 Li Ye
Li Ye Zheng Wang
Zheng Wang Hui Zhang1
Hui Zhang1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 15 May 2018
Sec. Pediatric Hematology and Hematological Malignancies
Volume 6 - 2018 | https://doi.org/10.3389/fped.2018.00141
The toxic dose of rodenticides in children is extremely difficult to be determined because of the uncertain exposure history. We established and validated a method to identify the toxic dose in children of 4-hydroxycoumarin (TDCH). Items were selected by Delphi method and weighted by analytic hierarchy process. Toxic doses were classified into three categories: high dose (>24 points), medium (15-24) and low (<15). Sixty-five children with 4-hydroxycoumarin rodenticide intoxication were included in the study. There were 29(44.6%), 8(12.3%), 28(43.1%) cases in high, medium, and low dose respectively. Patients in high-dose were more likely to have intentionally attempted suicide (5/29, 17.2%) or had no definite history of ingestion (17/29, 58.6%), arrived at the hospital later than 24 h (26/29, 90%), been misdiagnosed initially (25/29, 86.2%), not treated by gastric lavage (27/29, 93.1%), and developed severe hemorrhage. While most patients in low-dose were younger than 6 years (26/28, 92.9%), all have experienced accidental exposure, arrived at the hospital, and received gastric lavage within 24 h, obtained a definite diagnosis, and be asymptomatic. Of 38 patients arrived at hospital within 48 h, patients a score48h ≥ 15 had higher incidence of coagulopathy (6/8, 75.0%) than patients with a score48h < 15 (3/30, 10.0%). Of all patients, 37 in the high and medium dose with a score ≥ 15 has higher incidence (35/37, 94.6%) of prolonged administration with vitamin K1 (≥1 month) than other 28 patients with a score < 15 (0/28, 0%). The TDCH system could not only be used in evaluating toxic doses and predicting coagulopathy in the early stage, but also helps to guide appropriate treatment. Patients with a score48h ≥ 15 were in the high bleeding risk category. And patients with a scores ≥ 15 required treatment with vitamin K1 for more than a month.
Since the mid-1970s, the widespread use of 4-hydroxycoumarin instead of short-acting rodenticides (e.g., arsenic and strychnine) has increased the incidence of long-acting anticoagulant rodenticides (LAARs) poisoning (1). Currently, the majority of commercially available LAARs are second-generation 4-hydroxycoumarin such as brodifacoum and bromadiolone that have increased activity and a longer duration of action than those of the parent compound (2, 3). Thus, they are also referred to as “superwarfarins.” 4-Hydroxycoumarin inhibits the activity of hepatic vitamin K1 epoxide reductase, which is involved in the synthesis of the active form of vitamin K, and subsequently vitamin K-dependent blood clotting factors II, VII, IX, and X (4). The mean half-life of factors II, VII, IX, and X is 41.0, 6.2, 13.9, and 16.5 h, respectively (5). Therefore, after ingestion of 4-hydroxycoumarin, coagulopathy may be delayed by several hours to days until the preformed vitamin K and active clotting factors are exhausted.
Clinical manifestations of 4-hydroxycoumarin poisoning are characterized by prolonged multiple-site hemorrhage, and may range from no symptom to life-threatening bleeding, which is mainly determined by the ingested dose of the active ingredient. Significant coagulopathy usually results from the ingestion of large amounts of this active ingredient without timely diagnosis and treatment. And clinically important manifestation would not be observed in children who ingested less than 1 box of superwarfarin (6). However, in contrast to that in adults, the ingested dose of rodenticides in children is very difficult to be determined because of the uncertainties in the exposure history (7). Preschool children who comprise the largest at-risk population of rodenticide poisoning are usually unable to accurately describe the poisoning details including ingested doses. Suicidal adolescents, for various reasons, may intentionally conceal the facts. Meanwhile, some guardians do not witness the process of rodenticide ingestion. Furthermore, 4-hydroxycoumarin is usually unnoticed because it is flavorless (8). Some consumers use the concentrates to prepare bait in a manner not strictly in accordance with the instructions and, therefore, the amount of the active substance ingested is unknown.
These domestic and household challenges make it extremely difficult to estimate the ingested dose accurately. When the ingested dose is known, decontamination and treatment can increase the elimination of toxins resulting in the decrease of toxic in vivo dose, and vitamin K administration will decrease the toxic effects. As a result, toxic dose is not always consistent with ingested dose. To date, there are very little data available on the toxic dose estimation of 4-hydroxycoumarin in humans. Therefore, the following study was conducted to establish an evaluation system for toxic doses in pediatric patients with 4-hydroxycoumarin rodenticide intoxication. Using this evaluation system, we aimed to guide the accurate administration of poisoned patients.
A Delphi group consisted of 12 pediatric experts and 8 toxicologists were established to aid with item selection and gradation. A systematic review of the literature was performed using the following search items: “4-hydroxycoumarin,” “coumarins,” “anticoagulant,” “long-acting anticoagulant,” “anticoagulant rodenticide,” “superwarfarin,” “brodifacoum,” and “bromadiolone.” Databases queried included PubMed, Science Citation Index, and OVID. 10 items (age, amount ingested, reason, LAARs type, coagulation function, severity of bleeding, time from ingestion to first-time gastric lavage, time from ingestion to first-time plasmapheresis, time from ingestion to hospitalization, and frequency of plasmapheresis) which closely related to toxic dose and severity of disease were initially drafted through review of the literature. The Delphi group members ranked each item from 0(not important) to 4(extremely important) separately. The responses of all Delphi members were summarized, processed, and sent back to the experts. Consensus was reached after two rounds and 7 items (amount ingested, reason, coagulation function, severity of bleeding, time from ingestion to first-time gastric lavage, time from ingestion to first-time plasmapheresis and frequency of plasmapheresis) were selected finally. Then gradations were weighted by analytic hierarchy process. Finally, the scoring system for TDCH was established according to item weighting.
Trained physicians recorded the information, and prothrombin time (PT), activated partial prothrombin time (APTT), and international normalized ratio (INR) were measured for all patients on admission, and toxic dose grades of all patients were made by the TDCH scores. All patients were routinely followed up, and PT, APTT, and INR repeated at a month. For patients who needed vitamin K1 treatment more than a month, they were further followed until recovery. The ability of TDCH score48h predicting coagulopathy and TDCH score predicting prolonged administered with vitamin K1 was assessed with the area under the receiver operating characteristic (AUROC) analysis. In 38 patients who arrived at the hospital within 48 h, TDCH score48h were obtained according to manifestations and lab findings. And prolonged administration with vitamin K1 was defined as longer than a month.
Sixty-five children at the West China Second University Hospital of Sichuan University, who were diagnosed with 4-hydroxycoumarin rodenticide intoxication between May 2008 and September 2016, were included in the study. The diagnosis of 4-hydroxycoumarin rodenticide intoxication was based on exposure history, clinical effects, physical examination, and laboratory results. Main hemorrhagic symptoms of the enrolled patients included epistaxis, petechiae, gastro- intestinal bleeding, hematuria, ecchymoma, and gingival bleeding. In 17 cases who lacked a definitive history of ingestion, the diagnoses were confirmed using high-performance liquid chromatography with tandem mass spectrometry (LC-MS/MS) detection of blood samples (9). The following were the study exclusion criteria: (1) combined ingestion of other pesticides or anticoagulants such as warfarin; (2) hereditary coagulation deficiency; and (3) history of serious underlying disease such as heart, lung, renal, or liver disease.
The statistical package for the social sciences (SPSS) version 19.0 software was used for the statistical analyses. The measured data were expressed as the mean ± standard deviation (SD) and counted data were expressed as numbers and percentages in parentheses. The differences between groups were compared using the Student's t-test for continuous variables and the chi-square test for categorical variables. The Delphi method was used to select items. Analytic hierarchy process was used to determine the weight of each item. AUROC analysis was used to calculate cutoff values, sensitivity, and specificity. Differences with p-values < 0.05 were considered statistically significant.
This study was performed according to the Declaration of Helsinki and was approved by the Medical Ethics Review Committee of West China Second University Hospital of Sichuan University (reference number 2017032). All parents of participants signed an informed consent form prior to enrolment.
The specific calculation of the evaluation system is shown in Table 1.
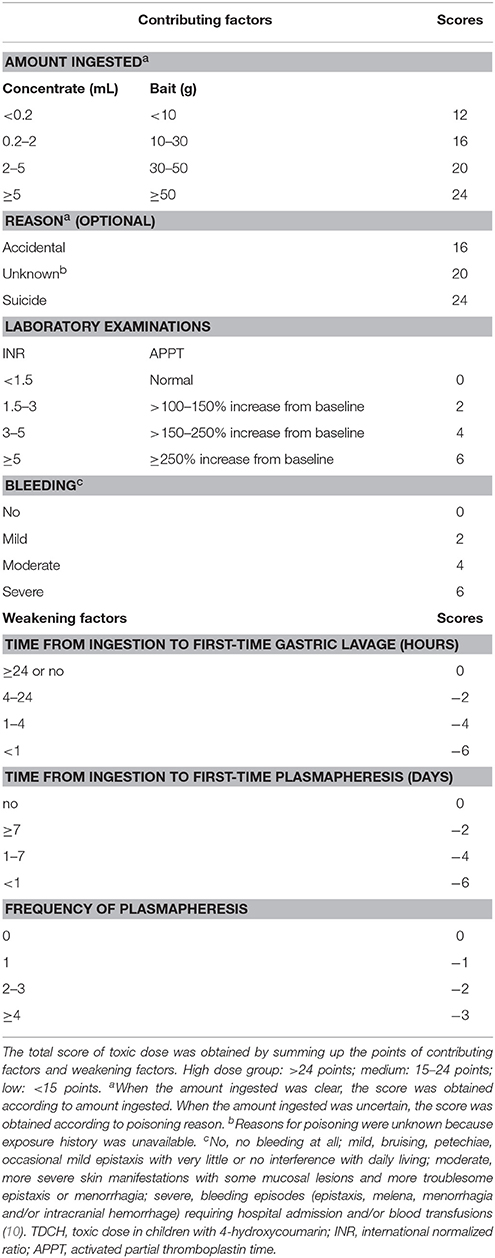
Table 1. Scoring system for toxic dose in children with 4-hydroxycoumarin (TDCH).
As shown in Table 2, 65 children with 4-hydroxycoumarin intoxication aged between 9 months and 15 years were included in the study. The pediatric 4-hydroxycoumarin poisoning cases exhibited a bimodal age distribution. Poisoning Reasons of 17 patients were unknown because their exposure history was unavailable, of whom, 9 repeatedly denied any exposure to rodenticides, and other 8 denied the ingestion despite evidence of the use of rodenticides in their household. The diagnosis of them was confirmed by LC-MS/MS method. Epistaxis (23/65) and petechiae (21/65) were main hemorrhagic symptoms, followed by gastro- intestinal bleeding (16/65), hematuria (7/65), ecchymoma (7/65) and gingival bleeding (6/65). Mortality rate was zero.
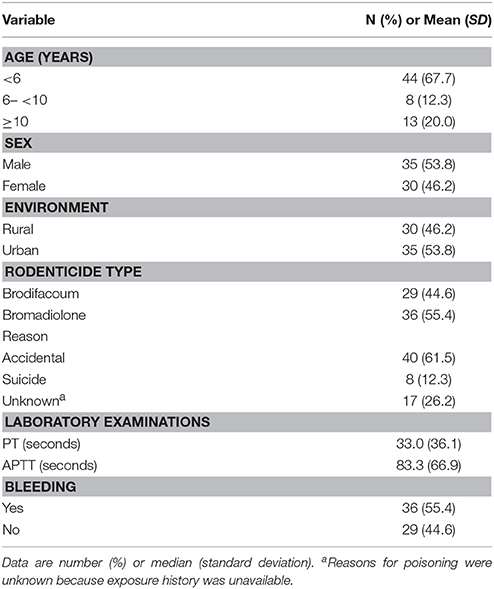
Table 2. Baseline characteristics of 65 children with 4-hydroxycoumarin intoxication.
Selected demographics and clinical characteristics of the high, medium, and low dose groups are shown in Table 3. There was no statistically significant difference in sex and environment (not shown in the table) among the three groups. Overall, patients in the high-dose had a wide age distribution, poisoned for various reasons, and arrived at the hospital later than 24 h (26/29, 89.7%), been misdiagnosed initially (25/29, 86.2%), not treated by gastric lavage (27/29, 93.1%), and developed severe hemorrhage. While most children in the low-dose were younger than 6 years (26/28, 92.9%), all have experienced accidental exposure, arrived at the hospital and received gastric lavage within 24 h, obtained a definite diagnosis, and be asymptomatic.
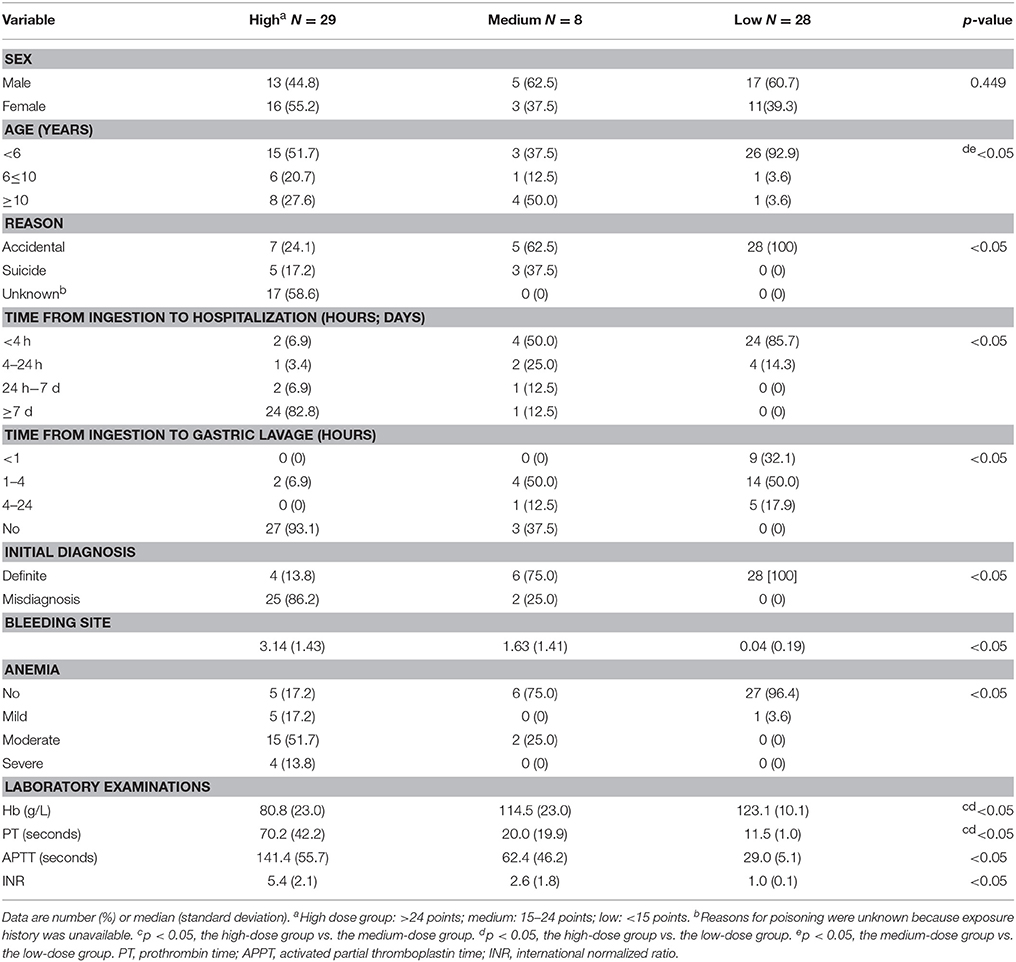
Table 3. Demographics and clinical characteristics of high, medium, and low dose group.
In the low-dose group, 24 of 28 patients usually consumed a few granules or had a “taste” of the rodenticides and did not develop coagulopathy. Although ingested large amounts (0.5–6 mL), the other four patients were also classified in the low-dose group and only one microscopic hematuria was observed. This might be because all of them were administered gastric lavage within an hour or plasmapheresis in the early phase, or both.
As shown in Table 4, accidental exposure patients were younger than 6 years (34/40, 85.0%), and have taken baits (23/40, 57.5%). In 8 intentional suicide patients, 7 cases were older than 10 years, other one was at 8 years and 9 months old, and all of them have ingested the concentrates.
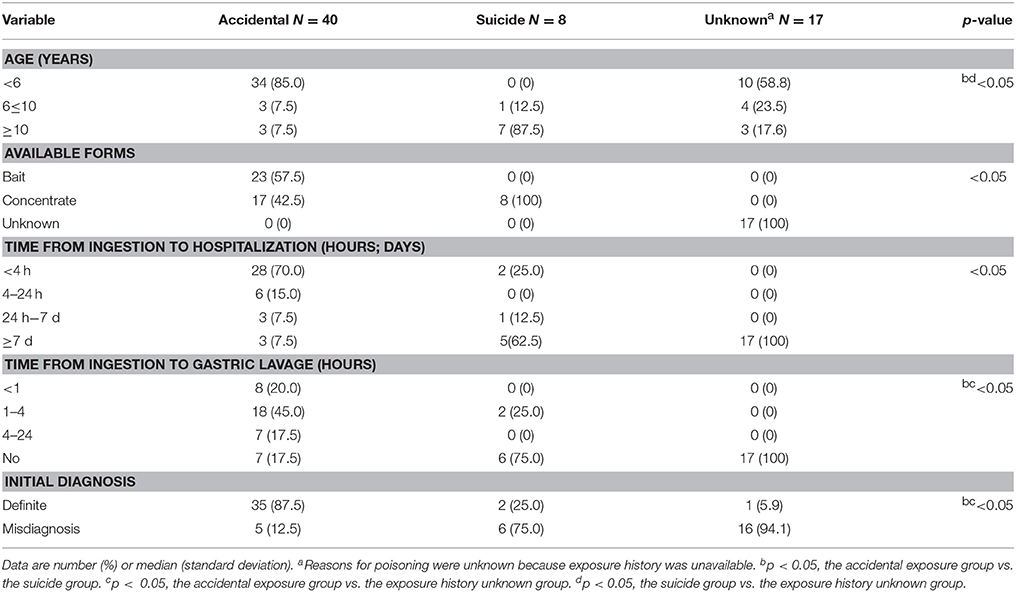
Table 4. Comparison of different reasons in children with 4-hydroxycoumarin intoxication.
Six of eight intentional suicide patients concealed what they ingested and 17 patients had no definite history of ingestion. These patients were more likely to arrive at the hospital after 24 h (suicide 6/8 and unknown 16/17), experience higher incidence of misdiagnosis (suicide 6/8 and unknown 16/17), thus not receive gastric lavage treatment (suicide 7/8 and unknown 17/17), and eventually be divided to high (suicide 5/8 and unknown 17/17), or medium (suicide 3/8) dose group than accidental exposure were. Moreover, since the parents of 5 accidental exposure patients did not realize the risk of consuming the agent, neither did provide exposure history to physicians on admission, their kids were also misdiagnosed initially, and were divided to high (4/5) or medium (1/5) dose finally. Of 27 misdiagnosed patients, 11 were misdiagnosed once, another 11 misdiagnosed twice, 2 misdiagnosed thrice, and remaining 3 misdiagnosed more than thrice. No exposure was identified in a one-year-old boy, leading to misdiagnosis with hemophilia. And it took 1 year to make a definite diagnosis using LC-MS/MS method.
Firstly, the AUROC, Youden index, sensitivity, and specificity were calculated to determine the predictability for coagulopathy of TDCH (Table 5). Of 38 patients arrived at hospital within 48 h, patients a score48h ≥ 15 had higher incidence of coagulopathy (6/8, 75.0%) than patients with a score48h < 15 (3/30, 10.0%). The AUROC, Youden index, sensitivity and specificity were 0.912, 0.727, 0.727, 1.000, respectively, which showed middle sensitivity and high specificity in predicting for coagulopathy of TDCH. 27 patients who arrived at hospital after 48 h all presented with coagulopathy when admitted. So we did not use TDCH to predict coagulopathy in these patients.
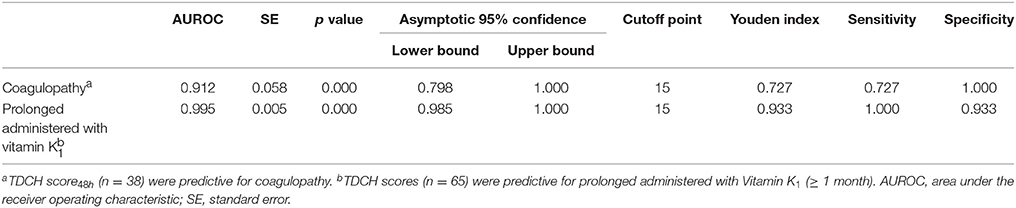
Table 5. Predictability of TDCH.
Secondly, the predictability for prolonged administration with vitamin K1 (≥ 1 month) of TDCH was analyzed by AUROC. Of all patients, 37 in the high and medium dose group with a score ≥ 15 has higher incidence (35/37, 94.6%) of prolonged administration with vitamin K1 (≥ 1 month) than other 28 patients with a score < 15 (0/28, 0%). The AUROC, Youden index, sensitivity and specificity were 0.995, 0.933, 1.000, 0.933, respectively. The results above showed high predictability for prolonged administration with vitamin K1.
We introduced a novel evaluation system for the determination of toxic dose in children with 4-hydroxycoumarin rodenticide intoxication. In this study, deliberate suicide patients (8/8, 100%) presented with obvious hemorrhage and were divided to high or medium dose group, while (28/40, 70%) accidental exposure patients were often asymptomatic and were divided to low dose. Our observations were consistent with an analysis of the American Association of Poison Control Centers' National Poison Data System (NPDS) showing that intentional exposures had a greater frequency of serious outcomes than unintentional exposures did (11). In addition, we found that 17 patients whose exposure information was unavailable all presented with severe hemorrhage and were divided to high dose. Interestingly, 18 patients younger than 6 years were divided into the high or medium group in our study. They presented with coagulopathy, inconsistent with a previous study showing that preschool-aged children with unintentional acute exposure to superwarfarin rodenticides would not likely develop any significant coagulation abnormalities (12). Of the 18 patients, ten denied ingestion of rodenticides and, therefore, they were not administered with gastric lavage. Five with accidental exposures ingested large amounts of concentrations (ranging from 0.5 to 2.5 mL), and three of the five subjects were administered with gastric lavage within 4 h. The remaining three with accidental exposures ingested unclear amounts and only one of them received gastric lavage. Ingestion of large amounts and delayed treatment may be the main causes of coagulopathy in these patients.
Misdiagnosis is the most common clinical challenge of 4-hydroxycoumarin rodenticide poisoning. It mainly occurred both in intentional suicide patients (6/8, 75.0%) and those who had no definite history of ingestion (16/17, 94.1%). The key element of diagnosis, the history of ingestion, is often unavailable in these patients. As a result, misdiagnosis and delayed treatment are common, often leading to severe consequences. 4-Hydroxycoumarin rodenticide poisoning is usually misdiagnosed as hemophilia when it occurs in little children without a definite history of ingestion. Because the onset is insidious, the hemorrhage is prolonged and recurrent, and factors IX and X is decreased. Anticoagulant rodenticides poisoning should be considered in cases of unexplained multi-site bleeding and vitamin K-dependent coagulation disorder. The key to avoiding misdiagnosis is to obtain a clear history of rodenticides ingestion or have access to a toxicology screen, such as LC-MS/MS.
The TDCH could evaluate toxic doses, predict coagulopathy in the early and guide the administration of vitamin K1. Limited studies have shown that a child weighing 10 kg would need to acutely ingest a minimum of 0.15 mg/kg of brodifacoum for coagulopathy to develop (13). However, four of our patients ingested large amounts of rodenticides, but they did not present with obvious coagulopathy because of the timely gastric lavage and plasmapheresis. Thus, the amount ingested could not be predictive of coagulopathy. Using TDCH, we found patients with a score48h ≥ 15 were in the high bleeding risk category. Early identification of these patients is crucial for not only promoting precise early treatment of high-risk patients, but also avoiding unnecessary examinations and treatments in those with low risks. For high-risk patients, vitamin K1 should be administered preventively as soon as possible. Up to now, there was no clear consensus on the appropriate use of vitamin K1 (14). According to a literature review (7), the duration of vitamin K1 ranged from 28 days to 730 days. And in our observation, patients with obvious coagulopathy required vitamin K1 at least for one month because of ongoing bleeding or coagulopathy. So we chose longer than a month as the length of vitamin K1 treatment. We found that patients in the high and medium dose with TDCH scores ≥ 15 required treatment with vitamin K1 for more than a month. With an AUROC of 0.995 and sensitivity of 0.933 and specificity of 1.000, the TDCH has high predictability.
However, this study still has some limitations. First, most diagnoses were based on the history of exposure to the rodenticides without qualitative identification of 4-hydroxycoumarin. Qualitative identification of 4-hydroxycoumarin in the blood was performed only in some patients, and none of the patients were subjected to quantitative analysis of the toxin. But this measurement is not currently widely performed even in the developed countries. Quantitative analyses, which can objectively reflect the toxic in vivo dose, are gold standard criteria for diagnosis. The TDCH could be further developed by using quantitative analyses. Second, the number of patients was insufficient in our study, and the TDCH score should be further verified and improved in larger, prospective studies.
The TDCH system is not only suitable for evaluating toxic doses on admission and predicting the risk of coagulopathy in the early stage, but also helps to appropriate treatment. Using TDCH, we found patients with a score48h ≥ 15 were in the high bleeding risk category. And patients with a scores ≥ 15 required treatment with vitamin K1 for more than a month. It is a simple and non-invasive method, and can be widely used in all areas, especially in developing countries. We hypothesize that modified TDCH can also be applied to other intoxication in children.
ZW designed and conducted the studies, edited the manuscript, PI of the funding; LY collected and analyzed the data, and drafted the manuscript; HZ and HG collected the data and edited the manuscript; YG and LC analyzed the data and edited the manuscript. All authors approved the final manuscript.
This work was supported by grants from the National Natural Science Foundation of China (No. 0388015, 39870747, 81370807).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer CO and handling Editor declared their shared affiliation.
1. Hadler MR, Shadbolt RS. Novel 4-hydroxycoumarin anticoagulants active against resistant rats. Nature (1975) 253:275–7. doi: 10.1038/253275a0
2. Lipton RA, Klass EM. Human ingestion of a 'superwarfarin' rodenticide resulting in a prolonged anticoagulant effect. JAMA (1984) 252:3004–5. doi: 10.1001/jama.1984.03350210052030
3. Sarin S, Mukhtar H, Mirza MA. Prolonged coagulopathy related to superwarfarin overdose. Ann Intern Med. (2005) 142:156. doi: 10.7326/0003-4819-142-2-200501180-00024
4. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet (2005) 365:552–3. doi: 10.1016/S0140-6736(05)70773-X
5. Hellemans J, Vorlat M, Verstraete M. Survival time of prothrombin and factors VII, IX and X after completely synthesis blocking doses of coumarin derivatives. Br J Haematol. (1963) 9:506–12. doi: 10.1111/j.1365-2141.1963.tb05475.x
6. Ingels M, Lai C, Tai W, Manning BH. A prospective study of acute, unintentional, pediatric superwarfarin ingestions managed without decontamination. Ann Emerg Med. (2002) 40:73–8. doi: 10.1067/mem.2002.125449
7. Caravati EM, Erdman AR, Scharman EJ, Woolf AD, Chyka PA, Cobaugh DJ, et al. Long-acting anticoagulant rodenticide poisoning: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol. (2007) 45:1–22. doi: 10.1080/15563650600795487
8. Patocka J, Petroianu G, Kuca K. Toxic potential of superwarfarin: Brodifacoum. Mil. Med. Sci. Lett. (2013) 82:32–7.
9. Schaff JE, Montgomery MA. An HPLC-HR-MS-MS method for identification of anticoagulant rodenticides in blood. J Anal Toxicol. (2013) 37:321–5. doi: 10.1093/jat/bkt036
10. Bolton-Maggs P, Moon I. Assessment of UK practice for management of acute childhood idiopathic thrombocytopenic purpura against published guidelines. Lancet (1997) 350:620–3. doi: 10.1016/S0140-6736(97)04143-3
11. Mowry JB, Spyker DA, Brooks DE, Zimmerman A, Schauben JL. 2015 Annual Report of the American Association of Poison Control Centers' National Poison Data System (NPDS): 33rd Annual Report. Clin Toxicol. (2016) 54:924–1109. doi: 10.1080/15563650.2016.1245421
12. Mullins ME, Brands CL, Daya MR. Unintentional pediatric superwarfarin exposures: do we really need a prothrombin time? Pediatrics (2000) 105:402–4. doi: 10.1542/peds.105.2.402
13. Smolinske SC, Scherger DL, Kearns PS, Wruk KM, Kulig KW, Rumack BH. Superwarfarin poisoning in children: a prospective study. Pediatrics (1989) 84:490–4.
Keywords: 4-hydroxycoumarins, rodenticide, poisoning, child, Vitamin K1, acquired coagulopathy
Citation: Ye L, Wang Z, Zhang H, Guo H, Guo Y and Chen L (2018) Application of a New Established System for Toxic Doses in Children With 4-Hydroxycoumarin Rodenticide Intoxication. Front. Pediatr. 6:141. doi: 10.3389/fped.2018.00141
Received: 21 September 2017; Accepted: 26 April 2018;
Published: 15 May 2018.
Edited by:
John Joseph Strouse, Duke University, United StatesReviewed by:
Daniele Zama, Policlinico S. Orsola Malpighi, ItalyCopyright © 2018 Ye, Wang, Zhang, Guo, Guo and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zheng Wang, d2FuZ3poZW5nNDhAMjFjbi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.