 Francesco Savino1*
Francesco Savino1* Ilaria Galliano2Andrea Savino2Valentina Daprà2Paola Montanari2Cristina Calvi2
Ilaria Galliano2Andrea Savino2Valentina Daprà2Paola Montanari2Cristina Calvi2 Massimiliano Bergallo2
Massimiliano Bergallo2- 1Department of Paediatrics, Azienda Ospedaliera Universitaria Città della Salute e della Scienza di Torino, Turin, Italy
- 2Department of Public Health and Paediatric Sciences, Scuola di Medicina, Università degli Studi di Torino, Turin, Italy
Aim: Studies have shown that Lactobacilli reuteri probiotics can affect cells that play a key role in the immune system. This in vivo Italian study investigated how Lactobacillus reuteri DSM 17938 influenced CC-chemokine receptor 7 (CCR7) and interleukin 10 (IL-10) in breastfed colicky infants.
Methods: Our University hospital in Turin recruited 50 healthy outpatients, at a median age of approximately 1 month, from September 2017 to August 2018. They were randomized to daily Lactobacillus reuteri DSM17938 (1 × 108 cfu) or a placebo for 28 days from recruitment. We collected peripheral blood and evaluated the expression of CCR7 messenger ribonucleic acid using the real-time TaqMan reverse transcription polymerase chain reaction method at baseline and after the study period.
Results: We found increased expression of CC-chemokine receptor 7 in infants treated with the probiotic, but not the controls (p < 0.0026). No differences were observed for interleukin 10 after the study period in either group. At baseline, daily crying time was comparable in the probiotic and control groups: 341 (25) vs. 337 (29) min., respectively (p = 0.450). After 28 days, daily mean crying time decrease statistically in the probiotic group: 78 (23) vs. 232 (31), respectively (p < 0.001).
Conclusion: The increase in CC-chemokine receptor 7 might have been a response to probiotic treatment. As a relatively small sample was used to conduct this study, our research needs to be replicated in different settings, and over time, to produce comparable findings.
Key notes
• Lactobacilli reuteri can affect cells that play a key role in the immune system.
• This in vivo study investigated how Lactobacillus reuteri DSM 17938 influenced CC-chemokine receptor 7 (CCR7) and interleukin 10 (IL-10) in 50 colicky breastfed infants.
• We found increased expression of CC-chemokine receptor 7 in infants randomized to the probiotic, but not placebo, group and no differences in interleukin 10 in either group.
Introduction
Inflammatory mediators, such as cytokines, chemokines and chemokines receptors, have been linked to immune system alterations and they display a considerable amount of similarity of function in infants (1). However, their precise mechanisms in early life are not fully understood.
Historically, neonates were assumed to be deficient in regulatory T cells and other adaptive immune cells, but further research has been carried out in this area in the last decade (2).
Chemokine receptors are involved in organizing thymic architecture and function and lymph-node homing of naive and regulatory T cells. They also influence inflammation, particularly chemokine receptor type 7 (CCR7), which is essential for the directed migration of adaptive immune cells, and regulatory T cell generation (3). The CCR7 signaling system has been implicated in diverse biological processes, such as lymph node homeostasis, T cell activation, immune tolerance and inflammatory responses (3)
CCR7 is a member of the G protein-coupled receptor family (syn CD197). It is activated by two different ligands, chemokine ligand 19 and chemokine ligand 21, and is involved in the migration, activation and survival of multiple cell types, including dendritic cells, T cells, eosinophils, B cells and endothelial cells (4).
Interleukin-10 (IL-10) is arguably the most potent anti-inflammatory cytokine and it is produced by nearly all of the innate and adaptive immune cells. IL-10 plays an important role in the maintenance of gut homeostasis, due to its anti-inflammatory functions. During an infection, IL-10 inhibits the activity of type 1 T helper cells, natural killer cells, and macrophages, which are required for optimal pathogen clearance, and contribute to tissue damage (5).
In infants, the mucosal immune system is constantly exposed to a wide range of commensal and potentially pathogenic microbial species. Intestinal intraepithelial lymphocytes provide a first line of protection and investigating their role in immunity is critical (6).
Emerging evidence supports the concept that infant colic could represent gut inflammation and microbial dysbiosis (7, 8). Lactobacilli are widely used as probiotics and have been shown to have beneficial effects on diarrhea that is associated with infections (9). However, they have also been used in clinical trials that have examined necrotising enterocolitis (10), inflammatory bowel diseases, and infantile colic (11).
Probiotics provide beneficial bacteria and clinicians use them because they can improve modifications in the intestinal microbiota and influence the immunological status of the host (9).
The beneficial effect of probiotics are mediated by several mechanisms, such as immune receptor cascade signaling and cytokines and toll like receptors (10) modulating inflammation and gene networks regulating production of bacterial-derived immunoregulatory molecules (12).
In a study published in 2018 we reported that infants with colic who were treated with Lactobacilli reuteri DSM17938 for 30 days demonstrated a significant decrease in calprotectin values and crying time. The infants also showed increased forkhead box P3 concentrations and these resulted in a decreased retinoic acid-related orphan receptor T and forkhead box P3 ratio (13), while the expression of mRNA expression of Toll like receptor 2 and Toll like receptor 4 seem not influenced (14). An in vitro study Cervantes -Barragan reported that molecular mechanisms responded to the inflammatory status of the gut during treatment with Lactobacillus reuteri (15).
One of these regulatory molecules is the IL-10, which is an anti-inflammatory cytokine and its effects have been demonstrated in studies in both mice and humans (14). Indeed, IL-10 signaling is essential for intestinal homeostasis, particularly in macrophages. IL-10 dampens intestinal inflammation and it would be interesting to know if it can be modulated by probiotic treatment (16, 17).
The aim of the present study was to investigate CCR7 and IL-10 in breastfed colicky infants treated with Lactobacillus reuteri DSM 17938 for 28 days.
Patients and Methods
Subjects and Methods
This study was carried out at the Department of Pediatrics, Regina Margherita Children Hospital, Turin, Italy, between September 2017 and August 2018. We recruited 50 full-term exclusively breastfed infants aged <50 days and randomized equal numbers to receive either Lactobacillus reuteri DSM 17938 of a placebo for 28 days. The median age of the probiotic group at recruitment was 28.5 days and it was 32.5 days for the placebo group. They were included if they were born at a gestational age of between 37 and 40 weeks, with a birth weight of between 2,500 and 4,000 g and a 5-min Apgar score of more than seven. All the infants had colic and underwent blood tests during routine outpatient examinations. We used the modified Wessel's criteria for the diagnosis of infantile colic (13).
The study protocol was approved by the local Ethical Committee at Ospedale Mauriziano—Ospedale Infantile Regina Margherita—S. Anna Torino, and the infants' parents provided written consent to participate in the study.
Sample Collection
Venous blood samples were collected from the infants at 8 a.m., after a 3 h fasting period, which coincided with routine clinical blood sampling to minimize the disturbance to the infants. A tube of haemachrome was collected at recruitment, namely day 1 of the study period, for each infant and at the control visit after 28 days. Each sample was transferred to sterile Eppendorf tubes (Merck KGaA, Darmstadt, Germany) and stored in a freezer at −80°C until they were needed.
Intervention
The infants were randomized to receive the probiotic Lactobacilli reuteri DSM 17938 or placebo daily for 28 days using a computer programme. The active study product consisted of a suspension of freeze-dried Lactobacilli reuteri DSM 17938 in a mixture of sunflower oil and a medium-chain triglyceride oil, which was supplied in a 5 ml dark bottle fitted with a dropper cap. Five drops of the formulation delivered the daily dose of Lactobacilli reuteri 1 × 108 colony forming units and this was given 30 min before feeding. Both the Lactobacilli reuteri and placebo study products were provided by the Italian distributor (Nòos Srl, Roma, Italy). This oil suspension is stable for 21 months at 2°C to 8°C, as documented by the manufacturer (BioGaia AB, Stockholm. Sweden). During the study, parents were instructed to keep the product in the refrigerator when it was not in use.
Subjects received the study product free of charge after enrolment. Each child's pediatrician was informed, in writing, of the child's participation and parents were given a phone number so that they could ask the research team questions and report any perceived problems or concerns during the study.
Follow-Up Phase
Each participant was given a physical examination at enrolment, on day 1 and on day 28.
The parents completed a daily questionnaire for the duration of the study, which included the following data on the general health status of the infant, namely the occurrence of any illness and the use of antibiotics or other medication. It also included gastrointestinal signs and related symptoms, such as crying time, vomiting and regurgitation, and stooling habits.
Participants flow through study are reported in Figure 1.
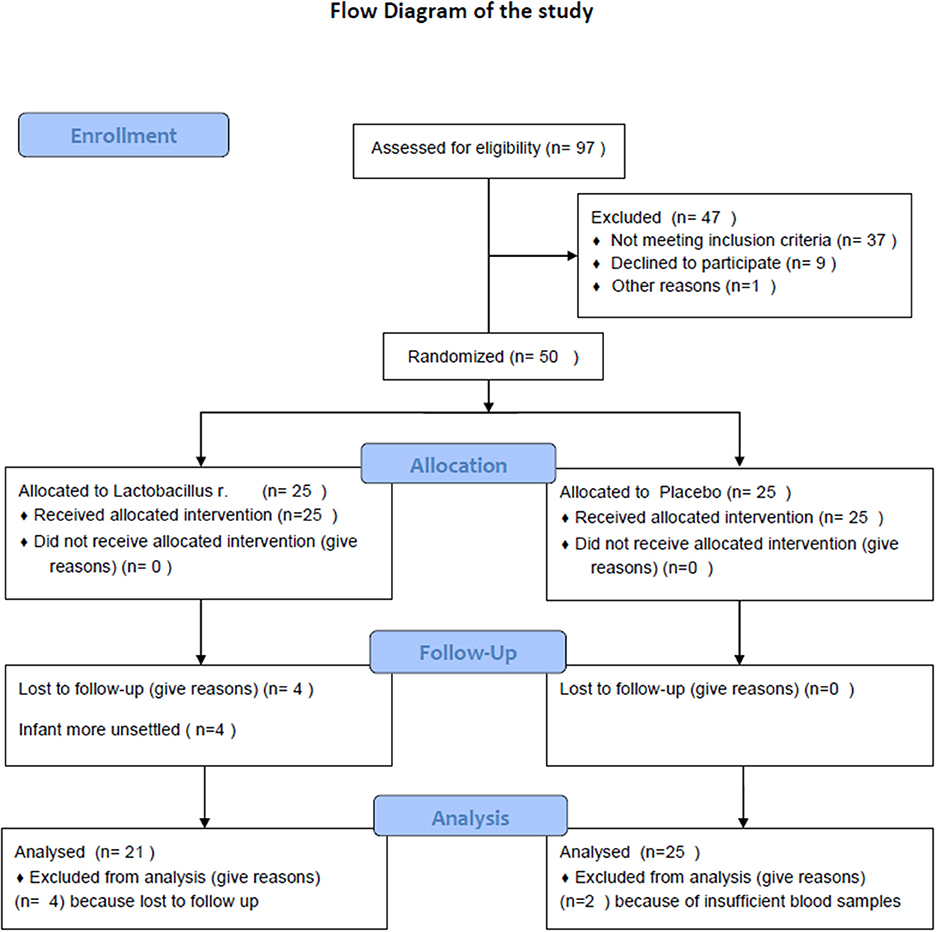
Figure 1. Flow diagram.
Ribonucleic Acid (RNA) Extraction
Total RNA was extracted from 200 μl of blood using a Maxwell automated extractor (Promega, Wisconsin, USA) and the simplyRNA Blood Kit protocol (Promega) without modification. One microgram of total RNA was reverse-transcribed with 8 μl of 10X buffer, 4.8 μl of 25 mM MgCl2, 2 μl of ImpromII (Promega), 1 μl of 40 U/l RNase inhibitor, 0.4 μl of 250 μM random hexamers (Promega), 2 μl of dNTP mix at 100 mM each (Promega) and double distilled water to create a final volume of 20 μl. The reaction was carried out using a GeneAmp PCR system 9700 Thermal Cycler (Applied Biosystems, California, USA) using the following conditions: 5 min at 25°C, 60 min at 42°C and 15 min at 70°C for enzyme inactivation. The complementary deoxyribonucleic acid (DNA) was stored at −80° until use.
Relative Quantification by Real-Time Polymerase Chain Reaction (PCR)
Relative quantification of the messenger RNA expression levels of the selected genes was achieved using TaqMan amplification (Lifetechnologies, Texas, USA) and normalization to glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as the reference gene. This was achieved using an ABI PRISM 7500 real-time system (Life Technologies, Texas, USA). The mRNA messenger RNA expression levels of CC R7 and IL10 were quantified using real-time PCR. Approximately 100 ng of cDNAcomplementary DNA was amplified in a total volume of 20 μl containing 2 × GoTaq® qPCR Master Mix (Promega, Madison, WI), 500 nmol of specific primers and 200 nmol of probe. Were used: CCR7 primers (CCR7F-5′- GCAACTCAACATCGCCTACG−3′)(CCR7R-5′- GAAGAGATCGTTGCGGAACTT−3′) and probe (CCR7P-6FAM- accctttcttgtacgccttcatcgg -TAMRA); IL10 primers (IL10F-5′- ATGAAGGATCAGCTGGACAACTT−3′) (IL10R-5′- CCTTGATGTCTGGGTCTTGGT-3′) and probe (IL10P-6FAM- ACCTGGGTTGCCAAGCCTTGTCTG -TAMRA); GAPDH primers (GAPDHF-5′-CCAAGGTCATCCATGACAAC-3′) (GAPDHR-5′- GTGGCAGTGATGGCATGGAC-3′) and probe (GAPDH-6FAM- TGGTATCGTGGAAGGA-3′ MGB). The amplifications were performed in a 96-well plate at 95°C for 2 min, followed by 40 cycles of 95°C for 15 s and 60°C for 1 min. Each sample was run in triplicate. The target gene relative expression in patients was compared with normal samples using the 2-ΔΔCt method, and the relative expression is expressed in arbitrary units (AU).
The messenger RNA expression levels of CCR7 and IL10 and GAPDH were quantified by real-time PCR, as previously described by Mareschi et al. (18).
Statistical Analysis
The sample size was calculated on the basis that we wanted to find a 50 min reduction in daily average crying time in the probiotic group, when it was compared to the placebo group. This was considered a clinically relevant difference and was based on previous studies. We calculated that 20 patients were needed in each group, based on an alpha value of 0.05, beta value of 0.20 and an estimated standard deviation (SD) within the groups of 50 min crying time. We decided to enroll 25 subjects per group to allow for a 20% drop-out rate.
Randomization was performed by the random-digit method, using computer-generated numbers. We used a two-treatment randomization scheme with random blocks of varying size, employing Stata Statistical Software, Release 9 (StataCorp LP, College Station, Texas, USA) and the ralloc procedure. Data were analyzed by SPSS, version 16 (SPSS Inc, Illinois, USA), while the sample size calculation was performed by NCSS-PASS 2000 (Number Cruncher Statistical Systems, Utah, USA).
Data are shown as means and standard deviations (SD) or medians and interquartile ranges (IQR) for continuous variables, as appropriate, and numbers and percentages for categorical variables. Differences between the groups were evaluated using the Student's t-test for paired samples, while associations between the categorical variables were evaluated by Fisher's exact test. The Wilcoxon signed-rank test and Friedman test were used to evaluate differences between paired samples for continuous variables, when appropriate.
All reported p-values were two-sided and differences were considered to be significant when p < 0.05.
Results
A total of 50 infants were enrolled to the study and allocated, according to the protocol, to receive the Lactobacilli reuteri DSM17938 probiotic or placebo. The characteristics of the subjects enrolled and treated with the probiotic and the placebo are reported in Table 1. There were no significant differences between groups at baseline (Table 1). We excluded six infants from the analysis because of sufficient blood samples: four in the probiotic group and two in the placebo group.
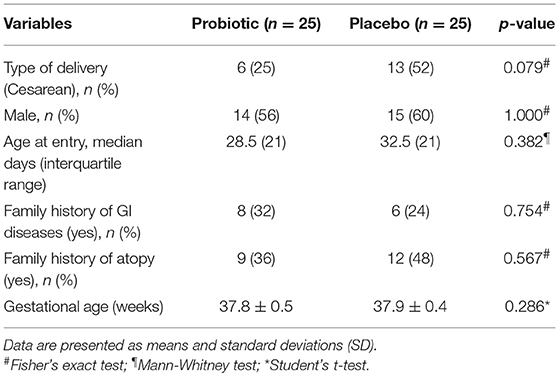
Table 1. Baseline characteristics of the participants in the two study groups.
The primary outcome was the measurement of the expression level of CC-chemokine receptor 7 messenger RNA in the study group at day 1 and at day 28.
The CC-chemokine receptor 7 values in the probiotic group on day 1 was 2.73 ± 1.1 ΔCt and on day 28 it was 1.82±1.45 ΔCt. In comparison, the CC-chemokine receptor 7 values in the placebo group was 1.86±1.1 ΔCt on day 1 and 1.21±0.6 ΔCt on day 28 (Table 2).
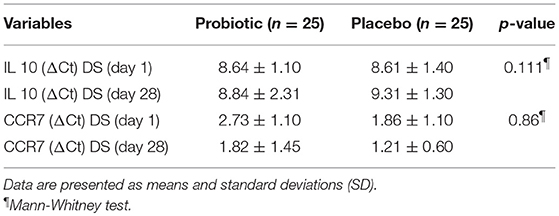
Table 2. Blood inflammatory markers (ΔCt), in infant with colic at enrolment and after 28 days of supplementation with L. reuteri or Placebo.
After the study period CC-chemokine receptor 7 were expressed at higher levels in the probiotic group than in the placebo group (p = 0.0020) (Figure 2).
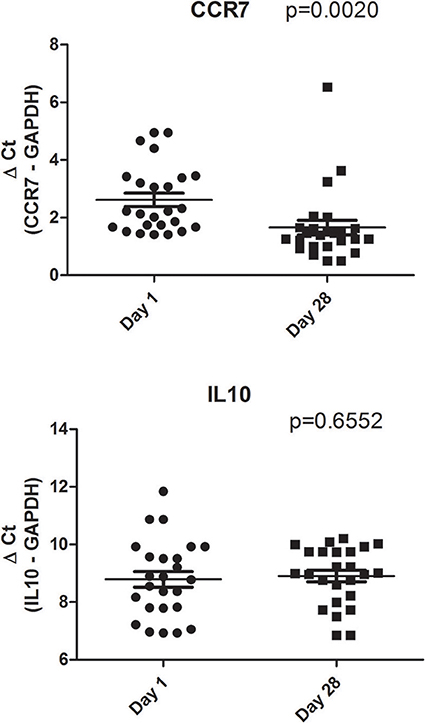
Figure 2. CCR7 and IL10 transcriptional levels in the venous blood of group treated with L Reuteri DSM 17938. Data are represented as circle plots (day 1) and box plots (day 28), with horizontal lines depicting the averages. Relative messenger RNA levels were analyzed by real-time PCR and represented by ΔCt. The Paired t-test was performed.
When we analyzed the placebo group we did not observe different CCR7 expression on day 1 and on day 28 (p = 0.26) (data not shown).
Secondary Outcome
The values of IL-10 in the probiotic group were 8.64 ± 1.32 ΔCt on day 1, and 8.84 ± 2.31 ΔCt on day 28 (p = 0.6552)(Figure 2). The values in the placebo group were 8.61 ± 1.40 ΔCt on day 1 and 9.31 ± 1.30 ΔCt on day 28 (p = 0.62) (data not shown). At day 28, IL10 was equally expressed in the probiotic (Figure 2) and control groups (p = 0.4375) (data not shown).
Crying time of infants treated with L. reuteri or Placebo are reported in Table 3.
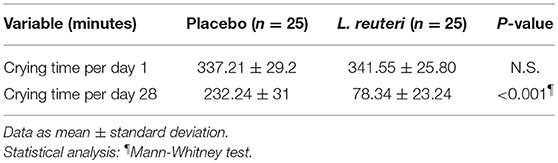
Table 3. Crying and fussing time (mean minutes per days) at day 1 and at day 28 in placebo and L. reuteri group.
After L. reuteri administration for 28 days in infants with colic, we observed a significant decrease of daily crying time (341.55 ± 25.80 min/day at day 0 vs. 78.34 ± 23.24 min/day at day 28, p = 0.001) (Table 3).
We conducted on response variable (crying time) an ITT (Intention to Treat) analysis too, including 4 infants dropped out. As they were all from the Placebo group we classified them as responders.
Infants Responders (with a reduction of 50% in crying time from baseline) were significantly higher in the L. reuteri group vs. placebo group on days 28 (21 vs. 11, p = 0.007).
Discussion
The role of the main cytokines, chemokines and their receptors in the pathophysiology of disorders that involve inflammation in an emerging issue of active research (15, 16, 19–22).
Gut microbiota and its metabolites have been shown to influence immune functions and immune homeostasis within the gut, particularly during the first few months of life. In addition, probiotics have been shown to have an effect on immunity throughout cytokines and the production of metabolites such as tryptophan (15). Haileselassie et al. reported that Lactobacillus reuteri was able to influence the generation of monocyte-derived dendritic cells and subsequent autologous T cell responses (23).
On the other hand an in vitro study by Cervantes et al. demonstrated that Lactobacillus reuteri induced gut intraepithelial CD4(+)CD8αα(+) T cells (15).
The immunological mechanism behind the effects of probiotic such as Lactobacillus reuteri are probably regulatory T cells cell, as previous studies have reported (13, 14, 22, 23).
In fact Yuying et al. showed that Lactobacillus reuteri DSM 17938 changed the frequency of forkhead box P3 ratio regulatory T cells in the intestine and mesenteric lymph node in experimental necrotising enterocolitis (24).
While the precise mechanism is unclear, we can argue that the reaction between Lactobacillus reuteri and both epithelial and non-epithelial enteric cells must be active in modulating intrinsic anti-inflammatory effects in the intestine, as shown in animal models in vivo (23–27).
In this study we showed that Lactobacillus. reuteri 17938 was effective in alleviation of crying time due to colic in breast fed infants. Our results are consistent with the recent meta-analysis of previous four randomized trials (11).
Our findings showed also an increased expression of CC-chemokine receptor 7 in infants treated with Lactobacilli reuteri DSM 17938 after 28 days (p = < 0.0020), compared to day 1, while no differences where observed for IL-10 values.
CCR7 is involved in efficient induction of immune reactions as well as their silencing and regulation. Most of the knowledge on the involvement of CCR7 in the development of immunity and tolerance has been derived from mouse models and data on CCR7 function in humans is rather sparse (3, 4). However, it has been discovered that CCR7 contributes to the induction and maintenance of tolerance and this suggests a possible new strategy for treatment using probiotics.
CCR7 has recently been shown to be up-regulated in peripheral blood DCs and in DCs derived from monocytes and CD34 progenitor cells after activation with a variety of agents (28).
Our in vivo results using peripheral blood mononuclear cells from treated infants with L reuteri showed up-regulation of CCR7 expression levels. that the baseline levels of CCR7 were low.
These results, preliminary in nature, are consistent with the hypothesis that level of expression of CCR7 maybe the response to recruitment to gut lymphatics systems.
While our data suggest that IL-10 cytokines seem not be involved by probiotic supplementation, but a larger sample is necessary to confirm our observations, which were echoed by an animal study carried out by Yan et al. (29).
Strength and Limitations
There were some limitations to our study. First, since this was an experimental study, it only provides preliminary data. It is difficult to obtain detailed information on many factors when carrying out a pilot study with a small number of subjects. That is why it is necessary to control for the effects of extraneous variables that might result in misleading interpretations of causality. As a result, the findings of this study cannot be generalized.
However, to the best of our knowledge this is the first research study that investigated CCR7 in healthy breastfed infants treated with Lactobacillus reuteri DSM 17938 compared to a placebo using real time PCR. Tompa et al. reported that cryopreservation of peripheral blood mononuclear cells could have an impact on the expression of CCR7 on regulatory T cells, but we did not use cytofluorimetry and our data were not influenced by storage (30).
The standardized approach that we used permits the study to be replicated in different settings, or over time, to produce comparable findings.
Conclusion
Our randomized study of breastfed infants with colic found a decreased crying time and an increased expression of CC-chemokine receptor 7 in infants treated with the probiotic Lactobacillus reuteri DSM 17938 for 28 days, but not the placebo group. No differences were observed for interleukin 10 after the study period in either group. The increase in CC-chemokine receptor 7 might have been a response to probiotic treatment.
Understanding the possible effect of probiotic supplements, particularly during the first few weeks of life, is interesting and could also help to induce oral tolerance. Future studies on CCR7 in human molecular medicine, as well as more refined microbiota models of site-specific and inducible CCR7 and the CCR7-ligand, will help our understanding of this important molecular pathway. It will also aid our understanding of the cellular responses driven by it during probiotic treatment. Taking advantage of these new features may lead to a tailored approach for regulatory T cells using probiotic treatment.
Data Availability
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The study protocol was approved by the local Ethical Committee at Ospedale Mauriziano—Ospedale Infantile Regina Margherita–S. Anna Torino, and the infants' parents provided written consent to participate in the study.
Author Contributions
FS had primary responsibility for protocol development as principal investigator and wrote the manuscript. IG performed PCR analysis and helped to write the manuscript. AS analyzed data and wrote the manuscript, edited references. VD performed PCR analysis and helped to write the manuscript. PM performed PCR analysis and helped to write the manuscript. CC performed analysis and wrote the manuscript. MB performed the final data analysis, supervised analysis and helped to write the manuscript.
Funding
This study was supported by Noos S.r.L. 00181 Roma, Italy. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer
The content is solely the responsibility of the authors.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors are grateful to Annette Whibley of Wizard Communications for editing the manuscript.
Abbreviations
CCR7, chemokine receptor type 7; IL10, interleukin 10; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; DNA, deoxyribonucleic acid; RNA, ribonucleic acid; PCR, polymerase chain reaction.
References
1. Basha S, Surendran N, Pichichero M. Immune responses in neonates. Expert Rev Clin Immunol. (2014) 10:1171–84. doi: 10.1586/1744666X.2014.942288
2. Adkins B, Leclerc C, Marshall-clarke S. neonatal adaptive immunity comes of age. Nat Rev Immunol. (2004) 4:553–64. doi: 10.1038/nri1394
3. Förster R, Davalos-Misslitz AC, Rot A. CCR7 and its ligands: balancing immunity and tolerance. Nat Rev Immunol. (2008) 8:362–71. doi: 10.1038/nri2297
4. Raju R, Gadakh S, Gopal P, George B, Advani J, Soman S, et al. Differential ligand-signaling network of CCL19/CCL21-CCR7 system. Database. (2015) 2015:bav106. doi: 10.1093/database/bav106
5. Couper KN, Blount DG, Riley EM. IL-10: the master regulator of immunity to infection. J Immunol. (2008) 180:5771–7. doi: 10.4049/jimmunol.180.9.5771
6. Sheridan BS, Lefrançois L. Intraepithelial lymphocytes: to serve and protect. Curr Gastroenterol Rep. (2010) 12:513–21. doi: 10.1007/s11894-010-0148-6
7. Mai T, Fatheree NY, Gleason W, Liu Y, Rhoads JM. Infantile colic: new insights into an old problem. Gastroenterol Clin North Am. (2018) 47:829–44. doi: 10.1016/j.gtc.2018.07.008
8. Rhoads JM, Collins J, Fatheree NY, Hashmi SS, Taylor CM, Luo M, et al. Infant colic represents gut inflammation and dysbiosis. J Pediatr. (2018) 203:55–61. doi: 10.1016/j.jpeds.2018.07.042
9. Plaza-Díaz J, Ruiz-Ojeda FJ, Gil-Campos M, Gil A. Immune-mediated mechanisms of action of probiotics and synbiotics in treating pediatric intestinal diseases. Nutrients. (2018) 10:E42. doi: 10.3390/nu10010042
10. Hoang TK, He B, Wang T, Tran DQ, Rhoads JM, Liu Y. Protective effect of Lactobacillus reuteri DSM 17938 against experimental necrotizing enterocolitis is mediated by Toll-like receptor 2. Am J Physiol Gastrointest Liver Physiol. (2018) 315:G231–40. doi: 10.1152/ajpgi.00084.2017
11. Sung V, D'Amico F, Cabana MD, Chau K, Koren G, Savino F, et al. Lactobacillus reuteri to treat infant colic: a meta-analysis. Pediatrics. (2018) 141:e20171811. doi: 10.1542/peds.2017-1811
12. Thomas CM, Saulnier DM, Spinler JK, Hemarajata P, Gao C, Jones SE, et al. Fol C2-mediated folate metabolism contributes to suppression of inflammation by probiotic Lactobacillus reuteri. Microbiol Open. (2016) 5:802–18. doi: 10.1002/mbo3.371
13. Savino F, Garro M, Montanari P, Galliano I, Bergallo M. Crying time and RORγ/FOXP3 expression in Lactobacillus reuteri DSM17938-treated infants with colic: a randomized trial. J Pediatr. (2018) 192:171–7.e1. doi: 10.1016/j.jpeds.2017.08.062
14. Savino F, Galliano I, Garro M, Savino A, Daprà V, Montanari P, et al. Regulatory T cells and Toll-like receptor 2 and 4 mRNA expression in infants with colic treated with Lactobacillus reuteri DSM17938. Benef Microbes. (2018) 8:1–10. doi: 10.3920/BM2017.0194
15. Cervantes-Barragan L, Chai JN, Tianero MD, Di Luccia B, Ahern PP, Merriman J, et al. Lactobacillus reuteri induces gut intraepithelial CD4(+)CD8αα(+) T cells. Science. (2017) 357:806–10. doi: 10.1126/science.aah5825
16. Cervantes-Barragan L, Colonna M. Chemical sensing in development and function of intestinal lymphocytes. Curr Opin Immunol. (2018) 50:112–6. doi: 10.1016/j.coi.2018.01.004
17. Engelhardt KR, Grimbacher B. IL-10 in humans: lessons from the gut, IL-10/IL-10 receptor deficiencies, and IL-10 polymorphisms. Curr Top Microbiol Immunol. (2014) 380:1–18. doi: 10.1007/978-3-662-43492-5_1
18. Mareschi K, Castiglia S, Sanavio F, Rustichelli D, Muraro M, Defedele D, et al. Immunoregulatory effects on T lymphocytes by human mesenchymal stromal cells isolated from bone marrow, amniotic fluid, and placenta. Exp Hematol. (2016) 44:138–50.e1. doi: 10.1016/j.exphem.2015.10.009
19. Turner MD, Nedjai B, Hurst T, Pennington DJ. Cytokines and chemokines: at the crossroads of cell signalling and inflammatory disease. Biochim Biophys Acta. (2014) 1843:2563–82. doi: 10.1016/j.bbamcr.2014.05.014
20. Dinan TG, Cryan JF. Regulation of the stress response by the gut microbiota: implications for psychoneuroendocrinology. Psychoneuroendocrinology. (2012) 37:1369–78. doi: 10.1016/j.psyneuen.2012.03.007
21. Gensollen T, Iyer SS, Kasper DL, Blumberg RS. How colonization by microbiota in early life shapes the immune system. Science. (2016) 352:539–44. doi: 10.1126/science.aad9378
22. Liu Y, Fatheree NY, Mangalat N, Rhoads JM. Human-derived probiotic Lactobacillus reuteri strains differentially reduce intestinal inflammation. Am J Physiol Gastrointest Liver Physiol. (2010) 299:1087–96. doi: 10.1152/ajpgi.00124.2010
23. Haileselassie Y, Navis M, Vu N, Qazi KR, Rethi B, Sverremark-Ekström E. Lactobacillus reuteri and Staphylococcus aureus differentially influence the generation of monocyte-derived dendritic cells and subsequent autologous T cell responses. Immun Inflamm Dis. (2016) 4:315–26. doi: 10.1002/iid3.115
24. Liu Y, Fatheree NY, Dingle BM, Tran DQ, Rhoads JM. Lactobacillus reuteri DSM 17938 changes the frequency of Foxp3+ regulatory T cells in the intestine and mesenteric lymph node in experimental necrotizing enterocolitis. PLoS ONE. (2013) 8:e56547. doi: 10.1371/journal.pone.0056547
25. Round JL, Mazmanian SK. Inducible Foxp3+ regulatory T-cell development by a commensal bacterium of the intestinal microbiota. Proc Natl Acad Sci USA. (2010) 107:12204–9. doi: 10.1073/pnas.0909122107
26. Taylor A, Hale J, Wiltschut J, Lehmann H, Dunstan JA, Prescott SL. Evaluation of the effects of probiotic supplementation from the neonatal period on innate immune development in infancy. Clin Exp Allergy. (2006) 36:1218–26. doi: 10.1111/j.1365-2222.2006.02552.x
27. He B, Hoang TK, Wang T, Ferris M, Taylor CM, Tian X, et al. Resetting microbiota by Lactobacillus reuteri inhibits T reg deficiency–induced autoimmunity via adenosine A2A receptors. J Exp Med. (2017) 214:107–23. doi: 10.1084/jem.20160961
28. Saeki H, Moore AM, Brown MJ, Hwang ST. Cutting edge: secondary lymphoid-tissue chemokine (SLC) and CC chemokine receptor 7 (CCR7) participate in the emigration pathway of mature dendritic cells from theskin to regional lymph nodes. J Immunol. (1999) 162:2472–5.
29. Yan FF, Murugesan GR, Cheng HW. Effects of probiotic supplementation on performance traits, bone mineralization, cecal microbial composition, cytokines and corticosterone in laying hens. Animal. (2019) 13:33–41. doi: 10.1017/S175173111800109X
Keywords: breastfeeding, CC-chemokine receptor 7, colicky infants, Lactobacillus reuteri, Interleukin 10
Citation: Savino F, Galliano I, Savino A, Daprà V, Montanari P, Calvi C and Bergallo M (2019) Lactobacillus reuteri DSM 17938 Probiotics May Increase CC-Chemokine Receptor 7 Expression in Infants Treated With for Colic. Front. Pediatr. 7:292. doi: 10.3389/fped.2019.00292
Received: 01 March 2019; Accepted: 28 June 2019;
Published: 16 July 2019.
Edited by:
Jorge Amil Dias, Centro Hospitalar de São João, PortugalReviewed by:
Duška Tješić-Drinković, University of Zagreb, CroatiaRajni Ahlawat, Marshfield Clinic, United States
Copyright © 2019 Savino, Galliano, Savino, Daprà, Montanari, Calvi and Bergallo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Savino, ZnJhbmNlc2NvLnNhdmlub0B1bml0by5pdA==