
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 10 September 2021
Sec. Children and Health
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.738294
This article is part of the Research Topic Effective Strategies for Promoting Health-Enhancing Children's Physical Activity View all 19 articles
 Giuseppe Battaglia1
Giuseppe Battaglia1 Valerio Giustino1*
Valerio Giustino1* Garden Tabacchi1Massimo Lanza2
Garden Tabacchi1Massimo Lanza2 Federico Schena2Valentina Biino2Matteo Giuriato2
Federico Schena2Valentina Biino2Matteo Giuriato2 Maria Chiara Gallotta3Laura Guidetti4
Maria Chiara Gallotta3Laura Guidetti4 Carlo Baldari5Antonino Gennaro6
Carlo Baldari5Antonino Gennaro6 Antonio Palma1
Antonio Palma1 Marianna Bellafiore1
Marianna Bellafiore1Although numerous evidences reported a negative correlation between motor coordination (MC) and overweight/obesity in children and adolescents, the interrelationship between age, gender, and weight status is still debatable. Hence, the aim of this cross-sectional study was to examine the association between MC and weight status according to age and gender across childhood and early adolescence in a large sample of Italian elementary and middle school students. A number of 1961 Italian school students (1,026 boys, 935 girls) was stratified in three consecutive age groups (6–7, 8–10, and 11–13 years) and four weight status categories (underweight, normal weight, overweight, and obese) according to Cole's body mass index (BMI) cut-off points for children. MC performance was assessed measuring motor quotient (MQ) with the Körperkoordinationstest für Kinder (KTK). Results showed significantly lower MQ levels in children in overweight (OW) and with obesity (OB) in both sexes for all age groups than peers in normal weight (NW), except in 6–7-year-old boys. Girls in OW and with OB had similar MQ levels across all age groups, while younger boys in OW and with OB showed higher MQ levels than older ones (p < 0.05). The 6–7-year-old boys showed better MQ levels than girls peers in NW, OW, and with OB, while 8–10-year-old boys in underweight (UW), NW, and OW; and 11–13-year-old boys only in NW (p < 0.05). No interaction effect was found between age, gender, and weight status on MQ levels. These outcomes showed the negative impact of higher weight status on MC performance according to age and gender, pointing out the importance of planning targeted motor programs that consider these variables to improve MC performance.
Motor coordination (MC), or motor competence, is a term that describes the ability to perform both fine and gross motor skills (1, 2). It is widely recognized that an adequate level of MC in children is fundamental to develop specialized sequences of movement for daily life tasks and for organized and non-organized physical activities. For this reason, it is crucial that a high level of MC is developed during the preschool and primary school period, to be perfected later (1, 3–6).
Furthermore, the scientific literature has highlighted the role of MC development on the consequent childhood obesity prevention and, similarly, several studies have highlighted the influence of body weight status on MC performance (7–11). The development of MC in children may be an important contributing factor to negative or positive weight trajectories (9, 12, 13). The importance of an adequate development in motor skills is also given by the fact that previous studies reported that childhood obesity involves not only locomotion and object control skills but also the ability in executing basic daily life activities (14).
Moreover, there is a body of studies in this field that have emphasized the relationship between MC and the practice of physical activity (PA) (15–17). As a matter of fact, D'Hondt et al. (9) showed that the associations between PA, MC, and body weight generally increase in childhood (9, 13).
In this perspective, the relationship between MC and weight status has been extensively studied in children and adolescents in overweight (OW) and with obesity (OB) showing impaired development of motor skills (18–21). To the best of our knowledge, an inverse relationship exists between body mass index (BMI) and MC in childhood and adolescence with similar associations between girls and boys over time (9, 12, 13, 21).
Although evidences suggest a negative correlation between MC performance and excess body mass (22–24), this relationship still remains debatable. In particular, there is a body of articles suggesting that children and adolescents in OW and with OB show lower level of MC than their peers in healthy-weight, regardless of age (21, 25–29).
Some research groups have investigated the association between children's body weight status and gross motor performances based on gender, reporting different results (29, 30). For instance, Cawley et al. (31) reported reduced MC only in boys with OB, while no differences were found among girls with OB girls and peers in normal weight (NW) (31).
The prevalence of children in OW and with OB is increasing worldwide, representing one of the most serious public health conditions nowadays and, as stated above, this weight status is related to sedentary behaviors and consequent lower MC proficiency (11, 32, 33). In detail, in Italy the prevalence of children in OW and with OB is 22.5 and 9.3%, respectively (34).
Therefore, the purpose of this study was to analyse the association between MC, assessed by the Körperkoordinationstest für Kinder (KTK), and weight status in 6– to 13-year-old Italian boys and girls. Moreover, we investigated the association between performances of KTK subtests (i.e., walking backward, jumping sideways, hopping for height, and moving sideways), and weight status according to age and gender.
Although some researches have investigated MC performance in different Italian regions during childhood and adolescence (26, 35), this study is the first to consider a large sample from all over the nation and taking into account the influence of weight status, age, and gender. The novelty of the study is not only the large sample recruited, but also the investigation of all subtest performances according to weight status, age, and gender.
We hypothesized that weight status similarly affects the levels of MC in girls and boys. In particular, children and adolescents with higher BMI (i.e., in OW and with OB) should show lower levels of MC than their peers in NW. Furthermore, we expected to find higher levels of motor competence in boys than girls, and in adolescents than children. As for the subtest performances, we expected that body weight could affect differently depending on the specificity of each subtest, that is, we hypothesized to find scores gradually decreasing with increasing body weight in motor skills that required greater effort to counteract the force of gravity (i.e., jumping sideways and hopping for height), regardless of age and gender.
A number of 1,961 participants (boys: n = 1,026; girls: n = 935), between 6 and 13 years of age (Table 1) were recruited from elementary and middle schools in northern, central, and southern Italy, chosen as widely representative schools of the three Italian geographical areas. The measurements of this cross-sectional study were conducted in the participating schools from January 2019 to February 2020 during the regular school hours and in the respective school gyms.
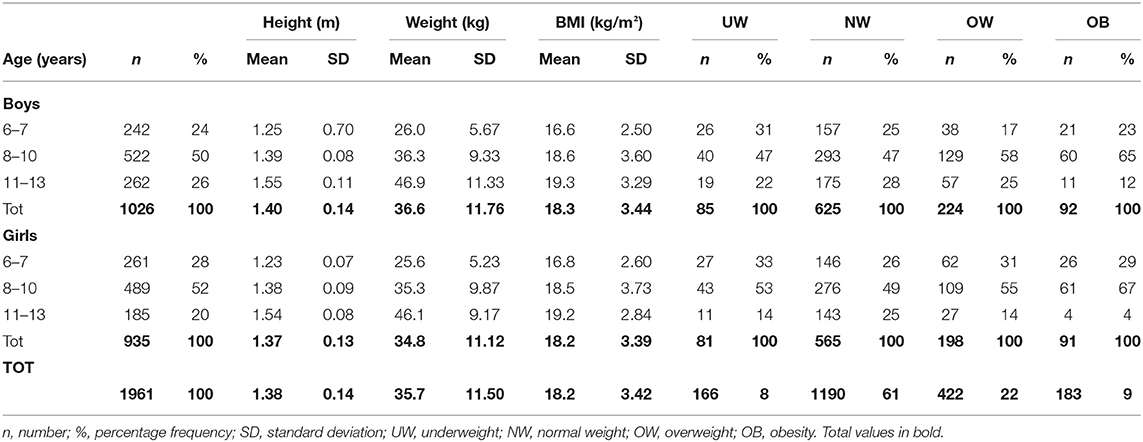
Table 1. Descriptive statistics for weight status categories and gender classes stratified by age groups.
This multicentre study has been led by department of Neuroscience, Biomedicine and Movement (University of Verona) and approved by the Ethical Board of Verona University (No. 2019-UNVRCLE-0298910) and Palermo University (No. 8/2019). The study complies with the criteria for the use of people in research defined in the Declaration of Helsinki. Moreover, school principals/administrators provided further authorizations for the study. After researchers explained the purpose of the investigation and the research methodology, all parents provided written informed consent prior to participating in the study.
As for the anthropometric measurements, participants' body weight (kg) and height (m) were measured using an electronic scale and a standard audiometer to the nearest 0.5 kg and 0.1 cm, respectively. Body mass index (BMI) was computed as body weight divided by height squared (kg/m2). All measures were collected by examiners who were trained in the measurement methods of height and weight.
According to the Cole's BMI percentiles for boys and girls aged 2–18 years (36), the following four categories of weight status were obtained: underweight (UW) below the 5th percentile, normal weight (NW) between 5th and 85th percentile, overweight (OW) between 85th and 95th percentile, and obesity (OB) over the 95th percentile.
Motor coordination (MC) was measured using the Körperkoordinationstest für Kinder (i.e., a body coordination test for children, referred to as KTK) by examiners who were trained in the administration of the KTK (37, 38). The KTK is a standardized, norm-referenced measure for age and gender that allows to assess MC, expressed as motor quotient (MQ), in children aged 5–14 years. The KTK was administered and scored according to the manual guidelines.
The test protocol included four subtests: (1) walking backward (WB) on a balance beam of 3 m in length of decreasing widths (6, 4.5, and 3 cm); (2) jumping sideways (JS) on two feet from side to side over a small beam (60 × 4 × 2cm) as fast as possible for 15 s; (3) hopping for height (HH) on one foot over a foam obstacle of increasing height (consecutive increments of 5 cm); (4) moving sideways (MS) on the floor in 20 s by stepping from one plate (25 × 25 × 2 cm, supported on four legs 3.7 cm high) to the next, moving onto the first plate, step ping on it, and so on.
The total MQ, standardized for age and gender, was calculated starting from the raw scores of each subtest, according to normative data tables provided by the manual. The total MQ was calculated by adding the four subtest scores. As indicated by Kiphard and Schilling (2007) KTK showed acceptable construct validity (38). In the test-retest for the raw score on the total test battery the reliability coefficient was 0.97, while corresponding coefficients for each subtest ranged from 0.80 to 0.96 (38).
For statistical analyses, participants were divided according to the four weight status categories aforementioned, three consecutive age groups (6–7, 8–10, and 11–13 years), and gender classes.
The Shapiro-Wilk test for normality was initially used to evaluate the distribution of data. Means and Standard Deviations (SD) of weight, height, and BMI were calculated. Number and percentage frequencies were displayed to describe the weight status by age and gender. The Chi-Square test was carried out to study any significance between frequencies of weight status categories according to age groups. The scores of the KTK performance were calculated and showed as means and SDs by age groups, gender classes, and weight status categories.
The one-way Analysis of Variance (ANOVA) with Bonferroni's correction was initially performed separately between the MQ/subtest scores and weight status, age, and gender to explore the influence of each of these three variables. In order to examine any significant difference across weight status categories according to age groups and gender classes, across age groups according to weight status categories and gender classes, and across gender classes according to weight status categories and age groups, the one-way ANOVA analyses were subsequently performed. The results of the one-way ANOVA were displayed through the F-values and level of significance, which was set at p < 0.05.
The three-way ANOVA was run to examine if there was an interaction effect between the independent variables weight status, age, and gender on MQ and subtests scores. The interaction results were showed as partial sum of squares (SS) that helps express the total variation that can be attributed to the single factors and to the interaction of factors, and degrees of freedom (df), F-values, and level of significance were also provided. The adjusted predictions of weight status, age, and gender on MQ were plotted in a graph.
The software STATA/MP 12.1 (StataCorp LP, College Station, TX, USA) was used to perform the statistical analyses.
Descriptive statistics of the participants are presented in Table 1, which shows data on the frequency of boys and girls in UW, NW, OW, and with OB categories by age groups (6–7, 8–10, 11–13 years old). The prevalence of UW, NW, OW, and with OB was 8, 61, 22, and 9%, respectively. In particular, the prevalence of participants in OW was significantly higher (p < 0.05) in 6–7-year-old girls than boys of the same age range (31 vs. 17%), while it was significantly lower (p < 0.05) in 11–13-year-old boys than girls' peers (14 vs. 25%). Higher prevalence of participants with OB was found out in boys aged 11–13-year-old than girls in the same age range (12 vs. 4%), but this difference was not significant.
The one-way ANOVA between MQ and weight status, age, and gender revealed that these three variables were strongly associated with MQ. In detail, MQ level was progressively reduced (p < 0.001) in: (1) weight status categories from UW/NW (in these two categories performances were not different) to OW and OB (F = 37.66); (2) older than younger ones (F = 25.25); (3) girls than boys (F = 67.22) (Table 2). The same trend was evidenced for the MS and HH subtests, with MS showing a very high significance (F = 128.41) across age groups, and HH across gender categories (F = 53.84). A significant (p < 0.001) inverse trend was revealed for the WB subtest, with performance significantly increasing in older participants (F = 12.64) and in girls (F = 17.47), while scores were decreasing in OW and OB categories (F = 40.38). No differences were found for the JS subtest across age groups, while decreasing performance was found out for girls (F = 268.38) and higher weight status categories (F = 15.82) (Table 2).
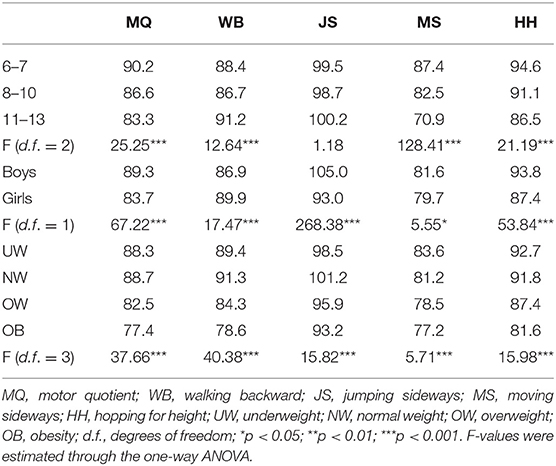
Table 2. Total MQ and subtest scores of the KTK by age groups, gender classes, and weight status categories, with F-values and significance levels across the single categories.
Significant differences were found out across weight status categories (decreasing performances from participants in OW to participants with OB), both in boys and girls and in all the age groups except for 6–7-year-old boys (Table 3). The strongest significant differences (p < 0.001) were evinced across the age groups 8–10 and 11–13 in boys (F = 13.45 and F = 10.61, respectively), and across the age group 8–10 in girls (F = 14.17); while the weakest changes in performance were revealed in age groups 6–7 and 11–13 in girls (F = 4.86, p < 0.01, and F = 2.81, p < 0.05, respectively). In most cases, performances in participants in UW were very close to those in NW, while in few cases they were different but non-statistically significant: in 11–13-year-old boys they were higher (mean 92.9 vs. 87.5, p > 0.05), and in 8–10 and 11–13-year-old girls they were lower (mean 82.5 vs. 87.0, and 73.8 vs. 81.3, p > 0.05, respectively). Subgroups analyses for subtests' scores (Table 3) revealed that the trend was similar to the MQ results, except for the WB and JS subtests that were not significantly different across girls in age groups 11–13 and 6–7, respectively. With regard to the MS subtest, no difference was evidenced across age groups 6–7 and 11–13 years in girls. Contrarily, a significant decreasing performance in the HH subtest was evidenced in boys within the age group 6–7 (F = 4.56, p < 0.01); while no difference was revealed in boys and in girls in the age group 11–13.
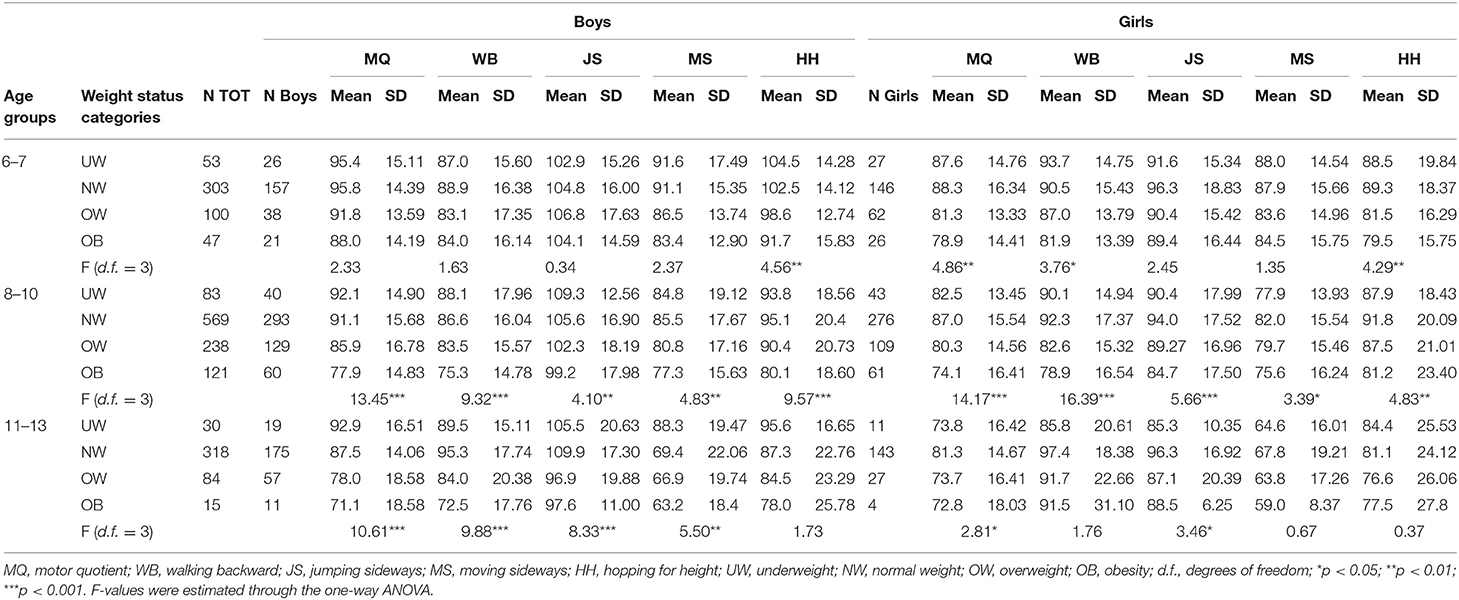
Table 3. Total MQ and subtest scores of the KTK by age groups, gender classes, and weight status categories, with F-values and significance levels across the weight status categories.
The one-way ANOVA performed to assess the significance level of the differences in MQ across age groups by gender and weight status (Table 4) showed that there was no difference across age groups in boys in UW, while this difference was found out in girls. Girls in OW and with OB had not significantly different MQ across age groups. In participants in NW, for both boys and girls, significantly higher performances were observed in 6–7-year-old children than 8–10 and 11–13 (F = 12.65, p < 0.001 and F = 8.55, p < 0.001, respectively). The same trend was found out in participants in OW and with OB, whose performances were better in younger groups (F = 8.81, p < 0.001 in OW category, and F = 5.29, p < 0.01 in OB category). With regard to the subtest scores, mostly the same trends with the highest significant differences were found out in the NW categories for all the subtests (except for the JS in girls), and in particular for the MS subtest (F = 64.97, p < 0.001 in boys in NW, and F = 57.07, p < 0.001 in girls in NW).
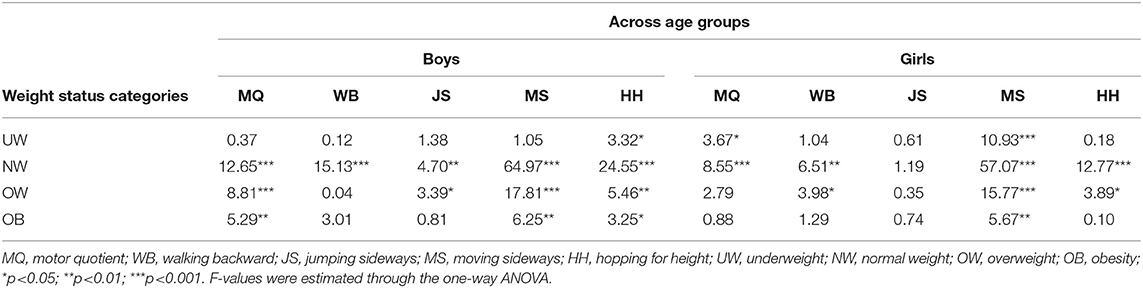
Table 4. F-values and significance levels of differences in the total MQ and subtest scores of the KTK across age groups by gender classes and weight status categories.
The one-way ANOVA carried out to assess the significance level of the differences in MQ across gender classes by age and weight status (Table 5), highlighted that 6–7-year-old boys had better performances than girls' peers in NW, OW, and OB categories (F = 18.10, p < 0.001; F = 14.50, p <0.001; F = 4.63, p < 0.05, respectively). This trend was similar in 8–10-year-old children in NW and OW, but not in the OB category, while it was observed only for the NW category in the 11–13 years-old group (Table 5). No differences were found out across gender categories for the WB subtest, except for the age group 8–10 (F = 16.60, p < 0.001). For the JS subtest, there were strong differences in all weight status categories and age groups, with the only exception of 11–13-year-old adolescents with OB, who did not differ in their performance between boys and girls (F = 2.40, p > 0.05). The MS subtest did not reveal any significance in all classes, except for 8–10-year-old children in NW and 11–13-year-old adolescents in UW. The HH subtest showed strong differences only in the age group 6–7, and small significant difference in 11–13-year-old adolescents in NW.
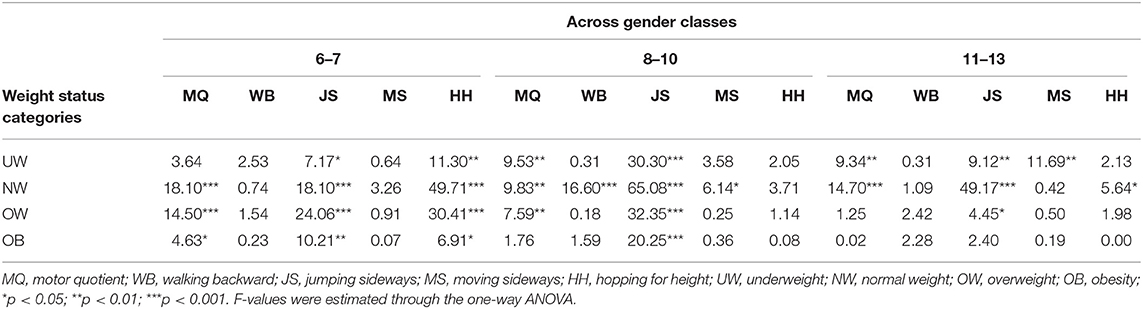
Table 5. F-values and significance levels of differences in the total MQ and subtest scores of the KTK across gender classes by age groups, and weight status categories.
The three-way ANOVA evidenced no interaction effect of weight status, age, and gender on MQ scores (Table 6 and Figure 1). Thus, it means that the joint effect of weight status, age, and gender on MQ is not statistically higher compared to the sum of the three effects individually.
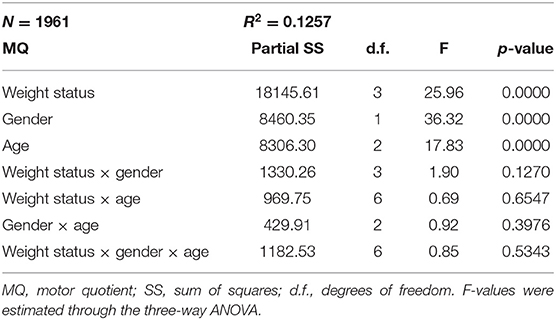
Table 6. Interaction effect of weight status, age, and gender on MQ.
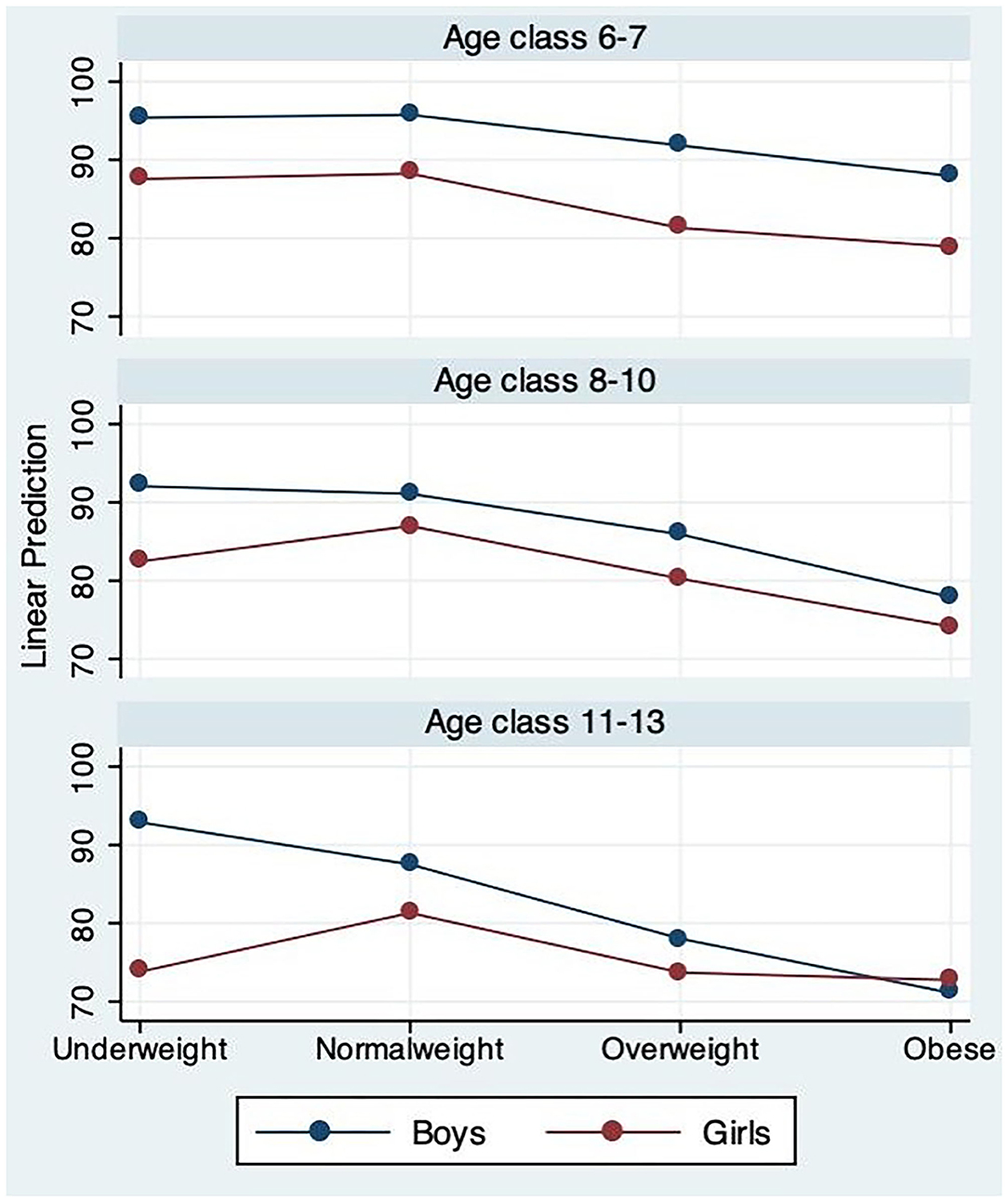
Figure 1. Adjusted predictions of weight status-age-gender on MQ.
The aim of the present study was to investigate the association between motor coordination (MC), expressed as motor quotient (MQ), and body weight status in Italian children and early adolescents aged 6–13 years according to age and gender. Similarly, we analyzed the associations between the four motor skills included in the test protocol for the MC assessment and weight status categories across age groups and gender classes.
First of all, it should be noted that the prevalence of participants in UW, NW, OW, and with OB was 8, 61, 22, and 9%, respectively, that is a proportion which is consistent with recent data on Italian children of the same age (39). Based on this premise, our hypothesis was mostly confirmed because the findings showed that weight status, age, and gender were strongly associated with MC. In fact, MQ level decreased (p < 0.001) from participants in OW to participants with OB (F = 37.66), in older than younger (F = 25.25), and in girls than boys (F = 67.22). Lower levels of MQ, HH, JS, WB, and MS (F = 128.41) were found in participants in OW and with OB than peers in NW, both in boys and girls, and in all the age groups except for the age group 6–7-year-old boys.
This latter result is consistent with outcomes obtained in our previous study, in which gross motor quotient, locomotor, and object control skills were not significantly different throughout the classes of underweight, normal overweight, and obesity in preschool children aged 3–5 years old (40). Therefore, MC performances appears to not be significantly affected by weight status in early childhood as also demonstrated in the present study by the highest levels of MQ scores in 6–7-year-old children. These findings could be explained with the relevant range of interindividual variation in early motor development. Indeed, development process can be continuous but also intermittent when periods of instability or negligible changes are followed by significant progresses, or when regression stages precede a more advanced stage (41). As a matter of the fact, according to the “reciprocal interweaving” model, during childhood and adolescence the development of motor competence can alternate periods of maturity followed by subsequent periods of immaturity, and so on (42).
Our findings relating to the negative influence of higher BMI levels on MC are in agreement with previous studies in which it was detected that children and adolescents in overweight or with obesity were more likely to possess lower MC than peers in healthy weight (3, 12, 21).
The lower MQ levels in older than younger ones (F = 25.25) could be also associated with the high prevalence of participants in OW and with OB in 8–10 and 11–13 age groups. In agreement with previous studies (9, 21), the reported deficiencies in MC associated with OW and OB do not seem to be temporary, and we found that, increasing age, MC even appeared to deteriorate. This could be related to a disadvantageous effect of an excessive body mass on MC. In fact, it increases as a greater body mass is involved in the action and when the body needs to be moved under time constraints or against gravity (8).
Our results showed significant differences in MQ (F = 67.22) and JS scores (F = 268.38) between girls and boys. These results are similar to those reported in other studies that exhibited significant differences in motor skills between boys and girls (9, 43). Gender differences in motor performance, in which boys performing better than girls, could be related to the difference both in the usual PA level and the sport practice, regardless of body weight status (9, 44, 45). Indeed, in a cohort of 2,815 children and adolescents of both sexes aged 3–15 years, in which ~ 90% of the participants had a healthy body weight status, Ishii et al. (45) reported that boys were more physically active than girls (45). Similar results were also found by Ridley et al. (46) in the practice of organized sports in which authors, among the findings, detected that between girls' and boys' soccer teams, the latter spent significantly higher time in moderate to vigorous physical activity (MVPA) (46). In a similar way, previous studies reported lower time spent in MVPA among children with obesity than peers without obesity (47).
The significant (p < 0.001) inverse trend revealed for the WB subtest, with a significant increasing performance in older participants (F = 12.64) and in girls (F = 17.47), is in agreement with seminal studies on this topic. For instance, D'Hondt et al. (9) detected increasingly higher scores in this motor skill with rising age in children, as well as in girls than boys of the same age in all weight categories (9). This outcome could be related to the better balance performance of adolescents than children (48), and that of girls than same-aged boys, regardless of body weight status (49–51). According to Woollacott and Shumway-Cook (48), we speculate that older participants exhibit better dynamic balance in WB subtest than younger ones because the maturation of balance control does not complete in childhood, but, possibly, continues throughout adolescence (52). However, the literature reports contrasting results on the impact of body weight on balance control in children and adolescents (53, 54).
No interaction effect was found between weight status, age, and gender on MQ. Thus, it means that the joint effect of weight status, age, and gender on MQ is not statistically higher compared to the sum of the three effects individually. For example, a girl in OW, who is also in the higher age group, has a lower performance, but, since there is not any interaction between being girls, OW, and belonging to the higher age groups, the effect on decreasing performance is not enhanced compared to the sum of the single aspects.
In conclusion, these data showed that weight status affects the development of MC throughout childhood and early adolescence.
It is known that children's and adolescents' general behavior, including daily activities and the practice of PA, is determined by MC (7). Furthermore, higher levels of MC during childhood and adolescence influence children's ability to successfully participate in movement situations and, moreover, to engage in lifelong PA (15–17). Since sedentary behaviors and a low level of PA negatively affect body weight across childhood and adolescence (25, 40, 55, 56), it is important to take into account MC in children and adolescents with excessive BMI.
Therefore, the adoption of a health-related educational strategy, such as motor plans that include the development of motor coordination, is crucial in school in order to promote an active and healthy lifestyle in children and adolescents (57–60).
The main strength of the study is the large Italian sample recruited. Furthermore, among the strengths it should be noted that not only the general level of MC was taken into consideration but also the score of each subtest.
Growth and maturity characteristics of children (morphological, physiological, and neuromuscular) might contribute to influence the development of MC during childhood and adolescence, therefore, the absence of data concerning these aspects represents a limitation of this study. Additionally, it is important to highlight among the limitations of the study that, although KTK is a reliable protocol test commonly used to measure MC performance in children and adolescents, it does not include the assessment of fine motor coordination.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethical Board of Verona University (No. 2019-UNVRCLE-0298910) and Palermo University (No. 8/2019). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
ML, MB, LG, and CB conceptualization and methodology. VB, MG, MCG, and AG Data collection. GT, GB, and MB data analysis. VG, ML, FS, and AP data interpretation. GB and VG writing—original draft preparation. MB writing—review & editing. MB and AP supervision. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are very grateful to Giovanni Caramazza for his contribution in the involvement of the schools, Jessica Brusa for her collaboration, schoolteachers and university students for their collaboration in the collecting data, and to schools and children participating in the study.
1. Barnett LM, Lai SK, Veldman SLC, Hardy LL, Cliff DP, Morgan PJ, et al. Correlates of gross motor competence in children and adolescents: a systematic review and meta-analysis. Sports Med. (2016) 46:1663–88. doi: 10.1007/s40279-016-0495-z
2. Cattuzzo MT, Dos Santos Henrique R, Re AH, de Oliveira IS, Melo BM, de Sousa Moura M, et al. Motor competence and health related physical fitness in youth: a systematic review. J Sci Med Sport. (2016) 19:123–9. doi: 10.1016/j.jsams.2014.12.004
3. Lubans DR, Morgan PJ, Cliff DP, Barnett LM, Okely AD. Fundamental movement skills in children and adolescents: review of associated health benefits. Sports Med. (2010) 40:1019–35. doi: 10.2165/11536850-000000000-00000
4. Clark JE, Metcalfe JS. The mountain of motor development: a metaphor. In: Clark J. E. HJH, Editors. Motor Development: Research and Reviews. Reston, VA: NASPE Publications (2002). p. 163–90.
5. Adamo KB, Wilson S, Harvey AL, Grattan KP, Naylor PJ, Temple VA, et al. Does intervening in childcare settings impact fundamental movement skill development? Med Sci Sports Exerc. (2016) 48:926–32. doi: 10.1249/MSS.0000000000000838
6. Battaglia G, Alesi M, Tabacchi G, Palma A, Bellafiore M. The development of motor and pre-literacy skills by a physical education program in preschool children: a non-randomized pilot trial. Front Psychol. (2018) 9:2694. doi: 10.3389/fpsyg.2018.02694
7. Stodden DF, Goodway JD, Langendorfer SJ, Roberton MA, Rudisill ME, Garcia C, et al. A developmental perspective on the role of motor skill competence in physical activity: an emergent relationship. Quest. (2008) 60:290–306. doi: 10.1080/00336297.2008.10483582
8. D'Hondt E, Deforche B, De Bourdeaudhuij I, Lenoir M. Relationship between motor skill and body mass index in 5- to 10-year-old children. Adapt Phys Activ Q. (2009) 26:21–37. doi: 10.1123/apaq.26.1.21
9. D'Hondt E, Deforche B, Vaeyens R, Vandorpe B, Vandendriessche J, Pion J, et al. Gross motor coordination in relation to weight status and age in 5- to 12-year-old boys and girls: a cross-sectional study. Int J Pediatr Obes. (2011) 6:e556–64. doi: 10.3109/17477166.2010.500388
10. D'Hondt E, Deforche B, Gentier I, De Bourdeaudhuij I, Vaeyens R, Philippaerts R, et al. A longitudinal analysis of gross motor coordination in overweight and obese children versus normal-weight peers. Int J Obes. (2013) 37:61–7. doi: 10.1038/ijo.2012.55
11. Cheng J, East P, Blanco E, Sim EK, Castillo M, Lozoff B, et al. Obesity leads to declines in motor skills across childhood. Child Care Health Dev. (2016) 42:343–50. doi: 10.1111/cch.12336
12. Castetbon K, Andreyeva T. Obesity and motor skills among 4 to 6-year-old children in the United States: nationally-representative surveys. BMC Pediatr. (2012) 12:28. doi: 10.1186/1471-2431-12-28
13. Lopes VP, Maia JAR, Rodrigues LP, Malina R. Motor coordination, physical activity and fitness as predictors of longitudinal change in adiposity during childhood. Eur J Sport Sci. (2012) 12:384–91. doi: 10.1080/17461391.2011.566368
14. Tsiros MD, Tian EJ, Shultz SP, Olds T, Hills AP, Duff J, et al. Obesity, the new childhood disability? An umbrella review on the association between adiposity and physical function. Obes Rev. (2020) 21:e13121. doi: 10.1111/obr.13121
15. Veldman SLC, Santos R, Jones RA, Sousa-Sa E, Okely AD. Associations between gross motor skills and cognitive development in toddlers. Early Hum Dev. (2019) 132:39–44. doi: 10.1016/j.earlhumdev.2019.04.005
16. Peyre H, Albaret JM, Bernard JY, Hoertel N, Melchior M, Forhan A, et al. Developmental trajectories of motor skills during the preschool period. Eur Child Adolesc Psychiatry. (2019) 28:1461–74. doi: 10.1007/s00787-019-01311-x
17. Lopes L, Silva Mota JAP, Moreira C, Abreu S, Agostinis Sobrinho C, Oliveira-Santos J, et al. Longitudinal associations between motor competence and different physical activity intensities: LabMed physical activity study. J Sports Sci. (2019) 37:285–90. doi: 10.1080/02640414.2018.1497424
18. DuBose KD, Gross McMillan A, Wood AP, Sisson SB. Joint relationship between physical activity, weight status, and motor skills in children aged 3 to 10 years. Percept Mot Skills. (2018) 125:478–92. doi: 10.1177/0031512518767008
19. Loprinzi PD, Davis RE, Fu YC. Early motor skill competence as a mediator of child and adult physical activity. Prev Med Rep. (2015) 2:833–8. doi: 10.1016/j.pmedr.2015.09.015
20. Tabacchi G, Battaglia G, Alesi M, Paoli A, Palma A, Bellafiore M. Food literacy predictors and associations with physical and emergent literacy in pre-schoolers: results from the training-to-health project. Public Health Nutr. (2020) 23:356–65. doi: 10.1017/S1368980019002404
21. Okely AD, Booth ML, Chey T. Relationships between body composition and fundamental movement skills among children and adolescents. Res Q Exerc Sport. (2004) 75:238–47. doi: 10.1080/02701367.2004.10609157
22. Coppens E, Bardid F, Deconinck FJA, Haerens L, Stodden D, D'Hondt E, et al. Developmental change in motor competence: a latent growth curve analysis. Front Physiol. (2019) 10:1273. doi: 10.3389/fphys.2019.01273
23. RuŽbarská I. Gross motor coordination in relation to weight status in 7- to 9-year-old children. Acta Gymnica. (2020) 50:105–12. doi: 10.5507/ag.2020.016
24. Chagas DdV, Batista LA. Associations between motor coordination and BMI in normal weight and overweight/obese adolescents. J Hum Growth Dev. (2016) 26:380–4. doi: 10.7322/jhgd.122914
25. Han A, Fu A, Cobley S, Sanders RH. Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: a systematic review. J Sci Med Sport. (2018) 21:89–102. doi: 10.1016/j.jsams.2017.07.001
26. Morano M, Colella D, Caroli M. Gross motor skill performance in a sample of overweight and non-overweight preschool children. Int J Pediatr Obes. (2011) 6(Suppl 2):42–6. doi: 10.3109/17477166.2011.613665
27. Roberts D, Veneri D, Decker R, Gannotti M. Weight status and gross motor skill in kindergarten children. Pediatr Phys Ther. (2012) 24:353–60. doi: 10.1097/PEP.0b013e3182680f19
28. Gentier I, D'Hondt E, Shultz S, Deforche B, Augustijn M, Hoorne S, et al. Fine and gross motor skills differ between healthy-weight and obese children. Res Dev Disabil. (2013) 34:4043–51. doi: 10.1016/j.ridd.2013.08.040
29. Marmeleira J, Veiga G, Cansado H, Raimundo A. Relationship between motor proficiency and body composition in 6- to 10-year-old children. J Paediatr Child Health. (2017) 53:348–53. doi: 10.1111/jpc.13446
30. Prskalo I, Badric M, Kunjesic M. The percentage of body fat in children and the level of their motor skills. Coll Antropol. (2015) 39(Suppl 1):21–8.
31. Cawley J, Spiess CK. Obesity and skill attainment in early childhood. Econ Hum Biol. (2008) 6:388–97. doi: 10.1016/j.ehb.2008.06.003
32. Gungor NK. Overweight and obesity in children and adolescents. J Clin Res Pediatr Endocrinol. (2014) 6:129–43. doi: 10.4274/jcrpe.1471
33. Ahrens W, Pigeot I, Pohlabeln H, De Henauw S, Lissner L, Molnar D, et al. Prevalence of overweight and obesity in European children below the age of 10. Int J Obes. (2014) 38(Suppl 2):S99–107. doi: 10.1038/ijo.2014.140
34. Silano M, Agostoni C, Fattore G. Italy's unsolved childhood obesity crisis. Arch Dis Child. (2019) 104:202–3. doi: 10.1136/archdischild-2018-315678
35. Sgrò F, Quinto A, Messana L, Pignato S, Lipoma M. Assessment of gross motor developmental level in Italian primary school children. J Phys Educ Sport. (2017) 17:1954.
36. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. (2000) 320:1240–3. doi: 10.1136/bmj.320.7244.1240
39. Nardone P, Spinelli A, Buoncristiano M, Lauria L, Pierannunzio D, Galeone D. Il Sistema Di Sorveglianza Okkio Alla SALUTE:Risultati 2016. Roma: Istituto Superiore di Sanità (2018) 7–8.
40. Battaglia G, Giustino V, Tabacchi G, Alesi M, Galassi C, Modica C, et al. Effectiveness of a physical education program on the motor and pre-literacy skills of preschoolers from the training-to-health project: a focus on weight status. Front Sports Act Living. (2020) 2:579421. doi: 10.3389/fspor.2020.579421
41. Malina RM. Motor development during infancy and early childhood: overview and suggested directions for research. Int J Sport Health Sci. (2004) 2:50–66. doi: 10.5432/ijshs.2.50
42. Gesell A. The Ontogenesis of Infant Behavior. Manual of Child Psychology. Hoboken, NJ: John Wiley & Sons Inc (1946) p. 295–331. doi: 10.1037/10756-006
43. Davies PL, Rose JD. Motor skills of typically developing adolescents: awkwardness or improvement? Phys Occup Ther Pediatr. (2000) 20:19–42. doi: 10.1080/J006v20n01_03
44. Vandorpe B, Vandendriessche J, Lefevre J, Pion J, Vaeyens R, Matthys S, et al. The korperkoordinationstest fur kinder: reference values and suitability for 6-12-year-old children in flanders. Scand J Med Sci Sports. (2011) 21:378–88. doi: 10.1111/j.1600-0838.2009.01067.x
45. Ishii K, Shibata A, Adachi M, Nonoue K, Oka K. Gender and grade differences in objectively measured physical activity and sedentary behavior patterns among Japanese children and adolescents: a cross-sectional study. BMC Public Health. (2015) 15:1254. doi: 10.1186/s12889-015-2607-3
46. Ridley K, Zabeen S, Lunnay BK. Children's physical activity levels during organised sports practices. J Sci Med Sport. (2018) 21:930–4. doi: 10.1016/j.jsams.2018.01.019
47. McManus AM, Mellecker RR. Physical activity and obese children. J Sport Health Sci. (2012) 1:141–8. doi: 10.1016/j.jshs.2012.09.004
48. Woollacott MH, Shumway-Cook A. Changes in posture control across the life span–a systems approach. Phys Ther. (1990) 70:799–807. doi: 10.1093/ptj/70.12.799
49. Steindl R, Kunz K, Schrott-Fischer A, Scholtz AW. Effect of age and sex on maturation of sensory systems and balance control. Dev Med Child Neurol. (2006) 48:477–82. doi: 10.1017/S0012162206001022
50. Eguchi R, Takada S. Usefulness of the tri-axial accelerometer for assessing balance function in children. Pediatr Int. (2014) 56:753–8. doi: 10.1111/ped.12370
51. Hirabayashi S, Iwasaki Y. Developmental perspective of sensory organization on postural control. Brain Dev. (1995) 17:111–3. doi: 10.1016/0387-7604(95)00009-Z
52. Woollacott M, Shumway-Cook A. Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture. (2002) 16:1–14. doi: 10.1016/S0966-6362(01)00156-4
53. Villarrasa-Sapina I, Garcia-Masso X, Serra-Ano P, Garcia-Lucerga C, Gonzalez LM, Lurbe E. Differences in intermittent postural control between normal-weight and obese children. Gait Posture. (2016) 49:1–6. doi: 10.1016/j.gaitpost.2016.06.012
54. D'Hondt E, Deforche B, De Bourdeaudhuij I, Gentier I, Tanghe A, Shultz S, et al. Postural balance under normal and altered sensory conditions in normal-weight and overweight children. Clin Biomech. (2011) 26:84–9. doi: 10.1016/j.clinbiomech.2010.08.007
55. Osinski W, Kantanista A. Physical activity in the therapy of overweight and obesity in children and adolescents. Needs and recommendations for intervention programs. J Mother Child. (2017) 21:224–34. doi: 10.34763/devperiodmed.20172103.224234
56. Rodriguez-Ayllon M, Cadenas-Sanchez C, Estevez-Lopez F, Munoz NE, Mora-Gonzalez J, Migueles JH, et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med. (2019) 49:1383–410. doi: 10.1007/s40279-019-01099-5
57. Giustino V, Parroco AM, Gennaro A, Musumeci G, Palma A, Battaglia G. Physical activity levels and related energy expenditure during COVID-19 quarantine among the sicilian active population: a cross-sectional online survey study. Sustainability. (2020) 12:4356. doi: 10.3390/su12114356
58. Baumgartner L, Postler T, Graf C, Ferrari N, Haller B, Oberhoffer-Fritz R, et al. can school-based physical activity projects such as skipping hearts have a long-term impact on health and health behavior? Front Public Health. (2020) 8:352. doi: 10.3389/fpubh.2020.00352
59. Lander N, Eather N, Morgan PJ, Salmon J, Barnett LM. Characteristics of teacher training in school-based physical education interventions to improve fundamental movement skills and/or physical activity: a systematic review. Sports Med. (2017) 47:135–61. doi: 10.1007/s40279-016-0561-6
Keywords: motor coordination, motor performance, motor quotient, weight status, body weight, overweight, obesity, children
Citation: Battaglia G, Giustino V, Tabacchi G, Lanza M, Schena F, Biino V, Giuriato M, Gallotta MC, Guidetti L, Baldari C, Gennaro A, Palma A and Bellafiore M (2021) Interrelationship Between Age, Gender, and Weight Status on Motor Coordination in Italian Children and Early Adolescents Aged 6–13 Years Old. Front. Pediatr. 9:738294. doi: 10.3389/fped.2021.738294
Received: 08 July 2021; Accepted: 17 August 2021;
Published: 10 September 2021.
Edited by:
Irena Valantine, Lithuanian Sports University, LithuaniaReviewed by:
Andreo Fernando Aguiar, Universidade Norte do Paraná, BrazilCopyright © 2021 Battaglia, Giustino, Tabacchi, Lanza, Schena, Biino, Giuriato, Gallotta, Guidetti, Baldari, Gennaro, Palma and Bellafiore. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valerio Giustino, dmFsZXJpby5naXVzdGlub0B1bmlwYS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.