 Ana Cristina Simões e Silva
Ana Cristina Simões e Silva
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr. , 15 May 2020
Sec. Neonatology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00276
This article is part of the Research Topic Coronavirus Disease (COVID-19): Pathophysiology, Epidemiology, Clinical Management and Public Health Response View all 400 articles
At the end of 2019, in Wuhan (China), the onset of a disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was observed. The disease, named COVID-19, has a wide spectrum of clinical presentations, ranging from asymptomatic or mild to critical, and for some patients the disease is even fatal. Apparently, being a child or being pregnant does not represent an additional risk for adverse outcomes. The purpose of this mini-review was to investigate what is in the scientific literature, so far, in regard to vertical transmission of SARS-CoV-2. Data were obtained independently by the two authors, who carried out a systematic search in the PubMed, Embase, LILACS, Cochrane, Scopus and SciELO databases using the Medical Subject Heading terms “coronavirus,” “COVID-19,” and “vertical transmission.” Few studies about the vertical transmission of SARS-CoV-2 are found in the literature. In all case reports and case series, the mothers' infection occurred in the third trimester of pregnancy, there were no maternal deaths, and most neonates had a favorable clinical course. The virus was not detected in the neonate nasopharyngeal swab samples at birth, in the placenta, in the umbilical cord, in the amniotic fluid, in the breast milk or in the maternal vaginal swab samples in any of these articles. Only three papers reported neonatal SARS-CoV-2 infection, but there is a bias that positive pharyngeal swab samples were collected at 36 h and on the 2nd, 4th, and 17th days of life. The possibility of intrauterine infection has been based mainly on the detection of IgM and IL-6 in the neonates' serum. In conclusion, to date, no convincing evidence has been found for vertical transmission of SARS-CoV-2.
At the end of 2019, in Wuhan (China), the onset of a disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was observed. SARS-CoV-2 caught the attention of the entire world due to its great potential for dissemination in a short time and soon gained the status of a public emergency of international concern. As of March 31, 2020, the World Health Organization (WHO) has reported a total of 750,890 cases and 36,405 deaths related to SARS-CoV-2 infection on its official website1.
The disease associated with SARS-Co-V-2 infection, designated by the WHO as COVID-19, has a wide spectrum of clinical presentations, ranging from asymptomatic or mild to critical, and for some patients the disease is even fatal. Most fatal cases have occurred in individuals with advanced age or with underlying medical conditions, including cardiovascular diseases, diabetes, and hypertension, among others (1). Apparently, being a child or being pregnant does not represent an additional risk for adverse outcomes (2).
SARS-CoV-2 is part of the family Coronaviridae, a family of enveloped, positive single-stranded large RNA viruses, which also includes severe acute respiratory syndrome coronavirus (SARS-CoV), discovered in 2003 (3), and Middle East respiratory syndrome coronavirus (MERS-CoV), discovered in 2012 (4). The viruses have bats and other mammals as natural reservoirs. Animal-human and human-human transmissions are very fast. Both viruses came into evidence after two major outbreaks of respiratory diseases, in China, in 2002–2003 for SARS-CoV and, in the Middle East, in 2012, for MERS-CoV. The mortality rates were estimated to be over 10% for SARS-CoV infection and >35% for MERS-CoV infection (5). Most coronaviruses are viruses that are highly pathogenic and have the potential to produce serious infections of the lower respiratory tract. Unlike what is observed among those infected with SARS-CoV-2, pregnant patients infected with SARS-CoV tend to have a high rate of adverse outcomes when compared to no pregnant women (6). However, no proven cases of vertical transmission of SARS-CoV or MERS-CoV have yet been described (7, 8). In this context, the purpose of this text was to investigate what is in the scientific literature, so far, in regard to the possibility of vertical transmission of SARS-CoV-2.
Data were obtained independently by the two authors, who carried out a comprehensive and systematic search in the PubMed, Embase, LILACS, Cochrane, Scopus and SciELO databases. Search strategies included the Medical Subject Heading terms “coronavirus,” “COVID-19,” and “vertical transmission.” The filters used were the reading of the title and abstract of the articles. The articles obtained were case reports or case series of women infected with SARS-CoV-2 during pregnancy or of neonates born to infected mothers. We found 10 articles to be included for a critical analysis in this review (9–18).
Due to the recent nature of the disease, few studies are found in the literature about the vertical transmission of SARS-CoV-2. In all case reports and case series, the mothers' infection occurred in the third trimester of pregnancy, there were no maternal deaths, and most neonates had a favorable clinical course. The methodology varied among studies, but in most articles, serum samples and swabs from the newborn's pharynx, samples of breast milk and samples of products of conception (placenta, amniotic fluid and umbilical cord blood) were collected for further laboratory testing (9–18). The main characteristics of each study are shown in Table 1. With the exception of two patients (17), all had cesarean section deliveries and without skin-to-skin contact with the newborn in the delivery room. Only in the study by Zhu et al. (17) was there a neonatal death. The case was a male newborn with a gestational age of 34 + 5/7 weeks. The newborn stayed in the hospital from the first day of life due to respiratory distress, and his condition deteriorated on the eighth day of life to refractory shock, multiple organ failure and disseminated intravascular coagulation; he died on the ninth day of life. The nasopharyngeal swab of this newborn, collected at birth, was negative for SARS-CoV-2. In all other studies, there were no fetal deaths, neonatal deaths or cases of severe intrauterine asphyxia. The virus was not detected in the neonate nasopharyngeal swab samples at birth, in the placenta, in the umbilical cord, in the amniotic fluid, in the breast milk or in the maternal vaginal swab samples in any of these articles (9–18). Only one study showed a SARS-CoV-2-positive pharynx swab, but the sample was collected at 36 h of age (13). Additional results were also found and were used to support the possibility of vertical infection by SARS-CoV-2 in two studies (14, 15): high levels of IgM for SARS-CoV-2 in the blood of neonates and increased concentrations of cytokines, including IL-6 and IL-10. It is important to mention that products of conception were not tested in these two studies.
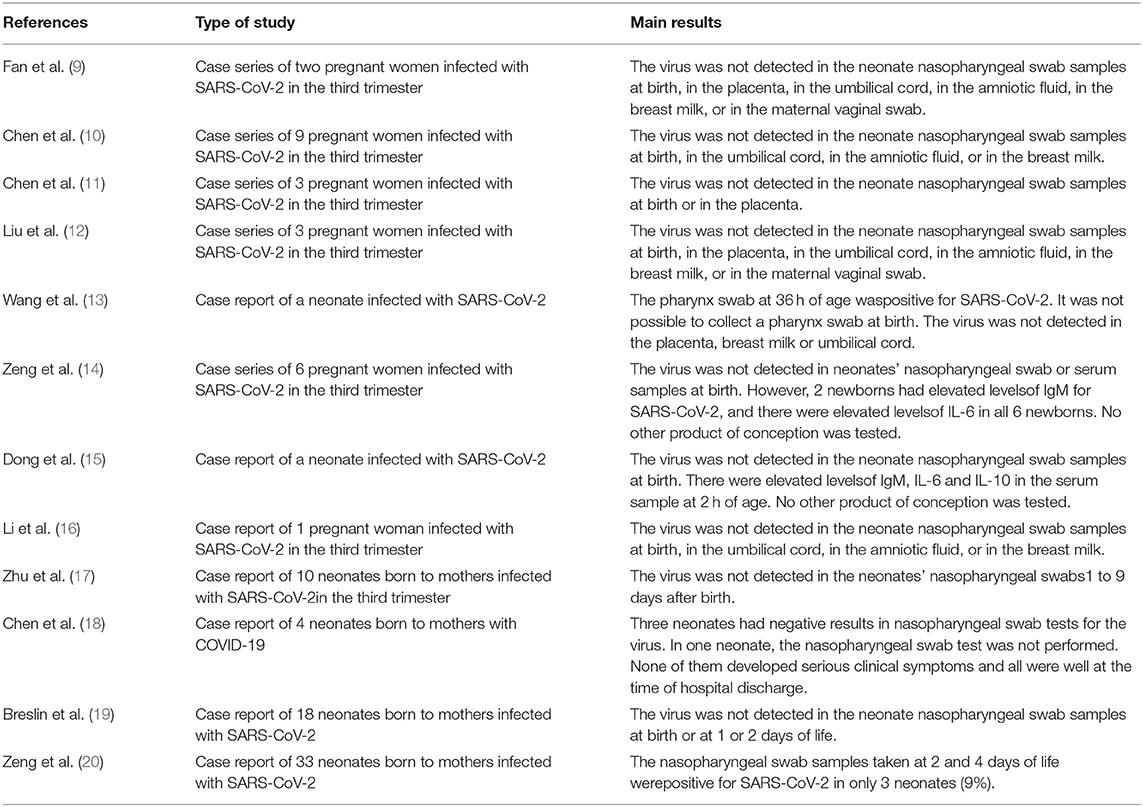
Table 1. Summary of studies about vertical transmission of SARS-CoV-2.
Concerning the outcomes of pregnant women and their newborns, these studies did not report deaths of the mothers, and most of the newborns were discharged in good health conditions (9–20).
After analyzing these studies, no convincing evidence was found for vertical transmission of SARS-CoV-2 in pregnant women infected during the third trimester of pregnancy, as also reported for SARS-CoV infection (21). SARS-CoV-2 was not detected in any of the patients analyzed in these papers in the amniotic fluid, placenta or umbilical cord using the reverse-transcription polymerase chain reaction (RT-PCR) technique. Currently, the RT-PCR technique in a sample of respiratory tract secretions—nasopharyngealswabs, sputum or bronchoalveolar lavage, for example—is considered the gold standard for the diagnosis of SARS-CoV-2 infection due its high specificity (22). However, the method presents some limitations, including the non-negligible number of false-negative results, the time necessary to obtain results and the need forspecialized equipment to perform the test (23). A positive RT-PCR test usually confirms the diagnosis, but in the case of a negative test when infection is very probable, samples from other sites in the respiratory tract should be analyzed, according to WHO guidelines, to increase the accuracy (24). False-negative tests can occur due to the limit of detection (LoD), which is the lowest concentration of viral RNA that can be detected by the technique at least 95% of the time (25).
There was no report of positivity of the nasopharyngeal swab PCR test of neonates at birth. Only three papers (13, 20, 26) reported neonatal SARS-CoV-2 infection, but there is a bias that positive pharyngeal swab samples were collected at 36 h and on the 2nd, 4th, and 17th day of life. Therefore, the possibility of nosocomial infection cannot be ruled out. In general, infants born to mothers with COVID-19 have a favorable clinical course (9–20).
An interesting issue to be analyzed is the difference in the clinical course between pregnant patients infected with SARS-CoV-2 and those infected with SARS-CoV. After the SARS-CoV epidemic that occurred in 2003–2004 in Asia, some studies showed that the infection led to some unfavorable outcomes in pregnant women, such as preterm delivery, spontaneous abortions and restricted intrauterine growth (27). The most recent data show that fetal complications related to SARS-CoV-2 maternal infection exist, but the rates are not high, with an estimated rate of miscarriage of ~2% and of restricted intrauterine growth of ~10% (28). In the case of SARS-CoV infection (27), a review (7) regarding the possibility of vertical transmission ofSARS-CoV was carried out based on a case series (29) including a total of 12 pregnant women: 7 infected during the first trimester and 5 infected during the second or third trimesters. In the first group, 4 women had spontaneous abortions. In the second group, all had live births, but 3 needed urgent cesarean sections; in those two who did not require early obstetric intervention, oligohydramnios and severe fetal growth restriction were found. The virus was not found in samples of amniotic fluid, blood culture of the newborn or endotracheal aspirate of the newborn in any of the patients. None of the neonates showed dysmorphisms at birth. In addition, all of the neonates exhibited a clinical course similar to that of other neonates under the same clinical conditions (7).
A recent editorial by Kimberlin and Stagno (30) discussed two articles (14, 15) that raised the possibility of intrauterine infection by showing high levels of IgM for SARS-CoV-2 and the cytokine IL-6 in neonate serum. In the case series of Zheng et al. (14), none of the 6 neonates had a SARS-CoV-2-positive nasopharynx swab at birth, nor was the virus identified in the serum, but 2 samples showed SARS-CoV-2-positive IgM, and in all samples, there were high levels of IL-6. In the case report by Dong et al. (15), there were high levels of IgM for SARS-CoV-2 and IL-6 and IL-10 at 2 h of life, but the nasopharynx swab was negative. The editorial then questions the reliability of IgM detection to determine intrauterine infection. Due to its molecular mass, IgM generally does not cross the placental barrier in large quantities, but the transfer of some types of immunoglobulins that do not normally cross the placental barrier (such as IgM or IgA) can happen in normal situations, even in small quantities, and this can be intensified in special situations, such as the inflammation of the birth canal (31). In addition, tests for the detection of IgM frequently present false-negative and false-positive results. For example, the first-generation IgM enzyme-linked immunosorbent assay test had a sensitivity of ~70% and a specificity of ~95% for congenital cytomegalovirus infection (30). The editorial also points out that the sharp decline in IgM levels in a short time does not show the same behavior as that shown for other congenital infections, such as rubella or Zikavirus infection (29).
It should also be noted that the cytokine IL-6 is a soluble mediator of the immune system response. IL-6 stimulates the body's defense response in several situations, including infections or autoimmune diseases. Its action on the pathogenesis of COVID-19 has been studied recently, and its measurement may have a fatality prediction value in adult patients (32). However, as with IgM, the assessment of IL-6 levels in neonates cannot be considered a good standard for the determination of whether vertical transmission of SARS-CoV-2 occurs, since IL-6 can pass through the placenta (33).
Thus, we considered that the assumption of vertical transmission of SARS-CoV-2 is not possible based only on the positivity of IgM antibodies or high levels of IL-6 in the neonate. Further studies are needed to assess the reliability of the assessment of neonatal IgM and other molecules, such as IL-6, in maternal SARS-CoV-2 infection. In addition, in the case series of Zheng et al. (14) and in the case report of Dong et al. (15), the virus was not detected in any laboratory examination, including nasopharynx swab of the newborn at birth, or in any product of conception.
In summary, unlike pregnant women infected with other coronaviruses (SARS-CoV or MERS-CoV) (7, 8, 17, 34), those infected with SARS-CoV-2 are not prone to unfavorable pregnancy outcomes. Additional studies are needed to assess whether there is in fact vertical transmission of the virus. To date, the possibility of intrauterine infection has been based mainly on the detection of IgM and IL-6 in neonates' serum. Studies that detected the virus in neonatal nasopharyngeal swabs did so hours or days after birth; therefore, the possibility of nosocomial infection cannot be ruled out. In addition, the virus was not detected in products of conception or breast milk. It should also be noted that pregnant women infected with SARS-CoV-2 have the same clinical course as non-pregnant women, and until now, all neonates with suspected COVID-19 due to vertical transmission of SARS-CoV-2 have had, in general, favorable evolution.
AS and CL independently performed the search of the literature, analyzed the articles, wrote the manuscript, and approved the final version. AS submitted the manuscript.
The authors acknowledge Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; grant #301037/2016-7 and grant #302153/2019-5).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. ^Available online at: https://www.who.int/emergencies/diseases/novelcoronavirus-2019/situation-reports/ (accessed March 31, 2020).
1. Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med. (2020) 20:124–7. doi: 10.7861/clinmed.2019-coron
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease (2019) (COVID-19) outbreak in china: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. (2020) 323:1239–42. doi: 10.1001/jama.2020.2648
3. Ksiazek TG, Erdman D, Goldsmith CS, Zaki SR, Peret T, Emery S, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. (2003) 348:1953–66. doi: 10.1056/NEJMoa030781
4. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. (2012) 367:1814–20. doi: 10.1056/NEJMoa1211721
5. Song Z, Xu Y, Bao L, Zhang L, Yu P, Qu Y, et al. From SARS to MERS, thrusting coronaviruses into the spotlight. Viruses. (2019) 11:59. doi: 10.3390/v11010059
6. Lam CM, Wong SF, Leung TN, Chow KM, Yu WC, Wong TY, et al. A case-controlled study comparing clinical course and outcomes of pregnant and non-pregnant women with severe acute respiratory syndrome. BJOG. (2004) 111:771–4. doi: 10.1111/j.1471-0528.2004.00199.x
7. Ng PC, Leung CW, Chiu WK, Wong SF, Hon EK. SARS in newborns and children. Biol Neonate. (2004) 85:293–8. doi: 10.1159/000078174
8. Schwartz D, Graham AL. Potential maternal and infant outcomes from coronavirus 2019-nCoV (SARS-CoV-2) infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses. (2020) 12:194. doi: 10.3390/v12020194
9. Fan C, Lei D, Fang C, Li C, Wang M, Liu Y, et al. Perinatal transmission of COVID-19 associated SARS-CoV-2: should we worry? Clin Infect Dis. (2020) ciaa226. doi: 10.1093/cid/ciaa226. [Epub ahead of print].
10. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. (2020) 395:809–15. doi: 10.1016/S0140-6736(20)30360-3
11. Chen S, Huang B, Luo DJ, Li X, Yang F, Zhao Y, et al. Pregnant women with new coronavirus infection: a clinical characteristics and placental pathological analysis of three cases. Zhonghua Bing Li XueZaZhi. (2020) 49:E005. doi: 10.3760/cma.j.cn112151-20200225-00138
12. Liu W, Wang Q, Zhang Q, Chen L, Chen J, Zhang B, et al. Coronavirus disease 2019 (COVID-19) during pregnancy: a case series. Preprint. (2020) 2020:2020020373.
13. Wang S, Guo L, Chen L, Liu W, Cao Y, Zhang J, et al. A case report of neonatal COVID-19 infection in China. Clin Infect Dis. (2020) ciaa225. doi: 10.1093/cid/ciaa225. [Epub ahead of print].
14. Zeng H, Xu C, Fan J, Tang Y, Deng Q, Zhang W, et al. Antibodies in infants born to mothers with COVID-19 pneumonia. JAMA. (2020). doi: 10.1001/jama.2020.4861. [Epub ahead of print].
15. Dong L, Tian J, He S, Zhu C, Wang J, Liu C, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. (2020). doi: 10.1001/jama.2020.4621. [Epub ahead of print].
16. Li Y, Zhao R, Zheng S, Chen X, Wang J, Sheng X, et al. Lack of vertical transmission of severe acute respiratory syndrome coronavirus 2, China. Emerg Infect Dis. (2020) 26. doi: 10.3201/eid2606.200287
17. Zhu H, Wang L, Fang C, Peng S, Zhang L, Chang G, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. TranslPediatr. (2020) 9:51–60. doi: 10.21037/tp.2020.02.06
18. Chen Y, Peng H, Wang L, Zhao Y, Zeng L, Gao H, et al. Infants Born to Mothers With a New Coronavirus (COVID-19). Front Pediatr. (2020) 8:104. doi: 10.3389/fped.2020.00104
19. Breslin N, Baptiste C, Gyamfi-Bannerman C, Miller R, Martinez R, Bernstein K, et al. COVID-19 infection among asymptomatic and symptomatic pregnant women: two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am J Obstetr Gynecol. (2020) 100118. doi: 10.1016/j.ajogmf.2020.100118. [Epub ahead of print].
20. Zeng L, Xia S, Yuan W, Yan K, Xiao F, Shao J, et al. Neonatal early-onset infection with sARS-CoV-2 in 33 neonates born to mothers with COVID-19 in Wuhan, China. JAMA Pediatr. (2020). doi: 10.1001/jamapediatrics.2020.0878. [Epub ahead of print].
21. Shek CC, Ng PC, Fung GP, Cheng FW, Chan PK, Peiris MJ, et al. Infants born to mothers with severe acute respiratory syndrome. Pediatrics. (2003) 112:e254. doi: 10.1542/peds.112.4.e254
22. Centers for Disease Control and Prevention. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Persons Under Investigation (PUIs) for Coronavirus Disease 2019. (COVID-19). (2020). Available online at: https://www.cdc.gov/coronavirus/2019-nCoV/lab/guidelines-clinical-specimens.html (accessed March 31, 2020).
23. Li Z, Yi Y, Luo X, Xiong N, Liu Y, Li S, et al. Development and clinical application of a Rapid IgM-IgG Combined Antibody Test for SARS-CoV-2 infection diagnosis. J Med Virol. (2020). doi: 10.1002/jmv.25727. [Epub ahead of print].
24. World Health Organization. Coronavirus disease (COVID-19) Technical Guidance: Surveillance and Case Definitions. Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/surveillance-and-case-definitions (accessed March 31, 2020).
25. Panther Fusion SARS-CoV-2 (Hologic, Inc.). Manufacturer Instructions/Package. U. S. Food & Drug Administration. (2020). Available online at: https://www.fda.gov/media/136156 (accessed April 1, 2020).
26. Schwartz DA. An analysis of 38 pregnant women with COVID-19, their newborn infants, and maternal-fetal transmission of SARS-CoV-2: maternal coronavirus infections and pregnancy outcomes. Arch Pathol Lab Med. (2020). doi: 10.5858/arpa.2020-0901-SA. [Epub ahead of print].
27. Jamieson DJ, Jernigan DB, Ellis JE, Treadwell TA. Emerging infections and pregnancy: West Nile virus, monkeypox, severe acute respiratory syndrome, and bioterrorism. Clin Perinatol. (2005) 32:765–76. doi: 10.1016/j.clp.2005.04.008
28. Dashraath P, Jeslyn Wong JL, Karen Lim MX, Lim LM, Li S, Biswas A, et al. Coronavirus disease (2019) (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol. (2020). doi: 10.1016/j.ajog.2020.03.021. [Epub ahead of print].
29. Wong SF, Chow KM, Leung TN, Ng WF, Ng TK, Shek CC, et al. Pregnancy and perinatal outcomes of women with severe acute respiratory syndrome. Am J ObstetGynecol. (2004) 191:292–7. doi: 10.1016/j.aog.2003.11.019
30. Kimberlin DW, Stagno S. Can SARS-CoV-2 infection be acquired in utero? JAMA. (2020). doi: 10.1001/jama.2020.4868. [Epub ahead of print].
31. Ben-Hur H, Gurevich P, Elhayany A, Avinoach I, Schneider DF, Zusman I. Transport of maternal immunoglobulins through the human placental barrier in normal pregnancy and during inflammation. Int J Mol Med. (2005) 16:401–7. doi: 10.3892/ijmm.16.3.401
32. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
33. Zaretsky MV, Alexander JM, Byrd W, Bawdon RE. Transfer of inflammatory cytokines across the placenta. Obstet Gynecol. (2004) 103:546–50. doi: 10.1097/01.AOG.0000114980.40445.83
Keywords: SARS-CoV-2, COVID-19, vertical transmission, pregnant women, neonate, intrauterine infection
Citation: Simões e Silva AC and Leal CRV (2020) Is SARS-CoV-2 Vertically Transmitted? Front. Pediatr. 8:276. doi: 10.3389/fped.2020.00276
Received: 02 April 2020; Accepted: 30 April 2020;
Published: 15 May 2020.
Edited by:
Maximo Vento, University and Polytechnic Hospital of La Fe, SpainReviewed by:
Claus Klingenberg, Arctic University of Norway, NorwayCopyright © 2020 Simões e Silva and Leal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Cristina Simões e Silva, acssilva@hotmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.