 Gema González-Luis1
Gema González-Luis1 Stefano Ghirardello2
Stefano Ghirardello2 Pilar Bas-Suárez3
Pilar Bas-Suárez3 Giacomo Cavallaro2Fabio Mosca2,4Ronald I Clyman5
Giacomo Cavallaro2Fabio Mosca2,4Ronald I Clyman5 Eduardo Villamor6*
Eduardo Villamor6*- 1Department of Neonatology, Complejo Hospitalario Universitario Insular Materno-Infantil (CHUIMI) de Canarias, Las Palmas de Gran Canaria, Spain
- 2Neonatal Intensive Care Unit, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy
- 3Department of Pediatrics, Hospital Vithas Santa Catalina, Las Palmas de Gran Canaria, Spain
- 4Department of Clinical Sciences and Community Health, Università degli Studi di Milano, Milan, Italy
- 5Cardiovascular Research Institute, Department of Pediatrics, University of California, San Francisco, San Francisco, CA, United States
- 6Department of Pediatrics, Maastricht University Medical Center (MUMC+), School for Oncology and Developmental Biology (GROW), Maastricht, Netherlands
Background: A meta-analysis published in 2015 showed a significant association between low platelet counts in the first day(s) of life and risk of patent ductus arteriosus (PDA). The meta-analysis pooled data from 11 studies cohorts (3,479 preterm infants).
Objective: To update the meta-analysis by adding new studies on the topic and including other platelet parameters different from platelet counts.
Methods: PubMed/Medline and Embase databases were searched. Random-effects risk ratios (RR) and differences in means (DM) and 95% confidence intervals (CI) were calculated.
Results: We included 31 studies (7,638 infants). Meta-analysis showed that the risk of developing any PDA was significantly associated with platelet counts<150 × 109/L (11 studies, RR 1.58, 95% CI 1.28 to 1.95), and <100 x 109/L (7 studies, RR 1.61, 95% CI 1.14 to 2.28), but not <50 x 109/L (4 studies, RR 1.34, 95% CI 0.77 to 2.32). Risk of developing hemodynamically significant PDA (hsPDA) was significantly associated with platelet counts<150 x 109/L (12 studies, RR 1.33, 95% CI 1.09 to 1.63), and <100 x 109/L (7 studies, RR 1.39, 95% CI 1.06 to 1.82), but not <50 x 109/L (6 studies, RR 1.24, 95% CI 0.86 to 1.79). Infants with hsPDA had significantly lower mean platelet counts (19 studies, DM 22.0 x 109, 95% CI 14.9 to 29.1) and platelet mass (11 studies, DM 214.4, 95% CI 131.2 to 297.5) and significantly higher platelet distribution width (PDW, 9 studies, DM −0.53, 95% CI −1.01 to −0.05) than infants without hsPDA. Meta-analysis could not demonstrate significant differences in mean platelet volume (MPV).
Conclusion: Compared to the previous analysis, this updated meta-analysis included 21 additional studies that provide stronger evidence of the association between low platelet counts and PDA/hsPDA. Other platelet parameters such as platelet mass and PDW are also associated with hsPDA risk. However, the low number of platelets may be an epiphenomenon associated with the maturity and clinical stability of preterm infants rather than a contributing factor in the pathogenesis of PDA.
Introduction
Failure of ductus arteriosus (DA) closure in preterm infants is a conundrum that neonatologists have faced for decades and whose pathophysiological and clinical implications are far from being solved (1–10). In 2010, Echtler et al. made a significant contribution to the understanding of DA pathobiology when they showed that normal number and function of platelets were key factors for mice DA closure (11). They also reported an association between low platelet counts in the first day of life and risk of developing patent DA (PDA) in a cohort of 123 infants born at 24 to 30 weeks of gestation (11). The publication of these results prompted numerous groups of neonatologists to analyze the potential association between the number of platelets at birth and the presence of PDA in their populations (12–18).
In 2015, we conducted a systematic review and meta-analysis on the topic of platelet counts in the first days of life and PDA (19). The meta-analysis pooled data from 11 study cohorts (3,479 preterm infants) and showed a significant association between PDA and platelet counts<150 × 109/L as well as platelet counts <100 × 109/L. However, the results were largely limited by the low robustness of the association and the high degree of statistical heterogeneity among studies. The evidence was therefore highly susceptible to being modified as more researchers published new data. The objective of the present study was to update our previous meta-analysis. Since our original report, we have located 20 additional studies that we have included in a new meta-analysis. Several studies included information about other platelet factors in addition to platelet counts. These factors have been also included in our updated meta-analysis.
Methods
The methodology employed in this updated systematic review and meta-analysis is similar to that previously described in our 2015 report (19).
Search
We set up a monthly electronic alert from PubMed for new articles containing the most relevant search terms of our previous meta-analysis (last update June 2020). In addition, a new search was conducted in Pubmed and Embase on April 15, 2020 and we searched the Science Citation Index and Google Scholar for articles citing our previous meta-analysis as well as the articles that were included in it.
Inclusion Criteria and Study Selection
Two investigators (G G-L, and EV) independently evaluated studies for inclusion and any disagreements were resolved by discussion. Studies were included for analysis if satisfying all following criteria: (1) full text was available in English, Spanish, Italian, Dutch, French, German, Portuguese, Galician, or Catalan; (2) a prospective or retrospective cohort study or case-control design was used; (3) primary data were reported in a manner that could be used to measure the association between PDA and platelet counts or other platelet parameters; and (4) the study population was comprised of preterm infants. As in our previous meta-analysis the studies were divided according to the way they considered small ductal shunts (19). Studies comparing closed DA vs. small plus large PDA, were classified as reporting on “any PDA.” Studies comparing closed DA and/or small PDA vs. large PDA, were classified as reporting on “hemodynamically significant PDA” (hsPDA).
Data Extraction and Assessment of Study Quality
Two investigators (GG-L, EV) independently extracted data on study design, demographics, rate of PDA and/or hsPDA, platelet counts, and other quantitative or qualitative platelet factors. A second group of investigators (SC, GC) checked the data extraction for completeness and accuracy. In cases in which necessary data were missing from the studies, additional information was requested from the authors. Methodological quality was assessed using the Newcastle-Ottawa Scale (NOS) for cohort or case-control studies (20).
Statistical Analysis
Studies were combined and analyzed using COMPREHENSIVE META-ANALYSIS V 3.0 software (Biostat Inc., Englewood, NJ, USA). For dichotomous outcomes, the risk ratio (RR) with 95% confidence interval (CI) was calculated from the data provided in the studies. For continuous outcomes, the difference in means (DM) with 95% CI was calculated. When studies reported continuous variables as median and range or interquartile range, we requested the mean and standard deviation from the authors or, alternatively, we estimated them using the method of Wan et al. (21). Due to anticipated heterogeneity, summary statistics were calculated with a random-effects model. This model accounts for variability between studies as well as within studies. To identify any study that may have exerted a disproportionate influence on the summary effect, we deleted studies one at a time. Heterogeneity was assessed with the Q statistic and quantified using the I2 statistic. Publication bias was assessed only for the analyses including at least 10 studies. We used the Egger's regression test and visual analysis of funnel plots to assess publication bias. Meta-regression, using random effects (method of moments estimator), was performed to explore the following sources of heterogeneity in the association between platelet counts and PDA/hSPDA: cohort mean or median gestational age (GA) and birth weight (BW), percent males, rate of PDA/hsPDA, thrombocytopenia rate, and number of infants included in the study. Meta-regression was performed only for the analyses including at least 10 studies. A probability value of <0.05 (0.10 for heterogeneity) was considered statistically significant.
Results
Included Studies
The new search identified 20 articles (22–41) that were added to the 11 already included in our previous meta-analysis (19). The PRISMA flow diagram of the search process is shown in Supplementary Figure 1. The 31 studies yielded a population of 7,638 preterm infants. The main characteristics of the studies are shown in Table 1. All the studies were cohort studies and only one (43) was prospective. Each study was allocated more than six NOS stars (Supplementary Table 1). The criteria used in each study for the definition of PDA and/or hsPDA are shown in Supplementary Table 2. From the included studies, 13 (11, 14–16, 19, 23, 32, 34, 37–39, 42, 43) reported on any PDA; that is, infants with a small PDA were included by the authors in the PDA group. Twenty-four studies (11–13, 16–19, 22–36, 41) compared infants with and without hsPDA; that is, infants with a small PDA were included by the authors in the non-PDA group. Six studies (11, 16, 19, 23, 32, 34) provided data on closed DA, small PDA and hsPDA. We included these studies in both analyses of any PDA and hsPDA. Twelve studies (22–27, 29–31, 35, 40, 41) reported data on mean platelet volume (MPV). Eleven studies (22–26, 29, 30, 35, 40, 41) reported data on platelet mass, and four studies (22, 26, 30, 41) reported data on plateletcrit. Since the plateletcrit is calculated with the formula platelet count (104/μl) × MPV (fL) × 10−3 (44) and the platelet mass is calculated with the formula platelet count (109/L) × MPV (fL) (45), plateletcrit values were converted into platelet mass values by multiplying by 104. Nine studies (22, 23, 25–27, 30, 35, 40, 41) reported data on platelet distribution width (PDW).
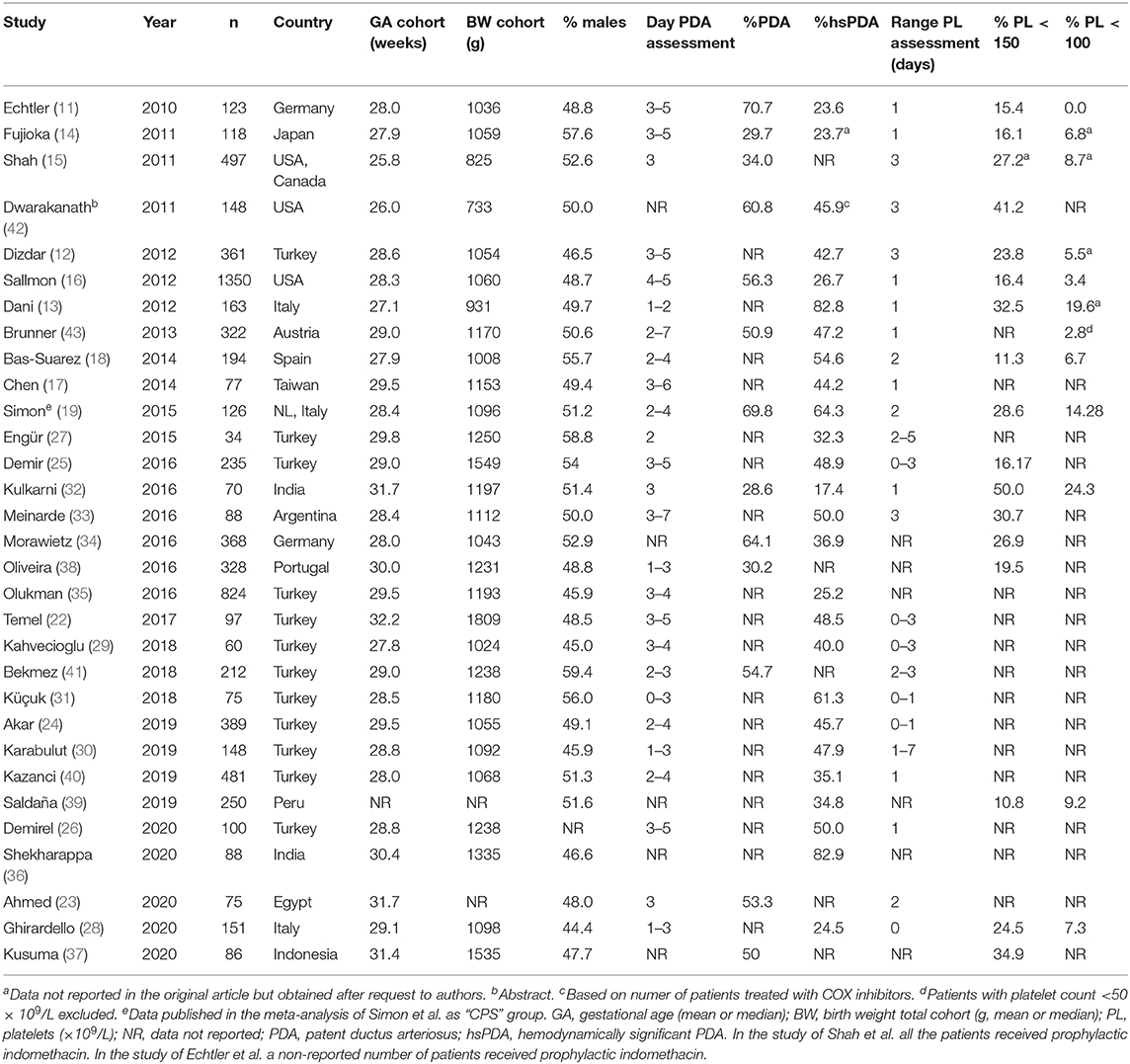
Table 1. Characteristics of the studies included in the meta-analysis.
Meta-Analysis
Any PDA
Data on rate of any PDA in infants with platelet counts above or below 150 × 109/L were available from 11 studies (11, 14–16, 19, 32, 34, 37–39, 42). There was a significant positive association between any PDA and platelet counts below 150 × 109/L (Figure 1A). The results of sensitivity analyses, excluding one study at a time, for this and all other analyses are shown in Supplementary Table 3. Neither visual inspection of the funnel plot (Supplementary Figure 2A) nor Egger's regression test (P = 0.066) revealed evidence of significant publication bias.
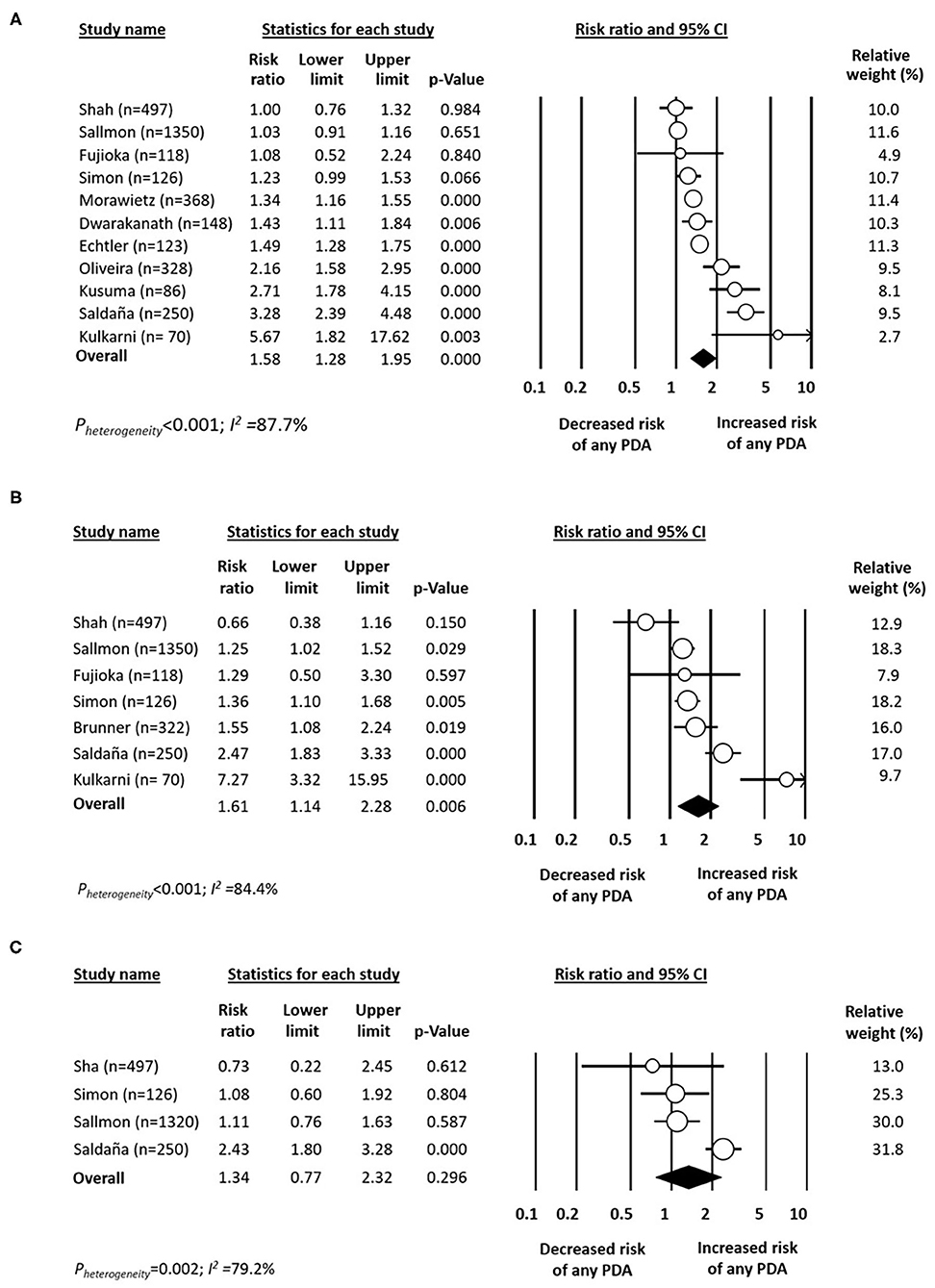
Figure 1. Forest plot for studies examining the association between platelet counts below (A) 150 × 109/L, (B) 100 × 109/L, and (C) 50 × 109/L in the first day(s) of life on patent ductus arteriosus (PDA). Risk ratio >1 indicates increased risk of PDA.
Data on rate of PDA in infants with platelet counts above or below 100 × 109/L were available from seven studies (14–16, 19, 32, 39, 43). There was a significant positive association between any PDA and platelet counts below 100 × 109/L (Figure 1B). Data on rate of any PDA in infants with platelet counts above or below 50 × 109/L were available from four studies (15, 16, 19, 39). Meta-analysis could not detect a significant association between any PDA and platelet counts below 50 × 109/L (Figure 1C). Mean (SD) platelet counts in infants with and without any PDA were available from four studies (14, 15, 19, 23). Meta-analysis could not demonstrate a significant difference in mean platelet counts between the two groups (Figure 2A).
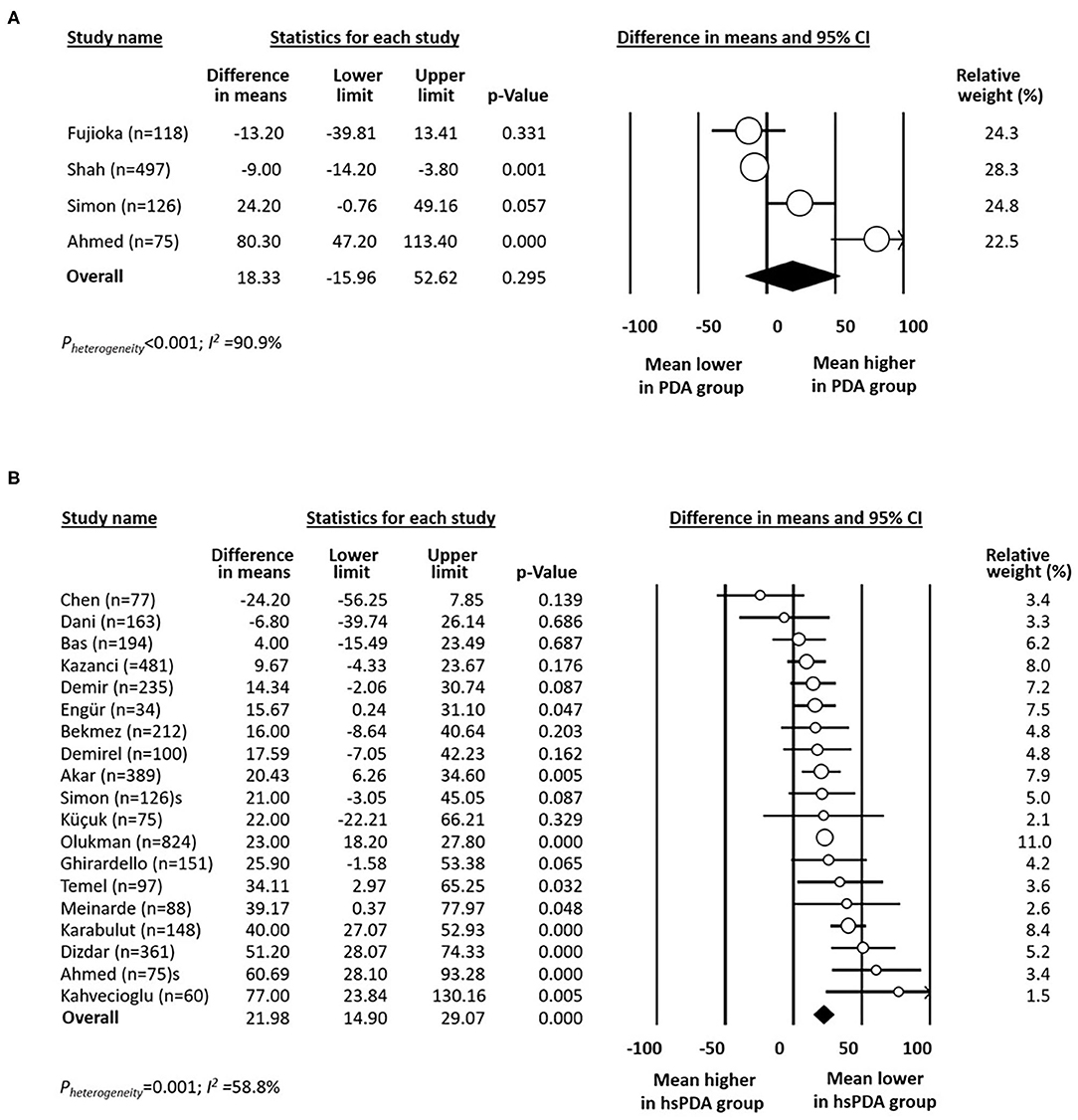
Figure 2. Forest plot for studies examining the difference (PDA-no minus PDA-yes) in mean platelet count (×109/L) in the first day(s) of life in infants with and without any patent ductus arteriosus (PDA, A) and with and without hemodynamically significant patent ductus arteriosus (hsPDA, B).
Hemodynamically Significant PDA
Data on rate of hsPDA in infants with platelet counts above or below 150 × 109/L were available from 12 studies (11–13, 16, 18, 19, 25, 28, 32–35). There was a significant positive association between hsPDA and platelet counts below 150 x 109/L (Figure 3A). Neither visual inspection of the funnel plot (Supplementary Figure 2B) nor Egger's regression test (P = 0.130) revealed evidence of significant publication bias.
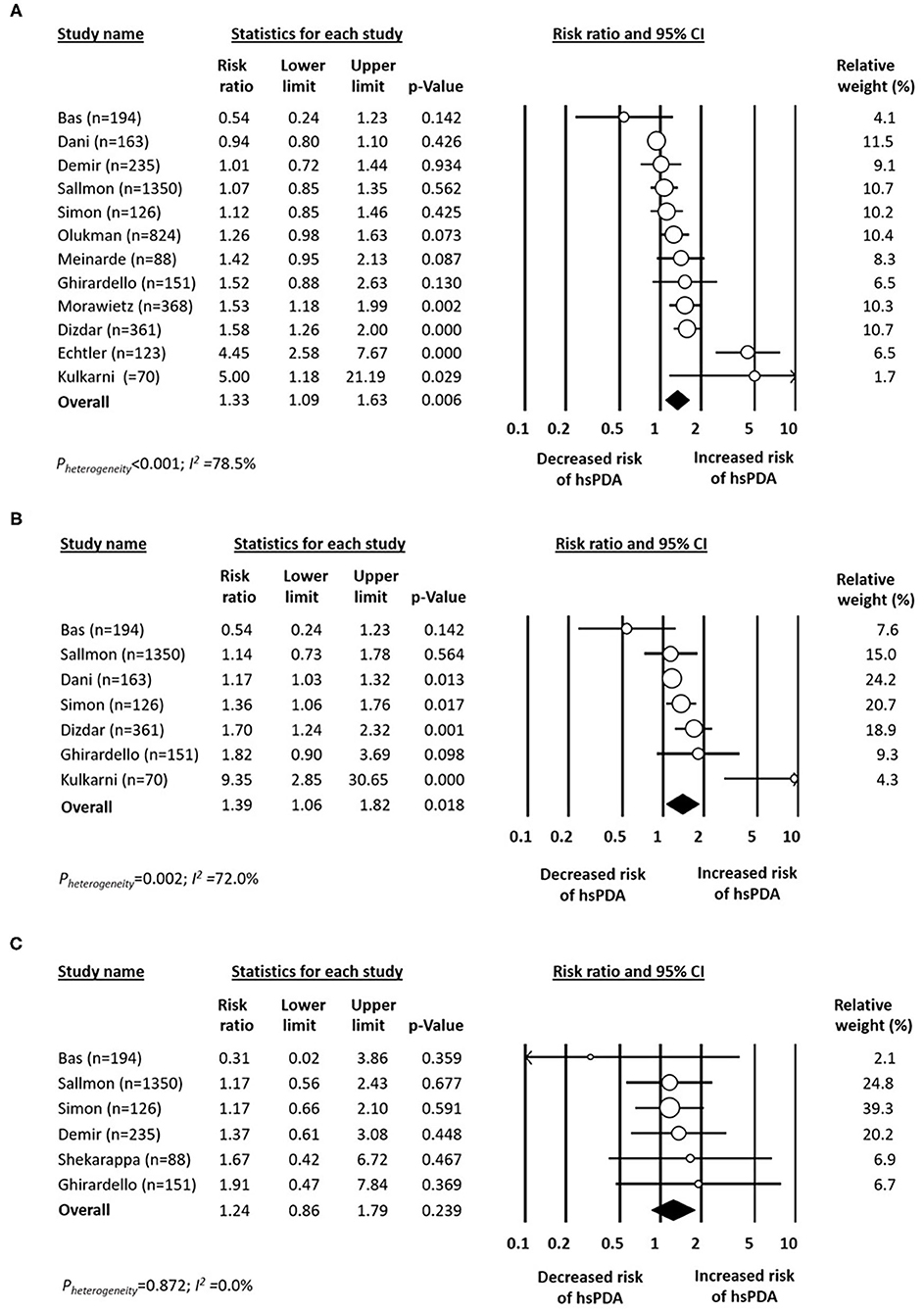
Figure 3. Forest plot for studies examining the association between platelet counts (A) below 150 × 109/L, (B) below 100 × 109/L, and (C) below 50 × 109/L in the first day(s) of life on hemodynamically significant patent ductus arteriosus (hsPDA). Risk ratio >1 indicates increased risk of hsPDA.
Data on rate of hsPDA in infants with platelet counts above or below 100 × 109/L were available from seven studies (12, 13, 16, 18, 19, 28, 32). There was a significant positive association between any PDA and platelet counts below 100 x 109/L (Figure 3B). Data on rate of hsPDA in infants with platelet counts above or below 50 × 109/L were available from six studies (16, 18, 19, 25, 28, 36). Meta-analysis could not detect a significant association between any PDA and platelet counts below 50 × 109/L (Figure 3C).
Mean (SD) platelet counts in infants with and without hsPDA were available from 19 studies (12, 13, 17–19, 22–31, 33, 35, 40, 41). Platelet counts were significantly higher in the group without hsPDA (Figure 2B). Neither visual inspection of the funnel plot (Supplementary Figure 2C) nor Egger's regression test (P = 0.941) revealed evidence of significant publication bias.
Data on mean MPV in infants with and without any hsPDA were available from 12 studies (22–27, 29–31, 35, 40). Meta-analysis could not demonstrate a significant difference in MPV mean between the two groups (Figure 4A). Neither visual inspection of the funnel plot (Supplementary Figure 2D) nor Egger's regression test (P = 0.678) revealed evidence of significant publication bias.
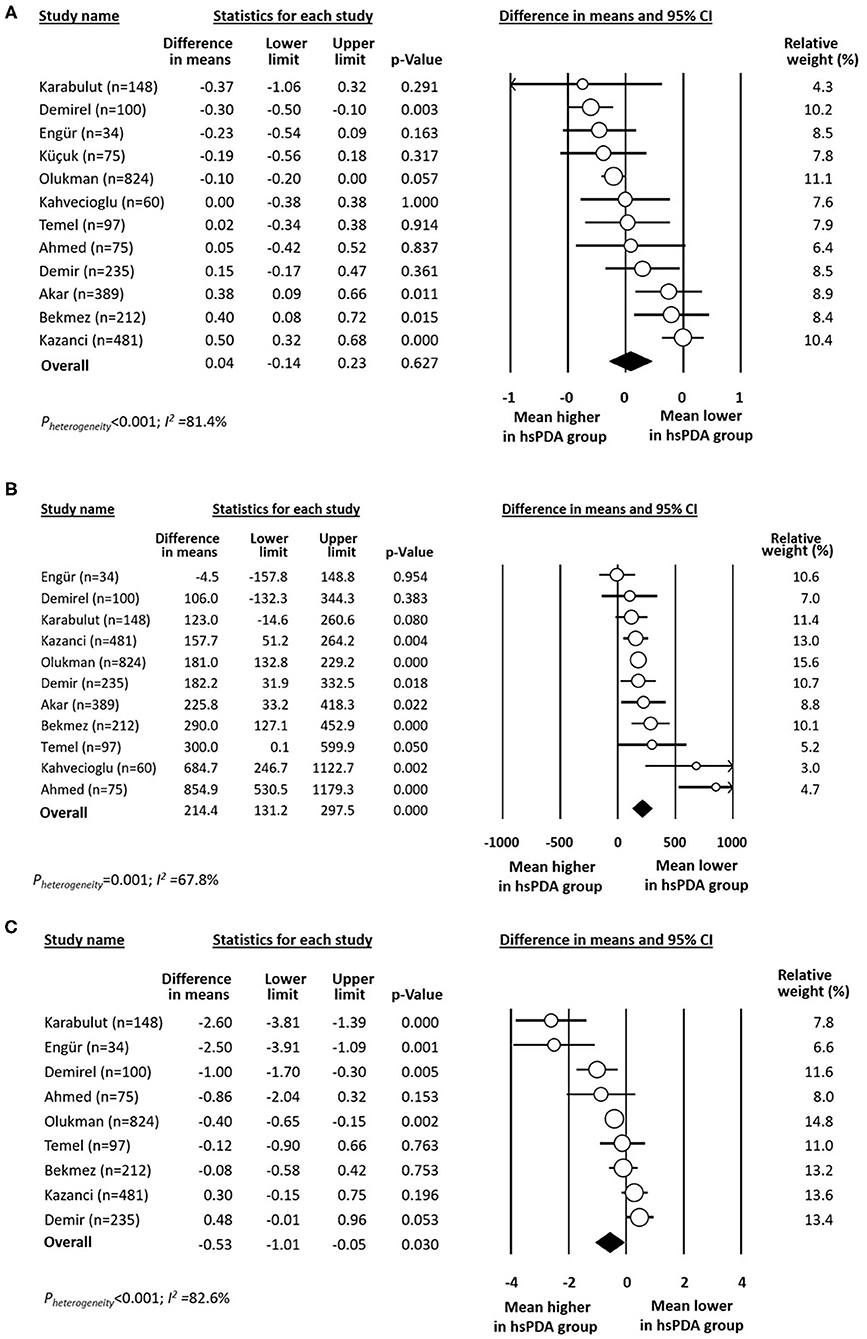
Figure 4. Forest plot for studies examining the difference (PDA-no minus PDA-yes) in (A) mean platelet volume (MPV), (B) platelet mass, and (C) platelet distribution width (PDW) in the first day(s) of life in infants with and without hemodynamically significant PDA (hsPDA).
Data on mean platelet mass in infants with and without any hsPDA were available from 11 studies (22–27, 29, 30, 35, 40, 41). Platelet mass was significantly higher in the group without hsPDA (Figure 4B). Neither visual inspection of the funnel plot (Supplementary Figure 2E) nor Egger's regression test (P = 0.212) revealed evidence of significant publication bias. Data on mean PDW in infants with and without any hsPDA were available from nine studies (22, 23, 25–27, 30, 35, 40, 41). Mean PDW was significantly lower in the hsPDA group (Figure 4C).
Meta-Regression Analyses
Potential sources of heterogeneity were assessed through random effects (method of moments) meta-regression analysis (46). Meta-regression was conducted only for the meta-analyses including 10 or more studies. The results of the meta-regression analyses are summarized in Supplementary Table 4. Meta-regression showed that the mean (or median) GA and BW of the cohort significantly correlated with the effect size of the association between any PDA and platelet counts <150 × 109/L (Supplementary Table 4 and Figure 2). The GA of the cohort was associated with 22% (R2 analog = 0.22) of the variance in the association between any PDA and platelet counts <150 × 109/L across studies. Each week that the GA of the cohort increased resulted in an increase in PDA log RR of 0.16 (the equivalent of going from a RR of 1.00 to a RR of 1.45). Similarly, the BW of the cohort was associated with 15% (R2 analog = 0.15) of the variance in the association between any PDA and platelet counts <150 × 109/L across studies. Each increment of 100 g in the BW of the cohort resulted in an increase in PDA log RR of 0.11 (the equivalent of going from a RR of 1.00 to a RR of 1.29).
Meta-regression also showed that the rate of hsPDA of the cohort significantly correlated with the effect size of the association between any hsPDA and platelet counts <150 × 109/L (Supplementary Table 4 and Figure 2). The hsPDA rate of the cohort was associated with 17% (R2 analog = 0.17) of the variance in the association between hsPDA and platelet counts <150 × 109/L across studies. Each 10% decrease in hsPDA rate resulted in an increase in hsPDA log RR of 0.12 (the equivalent of going from a RR of 1.00 to a RR of 1.32).
Discussion
This updated meta-analysis included 21 additional studies and doubled the number of infants, providing stronger evidence of the association between low platelet counts in the first day(s) of life and the risk of developing PDA or hsPDA. Besides low platelet counts, other platelet parameters such as platelet mass and PDW showed a significant association with hsPDA risk. Although the meta-analysis has gained in robustness with the increase in the number of studies and the inclusion of other platelet parameters, our results are still limited by the marked clinical and statistical heterogeneity among the different studies. In addition, the question that remains unanswered is to what extent the low number of platelets is an epiphenomenon associated with the maturity and clinical stability of preterm infants rather than a contributing factor in the pathogenesis of PDA (15).
As already discussed in the previous version of the meta-analysis, one of the main limitations for the study of the association between thrombocytopenia and PDA is the absence of uniform criteria to establish when these two entities have a clinical relevance (19). It has been argued that the definition of thrombocytopenia based on thresholds of 150 or even 100 × 109/L platelets is not clinically relevant for very preterm newborns (47, 48). In addition, neonatal thrombocytopenia and PDA share some potential etiopathogenic factors and this may confound the study of their potential association. The most frequent etiology of thrombocytopenia developing within the first days of life is intrauterine growth restriction (IUGR) and/or maternal hypertension (49, 50). This form of thrombocytopenia is rarely severe and platelet counts return to normal spontaneously in a short period of time (49, 50). The possible association between IUGR and PDA is controversial with studies reporting either a higher or lower risk of PDA in preterm infants with a history of IUGR (51). We analyzed this association in a recent meta-analysis (51). We observed a negative association between PDA and antenatal growth restriction (51). However, this association was only present in the meta-analysis pooling the studies that defined growth restriction as small for gestational age. The cohorts in which fetal growth assessment was conducted did not show a significant association with the risk of developing PDA (51). Therefore, the current evidence does not suggest that IUGR increases the incidence of PDA. Another pathological condition associated with both early-onset thrombocytopenia and PDA is perinatal infection (49, 50). Although individual studies and meta-analyses have shown an association between chorioamnionitis and PDA risk (52–54), this association was significantly biased by the lower GA of the group of infants exposed to chorioamnionitis (53). Nevertheless, neonatal sepsis is widely considered to be a major factor in the pathway leading from PDA to hsPDA (55).
Another important limitation of the previous (19) and present meta-analysis is the significant statistical heterogeneity observed in most of the analyses. We performed meta-regression analysis in order to investigate potential sources of heterogeneity. Meta-regression data suggest that the association between any PDA and platelet counts below 150 × 109/L correlated with the GA and BW of each cohort. That is, those studies that included children with higher GA and BW showed a stronger association between thrombocytopenia and PDA. However, this finding could not be confirmed in the other meta-regression analyses that we performed. The incidence of both PDA and hsPDA was highly variable across the different studies (see Table 1). This variability is probably a consequence of the lack of consensus on clinical or sonographic criteria to consider a ductal shunt as significant (1–10). Meta-regression showed that the association between hsPDA and low platelet counts (<150 × 109/L) was stronger in the studies with a lower rate of hsPDA. Nevertheless, our meta-regression results should be interpreted with caution. The minimum number of studies recommended to perform a meta-regression analysis is 10 (46). Our analyses were conducted in most cases with 10–11 studies but a higher number would have been necessary to obtain more reliable results.
Several investigators proposed that it is not the number of platelets but other quantitative or qualitative platelet parameters that are associated with a greater risk of developing PDA. Since large platelets are more reactive than small platelets, an elevated platelet size (i.e., a high MPV) is considered a marker of platelet activation (56, 57). Elevated MPV has been associated with cardiovascular disease in adults (58) and several studies have analyzed the association between MPV and complications of prematurity such as bronchopulmonary dysplasia, sepsis, intraventricular hemorrhage, retinopathy of prematurity, or PDA (59–63). Nevertheless, our meta-analysis could not demonstrate an association between MPV and hsPDA (Figure 4). In contrast, the platelet mass was significantly lower in the group of infants with hsPDA. The platelet mass and the plateletcrit are calculations obtained by multiplying the MPV by the platelet count (44, 45). For example, a platelet count of 100 × 109/L and a MPV of 10 fL would equate to a platelet mass of 1,000 (45). Since in the mathematical formula the platelet count has a factor of hundreds while the MPV has a factor of tens, the former will have a weight 10 times greater than the latter in the final value of the platelet mass. Therefore, our findings regarding the association of platelet mass with hsPDA may be only a repetition of the findings on the association of platelet counts and risk of hsPDA.
As mentioned above, large platelets are considered to be metabolically and enzymatically more active than small platelets. PDW reflects the variability in the platelet size and its increase is considered as a sign of platelet activation (56, 57). According to the hypothesis of the role of platelets in DA closure, a higher degree of platelet activation, and therefore a higher PDW, would be expected in the infants without PDA. However, our meta-analysis shows that infants with hsPDA have higher PDW values than infants without the condition. The heterogeneity of this meta-analysis was very high and the included studies showed either increased or reduced PDW in the hsPDA group. In addition, high PDW and MPV have been proposed as useful markers to distinguish thrombocytopenia associated with sepsis from other etiologies (56). Thus again, the etiology of thrombocytopenia (i.e., sepsis vs. IUGR) may be the factor leading to the differences in results of the studies addressing the association between platelet parameters and PDA.
The hypothesis that the important risk factor for PDA is altered platelet function, not decreased platelet number, has also been investigated. Unfortunately, the low number of studies that included information on this topic did not allow us to pool them in a meta-analysis. Immature platelets may have different functional features when compared to mature platelets (64). Sallmon et al. investigated the immature platelet fraction in a cohort of infants with and without hsPDA (64). Although higher immature platelet fraction values were associated with hsPDA, logistic regression analysis revealed that only mature platelet counts on postnatal day 7 were independently associated with the condition (64). Ghirardello et al. investigated thromboelastographic, a technique for bedside hemostatic assessment, in preterm infants with and without hsPDA (28). They could not demonstrate significant differences in thromboelastographic profile in children having hsPDA, or in those who failed pharmacological treatment, compared to their respective controls (28). Engur et al. (27) and Ahmed et al. (23) reported significant lower levels of platelet derived growth factor in the first days of life in preterm infants developing hsPDA. Finally, Kahvecioglou et al. reported that a higher collagen-ADP duration was an independent risk factor for hsPDA. All these findings need to be confirmed in future studies.
It is still unclear which long-term benefits or harms are achieved by treating a PDA (1–9). The attitude of neonatologists toward PDA has progressively changed in the last years from advocating widespread treatment to close the PDA to a call for watchful observation (1–9). Although our meta-analysis focused on the effect of thrombocytopenia on “spontaneous” DA closure, we must take into account that rate of PDA closure may have been affected by the variations in the management of PDA among centers (8, 9). In a recent meta-analysis, Mitra et al. reported that low platelet counts were associated with higher odds of failure to PDA treatment with ibuprofen or indomethacin (65). Therefore, taking together the results of the meta-analysis of Mitra et al. and the present one, the evidence points to an association between low platelet counts and the presence of PDA as well as the lack of response to pharmacological treatment. Nevertheless, association does not mean causation.
Besides the observational studies on the association between platelet counts and PDA, the potential effect of platelet transfusion on DA closure has been investigated in two randomized controlled trials (RCTs). Andrew et al. compared two platelet count thresholds for prophylactic platelet transfusion (150 × 109/L vs. 50 × 109/L) (66). The incidence of either the primary outcome, intraventricular hemorrhage, or PDA, which was one of the secondary outcomes, was not significantly different between the two thresholds. (66). Very recently, Kumar et al. conducted a RCT with PDA as primary outcome and prophylactic transfusion thresholds of 100 × 109/L vs. 20 × 109/L platelets (67). This RCT could not demonstrate any positive effect of the higher threshold on DA closure. Interestingly, the group of infants in the higher threshold had a higher incidence of intraventricular hemorrhage (67). As reviewed by Fustolo-Gunnink et al., results from several studies suggest that platelet transfusions do not reduce bleeding risk of preterm infants, and even might increase it (68). Moreover, a recent RCT, which included 660 preterm infants (GA < 34 weeks), reported a risk reduction of major bleeding and/or mortality in neonates assigned to a prophylactic platelet transfusion threshold of 25 × 109/L vs. a threshold of 50 × 109/L. These results have led to a revision of the criteria and guidelines for platelet transfusion in very preterm infants to be more restrictive (68–70). Altogether, the current evidence suggests that increasing platelet counts by transfusion to hypothetically accelerate DA closure may generate more harm than benefit.
In conclusion, the present updated meta-analysis provides stronger evidence of the association between low platelet counts in the first day(s) of life and risk of developing PDA and hsPDA. Identifying simple markers of platelet function may improve our diagnostic and therapeutic decisions in dealing with PDA or other neonatal conditions. However, due to the complexities involved with the pathogenesis of both neonatal thrombocytopenia and PDA, it is impossible to establish a cause-and-effect relationship between the two conditions. In fact, studies that have attempted to correct the thrombocytopenia through platelet transfusions have not only failed to alter the incidence of PDA, but also have even led to increased morbidity (67).
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
GG-L carried out the systematic search, selected studies for inclusion, extracted study data, contributed to statistical analyses, interpretation of results, and drafting of the manuscript. SG supervised study inclusion and data collection, contributed to interpretation of results, and reviewed and revised the manuscript. PB-S contributed to search and data collection, contributed to interpretation of results, and reviewed and revised the manuscript. GC supervised study inclusion and data collection, contributed to interpretation of results, and reviewed and revised the manuscript. FM and RC contributed to interpretation of results, and reviewed and revised the manuscript. EV conceptualized the study, carried out the systematic search, selected studies for inclusion, extracted study data, carried out the statistical analyses and interpretation of results, and drafted the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was partially supported by a grant from the Fundación Canaria del Colegio de Médicos de Las Palmas.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank I. Morioka, E. A. Dizdar, and C. Dani for kindly providing additional data and clarifications of their studies.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.613766/full#supplementary-material
References
1. Hundscheid T, Onland W, Van Overmeire B, Dijk P, van Kaam AH, Dijkman KP, et al. Early treatment versus expectative management of patent ductus arteriosus in preterm infants: a multicentre, randomised, non-inferiority trial in Europe (BeNeDuctus trial). BMC Pediatrics. (2018) 18:262. doi: 10.1186/s12887-018-1215-7
2. Smith A, EL-Khuffash AF. Defining “haemodynamic significance” of the patent ductus arteriosus: do we have all the answers? Neonatology. (2020) 117:1–8. doi: 10.1159/000506988
3. Mitra S, McNamara PJ. Patent ductus arteriosus—time for a definitive trial. Clin Perinatol. (2020) 47:617–39. doi: 10.1016/j.clp.2020.05.007
4. Reese J, Laughon MM. The patent ductus arteriosus problem: infants who still need treatment. J Pediatr. (2015) 167:954–6. doi: 10.1016/j.jpeds.2015.08.023
5. Clyman RI, Liebowitz M, Kaempf J, Erdeve O, Bulbul A, Håkansson S, et al. PDA-TOLERATE trial: an exploratory randomized controlled trial of treatment of moderate-to-large patent ductus arteriosus at 1 week of age. J Pediatr. (2019) 205:41–8. e6. doi: 10.1016/j.jpeds.2018.09.012
6. Sallmon H, Koehne P, Hansmann G. Recent advances in the treatment of preterm newborn infants with patent ductus arteriosus. Clin Perinatol. (2016) 43:113–29. doi: 10.1016/j.clp.2015.11.008
7. Clyman RI, Benitz WE. Transcatheter patent ductus arteriosus closure—will history repeat itself? J Perinatol. (2019) 39:1435–6. doi: 10.1038/s41372-019-0483-x
8. de Klerk J, Engbers A, van Beek F, Flint RB, Reiss I, Völler S, et al. Spontaneous closure of the ductus arteriosus in preterm infants: a systematic review. Front Pediatr. (2020) 8:541. doi: 10.3389/fped.2020.00541
9. Okulu E, Erdeve O, Arslan Z, Demirel N, Kaya H, Gokce IK, et al. An observational, prospective, multicenter, registry-based cohort study comparing conservative and medical management for patent ductus arteriosus. Front Pediatr. (2020) 8:434. doi: 10.3389/fped.2020.00434
10. Hamrick SE, Sallmon H, Rose AT, Porras D, Shelton EL, Reese J, et al. Patent ductus arteriosus of the preterm infant. Pediatrics. (2020) 146:e20201209. doi: 10.1542/peds.2020-1209
11. Echtler K, Stark K, Lorenz M, Kerstan S, Walch A, Jennen L, et al. Platelets contribute to postnatal occlusion of the ductus arteriosus. Nat Med. (2010) 16:75–82. doi: 10.1038/nm.2060
12. Dizdar AE, Ozdemir R, Nur Sari F, Yurttutan S, Gokmen T, Erdeve O, et al. Low platelet count is associated with ductus arteriosus patency in preterm newborns. Early Hum Dev. (2012) 88:813–6. doi: 10.1016/j.earlhumdev.2012.05.007
13. Dani C, Poggi C, Fontanelli G. Relationship between platelet count and volume and spontaneous and pharmacological closure of ductus arteriosus in preterm infants. Am J Perinatol. (2013) 30:359–64. doi: 10.1055/s-0032-1324702
14. Fujioka K, Morioka I, Miwa A, Morikawa S, Shibata A, Yokoyama N, et al. Does thrombocytopenia contribute to patent ductus arteriosus? Nat Med. (2011) 17:29–30. doi: 10.1038/nm0111-29
15. Shah NA, Hills NK, Waleh N, McCurnin D, Seidner S, Chemtob S, et al. Relationship between circulating platelet counts and ductus arteriosus patency after indomethacin treatment. J Pediatr. (2011) 158:919–23. e1–2. doi: 10.1016/j.jpeds.2010.11.018
16. Sallmon H, Weber SC, Huning B, Stein A, Horn PA, Metze BC, et al. Thrombocytopenia in the first 24 hours after birth and incidence of patent ductus arteriosus. Pediatrics. (2012) 130:e623–30. doi: 10.1542/peds.2012-0499
17. Chen YY, Wang HP, Chang JT, Chiou YH, Huang YF, Hsieh KS, et al. Perinatal factors in patent ductus arteriosus in very low-birthweight infants. Pediatr Int. (2014) 56:72–6. doi: 10.1111/ped.12199
18. Bas-Suarez MP, Gonzalez-Luis GE, Saavedra P, Villamor E. Platelet counts in the first seven days of life and patent ductus arteriosus in preterm very low-birth-weight infants. Neonatology. (2014) 106:188–94. doi: 10.1159/000362432
19. Simon SR, van Zogchel L, Bas-Suárez MP, Cavallaro G, Clyman RI, Villamor E. Platelet counts and patent ductus arteriosus in preterm infants: a systematic review and meta-analysis. Neonatology. (2015) 108:143–51. doi: 10.1159/000431281
20. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. (2019). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed May 15, 2020).
21. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
22. Temel M, Coskun M, Akbayram S, Demiryürek A. Association between neutrophil/lymphocyte ratio with ductus arteriosus patency in preterm newborns. Bratisl Lek Listy. (2017) 118:491–4. doi: 10.4149/BLL_2017_094
23. Ahmed EG, Samra NM, Amin SA, Borayek HA, Abdelrazek G. Platelets and platelet derived growth factor and ductus arteriosus in preterm neonates. Prog Pediatr Cardiol. (2020) 57:101226. doi: 10.1016/j.ppedcard.2020.101226
24. Akar S, Topcuoglu S, Tuten A, Ozalkaya E, Karatepe HO, Gokmen T, et al. Is the first postnatal platelet mass as an indicator of patent ductus arteriosus? Arch Iran Med. (2019) 22:687–91.
25. Demir N, Peker E, Ece I, Agengin K, Bulan KA, Tuncer O. Is platelet mass a more significant indicator than platelet count of closure of patent ductus arteriosus? J Matern Fetal Neonatal Med. (2016) 29:1915–8. doi: 10.3109/14767058.2015.1067296
26. Demirel G, Yilmaz A, Vatansever B, Tastekin A. Is high platelet distribution width in the first hours of life can predict hemodynamically significant patent ductus arteriosus in preterm newborns? J Matern Fetal Neonatal Med. (2020) 33:2049–53. doi: 10.1080/14767058.2018.1536743
27. Engür D, Kaynak-Türkmen M, Deveci M, Yenisey Ç. Platelets and platelet-derived growth factor in closure of the ductus arteriosus. Turk J Pediatr. (2015) 57:242–7.
28. Ghirardello S, Raffaeli G, Crippa BL, Gulden S, Amodeo I, Consonni D, et al. The thromboelastographic profile at birth in very preterm newborns with patent ductus arteriosus. Neonatology. (2020) 117:1–8. doi: 10.1159/000507553
29. Kahvecioglu D, Erdeve O, Akduman H, Ucar T, Alan S, Çakir U, et al. Influence of platelet count, platelet mass index, and platelet function on the spontaneous closure of ductus arteriosus in the prematurity. Pediatr Neonatol. (2018) 59:53–7. doi: 10.1016/j.pedneo.2017.01.006
30. Karabulut B, Arcagök BC, Simsek A. Utility of the platelet-to-lymphocyte ratio in diagnosing and predicting treatment success in preterm neonates with patent ductus arteriosus. Fetal Pediatr Pathol. (2019) 38:1–10. doi: 10.1080/15513815.2019.1686786
31. Küçük M, Bagci O, Igde M. The fate of patent ductus arteriosus is not affected by platelet count and mean platelet volume in premature infants <32 gestational weeks. Turkiye Klinikleri Cardiovascular Sciences. (2018) 30:53–7. doi: 10.5336/cardiosci.2018-62380
32. Kulkarni VV, Dutta S, Sundaram V, Saini SS. Preterm thrombocytopenia and delay of ductus arteriosus closure. Pediatrics. (2016) 138:e20161627. doi: 10.1542/peds.2016-1627
33. Meinarde L, Hillman M, Rizzotti A, Basquiera AL, Tabares A, Cuestas E. C-reactive protein, platelets, and patent ductus arteriosus. Platelets. (2016) 27:821–3. doi: 10.1080/09537104.2016.1203398
34. Morawietz S. Korrelation eines hämodynamisch relevanten persistierenden Ductus arteriosus mit einer Thrombozytopenie in den ersten zehn Lebenstagen sowie die Auswirkungen einer Thrombozytopenie auf das Outcome einer Behandlung mit NSAID. Munich: Lmu (2016).
35. Olukman O, Ozdemir R, Karadeniz C, Calkavur S, Mese T, Vergin C. Is there a relationship between platelet parameters and patency of ductus arteriosus in preterm infants? Blood Coagul Fibrinolysis. (2017) 28:8–13. doi: 10.1097/MBC.0000000000000520
36. Shekharappa CB, Elizabeth EAB, Balachander B. Association of patent ductus arteriosus size with clinical features and short-term outcomes in preterm infants less than 34 weeks. Indian J Child Health. (2020) 7:105–8. doi: 10.32677/IJCH.2020.v07.i03.003
37. Kusuma AAMW, Gunawijaya E, Putra IGNS, Yantie NPVK, Kardana IM, Utama IMGDL, et al. Risk factors of patent ductus arteriosus in preterm. Am J Pediatr. (2020) 6:168–72. doi: 10.11648/j.ajp.20200602.29
38. Oliveira A, Soares P, Flor-de-Lima F, Neves ALs, Guimarães Hl. PDA management in VLBW infants: experience of a level III NICU. J Pediatr Neonat Individ Med (JPNIM). (2016) 5:e050227. doi: 10.7363/050227
39. Saldaña-Díaz CV, Roque-Quezada JCE, Saldaña-Montes SP, De-la-Cruz-Vargas J. Trombocitopenia como indicador predictivo de cierre deficitario de ductus arterioso en prematuros del Instituto Nacional Materno Perinatal. Revista Peruana de Investigación Materno Perinatal. (2019) 8:21–6. doi: 10.33421/inmp.2019150
40. Kazanci EG, Buyuktiryaki M, Unsal H, Tayman C. Useful platelet indices for the diagnosis and follow-up of patent ductus arteriosus. Am J Perinatol. (2019) 36:1521–7. doi: 10.1055/s-0039-1688821
41. Özer Bekmez B, Tayman C, Büyüktiryaki M, Çetinkaya AK, Çakir U, Derme T. A promising, novel index in the diagnosis and follow-up of patent ductus arteriosus: red cell distribution width-to-platelet ratio. J Clin Lab Anal. (2018) 32:e22616. doi: 10.1002/jcla.22616
42. Dwarakanath K, Dereddy N, Chabra D, Schabacker C, Calo J, Parton L. Spontaneous and pharmacological closure of PDAs in ELBW infants is influenced by thrombocyto-penia (abstract). E-PAS 21. (2011).
43. Brunner B, Hoeck M, Schermer E, Streif W, Kiechl-Kohlendorfer U. Patent ductus arteriosus, low platelets, cyclooxygenase inhibitors, and intraventricular hemorrhage in very low birth weight preterm infants. J Pediatr. (2013) 163:23–8. doi: 10.1016/j.jpeds.2012.12.035
44. Kanda H, Yamakuchi M, Mastumoto K, Mukaihara K, Shigehisa Y, Tachioka S, et al. Dynamic changes in platelets caused by shear stress in aortic valve stenosis. Clin Hemorheol Microcirc. (2020). doi: 10.3233/CH-200928. [Epub ahead of print].
45. Christensen RD. Platelet transfusion in the neonatal intensive care unit: benefits, risks, alternatives. Neonatology. (2011) 100:311–8. doi: 10.1159/000329925
46. Borenstein M, Hedges LV, Higgins JPT, Rothstein HR (editors). Meta-regression. In: Introduction to Meta-Analysis. Sussex: John Wiley & Sons (2009). p. 187–203.
47. Chakravorty S, Roberts I. How I manage neonatal thrombocytopenia. Br J Haematol. (2012) 156:155–62. doi: 10.1111/j.1365-2141.2011.08892.x
48. Sola-Visner M. Platelets in the neonatal period: developmental differences in platelet production, function, and hemostasis and the potential impact of therapies. Hematology Am Soc Hematol Educ Program. (2012) 2012:506–11. doi: 10.1182/asheducation.V2012.1.506.3798532
49. Beiner ME, Simchen MJ, Sivan E, Chetrit A, Kuint J, Schiff E. Risk factors for neonatal thrombocytopenia in preterm infants. Am J Perinatol. (2003) 20:049–54. doi: 10.1055/s-2003-37948
50. Roberts I, Murray NA, editors. Neonatal thrombocytopenia. Seminars in Fetal And Neonatal Medicine. Elsevier (2008).
51. Villamor-Martinez E, Kilani MA, Degraeuwe PL, Clyman RI, Villamor E. Intrauterine growth restriction and patent ductus arteriosus in very and extremely preterm infants: a systematic review and meta-analysis. Front Endocrinol. (2019) 10:58. doi: 10.3389/fendo.2019.00058
52. Park HW, Choi Y-S, Kim KS, Kim S-N. Chorioamnionitis and patent ductus arteriosus: a systematic review and meta-analysis. PLoS ONE. (2015) 10:e0138114. doi: 10.1371/journal.pone.0138114
53. Behbodi E, Villamor-Martínez E, Degraeuwe PL, Villamor E. Chorioamnionitis appears not to be a risk factor for patent ductus arteriosus in preterm infants: a systematic review and meta-analysis. Sci Rep. (2016) 6:37967. doi: 10.1038/srep37967
54. Green CA, Westreich D, Laughon MM, Stamilio DM, Strauss RA, Reese J, et al. Association of chorioamnionitis and patent ductus arteriosus in a national US cohort. J Perinatol. (2020). doi: 10.1038/s41372-020-00866-x. [Epub ahead of print].
55. Vucovich MM, Cotton RB, Shelton EL, Goettel JA, Ehinger NJ, Poole SD, et al. Aminoglycoside-mediated relaxation of the ductus arteriosus in sepsis-associated PDA. Am J Physiol Heart Circ Physiol. (2014) 307:H732–40. doi: 10.1152/ajpheart.00838.2013
56. Kim JY, Yoon J, Lim CS, Choi BM, Yoon S-Y. Clinical significance of platelet-associated hematological parameters as an early supplementary diagnostic tool for sepsis in thrombocytopenic very-low-birth-weight infants. Platelets. (2015) 26:620–6. doi: 10.3109/09537104.2014.963542
57. Kannar V, Deepthi A, Kumar MLH, Junjegowda K, Mariyappa N. Effect of gestational age, prematurity and birth asphyxia on platelet indices in neonates. J Clin Neonatol. (2014) 3:144. doi: 10.4103/2249-4847.140399
58. Chu S, Becker R, Berger P, Bhatt D, Eikelboom J, Konkle B, et al. Mean platelet volume as a predictor of cardiovascular risk: a systematic review and meta-analysis. J Thromb Haemost. (2010) 8:148–56. doi: 10.1111/j.1538-7836.2009.03584.x
59. Go H, Ohto H, Nollet KE, Takano S, Kashiwabara N, Chishiki M, et al. Using platelet parameters to anticipate morbidity and mortality among preterm neonates: a retrospective study. Front Pediatr. (2020) 8:90. doi: 10.3389/fped.2020.00090
60. Tao Y, Dong Y, Lu C-w, Yang W. Mean platelet volume in retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. (2015) 253:2047–8. doi: 10.1007/s00417-015-3047-6
61. Dani C, Poggi C, Barp J, Berti E, Fontanelli G. Mean platelet volume and risk of bronchopulmonary dysplasia and intraventricular hemorrhage in extremely preterm infants. Am J Perinatol. (2011) 28:551–6. doi: 10.1055/s-0031-1274503
62. Grevsen AK, Hviid CV, Hansen AK, Hvas A-M, editors. The role of platelets in premature neonates with intraventricular hemorrhage: a systematic review and meta-analysis. Semin Thromb Hemost. (2020) 46:366–78. doi: 10.1055/s-0039-3402687
63. Wang J, Wang Z, Zhang M, Lou Z, Deng J, Li Q. Diagnostic value of mean platelet volume for neonatal sepsis: A systematic review and meta-analysis. Medicine. (2020) 99:e21649. doi: 10.1097/MD.0000000000021649
64. Sallmon H, Metze B, Koehne P, Opgen-Rhein B, Weiss K, Will JC, et al. Mature and immature platelets during the first week after birth and incidence of patent ductus arteriosus. Cardiol Young. (2020) 30:1–5. doi: 10.1017/S1047951120000943
65. Mitra S, Chan AK, Paes BA, Thrombosis, Group HiN. The association of platelets with failed patent ductus arteriosus closure after a primary course of indomethacin or ibuprofen: a systematic review and meta-analysis. J Matern-Fetal Neonat Med. (2017) 30:127–33. doi: 10.3109/14767058.2016.1163684
66. Andrew M, Vegh P, Caco C, Kirpalani H, Jefferies A, Ohlsson A, et al. A randomized, controlled trial of platelet transfusions in thrombocytopenic premature infants. J Pediatr. (1993) 123:285–91. doi: 10.1016/S0022-3476(05)81705-6
67. Kumar J, Dutta S, Sundaram V, Saini SS, Sharma RR, Varma N. Platelet transfusion for PDA closure in preterm infants: a randomized controlled trial. Pediatrics. (2019) 143:e20182565. doi: 10.1542/peds.2018-2565
68. Fustolo-Gunnink S, Huisman E, van der Bom J, van Hout F, Makineli S, Lopriore E, et al. Are thrombocytopenia and platelet transfusions associated with major bleeding in preterm neonates? A systematic review. Blood Rev. (2019) 36:1–9. doi: 10.1016/j.blre.2018.10.001
69. Fustolo-Gunnink SF, Fijnvandraat K, van Klaveren D, Stanworth SJ, Curley A, Onland W, et al. Preterm neonates benefit from low prophylactic platelet transfusion threshold despite varying risk of bleeding or death. Blood. (2019) 134:2354–60. doi: 10.1182/blood.2019000899
Keywords: ductus arteriosus, platelets, meta-analysis, platelet distribution width, thrombocytopenia
Citation: González-Luis G, Ghirardello S, Bas-Suárez P, Cavallaro G, Mosca F, Clyman RI and Villamor E (2021) Platelet Counts and Patent Ductus Arteriosus in Preterm Infants: An Updated Systematic Review and Meta-Analysis. Front. Pediatr. 8:613766. doi: 10.3389/fped.2020.613766
Received: 03 October 2020; Accepted: 21 December 2020;
Published: 20 January 2021.
Edited by:
Yogen Singh, Cambridge University Hospitals NHS Foundation Trust, United KingdomReviewed by:
Ömer Erdeve, Ankara University, TurkeyHannes Sallmon, Charité – Universitätsmedizin Berlin, Germany
Samir Gupta, Durham University, United Kingdom
Copyright © 2021 González-Luis, Ghirardello, Bas-Suárez, Cavallaro, Mosca, Clyman and Villamor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Villamor, ZS52aWxsYW1vckBtdW1jLm5s