
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 16 July 2020
Sec. Pediatric Cardiology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00384
This article is part of the Research Topic Kawasaki Disease View all 14 articles
 Elizabeth Moreno1
Elizabeth Moreno1 S. Diana Garcia1
S. Diana Garcia1 Emelia Bainto1Andrea P. Salgado2Austin Parish1,3Benjamin D. Rosellini1
Emelia Bainto1Andrea P. Salgado2Austin Parish1,3Benjamin D. Rosellini1 Rolando Ulloa-Gutierrez4
Rolando Ulloa-Gutierrez4 Luis M. Garrido-Garcia5Lourdes Dueñas6
Luis M. Garrido-Garcia5Lourdes Dueñas6 Dora Estripeaut7Kathia Luciani8
Dora Estripeaut7Kathia Luciani8 Francisco J. Rodríguez-Quiroz9Olguita del Aguila10Germán Camacho-Moreno11Virgen Gómez12Tamara Viviani13
Francisco J. Rodríguez-Quiroz9Olguita del Aguila10Germán Camacho-Moreno11Virgen Gómez12Tamara Viviani13 Martha I. Alvarez-Olmos14Heloisa Helena de Souza Marques15Enrique Faugier-Fuentes16Patricia Saltigeral-Simental17Eduardo López-Medina18
Martha I. Alvarez-Olmos14Heloisa Helena de Souza Marques15Enrique Faugier-Fuentes16Patricia Saltigeral-Simental17Eduardo López-Medina18 Greta Miño-León19Sandra Beltrán20Lucila Martínez-Medina21
Greta Miño-León19Sandra Beltrán20Lucila Martínez-Medina21 Maria C. Pirez22Fernanda Cofré23Adriana H. Tremoulet1* and the REKAMLATINA-2 Study Group Investigators
Maria C. Pirez22Fernanda Cofré23Adriana H. Tremoulet1* and the REKAMLATINA-2 Study Group InvestigatorsObjective: To characterize the clinical presentation and outcomes of Kawasaki disease (KD) in infants <6 months of age as compared to those ≥6 months in Latin America.
Methods: We evaluated 36 infants <6 months old and 940 infants ≥6 months old diagnosed with KD in Latin America. We compared differences in laboratory data, clinical presentation, treatment response, and coronary artery outcomes between the two cohorts.
Results: The majority (78.1%) of infants and children ≥6 months of age were initially diagnosed with KD, as compared to only 38.2% of infants <6 months. Clinical features of KD were more commonly observed in the older cohort: oral changes (92 vs. 75%, P = 0.0023), extremity changes (74.6 vs. 57.1%, P = 0.029), and cervical lymphadenopathy (67.6 vs. 37.1%, P = 0.0004). Whether treated in the first 10 days of illness or after the 10th day, infants <6 months were at greater risk of developing a coronary artery aneurysm compared to KD patients ≥6 months treated at the same point in the course of illness [ ≤ 10 days (53.8 vs. 9.4%, P = 0.00012); >10 days (50 vs. 7.4%, P = 0.043)].
Conclusion: Our data show that despite treatment in the first 10 days of illness, infants <6 months of age in Latin America have a higher risk of developing a coronary artery aneurysm. Delay in the diagnosis leads to larger coronary artery aneurysms disproportionately in these infants. Thus, suspicion for KD should be high in this vulnerable population.
Kawasaki disease (KD) is a medium-size vessel vasculitis of childhood with a clinical presentation that can be confused with other pediatric febrile illnesses. This can lead to a delay in diagnosis and treatment with intravenous immunoglobulin (IVIG), which in turn can lead to a higher rate of coronary artery abnormalities (CAA) and increased mortality and morbidity (1–6). Despite timely treatment with IVIG within the first 10 days of illness, up to 43.4% of infants <6 months in the United States have been reported to develop CAA (3).
Most of the epidemiological data for patients with KD <6 month of age are from regions outside of Latin America (LA) (2, 6–11). It is unknown whether the clinical presentation and outcomes are similar in infants <6 months in LA populations. Increasing collaborative academic and clinical efforts in Latin America to study the epidemiology and care of KD patients led to the development of a multinational network in LA entitled Red de Enfermedad de Kawasaki en America Latina (REKAMLATINA; Latin American KD Network) (8, 12). We aim to characterize the clinical presentation and outcomes of KD in infants <6 months old as compared to those ≥6 months of age in LA.
All study data were obtained from review of the REKAMLATINA Research Electronic Data Capture (REDCap) database, housed at the University of California San Diego KD Research Center, which contains demographic, clinical and laboratory data from KD patients throughout LA. We reviewed retrospectively collected data from 36 KD subjects <6 months and 940 ≥6 months diagnosed and treated in 16 Latin American countries and 35 hospitals between January 1, 2009, to December 31, 2013.
In accordance with the American Heart Association (AHA) guidelines, complete KD presentation was defined as fever ≥ 5 days and 4 or more of the following clinical signs: erythema and cracking of lips, strawberry tongue, and/or erythema of oral and pharyngeal mucosa; bilateral bulbar conjunctival injection without exudate; polymorphous skin rash; changes such as edema, redness, and/or peeling of the hands or feet; and cervical lymphadenopathy (13). Incomplete KD was defined per the AHA guidelines as fever and fewer than 4 of the KD clinical criteria with either supportive laboratory or an echocardiographic abnormality. Illness day 1 is defined as the first day of fever. Specifics on the treatment course, including treatment with IVIG or antibiotics, was collected as was the presence of IVIG resistance defined as persistent fever (T ≥ 38.0°C rectally or orally) > 36 h but less than 7 days after completion of the first IVIG infusion.
CAAs were classified as normal (Z < 2.5), dilated (Z ≥ 2.5 to ≤ 4), aneurysmal (Z > 4 to ≤ 10), or giant aneurysm (Z > 10) as per the 2004 AHA KD Guidelines by the local site study investigator, given that these were the published guidelines at the time of acquisition of the data (3, 14). For a subset in whom CAA measurements, height and weight were available (N = 481), the internal diameter normalized for body surface area (Z-score) of the proximal right coronary artery (RCA) and left anterior descending artery (LAD) were calculated. Height and weight were verified using age-appropriate normal values for males and females and the body surface area was calculated using the Haycock formula. Z-score was calculated using the formula from Dallaire and Dahdah (15). The maximal Z-score of either the RCA or LAD (Z-max) was identified as the largest Z-score for the subjects within the first 6 weeks of illness. The study received Institutional Review Board approval at the University of California, San Diego as well as at each individual institution enrolling subjects in the REKAMLATINA database.
The primary comparisons were made between infants <6 months old and infants and children ≥6 months old. Differences in counts and categorical variables were compared using two-sided Fisher's exact test. Continuous variables were compared using the Mann-Whitney test. Statistical processing was performed using R version 3.1.0 (available at: http://www.R-project.org) and GraphPad Prism version 8.2.1 (available at: (https://www.graphpad.com).
Over a five-year period, we identified a total of 976 patients <13 years of age with KD in LA. Retrospectively collected demographic and clinical data are presented in Table 1. Of the 976 patients, 36 (3.7%) were <6 months of age. The remaining 940 patients (96.3%) were between 6 months and 12 years of age (Table 1). Most of the children <6 months (25 of 36, 69.4%) were described as white (P = 0.0059). Most subjects were male and there was no difference in sex by age cohort (72.2 vs. 60.9%, P = 0.22). As compared to subjects ≥6 months old, infants <6 months had an illness day at hospitalization of 4 days as compared to illness day 6 (P = 0.00018). The younger cohort had longer hospital stays on average (8 vs. 5 days, P < 0.0001).
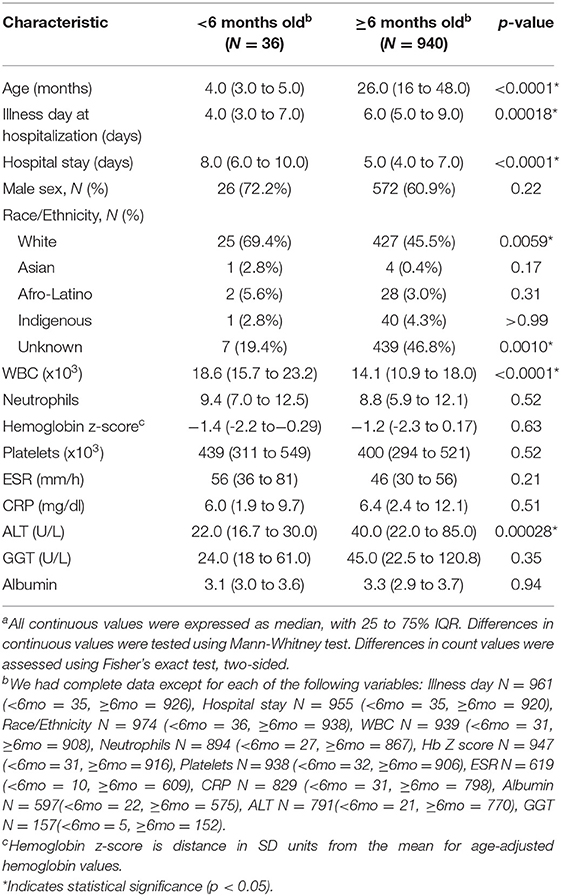
Table 1. Demographic and clinical characteristics of the study populationa.
Infants <6 months had a higher mean white blood cell count at diagnosis (18.6 vs. 14.1, P < 0.0001; Table 1). Other inflammatory markers such as neutrophils, ESR, and platelets were not significantly different between the two age groups. The younger cohort had lower levels of ALT, GGT, and albumin, but only the ALT difference was statistically significant between the age groups (22 vs. 40 U/L, P = 0.00028).
Infants <6 months were less likely to be initially diagnosed with KD (38.2 vs. 78.1%, OR = 0.17, 95% CI 0.084 to 0.35, P < 0.0001) and had an 11-fold increased risk of being diagnosed initially with sepsis or shock (26.5 vs. 2.4%, OR = 14.5, 95% CI 6.0 to 33.8, P < 0.0001) (Table 2). Furthermore, infants <6 months were 4 times more likely to be initially diagnosed with a urinary tract infection (14.7 vs. 3.8%, OR = 4.4, 95% CI 1.7 to 11.5, P = 0.011) and more likely to be suspected of occult bacteremia initially (11.4 vs. 2.3%, OR = 5.4, 95% CI 1.9 to 15.7, P = 0.012) as compared to older infants and children.
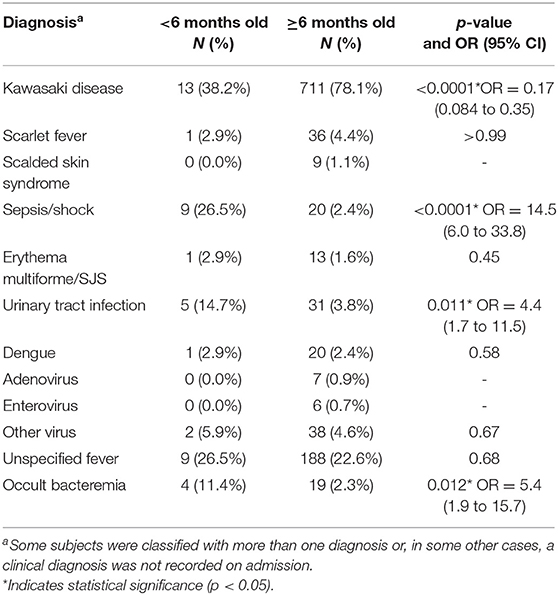
Table 2. Initial clinical diagnosis on admission.
Table 3 describes clinical findings related to diagnostic criteria for KD. Oral changes, including erythematous oropharynx or lips or strawberry tongue, were less commonly noted in the younger patients (75 vs. 92%, OR = 0.26, 95% CI 0.12 to 0.58, P = 0.0023). Cervical lymphadenopathy was also noted less frequently in younger patients (37.1 vs. 67.6%, OR = 0.28, 95% CI 0.14 to 0.55, P = 0.0004), as were extremity changes (57.1 vs. 74.6%, OR = 0.45, 95% CI 0.23 to 0.88, P = 0.029). Subjects were classified as having complete vs incomplete KD, based on AHA 2017 guidelines (13). Overall, we found significantly more older infants and children presenting with complete KD (44.4 vs. 76.6%, OR = 0.24, 95% CI 0.13 to 0.47, P < 0.0001). The younger cohort had over 4-fold greater odds of being diagnosed as incomplete KD compared to their older counterparts (55.6 vs. 23.4%, OR = 4.1, 95% CI 2.1 to 8.0, P < 0.0001).
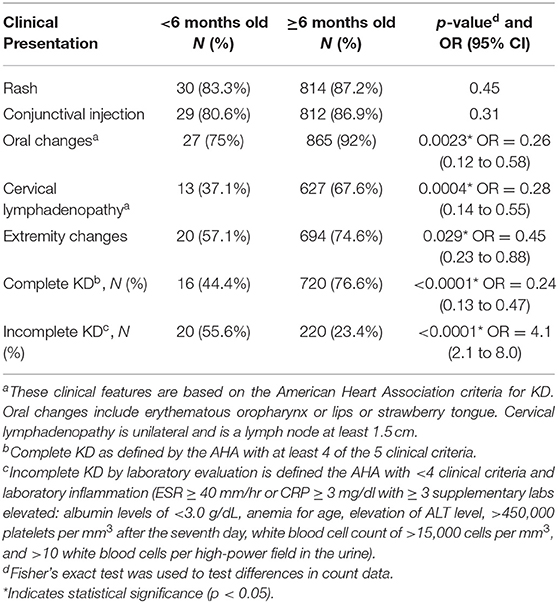
Table 3. Diagnostic criteria for KD.
Table 4 describes IVIG therapy as well as use of antibiotics. The initial use of antibiotics and the treatment of patients ultimately diagnosed with KD with IVIG was high in both groups, though not statistically different between the cohorts.
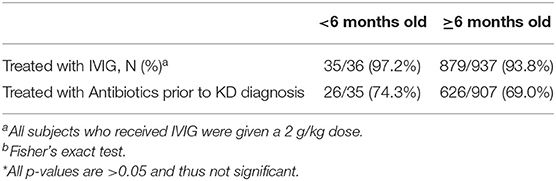
Table 4. IVIG therapy course, IVIG-resistance and rate of antibiotic use*.
Table 5 describes differences in the Z-max of the left anterior descending and right coronary arteries in young vs older KD patients by illness day. For children hospitalized in the first 10 days of illness, infants <6 months increased the aneurysm risk 6-fold compared to those subjects ≥6 months old (53.8 vs. 9.4%, OR = 11.25, 95% Cl 3.87 to 36.25, P = 0.00012). Infants <6 months hospitalized after day 10 of illness had a greater risk of having a giant coronary artery aneurysm as compared to older children (50 vs. 7.4%, OR = 12.50, 95% CI 1.62 to 84.97, P = 0.043). Infants <6 months had a higher baseline Z-score and Z-max compared to older patients, regardless of whether they were hospitalized in the first 10 days or after the 10th day of illness. When diagnosed within the first 10 days of illness, younger patients had a higher baseline Z-score and Z-max compared to older patients (2.37 vs. 0.77, P = 0.0059; 4.55 vs. 1.18, P = 0.0022), respectively. An even greater baseline Z-score and Z-max was observed for younger infants after the 10th day of illness (10.35 vs. 1.65, P = 0.0064; 8.04 vs. 1.86, P = 0.0045).
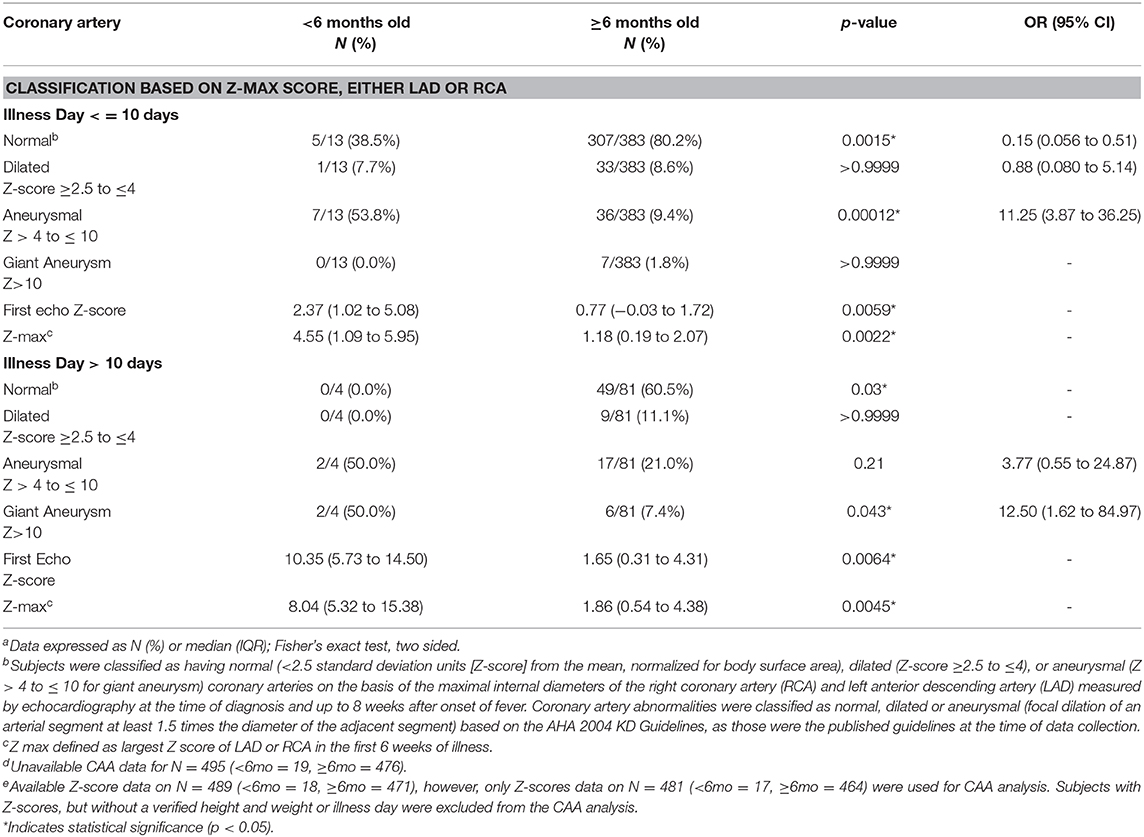
Table 5. Coronary artery abnormalities in KD subjects treated (All)a,d,e.
This is the first study to compare the clinical presentation, initial diagnosis and treatment, and coronary artery outcomes between infants <6 months compared to those 6 months and older throughout LA. As reflected in other recent studies, infants <6 months old with acute KD in LA are more likely to develop CAA than those older than 6 months old (2, 3, 6, 9, 16–18). In this study, based on calculated Z-max scores, 53.8% of infants <6 months with KD had an aneurysm or giant aneurysm compared to the older cohort 11.2%. By comparison, other studies have found ~20% of infants <6 months developed an aneurysm or great aneurysm, whereas only 5% of infants ≥6 months had an aneurysm or great aneurysm (3). In the Rosenfeld et al. study the CAA present in infants <6 months was as high as 79%, compared with 44% of infants ≥6 months (6). Similarly to LA, a high prevalence of coronary artery abnormalities in infants <6 months has been observed in other parts of the globe. In a study from Chandigarh, India it was reported 35% of infants <6 months had coronary artery abnormalities and 65% in a study in Taipei, Taiwan (2, 18). While the increased rate in this cohort may be due to Z-scores only being available in the most severely affected patients, it does warrant assessing whether there is in fact a higher rate of aneurysms in infants in LA in a follow up cohort study. Furthermore, as per the recommendations of the 2017 AHA guidelines, these higher risk infants may benefit from adjunctive therapy.
A novel data-point captured in our database was “Initial Diagnosis.” KD was the initial diagnosis in 74.2% of all subjects, but only in 38.2% of the infants <6 months, as sepsis and a urinary tract infection were the most common initial diagnoses. With nearly all patients being initially treated with antibiotics, it is important to continue to raise awareness that KD is not a diagnosis of exclusion and that in many cases antibiotics are not needed as KD alone is the leading diagnosis.
There are several strengths and limitations to our study. These data are from the largest international network and database of children with KD and provide the demographic and clinical data from an area of the world where little has been published widely about KD. That said, there were a larger proportion of infants and children ≥6 months as compared to those <6 months. For this specific retrospective database, illness day at diagnosis of KD was not available as some sites considered this to be protected health information. Instead illness day at hospitalization was recorded, keeping in mind that in some cases KD was not the initial diagnosis. In addition, Z-score could only be calculated in subjects in whom an accurate weight and height were available for calculating BSA.
In summary, our study shows that despite treatment in the first 10 days of illness, infants <6 months old in LA have a higher risk of developing a coronary artery aneurysm than older KD patients. Delay in the diagnosis leads to larger coronary artery aneurysms disproportionately in these infants. In addition, the majority of infants ultimately diagnosed with KD are initially thought to have an infectious issue initially and thus treated with antibiotics. Thus, the suspicion for KD should be high in infants <6 months old given the likelihood of misdiagnosis and increased risk for coronary artery aneurysm formation.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Review Board at the University of California, San Diego and by the ethics committee at each REKAMLATINA-2 Study participant site. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Presented in part as an abstract at the 9th World Congress of the World Society for Pediatric Infectious Diseases (WSPID 2015). Rio de Janeiro, Brasil. November 18-21, 2015 (19).
AS, RU-G, and AT developed the concept for this project. EM, SG, EB, AP, and AT were responsible for data cleaning and analysis. AT provided mentorship to SG, EM, and AP throughout the study period. All authors contributed to the article and approved the submitted version.
Lorena Franco, Nora Bueno (Hospital Infantil Municipal de Córdoba, Córdoba, Argentina), Jaime Deseda-Tous (Hospital Español Auxilio Mutuo, San Juan, Puerto Rico), Carlos F. Grazioso, Pablo J. Grazioso (Sanatorio Nuestra Sra. Del Pilar/Hospital General San Juan de Dios, Ciudad Guatemala, Guatemala), Mariella Vargas-Gutierrez, Susan Li-Chan, Maria L. Avila-Agüero, Kattia Camacho-Badilla, Alejandra Soriano-Fallas (Hospital Nacional de Niños “Dr. Carlos Sáenz Herrera, Centro de Ciencias Médicas de la Caja Costarricense de Seguro Social, San José, Costa Rica), Paola Pérez-Camacho (Fundación Valle del Lili, Cali, Colombia); Luisa B. Gámez-González (Hospital Infantil de Chihuahua, Chihuahua, México), Giannina Izquierdo, Pilar Picart (Hospital de Niños “Dr. Exequiel González Cortés, Santiago, Chile), Adrián Collia, Alejandro Ellis (Sanatorio Mater Dei, Buenos Aires, Argentina), Maria del Carmen Luis-Álvarez (Hospital Pediátrico Universitario “William Soler,” La Habana, Cuba); Stella Gutierrez, Estefanía Fynn, Elizabeth Assandri (Hospital CASMU, Montevideo, Uruguay), Mario Melgar (Hospital Roosevelt, Ciudad Guatemala, Guatemala), Carlos Daza (Hospital Materno Infantil José Domingo de Obaldía), Jacqueline Levy (Hospital del Niño Dr. José Renán Esquivel, Ciudad Panamá, Panamá), Isabel C. Hurtado-Palacios (Hospital Universitario del Valle, Centro Médico Imbanaco, Cali, Colombia), Angélica Calvache-Burbano, Antonio Fernández, Nelly Chávez-Solórzano, Marianella Layana-Coronel, Denisse Olaya-González (Hospital del Niño “Dr. Francisco de Icaza Bustamante, Guayaquil, Ecuador), Marco A. Yamazaki-Nakashimada, Raymundo Rodríguez-Herrera (Instituto Nacional de Pediatría, Ciudad de México, México), Sarbelio Moreno-Espinosa, Ángel Flores (Hospital Infantil de México Federico Gómez, Ciudad de México, México), Adriana Díaz-Maldonado, Kelly Marquez-Herrera, Roy Sanguino-Lobo (Fundación HOMI Hospital Pediátrico de la Misericordia; Bogotá, Colombia), Natalia Lara (Universidad Nacional de Colombia & Hospital de la Misericordia, Bogotá, Colombia), Diana López-Gallegos (Hospital Infantil Privado, Ciudad de México, México), Neusa Keico Sakita, María Fernanda Pereira Badue, Gabriela Leal (Hospital Das Clinicas da Faculdade Medicina da USP, Sao Paolo, Brazil), Diana C. Medina, Paula Araque (Fundación Cardioinfantil & Universidad El Bosque, Bogotá, Colombia), Pilar Guarnizo, Claudia Stapper, Manuel Huertas-Quiñones, María Fernanda García-Venegas (Fundación Cardioinfantil, Universidad Nacional de Colombia y Universidad del Rosario, Bogotá, Colombia), Pio López (Hospital Universitario del Valle, Cali, Colombia), Mónica Pujadas, Karina Machado, Federica Badía, Alejandra Vomero (Hospital Pediátrico Centro Hospitalario Pereira Rossell, Montevideo, Uruguay), Jaime Patiño, Daniela Cleves (Fundación Valle del Lili, Cali, Colombia), Margarita Martínez-Cruzado (Hospital Español Auxilio Mutuo, San Juan, Puerto Rico), Mario Gamero (Hospital de Niños Benjamín Bloom; San Salvador, El Salvador), Guillermo Soza, Carolina Cerda (Hospital Dr. Hernán Enríquez Aravena, Temuco, Chile), Sergio Bernal-Granillo (Hospital General de Zona 1/IMMS/Hospital Ángeles CMP, San Luis Potosí, México), Belén Amorín (Hospital Escuela del Litoral Paysandú, Paysandú, Uruguay).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Garrido-García LM, Morán-Villaseñor E, Yamazaki-Nakashimada MA, Cravioto P, Galván F. Giant coronary artery aneurysms complicating Kawasaki disease in Mexican children. Cardiol Young. (2018) 28:386–90. doi: 10.1017/S1047951117001470
2. Singh S, Agarwal S, Bhattad S, Gupta A, Suri D, Rawat A, et al. Kawasaki disease in infants below 6 months: a clinical conundrum? Int J Rheum Dis. (2016) 2016:1–5. doi: 10.1111/1756-185X.12854
3. Salgado AP, Ashouri N, Berry EK, Sun X, Jain S, Burns JC, et al. High risk of coronary artery aneurysms in infants younger than 6 months of age with Kawasaki disease. J Pediatr. (2017) 185:112–6.e1. doi: 10.1016/j.jpeds.2017.03.025
4. De Jesús Coria-Lorenzo J, Sotelo-Cruz N, Ramírez-Bouchand D, Enríque-Cisneros O, Díaz-Luna JL, Unda-Gómez JJ, et al. Experiencia de enfermedad de Kawasaki sin evidencia de exantema. Análisis de la Red de Kawasaki de México. Rev Mex Pediatr. (2015) 82:154–8.
5. Wilder MS, Palinkas LA, Kao AS, Bastian JF, Turner CL, Burns JC. Delayed diagnosis by physicians contributes to the development of coronary artery aneurysms in children with Kawasaki syndrome. Pediatr Infect Dis J. (2007) 26:256–60. doi: 10.1097/01.inf.0000256783.57041.66
6. Rosenfeld EA, Corydon KE, Shulman ST. Kawasaki disease in infants less than one year of age. J Pediatr. (1995) 126:524–9. doi: 10.1016/S0022-3476(95)70344-6
7. Sotelo-Cruz N. [A review of Kawasaki disease, a perspective from the articles published in Mexico since January 1977 to May 2012]. Arch Cardiol Mex. (2013) 83:214–22. doi: 10.1016/j.acmx.2013.02.004
8. González-Mata A, Ulloa-Gutiérrez R, Brea J, Soza G, Tremoulet AH. Origin and importance of the Latin American Kawasaki Disease Network (REKAMLATINA). Rev Chilena Infectol. (2014) 31:330–2. doi: 10.4067/S0716-10182014000300012
9. Yoon YM, Yun HW, Kim SH. Clinical characteristics of Kawasaki disease in infants younger than six months: a single-center study. Korean Circ J. (2016) 46:550–5. doi: 10.4070/kcj.2016.46.4.550
10. Friedman KG, Gauvreau K, Hamaoka-Okamoto A, Tang A, Berry E, Tremoulet AH, et al. Coronary artery aneurysms in Kawasaki disease: Risk factors for progressive disease and adverse cardiac events in the US Population. J Am Heart Assoc. (2016) 5:e003289. doi: 10.1161/JAHA.116.003289
11. Burns JC, Wiggins Jr. JW, Toews WH, Newburger JW, Leung DYM, Wilson H, et al. Clinical spectrum of Kawasaki disease in infants younger than 6 months of age. J Pediatr. (1986) 109:759–763. doi: 10.1016/S0022-3476(86)80689-8
12. Ulloa-Gutierrez R, Salgado AP, Tremoulet AH. Kawasaki disease in Latin American children: past, current, and future challenges. J Pediatric Infect Dis Soc. (2014) 3:280–1. doi: 10.1093/jpids/piu105
13. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of kawasaki disease: a scientific statement for health professionals from the american heart association. Circulation. (2017) 135:484. doi: 10.1161/CIR.0000000000000484
14. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on rheumatic fever, endocarditis and kawasaki disease, council on cardiovascular disease in the young, american heart association. Circulation. (2004) 110:2747–71. doi: 10.1161/01.CIR.0000145143.19711.78
15. Dallaire F, Dahdah N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J Am Soc Echocardiogr. (2011) 24:60–74. doi: 10.1016/j.echo.2010.10.004
16. Cameron SA, Carr M, Pahl E, DeMarais N, Shulman ST, Rowley AH. Coronary artery aneurysms are more severe in infants than in older children with Kawasaki disease. Arch Dis Child. (2019) 104:451–5. doi: 10.1136/archdischild-2018-314967
17. Takahashi M, Mason W, Lewis AB. Regression of coronary aneurysms in patients with Kawasaki syndrome. Circulation. (1987) 75:387–94. doi: 10.1161/01.CIR.75.2.387
18. Chang FY, Hwang B, Chen SJ, Lee PC, Meng CC, Lu JH. Characteristics of Kawasaki disease in infants younger than six months of age. Pediatr Infect Dis J. (2006) 25:241–4. doi: 10.1097/01.inf.0000202067.50975.90
19. Salgado A, Ulloa-Gutierrez R, Garrido-Garcia LM, Estripeaut D, Dueñas L, Luciani K, et al. Kawasaki disease in infants <6 months of age in Latin America: a retrospective multinational multicenter study of the REKAMLATINA network. In: 9th World Congress of the World Society for Pediatric Infectious Diseases (WSPID 2015). Rio de Janeiro (2015). Oral Abstract WSPID-0665.
Keywords: Kawasaki disease, Latin America, infants, coronary artery abnormalities, delayed diagnosis
Citation: Moreno E, Garcia SD, Bainto E, Salgado AP, Parish A, Rosellini BD, Ulloa-Gutierrez R, Garrido-Garcia LM, Dueñas L, Estripeaut D, Luciani K, Rodríguez-Quiroz FJ, del Aguila O, Camacho-Moreno G, Gómez V, Viviani T, Alvarez-Olmos MI, de Souza Marques HH, Faugier-Fuentes E, Saltigeral-Simental P, López-Medina E, Miño-León G, Beltrán S, Martínez-Medina L, Pirez MC, Cofré F, Tremoulet AH and the REKAMLATINA-2 Study Group Investigators (2020) Presentation and Outcomes of Kawasaki Disease in Latin American Infants Younger Than 6 Months of Age: A Multinational Multicenter Study of the REKAMLATINA Network. Front. Pediatr. 8:384. doi: 10.3389/fped.2020.00384
Received: 28 February 2020; Accepted: 05 June 2020;
Published: 16 July 2020.
Edited by:
Ruth Heying, University Hospital Leuven, BelgiumReviewed by:
Dimpna Calila Albert-Brotons, King Faisal Specialist Hospital & Research Centre, Saudi ArabiaCopyright © 2020 Moreno, Garcia, Bainto, Salgado, Parish, Rosellini, Ulloa-Gutierrez, Garrido-Garcia, Dueñas, Estripeaut, Luciani, Rodríguez-Quiroz, del Aguila, Camacho-Moreno, Gómez, Viviani, Alvarez-Olmos, de Souza Marques, Faugier-Fuentes, Saltigeral-Simental, López-Medina, Miño-León, Beltrán, Martínez-Medina, Pirez, Cofré, Tremoulet and the REKAMLATINA-2 Study Group Investigators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana H. Tremoulet, YXRyZW1vdWxldEBoZWFsdGgudWNzZC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.