
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 05 May 2021
Sec. Pediatric Surgery
Volume 9 - 2021 | https://doi.org/10.3389/fped.2021.651951
This article is part of the Research TopicCleft Lip and Palate Anomalies/SyndromesView all 11 articles
 Mohammad Khursheed Alam1*†
Mohammad Khursheed Alam1*† Ahmed Ali Alfawzan2†
Ahmed Ali Alfawzan2† Sanjida Haque3
Sanjida Haque3 Pooi Ling Mok4,5
Pooi Ling Mok4,5 Anand Marya6
Anand Marya6 Adith Venugopal7
Adith Venugopal7 Nafij Bin Jamayet8
Nafij Bin Jamayet8 Ammar A. Siddiqui9
Ammar A. Siddiqui9To investigate whether the craniofacial sagittal jaw relationship in patients with non-syndromic cleft differed from non-cleft (NC) individuals by artificial intelligence (A.I.)-driven lateral cephalometric (Late. Ceph.) analysis. The study group comprised 123 subjects with different types of clefts including 29 = BCLP (bilateral cleft lip and palate), 41 = UCLP (unilateral cleft lip and palate), 9 = UCLA (unilateral cleft lip and alveolus), 13 = UCL (unilateral cleft lip) and NC = 31. The mean age was 14.77 years. SNA, SNB, ANB angle and Wits appraisal was measured in lateral cephalogram using a new innovative A.I driven Webceph software. Two-way ANOVA and multiple-comparison statistics tests were applied to see the differences between gender and among different types of clefts vs. NC individuals. A significant decrease (p < 0.005) in SNA, ANB, Wits appraisal was observed in different types of clefts vs. NC individuals. SNB (p > 0.005) showed insignificant variables in relation to type of clefts. No significant difference was also found in terms of gender in relation to any type of clefts and NC group. The present study advocates a decrease in sagittal development (SNA, ANB and Wits appraisal) in different types of cleft compared to NC individuals.
Cleft lip and palate; the second most common developmental abnormalities which extant during birth by presenting anatomical alteration of the lip and/or palate (1). This craniofacial malformation is caused by the effects of both genetic and environmental factors such as maternal smoking and alcohol consumption, stress, viral infection during the first 8 weeks of pregnancy, teratogenic drug etc. (2).
The treatment of cleft lip and palate (CLP) is multidisciplinary where the only purpose is to restore the functional and aesthetic value. Many beneficial approaches have been carried out previously such as: dental arch relationship (3), arch dimension (4), tooth size morphometry (5) and craniofacial morphology (6) to evaluate the outcome of CLP patients.
Atypical sagittal growth of maxilla is a common manifestation in patients with UCLP; acknowledged by many researchers yet all of them came to an understanding that the growth and direction of the jaw utterly influenced by the earlier treatment protocol such as time and techniques of primary surgeries (7–12). The detrimental effect of palatoplasty on sagittal growth of maxilla has been widely documented in literature (9) but whether cheiloplasty impedes the growth is still in controversy (8, 13). A number of researchers found that cheiloplasty has an effect on maxillary incisors, alveolar bone and development of maxilla as well whether some researchers claimed no effect on maxillary development (7, 11, 12, 14, 15).
The craniofacial characteristics of CLP can be assessed from cephalogram (16) and cone-beam computed tomography (17) as well. Abundant cephalometric studies have been done on CLP yet restricted to three-dimensionally. Artificial intelligence (A.I.) into dentistry, especially in cleft research is still a new-fangled and robust technique (18–21).
Use of A.I driven Webceph software for the measurements of all variables in cephalogram were the particularities from previous study which is more accurate, precise, robust and reliable compared to manual measurements (18–21).
For the first time, the present study tried to disclose the sagittal development of Saudi Arabian CLP patients, by A. I driven lateral cephalometric analysis and compared it with the non-cleft (NC) individuals and also compared in relation to gender and types of cleft.
This retrospective study was limited to 123 individuals including 29 bilateral cleft lip and palate (BCLP), 41 unilateral cleft lip and palate (UCLP), 13 unilateral cleft lip UCL, 9 unilateral cleft lip and alveolus (UCLA) and 31 NC individuals with the average age of 13.29 [3.52] (NC), 14.07 [4.73] (BCLP), 14.32 [4.46] (UCLP), 12.78 [4.09] (UCLA), and 13.31 [4.46] (UCL) years, respectively. All the data (medical records and X-rays) of this study were collected from Saudi Board of Dental Residents and approved by the Ethical Committee of Al Rass Dental Research Center, Qassim University (DRC/009FA/20). Non-syndromic cleft individuals with good-quality x-ray images were included whereas any history of craniofacial surgery, bone grafting and orthodontic treatment was excluded from the study. Same age group of healthy non cleft individuals were also included as the control group. Convenient sampling has been done without randomization.
Digital Lateral Cephalogram X-rays were used to measure four different cephalometric parameters (SNA, SNA, ANB and Wits appraisal) to investigate sagittal characteristics of 123 individuals of cleft and non-cleft group. All the cephalometric parameters were measured by one examiner using automated (20, 21) A.I.-driven Webceph software (South Korea). The angular and linear measurements used in this study are detailed in Table 1.
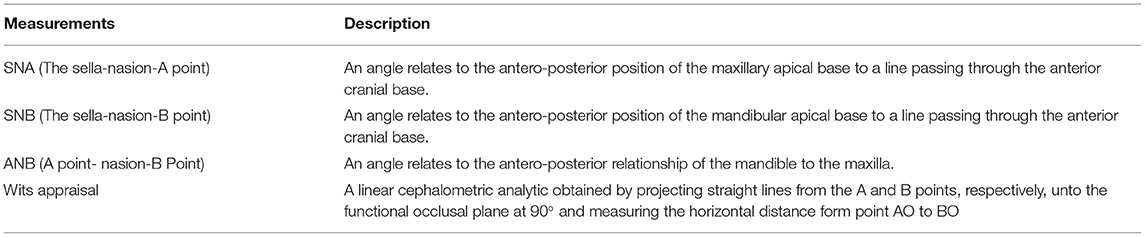
Table 1. The angular and linear cephalometric measurements with description.
Intra-class correlation coefficients were executed to assess the intra-examiner reliability with 20 randomly selected x-rays after 2-weeks interval and found 0.916–0.990 for all measurements which indicates excellent reliability. A two-way ANOVA examination was utilized for gender orientation, types of cleft and gender types of cleft. SPSS 24 (SPSS Inc., Chicago, IL, United States) was used to scrutinize all the data and p-value was set as <0.05.
The mean SNA angle of NC, UCLP, BCLP, UCL and UCLA were 79.795°, 76.158°, 74.953°, 79.443°, and 78.042°, respectively. UCLP (p < 0.001) and BCLP (p < 0.001) subjects had significantly smaller SNA angles compared to NC subjects. Significant difference also observed in two groups. They are BCLP vs. UCL (p-value 0.002) and BCLP vs. UCLA (p-value 0.001). However, no significant differences were found in terms of gender.
Table 2 shows the detailed results of SNA angle in relation to gender and types of cleft and NC.
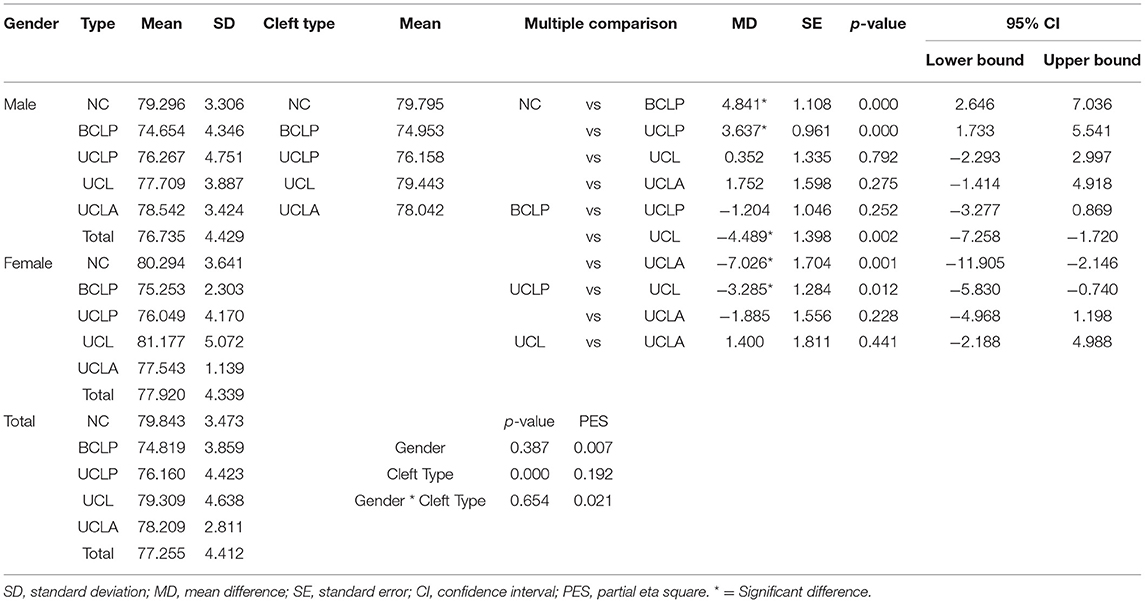
Table 2. Sagittal analysis—SNA: Gender, Types of Cleft and Gender times types of cleft two-way ANOVA analysis results.
The mean SNB angle of NC, UCLP, BCLP, UCL, and UCLA were 76.017°, 76.230°, 75.496°, 76.632°, and 75.917°, respectively. No significant differences found in terms of gender and types of cleft (Table 3).

Table 3. Sagittal analysis—SNB: Gender, Types of Cleft and Gender times types of cleft two-way ANOVA analysis results.
The mean ANB angle of NC, UCLP, BCLP, UCL and UCLA were 3.773°, −0.073°, −0.543°, 2.811°, and 2.128°, respectively. UCLP (p-value <0.001) and BCLP (p-value <0.001) subjects had significantly smaller ANB angles compared to NC subjects. However, no significant differences were found in terms of gender (Table 4).

Table 4. Sagittal analysis—ANB: Gender, Types of Cleft and Gender times types of cleft two-way ANOVA analysis results.
The mean dimensions of NC, UCLP, BCLP, UCL and UCLA were 0.474, −2.599, −3.216, −0.635, and −1.068 mm, respectively. UCLP (p-value 0.003) and BCLP (p-value 0.002) subjects had significantly smaller Wits appraisal compared to NC subjects. However, no significant differences were found in terms of gender.
Table 5 shows the detailed results of Wits appraisal in relation to gender and types of cleft and NC. The profile plot of estimated marginal means of types of cleft and gender*types of cleft has been shown in Figure 1.
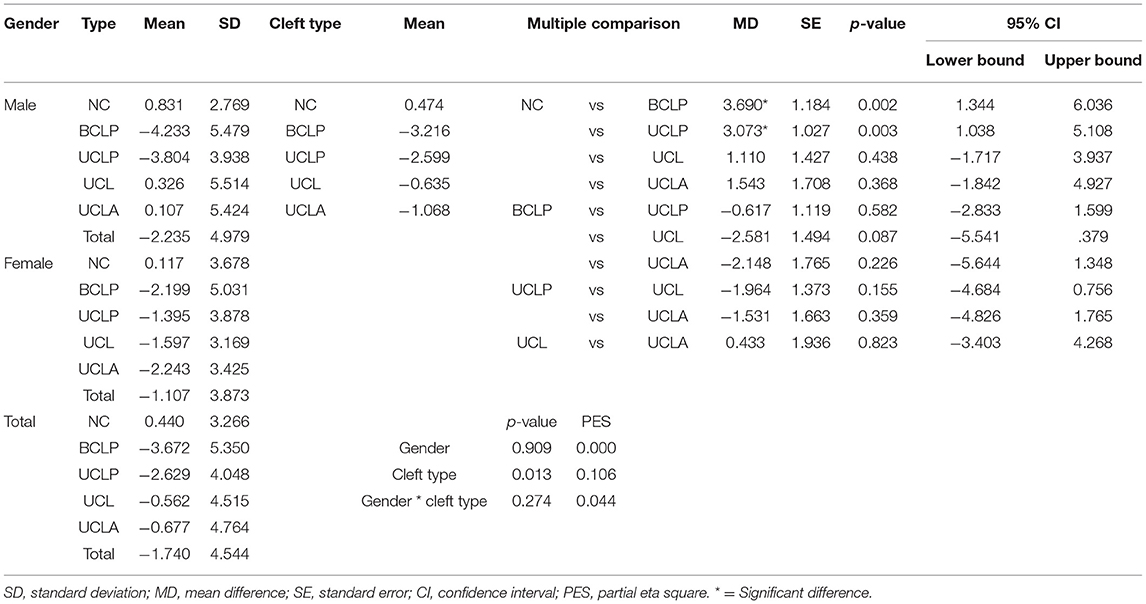
Table 5. Sagittal analysis—Witts analysis: Gender, Types of Cleft and Gender times types of cleft two-way ANOVA analysis results.
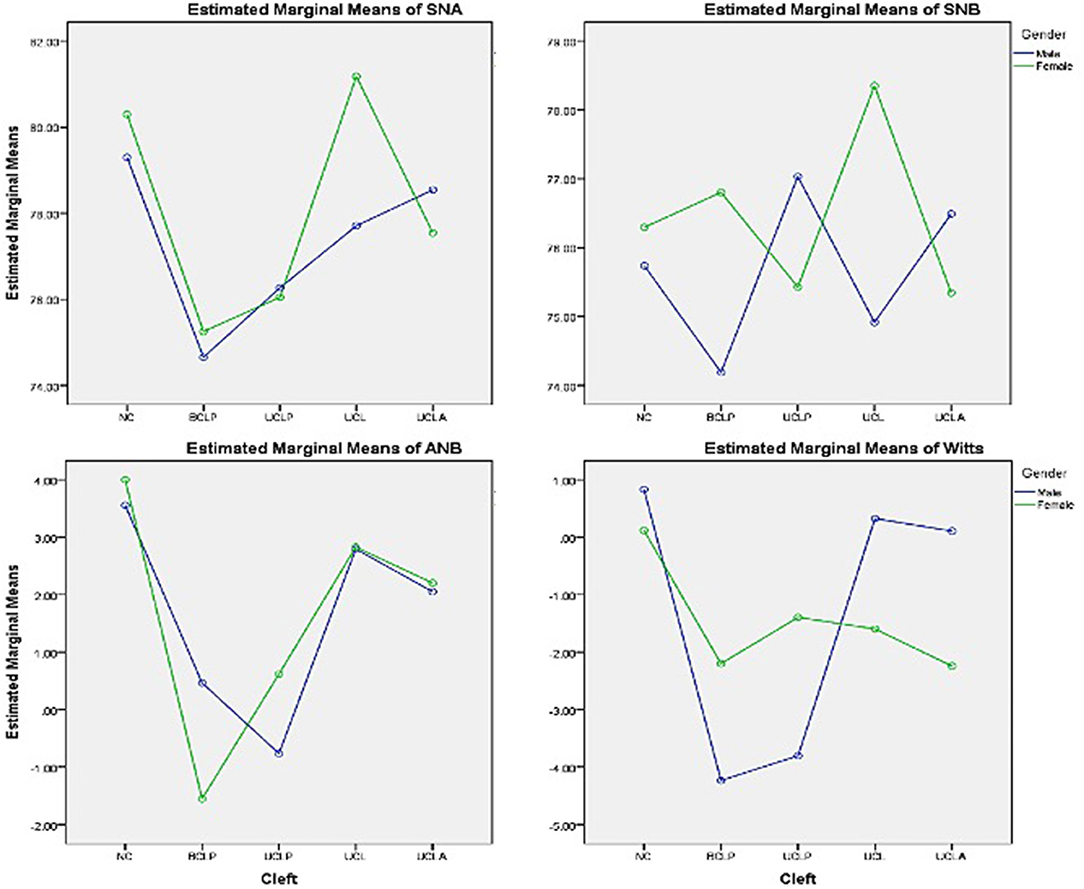
Figure 1. Profile plot of the estimated marginal means of types of cleft and gender*types of cleft.
The prime objective of this paper was to find out and compare the sagittal development among different types of Saudi CLP patients with NC group and also compare it in relation to gender and types of clefts. Even though several researchers were researched on different issues of CLP patients, very few researchers were described on sagittal development of CLP patients. However, no study was documented previously in Saudi population about sagittal development. For the first time, the present work studied the sagittal development among Saudi population exclusively.
In this present study, we measured SNA, SNB, ANB and Wits appraisal of non-syndromic Saudi CLP patients where all the patients completed their primary surgeries (lip surgery and palate surgery) by the first 2 years of life. The maxillofacial growth of a CLP patient is quite convoluted; affected by both congenital and postnatal treatment factors (3). Primary surgeries limited the maxillary growth which leads to maxillary hypoplasia and finally toward Class III malocclusion reported previously (22).
Poor maxillary growth of CLP patients is one of the chief apprehensions of orthodontists for the corrections of the dento-facial discrepancies especially during the period of early adolescence (7). The outcome of the current study may help and support the surgeon to bring out the proper primary surgical techniques and also to the orthodontist to make better treatment plans for CLP patients. The patient who exhibited smaller SNA, ANB and Wits appraisal specifies the poor maxillary growth may perhaps have need of orthognathic surgery in future for the complete correction of dento-facial divergences (7, 23). Wits appraisal is a supreme linear cephalometric parameter which is used to evaluate and assist an additional information with ANB angle for the assessment of skeletal base discrepancies (24).
In our study we found significant reduction of SNA, ANB and Wits appraisal in cleft individuals compared NC individuals which indicated the maxillofacial growth deficiency. However, SNB was an insignificant variable which is a respectable evidence that cleft does not affect on mandibular growth and coincides with one of the earlier studies (25).
The results of current study also match with the outcome of (26) who assessed 45 lateral cephalograms including both cleft and NC individuals reported significantly decreased SNA and ANB between cleft and NC groups and also did not found any significant difference in SNB angle.
An observational study by Holts et al. (27) using German UCLP, BCLP and NC group showed reduced SNA and ANB angle with minor Class III malocclusion in both UCLP and BCLP groups.
Haque et al. (7) put the idea that Modified Millard techniques of Cheiloplasty and Bardach technique of palatoplasty had noticeable negative effect on anterior segment of maxillae especially on inter canine width by studying maxillary arch dimension of Malaysian UCLP subjects. After analyzing the cephalograms of operated Japanese UCLP subjects, Alam et al. (6, 10) also found altered craniofacial morphology in relation to both postnatal treatment factors and congenital factors.
Lisson et al. (28) compared two centers of German children with BCLP ranging from 10 to 18 years in age: center 1 showed significant reduction of ANB and Wits appraisal and center 2 showed significant reduction of ANB and Wits appraisal and significant increase of SNB angle. The outcome of their study revealed underdeveloped maxilla in both centers even though the time and sequence of palatopasty was the main difference between the centers.
The present study also paid attention to gender disparities with sagittal jaw relationships, however did not get any significant difference. In an earlier Saudi cleft study by Alam and Alfawzan (20) on dental characteristics, did not find any significant relation with gender. Similar findings also reported in Bangladeshi UCLP children (11). In contrast, interestingly Arshad et al. (12) reported significant gender disparities in relation to treatment outcome among Pakistani UCLP children. This different result among different populations indicates the racial bias of UCLP subjects.
Although the present study has reached its aim, however, there were some unavoidable limitations. Because of insufficient data from other centers, this study was conducted from a single center. In a future study we plan to do a multi-center study after collection of sufficient data, especially on UCL and UCLA sample from other centers.
In this present study, we observed,
• significant reduction of SNA angle in UCLP, BCLP, UCL and UCLA; ANB angle and Wits appraisal in UCLP and BCLP compared to NC group.
• no significant difference in SNB angle in any cleft and NC group.
• no significant gender inequalities in relation to any type of CLP and NC group.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Ethical Committee of Al Rass Dental Research Center, Qassim University (DRC/009FA/20). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors extend their appreciation to the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number: 375213500 and central laboratory, Jouf University.
1. Haque S, Alam MK. Common dental anomalies in cleft lip and palate patients. Malaysian J Med Sci. (2015) 22:55–60. doi: 10.21315/mjms
2. Burg ML, Chai Y, Yao CA, Magee W, Figueiredo JC. Epidemiology, Etiology, and Treatment of Isolated Cleft Palate. Front Physiol. (2016) 7:67. doi: 10.3389/fphys.2016.00067
3. Haque S, Alam MK, Khamis MF. Treatment outcome of Bangladeshi UCLP patients based on both phenotype and postnatal treatment factors using modified Huddart Bodenham (mHB) index. Cleft Palate Craniofac J. (2018) 55:966–973. doi: 10.1597/15-293
4. Gopinath VK, Samsudin AR, Noor SNFM, Sharab HYM. Facial profile and maxillary arch dimensions in unilateral cleft lip and palate children in the mixed dentition stage. Eur J Dent. (2017) 11:76–82. doi: 10.4103/ejd.ejd_238_16
5. de Saboia TM, Kuchler EC, Tannure PN, Rey AC, Granjeiro JM, de Castro CM, et al. Mesio-distal and buccal-lingual tooth dimensions are part of the cleft spectrum: a pilot for future genetic studies. Cleft Palate Craniofac J. (2013) 50:678–83. doi: 10.1597/11-228
6. Alam MK, Iida J, Sato Y, Kajii TS. Postnatal treatment factors affecting craniofacial morphology of unilateral cleft lip and palate (UCLP) patients in a Japanese population. Br J Oral Maxillofac Surg. (2013) 51:205–10. doi: 10.1016/j.bjoms.2012.10.001
7. Haque S, Khamis MF, Alam MK, Ahmad WMAW. Effects of multiple factors on treatment outcome in the three-dimensional maxillary arch morphometry of children with unilateral cleft lip and palate. J Craniofac Surg. (2020) 31:e534–8. doi: 10.1097/SCS.0000000000006464
8. Adetayo AM, Adetayo MO, Adeyemo WL, James OO, Adeyemi MO. Unilateral cleft lip: evaluation and comparison of treatment outcome with two surgical techniques based on qualitative (subject/guardian and professional) assessment. J Korean Assoc Oral Maxillofac Surg. (2019) 45:141–51. doi: 10.5125/jkaoms.2019.45.3.141
9. Schilling GR, Cardoso MCAF, Maahs MAP. Effect of palatoplasty on speech, dental occlusion issues and upper dental arch in children and adolescents with cleft palate: an integrative literature review. Revista CEFAC. (2019) 21:e12418. doi: 10.1590/1982-0216/201921612418
10. Alam MK, Kajii TS, Sato Y, Iida J. Clinical investigation of congenital factor affecting craniofacial morphology of unilateral cleft lip and palate in Japanese patients. Pesqui Bra Odontopediatria Clín Integr. (2019) 19:4642. doi: 10.4034/PBOCI.2019.191.45
11. Haque S, Alam MK, Khamis MF. The effect of various factors on the dental arch relationship in non-syndromic unilateral cleft lip and palate children assessed by new approach: a retrospective study. BMC Pediatr. (2017) 17:119. doi: 10.1186/s12887-017-0870-4
12. Arshad AI, Alam MK, Khamis MF. Assessment of complete unilateral cleft lip and palate patients: Assessment of complete unilateral cleft lip and palate patients: Determination of factors effecting dental arch relationships. Int J Ped Otorhinolaryngol. (2017) 92:70–4. doi: 10.1016/j.ijporl.2016.11.006
13. Haque S, Alam MK. Spectrum of cheiloplasty has detrimental effect on maxillary growth: myth or fact? Bangladesh J Med Sci. (2014) 13:473–6. doi: 10.3329/bjms.v13i4.20653
14. Rousseau P, Metzger M, Frucht S, Schupp W, Hempel M, Otten JE. Effect of lip closure on early maxillary growth in patients with cleft lip and palate. JAMA Facial Plastic Surg. (2013) 15:369–73. doi: 10.1001/jamafacial.2013.335
15. Zaleckas L, Linkevicine L, Olekas J, Kutra N. The comparison of different surgical techniques used for repair of complete unilateral cleft lip. Medicina. (2012) 47:85–90. doi: 10.3390/medicina47020011
16. Batwa W, Almarhoon HA, Almoammar KA, Alqahtani N, Albarakati SF, Al-Jewair T. Dento-skeletal characteristics of cleft patients with missing teeth. Clin Cosmet Investig Dent. (2018) 10:237–44. doi: 10.2147/CCIDE.S170717
17. de Menezes LM, Azeredo FWA, André R, Juliana L, Rizzatto SMD. Cone-Beam computed tomography evaluation of maxillary expansion in twins with cleft lip and palate. Dent Press J Orthod. (2012) 17:42.e1–42.e11. doi: 10.1590/S2176-94512012000200009
18. Kunz F, Stellzig-Eisenhauer A, Zeman F, Boldt J. Evaluation of a fully automated cephalometric analysis using a customized convolutional neural network. J Orofac Orthop. (2020) 81:52–68. doi: 10.1007/s00056-019-00203-8
19. Lee KS, Ryu JJ, Jang HS, Lee DY, Jung SK. Deep convolutional neural networks based analysis of cephalometric radiographs for differential diagnosis of orthognathic surgery indications. Appl Sci. (2020) 10:2124. doi: 10.3390/app10062124
20. Alam MK, Alfawzan AA. Dental characteristics of different types of cleft and non-cleft individuals. Front Cell Dev Biol. (2020) 8:789. doi: 10.3389/fcell.2020.00789
21. Alam MK, Alfawzan AA. Evaluation of sella turcica bridging and morphology in different types of cleft patients. Front Cell Dev Biol. (2020) 8:656. doi: 10.3389/fcell.2020.00656
22. Alam MK, Kajii TS, Koshikawa-Matsuno M, Sugawara-Kato Y, Sato Y, Iida J. Multivariate analysis of factors affecting dental arch relationships in Japanese unilateral cleft lip and palate patients at Hokkaido University Hospital. Orthod Waves. (2008) 67:45–53. doi: 10.1016/j.odw.2007.12.001
23. Hay N, Patel B, Haria P, Sommerlad B. Maxillary growth in cleft lip and palate patients, with and without vomerine flap closure of the hard palate at the time of lip repair: a retrospective analysis of prospectively collected nonrandomized data, with 10-year cephalometric outcomes. Cleft Palate Craniofac J. (2018) 55:1205–10. doi: 10.1177/1055665618764960
24. Ucheonye IJ, Tokunbo AA, Donald OO. The Wits appraisal among a Nigerian sub-population: an assessment of dental base geometric factors. Brazilian J Oral Sci. (2013) 12:275–9. doi: 10.1590/S1677-32252013000400001
25. Ye B, Wu Y, Zhou Y, Jing H, Hu J, Zhang G. A comparative cephalometric study for adult operated cleft palate and unoperated cleft palate patients. J Craniomaxillofac Surg. (2015) 43:1218–23. doi: 10.1016/j.jcms.2015.04.015
26. Aras I, Baykal D, Bulut M, Dogan S. Evaluation of mandibular hard and soft tissues in cleft patients. J Istanb Univ Fac Dent. (2017) 51:14–22. doi: 10.17096/jiufd.95754
27. Holst AI, Holst S, Nkenke E, Fenner M, Hirschfelder U. Vertical and sagittal growth in patients with unilateral and bilateral cleft lip and palate-a retrospective cephalometric evaluation. Cleft Palate Craniofac J. (2009) 46:512–20. doi: 10.1597/08-041.1
Keywords: sagittal jaw relationship, cleft lip and palate, cephalometric analysis, wits appraisal, SNA angle, SNB angle, ANB angle, artificial intelligence
Citation: Alam MK, Alfawzan AA, Haque S, Mok PL, Marya A, Venugopal A, Jamayet NB and Siddiqui AA (2021) Sagittal Jaw Relationship of Different Types of Cleft and Non-cleft Individuals. Front. Pediatr. 9:651951. doi: 10.3389/fped.2021.651951
Received: 11 January 2021; Accepted: 06 April 2021;
Published: 05 May 2021.
Edited by:
Francesco Morini, Meyer Children's Hospital, ItalyReviewed by:
Ciro Esposito, University of Naples Federico II, ItalyCopyright © 2021 Alam, Alfawzan, Haque, Mok, Marya, Venugopal, Jamayet and Siddiqui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Khursheed Alam, ZHJhbGFtQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.