSC treated in 2018–2021 in one tertiary center of pediatric nephrology. The criterion for inclusion in the study was confirmed TSC following ITSCCG recommendations (1, 16). The exclusion criteria were: height below 120 cm or acute infectious disease (temporary 2-week exclusion). Thirty-three age- and sex-matched healthy subjects were included in the control group. Healthy children were recruited from patients of outpatient University Hospital. Participation in the study was proposed with the following exclusion criteria: height below 120 cm, acute infectious disease, known chronic illness (including kidney, heart, and inflammatory disease), obesity, and arterial hypertension. The flowcharts of the study and control groups are presented in Figures 1, 2, respectively.
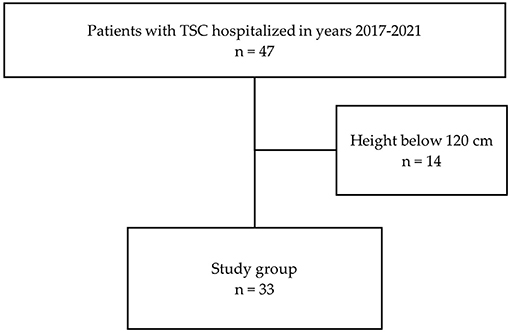
Figure 1. Flowchart of the patients' recruitment (TSC—tuberous sclerosis complex).
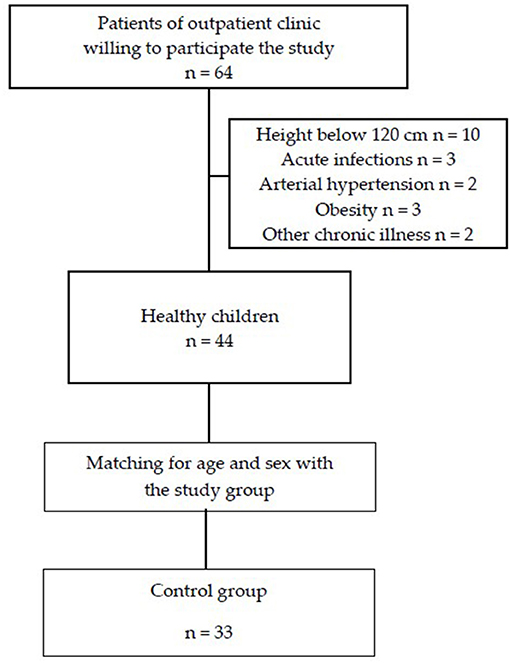
Figure 2. Flowchart of the control group recruitment.
The authors obtained approval from the local Bioethical Committee before initiating the research (approval no. KB/145/2017, 4th July 2017). All procedures involving human participants were in accordance with the highest ethical standards of the institutional research committee and were performed according to the Declaration of Helsinki on the treatment of human subjects and its later amendments. Informed consent was obtained from all participants' representatives and participants (≥16 years) before enrolling in the study.
Based on individual medical records, we evaluated the following clinical parameters in all TSC individuals: family history of tuberous sclerosis complex, presence of TSC-related neurological symptoms: developmental delay and epilepsy, presence of arterial hypertension, and medications used, including mTOR inhibitors, antiepileptic and antihypertensive drugs. In all children with TSC, the following basic anthropometric parameters were assessed: age [years], sex, body height [cm], body weight [kg], and body mass index [kg/m2]. Anthropometric parameters were compared with the standards for the Polish population and presented in the form of a Z-score (17). According to WHO recommendations, overweight and obesity were defined as a BMI Z-score above 1 and 2, respectively.
All TSC patients had following biochemical parameters evaluated: serum concentrations of creatinine [mg/dL], urea [mg/dL], cystatin C [ng/mL], uric acid [mg/dL], total, HDL- and LDL-cholesterol [mg/dL], and triglyceride [mg/dL]. Also, daily urinary albumin loss was assessed in all the children. The estimated glomerular filtration rate (eGFR) was calculated in all patients [mL/min/1.73 m2] according to the revised 2009 Schwartz formula (18). Impaired renal function was defined as eGFR below 60 mL/min/1.73 m2 [which responses to chronic kidney disease 3G according to (19)], and hyperfiltration was diagnosed when eGFR was equal or exceeded 140 mL/min/1.73 m2 (20). Normal values of cholesterol and triglycerides were taken from the Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute (21), and hyperuricemia was recognized when uric acid was ≥5.5 [mg/dL] (22). Elevated urinary albumin loss was defined as daily albuminuria >30 mg/24 h.
Blood pressure measurements were performed using the oscillometric method (Welch Allyn Patient Monitor, Welch Allyn, Skaneateles Falls, NY, USA) in line with ESH recommendations. They were analyzed using pediatric normative values ([mm Hg], Z-scores) (23, 24). According to the American Heart Association guidelines, all the TSC children also had 24 h ambulatory blood pressure measurement performed (Oscar 2 Suntech with Sphygmocor Inside, SunTech Medical Inc., Morrisville, NC, USA) (25). Systolic, diastolic, and mean blood pressures (SBP, DBP, MAP, respectively), blood pressure loads, and nighttime blood pressure dipping (DIP) were analyzed. DIP below 10% was considered as disturbed circadian rhythm (25). The blood pressure cuff was chosen following ESH recommendations and the devices' instructions (26).
The assessment for early vascular aging was performed using the following methods: an ultrasonographic examination of the common carotid artery (ALOKA Prosound Alpha 6, Hitachi Aloka Medical Ltd., Tokyo, Japan)—common carotid artery intima-media thickness (cIMT) [mm], Z-score (27), and common carotid artery local stiffness (E-tracking); applanation tonometry (Sphygmocor, ATCOR, Sydney, Australia)—central aortic blood pressure, pulse wave analysis, and aortic (carotid-femoral) pulse wave velocity (aPWV) [m/s], Z-score (28). All arterial measurements were performed by a single investigator (P.S.) in a quiet room with a controlled temperature (20 ± 5°C) after 5 min rest. cIMT was measured in all patients in a supine position using a manual method approximately 1 cm proximal to the carotid bulb on the distal carotid wall. Six cIMT measurements were obtained and averaged, three on the left and three on the right side. Peripheral pressure waveforms were recorded from the right radial artery at the wrist in a sitting position, and the transfer function was used to generate the central pressure waveform. aPWV was measured in a supine position and calculated as a difference in the carotid-to-femoral path length divided by the difference in R wave to the foot of the pressure wave taken from the superimposed ECG and pressure tracings. The path length was measured as the distance from the right carotid sampling site to the jugular notch, subtracted from the distance from the jugular notch to the right femoral sampling site (27). Peripheral pressure waveform and aPWV were obtained three times, and the mean value was analyzed.
In all patients, abdominal ultrasonography was performed using a Philips Epiq 5G device (Royal Philips, Amsterdam, The Netherlands) in B-mode. Renal length [mm], echogenicity and corticomedullary differentiation, and the presence of renal parenchymal changes, including typical TSC lesions: angiomyolipoma (AML) and cysts were evaluated. The longest dimension of the largest lesion [mm] was assessed for AML and cysts. In patients diagnosed with arterial hypertension duplex Doppler ultrasonography was performed to exclude renal artery stenosis. In 24/33 (72.7%) patients, magnetic resonance imaging (MRI) of the abdomen was performed with a MAGNETOM Skyra 3T 3-tesla scanner (Siemens AG, Berlin, Germany) in T2-weighted, DWI, and T1-weighted sequences before and after intravenous administration of the contrast agent—Gadovist (gadobutrol) (Bayer AG, Leverkusen, Germany). Renal length [mm], renal cortical signal and differentiation, and presence of renal parenchymal lesions (angiomyolipomas, cysts) with the assessment of the largest dimension of the largest lesion [mm] were evaluated. Fat-poor AMLs were recognized according to the Polish Society of Nephrology recommendations (29). In case of discrepancy between MRI and ultrasound findings, MRI findings were considered conclusive.
The results were statistically analyzed using TIBCO Statistica 13.3 software (TIBCO Software Inc., Palo Alto, CA, USA). The normality of variables was studied using the Shapiro–Wilk test. The numerical data obtained were presented as mean and standard deviation (SD) (normally distributed data) or median and interquartile range (IQR, Q1–Q3) (non-normally distributed data). Normally distributed data were compared with Student t-test for independent groups and non-normally distributed data using the Mann–Whitney U test. The relationship between the two groups of variables was analyzed using Pearson correlation or Spearman rank correlation (depending on the distribution). Percentages in both groups were compared using the chi-square test. A p-value < 0.05 was considered statistically significant.
Clinical and biochemical parameters in the studied children were presented in Table 1. In the group of 33 children with TSC, there were 4 (12.1%) overweight patients and no obese children. Three (9.1%) patients had previously diagnosed arterial hypertension—all these patients were treated with angiotensin-converting enzyme inhibitors (2 with enalapril, 1 with ramipril). In addition, arterial hypertension was diagnosed at the moment of evaluation in 4 patients based on abnormal ambulatory blood pressure monitoring (including three masked hypertension patients). Most of the children had developmental delay and epilepsy. Four (12.1%) patients were treated with mTOR inhibitors. Three children received mTOR inhibitors due to large (>3 cm) renal angiomyolipomas (rapamycin in 2 and everolimus in 1), and one child was treated with everolimus due to the presence of non-operative SEGA tumors. Most patients had kidney involvement revealed in MRI or US. There were only 3 (9.1%) children without renal lesions. The largest AML (71 mm in maximal diameter) was found in a 17-year-old female patient who started rapamycin treatment. Two male patients aged 7.7 and 9.3 years had genetically confirmed contagious genes syndrome (deletion involving TSC2 and PKD1 genes) with very large renal cysts (maximal cyst diameter −35 and 44 mm, respectively). Impaired renal function was found in none of the patients, but in 11 (33.3%) children, hyperfiltration was revealed. Hyperuricemia was found in 6 (18.2%) children with the highest uric acid concentration 6.3 mg/dL. Acceptable total cholesterol (<170 mg/dL) was found in 26 (78.8%), borderline high total cholesterol (170–199 mg/dL) in 5 (15.2%) and high (≥200 mg/dL) in 2 (6.0%) children; acceptable triglycerides (<75 mg/dL in 0–9 years and <90 mg/dl in 10–19 years) was revealed in 24 (72.7%), borderline high triglycerides (75–99 mg/dL in 0–9 years and 90–129 mg/dl in 10–19 years) in 5 (15.2%) and high triglycerides (>100 mg/dL in 0–9 years and >130 mg/dl in 10–19 years) in 4 (12.1%) patients. Elevated urinary albumin loss was found in 3 (9.1%) of the children.
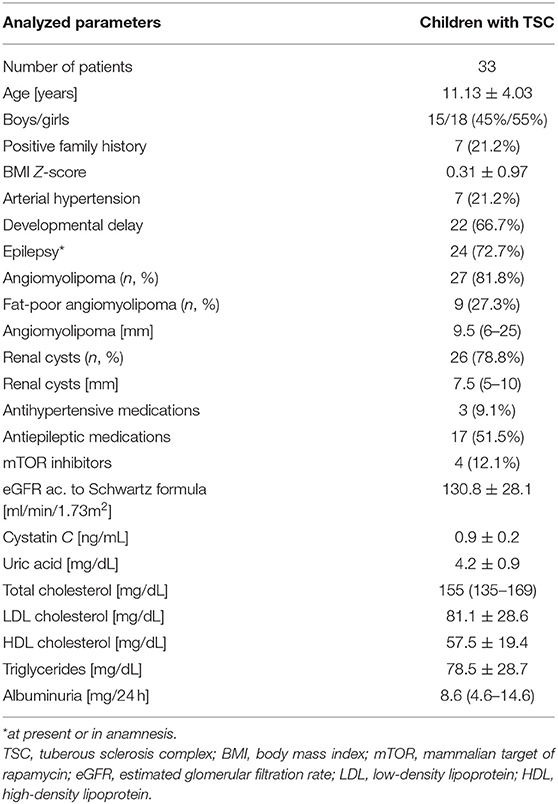
Table 1. Clinical and biochemical parameters in children with tuberous sclerosis complex.
The comparison of blood pressure in children with TSC and healthy children was depicted in Table 2. There were no differences between the groups in terms of age, sex, and BMI Z-score. In the group of TSC patients, elevated (≥95th percentile) office systolic or diastolic blood pressure was revealed in 10 (30.3%) patients, including two patients with previously recognized arterial hypertension. Elevated blood pressure in ABPM was revealed in 4 (12.1%) patients—all of them were considered as normotensives before the study. Among these four patients, one 13-year-old girl also had elevated office blood pressure. Additionally, ABPM revealed masked hypertension in three patients. All three patients with previously recognized and treated arterial hypertension had normal ABPM results at the moment of the study. The analysis of blood pressure in TSC children was depicted in Figure 3. A disturbed circadian blood pressure profile was recognized in 16 TSC patients (including five patients with arterial hypertension). Children with TSC were characterized by significantly higher office peripheral and central blood pressure and 24-h ambulatory blood pressure than healthy peers. The groups did not differ significantly in 24-h pulse pressure, heart rate, and systolic and diastolic blood pressure dipping.
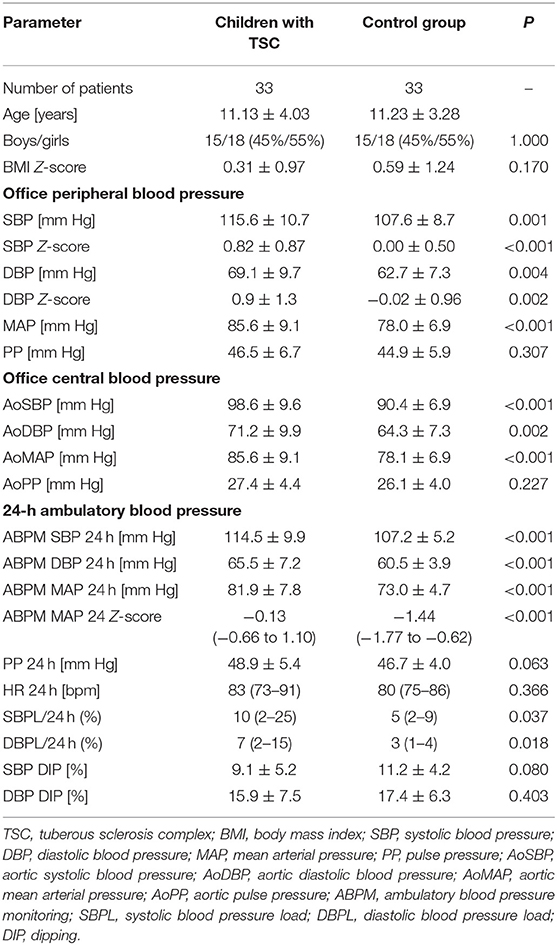
Table 2. Blood pressure in children with TSC and in healthy children.
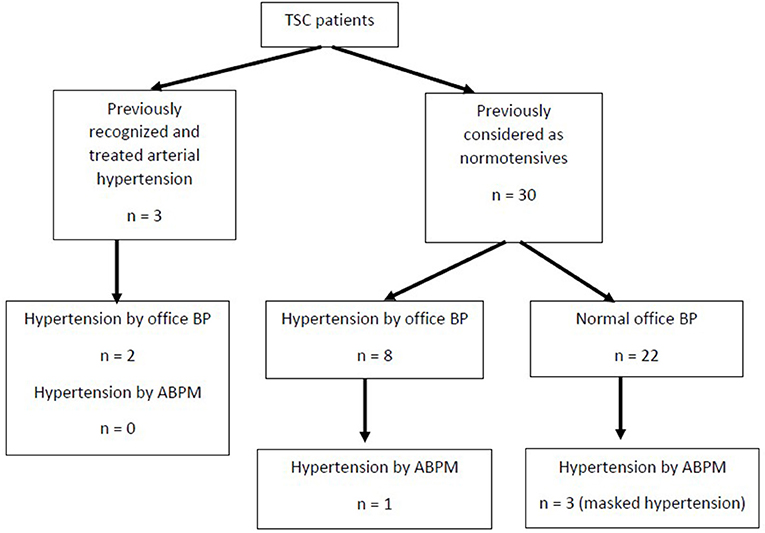
Figure 3. The results of blood pressure measurement in children with tuberous sclerosis complex (TSC, tuberous sclerosis complex; BP, blood pressure; ABPM, ambulatory blood pressure monitoring).
Parameters of arterial damage in both groups were presented in Table 3. Patients with TSC were characterized by significantly faster aortic pulse wave velocity (4.76 ± 0.81 vs. 4.25 ± 0.56 [m/s], p = 0.003) and thicker common carotid artery intima-media thickness (0.42 ± 0.05 vs. 0.39 ± 0.03 [mm], p = 0.011) than healthy individuals. There were no differences between the groups regarding augmentation index, subendocardial viability ratio, local carotid arterial dimension, or stiffness parameters. Central systolic blood pressure, aortic pulse wave velocity, and common carotid intima-media thickness in both groups were presented in Figures 4–6, respectively.
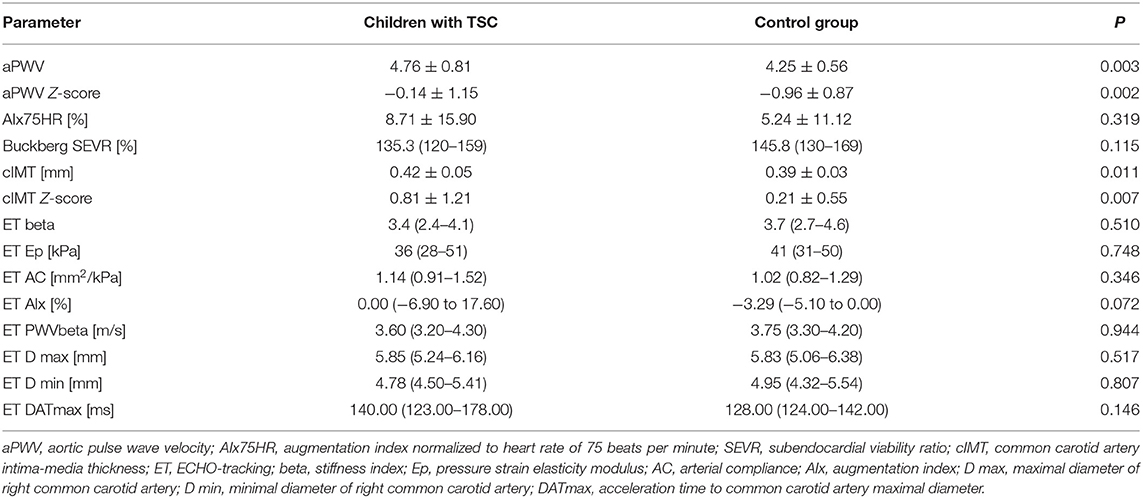
Table 3. Parameters of arterial damage (early vascular aging) in children with tuberous sclerosis complex and in healthy children.
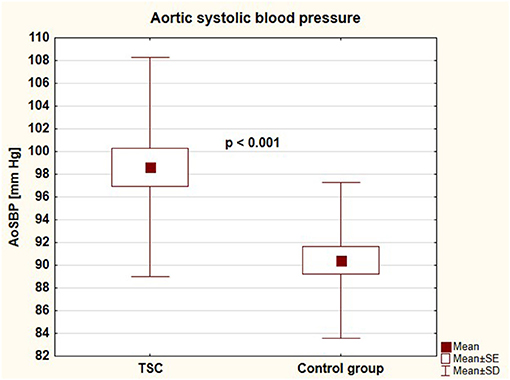
Figure 4. Aortic systolic blood pressure in children with tuberous sclerosis complex and in control group (AoSBP, aortic systolic blood pressure; TSC, tuberous sclerosis complex; SE, standard error; SD, standard deviation).
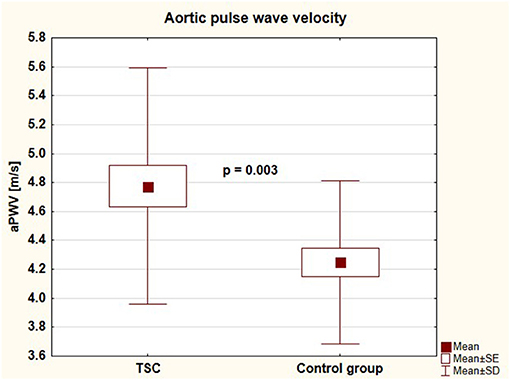
Figure 5. Aortic pulse wave velocity in children with tuberous sclerosis complex and in control group (aPWV, aortic pulse wave velocity; TSC, tuberous sclerosis complex; SE, standard error; SD, standard deviation).
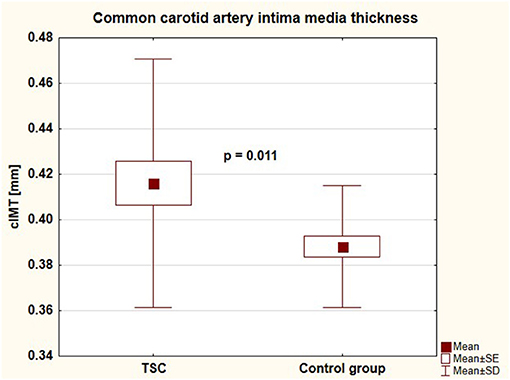
Figure 6. Common carotid artery intima media thickness in children with tuberous sclerosis complex and in control group (cIMT, common carotid artery intima media thickness; TSC, tuberous sclerosis complex; SE, standard error; SD, standard deviation).
When we excluded 7 children with arterial hypertension from the study group, we found that remaining 26 children with TSC were still characterized by significantly faster aortic pulse wave velocity (aPWV: 4.73 ± 0.83 vs. 4.25 ± 0.56 [m/s], p = 0.011, aPWV Z-score: −0.18 ± 1.18 vs. −0.96 ± 0.87, p = 0.006) and thicker common carotid artery intima media thickness (cIMT: 0.41 ± 0.05 vs. 0.39 ± 0.03 [mm], p = 0.042). The groups still did not differed in age (10.93 ± 4.07 vs. 11.23 ± 3.28 [years], p = 0.754) and sex (boys/girls-−11/15 vs. 15/18, p = 0.809).
In TSC patients, aortic systolic blood pressure and peripheral office diastolic blood pressure Z-score correlated significantly with maximal diameter of the renal cyst (R = 0.419, p = 0.033 and R = 0.484, p = 0.012, respectively). Aortic systolic blood pressure and mean arterial pressure during 24 h Z-score correlated with serum cystatin C concentration (r = 0.377, p = 0.030 and R = 0.433, p = 0.013, respectively).
Boys with TSC did not differ from girls in terms of aortic pulse wave velocity (aPWV [m/s]: 4.85 ± 0.84 vs. 4.72 ± 0.81 [m/s], p = 0.660; aPWV Z-score:−0.07 ± 1.12 vs.−0.21 ± 1,21, p = 0.752) or common carotid artery intima media thickness (cIMT [mm]: 0.43 ± 0.06 vs. 0.41 ± 0.05, p = 0.383; cIMT Z-score: 0.87 ± 1.14 vs. 0.75 ± 1.30, p = 0.797). We found a positive correlation between aPWV Z-score and daily urinary albumin loss (R = 0.412, p = 0.029) and trend toward a positive correlation between aPWV Z-score and maximal AML diameter (R = 0.339, p = 0.058).
As for parameters of local carotid artery stiffness in patients with TSC, pressure strain elasticity modulus (Ep) correlated with mean arterial pressure during 24 h Z-score (MAP 24 h Z-score) (R = 0.409, p = 0.020), arterial compliance (AC) correlated with systolic blood pressure load during 24 h (R = −0.367, p = 0.036) and with MAP 24 h Z-score (R = −0.538, p = 0.001) and local pulse wave velocity (PWVbeta) also correlated with MAP 24 h Z-score (R = 0.411, p = 0.019).
This is the first study to analyze central blood pressure and the phenomenon of early vascular aging in pediatric patients with tuberous sclerosis complex. We have compared our results with perfectly sex- and age-matched healthy peers. Our analysis revealed that TSC patients were characterized by significantly higher central systolic blood pressure, aortic pulse wave velocity, and common carotid artery intima-media thickness. We have found that blood pressure correlated with serum cystatin C and renal cyst diameter in this group of patients. There was also positive relation between pulse wave velocity and the extent of renal involvement. Parameters of local artery stiffness correlated with ambulatory blood pressure.
Our analysis has involved 33 children with already diagnosed TSC hospitalized in one tertiary center of pediatric nephrology. Our center has developed a program of nephrological care for pediatric TSC patients in 2017 based on ITSCCG and the Polish Society of Nephrology recommendations (16, 29). The preliminary analysis of our TSC cohort has already been published in a local medical journal (30). In addition, we aimed to analyze blood pressure and vascular phenotype in these patients. The clinical characteristics of our cohort do not differ from those of patients with TSC in large international registries including TOSCA registry (TuberOus SClerosis registry to increase disease Awareness) (3).
Renal lesions including AMLs were more frequently found in our group (90.9% of children) than in other pediatric patients groups—renal involvement is estimated to occur in approximately 38.5−55% of preschool children and 75–80% of schoolchildren (13, 20, 31, 32). The higher incidence of renal manifestations in our group results from the specificity of patients referred to our Department—the main indication was the presence of focal renal lesions found on imaging studies. In the analysis of patients from the TOSCA registry, AML lesions were present in 51.8% of patients (13). Renal cysts in most patients with TSC are small and localized in the subcortical region. Patients with simultaneous deletion of TSC2 and PKD1 genes are characterized by a very severe phenotype with large cysts from early childhood. Many of these patients develop a rapid progression to end-stage renal disease already in the second or third decade of life (13, 32). In our study group, renal cysts were found in three-quarters of patients. The largest cysts were found in two boys with a genetically confirmed mutation in the PKD1 gene. Of note, in our group of patients, hyperfiltration was found in as many as one-third of the subjects. This frequency is even higher than in the study of Belgian authors (20). It has been postulated that hyperfiltration in patients with TSC is caused by overactivation of the mTOR pathway in the glomerulus and, as in diabetic nephropathy, may be a risk factor for progression of renal disease.
In the analyzed group of patients with TSC, hypertension was present in 21.2% of patients, which is higher than the average prevalence of hypertension in the population of healthy children (3–5%) (33) and is also higher compared to the percentage of patients with hypertension in the Belgian study (13.0%) (20). In adults with TSC, arterial pressure has been shown to depend on the size and number of both AML lesions and cysts (32, 34). Severe hypertension in this group of patients may also be related to the presence of vascular lesions—renal artery stenosis sometimes accompanied by mid-aortic syndrome (MAS) (10). The ITSCCG recommendations clearly state the need for regular blood pressure measurements in this group of patients (1). The idea of measurement of central blood pressure has gained much attraction in recent years (35). Also, pediatric data indicate that central systolic blood pressure is a significant predictor of target organ damage, as valuable as 24-h peripheral blood pressure monitoring (36). We found that pediatric patients with TSC were characterized by a significantly higher central systolic blood pressure than healthy peers. Cystatin C and renal cyst diameter were significant determinants of elevated blood pressure in our cohort. The latter finding is consistent with the results of a multicenter study in children with autosomal dominant polycystic kidney disease (37) and adult TSC registries (32, 34).
Arterial damage is one of the first alterations observed in pediatric populations with increased cardiovascular risk, such as chronic kidney disease (CKD) (38), primary hypertension (PH) (39), diabetes mellitus (DM) type 1 (40), or familial hypercholesterolemia (41). Elastic properties of arteries in high-risk pediatric patients are similar to vascular changes in the elderly and are defined as early vascular aging. The concept of EVA is based on findings that individuals with PH, DM or CKD present with more advanced signs of arterial aging than their healthy peers (15, 42). Among different indices of EVA, evaluation of common carotid artery intima-media thickness and aortic (carotid-femoral) pulse wave velocity are considered as the most valuable ones with generally accepted pediatric normative values (27, 28, 43) and well-established association with hard-end points in the adult population (44, 45).
Our study is the first to reveal signs of EVA in pediatric patients with TSC. The primary cause of EVA in this group of patients is yet to be solved. Nevertheless, there is some possible explanation for this result. Firstly, vascular senescence in this population could be the effect of blood pressure rise as blood pressure is the primary determinant of cIMT and aPWV in the general pediatric population (27, 43). Moreover, initial functional and morphological vascular changes can be regarded as adaptive in response to increased blood pressure (42). Indeed, office peripheral and central blood pressure was significantly higher in this group of TSC patients compared to healthy age- and sex-matched peers. Nevertheless, blood pressure remained within normal limits in most of these patients, and arterial hypertension was found in approximately 20% of the studied children. In addition, no significant correlation between blood pressure and parameters of arterial damage except for carotid artery stiffness has been revealed in our patients. Also, cIMT and aPWV were still elevated in TSC patients after the exclusion of 7 hypertensive children. Metabolic factors do not seem to play a role either, as these children generally had normal lipid parameters and did not differ in BMI from the control group. Thus, it is possible that other factors might be to blame.
Vascular anomalies have been described in TSC patients for decades (9, 10), including renal artery stenosis (sometimes with the mid-aortic syndrome) and aortal aneurysms also in small children. The youngest reported TSC case is an infant who died of aortic aneurysm rupture at the age of 4.5 months (46). Vascular smooth muscle cells (SMCs) are not terminally differentiated and can transform to proliferating and migrating cells with loss of contractile protein expression and increased synthesis of extracellular matrix proteins. In SMCs, mTOR signaling was found to influence cell differentiation. Cao et al. revealed in an experimental model that the activation of the mTOR pathway with Tsc2 deficiency leads to SMC proliferation and de-differentiation in vitro and in vivo, which can be reversed with rapamycin treatment (8). Recently, a disruption of the Tsc1 gene was also found to induce a degradative smooth muscle cell phenotype (47). The authors hypothesize that the proliferation of degradative SMCs within the media causes arterial dysfunction in TSC patients. A histological study of a thoracoabdominal aneurysm in a child with TSC revealed SMC hyperplasia in the inner media with diminished actin expression and extensive fragmentation of elastic fibers (8). Our preliminary results suggest that the proliferation and degradation of vascular SMCs are already present in children with TSC without macroscopically evident arterial dilations or stenoses.
In addition, the extent of renal involvement might play a role in the development of blood pressure rise and arterial damage as blood pressure was associated with cystatin C and cyst diameter and aortic pulse wave velocity with urine albumin loss and AML diameter. A positive correlation between albuminuria and arterial stiffness has been revealed in adults with CKD (48) and DM 2 (49) and in the general young adult population from the Malmö offspring study (50). Albuminuria is not only a marker of renal damage but is a well-established indicator of endothelial dysfunction, which may result in an altered arterial wall and increased arterial stiffness. Gil-Ortega et al. found that increased albuminuria was associated with abnormalities in arterial wall structure (elastin loss) in an experimental rat model (51). A similar association might also be seen in TSC patients. Inversely, increased urinary albumin loss could be the result of the downstream transmission of pressure pulsatility to the level of renal microcirculation (52).
TSC is one of those rare entities for which there is a targeted treatment that directly affects the mechanism of the disease. Numerous data from both single case reports and multicenter clinical trials indicate high efficacy of mTOR inhibitors (everolimus and sirolimus/rapamycin) in the treatment of virtually all symptoms of the disease, including central nervous system lesions (53), renal AML (54) or lung lesions (55). The timing of initiation of mTOR inhibitors in TSC patients is a matter of debate. Recent multicenter studies have proven the safety and efficacy of mTOR inhibition in TSC patients even younger than 2 years (56, 57). Of note, in vitro studies showed that the mTOR inhibitor rapamycin promotes SMC differentiation toward a contractile phenotype (58). Inhibition of the mTOR signaling pathway has been used for many years in medicine in rapamycin-diluting stents that prevent SMC proliferation and artery occlusion after percutaneous interventions (59). There is already some evidence indicating that early treatment in high-risk children and adolescents [e.g., in patients with CKD (60) or PH (61)] could reverse EVA and possibly prevent premature cardiovascular events. Whether mTOR inhibitor treatment or any other medical measures (e.g., antihypertensive treatment) would prevent or even reverse negative alterations in arteries of TSC patients is still unknown and should certainly be investigated in years to come.
Some limitations to our research need to be listed. Firstly, the study's cross-sectional nature precludes drawing final conclusions on the relation between blood pressure, arterial damage, and clinical parameters in the studied TSC patients (e.g., the link between aPWV and albuminuria). Secondly, the study population was small and heterogeneous in terms of age, presence of arterial hypertension, the extent of renal involvement, genetic background (TSC1, TSC2, TSC2+PKD1), and treatment with mTOR inhibitors. As arterial hypertension was recognized previously in only 3 patients, we could not analyze the influence of duration of hypertension on arterial damage in TSC patients.
Children with tuberous sclerosis complex are at risk of elevated central blood pressure and early vascular aging. In this group of patients, early vascular aging might be caused by uncontrolled activation of the mTOR signaling pathway in vascular smooth muscle cells. Additionally, in children with TSC, blood pressure and arterial stiffness are related to renal involvement. There is a need for studies on possible vasoprotective measures in TSC patients, including the use of mTOR inhibitors.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Bioethics Committee, Medical University of Warsaw (approval no. KB/145/2017, 4th July 2017). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin and the participants (≥16 years).
PS, AMW, and MS drafted and revised the manuscript. PS, SJ, MB, and MP-T contributed to the conception and design of the work. PS, AMW, MS, MB, AJ-K, and PB contributed to the acquisition of data. PS, AMW, MS, SJ, MB, AJ-K, PB, and MP-T contributed to the analysis or interpretation of the data. SJ and MP-T critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of this work ensuring its integrity and accuracy.
This research was funded from the statutory funds of the Department of Pediatrics and Nephrology, Medical University of Warsaw.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Northrup H, Aronow ME, Bebin EM, Bissler J, Darling TN, de Vries PJ, et al. Updated international tuberous sclerosis complex diagnostic criteria and surveillance and management recommendations. Pediatr Neurol. (2021) 123:50–66. doi: 10.1016/j.pediatrneurol.2021.07.011
2. Tyburczy ME, Dies KA, Glass J, Camposano S, Chekaluk Y, Thorner AR, et al. Mosaic and Intronic Mutations in TSC1/TSC2 Explain the majority of TSC Patients with no mutation identified by conventional testing. PLoS Genet. (2015) 11:e1005637. doi: 10.1371/journal.pgen.1005637
3. Kingswood JC, d'Augères GB, Belousova E, Ferreira JC, Carter T, Castellana R, et al. TuberOus SClerosis registry to increase disease Awareness (TOSCA)—baseline data on 2093 patients. Orphanet J Rare Dis. (2017) 12:2. doi: 10.1186/s13023-016-0553-5
4. Trnka P, Kennedy SE. Renal tumors in tuberous sclerosis complex. Pediatr Nephrol. (2021) 36: 1427–38. doi: 10.1007/s00467-020-04775-1
5. Lam HC, Siroky BJ, Henske EP. Renal disease in tuberous sclerosis complex: pathogenesis and therapy. Nat Rev Nephrol. (2018) 14:704–16. doi: 10.1038/s41581-018-0059-6
6. Vos N, Oyen R. Renal angiomyolipoma: the good, the bad, and the ugly. J Belg Soc Radiol. (2018) 102:41. doi: 10.5334/jbsr.1536
7. Bellini C, Bersi MR, Caulk AW, Ferruzzi J, Milewicz DM, Ramirez F, et al. Comparison of 10 murine models reveals a distinct biomechanical phenotype in thoracic aortic aneurysms. J R Soc Interface. (2017) 14:20161036. doi: 10.1098/rsif.2016.1036
8. Cao J, Gong L, Guo DC, Mietzsch U, Kuang SQ, Kwartler CS, et al. Thoracic aortic disease in tuberous sclerosis complex: molecular pathogenesis and potential therapies in Tsc2+/- mice. Hum Mol Genet. (2010) 19: 1908–20. doi: 10.1093/hmg/ddq066
9. Defraigne JO, Paquot JP, Creemers E, Limet R. Aneurysm of the abdominal aorta in an eighteen-month-old child. Ann Vasc Surg. (1988) 2:193–5. doi: 10.1016/S0890-5096(06)60805-4
10. Salerno AE, Marsenic O, Meyers KE, Kaplan BS, Hellinger JC. Vascular involvement in tuberous sclerosis. Pediatr Nephrol. (2010) 25:1555–61. doi: 10.1007/s00467-010-1466-5
11. Patzer L, Basche S, Misselwitz J. Renal artery stenosis and aneurysmatic dilatation of arteria carotis interna in tuberous sclerosis complex. Pediatr Nephrol. (2002) 17:193–6. doi: 10.1007/s00467-001-0799-5
12. Wong H, Hadi M, Khoury T, Geary D, Rubin B, Filler G. Management of severe hypertension in a child with tuberous sclerosis-related major vascular abnormalities. J Hypertens. (2006) 24:597–9. doi: 10.1097/01.hjh.0000209994.33680.11
13. Kingswood JC, Belousova E, Benedik MP, Carter T, Cottin V, Curatolo P, et al. Renal angiomyolipoma in patients with tuberous sclerosis complex: findings from the TuberOus SClerosis registry to increase disease Awareness. Nephrol Dial Transplant. (2019) 34: 502-508. doi: 10.1093/ndt/gfy063
14. Kruger R, Gafane-Matemane LF, Kagura J. Racial differences of early vascular aging in children and adolescents. Pediatr Nephrol. (2021) 36:1087–108. doi: 10.1007/s00467-020-04593-5
15. Climie RE, Park C, Avolio A, Mynard JP, Kruger R, Bruno RM. Vascular ageing in youth: a call to action. Heart Lung Circ. (2021) 30:1613–26. doi: 10.1016/j.hlc.2021.06.516
16. Northrup H, Krueger DA. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. (2013) 49:243–54. doi: 10.1016/j.pediatrneurol.2013.08.001
17. Kułaga Z, Litwin M, Tkaczyk M, Palczewska I, Zajaczkowska M, Zwolińska D, et al. Polish 2010 growth references for school-aged children and adolescents. Eur J Pediatr. (2011) 170:599–609. doi: 10.1007/s00431-010-1329-x
18. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. (2009) 20:629–37. doi: 10.1681/ASN.2008030287
19. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. (2013) 3:1–150. doi: 10.1038/kisup.2012.73
20. Janssens P, Van Hoeve K, De Waele L, De Rechter S, Claes KJ, Van de Perre E, et al. Renal progression factors in young patients with tuberous sclerosis complex: a retrospective cohort study. Pediatr Nephrol. (2018) 33:2085–93. doi: 10.1007/s00467-018-4003-6
21. Stewart J, McCallin T, Martinez J, Chacko S, Yusuf S. Hyperlipidemia. Pediatrics Rev. (2020) 41:393–402. doi: 10.1542/pir.2019-0053
22. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. (2008) 359:1811–21. doi: 10.1056/NEJMra0800885
23. Kułaga Z, Litwin M, Grajda A, Kułaga K, Gurzkowska B, Gózdz M, et al. Oscillometric blood pressure percentiles for Polish normal-weight school-aged children and adolescents. J Hypertens. (2012) 30:1942–54. doi: 10.1097/HJH.0b013e328356abad
24. Grajda A, Kułaga Z, Gurzkowska B, Wojtyło M, Gózdz M, Litwin M. Preschool children blood pressure percentiles by age and height. J Hum Hypertens. (2017) 31:400–8. doi: 10.1038/jhh.2016.90
25. Flynn JT, Daniels SR, Hayman LL, Maahs DM, McCrindle BW, Mitsnefes M, et al. Update: ambulatory blood pressure monitoring in children and adolescents: a scientific statement from the American Heart Association. Hypertension. (2014) 63:1116–35. doi: 10.1161/HYP.0000000000000007
26. Stergiou GS, Palatini P, Parati G, O'Brien E, Januszewicz A, Lurbe E, et al. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens. (2021) 39:1293–302. doi: 10.1097/HJH.0000000000002843
27. Doyon A, Kracht D, Bayazit AK, Deveci M, Duzova A, Krmar RT, et al. Carotid artery intima-media thickness and distensibility in children and adolescents: reference values and role of body dimensions. Hypertension. (2013) 62:550–6. doi: 10.1161/HYPERTENSIONAHA.113.01297
28. Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, et al. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension. (2010) 56:217–24. doi: 10.1161/HYPERTENSIONAHA.110.152686
29. Dębska-Ślizień A, Tarasewicz A, Król E, Matuszewski M, Wierzba J, Szurowska E, et al. The recommendations for the management of tuberous sclerosis complex patients with kidney manifestation. The consensus statement of Tuberous Sclerosis Complex Work Group of Polish Society of Nephrology. Nefrol Dial Pol. (2016) 20:134–47.
30. Skrzypczyk P, Wojciechowska B, Szydło A, Jóźwiak S, Brzewski M, Bombiński P, et al. Evaluation of renal lesions in children with tuberous sclerosis - summary of the first year of 512 follow-up program. Pol Merkur Lekarski. (2019) 47:52–9.
31. Józwiak S, Schwartz RA, Janniger CK, Bielicka-Cymerman J. Usefulness of diagnostic 514 criteria of tuberous sclerosis complex in pediatric patients. J Child Neurol. (2000) 15:652–9. doi: 10.1177/088307380001501003
32. Rakowski SK, Winterkorn EB, Paul E, Steele DJ, Halpern EF, Thiele EA. Renal manifestations of tuberous sclerosis complex: incidence, prognosis, and predictive factors. Kidney Int. (2006) 70:1777–82. doi: 10.1038/sj.ki.5001853
33. Bell CS, Samuel JP, Samuels JA. Prevalence of Hypertension in Children. Hypertension. (2019) 73:148–52. doi: 10.1161/HYPERTENSIONAHA.118.11673
34. Eijkemans MJ, van der Wal W, Reijnders LJ, Roes KC, van Waalwijk van Doorn-Khosrovani SB, Pelletier C, et al. Long-term follow-up assessing renal angiomyolipoma treatment patterns, morbidity, and mortality: an observational study in tuberous sclerosis complex patients in the Netherlands. Am J Kidney Dis. (2015) 66:638–45. doi: 10.1053/j.ajkd.2015.05.016
35. Palatini P, Rosei EA, Avolio A, Bilo G, Casiglia E, Ghiadoni L, et al. Isolated systolic hypertension in the young: a position paper endorsed by the European Society of Hypertension. J Hypertens. (2018) 36:1222–36. doi: 10.1097/HJH.0000000000001726
36. Litwin M, Obrycki Ł, Niemirska A, Sarnecki J, Kułaga Z. Central systolic blood pressure and central pulse pressure predict left ventricular hypertrophy in hypertensive children. Pediatr Nephrol. (2019) 34:703–12. doi: 10.1007/s00467-018-4136-7
37. Massella L, Mekahli D, Paripović D, Prikhodina L, Godefroid N, Niemirska A, et al. Prevalence of hypertension in children with early-stage ADPKD. Clin J Am Soc Nephrol. (2018) 13:874–83. doi: 10.2215/CJN.11401017
38. Taşdemir M, Eroglu AG, Canpolat N, Konukoglu D, Agbaş A, Sevim MD, et al. Cardiovascular alterations do exist in children with stage-2 chronic kidney disease. Clin Exp Nephrol. (2016) 20:926–33. doi: 10.1007/s10157-016-1234-3
39. Litwin M, Trelewicz J, Wawer Z, Antoniewicz J, Wierzbicka A, Rajszys P, et al. Intima-media thickness and arterial elasticity in hypertensive children: controlled study. Pediatr Nephrol. (2004) 19:767–74. doi: 10.1007/s00467-004-1480-6
40. Galler A, Heitmann A, Siekmeyer W, Gelbrich G, Kapellen T, Kratzsch J, et al. Increased arterial stiffness in children and adolescents with type 1 diabetes: no association between arterial stiffness and serum levels of adiponectin. Pediatr Diabetes. (2010) 11:38–46. doi: 10.1111/j.1399-5448.2009.00525.x
41. Kusters DM, Wiegman A, Kastelein JJ, Hutten BA. Carotid intima-media thickness in children with familial hypercholesterolemia. Circ Res. (2014) 114:307–10. doi: 10.1161/CIRCRESAHA.114.301430
42. Litwin M, Feber J, Ruzicka M. Vascular aging: lessons from pediatric hypertension. Can J Cardiol. (2016) 32:642–9. doi: 10.1016/j.cjca.2016.02.064
43. Thurn D, Doyon A, Sözeri B, Bayazit AK, Canpolat N, Duzova A, et al. Aortic pulse wave velocity in healthy children and adolescents: reference values for the Vicorder device and modifying factors. Am J Hypertens. (2015) 28:1480–8. doi: 10.1093/ajh/hpv048
44. Willeit P, Tschiderer L, Allara E, Reuber K, Seekircher L, Gao L, et al. Carotid intima-media thickness progression as surrogate marker for cardiovascular risk: meta-analysis of 119 clinical trials involving 100 667 patients. Circulation. (2020) 142:621–42. doi: 10.1161/CIRCULATIONAHA.120.046361
45. Sequí-Domínguez I, Cavero-Redondo I, Álvarez-Bueno C, Pozuelo-Carrascosa DP, Nuñez de Arenas-Arroyo S, Martínez-Vizcaíno V. Accuracy of pulse wave velocity predicting cardiovascular and all-cause mortality. a systematic review and meta-analysis. J Clin Med. (2020) 9:2080. doi: 10.3390/jcm9072080
46. Lavocat MP, Teyssier G, Allard D, Tronchet M, Freycon F. Abdominal aortic aneurysm and Bourneville's tuberous sclerosis. Pediatrie. (1992) 47:517–9.
47. Li G, Wang M, Caulk AW, Cilfone NA, Gujja S, Qin L, et al. Chronic mTOR activation induces a degradative smooth muscle cell phenotype. J Clin Invest. (2020) 130:1233–51. doi: 10.1172/jci131048
48. Kalaitzidis RG, Karasavvidou DP, Tatsioni A, Pappas K, Katatsis G, Liontos A, et al. Albuminuria as a marker of arterial stiffness in chronic kidney disease patients. World J Nephrol. (2015) 4:406–14. doi: 10.5527/wjn.v4.i3.406
49. Smith A, Karalliedde J, De Angelis L, Goldsmith D, Viberti G. Aortic pulse wave velocity and albuminuria in patients with type 2 diabetes. J Am Soc Nephrol. (2005) 16:1069–75. doi: 10.1681/ASN.2004090769
50. Swärd P, Tofik R, Bakoush O, Torffvit O, Nilsson PM, Christensson A. Patterns of urinary albumin and IgM associate with markers of vascular ageing in young to middle-aged individuals in the Malmö offspring study. BMC Cardiovasc Disord. (2020) 20:358. doi: 10.1186/s12872-020-01638-3
51. Gil-Ortega M, García-Prieto CF, Ruiz-Hurtado G, Steireif C, González MC, Schulz A, et al. Genetic predisposition to albuminuria is associated with increased arterial stiffness: role of elastin. Br J Pharmacol. (2015) 172:4406–18. doi: 10.1111/bph.13223
52. Climie RE, Gallo A, Picone DS, Di Lascio N, van Sloten TT, Guala A, et al. Measuring the interaction between the macro- and micro-vasculature. Front Cardiovasc Med. (2019) 6:169. doi: 10.3389/fcvm.2019.00169
53. Franz DN, Belousova E, Sparagana S, Bebin EM, Frost M, Kuperman R, et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. (2013) 381:125–32. doi: 10.1016/S0140-6736(12)61134-9
54. Bissler JJ, Kingswood JC, Radzikowska E, Zonnenberg BA, Frost M, Belousova E, et al. Everolimus for angiomyolipoma associated with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis (EXIST-2): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. (2013) 381:817–24. doi: 10.1016/S0140-6736(12)61767-X
55. Aghaeimeybodi F, Najafizadeh K, Razavi-Ratki SK, Namiranian N. Effects of sirolimus on lung function in patients with lymphangioleiomyomatosis. Caspian J Intern Med. (2019) 10:7–10. doi: 10.22088/cjim.10.1.7
56. Saffari A, Brösse I, Wiemer-Kruel A, Wilken B, Kreuzaler P, Hahn A, et al. Safety and efficacy of mTOR inhibitor treatment in patients with tuberous sclerosis complex under 2 years of age—a multicenter retrospective study. Orphanet J Rare Dis. (2019) 14:96. doi: 10.1186/s13023-019-1077-6
57. Krueger DA, Capal JK, Curatolo P, Devinsky O, Ess K, Tzadok M, et al. Short-term safety of mTOR inhibitors in infants and very young children with tuberous sclerosis complex (TSC): multicentre clinical experience. Eur J Paediatr Neurol. (2018) 22:1066–73. doi: 10.1016/j.ejpn.2018.06.007
58. Martin KA, Merenick BL, Ding M, Fetalvero KM, Rzucidlo EM, Kozul CD, et al. Rapamycin promotes vascular smooth muscle cell differentiation through insulin receptor substrate-1/phosphatidylinositol 3-kinase/Akt2 feedback signaling. J Biol Chem. (2007) 282:36112–20. doi: 10.1074/jbc.M703914200
59. Abizaid A. Sirolimus-eluting coronary stents: a review. Vasc Health Risk Manag. (2007) 3:191–201. doi: 10.2147/vhrm.2007.3.2.191
60. Litwin M, Wühl E, Jourdan C, Trelewicz J, Niemirska A, Fahr K, et al. Altered morphologic properties of large arteries in children with chronic renal failure and after renal transplantation. J Am Soc Nephrol. (2005) 16:1494–500. doi: 10.1681/ASN.2004110932
Keywords: tuberous sclerosis complex, early vascular aging, central blood pressure, arterial stiffness, common carotid artery intima-media thickness, arterial hypertension, children
Citation: Skrzypczyk P, Wabik AM, Szyszka M, Józwiak S, Bombiński P, Jakimów-Kostrzewa A, Brzewski M and Pańczyk-Tomaszewska M (2021) Early Vascular Aging in Children With Tuberous Sclerosis Complex. Front. Pediatr. 9:767394. doi: 10.3389/fped.2021.767394
Received: 30 August 2021; Accepted: 09 November 2021;
Published: 29 November 2021.
Edited by:
Mieczyslaw Litwin, Children's Memorial Health Institute (IPCZD), PolandReviewed by:
Stella Stabouli, Aristotle University of Thessaloniki, GreeceCopyright © 2021 Skrzypczyk, Wabik, Szyszka, Józwiak, Bombiński, Jakimów-Kostrzewa, Brzewski and Pańczyk-Tomaszewska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Piotr Skrzypczyk, cHNrcnp5cGN6eWtAd3VtLmVkdS5wbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.