
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr., 05 January 2021
Sec. Pediatric Rheumatology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.594127
This article is part of the Research TopicClinical Heterogeneity, Immunological Features, and Health Impact of the COVID-19 Pandemic in ChildrenView all 30 articles
 Athina Fouriki1,2*
Athina Fouriki1,2* Yves Fougère3
Yves Fougère3 Caroline De Camaret1,2
Caroline De Camaret1,2 Géraldine Blanchard Rohner4
Géraldine Blanchard Rohner4 Serge Grazioli5
Serge Grazioli5 Noémie Wagner6
Noémie Wagner6 Christa Relly7
Christa Relly7 Jana Pachlopnik Schmid8
Jana Pachlopnik Schmid8 Johannes Trück7,8Lisa Kottanatu9
Johannes Trück7,8Lisa Kottanatu9 Estefania Perez10
Estefania Perez10 Marie-Helene Perez11
Marie-Helene Perez11 Damien Schaffner12
Damien Schaffner12 Sandra Andrea Asner3†
Sandra Andrea Asner3† Michael Hofer1,2†
Michael Hofer1,2†Since the beginning of the severe SARS-CoV-2 pandemic, an increasing number of countries reported cases of a systemic hyperinflammatory condition defined as multi-system inflammatory syndrome in children (MIS-C). The clinical features of MIS-C can be an overlap of Kawasaki Disease (KD), Toxic Shock Syndrome (TSS), Macrophage Activation Syndrome (MAS), or have often an acute abdominal presentation. Intravenous immunoglobulin (IVIG) is recommended as first line therapy in KD. Recent evidence suggests intravenous immunoglobulins (IVIG) resistance in some cases of SARS-CoV-2 related MIS-C, thereby questioning the benefit of immunomodulators such as IL-1 or IL-6 blocking agents. We report on a cohort of 6 Swiss children with SARS-CoV2 related MIS-C presenting with clinical features compatible with Incomplete KD and Toxic Shock Syndrome associated to a cytokine storm. Serum cytokine profile investigations showed increased IL1RA levels (8 to 22-fold) in 5 of the 6 patients (one patient had not been tested), whereas, IL-6 serum levels were increased only in the 3 patients of the 6 who were tested. With exception of one patient who had only benefited by Anakinra, all patients received at least one dose of IVIG. One patient has only received Anakinra with favorable evolution, and three patients had also a steroid treatment. In addition to all this anti-inflammatory medication two patients have also received one dose of anti-IL6. In conclusion, our case series reports on clinical and laboratory findings of most of Swiss cases with MIS-C and suggests the use of Anakinra as an alternative to steroids in these children, most of whom presented with high IL-1RA levels.
Since the beginning of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, an increasing number of countries reported cases of a systemic hyperinflammatory condition defined as multi-system inflammatory syndrome in children (MIS-C). This hyperinflammatory condition has also been termed as pediatric multisystem inflammatory syndrome (PIMS), pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIM-TS), pediatric hyperinflammatory syndrome, or pediatric hyperinflammatory shock (1–3). Initially published case series from France (4), New-York (5), and England (6) included 35, 33, and 58 children, respectively, whereas further cases are being published (7, 8). Clinical description revealed from 13 of the 30 British children aged between 4 and 14 years referred to either warm vasoplegic shock or acute abdominal and sepsis-like presentations (2). Italian data published on May 2020 described incomplete Kawasaki Disease-like presentations in 5 of their 10 children aged between 3-16 years of age, six of these ten patients presented with coronary inflammation and aneurysms (7). Common observations delineated from this MIS-C referred to overlapping clinical features of Kawasaki Disease (KD), Toxic Shock Syndrome, and Macrophage Activation Syndrome with acute abdominal presentations upon admission (1, 2, 9–13). While intravenous immunoglobulin (IVIG) is recommended as first line therapy and is successfully used in KD, some refractory cases may benefit from treatment with an interleukin-1 receptor antagonist (Anakinra). Recent evidence suggests IVIG resistance in some cases of SARS-CoV-2 related MIS-C, thereby questioning the benefit of immunomodulators such as IL-1 or IL-6 blocking agents (7, 14). Switzerland reported over 31,000 persons detected positive to SARS-CoV-2, 3.2% were children (0-18 years old) (15). From these, 9 children had MIS-C and documented SARS-CoV-2 infection by PCR or serologies. We describe the clinical characteristics, laboratory data and treatment management of the collected 6 of these 9 Swiss children with MIS-C, the remaining 3 have already been reported in another paper (16).
Our clinical study is a case series that includes all eligible patients identified during the study registration period (consecutive, formal). It describes the experience on a small group of patients (observational, descriptive research design), contains demographic information about them and was conducted retrospectively. The patients were treated in the order in which they were identified, without a group control.
All patients with a positive serology for SARS-CoV2 (IgG serology) and symptoms, signs, and laboratory markers in favor of a systemic hyperinflammatory condition. The patients were identified by their severe clinical presentation with need of hospitalization, the increased laboratory inflammatory markers and their positivity for SARS-CoV2.
Patients with evidence of a hyperinflammatory state having negative serology for SARS-CoV2 and negative nasopharyngeal smear. Patients whose clinical presentation had already been published in another study, by the hospital center that followed them. One patient whose parents did not sign the consent about the publication.
Four hospitals of Switzerland participated in this study, including the University Hospital of Lausanne (CHUV), of Geneva (HUG), of Zurich (USZ) and the Regional Hospital of Bellinzona.
The parents of all patients included in our study were informed about the management of these hyperinflammatory conditions, including the different treatments. They signed a consent form for the participation of their children in the publication and about their medium and long-term follow-up.
The quantification of cytokines was made by a commercially available multiplex beads immunoassay, based on the Luminex platform (Magnetic Luminex® Performance Assay, R&D Systems, Minneapolis, USA) according to supplier's instructions. Briefly, beads conjugated to the analyte-specific capture antibodies, samples, standards and controls, were incubated at room temperature for 3 h. Biotinylated detector antibodies and R-phycoerythrin–conjugated streptavidin (SAPE) were subsequently added. The mean fluorescence intensity of each analyte was read on the Bio-Plex 200 array reader (Bio-Rad Laboratories) using the Luminex xMAP Technology (Luminex Corporation). Sample concentrations were calculated using a five-parameter logistic regression curve (Bio-Plex Manager 6.0). Interassay variation coefficients were monitored using internal controls. These were below 15% for all (17).
Table 1 displays clinical characteristics, laboratory and imaging findings as well as treatments of all patients. Five of the 6 patients were males, with a median age of 10.5 years (Interquartile Range (IQR): 8.5-11 years). None presented any co-morbidity. Four patients were Caucasian, 1 African, and 1 Afro-Caucasian. None of the patients presented respiratory symptoms or fever suggestive of COVID-19 in the weeks (4–6 weeks) preceding their admission. However, family members from patient 1 and 2 presented respiratory symptoms consistent with COVID-19, a month prior to hospital admission, some family members of patient 4 had anosmia and mild respiratory symptoms three weeks prior to admission. SARS-CoV-2 was documented by real time (RT-PCR) collected from nasopharyngeal swabs (NPS) in 5 of the 6 patients. The PCR threshold cycle (TC) were >35 for E and N2 genes in patients 1 to 3, thereby supporting a low viral load. All patients presented a positive IgG serology (Roche serology) (18).
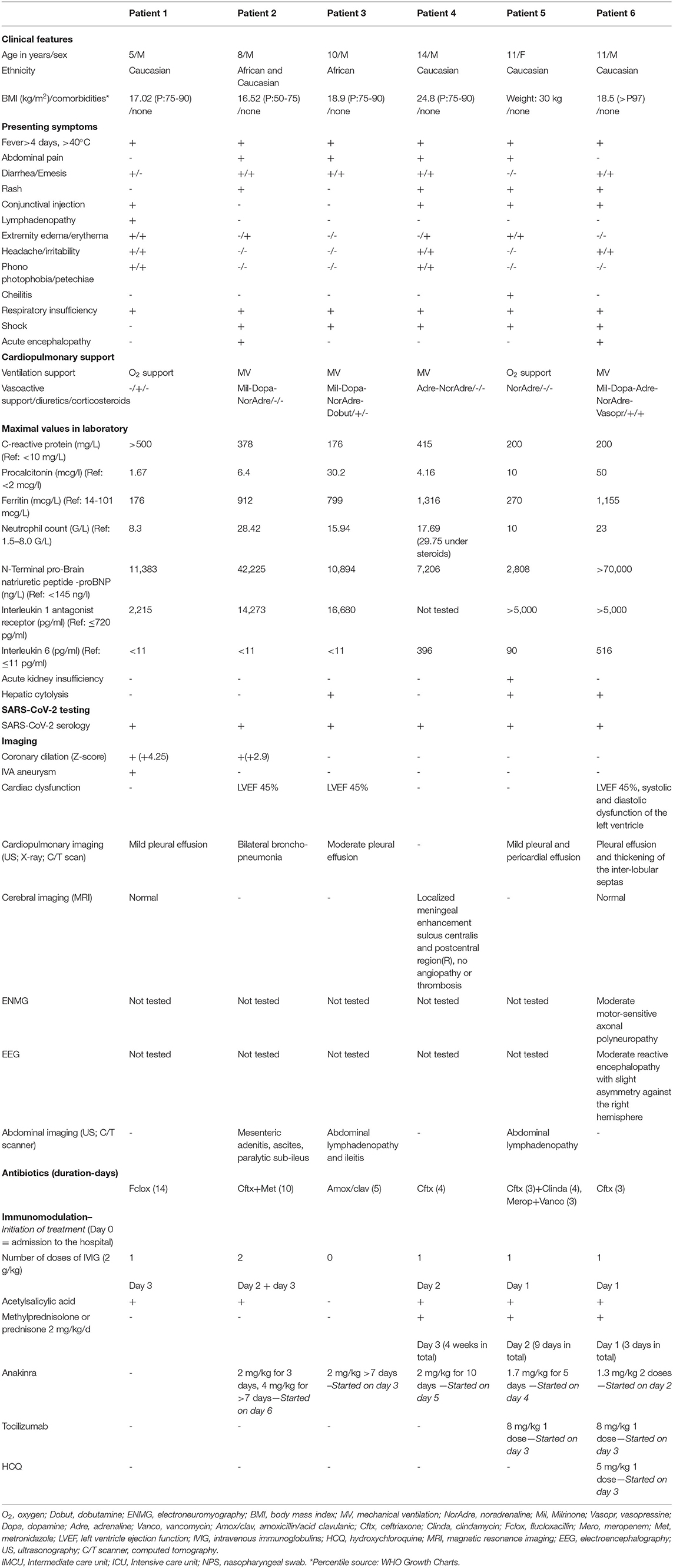
Table 1. Clinical and biological characteristics of Swiss children admitted in Hospital with MIS-C.
All 6 patients presented with persistent fever above 39°C (more than 5 days) and were treated with broad spectrum intravenous antibiotics at admission, despite negative blood cultures. None presented with respiratory symptoms or infiltrates on chest X-rays suggestive of a lower-respiratory tract SARS-CoV-2 infection. All presented an important inflammatory syndrome with high levels of CRP (median: 289 mg/l, IQR: 200-406 mg/l), neutrophilia and increased blood levels IL-1 receptor antagonist (IL-1RA), except for patient 4, where IL-1RA serum levels were not measured. Patients 2, 3 and 6 presented a transitory myocardial dysfunction and patients 1 and 2 with a coronary artery dilatation at the admission. None of the patients had a persistent cardiac dysfunction upon discharge from the hospital. In addition to fever, patients 1 and 4 initially presented with meningitis-like symptoms; albeit with normal cerebrospinal fluid findings. Both children subsequently presented clinical signs, suggestive of Kawasaki Disease (KD), including persistent fever lasting over 5 days, bilateral adenopathy, palmar erythema, hand edema and bilateral conjunctival injection. In addition, patient 1 presented with a coronary dilation [z-score +4.25 (19)] with IVA aneurysm (aneurysm of the left interventricular coronary) on cardiac echography. Patients 2, 3, 5, and 6 presented an acute abdominal clinical picture, with hemodynamic instability requiring aminergic support. Patients 2 and 3 presented with an acute-appendicitis-like clinical picture. Patients 5 and 6 presented some acute abdominal symptoms associated with conjunctival injection and a rash, albeit not meeting all criteria for complete KD. Serum cytokine profile investigations showed increased IL1RA levels (8 to 22-fold) in 5 of the 6 patients (one patient had not been tested), whereas IL-6 serum levels were increased only in the 3 patients of the 6 who were tested. The rest of the cytokine profile was normal.
The treatments introduced for each patient and their CRP values are shown in Figure 1. With exception of patient 3, all patients received at least one dose of intravenous immunoglobulins (IVIG 2 g/kg). Patient 1 benefited of one dose of IVIG with a positive clinical and biological response. Patient 2 received a second dose of IVIG (the same dose as the first one administrated, 2 g/kg) 48 h apart (on day 3 of admission) and subcutaneous anakinra at 2 mg/kg/day for 3 days (started on day 6), increased up to 4 mg/kg/day given his persistent fever and increased inflammatory parameters. Patient 3 only received anakinra (2 mg/kg) with favorable clinical and biological response. Patients 4, 5, and 6 required one dose of IVIG followed by anakinra (2 mg/kg) and steroids for patient 4, which resulted in the resolution of inflammatory parameters. Patient 4 was initially under methylprednisolone (for one week) and then he benefited from a relay by prednisone with a tapering regimen over 3 weeks. In addition, patients 5 and 6 also received one dose of tocilizumab (8 mg/kg). Patient 5 received tocilizumab in addition to steroids which were started the day before, because of persisting fever and hemodynamic instability, with a good initial response. However, after 24 h, the patient presented again fever, diffuse myalgia, burning on palms of hand and feet and hemodynamic instability, in tandem with persistence of inflammatory markers. All these reasons have motivated the addition of Anakinra. Patient 6 was remaining sub febrile with a massive inflammatory syndrome, pejoration of the Pro-BNP, and cardiac echography showing an alteration of the cardiac function with suspicion of myocarditis, despite 2 doses of Anakinra and those parameters have motivated the addition of Tocilizumab one day after the introduction of Anakinra and hydroxychloroquine.
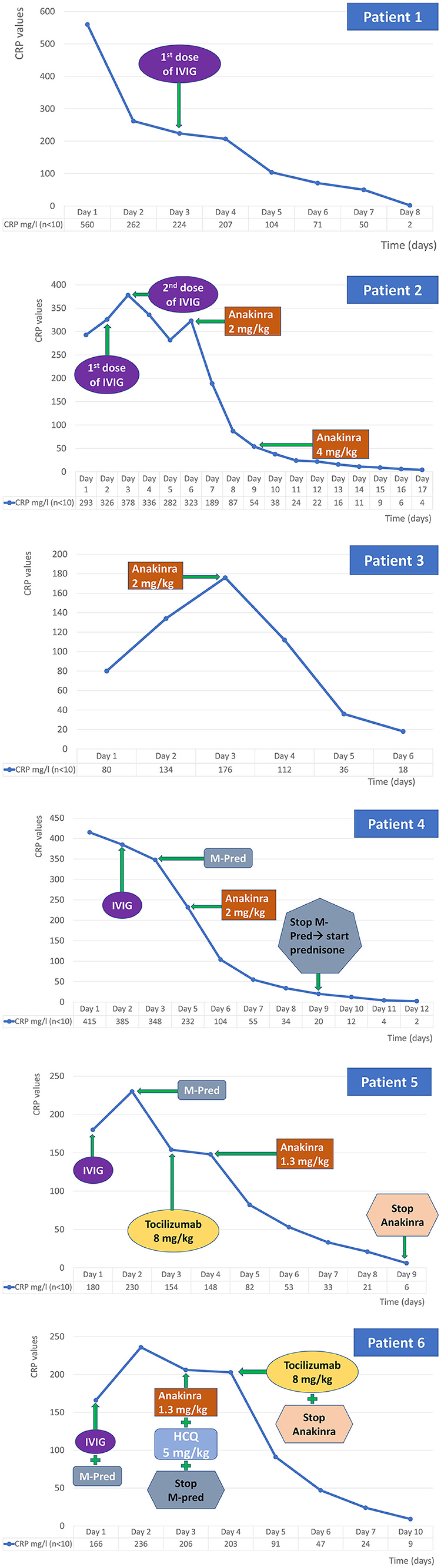
Figure 1. Chronology of the inflammatory markers and the treatments used. IVIG, intravenous immunoglobulins.
It is important to highlight that the results of the cytokines were not available when we considered to change treatments. Four patients (patient 1, 4, 5, and 6) were also treated with acetylsalicylic acid at anti-inflammatory doses.
We report on a cohort of Swiss children with SARS-CoV2 related MIS-C presenting with clinical features compatible with Incomplete KD and Toxic Shock Syndrome associated to a cytokine storm suggestive of a macrophage activation syndrome (MAS) without fulfilling the criteria for Hemophagocytic Lymphohistiocytosis (HLH). As already documented elsewhere (2, 4, 6, 7, 16, 20) and as described in 4 of our 6 patients, many children with MIS-C present some criteria for complete or incomplete KD, appendicitis-like abdominal symptoms and important hyperinflammatory syndrome. Important epidemiological differences between KD and MIS-C include the ethnicity and age of affected patients. While KD primarily affects infants and young children with a 20-fold increased incidence in Asian children (21, 22), MIS-C has been reported among older children, predominantly from an African and Hispanic ethnic background, but this is not always the case (21, 22). These findings could suggest an underlying specific host polymorphism triggering a cytokine cascade secondary to SARS-CoV-2 infection. Hospitalizations due to SARS-CoV-2 were higher in the same geographic areas in which we later discovered the cases of MIS-C, thereby reinforcing an association between MIS-C and SARS-CoV-2. The contribution of a specific SARS-CoV-2 strain is debated, as some of the European SARS-CoV-2 strains could harbor a mutation favoring TCR binding (23) thereby possibly explaining the occurrence of MIS-C in Western countries rather than in Asia. Yet, several different strains have been documented in Europe and in the US (24). As such, the pathophysiology of progression to MIS-C in specific children remains unclear. The contribution of a specific strain in our cohort of patients could not be documented given that genotyping analyses were limited due to the very low viral loads detection. MIS-C also differs from acute COVID-19 illness which tends to be most severe in infants <1 year of age (7, 25, 26). In addition, MIS-C is typically documented up to a month after the peak of SARS-CoV-2, thereby coinciding with the timing of acquired immunity and suggesting a post-infectious inflammatory reaction rather than an acute infectious process (7, 21, 22, 27).
The pathophysiology and the mechanisms by which SARS-CoV-2 triggers an abnormal immune response leading to MIS-C remain poorly understood. Current evidence reports a hyperinflammatory reaction presenting similarities with TSS, incomplete KD and MAS, suggesting activation of the innate immune response with massive pro-inflammatory production (28). SARS-CoV-2 may act as a superantigen (23) similarly to the staphylococcal enterotoxin B (SEB) known to bind to the costimulatory molecule CD28 and the T cell receptor (TCR), thus mediating TSS. The activation of the innate immunity during SARS-CoV-2 infection leads to a cytokine release syndrome named “cytokine storm” characterized by persistent fever and markedly elevated cytokines mostly TNF-α, IL-1β, IL-1RA, sIL-2Rα, IL-6, IL-10, IL-17, IL-18, IFN -γ, MCP-3, M-CSF, MIP-1a, G-CSF, IP-10, and MCP (29). Most of recent published case series of MIS-C patients documented increased IL-6 levels; (28, 30, 31) the serum levels of other pro-inflammatory cytokines being underreported, except for normal levels of IL-1ß in one case (28). Our case series differs in the documentation of very high serum interleukin-1 receptor antagonist (IL-1RA) levels, an important marker for innate immunity activation, among 5 patients; IL-6 serum levels being elevated in only 3 of our 6 patients. These findings may suggest that the activation of the IL-1 pathway also represents an important mechanism of activation in MIS-C as already documented in other conditions such as MAS, TSS, and KD (32). Given similarities between MIS-C and KD and the contribution of IVIG in TSS, all but one patient were first started on IVIG with or without corticosteroids (16, 21, 22). Three of our patients received either parenteral methylprednisolone or a short course of oral prednisone. Recent evidence reports on a one-third reduced deaths among intubated and ventilated adults with acute COVID-19 treated with dexamethasone for 10 days when compared with patients randomized to usual care alone (33). As such, the benefit of dexamethasone has mostly been suggested among adults with severe COVID-19 disease, although it might also be useful in MIS-C given its inhibition of cytokine production (33) In addition, glucocorticoids are also recommended for patients with KD with persistent fever after IVIG or coronary arteries dilatation and are considered among those with cytokine release syndrome. In this regard, the benefits of glucocorticoids as first-line treatment for inflammatory diseases remain undisputable, although biological agents are also attractive alternatives as reported from children with JIA (34). Several reports refer to the use of anakinra (an IL-1 receptor antagonist RA recombinant) and tocilizumab (an antibody against the IL-6 receptor) in patients infected by SARS-CoV-2 with hyperinflammatory state and in a minority of those with MIS-C in addition to IVIG and glucocorticoids (5, 20, 30, 35). Anakinra is specifically attractive due to its good safety profile and short half-life.
This case series displays a range of heterogeneous treatments, prescribed by different hospitals in Switzerland, which allows us to draw a first set of meaningful conclusions on the effectiveness of combinations of different drugs on patients infected by SARS-CoV-2. Specifically, only one patient (patient 1) received solely IVIG, and the remaining five received anakinra either alone or in combination with other drugs. From these five patients, one (patient 3) only received anakinra and the four others also received additional immunomodulators. Notably, one patient (patient 2) received solely IVIG as supplement treatment and the remaining three (patients 4,5 and 6) received steroids in addition to IVIG; two out of them (patients 5 and 6) also received one course of tocilizumab. All patients had a favorable response to these different treatments.
In conclusion two of our six patients were successfully treated with anakinra without receiving steroids or other immunosuppressive treatment. This observation combined with the documentation of increased IL-1RA levels in 5 of our 6 patients further supports the use of anakinra in children presenting a multi-system inflammatory syndrome (MIS-C). Concerning the other targeted treatments and notably the tocilizumab, it could be either an alternative or a supplementary treatment depending on the cytokine profile presented by the patient, which varies between individuals.
Despite the limited number of cases included in our study in addition to previous reports on 3 of the 9 Swiss MIS-C, we believe that we add on current published evidence by providing a complete cytokine profile from most of the included cases and provide some evidence on the use of anakinra in MIS-C. This type of study is most useful for describing the potential effectiveness of new interventions and for describing the effectiveness of interventions on unusual diagnoses.
In conclusion, our case series reports on clinical and laboratory findings of most of Swiss cases with MIS-C and suggests the use of anakinra as effective treatment, especially in children with documented high IL-1RA levels.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Commission cantonale (VD) d'éthique de la recherche sur l'être humain. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
AF, YF, SA, and MH were involved in the conception of the paper. AF, YF, CD, SA, and MH analyzed the cases. AF wrote the first draft of the manuscript. AF, YF, and SA wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Santé publique France. COVID-19: Point Épidémiologique du 14 Mai 2020. Saint-Maurice: Santé Publique France (2020).
2. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
3. Russo M. Up to 5 NY Children Dead, 100 Sickened by Rare COVID-Related Illness. New York, NY: NBC. (2020) Available online at: https://www.nbcnewyork.com/investigations/kawasaki-disease-up-to-5-ny-children-dead-85-sickened-by-rare-covid-related-illness/2411571/ (accessed May 15, 2020).
4. Latimer G, Corriveau C, DeBiasi RL, Jantausch B, Delaney M, Jacquot C, et al. Cardiac dysfunction and thrombocytopenia-associated multiple organ failure inflammation phenotype in a severe paediatric case of COVID-19. Lancet Child Adolesc Heal. (2020) 4:2. doi: 10.1016/S2352-4642(20)30163-2
5. Kaushik S, Aydin SI, Derespina KR, Bansal PB, Kowalsky S, Trachtman R, et al. Multisystem inflammatory syndrome in children (MIS-C) associated with SARS-CoV-2 infection: a multi-institutional study from New York City. J Pediatr. (2020) 224:24–9. doi: 10.1016/j.jpeds.2020.06.045
6. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. (2020) 324:259–69. doi: 10.1001/jama.2020.10369
7. Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. (2020) 395:1771–8. doi: 10.1016/S0140-6736(20)31103-X
8. Dufort EM, Koumans EH, Chow EJ, Rosenthal EM, Muse A, Rowlands J, et al. Multisystem inflammatory syndrome in children in New York State. N Engl J Med. (2020) 383:347–58. doi: 10.1056/NEJMoa2021756
9. Nisha MS, Oliver MT, Mullins EWS. SARS-CoV-2 (COVID-19): What do we know about children? A systematic review. Clin Infect Dis. (2020) 954162:1–4. doi: 10.2139/ssrn.3558015
10. Jones VG, Mills M, Suarez D, Hogan CA, Yeh D, Bradley Segal J, et al. COVID-19 and Kawasaki disease: novel virus and novel case. Hosp Pediatr. (2020) 10:537–40. doi: 10.1542/hpeds.2020-0123
11. Bourrely C. COVID-19 and Kawasaki Like Disease: the Known-Known, the Unknown- Known and the Unknown-Unknown. (2020). Available online at: https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-inflammatory~syndrome-20200501.pdf
12. Royal College of Paediatrics and Child Health. Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated With COVID-19. London: The Royal College of Paediatrics and Child Health (2020).
13. Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet. (2020) 395:1417–8. doi: 10.1016/S0140-6736(20)30937-5
14. Jamilloux Y, Henry T, Belot A, Viel S, Fauter M, El Jammal T, et al. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun Rev. (2020) 19:1–13. doi: 10.1016/j.autrev.2020.102567
15. Office Fédéral de la Santé Pulique Confédération. Maladie à Coronavirus 2019 (COVID-19): Rapport sur la Situation Épidémiologique en Suisse et dans la Principauté de Liechtenstein. Berne: Office Federal de la Santé Publique (2020).
16. Dallan C, Romano F, Siebert J, Politi S, Lacroix L, Sahyoun C. Septic shock presentation in adolescents with COVID-19. Lancet Child Adolesc Heal. (2020) 4:21–3. doi: 10.1016/S2352-4642(20)30164-4
17. Huttner A, Combescure C, Grillet S, Haks MC, Quinten E, Modoux C, et al. A dose-dependent plasma signature of the safety andimmunogenicity of the rVSV-Ebola vaccine in Europe and Africa. Sci. Transl. Med. (2017) 9:eaaj17011.
18. Roche. Elecsys® Anti-SARS-CoV-2 Immunoassay for the Qualitative Detection of Antibodies Against SARS-CoV-2. (2020). Available online at: https://diagnostics.roche.com/ch/fr/products/params/elecsys-anti-sars-cov-2.html.
19. Kobayashi T, Fuse S, Sakamoto N, Mikami M, Ogawa S, Hamaoka K, et al. A new z score curve of the coronary arterial internal diameter using the lambda-mu-sigma method in a pediatric population. J Am Soc Echocardiogr. (2016) 29:794–801.e29. doi: 10.1016/j.echo.2016.03.017
20. Belhadjer Z, Méot M, Bajolle F, Khraiche D, Legendre A, Abakka S, et al. Acute heart failure in multisystem inflammatory syndrome in children (MIS-C) in the context of global SARS-CoV-2 pandemic. Circulation. (2020) 142:429–36. doi: 10.1161/CIRCULATIONAHA.120.048360
21. Toubiana J, Poirault C, Corsia A, Bajolle F, Fourgeaud J, Angoulvant F, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. (2020) 369:m2094. doi: 10.1136/bmj.m2094
22. Center for Disease Control and Prevention, Center for Preparedness and Response. Webinar - Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). (2020). Available online at: https://emergency.cdc.gov/coca/calls/2020/callinfo_051920.asp?deliveryName=USCDC_1052-DM28623 (accessed June 23, 2020).
23. Cheng MH, Zhang S, Porritt RA, Arditi M, Bahar I. An insertion unique to SARS-CoV-2 exhibits superantigenic character strengthened by recent mutations. bioRxiv Prepr Serv Biol [Preprint]. (2020). doi: 10.1101/2020.05.21.109272
24. Cristina J, Castells M, Lopez-Tort F, Colina R, Juan C. Evidence of increasing diversification of emerging SARS-CoV-2 strains. J Med Virol. (2020) 92:2165–72.
25. World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. Available online at: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed June 23, 2020).
26. Licciardi F, Pruccoli G, Denina M, Parodi E, Taglietto M, Rosati S, et al. SARS-CoV-2-induced Kawasaki-like hyperinflammatory syndrome: a novel COVID phenotype in children. Pediatrics. (2020) 146:1–5. doi: 10.1542/peds.2020-1711
27. Mahase E. Covid-19: concerns grow over inflammatory syndrome emerging in children. BMJ. (2020) 369:m1710. doi: 10.1136/bmj.m1710
28. Dolinger MT, Person H, Smith R, Jarchin L, Pittman N, Dubinsky MC, et al. Pediatric Crohn's disease and multisystem inflammatory syndrome in children (MIS-C) and COVID-19 treated with infliximab. J Pediatr Gastroenterol Nutr. (2020) 2:153–5. doi: 10.1097/MPG.0000000000002809
29. Cavalli G, De Luca G, Campochiaro C, Della-Torre E, Ripa M, Canetti D, et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: a retrospective cohort study. Lancet Rheumatol. (2020) 2:e325–31. doi: 10.1016/S2665-9913(20)30127-2
30. Miller J, Cantor A, Zachariah P, Ahn D, Martinez M, Margolis K. Gastrointestinal symptoms as a major presentation component of a novel multisystem inflammatory syndrome in children (MIS-C) that is related to COVID-19: a single center experience of 44 cases. Gastroenterology. (2020) 159:1571–4. doi: 10.1053/j.gastro.2020.05.079
31. Greene AG, Saleh M, Roseman E, Sinert R. Toxic shock-like syndrome and COVID-19: a case report of multisystem inflammatory syndrome in children (MIS-C). Am J Emerg Med. (2020) 2:30492–7. doi: 10.1016/j.ajem.2020.05.117
32. Kone-Paut I, Cimaz R, Herberg J, Bates O, Carbasse A, Saulnier JP, et al. The use of interleukin 1 receptor antagonist (anakinra) in Kawasaki disease: a retrospective cases series. Autoimmun Rev. (2018) 17:768–74. doi: 10.1016/j.autrev.2018.01.024
33. Horby P, Landrey M. Low-Cost Dexamethasone Reduces Death by up to One Third in Hospitalised Patients With Severe Respiratory Complications of COVID-19 - Recovery Trial. (2020) Available online at: https://www.recoverytrial.net/news/low-cost-dexamethasone-reduces-death-by-up-to-one-third-in-hospitalised-patients-with-severe-respiratory-complications-of-covid-19 (accessed June 23, 2020).
34. ter Haar NM, van Dijkhuizen EHP, Swart JF, van Royen-Kerkhof A, el Idrissi A, Leek AP, et al. Treatment to target using recombinant interleukin-1 receptor antagonist as first-line monotherapy in new-onset systemic juvenile idiopathic arthritis: results from a five-year follow-up study. Arthritis Rheumatol. (2019) 71:1163–73. doi: 10.1002/art.40865
Keywords: SARS-CoV-2, child, MIS-C, IL-1ra, Anakinra
Citation: Fouriki A, Fougère Y, De Camaret C, Blanchard Rohner G, Grazioli S, Wagner N, Relly C, Pachlopnik Schmid J, Trück J, Kottanatu L, Perez E, Perez M-H, Schaffner D, Asner SA and Hofer M (2021) Case Report: Case Series of Children With Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Switzerland. Front. Pediatr. 8:594127. doi: 10.3389/fped.2020.594127
Received: 12 August 2020; Accepted: 23 November 2020;
Published: 05 January 2021.
Edited by:
Rolando Cimaz, University of Milan, ItalyReviewed by:
Natasa Toplak, Univerzitetnega Kliničnega Centra Ljubljana, SloveniaCopyright © 2021 Fouriki, Fougère, De Camaret, Blanchard Rohner, Grazioli, Wagner, Relly, Pachlopnik Schmid, Trück, Kottanatu, Perez, Perez, Schaffner, Asner and Hofer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Athina Fouriki, YXRoaW5hLmZvdXJpa2lAY2h1di5jaA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.