 Marie Isabel Rasmussen1*
Marie Isabel Rasmussen1* Mathias Lühr Hansen1
Mathias Lühr Hansen1 Gerhard Pichler2
Gerhard Pichler2 Eugene Dempsey3
Eugene Dempsey3 Adelina Pellicer4
Adelina Pellicer4 Afif EL-Khuffash5Shashidhar A6Salvador Piris-Borregas7Miguel Alsina8
Afif EL-Khuffash5Shashidhar A6Salvador Piris-Borregas7Miguel Alsina8 Merih Cetinkaya9
Merih Cetinkaya9 Lina Chalak10
Lina Chalak10 Hilal Özkan11
Hilal Özkan11 Mariana Baserga12Jan Sirc13
Mariana Baserga12Jan Sirc13 Hans Fuchs14
Hans Fuchs14 Ebru Ergenekon15
Ebru Ergenekon15 Luis Arruza16Amit Mathur17
Luis Arruza16Amit Mathur17 Martin Stocker18
Martin Stocker18 Olalla Otero Vaccarello19
Olalla Otero Vaccarello19 Tomasz Szczapa20
Tomasz Szczapa20 Kosmas Sarafidis21
Kosmas Sarafidis21 Barbara Królak-Olejnik22Asli Memisoglu23Hallvard Reigstad24Elżbieta Rafińska-Ważny25Eleftheria Hatzidaki26Zhang Peng27Despoina Gkentzi28Renaud Viellevoye29Julie De Buyst30Emmanuele Mastretta31Ping Wang32Gitte Holst Hahn1Lars Bender33Luc Cornette34Jakub Tkaczyk35Ruth del Rio36
Barbara Królak-Olejnik22Asli Memisoglu23Hallvard Reigstad24Elżbieta Rafińska-Ważny25Eleftheria Hatzidaki26Zhang Peng27Despoina Gkentzi28Renaud Viellevoye29Julie De Buyst30Emmanuele Mastretta31Ping Wang32Gitte Holst Hahn1Lars Bender33Luc Cornette34Jakub Tkaczyk35Ruth del Rio36 Monica Fumagalli37,38Evangelia Papathoma39
Monica Fumagalli37,38Evangelia Papathoma39 Maria Wilinska40
Maria Wilinska40 Gunnar Naulaers41Iwona Sadowska-Krawczenko42Chantal Lecart43
Gunnar Naulaers41Iwona Sadowska-Krawczenko42Chantal Lecart43 María Luz Couce44Siv Fredly45Anne Marie Heuchan46Tanja Karen47
María Luz Couce44Siv Fredly45Anne Marie Heuchan46Tanja Karen47 Gorm Greisen1
Gorm Greisen1- 1Department of Neonatology, Rigshospitalet, Copenhagen, Denmark
- 2Department of Pediatrics, Medical University of Graz, Graz, Austria
- 3Infant Centre and Department of Paediatrics and Child Health, University College Cork, Cork, Ireland
- 4Department of Neonatology, La Paz University Hospital, Madrid, Spain
- 5Department of Pediatrics, The Royal College of Surgeons in Ireland, Dublin, Ireland
- 6St. Johns Medical College Hospital, Bengaluru, India
- 7Department of Neonatology, 12 Octubre University Hospital, Madrid, Spain
- 8Neonatology Department, Hospital Clínic-Maternintat, Barcelona, Spain
- 9Department of Neonatology, Kanuni Sultan Suleyman Training and Research Hospital, Istanbul, Turkey
- 10Division of Pediatrics - Neonatal-Perinatal, University of Texas (UT) Southwestern, Dallas, TX, United States
- 11Division of Neonatology, Department of Pediatrics, Uludag University Medical Faculty, Uludag, Turkey
- 12Division of Neonatology, Department of Pediatrics, University of Utah, Salt Lake City, UT, United States
- 13Third Faculty of Medicine, Institute for the Care of the Mother and Child, Charles University, Prague, Czechia
- 14Center for Pediatrics, Department of Neonatology, Medical Center, University of Freiburg, Freiburg, Germany
- 15Department of Neonatology, Gazi University Hospital, Ankara, Turkey
- 16Division of Neonatology, Instituto del Niño y del Adolescente, Hospital Clinico San Carlos-Health Research Institute San Carlos (IdISSC), Madrid, Spain
- 17Department of Neonatal-Perinatal Medicine, Saint Louis University School of Medicine, St. Louis, MO, United States
- 18Neonatal and Pediatric Intensive Care Unit, Children's Hospital Lucerne, Lucerne, Switzerland
- 19Department of Neonatology, Hospital Universitario de Tarragona Juan XXIII, Tarragona, Spain
- 20Department of Neonatology, Neonatal Biophysical Monitoring and Cardiopulmonary Therapies Research Unit, Poznan University of Medical Sciences, Poznań, Poland
- 21First Department of Neonatology, Aristotle University, Hippokrateion General Hospital, Thessaloniki, Greece
- 22Department of Neonatology, Wrocław Medical University, Wrocław, Poland
- 23Department of Neonatology, Marmara University Pendik Training and Research Hospital, Istanbul, Turkey
- 24Department of Neonatology, Haukeland University Hospital, Bergen, Norway
- 25Department of Neonatology, Centrum Medyczne “Ujastek”, Krakow, Poland
- 26Department of Neonatology and Neonatal Intensive Care Unit (NICU), University Hospital of Heraklion, Crete, Greece
- 27Department of Neonatology, Children's Hospital of Fudan University, Shanghai, China
- 28Neonatal Intensive Care Unit (NICU), Department of Pediatrics, Patras Medical School, Patras, Greece
- 29Neonatal Intensive Care Unit, Department of Pediatrics, University of Liege, Liege, Belgium
- 30Neonatal Intensive Care Unit (NICU), Tivoli Hospital, La Louviere, Belgium
- 31S.C. Neonatologia - Pres Osp S. Anna – Citta della Salute e della Scienza di Torino, Torino, Italy
- 32Department of Neonatology, Guangzhou Women and Children's Medical Center, Guangzhou, China
- 33Department of Neonatology, Aalborg University Hospital, Aalborg, Denmark
- 34Department of Neonatology, AZ St-Jan Bruges, Bruges, Belgium
- 35Department of Neonatology, University Hospital Motol, Prague, Czechia
- 36Department of Neonatology, Hospital Sant Joan de Déu, Barcelona, Spain
- 37Department of Neonatology, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico Milan, Milan, Italy
- 38Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy
- 39Neonatal Intensive Care Unit, “Alexandra” University and State Maternity Hospital, Athens, Greece
- 40Neonatology Department, Centre of Postgraduate Medical Education, Warsaw, Poland
- 41Department of Neonatology, University Hospital Leuven, Leuven, Belgium
- 42Department of Neonatology, Collegium Medicum in Bydgoszcz Nicolaus Copernicus University, Toruń, Poland
- 43Department of Neonatology, Grand Hôpital de Charleroi (GHdC), Charleroi, Belgium
- 44Neonatology Department, University Clinical Hospital of Santiago de Compostela, Health Research Institute of Santiago de Compostela, Santiago, Spain
- 45Department of Neonatology, Oslo University Hospital, Oslo, Norway
- 46Department of Neonatology, Royal Hospital for Children, Glasgow, United Kingdom
- 47Department of Neonatology, University Hospital Zurich, Zurich, Switzerland
Objective: To evaluate if the number of admitted extremely preterm (EP) infants (born before 28 weeks of gestational age) differed in the neonatal intensive care units (NICUs) of the SafeBoosC-III consortium during the global lockdown when compared to the corresponding time period in 2019.
Design: This is a retrospective, observational study. Forty-six out of 79 NICUs (58%) from 17 countries participated. Principal investigators were asked to report the following information: (1) Total number of EP infant admissions to their NICU in the 3 months where the lockdown restrictions were most rigorous during the first phase of the COVID-19 pandemic, (2) Similar EP infant admissions in the corresponding 3 months of 2019, (3) the level of local restrictions during the lockdown period, and (4) the local impact of the COVID-19 lockdown on the everyday life of a pregnant woman.
Results: The number of EP infant admissions during the first wave of the COVID-19 pandemic was 428 compared to 457 in the corresponding 3 months in 2019 (−6.6%, 95% CI −18.2 to +7.1%, p = 0.33). There were no statistically significant differences within individual geographic regions and no significant association between the level of lockdown restrictions and difference in the number of EP infant admissions. A post-hoc analysis based on data from the 46 NICUs found a decrease of 10.3%in the total number of NICU admissions (n = 7,499 in 2020 vs. n = 8,362 in 2019).
Conclusion: This ad hoc study did not confirm previous reports of a major reduction in the number of extremely pretermbirths during the first phase of the COVID-19 pandemic.
Clinical Trial Registration: ClinicalTrial.gov, identifier: NCT04527601 (registered August 26, 2020), https://clinicaltrials.gov/ct2/show/NCT04527601.
Introduction
On the 11th of March 2020, COVID-19 was declared a pandemic by the World Health Organization, which led to an almost worldwide lockdown (1). Major reductions in the birth rates of extremely preterm and extremely low birth weight infants during the lockdown have been reported in Danish (2) and Irish (3) studies. The Danish study reported a decrease in the number of infants born extremely preterm (EP, infant born before 28 weeks gestational age); one EP infant from the 12th of March to the 14th of April of 2020 compared to a mean of 11.4 over the same time period of the preceding 5 years, in all of Denmark (2). The same trend was seen in the Irish study, relying on data from one hospital in Ireland, where no extremely low birth weight infants (<1,000 gm) were born from January to April in 2020, compared to a mean of 4.9 from January to April during the preceding 20 years (3). A Dutch study utilizing a 10-year time period found evidence of a moderate reduction of the whole spectrum of pre-maturity, follow the implementation of COVID-19 mitigation measures (4). In contrast, a Nepalese study (5) based on nine health institutions reported an increase in the preterm birth rate from 16.7 to 20.0%. A birth cohort from two hospitals in Philadelphia, United States, found no significant difference in preterm birth rates, when comparing the period of March to June 2020 (283 preterm births), to the same months during 2018 and 2019 (617 preterm births in total).
The total number of extremely preterm and extremely low birth weight infants in these studies are small and thus, the results should be interpreted with caution (6). The case was taken up in the New York Times, which reported that several neonatologists from neonatal intensive care units (NICU) worldwide, had observed a decrease in local pre-maturity rates, while other neonatologists observed the contrary (7).
The SafeBoosC-III trial investigates the effects of treatment guided by cerebral near-infrared spectroscopy monitoring in extremely preterm infants (8). Despite having a vulnerable population, potentially with an increased risk of complications to a COVID-19 infection, the trial was able to proceed in most countries. Furthermore, several NICUs were opened for randomisation in this time period. However, the average monthly number of randomisations per NICU was almost halved in March, simultaneously with the spread of COVID-19 across Europe (Figure 1). Given the contradictory reports in the published studies on pre-maturity rates during the COVID-19 lockdown, and the variability in observations from neonatologists worldwide and within the SafeBoosC consortium, we decided to formally investigate the effect of the COVID-19 pandemic within our NICUs. For the SafeBoosC-III trial, the difference in EP admissions is most relevant, as this is the eligibility criteria.
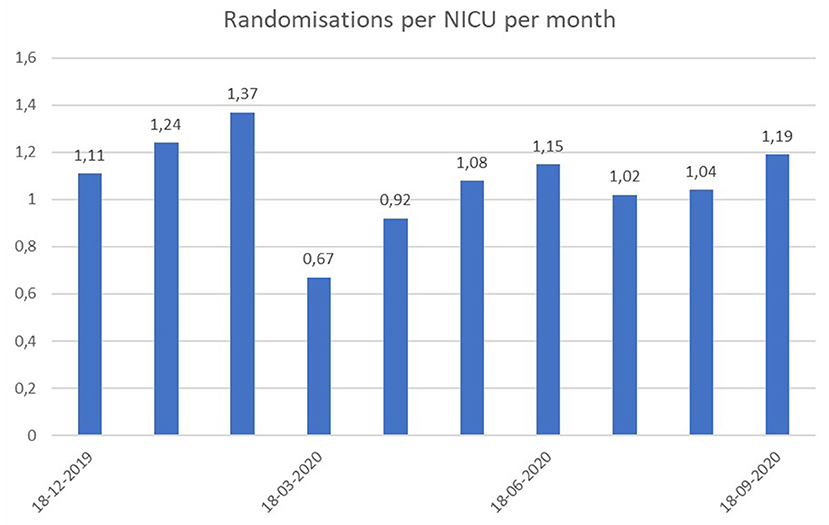
Figure 1. Number of randomisations per month within each NICU actively randomizing infants in the SafeBoosC-III trial during the last 9 months.
The purpose of this study was to evaluate, if the number of admitted EP infants differed in NICUs within the SafeBoosC-III consortium during the global lockdown. Furthermore, being an international consortium, we wished to evaluate if there were differences within geographical regions, or associations between the level of local lockdown restrictions and difference in the number of EP infant admissions.
Methods and Study Design
This is a retrospective, observational study, based on the NICUs in the consortium of the SafeBoosC-III randomized clinical trial (8). The principal investigators from all of the 79 NICUs in the consortium, were invited to participate in this study by e-mail and asked to report the following information: (1) the number of EP infants admitted to their NICU within the 3 months, where the lockdown restrictions were most rigorous during the first phase of the COVID-19 pandemic, (2) the number of EP infants admitted within the corresponding 3 months of 2019, and (3) the level of restrictions imposed upon the public, during the most rigorous 3 months of the lockdown period, in a Likert scale format from one to five. The consecutive 3 months where the lockdown restrictions were most rigorous during the first phase of the COVID-19 pandemic, were subjectively defined by local principal investigators. The scale used to classify the level of lockdown restriction, is a modified scale inspired from the New Zealand COVID-19 alert system (9), with one being the normal state of society, two being mild restrictions, three being moderate restrictions, four being strong restrictions and five being very strong restrictions (full scale in Appendix 1). Principal investigators reported that the data on the number of EP infant admissions was collected from admissions logbooks, NICU databases, hospital databases, and in one case, from a national registry.
Investigators were also asked to categorize the impact of the COVID-19 lockdown on the everyday life of a pregnant woman, and additionally, if they believed that the lockdown restrictions could possibly lead to a non-admittance of EP infants (e.g., intrauterine death due to delayed admittance of the mother, no possibility to transfer the baby from place of birth to a tertiary centre). Lastly, investigators were asked if there within the last year had been any major changes in the organization of perinatal care in their area/region, which may have changed the number of EP infant admissions to their respective NICU. The full data report template and data set can be found in Appendices 1, 2.
Outcomes
The primary outcome was the difference in the total number of EP infant admissions during the 3 months with the most rigorous lockdown restrictions during the first phase of the COVID-19 pandemic, compared to the corresponding 3 months in 2019.
Secondary outcomes were
1) The difference in the number of EP infant admissions within the following regions: Asia, Eastern Europe, Southern Europe, Northern Europe, Western Europe, North America
2) The correlation between the level of the local lockdown restrictions and difference in the number of EP infant admissions.
Exploratory outcomes were (1) the likelihood that restrictions inside or outside health institutions in the investigators country/region, have led to non-admittance of EP infants, (2) if any major changes in the organization of perinatal care had occurred locally, which may have changed the number of admissions of EP infants, and (3) the impact of the COVID-19 lockdown on the everyday life of a pregnant woman.
Statistical Analysis
The statistical analysis was decided a priori. The total number of EP infant admissions, during the 3 months with the most rigorous lockdown restrictions in 2020, during the corresponding three months in 2019, within each region and within each level of lockdown restriction, were to be reported as numbers (n). The primary outcome, as well as the secondary outcome regarding the difference in the number of EP infant admissions within each geographical region, were analyzed using Chi-square tests for 1 × 2 tables. To analyse the correlation between the local level of lockdown restrictions and the difference in number of EP infant admissions, we used simple linear regression. The exploratory outcomes did not undergo statistical analysis but were reported and discussed. For the primary outcome, an alfa level of 5% was chosen as a threshold for significance. To correct for multiple testing in the secondary outcomes, we chose an alfa level of 1%. Statistics were conducted in IBM SPSS Statistics 25 (IBM, Armonk, NY, US).
In a previous funding application for the SafeBoosC-III trial, the 93 NICUs taking part in the application, had reported an average of 30 admissions per year, i.e., 7 per 3 months period. Therefore, if half of the NICUs in the SafeBoosC-III consortium (i.e., 40 NICUs) participated, we would expect a total of 280 EP infant admissions within the 40 NICUs in 2019. Thus, a 16.5% difference in the primary outcome would be needed, to show a statistical significance with a 5% alfa level as threshold.
Pre-defined regions based on the active SafeBoosC-III NICUs can be found in Table 1.

Table 1. Pre-defined regions within the 79 NICUs in the SafeBoosC-III consortium.
Post-hoc Data Collection and Analysis
During the review process of a previous submission for publication of this manuscript, we were asked to provide the total number of NICU admissions. Therefore, in a second round, investigators were asked to report the total number of infant admissions to their NICU within the 3 months where the lockdown restrictions were most rigorous during the first phase of the COVID-19 pandemic, as well as within the corresponding 3 months of 2019.
Ethical Considerations
The Danish National Committee on Health Research Ethics ruled that this study did not constitute a health research project. Therefore, permission to conduct this study was not necessary. To our knowledge, two participating European NICUs consulted with their local ethical committee, regarding the need for approval, but this was not required either. This study was registered on clinicaltrials.gov (NCT04527601) before any data collection started.
Results
Data was delivered from 46 NICUs on a total of 885 EP infants across 17 countries (Austria, Belgium, China, Czech Republic, Denmark, Germany, Greece, India, Ireland, Italy, Norway, Poland, Switzerland, Spain, Turkey, UK, USA). The data source was reported to be an admission logbook (n = 16), a NICU database (n = 19), a hospital database (n = 10), and a national database (n = 1). During the 3 months with the most rigorous lockdown restrictions in 2020 the number of EP infant admissions was 428, compared to 457 in the corresponding 3 months of 2019 (a decrease of 6.6%, 95% CI −18.2 to +7.1%, p = 0.33). No significant differences were found in the number of EP admissions between 2020 and 2019 within the individual six pre-defined geographical regions (Table 2 and Figure 2).
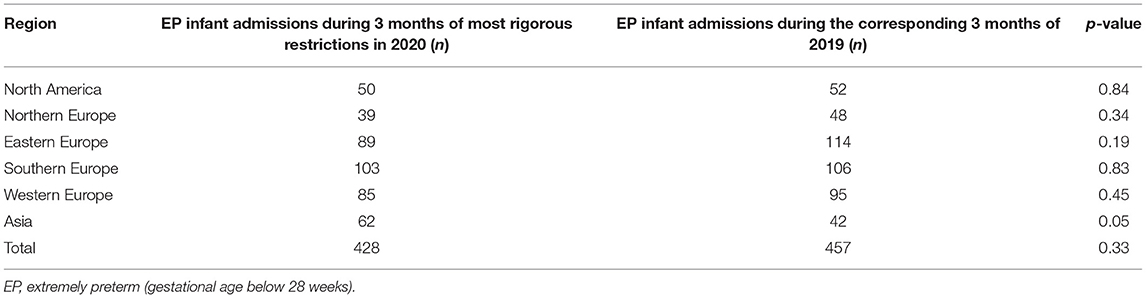
Table 2. EP infant admissions in 2020 and 2019 within each pre-defined geographic region.
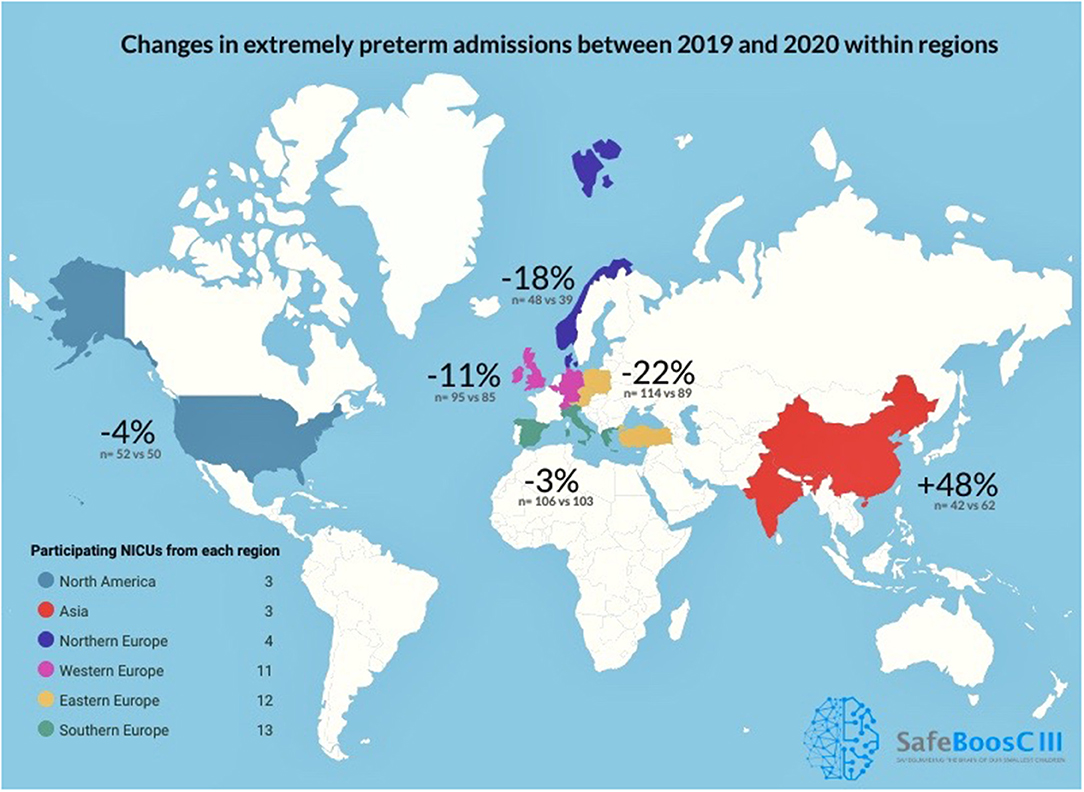
Figure 2. Change in percent in extremely preterm admissions between the 3 months with the most rigorous lockdown restrictions in 2020, compared to the corresponding months of 2019 in the 46 participating NICUs in the SafeBoosC-III consortium.
The linear regression analysis showed no significant correlation between the level of lockdown restriction and difference in the number of EP infant admissions (p = 0.3; Table 3).

Table 3. Number of EP infant admissions in 2020 and 2019 stratified by level of lockdown restriction.
When investigators were asked to describe the impact of the COVID-19 lockdown on the everyday life of a pregnant woman, 33 out of 46 (72%) answered that they thought the change had been radical or very radical (Table 4). Two out of 46 (4%) answered that they thought the change had been little or very little. Investigators were furthermore asked to classify the likelihood that restrictions outside or inside health institutions in their country/region, could have led to non-admittance of EP infants. Thirty-four out of 46 (74%) answered that they thought it was unlikely or very unlikely (Table 4). Three out of 46 (7%) answered that they thought it was likely or very likely.

Table 4. Reporting of exploratory outcome results.
Of the 46 participating investigators, three reported changes in the structure and organization of perinatal care within their NICU, during the lockdown period. This included reports of nursing staff being rotated to COVID-19 services, increase or decrease in the NICU bed capacity due to structural changes caused by COVID-19 and COVID-19 testing of all patients before admission. One investigator also suspected that online consultations instead of on-site consultations with mothers could have led to a greater amount of intrauterine complications and thus, preterm births.
Post-hoc Analysis Results
The post-hoc analysis was based on data from all 46 NICUs. The total amount of NICU admissions during the three most rigorous lockdown months of 2020 was 7,499 and the admissions of same time period in 2019 was 8,362. The overall difference was −10.3 percent. The percentage of extremely preterm infants of total admissions was 5.7 percent in 2020 compared to 5.5 percent in 2019. The difference between regions can be found in Table 5.
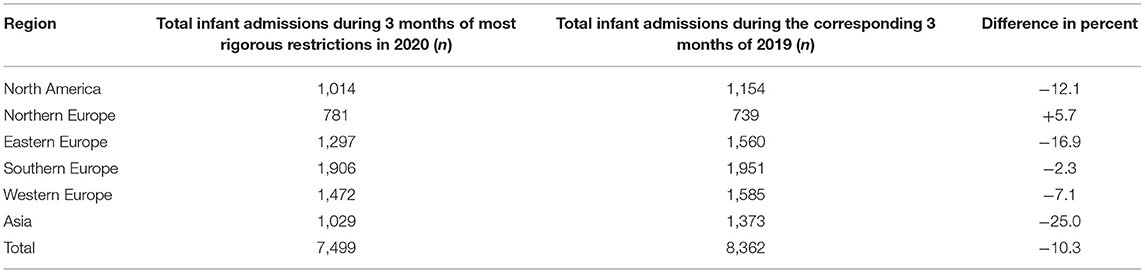
Table 5. Total NICU admissions in 2020 and 2019 within each pre-defined geographic region.
Discussion
Based on 885 EP infant admissions from 46 NICUs across 17 countries, this international retrospective, observational study found no major decrease in the number of EP infant admissions during the 3 months with the most rigorous lockdown restrictions during the first phase of the COVID-19 pandemic compared with the corresponding 3 months in 2019. Furthermore, no major changes in the number of EP infant admissions were seen within the geographical regions, although the statistical uncertainty was greater. There was no correlation between levels of lockdown restrictions and changes in the number of EP infant admissions. The post-hoc analysis, revealed an overall decrease of 10.3 percent in total NICU admissions, thus the EP infant admission percentage was very constant.
Our study has two important strengths. First, to our knowledge, this study is the largest evaluating the effect of the first phase of the COVID-19 pandemic on EP infant admissions, so far. We surpassed the indicative sample size, which decreases the risk of type II errors, and to some extent compensates for the correction for multiple testing in the secondary outcomes (10). Secondly, the protocol for this study, including the statistical analysis plan, was registered at clinicaltrials.gov before any data was collected, thereby reducing the risk of selective outcome reporting bias (11).
Our study has several weaknesses. First, as COVID-19 is an emergency, we decided to move quickly and therefore, the principal investigators had 3 weeks (August 28th–September 13th, 2020) to report the data. It is plausible that the participation would have been better if we had prolonged the data collection time. Thirty-three NICUs of the SafeBoosC-III consortium did not participate in this study, for reasons which are uncertain. This imposes a potential bias, although it may appear unlikely that this would tend to remove a real effect of the lockdown. Secondly, the data was self-reported, not verified by a third party, and collected in an unblinded fashion, although from well-defined sources. Thirdly, we compared only with the corresponding time period in 2019, not several preceding years, as done in previous studies. The previous studies, however, needed to do that to achieve statistical strength. This was not necessary in our case. It is unlikely that 2019 should have been unrepresentative for the preceding period, due to the large number of participating NICUs. Fourthly, the 3 months where the lockdown restrictions were deemed most rigorous, might not necessarily be the peak months in terms of COVID-19 cases. Thus, the results from this study do not necessarily reflect the number of admissions during the months with most COVID-19 cases. Furthermore, subjective judgements by the local investigators were used to judge the level of lockdown restriction, whether the lockdown had an impact on the life of pregnant women and whether lockdown restrictions could possibly lead to non-admittance of EP infants. This was done to provide simple background information since a more formal data collection for this purpose would have been a major undertaking. The subjective judgements may pose as a limitation in regard to response bias. It is plausible, however, that most of these biases would rather have induced a false association between the change in numbers and the possible explaining factors. The analysis of number of admissions within each geographical region had lower statistical power, due to correction for multiple testing in the secondary outcome analyses, as well as the smaller number of admissions within each region (10).
The most important weakness to consider is the self-selection of the NICUs in the SafeBoosC-III consortium. It is an “ad-hoc” group of neonatologists with an academic interest in brain-oriented neonatal care. Therefore, the NICUs that have provided data for this study are typically academic, tertiary NICUs and their admissions of EP infants may not represent EP infants in the regions they serve. It is again, however, difficult to see how this would bias the results as regards the effect of the initial COVID-19 lockdown. Also, only few investigators reported that the COVID-19 epidemic had affected the organization of neonatal intensive care in their regions. Finally, due to the drop in the randomisation rate in the SafeBoosC-III trial, an investigator-bias would most likely to have been in the direction of an exaggerated effect of the lockdown.
In summary, we conclude that our results may be a fair estimate of the general, global effect of the lockdown and that it is likely to have been small, a conclusion that is also supported by results in a previous report (12). Lockdown restrictions causing pregnant women to be more likely to stay home may certainly influence several risk factors for preterm birth, such as stress and prolonged standing at work as well as infections on one side and the clinical processes leading to physician-induced birth on the other side. It is also possible, that in some unfortunate cases, an extremely preterm delivery may have taken the form as a late miscarriage. But our results suggest that these effects have been at most moderate in magnitude.
Despite the number of EP admissions did not significantly differ much in 2020 from 2019, the average number of randomisations in the SafeBoosC-III trial, dropped significantly in March 2020, where the COVID-19 pandemic spread across Europe. Possible explanations for this specific finding, could be that some NICUs participating in the SafeBoosC-III trial, were forced to suspend all clinical research, due to the pandemic. In others, some staff members were re-allocated to clinical duty in COVID-19 departments. Furthermore, some NICUs split the clinical staff into smaller groups, so that fewer staff members were working simultaneously in the NICU, as a preventive measure to avoid the spread of COVID-19 within the department (personal communication). Such measures could all potentially affect the number of randomisations in SafeBoosC-III.
We have studied the immediate effects of lockdown. Delayed effects are also possible. The existence of neonatal networks and national registries will allow stronger epidemiological studies to be done, including examining the effects on the children themselves.
Conclusion
This larger ad hoc study did not confirm previous reports of a major reduction in the number of extremely preterm births during the first phase of the COVID-19 pandemic.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
MR, MH, and GG contributed to the conception and design of the study, drafted the protocol, collected data, drafted the manuscript, and gave final approval of the version to be published. TK, ED, AH, SF, MC, CL, IS-K, GN, MW, EP, MF, RR, JT, LCo, LB, GH, PW, EM, JD, RV, DG, ZP, EH, ER-W, HR, AE-K, AMa, SA, SP-B, BK-O, KS, TS, OO, MS, AMe, LA, EE, HF, JS, MB, AP, HO, LCh, GP, MC, and MA contributed to the data collection, revised the manuscript critically for important intellectual content, and gave final approval of the version to be published. All authors contributed to the article and approved the submitted version.
Funding
The sponsor/coordinating investigator, Professor of Paediatrics GG, is the initiator of the SafeBoosC-III project. He has no financial interest in the results of the trial. The Elsass Foundation, Aage and Johanne Louis-Hansen Foundation, and Svend Andersen Foundation supported the SafeBoosC-III trial through unconditional and unrestricted grants of DKK 3,300,000, DKK 1,000,000 and DKK 1,000,000, respectively. These funding sources had no role in the design of this study and will not have any role during its execution, analysis, interpretation of the data or decision to submit results.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This study was conducted utilizing the SafeBoosC-III consortium and we sincerely thank the principal investigators for their cooperation and rapid data collection.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.647880/full#supplementary-material
References
1. Hale T, Angrist N, Cameron-Blake E, Petheric A, Phillips T, Webster S, et al. Oxford Covid-19 Government Response Tracker. Oxford: Blavatnik School of Government (2020). p. 25.
2. Hedermann G, Hedley PL, Bækvad-Hansen M, Hjalgrim H, Rostgaard K, Poorisrisak P, et al. Danish premature birth rates during the COVID-19 lockdown. Arch Dis Child Fetal Neonatal Ed. (2020) 106:F93–F95. doi: 10.1136/archdischild-2020-319990
3. Philip RK, Purtill H, Reidy E, Daly M, Imcha M, McGrath D, et al. Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID-19 lockdown in Ireland: a ‘natural experiment’ allowing analysis of data from the prior two decades. BMJ Global Health. (2020) 5:e003075. doi: 10.1136/bmjgh-2020-003075
4. Been JV, Burgos Ochoa L, Bertens L, Schoenmakers S, Steegers E, Reiss I, et al. Impact of COVID-19 mitigation measures on the incidence of preterm birth: a national quasi-experimental study. Lancet Public Health. (2020) 5:e604–11. doi: 10.1016/S2468-2667(20)30223-1
5. Ashish KC, Gurung R, Kinney MV, Sunny AK, Moinuddin M, Basnet O, et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: a prospective observational study. Lancet Global Health. (2020) 8:1273–81. doi: 10.1016/S2214-109X(20)30345-4
6. Banerjee A, Chitnis U, Jadhav S, Bhawalkar JS, Chaudhur S. Hypothesis testing, type I and type II errors. Ind Psychiatry J. (2009) 18:127–31. doi: 10.4103/0972-6748.62274
7. Preston E. During Coronavirus Lockdowns, Some Doctors Wondered: Where Are the Preemies? The New York Times (2020): July 21:D:7. Available online at: https://www.nytimes.com/2020/07/19/health/coronavirus-premature-birth.html (accessed September 23, 2020).
8. Hansen ML, Pellicer A, Gluud C, Dempsey E, Mintzer J, Hyttel-Soerensen S, et al. Cerebral near-infrared spectroscopy monitoring versus treatment as usual for extremely preterm infants: a protocol for the SafeBoosC randomised clinical phase III trial. Trials. (2019) 20:811. doi: 10.1186/s13063-019-3955-6
9. Alert System Overview | Unite Against COVID-19. Available online at: https://covid19.govt.nz/alert-system/about-the-alert-system/ (accessed September 23, 2020).
10. Akobeng AK. Understanding type I and type II errors, statistical power and sample size. Acta Paediatr. (2016) 105:605–9. doi: 10.1111/apa.13384
11. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Bourtron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:bmj.l4898. doi: 10.1136/bmj.l4898
Keywords: extremely preterm, COVID-19, randomized clinical trial, pandemic, observational study, neonatal intensive care unit admission
Citation: Rasmussen MI, Hansen ML, Pichler G, Dempsey E, Pellicer A, EL-Khuffash A, A S, Piris-Borregas S, Alsina M, Cetinkaya M, Chalak L, Özkan H, Baserga M, Sirc J, Fuchs H, Ergenekon E, Arruza L, Mathur A, Stocker M, Otero Vaccarello O, Szczapa T, Sarafidis K, Królak-Olejnik B, Memisoglu A, Reigstad H, Rafińska-Ważny E, Hatzidaki E, Peng Z, Gkentzi D, Viellevoye R, De Buyst J, Mastretta E, Wang P, Hahn GH, Bender L, Cornette L, Tkaczyk J, del Rio R, Fumagalli M, Papathoma E, Wilinska M, Naulaers G, Sadowska-Krawczenko I, Lecart C, Couce ML, Fredly S, Heuchan AM, Karen T and Greisen G (2021) Extremely Preterm Infant Admissions Within the SafeBoosC-III Consortium During the COVID-19 Lockdown. Front. Pediatr. 9:647880. doi: 10.3389/fped.2021.647880
Received: 30 December 2020; Accepted: 15 June 2021;
Published: 12 July 2021.
Edited by:
Robert Cohen, Independent Researcher, Paris, FranceReviewed by:
Joseph Y. Ting, University of British Columbia, CanadaSven Wellmann, University of Regensburg, Germany
Copyright © 2021 Rasmussen, Hansen, Pichler, Dempsey, Pellicer, EL-Khuffash, A, Piris-Borregas, Alsina, Cetinkaya, Chalak, Özkan, Baserga, Sirc, Fuchs, Ergenekon, Arruza, Mathur, Stocker, Otero Vaccarello, Szczapa, Sarafidis, Królak-Olejnik, Memisoglu, Reigstad, Rafińska-Ważny, Hatzidaki, Peng, Gkentzi, Viellevoye, De Buyst, Mastretta, Wang, Hahn, Bender, Cornette, Tkaczyk, del Rio, Fumagalli, Papathoma, Wilinska, Naulaers, Sadowska-Krawczenko, Lecart, Couce, Fredly, Heuchan, Karen and Greisen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Isabel Rasmussen, bWFyaWUuaXNhYmVsLnNrb3YucmFzbXVzc2VuQHJlZ2lvbmguZGs=