 Annie Le-Nguyen1
Annie Le-Nguyen1 Maeve O'Neill Trudeau2Philippe Dodin3
Maeve O'Neill Trudeau2Philippe Dodin3 Mark R. Keezer4,5,6
Mark R. Keezer4,5,6 Christophe Faure7
Christophe Faure7 Nelson Piché2*
Nelson Piché2*- 1Department of General Surgery, Université de Montréal, Montréal, QC, Canada
- 2Department of Pediatric Surgery, Centre Hospitalier Universitaire Sainte-Justine, Université de Montréal, Montréal, QC, Canada
- 3Centre Hospitalier Universitaire Sainte-Justine, Université de Montréal, Montréal, QC, Canada
- 4Department of Neurosciences, Université de Montréal, Montréal, QC, Canada
- 5Centre Hospitalier de l'Université de Montréal (CHUM), Montréal, QC, Canada
- 6School of Public Health, Université de Montréal, Montréal, QC, Canada
- 7Department of Gastroenterology, Hepatology, and Nutrition, Centre Hospitalier Universitaire Sainte-Justine, Université de Montréal, Montréal, QC, Canada
Purpose: Indocyanine green fluorescence angiography (ICG-FA) is a validated non-invasive imaging technique used to assess tissue vascularization and guide intraoperative decisions in many surgical fields including plastic surgery, neurosurgery, and general surgery. While this technology is well-established in adult surgery, it remains sparsely used in pediatric surgery. Our aim was to systematically review and provide an overview of all available evidence on the perioperative use of indocyanine green fluorescence angiography in pediatric surgical patients.
Methods: We conducted a systematic review with narrative synthesis in conformity with the PRISMA guidelines using PubMed, Medline, All EBM Reviews, EMBASE, PsycINFO, and CINAHL COMPLETE databases to identify articles describing the perioperative use of ICG-FA in pediatric patients. Two independent authors screened all included articles for eligibility and inclusion criteria. We extracted data on study design, demographics, surgical indications, indocyanine green dose, and perioperative outcomes. We developed a risk of bias assessment tool to evaluate the methodological quality of included studies.
Results: Of 1,031 articles retrieved, a total of 64 articles published between 2003 and 2020 were included reporting on 664 pediatric patients. Most articles were case reports and case series (n = 36; 56%). No adverse events related to ICG-FA were reported in the included articles. Risk of bias was high. We did not conduct a meta-analysis given the heterogeneous nature of the populations, interventions, and outcome measures. A narrative synthesis is presented.
Conclusion: Indocyanine green fluorescence angiography is a safe imaging technology and its use is increasing rapidly in pediatric surgical specialties. However, the quality of evidence supporting this trend currently appears low. Case-control and randomized trials are needed to determine the adequate pediatric dose and to confirm the potential benefits of ICG-FA in pediatric surgical patients.
Systematic Review Registration: This study was registered on Prospero a priori, identifier: CRD42020151981.
Introduction
Indocyanine green fluorescence angiography (ICG-FA) is an imaging technology that allows real-time visualization of tissue perfusion (1). With a half-life of 3 to 5 min, ICG allows repeated injections during a procedure (1). Adverse events have been reported in 1 out of 42,000 patients and include anaphylactic reactions in patients with iodine allergy, making this a contraindication for ICG use (2). Initially, this dye was intended for use in ophthalmic angiography, cardiac output measurements, and hepatic function studies (3). In the early 2000s, the interest in ICG-FA importantly increased. Current surgical applications in adults include tumor detection, assessment of flap perfusion, and fluorescence imaging of tissue and organ perfusion in colorectal and hepatobiliary surgeries (1). Recently, the use of indocyanine green fluorescence angiography in the pediatric population has rapidly gained in popularity. We performed a systematic review and narrative synthesis of the literature to capture and analyze all available evidence on the use of ICG-FA in pediatric surgical patients. The objective of this review was to determine if current data support its use.
Materials and Methods
We conducted a comprehensive systematic review in conformity with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (4). Institutional review board approval was not necessary. Before data extraction, we registered our systematic review protocol with PROSPERO (ID number CRD42020151981). Six electronic databases were systematically searched in December 2019 with an updated search on January 14, 2021: PubMed (NLM), Medline (Ovid), All EBM Reviews (Ovid), EMBASE (Ovid), PsycINFO (Ovid), and CINAHL COMPLETE (EBSCO). The search strategy was designed in collaboration with a senior hospital librarian (PD) to identify all relevant articles reporting the use of ICG-FA in the pediatric population. There was no restriction to time, language, study subjects, and type of articles. References of included articles were hand-searched to identify additional relevant studies.
Study Selection and Data Extraction
Two authors (ALN and MOT) independently screened all titles and abstracts. When potentially relevant, the two authors independently screened all full texts to decide which articles to include in the final review. Any disagreements were resolved by consensus or with the help of the senior author (NP). Studies were included in the analysis if they: (1) included patients <18 years of age and (2) focused on the perioperative use of ICG-FA. We excluded reviews, letters to the editors, editorials, commentaries, abstracts, animal and adult studies, as well as ophthalmological surgical articles. Articles that included both pediatric and adult patients were included when the mean or median age was < 18 years old, or when enough data on pediatric patients allowed a separate analysis.
We classified studies as descriptive studies and analytic studies. Descriptive studies included case series and case reports whereas analytic studies were defined as cohort studies with a comparison group and experimental studies (e.g., randomized controlled trials) (5).
Study Quality Assessment
We developed a risk of bias tool based on the Newcastle-Ottawa (6), Methodological quality and synthesis of case series and case reports (7), and MINORS (Methodological Index for Non-Randomized Studies) tools (8). Additional support from an epidemiology expert (MRK) was obtained for selecting criteria and developing the risk of bias tool (see Table 1). Two reviewers (ALN and MOT) independently evaluated the risk of bias of every included study and reported them as high, low, or unclear (Table 2). Disagreements were solved by consensus.
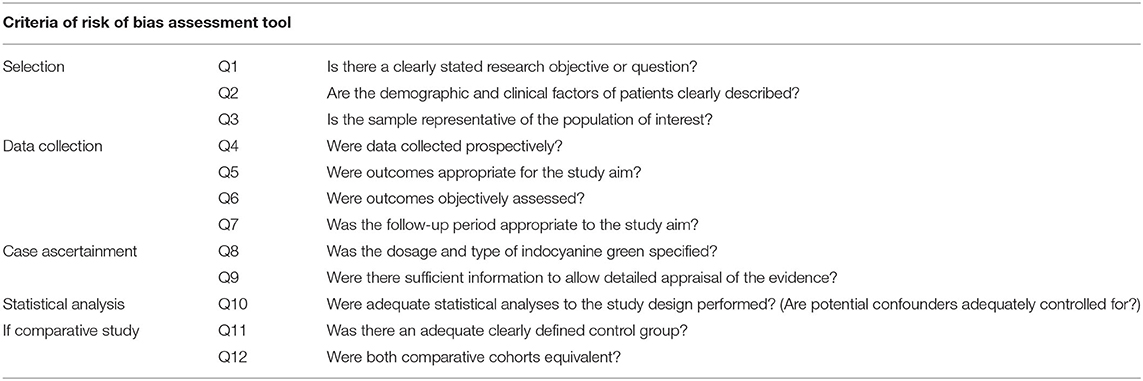
Table 1. Risk of bias assessment tool.
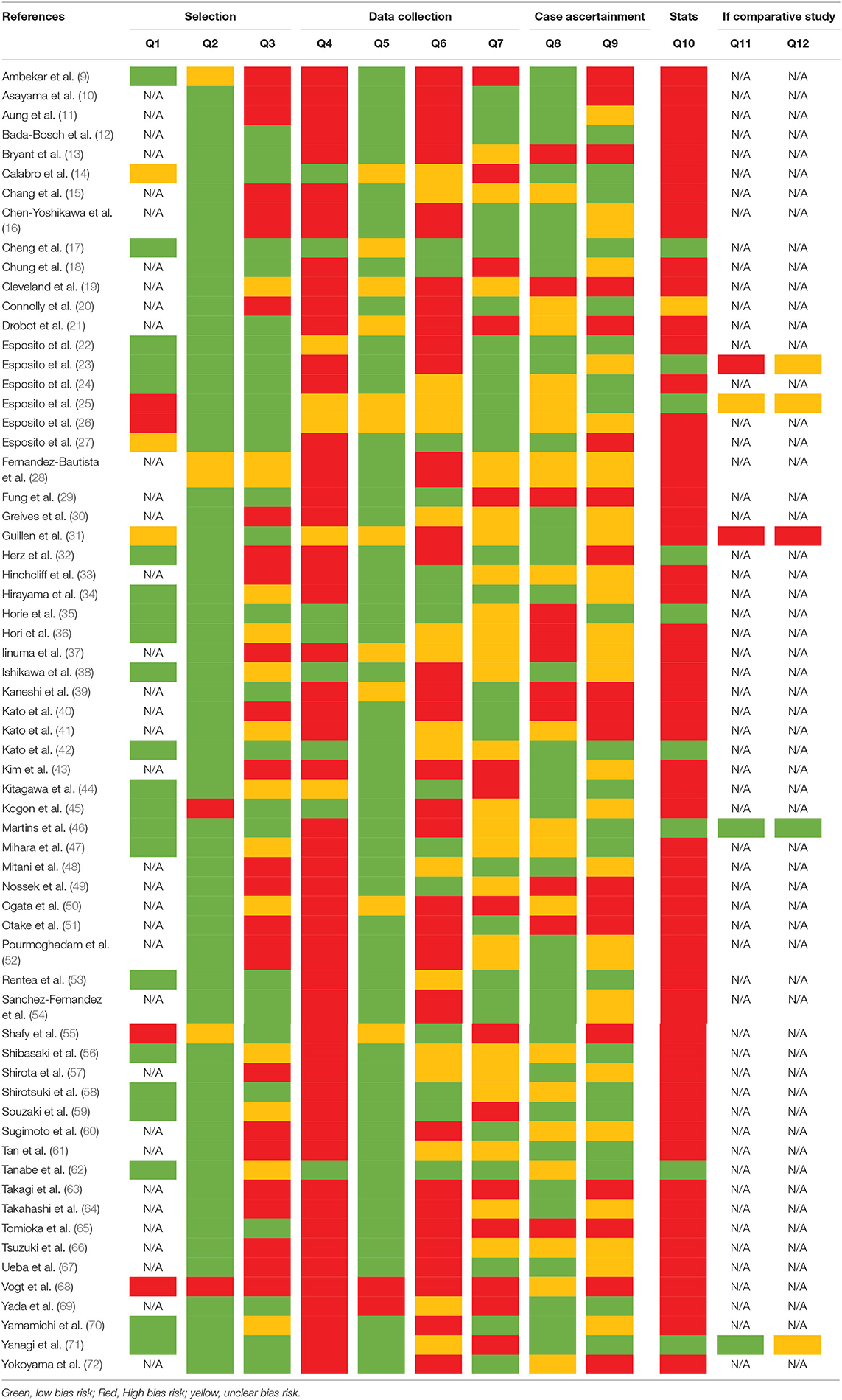
Table 2. Risk of bias of included studies.
Statistical Analysis
We did not perform a meta-analysis given the important heterogeneity of included studies. However, narrative synthesis is presented to guide clinicians with the current pediatric surgical indications and doses of indocyanine green angiography.
Results
The selection process of articles and reasons for study exclusion are reported in a PRISMA flowchart (Figure 1). A total of 937 articles were retrieved through the initial database search, and 93 were additionally identified in January 2021. One study was included after hand-searching references (53). Sixty-four articles, including 664 pediatric patients, from 2003 to 2020 met the inclusion criteria for narrative synthesis in our systematic review. Case reports and case series represented 38 and 19% of included studies, respectively. The remaining 43% were retrospective and prospective studies with no randomized controlled trials. Table 3 presents an outcome summary.
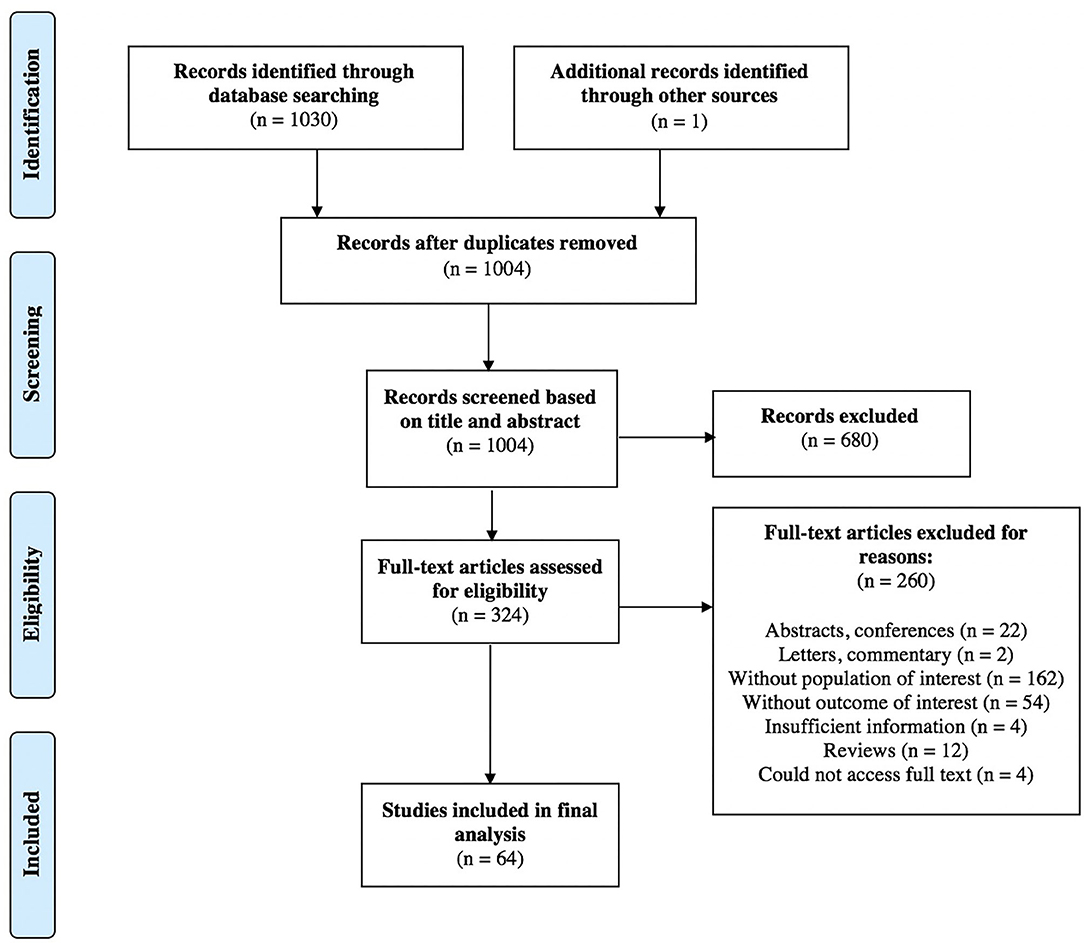
Figure 1. PRISMA flow diagram of selection of studies for inclusion in the systematic review.

Table 3. Study outcome summary separated in different surgical specialties.
Study Quality
The risk of bias assessment can be found in Table 2. Overall, the quality of evidence supporting the use of ICG-FA in surgical pediatric patients was predominantly of low or unknown risk. An important number of included studies (n = 37; 58%) were at high risk of selection bias as none of them were randomized and allocation of intervention was based on the surgeon's choice. Data collection was mentioned as prospective in only 13/64 studies (14, 22, 31, 34, 44). While outcomes were generally appropriate for the study aim, 80% of included studies were at high or unclear risk of information biases either because outcomes were not objectively assessed or blinding of surgeons to the intervention was not possible. Follow-ups were inconsistently reported making it difficult to assess whether the intervention was beneficial or not in the long-term. Statistical analyses were not conducted in 40/64 studies and power calculations were lacking in all studies.
Narrative Synthesis of the Results
Techniques
Most ICG-FA indications used a peripheral vein injection (n = 29; 45%). However, chylothorax and lymphatic/venous procedures (15, 30, 38, 40, 42, 47, 50, 51, 56, 57, 61) required subcutaneous ICG injections, and varicocelectomies (22, 24) needed direct injections into the ipsilateral testicle. Indocyanine green dose and injection timing varied according to surgical teams and indications and were adequately reported in only 29/64 (45%) studies. Other studies either overlooked stating the patient's weight, administration route, or ICG dilution making it difficult to generalize results. Injections were done intraoperatively except for specific indications including surgical procedures for primary (70) and metastatic (16, 44, 59, 64) hepatoblastoma and biliary atresia (34) as well as cholecystectomies (22, 23, 28, 31) for which ICG was injected from 18 to 72 h before the surgery.
Application of ICG by Pediatric Surgical Specialty
In pediatric surgery and pediatric urology, ICG-FA indications included cholecystectomy (n = 8) (13, 14, 22, 23, 26, 28, 31, 55), primary and metastatic hepatoblastoma (n = 6) (16, 44, 48, 59, 64, 70), varicocelectomy (n = 5) (22, 24–26, 31), nephrectomy (n = 5) (22, 25, 26, 28, 32), chylous leaks and ascites (n = 4) (15, 47, 51, 56), colorectal procedures including cloacal, anorectal malformation, and Hirschsprung reconstructions, intestinal resection for volvulus, as well as stoma closure (n = 4) (37, 53, 55, 69), hepatocellular carcinoma (n = 1) (18), abdominal mass excision (n = 1) (22), and tracheoesophageal fistula (n = 1) (58). Pediatric neurosurgeons used ICG-FA in patients with Moyamoya disease to evaluate the anatomy and confirm patency of their surgical anastomoses (n = 4) (9, 35, 36, 62). Tumor detection (n = 3) (10, 43, 66), arteriovenous malformations (n = 2) (63, 67), cerebral mycotic aneurysm (n = 1) (73), and intracranial pial arteriovenous fistula (n = 1) (60) were other neurosurgical indications. In pediatric cardiac surgery, ICG-FA was used for congenital cardiac surgeries (n = 3) (45, 52, 68) and post-operative chylothorax (n = 2) (40, 61). Reported indications in pediatric plastic surgery were lymphatic and venous malformations (n = 8) (17, 21, 30, 38, 39, 42, 50, 57) and tissue perfusion (n = 3) (33, 46, 65). Orthopedics indications were rare and included trauma surgeries (n = 2) (19, 20) and rotationplasty for patients with femoral sarcoma (n = 1) (11).
Benefits of ICG-FA
Indocyanine green appears mostly beneficial in the pediatric population for delineating vascular, lymphatic and hepatobiliary structures. A total of 57 pediatric studies (89%) reported potential benefits and successful outcomes with the use of ICG-FA. Shafy et al. (55) published a retrospective review of their general use of ICG-FA over a 2-year period, and confirmed safety of repeated injections in children (n = 8; 8%). After ICG was introduced, Esposito et al. (23) observed a decrease in operative time by a mean of 17 min in a 25-year retrospective study on laparoscopic cholecystectomies. ICG-FA can also confirm vascular anastomosis patency in children (22, 23, 74). In pediatric colorectal surgery, Rentea et al. (53) reported a change in the operative plan with ICG use in 4/12 (33%) patients undergoing surgery for anorectal malformations, cloaca, and Hirschsprung disease. In these four cases, the vascular supply of tissues seemed well-perfused on macroscopic inspection, but the use of ICG-FA demonstrated a poorly perfused proximal bowel which led to additional surgical steps including further resection (n = 2), splenic flexure mobilization (n = 1), and colostomy (n = 1). Overall, an early dehiscence of the anoplasty occurred in one patient (8%) who received intraoperative vasopressors; the remaining patients had an uneventful postoperative course. For patients who are critically ill and require lymphatic imaging, ICG-FA may represent a potential alternative because it can be performed at the patient's bedside (61). Furthermore, ICG-FA seems promising in pediatric surgical oncology. It has been reported useful for detecting pediatric tumors such as primary hepatoblastoma with or without lung and peritoneal metastases, even more when the surgery is performed by thoracoscopy and tactile sensation is not possible (16, 44, 59, 70). During Kasai procedures for biliary atresia, indocyanine green was helpful to detect bile leaks which may reduce postoperative morbidity and potentially have an impact on the postoperative normalization of hyperbilirubinemia of the patient (34). Two studies have also observed the fluorescence in patient's postoperative stools, and although this remains at an experimental stage, they found it useful to evaluate bile excretion (34) and bowel function (69). Assessment of skin flap vascularity in pediatric autologous ear reconstruction with ICG showed a decrease in surgical revisions (46).
Limitations of ICG-FA
Equipment access and associated costs are the main limitations of indocyanine green fluorescence angiography. While most studies found ICG useful during cholecystectomies, Bryant et al. (13) has described a case of gallbladder duplication during which intraoperative use of ICG did not provide adequate information for dissection. Although the author does not specify the timing of injection, this possibly reflects the importance of ICG administration 3 to 7 h before surgery to achieve adequate bile duct-to-liver fluorescence detection (75). Detection of fluorescence may also be limited by depth and size. Some studies reported that the detection of hepatoblastoma metastases was limited by size (<1.2 mm) (59) and distance from the surface (>3 mm) (70) of the parenchyma. One Japanese study including 250 fluorescence-positive resected lung lesions for metastatic hepatoblastoma revealed 29 false positive pulmonary lesions which were active alveolar cells and thromboses on pathological analysis (44). Another study has successfully detected hepatoblastoma pulmonary metastases of 1.2 mm at a dept of 6 mm from the lung surface (59). For lymphatic imaging, authors have also reported a limit of <1–2 cm in the depth of lymphatic vessels visualization (38, 42, 56). While most fluorescence lymphatic imaging were successful (15), ICG-FA failed to demonstrate the chylous leak in a patient who underwent a lymphatic imaging for a postoperative chylothorax. The authors hypothesized that the ICG transport toward the thorax was prevented by the high central venous pressure or lymphatics obstruction (61).
Adverse Events Associated With ICG
The reported incidence of adverse events is 1 out of 42 000 patients and most common reactions include urticaria, hypotension, syncope, and vasovagal reaction (2). In our review, no adverse events related to indocyanine green injection occurred in every full-text screened article. Tan et al. (61), on the other hand, described a 5-week-old patient with hypoplastic left heart syndrome who failed conservative management for bilateral chylothorax after a Norwood procedure and underwent a bedside lymphatic imaging using ICG-FA on postoperative day 18. Fluorescence lymphoscintigraphy allowed visualization of the proximal lymphatic drainage and helped to guide surgical treatment, but a few days later, the patient's clinical condition deteriorated as the abdominal ascites worsened and comfort care was offered (61). As chylothorax is a serious complication with high mortality rates, there were no adverse events associated with the ICG-FA and the patient's death was not considered related to ICG.
Discussion
Our review and narrative synthesis on the perioperative use of indocyanine green fluorescence angiography in pediatric patients included a total of 64 articles with 664 patients. It contains all articles relevant to the surgical use of ICG-FA in pediatrics and may serve as a reference guide for pediatric clinicians. Based on our results, ICG-FA technology is a promising surgical tool and appears safe for usage in pediatric patients. However, small sample sizes and types of included articles highlight the lack of robust evidence supporting the use of indocyanine green fluorescence angiography in the pediatric population.
There was remarkable heterogeneity across included studies. Indications, dose, and outcomes of indocyanine green fluorescence angiography were extremely variable. This made comparability between articles limited and quantitative analysis not possible in our study. Fluorescence interpretation was subjective in all of the included articles which made it difficult to compare, analyze, and draw conclusions from their results. Current published studies were of low-grade evidence and did not have a prospective calculation of study sample size.
We found that the doses and administration method of indocyanine green varied depending on surgical indications. While patients' demographic and clinical factors were generally well-presented, only 24 (38%) studies adequately mentioned the dose of indocyanine green. Other articles were either missing the weight of the patient or inconsistently reported the given dose amongst patients. In the United States, the suggested dose for tissue perfusion assessment is imprecise, ranging from 1.25 to 5 mg for children older than 1 month of age (2). For hepatobiliary anatomy visualization, 2.5 mg of the fluorescent agent is recommended for patients from 12 to 17 years old. In Europe, ICG dose recommendations are also vague and only focus on original ICG indications (ophthalmologic angiography, cardiac and hepatic function studies) (76). This wide dose range may lead to inaccurate dose of indocyanine green in children which can be either too high or insufficient, both compromising the fluorescence imaging. Conversely, Shafy et al. (55) have suggested ICG dosing guidelines based on a retrospective review of their dosing practices over a 2-year period. Dosing examples for fluorescence-guided oncology surgeries with ICG were also provided by Goldstein et al. (77). However, no phase I clinical trial has been conducted to test safety and adequate dose in children. There is, therefore, no consensus on the dose and timing of indocyanine green injection even in similar indications.
ICG-FA technology provides detailed anatomical and perfusion real-time assessment for different types of surgeries, but its interpretation remains subjective as there is no threshold for adequate perfusion in both adults and children. The SPY-Q software (Stryker, United States) is a postprocessing imaging analysis software which allows an objective quantification of the fluorescence and assessment of perfusion kinetics. However, no threshold value for necrosis has been previously determined (78). A retrospective study of 90 consecutive patients undergoing esophagectomy with gastric conduit reconstruction used an arbitrary value of 75% to position their anastomosis and showed a reduction of 20% of anastomotic leaks (79). In a Japanese prospective clinical trial of 70 consecutive adult patients undergoing a reconstructed gastric tube during esophagectomy, the authors reported that perfusion of the gastric tube anastomosis is sufficient if fluorescence appears within 60 s of the injection (80). Time to fluorescence is quantitative measure that has been studied and may be promising for correlation with tissue ischemia in the future.
Alternatives to indocyanine green fluorescence angiography have been reported in the literature, but ICG-FA appears superior. Doppler, fluorescein angiography, laser fluorescence angiography, pulse oximetry, laser tissue blood flowmetry, near-infrared spectroscopy are methods that have been reviewed (81, 82). ICG-FA tissue penetration is up to 10 mm (83) which allows better visualization of deeper vessels and creates an advantage over other analogous substances such as fluorescein (1). Its selective binding to plasma proteins reduces the leak from the circulation making this molecule ideal for angiography (81). Another advantage is its quick hepatic clearance rate that allows repeated injections during a procedure (1).
Whereas pediatric surgical indications for the use of ICG-FA remain scant, it is a frequently used and valid technology in adults. In 2015, a prospective multicenter clinical trial assessed the use of ICG-FA during left colectomies and anterior resection and observed a modification of the surgical plan in 11 patients (8%) (84). No anastomotic leak occurred in these patients. Multiple other studies demonstrated the potential benefits of this fluorescent agent including intraoperative decision improvement, decreased rate of postoperative complications (85), and avoiding stomas (84). In surgical oncology, ICG-FA is mainly used to improve identification of tumors and lymph nodes. In breast cancer, the fluorescence has a similar detection rate for sentinel lymph node compared to the current combination of radioactive technetium-99 m and lymphazuran blue (83). Recent studies have proven the ability of the ICG-FA to guide lymph node dissections and sentinel lymph nodes harvestings for metastatic melanoma, papillary thyroid microcarcinoma, and early ovarian cancer (1). ICG-FA can also be applied to the identification of ureters which can be very challenging in complex gynecological and colorectal cancer surgeries (86). Indocyanine green fluorescence angiography is also frequently used for adult reconstructive surgeries to facilitate intraoperative assessment of flap viability and anastomosis perfusion (87).
In the past years, indocyanine green fluorescence imaging has gained popularity in the pediatric population. After Lau and al.'s first overview of ICG applications in Pediatric Surgery in 2009, two other reviews have been published (74, 77, 88). Goldstein et al. (77) focused on the evolving applications in surgical oncology which still seem experimental, but promising for delineating tumor margins, localizing metastases, protecting important structures around the tumor, and assisting reconstruction. Paraboschi et al. (88) have published a systematic review including 21 studies on fluorescein sodium and indocyanine green imaging in pediatric surgery. Compared to our study, they included fluorescence imaging studies at large, excluded neurosurgical, vascular, ENT, and orthopedic articles, and their last search was in January 2020. These reviews confirm the growing interest in ICG-FA in pediatric surgical specialties but compared to our review, none of them critically assessed the risk of bias of published studies. Our systematic review and narrative synthesis include the highest number of published articles (n = 64), a rigorous methodology and risk of bias assessment.
The ongoing study of indocyanine green fluorescence angiography remains necessary for the full development of this technology amongst the pediatric population. Multiple preliminary experiences have shown the safety and usefulness of ICG-FA in pediatric abdominal surgeries including minimally invasive surgeries (22, 26), laparoscopic Palomo varicocelectomies (24), laparoscopic cholecystectomies (89), and laparoscopic partial nephrectomies (90). Currently, efforts are being made to standardize the technique and prove the benefits of the ICG-FA technology (89, 90). A study published after the updated search of this review suggested a dose of 0.35 mg/kg of indocyanine green, 16–18 h before performing a laparoscopic cholecystectomy (89). The authors reported a 17% technical failure of intra-operative ICG fluorescence visualization (n = 2). Absence of fluorescence was noted in one patient with Crigler-Najjar syndrome type 2 who was taking phenobarbital. Conversely, another patient experienced liver background hyperfluorescence due to the short delay of 8 h between the ICG injection and surgery. Another pediatric study compared indocyanine green fluorescence angiography to the standard technique during laparoscopic partial nephrectomy and showed a 53 min operative time reduction with the technology (p = 0.001) (90).
Results of this systematic review were mainly limited by the quality of available evidence. While 13/64 studies were prospective, they did not have a randomized allocation which may lead to bias. Most included articles were either case reports or case series (n = 36; 56%). Known limitations of the nature of these articles are the limited ability to generalize, retrospective design, and publication bias. Unpublished articles and abstracts were excluded. We recognize that including articles with mean or median age <18 years old is a limitation in our study. However, only 16% (10/64) of included studies combined an adult and pediatric population. Another limitation is that meta-analysis was not performed due to the important heterogeneity of the articles.
Conclusion
This systematic review and narrative synthesis bring together all relevant articles on the use of indocyanine green fluorescence angiography in pediatric patients. Indocyanine green fluorescence angiography is a safe surgical technology when used in the pediatric population. Pediatric applications of ICG currently remain limited, but there is an overall important increase in clinical applications of ICG-FA. Larger, controlled clinical studies are required to determine and standardize the adequate dose of ICG and timing of administration for various indications in children. Multicentric collaboration will likely be needed to accomplish this. The Delphi technique could be applied to gain consensus on indications and doses of ICG -FA in pediatric surgical specialties and improve data comparison.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
AL-N, PD, MK, CF, and NP contributed to conception and design of the study. AL-N organized the database. AL-N and MO'N analyzed all included studies. AL-N wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank our library technicians, Mélanie Durocher and Daniel Desrochers, for assistance with the articles search.
Abbreviations
ICG, indocyanine green; ICG-FA, indocyanine green fluorescence angiography; MINORS, methodological index for non-randomized studies; PRISMA, preferred reporting items for systematic reviews and meta-analyses.
References
1. Alander JT, Kaartinen I, Laakso A, Patila T, Spillmann T, Tuchin VV, et al. A review of indocyanine green fluorescent imaging in surgery. Int J Biomed Imaging. (2012) 2012:940585. doi: 10.1155/2012/940585
2. Technologies N. SPY AGENT Green (Product Monograph). (2018). Available online at: https://pdf.hres.ca/dpd_pm/00048972.PDF (accessed August 24, 2021).
3. Porcu EP, Salis A, Gavini E, Rassu G, Maestri M, Giunchedi P. Indocyanine green delivery systems for tumour detection and treatments. Biotechnol Adv. (2016) 34:768–89. doi: 10.1016/j.biotechadv.2016.04.001
4. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
5. Rothman KJ, Lash TL, VanderWeele TJ, Haneuse S. Modern Epidemiology. 4th ed. Philadelphia, PA: Wolters Kluwer (2021).
6. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2019). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed August 24, 2021).
7. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med. (2018) 23:60–3. doi: 10.1136/bmjebm-2017-110853
8. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. (2003) 73:712–6. doi: 10.1046/j.1445-2197.2003.02748.x
9. Ambekar S, Babu A, Pandey P, Devi IB. Intraoperative assessment of STA-MCA bypass patency using near-infrared indocyanine green video-angiography: a preliminary study. Neurol India. (2012) 60:604–7. doi: 10.4103/0028-3886.105194
10. Asayama B, Sato K, Fukui T, Okuma M, Nakagaki Y, Osato T, et al. Skull bone tumor resection with intraoperative indocyanine green fluorescence imaging: a series of four surgical cases. Interdiscipl Neurosurg. (2017) 9:8–13. doi: 10.1016/j.inat.2017.02.003
11. Aung T, Heidekrueger PI, Geis S, Von Kunow F, Taeger C, Strauss C, et al. A novel indication for indocyanine green (ICG): Intraoperative monitoring of limb and sciatic nerve perfusion during rotationplasty for sarcoma patients. Clin Hemorheol Microcirc. (2019) 70:441–7. doi: 10.3233/CH-189309
12. Bada-Bosch I, Mata DP, de la Torre M, Ordóñez J, Blanco MD, de Agustin J. Laparoscopic partial splenectomy assisted by fluorescence in a 13-year-old girl. Eur J Pediatr Surg Rep. (2020) 8:e81–e5. doi: 10.1055/s-0040-1716894
13. Bryant MK, Marulanda K, Phillips MR. Laparoscopic double cholecystectomy in a pediatric patient for gallbladder duplication: an unusual case of biliary anatomy. Am Surg. (2020) 86:1531–4. doi: 10.1177/0003134820933600
14. Calabro KA, Harmon CM, Vali K. Fluorescent cholangiography in laparoscopic cholecystectomy and the use in pediatric patients. J Laparoendosc Adv Surg Tech A. (2020) 30:586–9. doi: 10.1089/lap.2019.0204
15. Chang TI, Chen YS, Huang SC. Intraoperative indocyanine green fluorescence lymphography to detect chylous leakage sites after congenital heart surgery. J Thorac Cardiovasc Surg. (2014) 148:739–40. doi: 10.1016/j.jtcvs.2014.03.021
16. Chen-Yoshikawa TF, Hatano E, Yoshizawa A, Date H. Clinical application of projection mapping technology for surgical resection of lung metastasis. Interact Cardiovasc Thorac Surg. (2017) 25:1010–1. doi: 10.1093/icvts/ivx247
17. Cheng M-H, Liu TT-F. Lymphedema microsurgery improved outcomes of pediatric primary extremity lymphedema. Microsurgery. (2020) 40:7. doi: 10.1002/micr.30622
18. Chung PHY, Chok KSH, Wong KKY. Indocyanine green fluorescence-assisted laparoscopic hepatectomy for hepatocellular carcinoma in a pre-adolescent girl: a case report. Hong Kong medical journal = Xianggang yi xue za zhi. (2020) 26:342–4. doi: 10.12809/hkmj198106
19. Cleveland A, Abdelgawad A, Cook J, Pirela-Cruz M. Use of indocyanine green fluorescent dye video angiography in orthopaedic trauma: a pilot study. J Surg Orthop Adv. (2013) 22:310–5. doi: 10.3113/JSOA.2013.0310
20. Connolly PH, Meltzer AJ, Spector JA, Schneider DB. Indocyanine green angiography aids in prediction of limb salvage in vascular trauma. Ann Vasc Surg. (2015) 29:1453.e1–4. doi: 10.1016/j.avsg.2015.04.090
21. Drobot A, Ganam S, Karra N, Bickel A, Abu Shakra I, Kakiashvili E. Resection of an axillary macrocystic lymphatic malformation in a 14-year-old girl using intraoperative indocyanine green lymphography. J Vasc Surg Venous Lymphat Disord. (2020) 9:504–7. doi: 10.1016/j.jvsv.2020.04.003
22. Esposito C, Del Conte F, Cerulo M, Gargiulo F, Izzo S, Esposito G, et al. Clinical application and technical standardization of indocyanine green (ICG) fluorescence imaging in pediatric minimally invasive surgery. Pediatr Surg Int. (2019) 35:1043–50. doi: 10.1007/s00383-019-04519-9
23. Esposito C, Corcione F, Settimi A, Farina A, Centonze A, Esposito G, et al. Twenty-five year experience with laparoscopic cholecystectomy in the pediatric population-from 10 mm clips to indocyanine green fluorescence technology: long-term results and technical considerations. J Laparoendosc Adv Surg Tech A. (2019) 29:1185–91. doi: 10.1089/lap.2019.0254
24. Esposito C, Turra F, Del Conte F, Izzo S, Gargiulo F, Farina A, et al. Indocyanine green fluorescence lymphography: a new technique to perform lymphatic sparing laparoscopic palomo varicocelectomy in children. J Laparoendosc Adv Surg Tech A. (2019) 29:564–7. doi: 10.1089/lap.2018.0624
25. Esposito C, Coppola V, Del Conte F, Cerulo M, Esposito G, Farina A, et al. Near-infrared fluorescence imaging using indocyanine green (ICG): emerging applications in pediatric urology. J Pediatr Urol. (2020) 16:700–7. doi: 10.1016/j.jpurol.2020.07.008
26. Esposito C, Settimi A, Del Conte F, Cerulo M, Coppola V, Farina A, et al. Image-guided pediatric surgery using indocyanine green (icg) fluorescence in laparoscopic and robotic surgery. Front Pediatr. (2020) 8:314. doi: 10.3389/fped.2020.00314
27. Esposito C, Soria-Gondek A, Castagnetti M, Cerulo M, Del Conte F, Esposito G, et al. Laparoscopic or robotic deroofing guided by indocyanine green fluorescence and perirenal fat tissue wadding technique of pediatric simple renal cysts. J Laparoendosc Adv Surg Tech A. (2020) 30:471–6. doi: 10.1089/lap.2019.0650
28. Fernandez-Bautista B, Mata DP, Parente A, Perez-Caballero R, De Agustin JC. First experience with fluorescence in pediatric laparoscopy. Eur J Pediatr Surg Rep. (2019) 7:e43–e6. doi: 10.1055/s-0039-1692191
29. Fung CH, Lau CT, Wong KKY. Indocyanine green fluorescence-guided pulmonary wedge resection in a child: a case report. Hong Kong medical journal = Xianggang yi xue za zhi. (2020) 26:345–7. doi: 10.12809/hkmj198206
30. Greives MR, Aldrich MB, Sevick-Muraca EM, Rasmussen JC. Near-infrared fluorescence lymphatic imaging of a toddler with congenital lymphedema. Pediatrics. (2017) 139:e20154456. doi: 10.1542/peds.2015-4456
31. Guillén G, López-Fernández S, Molino JA, Bueno J, López M. Experiencia piloto con navegación mediante fluorescencia con verde de indocianina en cirugía pediátrica [Pilot experience with indocyanine green navigation in pediatric surgery]. Cir Pediatr. (2019) 32:121–27.
32. Herz D, DaJusta D, Ching C, McLeod D. Segmental arterial mapping during pediatric robot-assisted laparoscopic heminephrectomy: a descriptive series. J Pediatr Urol. (2016) 12:266. e1–6. doi: 10.1016/j.jpurol.2016.04.021
33. Hinchcliff KM, Yao A, Taub PJ. Laser-assisted indocyanine green imaging to assess perfusion of scalp closure in an infant. J Craniofac Surg. (2013) 24:2004–6. doi: 10.1097/SCS.0b013e3182a249ba
34. Hirayama Y, Iinuma Y, Yokoyama N, Otani T, Masui D, Komatsuzaki N, et al. Near-infrared fluorescence cholangiography with indocyanine green for biliary atresia. Real-time imaging during the Kasai procedure: a pilot study. Pediatr Surg Int. (2015) 31:1177–82. doi: 10.1007/s00383-015-3799-4
35. Horie N, Fukuda Y, Izumo T, Hayashi K, Suyama K, Nagata I. Indocyanine green videoangiography for assessment of postoperative hyperperfusion in moyamoya disease. Acta Neurochir. (2014) 156:919–26. doi: 10.1007/s00701-014-2054-4
36. Hori S, Kashiwazaki D, Akioka N, Hayashi T, Hori E, Umemura K, et al. Surgical anatomy and preservation of the middle meningeal artery during bypass surgery for moyamoya disease. Acta Neurochir. (2015) 157:29–36. doi: 10.1007/s00701-014-2282-7
37. Iinuma Y, Hirayama Y, Yokoyama N, Otani T, Nitta K, Hashidate H, et al. Intraoperative near-infrared indocyanine green fluorescence angiography (NIR-ICG AG) can predict delayed small bowel stricture after ischemic intestinal injury: report of a case. J Pediatr Surg. (2013) 48:1123–8. doi: 10.1016/j.jpedsurg.2013.03.067
38. Ishikawa K, Sasaki S, Furukawa H, Nagao M, Iwasaki D, Saito N, et al. Preliminary experience with intraoperative near-infrared fluorescence imaging in percutaneous sclerotherapy of soft-tissue venous malformations. Dermatol Surg. (2013) 39:907–12. doi: 10.1111/dsu.12152
39. Kaneshi Y, Shibasaki J, Aida N, Shimokaze T, Toyoshima K. Indocyanine green lymphography for congenital lymphatic dysplasia with tuberous sclerosis complex: a case report. Pediatr Int. (2020) 62:234–6. doi: 10.1111/ped.14071
40. Kato M, Nomura K, Ko Y, Kinami H, Tanami Y, Watanabe S, et al. The use of indocyanine green lymphography for the treatment of postoperative chylothorax with lipiodol lymphangiography in a 2-year-old child. J Pediatr Surg Case Rep. (2017) 23:46–9. doi: 10.1016/j.epsc.2017.06.005
41. Kato M, Watanabe S, Iida T, Watanabe A, Megumi F. Peri-orbital lymphangioma treated by lymphatic-venous anastomosis with indocyanine green lymphography analysis. J Pediatr Surg Case Rep. (2017) 23:9–14. doi: 10.1016/j.epsc.2017.05.008
42. Kato M, Watanabe S, Iida T, Watanabe A. Flow pattern classification in lymphatic malformations by indocyanine green lymphography. Plast Reconstr Surg. (2019) 143:558e−64e. doi: 10.1097/PRS.0000000000005362
43. Kim DL, Cohen-Gadol AA. Indocyanine-green videoangiogram to assess collateral circulation before arterial sacrifice for management of complex vascular and neoplastic lesions: technical note. World Neurosurg. (2013) 79:404.e1–6. doi: 10.1016/j.wneu.2012.07.028
44. Kitagawa N SM, Mochizuki K, Usui H, Miyagi H, Nakamura K, Tanaka M, et al. Navigation using indocyanine green fluorescence imaging for hepatoblastoma pulmonary metastases surgery. Pediatr Surg Int. (2015) 31:407–11. doi: 10.1007/s00383-015-3679-y
45. Kogon B, Fernandez J, Kanter K, Kirshbom P, Vincent B, Maher K, et al. The role of intraoperative indocyanine green fluorescence angiography in pediatric cardiac surgery. Ann Thorac Surg. (2009) 88:632–6. doi: 10.1016/j.athoracsur.2009.03.010
46. Martins DB, Farias-Eisner G, Mandelbaum RS, Hoang H, Bradley JP, Lee JC. Intraoperative indocyanine green laser angiography in pediatric autologous ear reconstruction. Plast Reconstr Surg Glob Open. (2016) 4:e709. doi: 10.1097/GOX.0000000000000696
47. Mihara M, Hara H, Shibasaki J, Seki Y, Hayashi A, Iida T, et al. Indocyanine green lymphography and lymphaticovenous anastomosis for generalized lymphatic dysplasia with pleural effusion and ascites in neonates. Ann Vasc Surg. (2015) 29:1111–22. doi: 10.1016/j.avsg.2015.02.013
48. Mitani Y, Kubota A, Ueno M, Takifuji K, Watanabe T, Hayami S, et al. Real-time identification of hepatoblastoma using a near infrared imaging with indocyanine green. J PediatrSurg Case Rep. (2014) 2:180–3. doi: 10.1016/j.epsc.2014.03.008
49. Nossek E, Setton A, Chalif DJ. Trapping and resection of cortical MCA mycotic aneurysm in eloquent area. Acta Neurochir. (2018) 160:579–82. doi: 10.1007/s00701-017-3401-z
50. Ogata F, Narushima M, Mihara M, Azuma R, Morimoto Y, Koshima I. Intraoperative lymphography using indocyanine green dye for near-infrared fluorescence labeling in lymphedema. Ann Plast Surg. (2007) 59:180–4. doi: 10.1097/01.sap.0000253341.70866.54
51. Otake K, Uchida K, Inoue M, Koike Y, Narushima M, Kusunoki M. Use of computed tomography-lymphangiography with direct injection of water-soluble contrast medium to identify the origin of chylous ascites. J Vasc Surg Venous Lymphat Disord. (2015) 3:90–3. doi: 10.1016/j.jvsv.2014.04.005
52. Pourmoghadam KK, Bunnell APM, O'Brien MC, DeCampli WM. Avoiding coronary injury in congenital heart surgery by laser-assisted indocyanine green dye imaging. World J Pediatr Congenit Heart Surg. (2014) 5:326–9. doi: 10.1177/2150135113514459
53. Rentea RM, Halleran DR, Ahmad H, Sanchez AV, Gasior AC, McCracken K, et al. Preliminary use of indocyanine green fluorescence angiography and value in predicting the vascular supply of tissues needed to perform cloacal, anorectal malformation, and hirschsprung reconstructions. Eur J Pediatr Surg. (2020) 30:505–11. doi: 10.1055/s-0039-1700548
54. Sanchez Fernandez C, Choque Cuba B, Rivero-Garvia M, Arteaga Romero FdB, Marquez Rivas JM. Combined microsurgical fluorescence for optimizing resection in refractory empyema and cerebritis. Child's Nervous Syst. (2020) 36:1835–41. doi: 10.1007/s00381-020-04762-9
55. Shafy SZ, Hakim M, Lynch S, Chen L, Tobias JD. Fluorescence imaging using indocyanine green dye in the pediatric population. J PediatrPharmacol Ther. (2020) 25:309–13. doi: 10.5863/1551-6776-25.4.309
56. Shibasaki J, Hara H, Mihara M, Adachi S, Uchida Y, Itani Y. Evaluation of lymphatic dysplasia in patients with congenital pleural effusion and ascites using indocyanine green lymphography. J Pediatr. (2014) 164:1116–20.e1. doi: 10.1016/j.jpeds.2013.12.052
57. Shirota C, Hinoki A, Takahashi M, Tanaka Y, Tainaka T, Sumida W, et al. New Navigation surgery for resection of lymphatic malformations using indocyanine green fluorescence imaging. Am J Case Rep. (2017) 18:529–31. doi: 10.12659/AJCR.903465
58. Shirotsuki R, Uchida H, Tanaka Y, Shirota C, Yokota K, Murase N, et al. Novel thoracoscopic navigation surgery for neonatal chylothorax using indocyanine-green fluorescent lymphography. J Pediatr Surg. (2018) 53:1246–9. doi: 10.1016/j.jpedsurg.2018.01.019
59. Souzaki R, Kawakubo N, Matsuura T, Yoshimaru K, Koga Y, Takemoto J, et al. Navigation surgery using indocyanine green fluorescent imaging for hepatoblastoma patients. Pediatr Surg Int. (2019) 35:551–7. doi: 10.1007/s00383-019-04458-5
60. Sugimoto T, Park YS, Nakagawa I, Nishimura F, Motoyama Y, Nakase H. Effectiveness of intraoperative indocyanine green videoangiography in direct surgical treatment of pediatric intracranial pial arteriovenous fistula. J Neurosurg Pediatr. (2015) 15:55–9. doi: 10.3171/2014.9.PEDS13683
61. Tan IC, Balaguru D, Rasmussen JC, Guilliod R, Bricker JT, Douglas WI, et al. Investigational lymphatic imaging at the bedside in a pediatric postoperative chylothorax patient. Pediatr Cardiol. (2014) 35:1295–300. doi: 10.1007/s00246-014-0946-y
62. Tanabe N, Yamamoto S, Kashiwazaki D, Akioka N, Kuwayama N, Noguchi K, et al. Indocyanine green visualization of middle meningeal artery before craniotomy during surgical revascularization for moyamoya disease. Acta Neurochir. (2017) 159:567–75. doi: 10.1007/s00701-016-3060-5
63. Takagi Y, Kikuta KI, Nozaki K, Sawamura K, Hashimoto N. Detection of a residual nidus by surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography in a child with a cerebral arteriovenous malformation—case report. J Neurosurg. (2007) 107:416–8. doi: 10.3171/PED-07/11/416
64. Takahashi N, Yamada Y, Hoshino K, Kawaida M, Mori T, Abe K, et al. Living donor liver re-transplantation for recurrent hepatoblastoma in the liver graft following complete eradication of peritoneal metastases under indocyanine green fluorescence imaging. Cancers. (2019) 11:730. doi: 10.3390/cancers11050730
65. Tomioka YK, Narushima M, Yamashita S, Ito A, Okazaki M. Foot web space transfer for congenital syndactyly. Plast Reconstr Surg Glob Open. (2020) 8:e3292. doi: 10.1097/GOX.0000000000003292
66. Tsuzuki S, Aihara Y, Eguchi S, Amano K, Kawamata T, Okada Y. Application of indocyanine green (ICG) fluorescence for endoscopic biopsy of intraventricular tumors. Childs Nerv Syst. (2014) 30:723–6. doi: 10.1007/s00381-013-2266-6
67. Ueba T, Abe H, Matsumoto J, Higashi T, Inoue T. Efficacy of indocyanine green videography and real-time evaluation by FLOW 800 in the resection of a spinal cord hemangioblastoma in a child: case report. J Neurosurg Pediatr. (2012) 9:428–31. doi: 10.3171/2011.12.PEDS11286
68. Vogt PR, Bauer EP, Graves K. Novadaq spy intraoperative imaging system—current status. Thorac Cardiovasc Surg. (2003) 51:49–51. doi: 10.1055/s-2003-37276
69. Yada K, Migita M, Nakamura R, Abe S, Matsufuji H. Indocyanine green fluorescence during pediatric stoma closure. J Pediatr Surg Case Rep. (2020) 61:4. doi: 10.1016/j.epsc.2020.101595
70. Yamamichi T, Oue T, Yonekura T, Owari M, Nakahata K, Umeda S, et al. Clinical application of indocyanine green (ICG) fluorescent imaging of hepatoblastoma. J Pediatr Surg. (2015) 50:833–6. doi: 10.1016/j.jpedsurg.2015.01.014
71. Yanagi Y, Yoshimaru K, Matsuura T, Shibui Y, Kohashi K, Takahashi Y, et al. The outcome of real-time evaluation of biliary flow using near-infrared fluorescence cholangiography with Indocyanine green in biliary atresia surgery. J Pediatr Surg. (2019) 54:2574–8. doi: 10.1016/j.jpedsurg.2019.08.029
72. Yokoyama S, Nakaoka T. Successful use of intraoperative ICG fluorescence lymphography and fibrin sealant with PGA felt for refractory chylous ascites in an infant: a novel procedure. Pediatr Int. (2020) 62:862–3. doi: 10.1111/ped.14190
73. Nossek E, Chalif DJ, Buciuc R, Gandras EJ, Anderer EG, Insigna S, et al. Intraoperative angiography for arteriovenous malformation resection in the prone and lateral positions, using upper extremity arterial access. Oper Neurosurg. (2017) 13:352–60. doi: 10.1093/ons/opw034
74. Lau CT, Au DM, Wong KKY. Application of indocyanine green in pediatric surgery. Pediatr Surg Int. (2019) 35:1035–41. doi: 10.1007/s00383-019-04502-4
75. Boogerd LSF, Handgraaf HJM, Huurman VAL, Lam HD, Mieog JSD, van der Made WJ, et al. The best approach for laparoscopic fluorescence cholangiography: overview of the literature and optimization of dose and dosing time. Surg Innov. (2017) 24:386–96. doi: 10.1177/1553350617702311
76. Green D. Available online at: https://diagnosticgreen.com/row/wp-content/uploads/sites/2/2019/08/Spain-PIL.pdf (accessed August 24, 2021).
77. Goldstein SD, Heaton TE, Bondoc A, Dasgupta R, Abdelhafeez A, Davidoff AM, et al. Evolving applications of fluorescence guided surgery in pediatric surgical oncology: A practical guide for surgeons. J Pediatr Surg. (2020) 56:215–23. doi: 10.1016/j.jpedsurg.2020.10.013
78. Newman MI, Jack MC, Samson MC. SPY-Q analysis toolkit values potentially predict mastectomy flap necrosis. Ann Plast Surg. (2013) 70:595–8. doi: 10.1097/SAP.0b013e3182650b4e
79. Campbell C, Reames MK, Robinson M, Symanowski J, Salo JC. Conduit vascular evaluation is associated with reduction in anastomotic leak after esophagectomy. J Gastrointest Surg. (2015) 19:806–12. doi: 10.1007/s11605-015-2794-3
80. Kumagai Y, Hatano S, Sobajima J, Ishiguro T, Fukuchi M, Ishibashi KI, et al. Indocyanine green fluorescence angiography of the reconstructed gastric tube during esophagectomy: efficacy of the 90-second rule. Dis Esophagus. (2018) 31:doy052. doi: 10.1093/dote/doy052
81. Urbanavicius L, Pattyn P, de Putte DV, Venskutonis D. How to assess intestinal viability during surgery: A review of techniques. World J Gastrointest Surg. (2011) 3:59–69. doi: 10.4240/wjgs.v3.i5.59
82. Gurtner GC, Jones GE, Neligan PC, Newman MI, Phillips BT, Sacks JM, et al. Intraoperative laser angiography using the SPY system: review of the literature and recommendations for use. Ann Surg Innov Res. (2013) 7:1. doi: 10.1186/1750-1164-7-1
83. Kitai T, Inomoto T, Miwa M, Shikayama T. Fluorescence navigation with indocyanine green for detecting sentinel lymph nodes in breast cancer. Breast Cancer. (2005) 12:211–5. doi: 10.2325/jbcs.12.211
84. Jafari MD, Wexner SD, Martz JE, McLemore EC, Margolin DA, Sherwinter DA, et al. Perfusion assessment in laparoscopic left-sided/anterior resection (PILLAR II): a multi-institutional study. J Am Coll Surg. (2015) 220:82–92.e1. doi: 10.1016/j.jamcollsurg.2014.09.015
85. Kudszus S, Roesel C, Schachtrupp A, Hoer JJ. Intraoperative laser fluorescence angiography in colorectal surgery: a noninvasive analysis to reduce the rate of anastomotic leakage. Langenbecks Arch Surg. (2010) 395:1025–30. doi: 10.1007/s00423-010-0699-x
86. Park H, Farnam RW. Novel use of indocyanine green for intraoperative, real-time localization of ureter during robot-assisted excision of endometriosis. J Minim Invasive Gynecol. (2015) 22:S69. doi: 10.1016/j.jmig.2015.08.185
87. Holm C, Mayr M, Hofter E, Dornseifer U, Ninkovic M. Assessment of the patency of microvascular anastomoses using microscope-integrated near-infrared angiography: a preliminary study. Microsurgery. (2009) 29:509–14. doi: 10.1002/micr.20645
88. Paraboschi I, De Coppi P, Stoyanov D, Anderson J, Giuliani S. Fluorescence imaging in pediatric surgery: state-of-the-art and future perspectives. J Pediatr Surg. (2020) 56:655–62. doi: 10.1016/j.jpedsurg.2020.08.004
89. Esposito C, Alberti D, Settimi A, Pecorelli S, Boroni G, Montanaro B, et al. Indocyanine green (ICG) fluorescent cholangiography during laparoscopic cholecystectomy using RUBINA technology: preliminary experience in two pediatric surgery centers. Surg Endosc. (2021). doi: 10.1007/s00464-021-08596-7. [Epub ahead of print].
90. Esposito C, Autorino G, Coppola V, Esposito G, Paternoster M, Castagnetti M, et al. Technical standardization of ICG near-infrared fluorescence (NIRF) laparoscopic partial nephrectomy for duplex kidney in pediatric patients. World J Urol. (2021). doi: 10.1007/s00345-021-03759-6. [Epub ahead of print].
Keywords: colorectal anastomosis, pediatric surgery, indocyanine green, fluorescence angiography, intraoperative assessment, perfusion
Citation: Le-Nguyen A, O'Neill Trudeau M, Dodin P, Keezer MR, Faure C and Piché N (2021) The Use of Indocyanine Green Fluorescence Angiography in Pediatric Surgery: A Systematic Review and Narrative Analysis. Front. Pediatr. 9:736242. doi: 10.3389/fped.2021.736242
Received: 04 July 2021; Accepted: 18 August 2021;
Published: 13 September 2021.
Edited by:
Francesco Morini, Meyer Children's Hospital, ItalyReviewed by:
Felice Crocetto, Federico II University Hospital, ItalyTakuro Ariga, University of the Ryukyus Hospital, Japan
Copyright © 2021 Le-Nguyen, O'Neill Trudeau, Dodin, Keezer, Faure and Piché. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nelson Piché, bmVsc29uLnBpY2hlLmhzaiYjeDAwMDQwO3Nzc3MuZ291di5xYy5jYQ==