
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 17 November 2020
Sec. Pediatric Infectious Diseases
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.580323
 Emma Lim1,2
Emma Lim1,2 Ravi D. Mistry1Alexandra Battersby1,2
Ravi D. Mistry1Alexandra Battersby1,2 Kerry Dockerty3Aaron Koshy4Michelle N. Chopra5Matthew C. Carey6
Kerry Dockerty3Aaron Koshy4Michelle N. Chopra5Matthew C. Carey6 Jos M. Latour6,7*
Jos M. Latour6,7*Background: Parents' health-seeking behaviors has changed during the COVID-19 pandemic. Providing parents with guidance in decision making might improve their confidence to seek timely advice when a child becomes ill. The aim of this study was to evaluate the “How to recognize if your child is seriously ill” leaflet on parents' confidence, health-seeking behaviors, and usefulness during the COVID-19 lockdown.
Method: A nine-item survey, codesigned with parent advisors, was used to measure confidence and health-seeking behavior. Social media was used for data collection in a 6-week period (April–June 2020) during COVID-19 lockdown in the United Kingdom. Categorical data were analyzed as frequencies, and inductive content analysis was performed with the qualitative data.
Results: In total, 171 parents responded. Most parents (n = 160, 93.6%) found the leaflet helpful. The leaflet increased the confidence among 116 parents (67.8%) to recognize if their child is ill, and 156 (91.2%) parents had a better understanding of when and where to seek help. Thirty-three (19.2%) parents used the leaflet, while their child was unwell during COVID-19 lockdown, and in 14 (42%) cases, the leaflet resulted in changing health-seeking behavior for that episode. Twelve of these parents decided to seek medical consultation when they had not planned to before. Content analysis revealed three categories. (1) Knowledge—parents found the leaflet an objective source to validate their concerns. (2) Usability—parents reported that the leaflet was clearly designed. (3) Decision aid—parents commented that the leaflet provided clarification around recognition of serious symptoms and when and where to seek appropriate care.
Conclusions: Our leaflet provided parents with guidance on decision making and risk assessment of ill children during COVID-19 lockdown. Parents found it helpful; it increased their confidence and positively changed their health-seeking behaviors. Providing parents with targeted information to recognize serious illness in children at home could potentially foster self-care and safely maintain a reduction in pediatric emergency attendances for self-limiting illnesses.
The COVID-19 pandemic has been marked by the sense of fear and anxiety experienced by both children and families (1, 2). The difference between the COVID-19 pandemic compared to other epidemics is the mandated social isolation and distancing measures. Closure of schools and nurseries has had a huge impact on families with children (3).
Pediatric emergency departments experienced a significant drop in attendances during the 1st months of lockdown (4). Rates of presentation have fallen by 70% since the start of the pandemic, and a report from Italy documented an increase in delayed presentations resulting in avoidable harms and increased pediatric intensive care admissions (5). Parents of unwell children might delay contacting healthcare services fearing nosocomial infection, being isolated from their child, or not wanting to burden the hospital during the pandemic. There were concerns from pediatricians that unwell children were more likely to be affected by non-COVID-19-related disease and collateral damage from delayed presentation could be significant. However, a recent study in the United Kingdom reported that delayed presentations at emergency departments were rare (4).
The COVID-19 pandemic has challenged hospitals in preparing effective response systems (6). Providing and disseminating timely, clear, and reliable information for parents has been challenging. The UK National Health Service (NHS) provided guidance for COVID-19 patients in primary care and family doctor services (7). For children, COVID-19 information has been described and explained by Alberca et al. (8), and children's hospitals created webpages to inform children and families (9).
Prior to the COVID-19 pandemic, our team of parents and healthcare professionals developed a parent decision-making and risk assessment leaflet (10) for parents to identify early deterioration of a seriously ill child, including parental concern as a trigger to escalate care (11). Due to the decrease in pediatric emergency department (PED) attendances at the early stages of the COVID-19 pandemic, we published our leaflet on the hospital website in February 2020 to support parents in the community. We considered that this intervention would give parents the confidence to access timely healthcare services. To our knowledge, there is limited evidence assessing the impact of advice around healthcare-seeking behavior and parental information during the COVID-19 pandemic.
The aim of this study was to evaluate the experiences of parents using this decision-making and risk assessment leaflet for a potentially seriously ill child during COVID-19 lockdown. More specifically, we explored the confidence of parents, their health-seeking behaviors, and usefulness of the leaflet.
An observational service evaluation design was adopted. The “Guidelines for Reporting Evaluations based on Observational Methodology” (GREOM) was used to report this study (12).
The Research and Design Service of the Newcastle Upon Tyne Hospitals NHS Foundation Trust approved this study as a service evaluation. The survey was anonymous, and confidentiality of information was assured.
The parent decision-making and risk assessment leaflet “How to recognize if your child is seriously ill” was developed with parents for parents (Electronic Supplementary Material 1). The content was designed using the NICE “Fever in under 5s: assessment and initial management” (13), pediatric sepsis guidelines, sepsis leaflets for parents (14–16), and studies reporting signs and symptoms of children presenting to pediatric emergency departments (17, 18). Based on the available evidence, the content of the risk assessment symptoms refers to preschool and primary school children, generally below 12 years of age. Some symptoms have been included when these are specifically related to children below 1 year or 1 month of age.
The leaflet includes two main sections. The first section explains how to use the leaflet and provides space to write down the details of the child and parental concerns. Additional practical tips and medication use are included. The second section is divided into green, amber, and red with guidance for decision making of where and how to seek health advice. The risk assessment includes six systems: (1) temperature; (2) breathing; (3) skin, lips, and tongue; (4), eating and drinking, (5) toilet/nappies; and (6) activity and body.
Ten parents from a local parent support group reviewed the content of the leaflet and compared it with another leaflet (19) published by the Royal College of Pediatrics and Child Health (RCPCH) during the early stages of the COVID-19 pandemic. Overall, there was consensus that our parent decision-making and risk assessment leaflet was preferred as it included parental concern, sufficiently detailed information, and options to write down observations.
The distribution of the parent leaflet was implemented without manipulation and could be used in the everyday context during the COVID-19 lockdown. The evaluation was conducted via an online survey with a minimum number of questions designed to be completed in < 5 min to reduce the burden to respondents during COVID-19 lockdown and was considered a low-intensity intervention in the context of the observational methods.
Participants were parents, carers, or guardians of children in the North East of England during the COVID-19 lockdown. The population in the North East of England is around 320,000, and the last census in 2011 documented that 97% of the population described themselves as white British (20).
We anticipated a sample size of around 100 parents based on previous work evaluating a parent sepsis leaflet in the South West of England (21). The sample size depended on the voluntary engagement of parents in the community and the promotion of the leaflet. Inclusion criteria were parents, caretakers, or guardians with children who downloaded the parent leaflet and the attached invitation with a website link to complete a short online survey.
The method of recruitment was via social media. The leaflet and an invitation to participate was distributed via Twitter, Facebook, and the website of our hospital. Local schools, social services, and COVID-19 support groups informed parents via their chat groups, tweets, and messages on Facebook containing a link to the leaflet and online survey.
The lockdown in the United Kingdom started on March 12, 2020 and was eased on June 15, 2020 allowing the opening of non-essential shops. The recruitment time via social media was 6 weeks, from April 29, 2020 to the first ease of the COVID-19 lockdown on June 15, 2020. We acknowledged that recruitment via social media might include respondents from outside North East of England. Therefore, we included all respondents in the United Kingdom but excluded those outside the United Kingdom.
The self-administered online survey was designed to address parent's confidence, health-seeking behavior, and general experience of the leaflet. The survey was developed together with our local parent advisory group. Ten parents reviewed the draft of the survey, and minor suggestions were provided to improve the clarity of the questions and answer option scales. Parents agreed that the final 10-item survey was acceptable to complete in the current COVID-19 climate.
The final survey included eight closed questions and two optional open-ended questions (Electronic Supplementary Material 2). The first three questions were demographic questions followed by questions measuring health-seeking behavior, experience of the leaflet, and confidence. Two open-ended questions were included to provide parents the option of sharing their experiences and opinions.
The quantitative analyses were performed using IBM-SPSS version 25.0 (IBM, New York, NY, USA). Categorical data are presented as frequency in percentages. The responses of the two open-ended questions were analyzed by inductive content analysis (22). This included open coding of the narratives and grouping into subcategories. Abstraction was further enhanced by generating categories described by content-characteristic words.
During the 6-week data collection, 171 parents responded to the online survey. Of the 170 respondents who completed the postcode question, 148 (86.5%) were living in the North East of England, and 22 (13.5%) were living in the rest of the United Kingdom. Half of the parents (n = 87; 50.9%) reported having two children in their household followed by 46 (26.9%) parents having one child (Table 1). Most of the parents (n = 159, 93%) were white British reflecting the population ethnicity in the North East of England (Table 1).
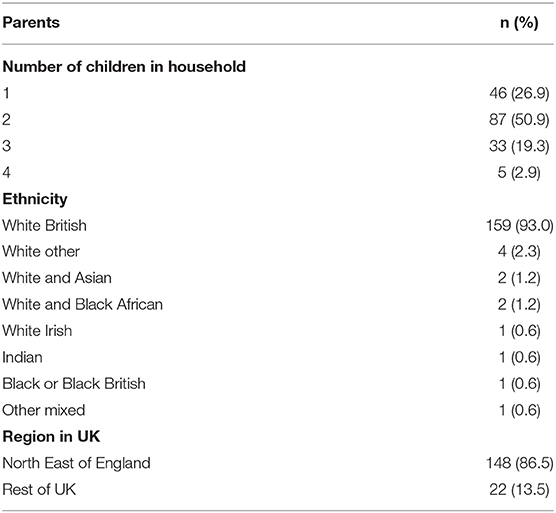
Table 1. Characteristics of participants (n = 171).
In terms of health-seeking behaviors and first point of contact when their child is unwell, 87 (50.9%) of the parents reported that they usually visit and seek advice from their family doctor. A further 59 (34.5%) parents reported that they first would call NHS 111, a free non-emergency medical helpline. Only 14 (8.2%) parents reported that they would visit the emergency department (Table 2).
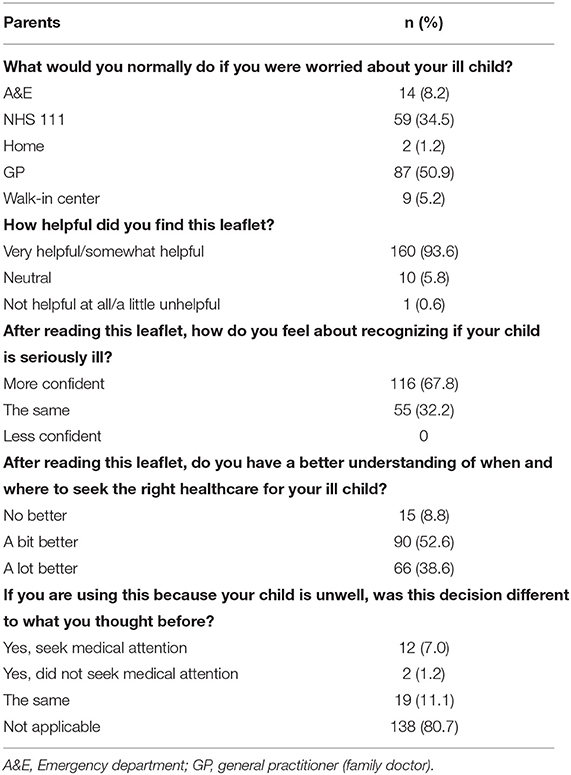
Table 2. Experiences of parent information leaflet (n = 171).
Overall, most parents perceived the leaflet as being helpful (93.6%). Of these, 89 (52%) parents found the leaflet very helpful, and 71 (41.5%) as somewhat helpful. The leaflet increased the confidence of parents (n = 116, 67.8%) in recognizing if their child is seriously ill (Table 2). Furthermore, 156 (91.2%) parents reported that they had a better understanding of when and where to seek help. There were 33 (19.3%) parents who used the leaflet while their child was unwell, and in 14 (42%) cases, the leaflet resulted in changing the health-seeking behavior for that episode. Of these, 12 parents chose to take their child to seek medical attention where they had not planned to before, and 12 of these 14 parents reported an increased in confidence in recognizing if their child was unwell. In the group of parents where their health-seeking behavior was not changed (n = 19), only 10 parents reported an increase in confidence.
Content analysis of the free text responses revealed three categories: Knowledge, Usability, and Decision aid (Table 3). The category Knowledge included three subcategories where parents commented on the leaflet as being an objective source to validate their concerns. Parents wrote that the leaflet was an essential resource while staying at home. The leaflet was valued by parents because of the age specificity of some of its information. This helped parents in their medical assessment when their child was becoming sick. The category Usability included the subcategories linguistic clarity and visual clarity where parents reported that the leaflet was clearly designed including the traffic light color coding system on when and how to seek medical attention. The category Decision aid had two subcategories. The subcategory response calibration was related to the systematic breakdown of symptoms that provided clarification about what to observe, when to make the decision to seek further advice, and who to contact. Some parents reported that the leaflet gave them more confidence in their decision making.
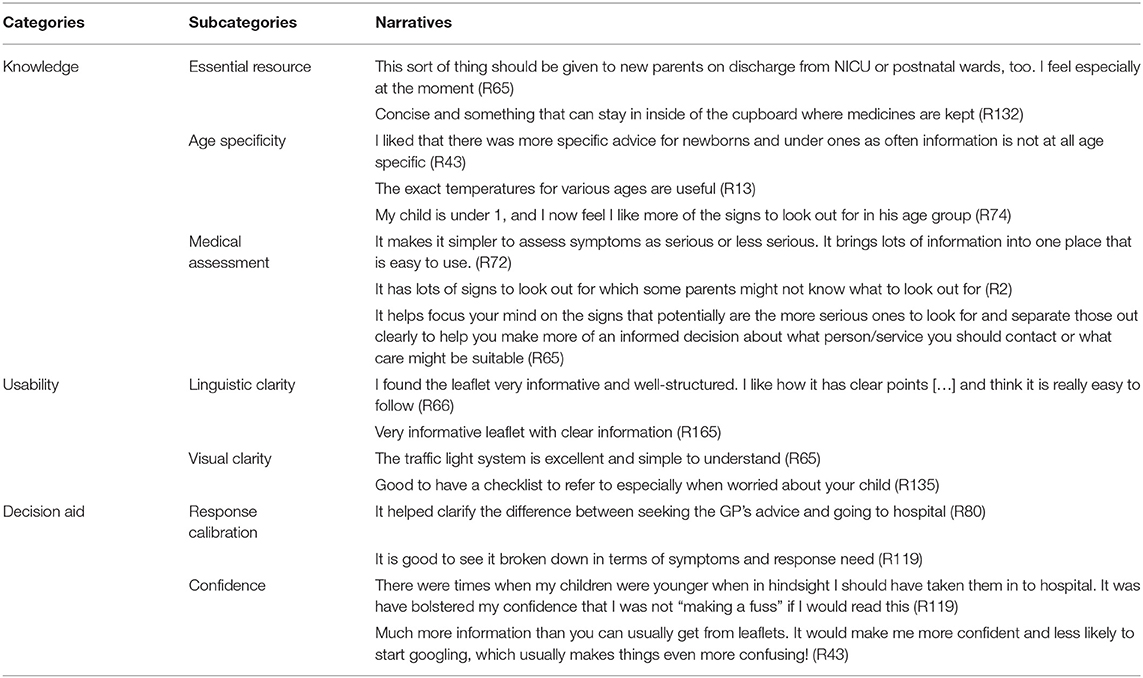
Table 3. Parent's experiences of leaflet.
The same categories were used in analyzing the free-text responses related to suggestions for improvements (Table 4). In the Knowledge category, the risk guidance was deemed to be unclear by some parents, and they cautioned over the ambiguity of symptoms to seek help in the amber category of the leaflet. The category Usability included comments on the linguistic and visual clarity. Two parents commented that the leaflet could be written in easier language as the leaflet could be challenging for parents with low literacy skills. Another parent suggested using bullet points rather than tick boxes before every symptom. In the Decision aid category, parents suggested that the leaflet could increase confidence by emphasizing parental concern (or gut instinct) more prominently. Three parents highlighted that the leaflet does not cover specific emergencies such as anaphylaxis, diabetic ketoacidosis, febrile convulsions, or meningitis.
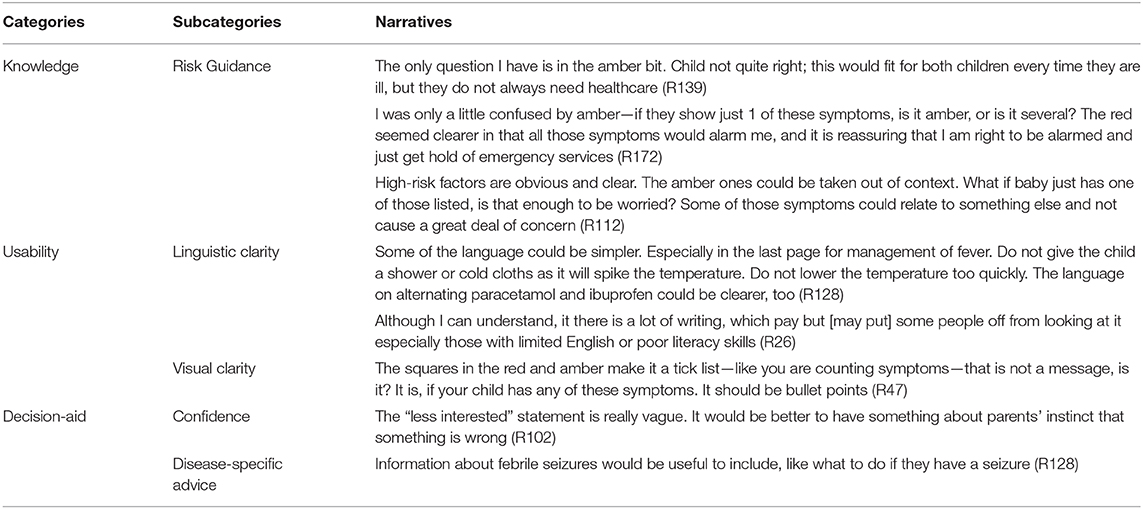
Table 4. Suggestions provided by parents.
This project aimed to explore the experiences of parents using an information leaflet to help them recognize serious illness in their children and respond appropriately during the COVID-19 lockdown. The leaflet provided parents with detailed information to support decision making and seek timely medical advice. Our leaflet was coproduced with local parents via an iterative process. Information material that is coproduced and evaluated by target stakeholders has been shown to be more effective in improving knowledge and health-seeking behaviors (23).
Parents of unwell children are in a position of vulnerability and are aware of being perceived as worriers by healthcare professionals and their friends/family (24, 25). Parents fear hospital attendance with its perceived risks, while social distancing has removed normal access to formal and informal social support structures. Febrile illnesses increase parental anxiety (26), especially when other symptoms are already present (25). This was clearly heightened during the COVID-19 pandemic (27), especially with fever being a central tenet of the case definition. Parents desire a clear source of information that they can independently access to empower themselves, validate their concerns, and reassure them that they have taken the appropriate course of action when caring for their febrile child (25). Our leaflet provided this through detailed and comprehensive information.
Baseline knowledge is vital, and gaps in parents' knowledge have been identified; most parents cannot identify the temperature at which a child is said to be febrile (25). This has resonance with our findings as many respondents commented positively on our inclusion of age-specific temperature thresholds. Supplying information on management is crucial to guide appropriate and timely use of healthcare services for parents and avoid unnecessary consultations (28). Importantly, comprehensive multitopic information on febrile illness is more effective at reducing parental anxiety and increasing confidence than single differentials of fevers (26). This is because children often present with a constellation of symptoms alongside a fever.
Most parents in our study would see their GP first. This health-seeking behavior is well-established with parents in high-income countries (25). Often parents consult printed or electronic reference material before deciding what course of action to take (26). There is limited evidence on parents' health-seeking behavior during COVID-19. The NHS has noted a one-third drop in emergency department attendances (29) and GP appointments (30) coupled with a 50-time rise in online triage information being accessed (31) during the current outbreak. This indicates many more people are seeking authoritative reference material prior to attending and suggests there is an opportunity to influence primary care and PED attendance.
Several limitations need to be addressed. We used an online web-based survey and recruitment via social media both of which could have resulted in selection bias. Parents who have limited access to social media platforms, the Internet, computers, or smartphones may not have had the opportunity to be included or been able to access the leaflet. This may be a particular issue in socially deprived areas or in middle- and low-income countries without ready Internet access. Newcastle-upon-Tyne has large socially deprived areas, and we worked together with local charities such as the Newcastle West End Schools Trust and Newcastle local authority and agencies affiliated with the West Partnership who kindly supported the project in printing and distributing the parent leaflet to ensure wide access. We also received support from community groups, schools, and health visitors who were willing to advertise the parent leaflet on their websites. We also acknowledge the limitation of the short survey. The survey was designed to generate a general understanding of the parents' experiences, confidence, and health-seeking behaviors and was intentionally kept short to reduce the burden of parents to complete the survey. Validated instruments exist, such as the 34-item Family Empowerment Scale (32) and the 15-item Karitane Parenting Confidence Scale (33), but are significantly longer to administer.
In conclusion, the majority of parents found our parent information leaflet on decision making and risk assessment in ill children helpful and improved their confidence. The leaflet may have changed health-seeking behavior during the COVID-19 social isolation period and contributed to patents' better understanding of when and where to seek medical attention if their child becomes unwell.
The silver lining to the COVID-19 pandemic has been the reduction in PED attendances. Providing parents with targeted information when a child becomes seriously ill at home could potentially foster self-care and safely maintain this reduction of PED attendances for self-limiting illnesses. Our study shows parents welcoming this information and are actively seeking trusted sources of healthcare information and acting on them. The onus is on healthcare practitioners and institutions to understand this need and deliver quality healthcare support and education widely. Now, we need further research to understand the effectiveness of our parent information leaflet during the “new normal” including children's (long-term) health outcomes, particularly focusing on the most disadvantaged sectors and their access to health information.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The Research and Design Service of the Newcastle upon Tyne Hospitals NHS Foundation Trust approved this study as a service evaluation.
EL, AB, KD, and JML developed the intervention. EL, AB, KD, AK, MNC, MCC, and JML initiated the evaluation and contributed to the design of the study. EL, AB, KD, and RM contributed to the data collection. EL, RM, MCC, and JML contributed to the data analysis and interpretation. EL and JML drafted the first manuscript. All authors contributed to manuscript revisions, approved the final version of the manuscript, and agreed to be accountable for the content of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors like to thank all parents who have been involved in the development of the leaflet. We like to thank Joanne Mulholland and Annemarie Troy-Smith for their support and valuable advice on the leaflet. We thank all parents for completing the survey during the COVID-19 lockdown; your advice has been invaluable.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.580323/full#supplementary-material
1. Fegert JM, Vitiello B, Plener PL, Clemens V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatr Ment Health. (2020) 14:20. doi: 10.1186/s13034-020-00329-3
2. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
3. Viner RM, Russell SJ, Croker H, Packer J, Ward J, Stansfield C, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. (2020) 4:397–404. doi: 10.1016/S2352-4642(20)30095-X
4. Roland D, Harwood R, Bishop N, Hargreaves D, Patel S, Sinha I. Children's emergency presentations during the COVID-19 pandemic. Lancet Child Adolesc Health. (2020) 4:e32–3. doi: 10.1016/S2352-4642(20)30206-6
5. Lazzerini M, Barbi E, Apicella A, Marchetti F, Cardinale F, Trobia G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc Health. (2020) 4:e10. doi: 10.1016/S2352-4642(20)30108-5
6. Zhang Y, Sun Z, Latour JM, Hu B, Qian J. Hospital response to the COVID-19 outbreak: the experience in Shanghai, China. J Adv Nurs. (2020) 76:1483–5. doi: 10.1111/jan.14364
7. Razai MS, Doerholt K, Ladhani S, Oakeshott P. Coronavirus disease 2019 (covid-19): a guide for UK GPs. BMJ. (2020) 368:m800. doi: 10.1136/bmj.m800
8. Alberca G, Fernandes I, Sato M, Alberca R. What is COVID-19? Front Young Minds. (2020) 8:74. doi: 10.3389/frym.2020.00074
9. Hospital GOS. Coronavirus (COVID-19) – Information for Children, Young People and Families. (2020). Available online at: https://www.gosh.nhs.uk/news/coronavirus-covid-19-information-children-young-people-and-families (accessed July 5, 2020).
10. Hospital TGNCs. How to Recognise if Your Child is Seriously Ill. (2020). Available online at: http://www.newcastle-hospitals.org.uk/_assets/media/How_to_recognise_if_your_child_is_seriously_ill.pdf (accessed July 5, 2020).
11. Harley A, Latour JM, Schlapbach LJ. The role of parental concerns in the recognition of sepsis in children: a literature review. Front Pediatr. (2019) 7:161. doi: 10.3389/fped.2019.00161
12. Portell M, Anguera MT, Chacón-Moscoso S, Sanduvete-Chaves S. Guidelines for reporting evaluations based on observational methodology. Psicothema. (2015) 27:283–9. doi: 10.7334/psicothema2014.276
13. National Institiute of Health and Care Excellence. Fever in Under 5s: Assessment and Initial Management NICE Guideline [NG143]. (2019). Available online at: https://www.nice.org.uk/guidance/ng143 (accessed July 5, 2020).
14. Latour J, Bracefield S, Sadler P, O'Connor A, Endacott R. Assessment of early sepsis in children by parents and general practitioners: an evaluation. Eur J Pediatr. (2016) 175:1558–9. doi: 10.1007/s00431-016-2785-8
15. Tavaré A, O'Flynn N. Recognition, diagnosis, and early management of sepsis: NICE guideline. Br J Gen Pract. (2017) 67:185–6. doi: 10.3399/bjgp17X690401
16. Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr Crit Care Med. (2020) 21:e52–106. doi: 10.1097/PCC.0000000000002197
17. Elshout G, van Ierland Y, Bohnen AM, de Wilde M, Oostenbrink R, Moll HA, et al. Alarm signs and antibiotic prescription in febrile children in primary care: an observational cohort study. Br J Gen Pract. (2013) 63:e437–44. doi: 10.3399/bjgp13X669158
18. van Ierland Y, Elshout G, Moll HA, Nijman RG, Vergouwe Y, van der Lei J, et al. Use of alarm features in referral of febrile children to the emergency department: an observational study. Br J Gen Pract. (2014) 64:e1–9. doi: 10.3399/bjgp14X676393
19. Royal College of Paediatrics and Child Health. Advice for Parents During Coronavirus. (2020). Available online at: https://www.rcpch.ac.uk/sites/default/files/2020-04/covid19_advice_for_parents_when_child_unwell_or_injured_poster.pdf (acccessed July 5, 2020).
20. Jamieson M. Northumberland County Council. Ethnicity and Religion in Northumberland: Northumberland Knowledge Research Report. (2013) Available online at: https://www.northumberland.gov.uk/NorthumberlandCountyCouncil/media/Northumberland-Knowledge/NK%20people/Demographics/Ethnicity-and-Religion-March-2013.pdf (accessed July 5, 2020).
21. Latour J, Bracefield S, Sadler P, Endacott R, O'Connor A. Early Sepsis in Children Assessment by Parents: an Evaluation. (2016). Available online at: https://pearl.plymouth.ac.uk/bitstream/handle/10026.1/15571/EarlySepsisChildrenAssessmentParentsEvaluation_ESCAPE-Report_20160216.pdf?sequence=1&isAllowed=y. (accessed July 5, 2020).
22. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. (2008) 62:107–15. doi: 10.1111/j.1365-2648.2007.04569.x
23. van de Maat JS, van Klink D, den Hartogh-Griffioen A, Schmidt-Cnossen E, Rippen H, Hoek A, et al. Development and evaluation of a hospital discharge information package to empower parents in caring for a child with a fever. BMJ Open. (2018) 8:e021697. doi: 10.1136/bmjopen-2018-021697
24. De S, Tong A, Isaacs D, Craig JC. Parental perspectives on evaluation and management of fever in young infants: an interview study. Arch Dis Child. (2014) 99:717–23. doi: 10.1136/archdischild-2013-305736
25. Thompson AP, Nesari M, Hartling L, Scott SD. Parents' experiences and information needs related to childhood fever: a systematic review. Patient Educ Couns. (2020) 103:750–63. doi: 10.1016/j.pec.2019.10.004
26. Neill S, Roland D, Jones CH, Thompson M, Lakhanpaul M. Information resources to aid parental decision-making on when to seek medical care for their acutely sick child: a narrative systematic review. BMJ Open. (2015) 5:e008280. doi: 10.1136/bmjopen-2015-008280
27. Ebrahim AH, Saif ZQ, Buheji M, AlBasri N, Al-Husaini FA, Jahrami H. COVID-19 information-seeking behavior and anxiety symptoms among parents. OSP J Health Care Med. (2020) 1:1–9. Available online at: https://www.ospublishers.com/pdf/HCM-1-105.pdf
28. de Bont EG, Loonen N, Hendrix DA, Lepot JM, Dinant GJ, Cals JW. Childhood fever: a qualitative study on parents' expectations and experiences during general practice out-of-hours care consultations. BMC Fam Pract. (2015) 16:131. doi: 10.1186/s12875-015-0348-0
29. NHS England. A&E Attendances and Emergency Admissions. (2020). Available online at: https://www.england.nhs.uk/statistics/statistical-work-areas/ae-waiting-times-and-activity/ (accessed July 5, 2020).
30. NHS Digital. Appointments in General Practice. (2020). Available online at: https://digital.nhs.uk/data-and-information/publications/statistical/appointments-in-general-practice/march-2020 (accessed July 5, 2020).
31. NHS Digital. Coronavirus (COVID-19) Increase in Use of NHS Digital Tech. (2020). Available online at: https://digital.nhs.uk/coronavirus/nhs-digital-tech-analytics#nhs-111-online (accessed July 5, 2020).
32. Koren PE, DeChillo N, Friesen BL. Measuring empowerment in families whose children have emotional disabilities: a brief questionnaire. Rehab Psychol. (1992) 37:305–21. doi: 10.1037/h0079106
Keywords: COVID-19, parents, confidence, anxiety, health behavior, children, social isolation, impact
Citation: Lim E, Mistry RD, Battersby A, Dockerty K, Koshy A, Chopra MN, Carey MC and Latour JM (2020) “How to Recognize if Your Child Is Seriously Ill” During COVID-19 Lockdown: An Evaluation of Parents' Confidence and Health-Seeking Behaviors. Front. Pediatr. 8:580323. doi: 10.3389/fped.2020.580323
Received: 06 July 2020; Accepted: 02 October 2020;
Published: 17 November 2020.
Edited by:
Jan Hau Lee, KK Women's and Children's Hospital, SingaporeReviewed by:
Charlene Pringle, University of Florida, United StatesCopyright © 2020 Lim, Mistry, Battersby, Dockerty, Koshy, Chopra, Carey and Latour. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jos M. Latour, am9zLmxhdG91ckBwbHltb3V0aC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.