
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 09 June 2021
Sec. Neonatology
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.682097
 Bárbara Moreno-Sanz1,2*
Bárbara Moreno-Sanz1,2* María Teresa Montes1,2
María Teresa Montes1,2 Marta Antón1María Teresa Serrada1Marta Cabrera1
Marta Antón1María Teresa Serrada1Marta Cabrera1 Adelina Pellicer1,2
Adelina Pellicer1,2Background: Family Integrated Care (FICare) integrates parents in the direct care of their child while the healthcare personnel act as teachers and guides. To this date, most reports on the feasibility of this model refer to stable preterm infants admitted to Neonatal Intensive Care Units (NICUs).
Objectives: To scale up and adapt FICare to make it suitable in level IIIC NICUs, which care for extreme prematurity and other complex medical or surgical neonatal conditions.
Materials and Methods: Step 1 was the creation of the FICare implementation team (FICare-IT) and baseline analysis of current procedures for critical care to identify needs, wishes, and requirements; we aimed for protocol elaboration tailored to our cultural, architectural, and clinical context (March 2017 to April 2018). Step 2 as a dissemination strategy by FICare-IT acting as primary trainers and mentors to ensure the education of 90% of nursing staff (May 2018 to July 2018). Step 3 involved piloting and evaluation with the aim to refine the procedure (July 2018 to December 2020).
Results: A rigorous but flexible protocol was edited. The FICare educational manual included two curricula: for healthcare professionals/staff (Training the trainers) and for families (Education of caregivers), the latter being categorized in two intervention levels (basic and advanced), depending on the infant care needs and parent's decision. In total, 76 families and 91 infants (74.7% preterm; 18.7% complex surgery; 6.6% others) were enrolled in the pilot. No differences in acceptance rate (overall 86.4%) or in the number of infant-family dyads in the program per month were observed when considering the pre- and post-Covid-19 pandemic periods. All families, except for one who dropped out of the program, completed the agreed individualized training. Mothers spent more time in NICU than fathers (p < 0.05); uninterrupted time spent by mothers in NICU was longer during the pre-pandemic period (p < 0.01). Observed time to reach proficiency by task was within the expected time in 70% of the program contents. The parents revealed educational manuals, workshops, and cot-side teaching sessions as essential for their training, and 100% said they would accept entry into the FICare program again.
Conclusions: The principles of the FICare model are suitable for all levels of care in NICUs. Leadership and continuous evaluation/refinement of implementation procedures are essential components to achieve the objectives.
Extremely low gestational age neonates are at risk of developing short and long-term complications that can alter their life course (1–5). This patient group, in addition to other preterm and non-preterm infants who suffer severe neonatal acquired diseases, congenital malformations subsidiary of complex surgery, or rare diseases, sees prolonged hospital stay and faces similar burdens and challenges (6). Together, they can be referred to as high-risk neonates. In this context, parental stress, anxiety, and depression are frequently reported, and these may negatively impact normal bonding and the psychosocial evolution of the individual (1, 7–9). In fact, the power of intense parental stress during the first years of a child's development can be just as important as the biological condition at birth (10, 11). In addition to higher rates of family dysfunctions and economic problems reported, the parents' overprotective reactions toward the vulnerable child, partly motivated by the lack of security in their own abilities and that of the child, hinder the establishment of social relationships and the incorporation of the child into the labor market in adulthood (12, 13). To avoid abiding by these mechanisms, adequate parental training and information are critical (2, 3, 14–18). Therefore, new healthcare models for high-risk newborns are necessary, and these should take into account the global nature of the child, including the care of the family.
Family Integrated Care (FICare) is trademarked by Mount Sinai Hospital in Toronto, and it includes a four-pillar model of care proposed to foster feelings of self-confidence and competence regarding interaction with the child and the ability to be involved in their upbringing (3, 4, 19–23). The FICare model integrates parents into the direct care of their child by having them work together with responsible healthcare personnel who continue to provide medical treatment. To reach proficiency, parents undergo specific training by professionals who act as teachers and guides. Short-term clinical benefits have been reported (23–27) in addition to decreased levels of stress and anxiety in their families (23, 24). The empowerment of parents allows them to feel more secure in caring which in turn will reduce hospital stay and use of emergency services after discharge. Therefore, not only benefits in health are expected but also socioeconomic benefits (28–31). Up to date, reports on FICare model implementation are almost limited to stable preterm infants admitted to NICUs (23–31). However, turning parents into true experts in child care and development, as well as a source of love, protection, and support, is a path that should not be followed without careful planning.
Given the benefits already described, our purpose was to scale up the FICare model by offering two implementation levels (basic and advanced), making it suitable across the whole spectrum of care of the high-risk neonate.
The present report describes the FICare model implementation strategy used in our clinical setting, a level IIIC NICU, and evaluates the methodology followed and the effort used for its development. As one of the most determining elements of the success of the program is the uninterrupted time spent by parents in the NICU, a special focus was placed on analyzing the impact that the Covid-19 pandemic had on the workplan. In addition, at the time the project started, there were not single-family room facilities in our NICU, so that infants remained in open-ward rooms gathering a variable (from 5 to 8) number of patients.
The Department of Neonatology at La Paz University Hospital holds the largest NICU in the Madrid region, and it is one of the largest in Spain. The maternal and child hospital covers a population of approximately 600,000 inhabitants, attends 6,000 deliveries per year, and is a national referral center for fetal surgery, cardiovascular surgery, extracorporeal membrane oxygenation (ECMO), or treatment of retinopathy of prematurity, among other complex processes. Of a total of 67 beds, the NICU has 24 beds for infants on mechanical ventilation plus 15 additional beds for highly dependent non-ventilated infants. More than 200 nurses and nursing assistants (33 per shift) work in the department. There is also active teaching activity among the staff that includes nurse residents (18/year) and students (16/year). The average annual activity at the Department of Neonatology is above 1,500 admissions, and 3,600 visits at the outpatient clinic. The NICU attends all kinds of medical and surgical diseases, has its own Human Milk Bank facilities, and a Royal McDonald House Charities-Family Room.
Our NICU policies allow parents to remain at their infant's cot-side 24 h around the clock. However, the visitors' policies changed during the lockdown period imposed by the COVID-19 pandemic. Accordingly, from mid-March to the end of June 2020 (first wave lockdown), only one visitor per child was allowed to stay for a maximum of 2 consecutive hours at the hospital; from July 2020 to the present, no time restriction was imposed but the number of visitors per infant remained unchanged. Most of the attended population at our NICU is Caucasian or American-Hispanic, with a low proportion of other cultures/ethnicities (mainly Muslims from Morocco).
The project leader (AP) conceptualized the idea and elaborated a step-wise workplan (Figure 1).
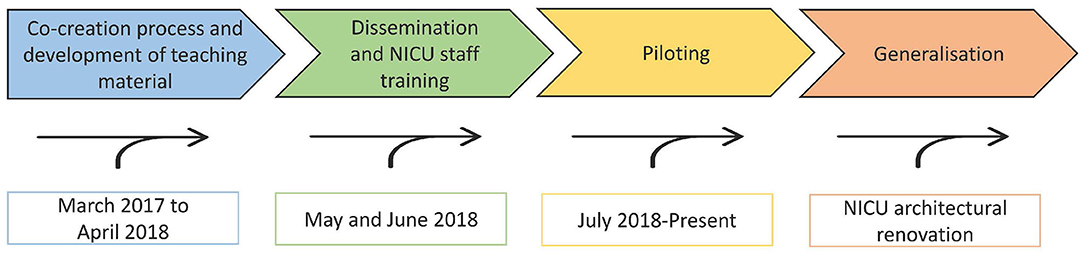
Figure 1. FICare program development and implementation workplan.
The first step was to create the FICare implementation team (FICare-IT). The FICare-IT gathered members of the local associations of veteran parents and included a variety of professional (social workers, psychologists, speech therapists, and sociologists) and non-professional partners in addition to NICU staff (10% of the nursing staff and four neonatologists). A FICare clinical staff co-ordinator was nominated (MTM). The FICare program development and implementation calendar was agreed upon by the FICare-IT in March 2017 (Figure 1).
FICare-IT conducted an analysis of current procedures for critical care to identify needs, wishes, and requirements. As a result of the analysis, the following components of the FICare program to be implemented were defined: the educational component for staff (nurses and doctors) and family primary caregivers to support their roles; psychological support for parents, with a leading role for veteran parents pertaining to the FICare-IT, or individual interventions by hospital psychologist if requested; and the physical support, which included comfortable cot-side chairs and breast-pumps as well as the facilities provided by the Ronald McDonald Family Room (chill-out area, living-room with TV, kitchen, and complete bathroom with shower and personal locker among others). The procedures and main topics to be covered in the FICare training program, ensuring the diverse needs and challenges were properly covered; the specifications of the tools and materials required for training and for pilot's data gathering; and the questionnaires for experience and psychological data gathering were also decided. Expected deliverables were the FICare implementation protocol (procedures and materials for the overall implementation strategy) and the FICare teaching material.
The second step was the dissemination of the FICare program and training on FICare standards among the NICU clinical staff. The FICare-IT at this stage acted as primary trainers and mentors to ensure that the provision of nurse education covered 90% of active nursing staff in the NICU, as recommended (32). Groups of 10–15 nurses and nurse assistants were created and assigned to a member of the FICare-IT for FICare staff training (Figure 2).
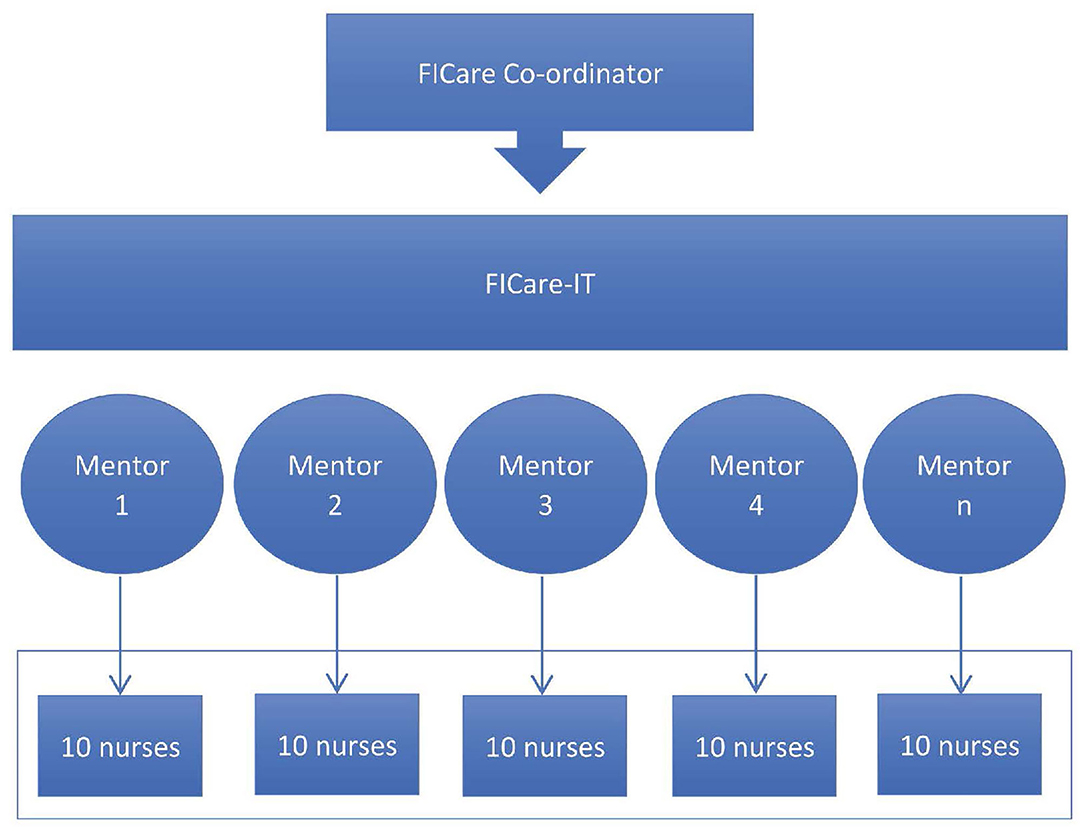
Figure 2. Dissemination strategy at the clinical site following a primary training and mentoring system throughout the whole implementation process.
The third step was piloting and evaluation of the FICare program before opening to all potential beneficiaries (a generalization of FICare policies within the NICU); the latter was scheduled for when the new NICU with single-family room facilities opens. Serial FICare-IT meetings were held to evaluate, refine and enrich the preliminary protocol. Barriers and other unforeseen difficulties that were found after a running-in period were taken into account for these purposes.
The data were analyzed with the statistical program SAS 9.3 (SAS Institute, Cary, NC, USA). Qualitative data are expressed as counts and percentages and quantitative data as mean (SD) or medians (IQR). The pre- and post-Covid-19 pandemic periods during the pilot were defined as July 2018 to March 2020 (21 months) and May 2020 to December 2020 (8 months), respectively. Enrolment during April 2020 was stopped due to lockdown constraints. Non-parametric tests (Mann-Whitney test and Kolmogorov-Smirnov) were used for comparisons. The values were considered statistically significant with p < 0.05.
A rigorous but flexible protocol tailored to the cultural, architectural, and clinical context of our NICU, with two implementation levels (basic and advanced), was edited and approved by the Research Ethics Committee of La Paz University Hospital. The scope of the program covered preterm and term neonates (and their families), admitted to NICU due to complex congenital or acquired diseases or immaturity-related issues, for which a long length of stay was anticipated (i.e., at least three consecutive weeks), providing all inclusion criteria were fulfilled and none of the exclusion criteria applied (Table 1).
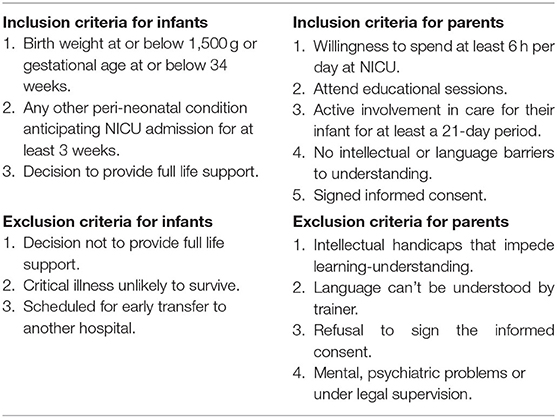
Table 1. Eligibility and exclusion criteria for FICare program.
A strategy for recruitment was established to avoid overloading parents with information during the critical period after birth when they are most vulnerable. Whenever possible, preliminary information about the FICare program was distributed to parents of potential candidates antenatally. Perinatal committees, where complicated pregnancies are discussed among obstetricians and neonatologists, were the ideal forum to comment on potential candidates. An appointment with eligible families was scheduled according to the information gathered in these meetings. In the case antenatal information was not provided, families were approached after NICU admission. Once the families accepted to participate in the FICare program and signed the informed consent, the training tools were provided. A maximum of four infant-family dyads on FICare at a given time was proposed for the pilot. This policy was changed after a 6-month running period of the program when a maximum number accepted was scaled up to 10 infant-family dyads.
The FICare training program was divided into two curricula: for healthcare professionals/staff (Training the trainers) and for families (Education of caregivers), the latter being categorized in two intervention levels (basic and advanced) depending on the infant care needs and parent's decision (Table 2). The following modules were identified as the minimum training contents to be delivered to foster FICare:
• Training the trainers: (1) understanding the boundaries of the FICare model and how to promote FICare among families; (2) psychosocial needs of families (resilience, stress and anxiety, or mourning) and communication skills (assertive communication); (3) how to involve families in NICU (safe conduct in NICU environment, attachment and bonding, how to perform family-centered medical rounds); and (4) professional self-care (burnout and compassion fatigue).
• Education of caregivers: (1) comprehensive description of the FICare model (the strengths and training methodology) and the functional and architectural structure of the NICU; (2) family self-care (stress and anxiety, resilience, or mourning); (3) learning about infants' neurobehavior, stress, and pain; (4) taking part in baby care (basic level), where parents will be “professionalized” to become the first-line care providers of their children; (5) taking part in baby care (advanced level), specific task's training for infants who require even more specialist care; and (6) parents will be prepared for home, and a map of the social resources available at the local setting will be provided.
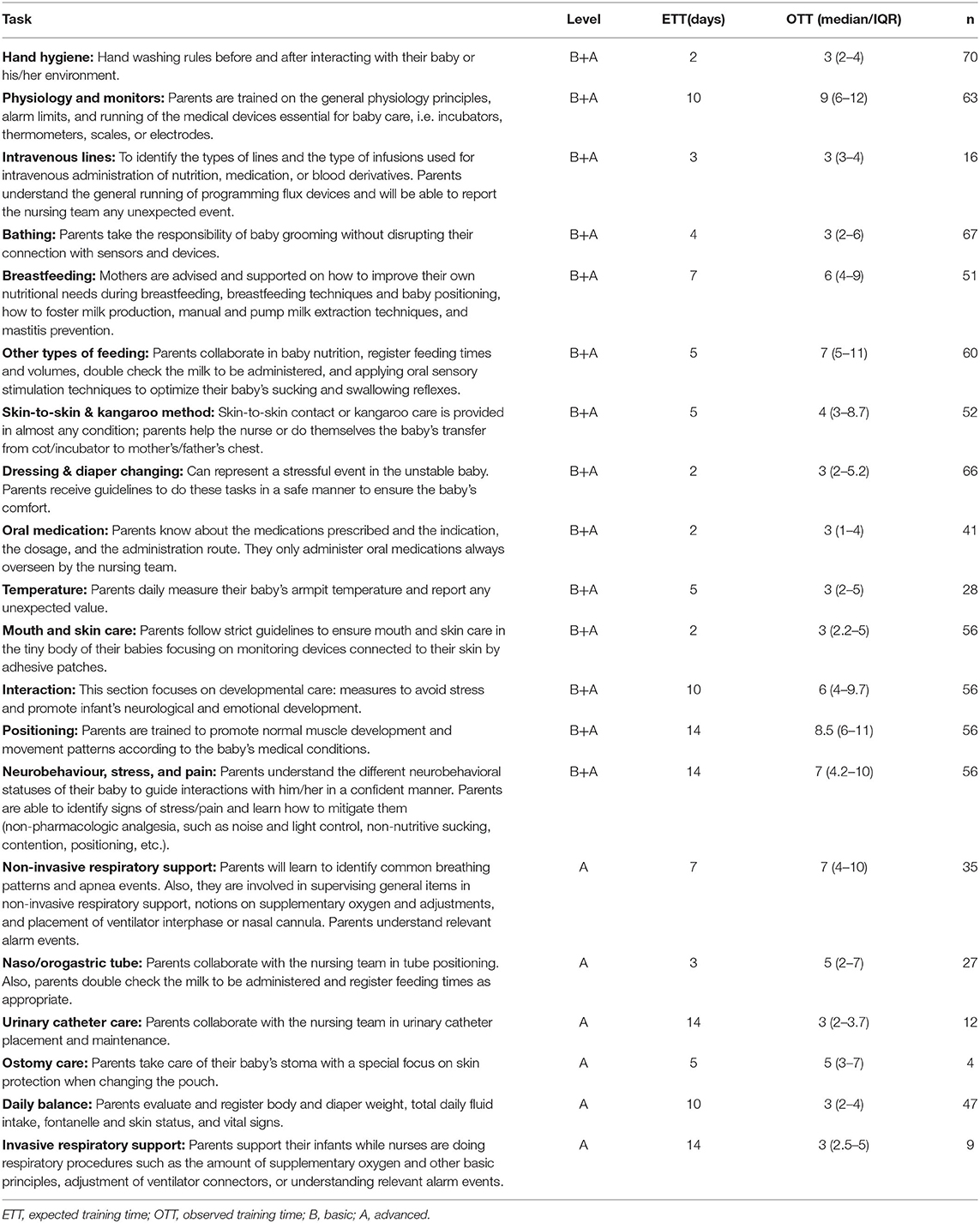
Table 2. “Taking part in baby care”: description of contents by FICare implementation level (basic and advanced), the expected and observed training time, and the number of families certified by task.
The FICare training tools included an educational manual (14) on all the contents described above provided in both printed and PDF format to caregivers and a notebook to be used by parents for systematic daily data recordings (anthropometry, vital signs, oxygen supply, or nutrition parameters), as well as a space for free text. The training material was ready by April 2018.
A teacher education system started in May 2018. The Chief Nurse and FICare co-ordinator defined the mentor-assigned trainee groups and the calendar. Face-to-face meetings took place for 2 months. By June 2018, the program and procedures were disseminated among 90% of the NICU staff (doctors, nurses, and nurse assistants) to become facilitators of FICare. In these meetings, mentors particularly focused on the relevance of training harmonization and the requested adherence to the contents and procedures as described in the educational manual (14). Mentors were available by phone or email to attend to any doubt/request from their respective trainees.
The family training process relayed on three cornerstones that were agreed upon between mentors and the staff facilitators:
• Individualized theoretical and practical learning by tasks: two family caregivers per family were trained through cot-side face-to-face sessions, following an individualized teaching plan adjusted to the baby's clinical condition and the wish of the parents. Once proficiency was fully accredited in a given task, the family caregiver was certified by the training nurse (and registered) and was allowed to do this task autonomously.
• Workshops: family caregivers were invited to attend 45-min open sessions on relevant topics of the learning contents, to express their doubts and concerns, as well as to share their experiences with other families. Three meetings per week were programmed; selected topics were sequentially repeated every 4 weeks.
• Registry of teaching activities and task certifications in the corresponding logbook.
In February 2020 a FICare workshop for all the NICU staff (doctors and nurses/nurse assistants) was organized to refresh the knowledge and share the experiences lived during the previous months of piloting.
From July 2018 to December 2020, 88 families who fulfilled the FICare program entry criteria were approached (57 families pre-COVID-19 pandemic; 31 families post-COVID-19 pandemic); we saw an 86.4% acceptance rate (91.2% pre-COVID-19 pandemic; 77.4% post-COVID-19 pandemic), resulting in a total of 76 parents and 91 infants being enrolled in the pilot. The main neonatal diagnoses of the participating infants were as follows: prematurity (n = 68, 74.7%), congenital heart defects (n = 13, 14.3%), a variety of genetic syndromes (n = 5, 5.5%), congenital diaphragmatic hernia assisted by extracorporeal membrane oxygenation (ECMO) (n = 2, 2.2%), kidney dysplasia (n = 1, 1.1%), esophageal atresia (n = 1, 1.1%), and ileal atresia (n = 1, 1.1%). Relevant clinical data of the infants included are displayed in Table 3.
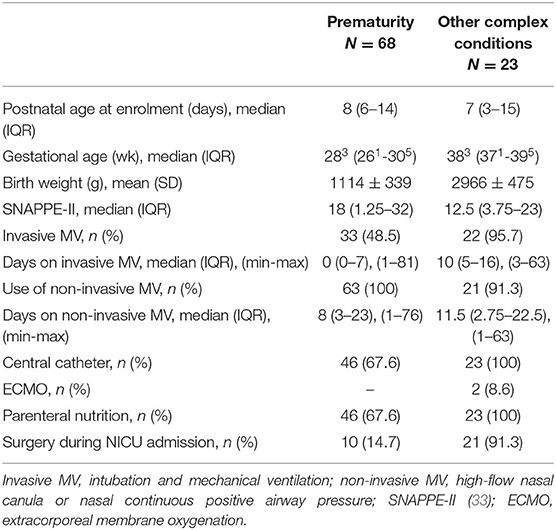
Table 3. Clinical features of the infants enrolled in the FICare pilot according to main neonatal diagnosis.
The median number of infant-family dyads included in the program per month was 3 (1–5) and 4 (2.25–5.75) for the pre- and post-COVID-19 pandemic periods, respectively (p = 0.237). Systematic surveillance of uninterrupted daily time spent by parents in the NICU started in January 2020. The observed pre-pandemic period revealed that the median time for mothers was 10 (7–10.5) h, while the median time for fathers was 7 (5.5–10) h. During the post-pandemic period, the median uninterrupted time in the NICU was 7 (4.5–8) h and 5 (4–8) h for mothers and fathers, respectively. Mothers spent more time in the NICU than fathers irrespective of the period that was observed (p < 0.05). Uninterrupted time spent in the NICU differed between periods, being significantly longer for mothers during the pre-pandemic period (p < 0.01).
All families enrolled in the pilot completed the individualized training plan that was agreed on enrolment except one, who voluntarily expressed the desire to abandon FICare. Time spent for parents to reach full proficiency to get certification by task is described in Table 2. Family caregivers regularly participated in daily clinical rounds held by the attending physician and the shift nurse, and their comments and suggestions were considered when making decisions.
The median number of parents attending workshops was two (one to three). The main argument given by parents to decline workshop participation was the coincidence with the infants' feeding time.
The results on the satisfaction questionnaire about the FICare program for families are depicted in Table 4. In general, learning material, workshops, and cot-side teaching sessions were judged as essential for their training. Among the experiences described by parents, it is worth mentioning the gain in safety and self-confidence in caring for their children both in the hospital and after discharge:
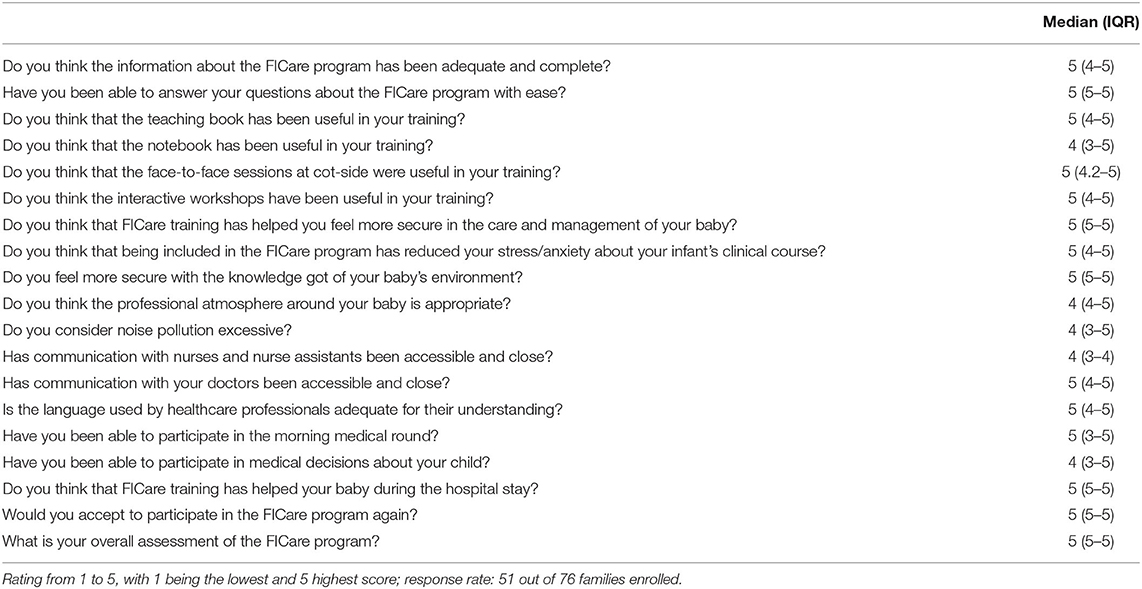
Table 4. The FICare program satisfaction questionnaire for families.
“Our perception is that the program helped us to foster discharge; in complex cases, such as the care of our daughter, this training enable parents to feel ready to care (for) the baby and manage all the devices the baby needs, such as oxygen, home monitoring, or feeding by tube. We have also learned how to deal (with) and respond to “scares”; we are now prepared to keep calm and react appropriately when needed. Hav(ing) learned when it is time to ask for help is a great achievement.”
Another important issue that parents refer to is decreased stress and anxiety as they are really aware pf their baby and his/her context:
“Knowledge is power. Knowing what our babies are like and how to address their needs was essential to reduce the stress and anxiety we had due to the entrance of our twins; it has even allowed us to enjoy this stage that we have had to go (sic).”
As a final point of the parents' evaluation, they were asked whether they would accept to enter the FICare program again, to which all the families were aligned:
“My answer is yes, a thousand times yes. This program was determinant to learn how to deliver the care that my baby needs (sic). The program allowed us to behave as real parents and not mere observers of our baby's life.”
During the pilot, weekly FICare rounds were held by at least three members of the FICare-IT. During these rounds, direct contact with families currently involved in the training was established. Parents were invited to report any queries, doubts, or complaints about the program. Teaching notebooks and certification registries were collated, and adjustments to the individual teaching plan were carried out. The feedback on the individual progress reported by either parents or professionals involved in the training was used to adjust and refine the workplan to overcome project barriers and strengthen dissemination (Table 5).
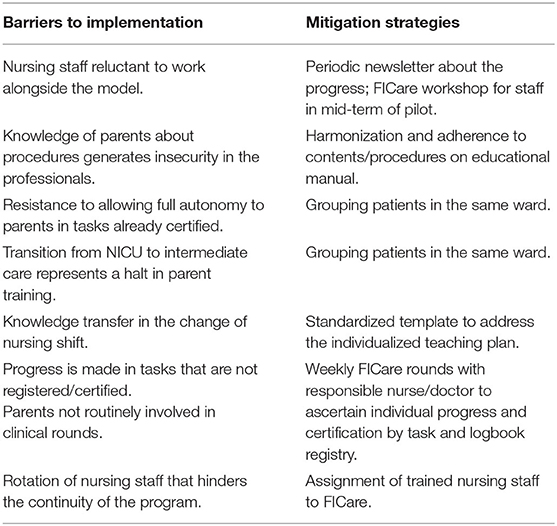
Table 5. Measures to overcome difficulties to foster FICare during the pilot.
This is the first study reporting on the feasibility of FICare model implementation in a complex, level IIIC NICU, that gathers surgical and non-surgical processes involving both, the preterm and term infant. The scaling up of the FICare model explored in this work included two levels of care: training parents in the basic tasks, as reported previously (23–31), and the advanced level, which introduces additional tasks that pertain to more specialized care, such as respiratory support-related topics, tube feeding, urinary catheter or ostomy care, and daily balance. Therefore, the main strength of this work is to make the principles of the FICare model suitable across the whole spectrum of care of the high-risk neonate. The scope of the impact is very relevant, given that the variety of professionals involved in the care of these patients far exceeds the exclusively neonatal workforce.
Another important achievement of this workplan was developing and implementing the FICare model in an a priori unfavorable architectural configuration of the NICU, as we had no single-family room for NICU admission at the time the project started. Although not a pre-requisite, single-family rooms positively influence the expected FICare health outcomes (25). This kind of facility favors longer uninterrupted time spent by parents at the hospital and promotes interaction with nurses as the private habitat ensures that there are no “observers” in the environment. In spite of these constraints, and although the NICU architectural remodeling was already scheduled, we decided to start piloting the model with the aim of generalizing FICare policies as future routine NICU standard when the new hospitalization area, which will have such facilities, is inaugurated. No doubt that the current availability of a common area for parents, fitted with a kitchen, complete bathroom, chill-out room, and seating area with TV and internet access, has been a key element in supporting the program.
The experience gained during the 30 months of running the project allowed the FICare-IT to make sequential adjustments in procedures to overcome difficulties and barriers that were found. For instance, in the beginning, a maximum of four infant-family dyads on FICare at a given time was proposed: a decision based on avoiding nurse work overload and guaranteeing that the family training and accreditation by task was correct. We also thought that it was easier to group FICare patients in the same ward if the number of families being trained at a time was smaller. As time went by, we realized that this approach was wrong because, even if intended, the reality was that, for different reasons, patients were not “grouped.” In addition, it was realized that many of the teaching activities had more learning inertia if there were more people in the program at any given time. Consequently, the FICare-IT decided to increase the maximum number of infant-family dyads for training by 3-fold.
The COVID-19 lockdown period imposed new visitors' policies at our hospital, limiting the number and the time allowed for visits. In spite of that, enrolment in the pilot was halted only during the peak of the pandemic in our region (April 2020), while training of parents who already were participating in the program continued as scheduled. In fact, no differences in the enrolment rates were observed when the pre- (91.2%) and post-pandemic (77.4%) periods were compared, with a similar number of infant-family dyads in the program per month. Although mothers spent more time in NICU than fathers, irrespective of the period that was observed, our understanding is that the revised visitors' policies during the post-pandemic period justify the larger uninterrupted time spent in NICU by the mothers observed during the pre-pandemic period.
FICare represents a change in people that involve professionals and families as main actors influencing their attitudes, skills, expectations, perceptions, and behaviors. The participation of all health personnel is critical for a successful implementation of a project that promotes a change in the working method and in the established roles. To do so, thorough project planning is essential and should include the development of theoretical and practical support, as well as a good dissemination strategy within the NICU staff. With regards to the first cornerstone, no remarks were raised among the staff regarding the teaching material contents, as expected, because in the educational manual (14) all chapters directly related to how to provide infant care were written by NICU personnel, based on our current protocols, and, as far as possible, adapted to the general population for their better understanding. The feedback obtained from the parents' questionnaires, relative to the educational manual and the notebook, was aligned with that as both got very high scores. In relation to dissemination strategies, continuous action is needed, however. We felt quite “silent resistance” in the different levels of staff, which regrettably has not been systematically evaluated by means of specific questionnaires for professionals. These negative feelings had to be counteracted with a variety of adjustments in the procedures along time, as summarized in Table 5. Increasing the number of participants in the program at a given time, or grouping FICare patients in the same ward for an easier nurse shift programming to optimize the teaching and certification processes, were among the most productive actions taken.
Planning the time needed for task certification is critical, as it is an indicator of the nurse effort required and the moment when parents are allowed to do this task autonomously. We had no a priori experience for this, and our predictions were thus based on the theoretical complexity of the task or how frequently it was to be practiced (Table 2). In 70% of the scheduled tasks, certification was accomplished within the expected time or earlier. In total, 6 out of the 20 blocks of tasks, however, took more time than expected for full accreditation. Most of them relate to common procedures, such as hand hygiene, skin care, or dressing and diaper changes. We suspect that, even though these are “common” routines in NICUs, the fact that our patients were complex and very often clinically unstable showed that more time is needed for parents to overcome fears. It is very interesting, however, that really advanced care, such as naso/orogastric tube care or invasive respiratory-support-related care, took a much shorter time for certification than expected. We think that the explanation for these findings lies in the fact that these tasks always require the participation of the nursing staff, which makes both the professional and the parents feel safer and removes fears.
The way to deliver training to the parents by the nurse staff was acknowledged in general. However, attendance at workshops was much lower than expected. We think this is a weakness of our working plan, as we envisage these open interactive sessions as an opportunity to create good dynamics: a way to heal scars and strengthen knowledge. The justification given by parents was, in general, unsuitable timetables because the sessions were held in a separate room and not at their baby's cot-side. Moving to the admission wards for this purpose prevents gathering a sound number of parents at a given time, and although interaction may be improved (like intimate relations between neighbors), the reaching is lower. The parental feelings about our FICare program, in general, were very positive, and all parents would accept to participate again. Individual comments/remarks were intended to be addressed during the weekly FICare rounds routinely held by members of the FICare-IT. However, it is possible that the items included in the parents' satisfaction questionnaire were leading the participants' responses to some extent.
In summary, this report describes the procedures followed to develop and implement the FICare model at a complex, level IIIC NICU that cares for all kinds of medical and surgical neonatal processes. The adapted protocol scales up the FICare model, introducing two implementation levels: basic (routine tasks addressed in previous FICare experiences) and advanced (specific tasks aimed to prepare parents for infants who require even more specialist care). Our results support that FICare implementation is feasible in this context, even when facing two important adverse conditions: absence of single-family room facilities for hospitalization during the prolonged NICU stay and strict visitors' restrictive policies during the Covid-19 pandemic. Even in the case of thorough planning, continuous follow-up of the protocol procedures and eventual adjustments and adaptations according to the current conditions to solve difficulties raised by both professionals and families are key elements for project success. A limitation of this study is the lack of a systematic assessment of the professional perception of the model. Future studies should address the impact of this adapted scaled-up FICare model on the infants' outcome, the parental stress profiles, the professionals' viewpoint, and the health system economy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee for Human Studies at La Paz University Hospital. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
BM-S participated in the development of training material and FICare dissemination-implementation strategy among NICU staff, conceptualized and designed the pilot, and participated in recruitment and data analysis, drafted the initial manuscript, and approved the final manuscript as submitted. MM and MA participated in the development of training material and FICare dissemination-implementation strategy among NICU staff, participated in recruitment and training during the pilot, reviewed the manuscript, and approved the final manuscript as submitted. MS and MC participated in the development of training material and FICare dissemination-implementation strategy among NICU staff, reviewed the manuscript, and approved the final manuscript as submitted. AP conceptualized and designed the workplan and participated in the development of training material and FICare dissemination-implementation strategy among NICU staff, conceptualized and designed the pilot, drafted the initial manuscript, and approved the final manuscript as submitted. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank the FICare-IT for the efforts and time dedicated to developing and implementing the FICare model at our NICU. In particular, special mention to the Association of Parents of Preterm Infants of Madrid (APREM), Down Madrid, the Spanish Federation of Rare Diseases (FEDER), and the Association of Congenital Heart Defects of Madrid (Menudos Corazones) for their commitment and continuous support; and to the Spanish Division of the Ronald McDonald House Charities for building and running a real home within the hospital.
1. Pennestri M, Gaudreau H, Bouvette-turcot A, Moss E, Lecompte V, Atkinson L, et al. Attachment disorganization among children in neonatal intensive care unit : preliminary results. Early Hum Dev. (2020) 91:601–6. doi: 10.1016/j.earlhumdev.2015.07.005
2. Melnyk BM, Feinstein NF. Reducing hospital expenditures with the COPE (creating opportunities for parent empowerment) program for parents and premature infants. Nurs Adm Q. (2009) 33:32–7. doi: 10.1097/01.NAQ.0000343346.47795.13
3. Benzies KM, Magill-Evans JE, Hayden KA, Ballantyne M. Key components of early intervention programs for preterm infants and their parents: a systematic review and meta-analysis. BMC Pregnancy Childbirth. (2013) 13(Suppl. 1):S10. doi: 10.1186/1471-2393-13-S1-S10
4. Melnyk BM, Feinstein NF, Alpert-Gillis L, Fairbanks E, Crean HF, Sinkin RA, et al. Reducing premature infants' length of stay and improving parents' mental health outcomes with the creating opportunities for parent empowerment (COPE) neonatal intensive care unit program: a randomized, controlled trial. Pediatrics. (2006) 118:e1414–27. doi: 10.1542/peds.2005-2580
5. Luu TM, Rehman Mian MO, Nuyt AM. Long-term impact of preterm birth: neurodevelopmental and physical health outcomes. Clin Perinatol. (2017) 44:305–14. doi: 10.1016/j.clp.2017.01.003
6. Levey A. The impact of prenatal diagnosis of complex congenital heart disease on neonatal outcomes. (2011) 31:587–97. doi: 10.1007/s00246-010-9648-2
7. Kim AR, Tak YR, Shin YS, Yun EH, Park HK. Mothers' perceptions of quality of family-centered care and environmental stressors in neonatal intensive care units: predictors of and relationships with psycho-emotional outcomes and postpartum attachment. Matern Child Health J. (2020) 24:601–11. doi: 10.1007/s10995-020-02876-9
8. Al F, Abdullah KL, Chan CM, Piaw CY. Systematic review of qualitative studies exploring parental experiences in the neonatal intensive care unit. (2016) 25:2745–56. doi: 10.1111/jocn.13259
9. Obeidat HM, Bond EA. The parental experience of having an infant in the newborn intensive care unit. Vol. 18 (2009). p. 23–9. doi: 10.1624/105812409X461199
10. Serrano González F. Nacer de nuevo: la crianza de los niños prematuros: la relación temprana y el apego. Cuad Psiquiatr Psicoter Niño Adolesc Soc. (2009) 48:61–80.
11. Fava Vizziello G, Rebecca L, Calvo V. Representaciones maternas, apego y desarrollo en los niños prematuros. Cuad Psiquiatr Psicoter Niño Adolesc. (1997) 23–24:23–50.
12. Saigal S, Pinelli J, Streiner DL, Boyle M, Stoskopf B. Impact of extreme prematurity on family functioning and maternal health 20 years later. Pediatrics. (2010) 126:e81–8. doi: 10.1542/peds.2009-2527
13. Gómez Esteban C, Martín Carballo M. y Vicente Olmo A. Dificultades biosociales de la gran prematuridad. In: Crisis Y Cambio: Propuestas Desde la Sociología (Vol III). XI Congreso Español de Sociología, Vol. 1 (2014). p. 1229–38.
14. Grupo de Trabajo en FICare. Un Mundo Creado para Mí. Madrid: La Familia Integrada en los Cuidados. Monografía FICare, Servicio de Neonatología Hospital Universitario La Paz (2018).
15. Hynan MT, Mounts KO, Vanderbilt DL. Screening parents of high-risk infants for emotional distress: rationale and recommendations. J Perinatol. (2013) 33:748–53. doi: 10.1038/jp.2013.72
16. Hynan MT, Hall SL. Psychosocial program standards for NICU parents. J Perinatol. (2015) 35(Supple. 1):S1–4. doi: 10.1038/jp.2015.141
17. Escartí A, Boronat N, Llopis R, Torres R, Vento M. Estudio piloto sobre el estrés y la resiliencia familiar en recién nacidos prematuros. An Pediatr. (2016) 84:3–9. doi: 10.1016/j.anpedi.2015.03.001
18. Carter JD, Mulder RT, Bartram AF, Darlow BA. Infants in a neonatal intensive care unit: parental response. Arch Dis Child Fetal Neonatal Ed. (2005) 90:109–14. doi: 10.1136/adc.2003.031641
19. Purdy IB, Craig JW, Zeanah P. NICU discharge planning and beyond: recommendations for parent psychosocial support. J Perinatol. (2015) 35(Supple. 1):S24–8. doi: 10.1038/jp.2015.146
20. Craig JW, Glick C, Phillips R, Hall SL, Smith J, Browne J. Recommendations for involving the family in developmental care of the NICU baby. J Perinatol. (2015) 35(Supple. 1):S5–8. doi: 10.1038/jp.2015.142
21. Dunn MS, Reilly MC, Johnston AM, Hoopes RD, Abraham MR. Development and dissemination of potentially better practices for the provision of family-centered care in neonatology: the family-centered care map. Pediatrics. (2006) 118(Suppl. 2):S95–107. doi: 10.1542/peds.2006-0913F
22. Gooding JS, Cooper LG, Blaine AI, Franck LS, Howse JL, Berns SD. Family support and family-centered care in the neonatal intensive care unit: origins, advances, impact. Semin Perinatol. (2011) 35:20–8. doi: 10.1053/j.semperi.2010.10.004
23. O'Brien K, Bracht M, Macdonell K, McBride T, Robson K, O'Leary L, et al. A pilot cohort analytic study of family integrated care in a canadian neonatal intensive care unit. BMC Pregnancy Childbirth. (2013) 13 (Suppl. 1):S12. doi: 10.1186/1471-2393-13-S1-S12
24. O'Brien K, Robson K, Bracht M, Cruz M, Lui K, Alvaro R, et al. Effectiveness of family integrated care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc Heal. (2018) 2:245–54. doi: 10.1016/S2352-4642(18)30039-7
25. van Veenendaal NR, van der Schoor SRD, Heideman WH, Rijnhart JJM, Heymans MW, Twisk JWR, et al. Family integrated care in single family rooms for preterm infants and late-onset sepsis: a retrospective study and mediation analysis. Pediatr Res. (2020) 88:593–600. doi: 10.1038/s41390-020-0875-9
26. Örtenstrand A, Westrup B, Broström EB, Sarman I, Åkerström S, Brune T, et al. The Stockholm neonatal family centered care study: effects on length of stay and infant morbidity. Pediatrics. (2010) 125:e278–85. doi: 10.1542/peds.2009-1511
27. Banerjee J, Aloysius A, Mitchell K, Silva I, Rallis D, Godambe S V, et al. Improving infant outcomes through implementation of a family integrated care bundle including a parent supporting mobile application. Arch Dis Child Fetal Neonatal Ed. (2020) 105:F172–7. doi: 10.1136/archdischild-2018-316435
28. O'Brien K, Bracht M, Robson K, Ye XY, Mirea L, Cruz M, et al. Evaluation of the family integrated care model of neonatal intensive care: a cluster randomized controlled trial in Canada and Australia. BMC Pediatr. (2015) 15:1–9. doi: 10.1186/s12887-015-0527-0
29. Benzies KM, Shah V, Aziz K, Isaranuwatchai W, Palacio-Derflingher L, Scotland J, et al. Family integrated care (FICare) in level II neonatal intensive care units: study protocol for a cluster randomized controlled trial. Trials. (2017) 18:1–12. doi: 10.1186/s13063-017-2181-3
30. Hei M, Gao X, Gao X, Nong S, Zhang A, Zhang Q, et al. Is family integrated care in neonatal intensive care units feasible and good for preterm infants in China: Study protocol for a cluster randomized controlled trial. Trials. (2016) 17:1–8. doi: 10.1186/s13063-015-1152-9
31. Hei M, Gao X, Li Y, Gao X, Li Z, Xia S, et al. Family integrated care for preterm infants in China: a cluster randomized controlled trial. J Pediatr. (2021) 228:36–43.e2. doi: 10.1016/j.jpeds.2020.09.006
32. Milette I, Martel MJ, Ribeiro da Silva M, Coughlin McNeil M. Guidelines for the institutional implementation of developmental neuroprotective care in the neonatal intensive care unit. Part A: background and rationale. A joint position statement from the CANN, CAPWHN, NANN, and COINN. Can J Nurs Res. (2017) 49:46–62. doi: 10.1177/0844562117706882
Keywords: FICare, family integrated care, parent education, parent training, parent empowerment
Citation: Moreno-Sanz B, Montes MT, Antón M, Serrada MT, Cabrera M and Pellicer A (2021) Scaling Up the Family Integrated Care Model in a Level IIIC Neonatal Intensive Care Unit: A Systematic Approach to the Methods and Effort Taken for Implementation. Front. Pediatr. 9:682097. doi: 10.3389/fped.2021.682097
Received: 17 March 2021; Accepted: 26 April 2021;
Published: 09 June 2021.
Edited by:
Po-Yin Cheung, University of Alberta, CanadaReviewed by:
Karen M. Benzies, University of Calgary, CanadaCopyright © 2021 Moreno-Sanz, Montes, Antón, Serrada, Cabrera and Pellicer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bárbara Moreno-Sanz, Ym1vcmVub3NAc2FsdWQubWFkcmlkLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.