 Anne Lee Solevåg
Anne Lee Solevåg Georg M. Schmölzer
Georg M. Schmölzer Po-Yin Cheung
Po-Yin Cheung- 1Department of Paediatric and Adolescent Medicine, Akershus University Hospital, Lørenskog, Norway
- 2Neonatal Research Unit, Centre for the Studies of Asphyxia and Resuscitation, Royal Alexandra Hospital, Edmonton, AB, Canada
- 3Department of Pediatrics, University of Alberta, Edmonton, AB, Canada
Background: Previous studies have investigated hemodynamic recovery using 21% vs. 100% oxygen during cardiopulmonary resuscitation (CPR) with chest compression (CC) in term infants. Animal studies indicate that systemic circulatory recovery is the same whether 21 or 100% oxygen is used during neonatal CPR. One of the main goals of resuscitation is to maintain cerebral oxygen delivery and prevent cerebral hypo- and hyperoxygenation. Oxygen delivery to the brain depends on cerebral hemodynamics, concentration of inhaled oxygen and blood oxygen content. The aim of this paper was to synthesize available research about cerebral oxygen delivery during CPR using different oxygen concentrations. Our research questions included how do different oxygen concentrations during CPR with CC influence cerebral perfusion and oxygen delivery, and how do cerebral hemodynamics during CC influence outcomes.
Methods: A search in Medline Ovid using the search terms hypoxia AND oxygen AND cerebrovascular circulation AND infant, newborn. Inclusion criteria included studies of hypoxia and resuscitation of term infants. Studies were excluded if no measures of cerebral blood flow (CBF), oxygenation, or perfusion were reported.
Results: The search retrieved 21 papers. None of the studies directly fulfilled our inclusion criteria. The reference lists of some of the retrieved papers provided relevant animal studies with slightly conflicting results regarding blood flow and oxygen delivery to the brain using 21 or 100% oxygen. No study in term infants was identified, but we included one study in preterm infants. Studies in asphyxiated animals indicate that 100% oxygen increases CBF and oxygenation during and after CC with a potential increase in oxidative stress.
Conclusion: In asphyxia, cerebral autoregulation may be impaired. Pure oxygen administration during CC may result in cerebral hyperperfusion and increased cerebral oxygen delivery, which may be associated with oxidative stress-related damage to the brain tissue. As systemic circulatory recovery is the same whether 21 or 100% oxygen is used during neonatal CPR, it is important to investigate whether brain damage could be aggravated when 100% oxygen is used.
Introduction
Despite a lack of scientific evidence, supplemental oxygen has been used in neonatal resuscitation for more than 200 years (1). For the last few decades, research has been focused on the balancing benefits and potential harms associated with different oxygen concentrations used in delivery room resuscitation. In term infants exposed to a high initial oxygen concentration in the delivery room, neonatal mortality is increased (2). Since 2010, an initial oxygen concentration of 21% has been recommended to term infants that require assisted ventilation, but 100% oxygen is recommended as soon as chest compression (CC) is needed (3). Exposure to oxygen during resuscitation can be limited in two ways, either by reducing the fraction of inspired oxygen (FiO2) or by limiting the time of exposure (4). In term infants, the oxygen concentration has been the focus of interest, although some animal studies have addressed the effect of very brief (e.g., 3 min) or limited exposure to 100% oxygen (5–7). No study has assessed the safety and effect of different oxygen exposures after return of spontaneous circulation (ROSC) in term asphyxiated infants, i.e., cumulative oxygen exposure. In addition, long-term data applicable to term infants after CC are lacking. Although data from the Canadian Neonatal Network indicated an increased risk of neurodevelopmental impairment in premature infants <29 weeks resuscitated with 100% oxygen (8), a meta-analysis of eight studies showed no difference in the risk of bronchopulmonary dysplasia, intraventricular hemorrhage >grade 3, or death in premature infants <29 weeks of gestation receiving higher vs. lower oxygen strategies in the delivery room (9). In premature infants <32 weeks of gestation, Oei et al. (10) aimed to examine disability at 2 years after initial delivery room exposure to 21 or 100% oxygen. FiO2 was adjusted to target SpO2 65–95% at 5 min and 85–95% until admission to the neonatal intensive care unit. At 2 years of age, 215 out of 240 survivors were assessed (11). There was no difference in disability between infants initially receiving 21% vs. 100% oxygen (11). This was in agreement with a meta-analysis of two trials (n = 208) that showed no difference in neurodevelopmental disability at 18–24 months between premature infants (<32 weeks and extremely low birth weight, respectively) receiving lower (FiO2 < 0.4) vs. higher (FiO2 > 0.4) initial oxygen concentrations targeted to oxygen saturation (12).
One of the main goals of resuscitation is to maintain cerebral oxygen delivery and prevent cerebral hypo- and hyperoxygenation (13). Cerebral oxygen delivery is determined by cerebral hemodynamics, concentration of inhaled oxygen, and blood oxygen content as determined by pulmonary gas exchange and hemoglobin concentration (14). Cerebral hemodynamic measurements include cerebral blood flow (CBF) and cerebral blood flow velocity (CBFV). Both hypoxemia and hyperoxemia influence CBF (15). A review (16) and a meta-analysis (17) have concluded that 21% oxygen is equivalent to 100% oxygen regarding the rate of and time to ROSC, as well as post resuscitation mortality and morbidity in asphyxiated animals The aim of this paper is to provide an overview of studies that assessed CBF, directly or indirectly, during cardiopulmonary resuscitation (CPR) including CC with different FiO2. Our research questions were how did FiO2 during CPR with CC influence cerebral perfusion and oxygenation, and how did cerebral hemodynamics during CC influence outcomes. We hypothesized that cerebral autoregulation was impaired in infants that required delivery room CPR with CC, and that high cerebral perfusion and oxygen delivery was not beneficial.
Materials and Methods
A search in Medline Ovid was performed in July 2019 including the search terms hypoxia AND oxygen AND cerebrovascular circulation AND infant, newborn. Conference proceedings and the reference list of retrieved papers were hand searched for relevant researchers and papers. Publications were assessed based on title, abstract, and methods. Studies were included if they addressed hypoxia and resuscitation in term infants. Studies were excluded if no measures of CBF/perfusion and/or oxygenation were reported, or if they were in a different language than English or Scandinavian.
Results
Results of the Literature Search
(1) The Medline Ovid search retrieved 21 papers that were all excluded: 7 because they addressed premature infants (18–24). One paper in Japanese (25) and one in German (26) was excluded, and 12 papers did not address resuscitation (27–38). From the reference list of (21), we identified (4), which further identified (39).
(2) Papers that we identified from hand searches of conference proceedings and reference lists: there were no clinical data evaluating cerebral hemodynamics and oxygenation during CC in newborn term infants, but four animal studies were identified where CBF/perfusion and/or oxygenation were reported during CC (Table 1 presents CBF/perfusion/oxygen data).
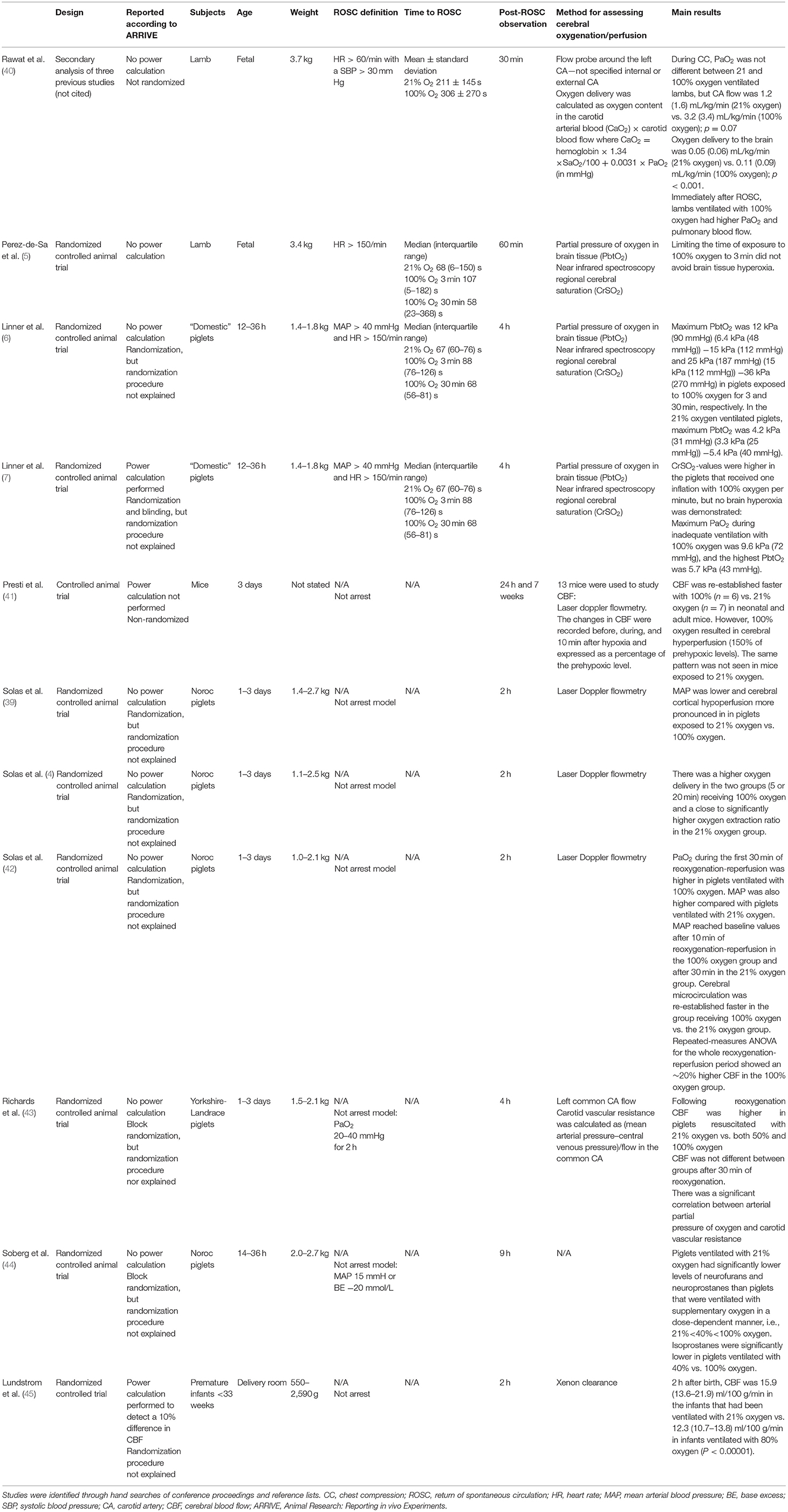
Table 1. Study design, subjects, and main findings related to cerebral oxygenation/perfusion.
Table 1 gives an overview of the studies identified through hand searches with regards to study design, subjects and main findings related to cerebral oxygenation/perfusion and oxygenation.
Rawat et al. (40) performed secondary analyses of data from transitional lambs with cardiac arrest induced by umbilical cord occlusion (PaCO2 125 mmHg = 16.7 kPa). After 5 min of asystole, ventilation was initiated with 21% oxygen. When CC was started, oxygen was increased to 100% (n = 25) or kept at 21% (n = 9). Lambs were observed for 30 min after ROSC during which FiO2 was titrated to a preductal SpO2 85–95%. All lambs achieved ROSC after the same number of epinephrine doses. The authors concluded that carotid artery (CA) flow, systemic PaO2, and oxygen delivery to the brain were very low during CC irrespective of ventilation with 21 or 100% oxygen during CPR.
From the reference list of Rawat et al. (40), we identified a randomized trial by Perez-de-Sa et al. (5). They examined asphyxiated (PaCO2 17 kPa = 127 mmHg) transitional lambs; CC was performed with 21% oxygen (n = 7) or 100% oxygen for 3 min (n = 6) or 30 min (n = 6). Systemic circulatory recovery measured by heart rate and blood pressure was similar in the three groups. One lamb randomized to resuscitation with oxygen for 30 min was excluded because of anemia. The remaining lambs survived to completion of the protocol. Messenger ribonucleic acid expression in the brain of interleukin (IL)-1ß, IL-12, and IL-18 were not different between the groups.
Also, from the reference list of Rawat et al. (40), we identified a randomized trial by Linner et al. (6) who used asphyxiated (PaCO2 21 kPa = 157 mmHg) piglets to investigate if ventilation with 100% oxygen [for 3 min (n = 12) + for 30 min (n = 13)], instead of 21% oxygen (n = 13) would improve ROSC during CC. One piglet resuscitated with 21% oxygen did not achieve ROSC, whereas one piglet that was assigned to ventilation with oxygen for 30 min achieved ROSC, but died 10 min after initiation of ventilation. The time to recovery of cerebral oxygenation was defined as the time when CrSO2 reached 30%, and when PbtO2 had increased 0.1 kPa (0.75 mmHg) from its lowest level. They concluded that shortening the time of exposure to 100% oxygen to 3 min did not prevent brain tissue hyperoxia.
In a randomized controlled trial, Linner et al. (7) used the same piglet model to investigate whether one inflation per minute with 100% oxygen (n = 8) would improve recovery compared to one inflation per minute with 21% oxygen (n = 8). The setup was designed to mimic a situation with severely inadequate ventilation. At the end of 10 min of inadequate ventilation, the 21% oxygen group had a higher lactate and lower PaCO2 than the oxygen group. Two animals in the 21% oxygen group did not achieve ROSC.
(3) Several studies where no CC was provided were included to supplement the scarce data available from CC animal studies (Table 1).
Supplemental Oxygen Increases CBF
Presti et al. (41) investigated CA ligated neonatal and adult mice that had been exposed to 20 min of 8% oxygen, followed by 30 min of 21 or 100% oxygen. PaCO2 values were not reported, but presumably, this was a model of normocapnia.
Laser Doppler flowmetry revealed a CBF of 150% of prehypoxic levels in mice exposed to 100% oxygen. Neonatal mice exposed to 100% oxygen (n = 32) had significantly delayed geotaxis reflex at 24 h, when compared with neonatal mice exposed to 21% oxygen (n = 37). In contrast, adult mice exposed to 100% oxygen (n = 18) demonstrated significantly better spatial learning and orientation with a tendency toward better memory preservation vs. mice exposed to 21% oxygen (n = 27). There was a trend toward a higher mortality among 100% resuscitated mice vs. those resuscitated with 21% oxygen.
In a randomized controlled design, Solas et al. (39) used a piglet model of cerebral hypoxemia-ischemia (8% oxygen and bilateral common CA occlusion) and demonstrated a significantly higher mean arterial blood pressure (MAP) and faster re-establishment of cerebral cortical microcirculation during ventilation with 100% oxygen for 30 min (n = 12) compared with 21% oxygen (n = 12) (39). Excitatory amino acids in the striatum were higher in the 21% oxygen group. No pig died in either group.
The investigators subsequently added moderate hypercapnia (mean PaCO2 8.4 kPa = 63 mmHg) to the model and confirmed that cerebral cortical microcirculation was higher when piglets were ventilated with 100% oxygen for 5 min (n = 12) or 20 min (n = 12) compared with 21% oxygen (n = 12) (4). There were no differences in biochemical markers including excitatory amino acids in the striatum between the groups. No pig died in either group.
In a third randomized study by Solas et al. (42), piglets with moderate hypercapnia to more closely simulate perinatal asphyxia, were subjected to 20 min of combined hypoxemia-ischemia-hypercapnia followed by reperfusion and reoxygenation: (1) with 100% oxygen for the first 30 min and then 21% oxygen for another 90 min (n = 11), or (2) with 21% oxygen for 120 min (n = 13). No differences in biochemical markers were found between the two groups. No pig died in either group.
Supplemental Oxygen Reduces CBF
In a randomized controlled trial of normocapnic hypoxemia, Richards et al. (43) subjected piglets to FiO2 0.10–0.15 for 2 h and randomized them to reoxygenation with 21% oxygen (n = 8), 50% oxygen (n = 8), or 100% oxygen (n = 8) for 1 h, followed by 21% oxygen for 3 h. They found an oxygen dose-dependent increase in global matrix metalloproteinase-2 (MMP-2) activity in the brain. Based on the relationship between FiO2, CA vascular resistance and cerebral MMP-2 activity, the authors speculated that a higher PaO2 may play a role in vasoregulation through an oxidative stress related activation of peroxynitrite and vascular MMP-2.
Solberg et al. (44) conducted a randomized controlled trial in asphyxiated piglets (PaCO2 8.6–8.9 kPa = 64–67 mmHg) to measure the levels of oxidative stress markers (lipid peroxidation-oxidation products of arachidonic acid and docosahexanoic acid) in the cerebral cortex after hypoxia and reoxygenation with 21% (n = 9), 40% (n = 12) or 100% oxygen (n = 8). Solberg et al. (44) did not measure CBF of perfusion, but discussed the fact that isoprostanes have been reported to be potent vasoconstrictors of brain vasculature (46). High values of isoprostanes measured in the 100% group could thereby promote cerebral vasoconstriction.
Lundstrom et al. (45) used Xenon clearance to measure CBF in premature infants <33 completed weeks of gestation. CBF was lower 2 h after randomization to <10 min ventilation with 80% oxygen (n = 35) compared to <10 min ventilation with 21% oxygen (n = 34) at birth. Median PaCO2 was 6 kPa (45 mmHg) (not different between the groups) at the time of measurement. The authors suggested a prolonged effect of hyperoxaemia, possibly mediated by an effect of toxic oxygen metabolites on the cerebral vasculature in premature infants. Cardiac left ventricular output was not significantly lower in the infants treated with 80% oxygen.
Discussion
A fine balance exists between relaxing and contracting factors in vascular endothelial cells during asphyxia and reoxygenation-reperfusion, and oxygen radicals are potent regulators of cerebral arteriole and artery tone (47, 48). The results of this literature review were slightly conflicting regarding how FiO2 influences cerebral perfusion and oxygenation in neonatal animals and premature infants. Epinephrine and anesthetics may influence cerebral perfusion and -autoregulation, which may explain some of the differences in experimental animal studies. Epinephrine increases cerebral perfusion pressure (49), CBF (50, 51), and cerebral oxygen uptake (51). Solberg et al. (44) used isoflurane for induction in piglets. Isoflurane abolishes CBF autoregulation (52), but has a short half-life and was only used in the initial phases of the experiment.
Moderate hypercapnia may protect the brain from hypoxic-ischemic injury (39, 53). The mechanisms include reduced cerebral energy utilization (54) and preserved high-energy phosphate reserves (55). Hypercapnia also shifts the oxygen-hemoglobin dissociation curve to the right, resulting in increased oxygen unloading to the tissues despite tissue hypoperfusion. Solas et al. (42) demonstrated that MAP and microcirculation in the cerebral cortex decreased somewhat less during hypoxia-ischemia, and recovered more rapidly during reoxygenation-reperfusion when CO2 was added to the model. Although a higher MAP and cortical microcirculation was found in the 100% compared with the 21% group, the difference between the groups was less marked than in normocapnia (39). CO2 influences CBF, and both term animals and humans have a strong cerebrovascular sensitivity to changing PaCO2 (56–58), with an increase in CBF of 25%/kPa PaCO2 in healthy term babies. However, this CO2 reactivity may be lost in severe asphyxia (57).
Richards et al. (43) and Solberg et al. (44) speculated that elevated MMP-2 and isoprostanes, respectively, in piglets resuscitated with supplemental oxygen could promote cerebral vasoconstriction and thus a lower CBF. Based on other investigations reported in this paper, it is perhaps more likely that 100% oxygen, when administered after asphyxia, increases CBF. However, the results of Richards et al. (43) and Solberg et al. (44) are in agreement with studies that indicate that 100% oxygen exacerbates reperfusion injury and reduces cerebral perfusion in premature infants (45).
Autoregulation ensures cerebral perfusion and oxygenation by maintaining CBF if cerebral perfusion pressure changes (59). Under normal conditions, hyperoxia induces cerebral vasoconstriction (60), but this oxygen reactivity may be lost during tissue ischemia (61). Hyperoxia may work directly on vascular tone, but also indirectly through the formation of reactive oxygen species (62). The effects of hydrogen peroxide (H2O2) on vascular tone have been the most extensively studied. Exogenous H2O2 produces relaxation of cerebral arteries in vitro (48, 63–65).
Neonatal oxygen requirements and responsiveness of the cerebral vasculature to hyperoxia may differ at different levels of maturity and depend on perinatal factors. Fetal oxygen saturation is about 50%, and a healthy newborn requires at least 5 min to achieve an oxygen saturation >90% (66). The increase in oxygenation is delayed in infants with halted pulmonary vasodilatation, e.g., in chorioamnionitis where inflammation and pulmonary remodeling predispose to impaired gas exchange and persistent pulmonary hypertension. Initiation of breathing, together with the use of oxygen and mechanical ventilation contribute to oxidative stress and inflammation (67, 68), not only in the lungs, but systemically with consequences for other organs including the brain. In addition, altered pulmonary venous return and, subsequently, left ventricular output, result in CBF fluctuations. Supplemental oxygen contributes to decreased pulmonary vascular resistance and increased PBF and may thus be needed in e.g., infants born to mothers with chorioamnionitis. The effect of arterial oxygen tension on pulmonary arterial pressure and ductal shunting is gestational age dependent. Left to right ductal shunting may result in cerebral hypoperfusion secondary to reduced perfusion pressure in preterm infants and might explain why ventilation with 100% oxygen resulted in ~15% reduction in CBF in premature infants (40, 41). Exposure to supplemental oxygen at birth also resulted in prolonged cerebral vasoconstriction in preterm infants (6). Tsuji et al. (69) documented that a high oxygen saturation was associated with impaired cerebrovascular autoregulation and brain injury in premature infants. Niijima et al. (60) observed a fall in CBFV in healthy premature infants with hyperoxemia. Similarly, Leahy et al. (70) observed a significant decrease in CBF in healthy premature neonates after inhalation of 100% oxygen (25). Mechanisms of impaired autoregulation in hyperoxemia include oxidative stress, local production of vasodilators like nitric oxide, and direct vasoparalysis. These responses are gestational age dependent, which may explain that the data by Lundtrom et al. (45) in premature infants contrast to results in term equivalent animals that 100% oxygen increases CBF.
The result by Presti et al. (41) in mice is consistent with the report by Solas et al. (4) who demonstrated that 100% oxygen restored cerebral cortical microcirculation faster than 21% oxygen in piglets following hypoxia-ischemia (20). Even though threshold values for regional CBF after asphyxia have not been established, Solas et al. (39) concluded that a fast restoration of the cerebral microcirculation is beneficial as it was associated with less excitatory amino acids in the striatum. However, Presti et al. (41) demonstrated a trend toward a higher mortality among 100% resuscitated mice vs. mice resuscitated with 21% oxygen and concluded that 100% oxygen may be deleterious at the early stage of recovery due to reactive vasodilatation (71).
Limitations of this review include that we failed in optimizing our search strategy to capture studies that addressed our research questions. Thus, selection of the included studies was more subjective. We did not identify clinical studies that fulfilled our inclusion criteria, and studies in mainly severely asphyxiated post-transitional animals, as well as one study in premature infants were included. During perinatal transition with fluid filled lungs and less surface area for gas exchange, the effects of any given FiO2 is likely to differ from the post-transitional state. During initial stabilization, guidelines recommend that oxygen should be titrated to achieve a preductal SpO2 that is reflective of what healthy term infants experience. We identified no study that investigated weaning/titration of FiO2 after CC with 100% oxygen. None of the included studies reported PaO2 levels during CC. Most studies used SpO2 to measures blood oxygenation. SpO2 does not necessarily represent oxygen uptake and usage by organs, including the brain. Increased blood flow and/or oxygen extraction may serve to maintain oxygen delivery during hypoxemia. Thus, SpO2 alone provides limited information on oxygen consumption by tissues at high or low blood oxygen levels. Near-infrared spectroscopy (NIRS) measures tissue oxygen saturation continuously in a non-invasive manner (72), and was used in some of the studies. Finally, the use of CA flow as a surrogate of CBF could be criticized. However, Gratton et al. (73) demonstrated a direct correlation between CA flow and CBF during hypoxia and reoxygenation in lambs.
In conclusion, CPR with 100% oxygen may more rapidly restore CBF after hypoxia-ischemia, and increases cerebral oxygen delivery. Indeed, the latter may incur oxidative stress-related damage to the ischemic brain while systemic circulatory recovery is the same whether 21 or 100% oxygen is used during neonatal CPR. The advantage of using pure oxygen in neonatal CPR remains to be determined.
Author Contributions
AS, GS, and P-YC: conception and design, collection, assembly, analysis, and interpretation of the data, drafting of the article, critical revision of the article for important intellectual content, and final approval of the article.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank the public for donating money to our funding agencies: GS is a recipient of the Heart and Stroke Foundation/University of Alberta Professorship of Neonatal Resuscitation, a National New Investigator of the Heart and Stroke Foundation Canada and an Alberta New Investigator of the Heart and Stroke Foundation Alberta. The study was supported by a Grant from the SickKids Foundation in partnership with the Canadian Institutes of Health Research [CIHR—Institute of Human Development, Child and Youth Health (IHDCYH)], New Investigator Research Grant Program (Grant No. NI17-033).
References
1. Obladen M. History of neonatal resuscitation. Part 2: oxygen and other drugs. Neonatology. (2009) 95:91–6. doi: 10.1159/000151761
2. Tan A, Schulze A, O'Donnell CP, Davis PG. Air versus oxygen for resuscitation of infants at birth. Cochrane Database Syst Rev. (2005) CD002273. doi: 10.1002/14651858.CD002273.pub3
3. Wyckoff MH, Aziz K, Escobedo MB, Kapadia VS, Kattwinkel J, Perlman JM, et al. Part 13: Neonatal Resuscitation: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. (2015) 132:S543–60. doi: 10.1161/CIR.0000000000000267
4. Solas AB, Munkeby BH, Saugstad OD. Comparison of short- and long-duration oxygen treatment after cerebral asphyxia in newborn piglets. Pediatr Res. (2004) 56:125–31. doi: 10.1203/01.PDR.0000128978.90201.1D
5. Perez-de-Sa V, Cunha-Goncalves D, Nordh A, Hansson S, Larsson A, Ley D, et al. High brain tissue oxygen tension during ventilation with 100% oxygen after fetal asphyxia in newborn sheep. Pediatr Res. (2009) 65:57–61. doi: 10.1203/PDR.0b013e31818a01a4
6. Linner R, Werner O, Perez-de-Sa V, Cunha-Goncalves D. Circulatory recovery is as fast with air ventilation as with 100% oxygen after asphyxia-induced cardiac arrest in piglets. Pediatr Res. (2009) 66:391–4. doi: 10.1203/PDR.0b013e3181b3b110
7. Linner R, Cunha-Goncalves D, Perez-de-Sa V. One oxygen breath shortened the time to return of spontaneous circulation in severely asphyxiated piglets. Acta Paediatr. (2017) 106:1556–63. doi: 10.1111/apa.13920
8. Soraisham AS, Rabi Y, Shah PS, Singhal N, Synnes A, Yang J, et al. Neurodevelopmental outcomes of preterm infants resuscitated with different oxygen concentration at birth. J Perinatol. (2017) 37:1141–7. doi: 10.1038/jp.2017.83
9. Oei JL, Vento M, Rabi Y, Wright I, Finer N, Rich W, et al. Higher or lower oxygen for delivery room resuscitation of preterm infants below 28 completed weeks gestation: a meta-analysis. Arch Dis Child Fetal Neonatal Ed. (2017) 102:F24–F30. doi: 10.1136/archdischild-2016-310435
10. Oei JL, Saugstad OD, Lui K, Wright IM, Smyth JP, Craven P, et al. Targeted oxygen in the resuscitation of preterm infants, a randomized clinical trial. Pediatrics. (2017) 139:e20161452. doi: 10.1542/peds.2016-1452
11. Thamrin V, Saugstad OD, Tarnow-Mordi W, Wang YA, Lui K, Wright IM, et al. Preterm infant outcomes after randomization to initial resuscitation with FiO2 0.21 or 1.0. J Pediatr. (2018) 201:55–61.e1. doi: 10.1016/j.jpeds.2018.05.053
12. Lui K, Jones LJ, Foster JP, Davis PG, Ching SK, Oei JL, et al. Lower versus higher oxygen concentrations titrated to target oxygen saturations during resuscitation of preterm infants at birth. Cochrane Database Syst Rev. (2018) 5:CD010239. doi: 10.1002/14651858.CD010239.pub2
13. Pichler G, Cheung PY, Aziz K, Urlesberger B, Schmolzer GM. How to monitor the brain during immediate neonatal transition and resuscitation? A systematic qualitative review of the literature. Neonatology. (2014) 105:205–10. doi: 10.1159/000357162
14. Pena JP, Tomimatsu T, Hatran DP, McGill LL, Longo LD. Cerebral blood flow and oxygenation in ovine fetus: responses to superimposed hypoxia at both low and high altitude. J Physiol. (2007) 578:359–70. doi: 10.1113/jphysiol.2006.119925
15. Macri MA, D'Alessandro N, Di Giulio C, Di Iorio P, Di Luzio S, Giuliani P, et al. Region-specific effects on brain metabolites of hypoxia and hyperoxia overlaid on cerebral ischemia in young and old rats: a quantitative proton magnetic resonance spectroscopy study. J Biomed Sci. (2010) 17:14. doi: 10.1186/1423-0127-17-14
16. Solevag AL, Cheung PY, Lie H, O'Reilly M, Aziz K, Nakstad B, et al. Chest compressions in newborn animal models: a review. Resuscitation. (2015) 96:151–5. doi: 10.1016/j.resuscitation.2015.08.001
17. Garcia-Hidalgo C, Cheung PY, Solevag AL, Vento M, O'Reilly M, Saugstad O, et al. A review of oxygen use during chest compressions in newborns-a meta-analysis of animal data. Front Pediatr. (2018) 6:400. doi: 10.3389/fped.2018.00400
18. Livera LN, Spencer SA, Thorniley MS, Wickramasinghe YA, Rolfe P. Effects of hypoxaemia and bradycardia on neonatal cerebral haemodynamics. Arch Dis Child. (1991) 66:376–80. doi: 10.1136/adc.66.4_Spec_No.376
19. Tekgunduz KS, Tekgunduz SE. Hypobaric birth room may prevent intraventricular hemorrhage in extremely low birth weights infants. Med Hypotheses. (2018) 119:11–3. doi: 10.1016/j.mehy.2018.07.013
20. Plomgaard AM, Hagmann C, Alderliesten T, Austin T, van Bel F, Claris O, et al. Brain injury in the international multicenter randomized SafeBoosC phase II feasibility trial: cranial ultrasound and magnetic resonance imaging assessments. Pediatr Res. (2016) 79:466–72. doi: 10.1038/pr.2015.239
21. Kenosi M, O'Toole JM, Livingston V, Hawkes GA, Boylan GB, O'Halloran KD, et al. Effects of fractional inspired oxygen on cerebral oxygenation in preterm infants following delivery. J Pediatr. (2015) 167:1007–12.e1. doi: 10.1016/j.jpeds.2015.07.063
22. Basu S, Barman S, Shukla R, Kumar A. Effect of oxygen inhalation on cerebral blood flow velocity in premature neonates. Pediatr Res. (2014) 75:328–35. doi: 10.1038/pr.2013.219
23. Hyttel-Sorensen S, Austin T, van Bel F, Benders M, Claris O, Dempsey E, et al. A phase II randomized clinical trial on cerebral near-infrared spectroscopy plus a treatment guideline versus treatment as usual for extremely preterm infants during the first three days of life (SafeBoosC): study protocol for a randomized controlled trial. Trials. (2013) 14:120. doi: 10.1186/1745-6215-14-120
24. Petrova A, Mehta R. Regional tissue oxygenation in association with duration of hypoxaemia and haemodynamic variability in preterm neonates. Arch Dis Child Fetal Neonatal Ed. (2010) 95:F213–9. doi: 10.1136/adc.2009.161604
25. Takashima S, Houdou S, Hasegawa M, Hashimoto K, Takeuchi Y. Hypoxic-ischemic brain damage: detection of early stage. No To Hattatsu. (1991) 23:147–52.
26. Diemer K. The effect of chronic oxygen deficiency on capillary development in the brain of infants. Monatsschr Kinderheilkd. (1965) 113:281–3.
27. De Vis JB, Alderliesten T, Hendrikse J, Petersen ET, Benders MJ. Magnetic resonance imaging based noninvasive measurements of brain hemodynamics in neonates: a review. Pediatr Res. (2016) 80:641–50. doi: 10.1038/pr.2016.146
28. Koch HW, Hansen TG. Perioperative use of cerebral and renal near-infrared spectroscopy in neonates: a 24-h observational study. Paediatr Anaesth. (2016) 26:190–8. doi: 10.1111/pan.12831
29. Tehrani FT. A computerized decision support system to predict the variations in the cerebral blood flow of mechanically ventilated infants. Comput Biol Med. (2013) 43:1402–6. doi: 10.1016/j.compbiomed.2013.06.015
30. Van Heijst A, Liem D, Hopman J, Van Der Staak F, Sengers R. Oxygenation and hemodynamics in left and right cerebral hemispheres during induction of veno-arterial extracorporeal membrane oxygenation. J Pediatr. (2004) 144:223–8. doi: 10.1016/j.jpeds.2003.11.006
31. Watzman HM, Kurth CD, Montenegro LM, Rome J, Steven JM, Nicolson SC. Arterial and venous contributions to near-infrared cerebral oximetry. Anesthesiology. (2000) 93:947–53. doi: 10.1097/00000542-200010000-00012
33. Lahiri S. Physiological responses and adaptations to high altitude. Int Rev Physiol. (1977) 15:217–51.
34. Rosan RC, Lauweryns JM, Brand MM. Recent advances in pathologic aspects of neonatal respiratory distress. Pathol Annu. (1973) 8:407–52.
35. Rudolph AM. The changes in the circulation after birth. Their importance in congenital heart disease. Circulation. (1970) 41:343–59. doi: 10.1161/01.CIR.41.2.343
36. Longo LD, Pearce WJ. Fetal and newborn cerebral vascular responses and adaptations to hypoxia. Semin Perinatol. (1991) 15:49–57.
37. van Bel F, van de Bor M, Baan J, Ruys JH. The influence of abnormal blood gases on cerebral blood flow velocity in the preterm newborn. Neuropediatrics. (1988) 19:27–32. doi: 10.1055/s-2008-1052397
38. Smith AL, Wollman H. Cerebral blood flow and metabolism: effects of anesthetic drugs and techniques. Anesthesiology. (1972) 36:378–400. doi: 10.1097/00000542-197204000-00015
39. Solas AB, Kutzsche S, Vinje M, Saugstad OD. Cerebral hypoxemia-ischemia and reoxygenation with 21 or 100% oxygen in newborn piglets: effects on extracellular levels of excitatory amino acids and microcirculation. Pediatr Crit Care Med. (2001) 2:340–5. doi: 10.1097/00130478-200110000-00011
40. Rawat M, Chandrasekharan P, Gugino S, Koenigsknecht C, Helman J, Alsaleem M, et al. Oxygenation and hemodynamics during chest compressions in a lamb model of perinatal asphyxia induced cardiac arrest. Children. (2019) 6:E52. doi: 10.3390/children6040052
41. Presti AL, Kishkurno SV, Slinko SK, Randis TM, Ratner VI, Polin RA, et al. Reoxygenation with 100% oxygen versus room air: late neuroanatomical and neurofunctional outcome in neonatal mice with hypoxic-ischemic brain injury. Pediatr Res. (2006) 60:55–9. doi: 10.1203/01.pdr.0000223766.98760.88
42. Solas AB, Kalous P, Saugstad OD. Reoxygenation with 100 or 21% oxygen after cerebral hypoxemia-ischemia-hypercapnia in newborn piglets. Biol Neonate. (2004) 85:105–11. doi: 10.1159/000074966
43. Richards JG, Todd KG, Emara M, Haase E, Cooper SL, Bigam DL, et al. A dose-response study of graded reoxygenation on the carotid haemodynamics, matrix metalloproteinase-2 activities and amino acid concentrations in the brain of asphyxiated newborn piglets. Resuscitation. (2006) 69:319–27. doi: 10.1016/j.resuscitation.2005.08.012
44. Solberg R, Longini M, Proietti F, Vezzosi P, Saugstad OD, Buonocore G. Resuscitation with supplementary oxygen induces oxidative injury in the cerebral cortex. Free Radic Biol Med. (2012) 53:1061–7. doi: 10.1016/j.freeradbiomed.2012.07.022
45. Lundstrom KE, Pryds O, Greisen G. Oxygen at birth and prolonged cerebral vasoconstriction in preterm infants. Arch Dis Child Fetal Neonatal Ed. (1995) 73:F81–6. doi: 10.1136/fn.73.2.F81
46. Hou X, Roberts LJ II, Gobeil F Jr, Taber D, Kanai K, Abran D, et al. Isomer-specific contractile effects of a series of synthetic f2-isoprostanes on retinal and cerebral microvasculature. Free Radic Biol Med. (2004) 36:163–72. doi: 10.1016/j.freeradbiomed.2003.10.024
47. Wei EP, Christman CW, Kontos HA, Povlishock JT. Effects of oxygen radicals on cerebral arterioles. Am J Physiol. (1985) 248:H157–62. doi: 10.1152/ajpheart.1985.248.2.H157
48. Iida Y, Katusic ZS. Mechanisms of cerebral arterial relaxations to hydrogen peroxide. Stroke. (2000) 31:2224–30. doi: 10.1161/01.STR.31.9.2224
49. Burnett AM, Segal N, Salzman JG, McKnite MS, Frascone RJ. Potential negative effects of epinephrine on carotid blood flow and ETCO2 during active compression-decompression CPR utilizing an impedance threshold device. Resuscitation. (2012) 83:1021–4. doi: 10.1016/j.resuscitation.2012.03.018
50. Michael JR, Guerci AD, Koehler RC, Shi AY, Tsitlik J, Chandra N, et al. Mechanisms by which epinephrine augments cerebral and myocardial perfusion during cardiopulmonary resuscitation in dogs. Circulation. (1984) 69:822–35. doi: 10.1161/01.CIR.69.4.822
51. Schleien CL, Dean JM, Koehler RC, Michael JR, Chantarojanasiri T, Traystman R, et al. Effect of epinephrine on cerebral and myocardial perfusion in an infant animal preparation of cardiopulmonary resuscitation. Circulation. (1986) 73:809–17. doi: 10.1161/01.CIR.73.4.809
52. Wang Z, Schuler B, Vogel O, Arras M, Vogel J. What is the optimal anesthetic protocol for measurements of cerebral autoregulation in spontaneously breathing mice? Exp Brain Res. (2010) 207:249–58. doi: 10.1007/s00221-010-2447-4
53. Vannucci RC, Towfighi J, Heitjan DF, Brucklacher RM. Carbon dioxide protects the perinatal brain from hypoxic-ischemic damage: an experimental study in the immature rat. Pediatrics. (1995) 95:868–74.
54. Miller AL, Corddry DH. Brain carbohydrate metabolism in developing rats during hypercapnia. J Neurochem. (1981) 36:1202–10. doi: 10.1111/j.1471-4159.1981.tb01719.x
55. Vannucci RC, Duffy TE. Carbohydrate metabolism in fetal and neonatal rat brain during anoxia and recovery. Am J Physiol. (1976) 230:1269–75. doi: 10.1152/ajplegacy.1976.230.5.1269
56. Ashwal S, Dale PS, Longo LD. Regional cerebral blood flow: studies in the fetal lamb during hypoxia, hypercapnia, acidosis, and hypotension. Pediatr Res. (1984) 18:1309–16. doi: 10.1203/00006450-198412000-00018
57. Pryds O, Greisen G, Lou H, Friis-Hansen B. Vasoparalysis associated with brain damage in asphyxiated term infants. J Pediatr. (1990) 117:119–25. doi: 10.1016/S0022-3476(05)72459-8
58. Wyatt JS, Edwards AD, Cope M, Delpy DT, McCormick DC, Potter A, et al. Response of cerebral blood volume to changes in arterial carbon dioxide tension in preterm and term infants. Pediatr Res. (1991) 29:553–7. doi: 10.1203/00006450-199106010-00007
59. Lassen NA. Cerebral blood flow and oxygen consumption in man. Physiol Rev. (1959) 39:183–238. doi: 10.1152/physrev.1959.39.2.183
60. Niijima S, Shortland DB, Levene MI, Evans DH. Transient hyperoxia and cerebral blood flow velocity in infants born prematurely and at full term. Arch Dis Child. (1988) 63:1126–30. doi: 10.1136/adc.63.10_Spec_No.1126
61. Menzel M, Doppenberg EM, Zauner A, Soukup J, Reinert MM, Clausen T, et al. Cerebral oxygenation in patients after severe head injury: monitoring and effects of arterial hyperoxia on cerebral blood flow, metabolism and intracranial pressure. J Neurosurg Anesthesiol. (1999) 11:240–51. doi: 10.1097/00008506-199910000-00003
62. Faraci FM. Reactive oxygen species: influence on cerebral vascular tone. J Appl Physiol. (2006) 100:739–43. doi: 10.1152/japplphysiol.01044.2005
63. Fraile ML, Conde MV, Sanz L, Moreno MJ, Marco EJ, Lopez de Pablo AL. Different influence of superoxide anions and hydrogen peroxide on endothelial function of isolated cat cerebral and pulmonary arteries. Gen Pharmacol. (1994) 25:1197–205. doi: 10.1016/0306-3623(94)90138-4
64. Yang ZW, Zhang A, Altura BT, Altura BM. Endothelium-dependent relaxation to hydrogen peroxide in canine basilar artery: a potential new cerebral dilator mechanism. Brain Res Bull. (1998) 47:257–63. doi: 10.1016/S0361-9230(98)00120-8
65. You J, Golding EM, Bryan RM Jr. Arachidonic acid metabolites, hydrogen peroxide, and EDHF in cerebral arteries. Am J Physiol Heart Circ Physiol. (2005) 289:H1077–83. doi: 10.1152/ajpheart.01046.2004
66. Kamlin CO, O'Donnell CP, Davis PG, Morley CJ. Oxygen saturation in healthy infants immediately after birth. J Pediatr. (2006) 148:585–9. doi: 10.1016/j.jpeds.2005.12.050
67. Andersson S, Kheiter A, Merritt TA. Oxidative inactivation of surfactants. Lung. (1999) 177:179–89. doi: 10.1007/PL00007639
68. Bunt JE, Carnielli VP, Darcos Wattimena JL, Hop WC, Sauer PJ, Zimmermann LJ. The effect in premature infants of prenatal corticosteroids on endogenous surfactant synthesis as measured with stable isotopes. Am J Respir Crit Care Med. (2000) 162:844–9. doi: 10.1164/ajrccm.162.3.9906139
69. Tsuji M, Saul JP, du Plessis A, Eichenwald E, Sobh J, Crocker R, et al. Cerebral intravascular oxygenation correlates with mean arterial pressure in critically ill premature infants. Pediatrics. (2000) 106:625–32. doi: 10.1542/peds.106.4.625
70. Leahy FA, Cates D, MacCallum M, Rigatto H. Effect of CO2 and 100% O2 on cerebral blood flow in preterm infants. J Appl Physiol Respir Environ Exerc Physiol. (1980) 48:468–72. doi: 10.1152/jappl.1980.48.3.468
71. Lassen NA. The luxury-perfusion syndrome and its possible relation to acute metabolic acidosis localised within the brain. Lancet. (1966) 2:1113–5. doi: 10.1016/S0140-6736(66)92199-4
72. Murkin JM, Arango M. Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br J Anaesth. (2009) 103 (Suppl. 1):i3–13. doi: 10.1093/bja/aep299
Keywords: newborn infant, asphyxia, oxygen, chest compression, cerebral perfusion
Citation: Solevåg AL, Schmölzer GM and Cheung P-Y (2019) Is Supplemental Oxygen Needed in Cardiac Compression?—The Influence of Oxygen on Cerebral Perfusion in Severely Asphyxiated Neonates With Bradycardia or Cardiac Asystole. Front. Pediatr. 7:486. doi: 10.3389/fped.2019.00486
Received: 24 August 2019; Accepted: 06 November 2019;
Published: 20 November 2019.
Edited by:
Anup C. Katheria, Sharp Mary Birch Hospital for Women & Newborns, United StatesReviewed by:
Praveen Chandrasekharan, University at Buffalo, United StatesJayasree Nair, University at Buffalo, United States
Payam Vali, University of California, Davis, United States
Copyright © 2019 Solevåg, Schmölzer and Cheung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne Lee Solevåg, YS5sLnNvbGV2YWdAbWVkaXNpbi51aW8ubm8=