 Fengming Ji
Fengming Ji Haoyu Tang
Haoyu Tang Chengchuang Wu
Chengchuang Wu Li Chen
Li Chen Huake Wang
Huake Wang Bing Yan1*
Bing Yan1*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 13 September 2021
Sec. Pediatric Urology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.690863
Background: This study explored the predictive value of postoperative C-reactive protein in children with hypospadias for postoperative complications and the risk factors.
Methods: The clinical and follow-up data of 106 children with hypospadias who were treated with operations at Kunming Children's Hospital in 2020 were, respectively, analyzed. According to the occurrence of postoperative complications, the patients were divided into two groups: 25 patients with postoperative complications were the complications group, and 81 without postoperative complications were the control group. The baseline data, clinical characteristics, laboratory test indexes, and outcome of the two groups were collected. Receiver operating characteristic (ROC) was used to calculate the optimal cutoff value of C-reaction protein (CRP). Logistic regression was used to analyze the risk factors of hypospadias after surgery. A probability value (P) < 0.05 was considered statistically significant.
Results: According to the result of the ROC curve, the optimal cutoff value of CRP was 11.7 mg/L. Logistic regression showed that the length of urethral defect, the urethral material, the operative produce, and the postoperative CRP level were related to the occurrence of postoperative complications of patients with DCC. The length of the urethral defect and the CRP level were the independent risk factors of the prognosis of hypospadias patients. The CRP level was related to the occurrence of postoperative complications and fistula.
Conclusions: Postoperative CRP level can be used as a reliable marker for predicting the prognosis of hypospadias patients.
Hypospadias is a common congenital malformation in male individuals, which is mainly manifested by an abnormal ventral opening of the urethral meatus, abnormal distribution of foreskin, and chordee. The incidence of hypospadias is about 1/300–1/250 (1, 2). In the past 30 years, the incidence of hypospadias has been on the rise (3, 4). Heredity and gene mutations are common causes of hypospadias, and mutations of androgen receptor, Wilms tumor protein-1, steroid-α reductase, and other genes are closely related to the occurrence of hypospadias. Moreover, ecological environmental pollution, maternal exposure history of estrogen and antiepileptic drugs during pregnancy, maternal history of hypertension or hepatitis B virus infection, multiple births, and placental insufficiency are also potential risk factors for hypospadias (1, 5, 6).
Surgery is the only cure for hypospadias, and the repair of hypospadias aims to create a straight penis, a neourethra with a meatus at the tip of glans, and a normal appearance of a circumcised phallus (7, 8). However, long-term follow-up studies have found that adults with hypospadias may have abnormal urethral function, unsatisfactory appearance of the penis, and problems with erection, ejaculation, or sexual intercourse, which often negatively affect their quality of life (9). Many people with hypospadias need psychological treatment as adults. Improving the operative success rate is the key to cure genitalia malformations and meet the cosmetic needs of patients.
After more than 100 years of accumulation and evolution, there are more than 300 kinds of hypospadias surgical methods (10). However, due to the delicate and complex operation and the high technical difficulty of the operation itself, restricted by own conditions of the patient, the success rate after hypospadias is still low at present. Nearly 15–50% of patients need repeated operations, which not only causes a waste of medical resources but also seriously affects the appearance and function of the external genitalia of the patient' (11, 12). Therefore, how to improve the success rate of hypospadias surgery is still an important challenge for urologists for a long time.
In recent years, inflammatory markers have played an important role in the study of various postoperative complications. The acute-phase protein C-reactive protein (CRP) is a key factor in the clearance of bacteria and dying cells, so CRP is an important biomarker for inflammation (13). We hypothesized that CRP is associated with surgical outcomes in patients with hypospadias. Elevated CRP leads to an increased incidence of postoperative complications. The aim of this study was to confirm the relationship between postoperative complications of hypospadias and CRP.
A retrospective database on patients with a primary hypospadias repair at Kunming Children's Hospital was performed in 2020. All the children included in the study signed the relevant informed consent before surgery. According to the location of the ventral opening, the degree of curvature, the condition of the urethral plate, and the distribution of foreskin, the operation produced was selected. All operations were performed by the same experienced surgeon. Blood routine and CRP tests were performed on the first day after surgery. Cefazolin sodium pentahydrate was routinely given half an hour before surgery and 5–7 days after surgery as prophylactic antibiotics (14). If surgical site infections occur, the duration of antibiotic use and the types of antibiotics were extended according to the infection situation. All patients were routinely indwelling an F6 or F8 all-silicone urethral catheter after the surgery, and the catheter was removed 10–30 days after the operation. The diameter of the urethral stent was according to the condition of the children.
All blood samples were obtained 24 h after surgery. The inclusion criteria of this study were as follows: (1) The clinical information of patients were complete; (2) Follow-up data were obtained for all patients; and (3) Patients only underwent urethral repair. The exclusion criteria included the following conditions: (1) the clinical information of the patients was incomplete, (2) patients who underwent urethral repair and other surgery (undescended testis or inguinal hernia), (3) patients were lost to follow-up.
All the patients were followed up by outpatient consultation and telephone, and the follow-up deadline was February 1, 2021. The complications included overall complications, fistula, stricture, diverticulum, and glans split.
The optimal cutoff values of CRP and WBC were determined by ROC curves. Enumeration data were expressed as median and interquartile range (IQR). The analysis of risk factors for overall complications adopted univariate and multivariate binary logistic regression analysis, and the results were expressed as a hazard ratio with 95% confidence interval (95% CI). t-test was used to analyze the correlation between CRP and complications. P < 0.05 was considered a statistically significant difference. The statistical analyses were performed with the Statistical Package of the Social Sciences (SPSS), version 21.0.
A total of 106 children were included in this study (the general information of the patients is shown in Table 1). The median follow-up was 6 months (IQR: 5–10). There were 25 cases in the complications group and 81 cases in the control group. The median age was 42 months (IQR: 35–58). The hypospadias classification included were 37 proximal, 47 middle, and 22 distal, respectively. The surgical procedures included MAGPI, tubularized incised urethral plate urethroplasty (TIP), Onlay island flap urethroplasty (Onlay), Koyanagi, two-stage urethroplasty, and Duplay (the general information of the patients and the results of the binary logistic regression univariate analysis are shown in Table 1). A total of 25 children had postoperative complications. Among all complications, the most common one was fistula with 16 on 25 complications. A total of 81 patients were cured, and the overall operation success rate was 76.42% at a median follow-up of 6 months.
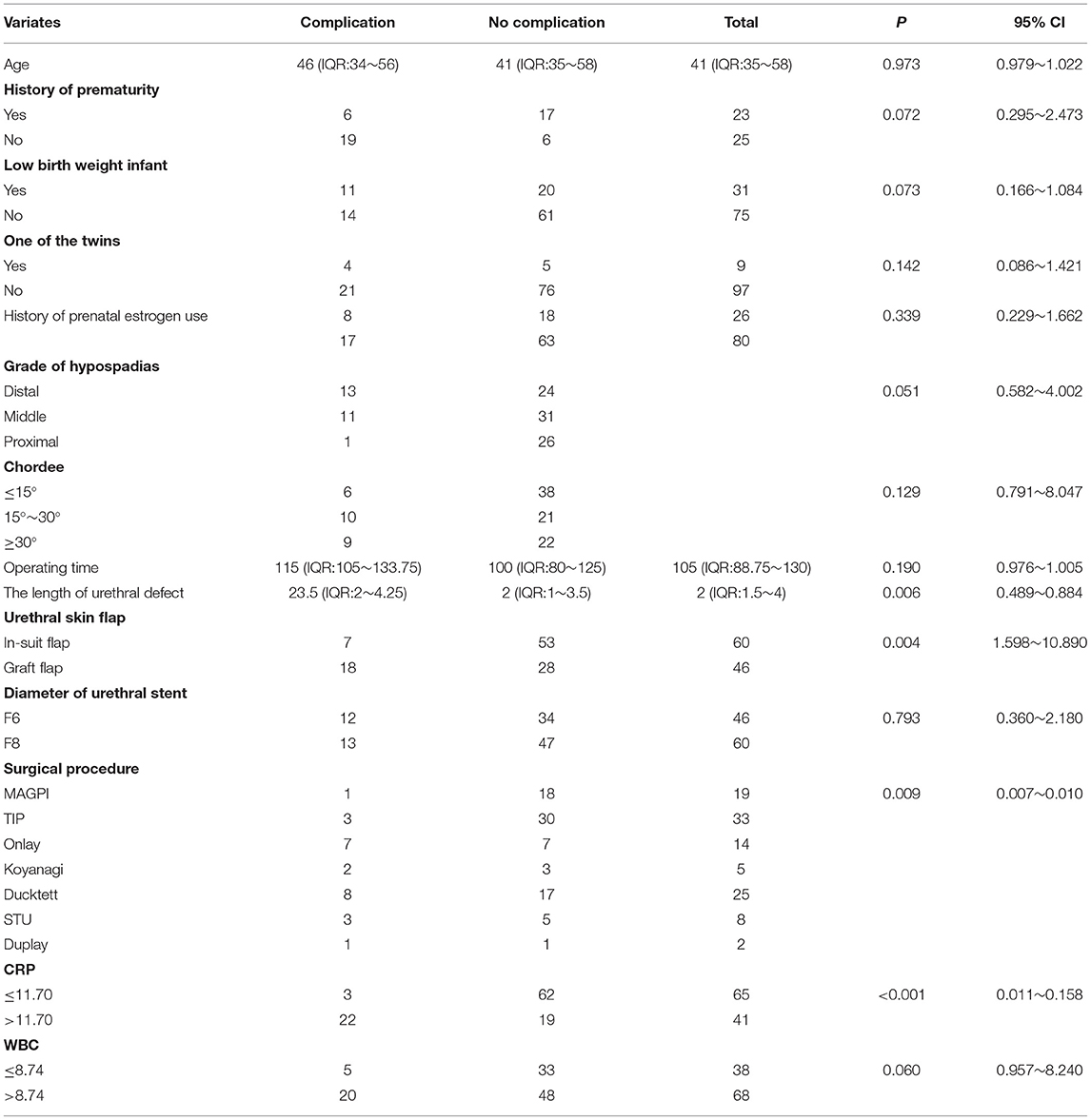
Table 1. The results of binary logistic regression univariate analysis.
According to the ROC curve analysis, the optimal cutoff value of CRP was 11.70 for predicting postoperative overall complication. The area under ROC curve for survival status was 0.882, with 95% CI of 0.820–0.944 (P < 0.001). The sensitivity and the specificity of CRP for hypospadias were 100 and 76.2%, respectively (Figure 1).

Figure 1. ROC curve of CRP.
The optimal cutoff value of WBC was 8.74 for predicting postoperative overall complication. The area under ROC curve for survival status was 0.620, with 95% CI of 0.493–0.0.747 (P = 0.071). The sensitivity and the specificity of WBC for hypospadias were 80 and 42.5%, respectively (Figure 2).

Figure 2. ROC curve of WBC.
A binary logistic regression model was used to find the risk factors for the overall complications, and the analyzed factors include age, operative time, the length of urethral defect, urethral material (in-suit flap or graft flap from foreskin or scrotum), the diameter of the urethral stent, surgical procedure, CRP, and WBC. The results showed that the length of the urethral defect (P = 0.006), the resource of urethral skin flap (P = 0.004), the surgical procedure (P = 0.009), and CRP (P < 0.001) were the risk factors affecting the success rate of hypospadias. Among the four risk factors, urethral material and CRP (<0.001) were independent risk factors for the overall complications (the result of the binary logistic regression model is shown in Table 2).
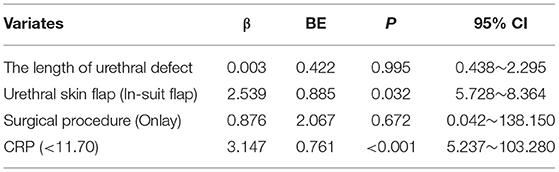
Table 2. The result of binary logistic regression model.
An independent-sample t-test was used to analyze the correlation between CRP value and overall complications, fistula, stricture, diverticulum, and glans split. The results showed that CRP was associated with overall complications (P < 0.001) and urethral fistula (P < 0.001), and the difference was statistically significant (the relationship between CRP and clinical characteristics in hypospadias is shown in Table 3).
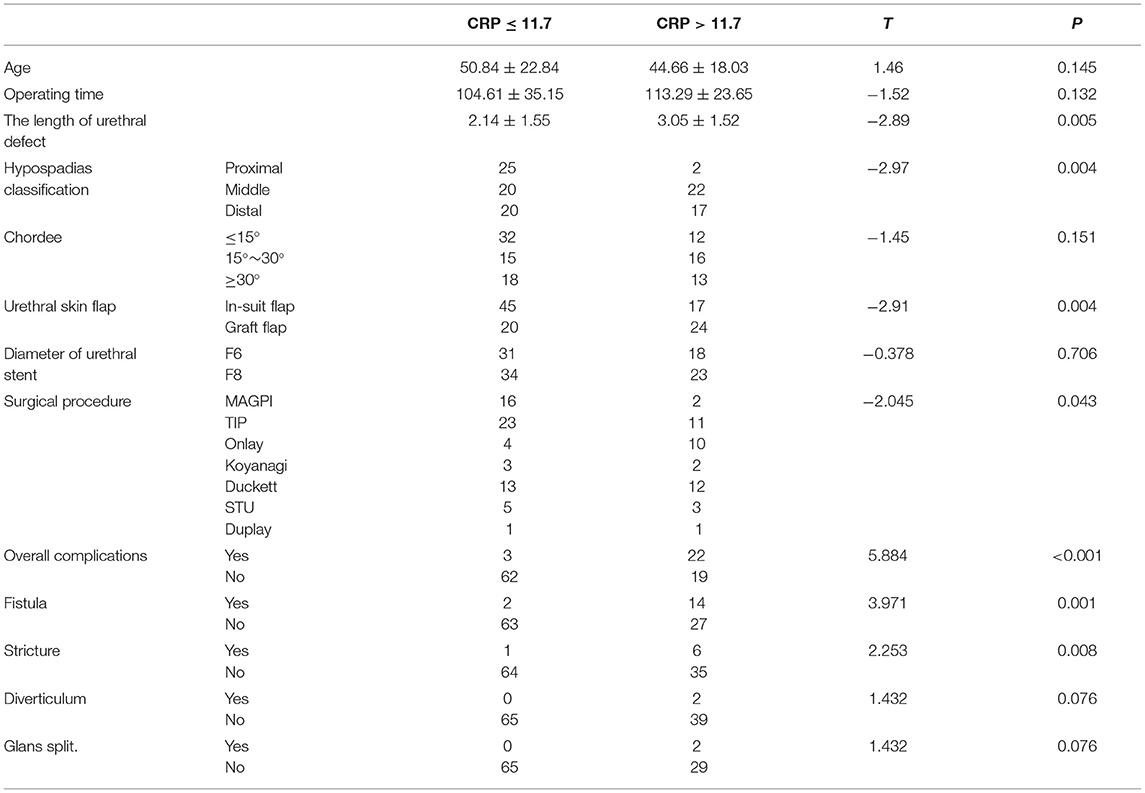
Table 3. Relationship between CRP and clinical characteristics in hypospadias.
The repair of hypospadias was recorded by Galen in the first to second century AD. In 1994, Snodgrass successfully performed and reported the TIP procedure for the first time. Up to now, TIP has become the most commonly used technique for the treatment of proximal and middle hypospadias, and it is the most popular procedure in Europe (15, 16). In 1980 and 1987, Duckett successively performed the Duckett and Onlay surgical procedures, in which the newly formed urethra was composed entirely or with the involvement of the prepuce inner plate with a vascularized pedicle, which greatly improved the primary cure rate of patients with hypospadias (17, 18). Although the surgical methods of hypospadias are constantly improving and evolving, there is still no surgical procedure that can be used as the gold standard for all types of hypospadias. Common complications of hypospadias include fistula, stricture, diverticula, and glans split (19). Studies have pointed out that the age of the patient, the length of the urethral defect, chordee, glans width, surgical procedure, anesthesia method, the diameter of the urethral stent, and preoperative hormone use history are all related to the success rate of surgery (7, 20–22).
This study retrospectively analyzed the clinical and follow-up data of 106 children with hypospadias and found that the urethral skin flap and CRP, as independent risk factors, had a high predictive value for postoperative complications. The incidence of postoperative complications in patients with CRP > 11.7 on the first day after surgery was significantly higher than that in patients with CRP ≤ 11.7, and the sensitivity and the specificity were 100 and 76.2%, respectively. The role of CRP has attracted a lot of attention in recent years, and many studies have pointed out that CRP is closely related to the prognosis of surgical patients. Hoeller et al. (23) pointed out that CRP had a high predictive value for postoperative surgical site infection after dorsal spondylodesis, with sensitivity of 92.9% and specificity of 78.2%. Messies et al. (24) demonstrated that CRP ≥ 180 mg/L on the 4th day after surgery was an independent risk factor for predicting anastomotic fistula after primary anastomosis in patients with rectal cancer (P = 0.002), with sensitivity and specificity of 72.3 and 88.9%, respectively. Johnson et al. (25) found that postoperative CRP value was an independent risk factor affecting 1-year tumor-free survival (P < 0.001) and 1-year overall survival (P < 0.001) after nephrectomy in patients with local renal cancer.
CRP is an acute-phase protein that appears in the process of the acute inflammatory response of the body. The level of plasma CRP in healthy individuals is <1 mg/L (26). When an inflammatory response occurs in the body, interleukin-6 can stimulate the liver cells to produce and secrete CRP rapidly, so that plasma CRP level can rise rapidly within 24–72 h, and then CRP can be produced by vascular smooth muscle cells, adipocytes, and kidneys (27). Now that CRP is highly sensitive to bacterial infection and is not affected by gender, age, anemia, and other factors, CRP has a high diagnostic value for infection-related diseases (28). CRP is a member of the superfamily of pentraxins, and it consists of five identical, non-covalently attached subunits (29). The pentameric structure of CRP includes an effector surface with an affinity for C1q and Fcy receptors and a recognition surface, which can bind phosphoric acid to dead cells and pathogens as well as nuclear components exposed in the process of apoptosis to clear necrotic cells and pathogens and protect autoimmunity (30–32). The half-life of CRP in the circulation is very short, about 19 h, and decreases rapidly after the relief of the acute reaction. Therefore, CRP is widely used in clinical practice as an important marker of acute infection (33).
Urethral fistula is the most common postoperative complication of hypospadias, with an incidence of about 5–10% (34, 35). Urethral fistula is related to flap ischemia, infection, high tension of the shaped urethra, and improper or too thin urethral covering (36, 37). In this study, the CRP value on the first postoperative day was associated with the occurrence of a urethral fistula (P < 0.001), and both urethral skin flap and CRP were independent risk factors affecting the success rate of hypospadias surgery. The reason is that the blood supply and the nutrition of the migratory skin flap completely depended on the vessel pedicle at the early stage, and the new blood circulation system was gradually established for the skin flap about 3 weeks after the operation (37). In the process of dissection, the migration flap is prone to damage excessive nourishing vessels, leading to the fistula due to the ischemic necrosis of the flap and stimulating the increase of CRP in peripheral blood.
Due to the small sample size and short follow-up time included in the study, the surgical method and length of the urethral defect in this study did not have great predictive value, which was different from existing studies. Due to the short follow-up time, the rate of stricture and diverticulum appeared to be low, actual surgical success need to be time censored with further follow-up. WBC is highly sensitive to predict bacterial infection, but this study found that WBC value is not correlated with postoperative complications of hypospadias. It is considered that peripheral blood white blood cells have poor stability, and bacterial infection, trauma, and stress can lead to the increase of WBC. Secondly, this study is a retrospective study, with some deficiencies in the integrity and homogeneity of the sample data, and the results of the study inevitably have a certain degree of recall bias. Finally, other variables including weight and BMI, history of prematurity, IGR, weight at birth, grade of hypospadias may be other potential risk factors but were not analyzed in this study.
In conclusion, the length of the urethral defect, urethral material, surgical method, and CRP are related to the prognosis of patients with hypospadias. Urethral material and postoperative CRP value are independent risk factors for the prognosis of patients with hypospadias. The CRP value is easy to obtain and cheap in practical clinical work. Routine test of CRP value after surgery is helpful for the early identification of high-risk patients. For the high-risk patients, intervention measures should be given timely, such as keeping on antibiotics for a longer time or keeping the catheter for more days, which has a great significance for improving the success rate of hypospadias surgery.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
This study was approved by the Medical Ethics Committee of Kunming Children's Hospital.
FJ collected, analyzed data, and drafted the original manuscript. HT and LC collected data and participated in amending the manuscript. CW collected and analyzed data. HW analyzed data. BY designed the present study and amended the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lin HC, Guo JM, Ge P, Ou P. Association between prenatal exposure to ambient particulate matter and risk of hypospadias in offspring: a systematic review and meta-analysis. Environ Res. (2021) 192:110190. doi: 10.1016/j.envres.2020.110190
2. Ghazarian AA, Trabert B, Graubard BI, Longnecker MP, Klebanoff MA, McGlynn KA. Placental weight and risk of Cryptorchidism and Hypospadias in the collaborative perinatal project. Am J Epidemiol. (2018) 187:1354–61. doi: 10.1093/aje/kwy005
3. Czeizel A. Increasing trends in congenital malformations of male external genitalia. Lancet. (1985) 1:462–3. doi: 10.1016/S0140-6736(85)91185-7
4. Nassar N, Bower C, Barker A. Increasing prevalence of hypospadias in Western Australia, 1980-2000. Arch Dis Child. (2007) 92:580–4. doi: 10.1136/adc.2006.112862
5. Zhu C, Zhang B, Peng T, Li MQ, Ren YY, Wu JN. Association of abnormal placental perfusion with the risk of male hypospadias: a hospital-based retrospective cohort study. BMC Pregnancy Childbirth. (2020) 20:673. doi: 10.1186/s12884-020-03381-1
6. Sun G, Tang D, Liang J, Wu M. Increasing prevalence of hypospadias associated with various perinatal risk factors in chinese newborns. Urology. (2009) 73:1241–5. doi: 10.1016/j.urology.2008.12.081
7. Yang H, Xuan XX, Hu DL, Zhang H, Shu Q, Guo XD, et al. Comparison of effect between dartos fascia and tunica vaginalis fascia in TIP urethroplasty: a meta-analysis of comparative studies. BMC Urol. (2020) 20:161. doi: 10.1186/s12894-020-00737-9
8. Wu Y, Wang J, Zhao T, Wei Y, Han L, Liu X, et al. Complications following primary repair of non-proximal Hypospadias in children: a systematic review and meta-analysis. Front Pediatr. (2020) 8:579364. doi: 10.3389/fped.2020.579364
9. Hoag CC, Gotto GT, Morrison KB, Coleman GU, Macneily AE. Long-term functional outcome and satisfaction of patients with hypospadias repaired in childhood. Can Urol Assoc J. (2008) 2:23–31. doi: 10.5489/cuaj.521
10. Huang Y, Xie H, Lv Y, Yu L, Sun L, Li X, et al. One-stage repair of proximal hypospadias with severe chordee by in situ tubularization of the transverse preputial island flap. J Pediatr Urol. (2017) 13:296–9. doi: 10.1016/j.jpurol.2017.02.015
11. Xiao D, Nie X, Wang W, Zhou J, Zhang M, Zhou Z, et al. Comparison of transverse island flap onlay and tubularized incised-plate urethroplasties for primary proximal hypospadias: a systematic review and meta-analysis. PLoS ONE. (2014) 9:e106917. doi: 10.1371/journal.pone.0106917
12. Duarsa G, Tirtayasa P, Daryanto B, Nurhadi P, Renaldo J, Tarmono T, et al. Common practice of Hypospadias Management by Pediatric Urologists in Indonesia: a multi-center descriptive study from Referral Hospitals. Open Access Maced J Med Sci. (2019) 7:2242–5. doi: 10.3889/oamjms.2019.628
13. Enocsson H, Gullstrand B, Eloranta ML, Wetterö J, Leonard D, Rönnblom L, et al. C-reactive protein levels in systemic lupus erythematosus are modulated by the interferon gene signature and CRP gene polymorphism rs1205. Front Immunol. (2020) 11:622326. doi: 10.3389/fimmu.2020.622326
14. Canon SJ, Smith JC, Sullivan E, Patel A, Zamilpa I. Comparative analysis of perioperative prophylactic antibiotics in prevention of surgical site infections in stented, distal hypospadias repair. J Pediatr Urol. (2021) 17:256.e1–256.e5. doi: 10.1016/j.jpurol.2020.11.033
15. Springer A, Krois W, Horcher E. Trends in hypospadias surgery: results of a worldwide survey. Eur Urol. (2011) 60:1184–9. doi: 10.1016/j.eururo.2011.08.031
16. Cook A, Khoury AE, Neville C, Bagli DJ, Farhat WA, Pippi Salle JL. A multicenter evaluation of technical preferences for primary hypospadias repair. J Urol. (2005) 174:2354–7, discussion 2357. doi: 10.1097/01.ju.0000180643.01803.43
17. Hueber PA, Salgado Diaz M, Chaussy Y, Franc-Guimond J, Barrieras D, Houle AM. Long-term functional outcomes after penoscrotal hypospadias repair: a retrospective comparative study of proximal TIP, Onlay, and Duckett. J Pediatr Urol. (2016) 12:198.e1–6. doi: 10.1016/j.jpurol.2016.04.034
18. Lyu Y, Yu L, Xie H, Huang Y, Li X, Sun L, et al. Comparison of short-term complications between Onlay and Duckett urethroplasty and the analysis of risk factors. Int Urol Nephrol. (2019) 51:783–8. doi: 10.1007/s11255-019-02125-1
19. Patel RP, Shukla AR, Snyder HM III. The island tube and island onlay hypospadias repairs offer excellent long-term outcomes: a 14-year followup. J Urol. (2004) 172:1717–9; discussion 1719. doi: 10.1097/01.ju.0000138903.20136.22
20. Dokter EM, Mouës CM, Rooij I, Biezen J. Complications after Hypospadias correction: prognostic factors and impact on final clinical outcome. Eur J Pediatr Surg. (2018) 28:200–6. doi: 10.1055/s-0037-1599230
21. Yildiz T, Tahtali IN, Ates DC, Keles I, Ilce Z. Age of patient is a risk factor for urethrocutaneous fistula in hypospadias surgery. J Pediatr Urol. (2013) 9:900–3. doi: 10.1016/j.jpurol.2012.12.007
22. Bush NC, Villanueva C, Snodgrass W. Glans size is an independent risk factor for urethroplasty complications after hypospadias repair. J Pediatr Urol. (2015) 11:355.e1–5. doi: 10.1016/j.jpurol.2015.05.029
23. Hoeller S, Roch PJ, Weiser L, Hubert J, Lehmann W, Saul D. C-reactive protein in spinal surgery: more predictive than prehistoric. Eur Spine J. (2021) 30:1261–9. doi: 10.1007/s00586-021-06782-8
24. Messias BA, Botelho RV, Saad SS, Mocchetti ER, Turke KC, Waisberg J. Serum C-reactive protein is a useful marker to exclude anastomotic leakage after colorectal surgery. Sci Rep. (2020) 10:1687. doi: 10.1038/s41598-020-58780-3
25. Johnson TV, Abbasi A, Owen-Smith A, Young AN, Kucuk O, Harris WB, et al. Postoperative better than preoperative C-reactive protein at predicting outcome after potentially curative nephrectomy for renal cell carcinoma. Urology. (2010) 76:766.e1–5. doi: 10.1016/j.urology.2010.01.052
26. Liu J, Zhu W, Sun H, Song D, Xiao P, Xu B, et al. Development of a primary reference material of natural C-reactive protein: verification of its natural pentameric structure and certification by two isotope dilution mass spectrometry. Anal Methods. (2021) 13:626–35. doi: 10.1039/D0AY02289F
27. Yayla C, Gayretli Yayla K. C-Reactive protein to albumin ratio in patients with saphenous vein graft disease. Angiology. (2021) 72:770–5. doi: 10.1177/0003319721998863
28. Pepys MB, Baltz ML. Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv Immunol. (1983) 34:141–212. doi: 10.1016/S0065-2776(08)60379-X
29. Thiele JR, Zeller J, Bannasch H, Stark GB, Peter K, Eisenhardt SU. Targeting C-reactive protein in inflammatory disease by preventing conformational changes. Mediators Inflamm. (2015) 2015:372432. doi: 10.1155/2015/372432
30. Pathak A, Agrawal A. Evolution of C-reactive protein. Front Immunol. (2019) 10:943. doi: 10.3389/fimmu.2019.00943
31. Lu J, Mold C, Du Clos TW, Sun PD. Pentraxins and Fc receptor-mediated immune responses. Front Immunol. (2018) 9:2607. doi: 10.3389/fimmu.2018.02607
32. Jimenez RV, Szalai AJ. Therapeutic lowering of C-reactive protein. Front Immunol. (2020) 11:619564. doi: 10.3389/fimmu.2020.619564
33. Wetterö J, von Löhneysen S, Cobar F, Kristenson M, Garvin P, Sjöwall C. Pronounced diurnal pattern of salivary C-reactive protein (CRP) with modest associations to circulating CRP levels. Front Immunol. (2020) 11:607166. doi: 10.3389/fimmu.2020.607166
34. Duarsa GWK, Tirtayasa PMW, Daryanto B, Nurhadi P, Renaldo J, Tarmono, et al. Risk factors for urethrocutaneous fistula following hypospadias repair surgery in Indonesia. J Pediatr Urol. (2020) 16:317.e1–317.e6. doi: 10.1016/j.jpurol.2020.04.011
35. Hardwicke JT, Bechar JA, Hodson J, Osmani O, Park AJ. Fistula after single-stage primary hypospadias repair - a systematic review of the literature. J Plast Reconstr Aesthet Surg. (2015) 68:1647–55. doi: 10.1016/j.bjps.2015.07.024
36. Nuhoglu B, Ayyildiz A, Balci U, Ersoy E, Gürdal M, Germiyanoglu C, et al. Surgical treatment options in proximal hypospadias: retrospective analysis of 171 cases at a single institution. Int Urol Nephrol. (2006) 38:593–8. doi: 10.1007/s11255-006-0097-z
Keywords: hypospadias, C-reactive protein, complications, fistula, risk factor
Citation: Ji F, Tang H, Wu C, Chen L, Wang H and Yan B (2021) Predictive Value of C-Reactive Protein for Early Postoperative Complications in Children After Hypospadias Surgery. Front. Pediatr. 9:690863. doi: 10.3389/fped.2021.690863
Received: 04 April 2021; Accepted: 27 July 2021;
Published: 13 September 2021.
Edited by:
Marco Castagnetti, University Hospital of Padua, ItalyReviewed by:
Alexander Springer, Medical University of Vienna, AustriaCopyright © 2021 Ji, Tang, Wu, Chen, Wang and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bing Yan, eWFuYmluZzI5QDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.